For an overview and description of Transfeminine Science, please visit our Home page.
Authors
The authors for Transfeminine Science include Aly, Lain, Sam, Mitzi, and Luna.
Aly
Aly (“she/her”) is a transgender woman from California. She has long had a passionate interest in transfeminine hormone therapy and pharmacology generally. Aly began her transition in the early 2010s and has studied the transgender medical literature since. She has a bachelor’s degree with summa cum laude distinction from a University of California. Aly also completed some of the pre-medicine curriculum and worked for about a year as an appointed volunteer faculty member in research labs at the university. Aside from medical areas, Aly has experience with computer programming and web development.
Aly was a volunteer editor on Wikipedia for many years. She was a prolific medical editor at the online encyclopedia and contributed a large amount of content in the area of sex hormone pharmacology over time. Since then, Aly decided to retire from Wikipedia editing. When Aly has included inline citations to Wikipedia on Transfeminine Science, they have usually been to content that she herself authored.
Lain (“they/them”) is non-binary and transfeminine. They completed a bachelor’s degree in applied mathematics and studied bioinformatics and computational biology at the Rochester Institute of Technology in New York. After withdrawing from their Ph.D. program, Lain migrated to the much warmer climes of the San Francisco Bay Area to work in tech.
As a person entrenched in nightlife community, specifically raving, Lain reformed and ran a nightlife harm reduction non-profit chapter for over 3 years, Bay Area DanceSafe. At DanceSafe they produced harm reductive literature on pertinent drugs and organized harm reduction booths at various festivals and raves. Through this direct outreach to the nightlife community, Lain led volunteers providing peer education on drugs, consent, sex education, and other pertinent topics as well as substance adulterant testing and harm reduction interventions. As a chapter head, they advocated for the normalization of harm reduction and the reform of drug policy working with peer organizations such as the Drug Policy Alliance (DPA), the Students for Sensible Drug Policy (SSDP), the Multidisciplinary Association for Psychedelic Studies (MAPS), and also by speaking at several events in the Bay Area.
As Lain began to medically transition, they began to passionately research endocrinology and transgender medicine and became involved with Transfeminine Science for a few years.
Sam (“she/her”) is a transgender woman from London, United Kingdom. She has no formal medical or research qualifications, but has an intense interest in evidence-based medicine and adherence to the scientific method. Her major interests in transgender health include the relatively uncommon to rare adverse effects of hormone therapy in transfeminine people, such as thromboembolism and other cardiovascular diseases. Specifically, she is interested in how the safety of different hormone therapy medications and dosages might compare. Sam read and kept up to date with the formal medical literature since she began to hormonally transition in 2018. She was involved with Transfeminine Science for a few years and contributed several articles to the site.
Mitzi (“she/they”) is a non-binary transfeminine person who lives in London, United Kingdom. She is prolifically active in DIY HRT communities, where she acts as an educator and advocates a harm reduction approach to self-medication. Mitzi frequently navigates situations that involve transgender homelessness, domestic violence, healthcare discrimination, and substance use both online and locally, and has held advisory roles for a variety of small grassroots organizations, including Trans Healthcare Network, Gender Construction Kit, and Bluelight.
Mitzi has a broad interest in medical academia, with a particular passion for endocrinology and psychopharmacology. She is an outspoken critic of her country’s transgender healthcare system, and has self-medicated for the duration of her own transition.
Transfeminine Science is no longer accepting contact inquiries. For questions and advice about hormone therapy, please refer instead to the online transgender community.
History
Transfeminine Science originated from the informational content on transfeminine hormone therapy that was created by transfeminine people in the transgender hormone therapy community on the social media website Reddit. Aly began creating content in August 2018, with other authors soon joining the effort. A couple years later, Aly developed and founded Transfeminine Science, which was launched in October 2020, and the existing content on Reddit was adapted and moved to the site. Transfeminine Science has served as a dedicated platform for the articles and for new content since it was started.
Disclaimer
The writers of Transfeminine Science are not medical professionals, academic researchers, or recognized experts in transgender health. Transfeminine Science articles emulate the format of scientific journal articles because this is an excellent format for scientific writing. However, it should be noted that Transfeminine Science itself is not a scientific journal and the content on this site has not been formally published nor scholarly peer-reviewed. Readers should not take the content on Transfeminine Science as authoritative. Instead, it should be considered as a supplementary resource to the information contained in transgender care guidelines and the medical literature in general.
Transfeminine Science is not specifically aimed at transfeminine people on do-it-yourself (DIY) hormone therapy. Rather, it is intended for transfeminine people on hormone therapy generally, as well as for medical providers and academics in transgender health. The authors of Transfeminine Science feel that wherever possible, decisions about medical care should be made in partnership with a health care professional. We recognize that this is not the case for many however, due to choice or circumstances, and we aim to help inform this important and undeserved community of individuals as well.
License
Transfeminine Science is copyright of Aly and the other authors of Transfeminine Science. We reserve all rights. We ask that readers please don’t reproduce content from Transfeminine Science unless given permission from Aly (e.g., for translation projects). If permission to reproduce content has been given, we ask that the content be appropriately attributed and linked back to the original page(s) on this site.
\ No newline at end of file
+About - Transfeminine Science
For an overview and description of Transfeminine Science, please visit our Home page.
Authors
The authors for Transfeminine Science include Aly, Lain, Sam, Mitzi, and Luna.
Aly
Aly (“she/her”) is a transgender woman from California. She has long had a passionate interest in transfeminine hormone therapy and pharmacology generally. Aly began her transition in the early 2010s and has studied the transgender medical literature since. She has a bachelor’s degree with summa cum laude distinction from a University of California. Aly also completed some of the pre-medicine curriculum and worked for about a year as an appointed volunteer faculty member in research labs at the university. Aside from medical areas, Aly has experience with computer programming and web development.
Aly was a volunteer editor on Wikipedia for many years. She was a prolific medical editor at the online encyclopedia and contributed a large amount of content in the area of sex hormone pharmacology over time. Since then, Aly decided to retire from Wikipedia editing. When Aly has included inline citations to Wikipedia on Transfeminine Science, they have usually been to content that she herself authored.
Lain (“they/them”) is non-binary and transfeminine. They completed a bachelor’s degree in applied mathematics and studied bioinformatics and computational biology at the Rochester Institute of Technology in New York. After withdrawing from their Ph.D. program, Lain migrated to the much warmer climes of the San Francisco Bay Area to work in tech.
As a person entrenched in nightlife community, specifically raving, Lain reformed and ran a nightlife harm reduction non-profit chapter for over 3 years, Bay Area DanceSafe. At DanceSafe they produced harm reductive literature on pertinent drugs and organized harm reduction booths at various festivals and raves. Through this direct outreach to the nightlife community, Lain led volunteers providing peer education on drugs, consent, sex education, and other pertinent topics as well as substance adulterant testing and harm reduction interventions. As a chapter head, they advocated for the normalization of harm reduction and the reform of drug policy working with peer organizations such as the Drug Policy Alliance (DPA), the Students for Sensible Drug Policy (SSDP), the Multidisciplinary Association for Psychedelic Studies (MAPS), and also by speaking at several events in the Bay Area.
As Lain began to medically transition, they began to passionately research endocrinology and transgender medicine and became involved with Transfeminine Science for a few years.
Sam (“she/her”) is a transgender woman from London, United Kingdom. She has no formal medical or research qualifications, but has an intense interest in evidence-based medicine and adherence to the scientific method. Her major interests in transgender health include the relatively uncommon to rare adverse effects of hormone therapy in transfeminine people, such as thromboembolism and other cardiovascular diseases. Specifically, she is interested in how the safety of different hormone therapy medications and dosages might compare. Sam read and kept up to date with the formal medical literature since she began to hormonally transition in 2018. She was involved with Transfeminine Science for a few years and contributed several articles to the site.
Mitzi (“she/they”) is a non-binary transfeminine person who lives in London, United Kingdom. She is prolifically active in DIY HRT communities, where she acts as an educator and advocates a harm reduction approach to self-medication. Mitzi frequently navigates situations that involve transgender homelessness, domestic violence, healthcare discrimination, and substance use both online and locally, and has held advisory roles for a variety of small grassroots organizations, including Trans Healthcare Network, Gender Construction Kit, and Bluelight.
Mitzi has a broad interest in medical academia, with a particular passion for endocrinology and psychopharmacology. She is an outspoken critic of her country’s transgender healthcare system, and has self-medicated for the duration of her own transition.
Transfeminine Science is no longer accepting contact inquiries. For questions and advice about hormone therapy, please refer instead to the online transgender community.
History
Transfeminine Science originated from the informational content on transfeminine hormone therapy that was created by transfeminine people in the transgender hormone therapy community on the social media website Reddit. Aly began creating content in August 2018, with other authors soon joining the effort. A couple years later, Aly developed and founded Transfeminine Science, which was launched in October 2020, and the existing content on Reddit was adapted and moved to the site. Transfeminine Science has served as a dedicated platform for the articles and for new content since it was started.
Disclaimer
The writers of Transfeminine Science are not medical professionals, academic researchers, or recognized experts in transgender health. Transfeminine Science articles emulate the format of scientific journal articles because this is an excellent format for scientific writing. However, it should be noted that Transfeminine Science itself is not a scientific journal and the content on this site has not been formally published nor scholarly peer-reviewed. Readers should not take the content on Transfeminine Science as authoritative. Instead, it should be considered as a supplementary resource to the information contained in transgender care guidelines and the medical literature in general.
Transfeminine Science is not specifically aimed at transfeminine people on do-it-yourself (DIY) hormone therapy. Rather, it is intended for transfeminine people on hormone therapy generally, as well as for medical providers and academics in transgender health. The authors of Transfeminine Science feel that wherever possible, decisions about medical care should be made in partnership with a health care professional. We recognize that this is not the case for many however, due to choice or circumstances, and we aim to help inform this important and undeserved community of individuals as well.
Recognition
Transfeminine Science has been cited, mentioned, and/or recognized in the published scientific literature by various academics. A partial list of these instances, with citations and excerpts, can be found here.
License
Transfeminine Science is copyright of Aly and the other authors of Transfeminine Science. We reserve all rights. We ask that readers please don’t reproduce content from Transfeminine Science unless given permission from Aly (e.g., for translation projects). If permission to reproduce content has been given, we ask that the content be appropriately attributed and linked back to the original page(s) on this site.
\ No newline at end of file
diff --git a/transfemscience.org/articles/cpa-dosage/index.html b/transfemscience.org/articles/cpa-dosage/index.html
index 1af36c15..aac59973 100644
--- a/transfemscience.org/articles/cpa-dosage/index.html
+++ b/transfemscience.org/articles/cpa-dosage/index.html
@@ -1 +1 @@
-Low Doses of Cyproterone Acetate Are Maximally Effective for Testosterone Suppression in Transfeminine People - Transfeminine Science
Low Doses of Cyproterone Acetate Are Maximally Effective for Testosterone Suppression in Transfeminine People
By Aly | First published July 1, 2019 | Last modified March 30, 2024
Abstract / TL;DR
Cyproterone acetate (CPA) is a progestogen and antiandrogen which is widely used in transfeminine hormone therapy. It is far more potent as a progestogen than as an androgen receptor antagonist. CPA has typically been used at doses of 1 to 2 mg/day as a progestogen in cisgender women and at doses of 50 to 300 mg/day as an antiandrogen. At typical antiandrogen doses of CPA, there is profound progestogenic overdosage as well as associated side effects and risks. CPA has antigonadotropic effects due to its progestogenic activity and thereby suppresses testosterone levels. By itself, CPA can maximally suppress testosterone levels by 50 to 70%, and in combination with even small amounts of estrogen, it can fully suppress gonadal testosterone production and thereby reduce testosterone levels by about 95%—or well into the female range. Although doses of CPA of 50 to 100 mg/day have been used in transfeminine people historically, it is now clear that 5 to 10 mg/day CPA has maximal or near-maximal effectiveness in terms of suppression of testosterone levels. CPA alone is most commonly available as 50-mg tablets. These tablets can be split with a pill cutter and taken once every day to once every other day to achieve an overall CPA dosage of 6.25 to 12.5 mg/day. These lower doses of CPA are not only much more cost-effective than traditional doses but are also likely to have better tolerability and safety. Due to the retained effectiveness of lower CPA doses and the known dose-dependent risks of CPA, doses of CPA used clinically in transfeminine people have been in a rapid decline.
Introduction
This article is about the dosage of cyproterone acetate (CPA), a progestin and antiandrogen, for use in hormone therapy for transfeminine people. It argues for the use of lower doses of CPA and goes fairly in-depth to justify these doses. If you are only interested in recommended doses of CPA for transfeminine people, they can be found in the Recommended Dosages section below.
Potency, Conventional Dosages, and Health Risks
CPA is a potent progestogen, with an ovulation-inhibiting dosage of about 1 mg/day and endometrial transformation dosage of about 1 to 3 mg/day in cisgender women (Wiki; Table; Endrikat et al., 2011). These dosages of CPA are similar in strength of progestogenic effect to those of normal progesterone production and levels during the luteal phase of the menstrual cycle in premenopausal women (which are about 25 mg/day and 15 ng/mL, respectively). In relation to the preceding, when CPA is used as a progestogen in cisgender women, for instance in birth control pills and menopausal hormone therapy preparations, it is formulated at a dose of 1 or 2 mg per tablet (Wiki).
In contrast to its progestogenic activity, CPA is far less potent as an androgen receptor antagonist (Wiki). When used as an antiandrogen, it is generally given at a dosage of 50 to 300 mg/day, both in cisgender women and men. A dosage of 50 to 100 mg/day is typical for androgen-dependent skin and hair conditions like acne and hirsutism in women and a dosage of 100 to 300 mg/day is typically used for prostate cancer in men (specifically 100–200 mg/day for CPA combined with castration and 200–300 mg/day for CPA monotherapy) (Wiki). As such, CPA is generally formulated at a dose of 50 or 100 mg per tablet for use in androgen-dependent conditions (Wiki). As an antiandrogen, CPA has a dual mechanism of action of both suppressing testosterone levels via its progestogenic activity at low doses and additionally blocking the actions of testosterone directly at the androgen receptor at higher doses.
Because CPA is so much more potent as a progestogen than as an androgen receptor antagonist, there is profound overdosage of progestogenic effect when CPA is used as an antiandrogen at typical clinical dosages. This is described in the following three literature excerpts by Jürgen Hammerstein, one of the scientists who developed CPA (Hammerstein et al., 1975; Hammerstein, 1990; Hammerstein, 1979):
Like chlormadinone acetate, its parent compound, CPA is also a strong progestogen with the endometrial transformation dose of both drugs being between 20 and 30 mg. […] To take full therapeutic advantage of its antiandrogenicity, CPA must be administered in doses per month that are 30 times the physiological equivalent of progesterone production in the cycle. CPA, although the most useful compound available in this field at the moment, cannot be considered therefore an ideal antiandrogen, all the more as some of the side effects may be related to the progestational overdosage rather than to the administered antiandrogenic activity. […] Adverse reactions like tiredness, lassitude, and increase in body weight are possibly due to the enormous overdose of progestational activity in the formula which is necessary to take full advantage of the antiandrogenicity of CPA.
Fixson (1963) tested CPA in ovariectomized women after pre-treatment with oestrogens; with a transformation dose of 20–30 mg this proved a powerful progestogen. The potency of CPA in the menses delay test is not exactly known, but has been estimated to be below 1 mg/day (Miller and Jacobs 1986). In relation to this progestational potency, its antiandrogenicity must be considered rather weak. Thus, in order to take full advantage of the latter, 100 mg CPA must be given daily, i.e. three times the cyclic transformation dose per day (Hammerstein and Cupceancu 1969); notably, this parameter is equivalent to the total progesterone production of a corpus luteum throughout its entire cyclic life span.
CPA may be characterized endocrinologically as possessing strong progestational [and] moderate anti-androgenic […] potencies. […] Its progestational activity, in terms of the transformation dose in the oestrogen-primed human endometrium, is 20–30 mg [per month/cycle] which is comparable to that of chlormadinone acetate and other strong progestogens. To take full clinical advantage of its anti-androgenicity not less than 50–100 mg CPA must be taken orally per day, which totals 2 to 3 times the progestational activity the female organism is exposed to throughout a complete ovulatory menstrual cycle. Thus unless much lower and less efficacious doses of CPA are used, a tremendous progestational overdosage must be accepted. […] As already pointed out CPA is endocrinologically not a well-balanced compound because of the strong preponderance of the progestational over the anti-androgenic potency. A way to avoid the heavy progestogen overdosage inherent with the high-dose reverse sequential therapy would be to combine the low-dose contraceptive formulation just mentioned with a pure anti-androgen such as free cyproterone. […] It must be emphasized that CPA is far from being an ideal drug for the anti-androgenic treatment of hirsutism because its progestational potency is much too strong and it is not effective when administered topically. Therefore it is worthwhile looking for better-balanced anti-androgenic compounds for the future.
The massive overdosage of progestogenic effect that occurs at such doses of CPA is likely responsible for the known adverse effects and risks of higher doses of CPA (Wiki). Examples of these side effects include fatigue, depression, weight gain, high prolactin levels (Wiki), benign brain tumors (Aly, 2020; Wiki; Table; Table), blood clots (Wiki), and cardiovascular problems (Wiki). Such risks are dose-dependent and have not been associated with 1 or 2 mg/day CPA (with the exception of an expected increase in the risk of blood clots in combination with oral estrogens for birth control or menopausal hormone therapy). The risk of liver toxicity with CPA is also dose-dependent, with elevated liver enzymes occurring mostly only at a dosage of 20 mg/day and above and rare cases of liver failure occurring almost exclusively at dosages of 100 mg/day and above (Wiki; Table). As such, there is good rationale for using the lowest possible effective dosage of CPA, an approach that is likely to minimize risks.
In transfeminine people, CPA has historically been used at a dosage of 50 to 100 mg/day (e.g., Moore, Wisniewski, & Dobs, 2003). Some earlier papers have recommended even higher doses of CPA, for instance 100 to 150 mg/day (Asscheman & Gooren, 1993). In 2017, the Endocrine Society published the latest edition of their clinical practice guidelines on hormone therapy for transgender people and reduced their recommended dosage of CPA from 50–100 mg/day to 25–50 mg/day (Hembree et al., 2017; Hembree et al., 2009). This was motivated in part by increasing knowledge and awareness of the risks of higher doses of CPA and by findings that these lower doses of CPA were still effective. However, it is likely that even these new lower dosages are still far in excess of what is really needed.
Testosterone Suppression with Low and High Doses
Progestogens by themselves, including CPA, are able to considerably suppress testosterone levels in gonadally intact people assigned male at birth. Around a dozen small and low-quality but nonetheless notable studies of low-dose CPA from the 1970s and early 1980s found that 5 to 10 mg/day CPA suppressed testosterone levels by about 40 to 70% in healthy young men (Table 1). A couple of individual studies notably reported virtually identical suppression of testosterone levels with 5 mg/day versus 10 mg/day CPA (both ~50% suppression) (Wang & Yeung, 1980; Graph) and with 10 mg/day versus 20 mg/day CPA (both ~60–70% suppression) (Koch et al., 1976; Koch et al., 1975; Graph). This lack of additional testosterone suppression with a doubling of dosage within studies suggests that testosterone suppression with CPA might have actually been maximal at a dosage of only 5 or 10 mg/day. A more modern study, which used a newer and more reliable analytic method for quantification of blood testosterone, found that 10 mg/day CPA suppressed testosterone levels by 66%, from about 600 ± 150 ng/dL to about 185 ng/dL (Meriggiola et al., 2002a; Graph). Similarly, another more modern study found that 10 to 20 mg/day CPA suppressed testosterone levels by 65%, from about 431 ng/dL to about 149 ng/dL, with no reported differences between doses (Zitzmann et al., 2017; Graph).
Table 1: Levels of testosterone and other sex hormones with CPA at low doses (5–30 mg/day):
Treatment and subjects
Findings
Source(s)
30 mg/day CPA in 5 normal males
T decreased “remarkably”. Exact values not given, but has graphs of T levels in a few individuals. After 30 mg/day, 5 mg/day was tried in one case and was not as effective in suppressing sperm production or T. Also reported decreases in gonadotropin excretion.
10 or 20 mg/day CPA in 15 normal healthy fertile males (age 25–35 years) (7 in 10 mg/day group and 8 in 20 mg/day group)
“Androgens (mainly T)” decreased by 60% for both 10 and 20 mg/day. Inconsistent changes in LH and slight decrease in FSH. Exact values not given, except in graphs.
10 mg/day CPA in 10 young healthy fertile men (age mean 27.2 ± 3.2 (range 21–35) years)
T decreased by 70%, DHT by 50%, LH by 30%, and FSH by 40%, while PRL increased by 75%. T was 495 ± 66 ng/dL before, 154 ± 23 ng/dL after 4 weeks, and 187 ± 38 ng/dL after 12 weeks. Also has values and graphs for other hormones.
20 mg/day CPA in 10 healthy males (age 26–55 years)
T decreased by 73% (range 71–75%), from 482 ng/dL (range 410–560 ng/dL) to 130 ng/dL (110–162 ng/dL). DHT decreased by 51% (range 47–55%), LH by 39% (range 34–45%), FSH by 66% (range 47–78%), 17-OH-P4 by 59%, A4 by 30%, TS by 34%, and DHTS by 35%. Also has exact values and graphs for other hormones.
5 or 10 mg/day CPA in 7 males (4 in each group; 1 received both 5 and 10 mg/day CPA at different times)
T change was “−40%” or “–50%”. At 5 mg/day, T was 745 ng/dL before, 460 ng/dL with treatment (–38%), and 668 ng/dL after discontinuation. At 10 mg/day, T was 708 ng/dL before, 398 ng/dL with t (reatment–44%), and 670 ng/dL after discontinuation. Also reported LH and FSH levels.
0, 5, or 10 mg/day CPA in 25 normal healthy males (age 20–51 years); 7 in 5 mg group (mean 37 ± 10 years), 8 in 10 mg group (mean 32 ± 8 years), 10 in 0 mg group (mean 32 ± 10 years)
At 5 mg/day, T decreased from 663 ± 120 ng/dL to 320 ± 160 ng/dL (−52%), and at 10 mg/day, T decreased from 692 ± 180 ng/dL to 340 ± 160 ng/dL (−51%). E2 decreased in parallel to T. At 5 mg/day, LH decreased from 2.1 ± 0.7 IU/L to 1.4 ± 0.5 IU/L (−33%), and at 10 mg/day, LH decreased from 2.3 ± 1.0 IU/L to 1.2 ± 0.5 IU/L (−48%). At 5 mg/day, FSH decreased from 3.1 ± 1.9 IU/L to 1.8 ± 0.9 IU/L (−42%), and at 10 mg/day, FSH decreased from 2.7 ± 1.0 IU/L to 1.5 ± 0.7 IU/L (−44%).
10 or 25 mg/day CPA in 4 healthy men (age 29–37 years); 3 in 10 mg group, 1 in 25 mg group
T “slightly reduced”. E “more significantly lowered”. LH not significantly changed. FSH “reduced” in “more or less all cases”. Exact hormone levels not given, but graphs provided with the values.
10 mg/day CPA (also placebo and 2, 5, and 10 mg/day dienogest) in 5 healthy men in each group
With CPA, T decreased from ~600 ± 150 ng/dL to ~185 ng/dL (–66 ± 4%). Also reported LH, FSH, and SHBG, as well as hormonal changes with placebo and dienogest (2, 5, and 10 mg/day).
10 or 20 mg/day CPA in 14 healthy young men (7 in each group)
T decreased from ~431 ng/dL at baseline to ~149 ng/dL with CPA (–65%) for the 10 and 20 mg/day doses combined. Values for dose subgroups not given. No significant differences between LH/FSH suppression between groups (which is indirectly suggestive of no differences in T suppression as well). Also reported hormone levels with other progestins.
Studies with other progestogens, such as desogestrel, dienogest, and medroxyprogesterone acetate, have consistently found that maximal suppression of testosterone levels in men occurs at a dosage that is between 5 and 10 times that of the ovulation-inhibiting dosage in cisgender women (Wiki; Wiki; Wiki). Another study is likewise suggestive of this for norethisterone acetate and levonorgestrel (Zitzmann et al., 2017; Graph). Along similar lines, doses of progestogens investigated for use in male hormonal contraception, in which the goal is antigonadotropic effects and the lowest fully effective dose is targeted, have been noted as being between 5 and 12 times the doses used in cisgender women (Foegh, 1983). Based on an ovulation-inhibiting dosage of CPA of 1 mg/day, these findings would imply that suppression of testosterone levels with CPA would likely be maximal at a dose of between 5 and 10 mg/day. In accordance, this dose range matches up with the findings of the studies above.
Although progestogens can considerably suppress testosterone levels at maximally effective dosages, it has been found that a “recovery” or “escape phenomenon”, in which testosterone levels eventually increase back to higher levels, occurs when progestogen monotherapy is used on a long-term basis. This has most notably been observed with the related progestogen megestrol acetate (Wiki), but has also been seen with CPA (Goldenberg & Bruchovsky, 1991; Saborowski, 1987; Jacobi, Tunn, & Senge, 1982). In one of these studies, testosterone levels were initially suppressed by CPA by about 70%, but increased back to about 50% of baseline between 6 and 12 months of therapy, remaining stable thereafter up to 24 months. The testosterone escape phenomenon should be kept in mind in the context of progestogen monotherapy for testosterone suppression. In contrast to progestogen monotherapy, this phenomenon has not been associated with combined estrogen and progestogen therapy.
Testosterone Suppression in Combination with Estrogen
CPA is generally used in combination with an estrogen in transfeminine people. Estrogens suppress testosterone levels similarly to progestogens. The combination of an estrogen and a progestogen is synergistic in terms of testosterone suppression and results in suppression of testosterone levels with lower doses than with either an estrogen or progestogen alone (Fink, 1979; Geller & Albert, 1983; Bastianelli et al., 2018). Although estrogens can suppress testosterone levels to an equivalent extent as surgical or medical castration (i.e., orchiectomy or GnRH agonists/antagonists), this usually requires relatively high estrogen levels, for instance in the range of 200 to 500 pg/mL (Wiki; Graphs). Because of the high and supraphysiological estradiol levels required for maximal or near-maximal suppression of testosterone levels, lower doses of estradiol are frequently combined with antiandrogens and/or progestogens to block or suppress remaining testosterone levels instead.
CPA, as mentioned earlier, leads to an incomplete suppression of plasma testosterone levels, which decrease by about 70% and remain at about three times castration values. In a very systematic approach to the problem, Rennie et al. (59) investigated and compared 12 different procedures of androgen deprivation. These authors found that the combination of CPA with an extremely low dose (0.1 mg/d) of [diethylstilbestrol (DES)] led to a very effective withdrawal of androgens in terms of plasma testosterone and tissue dihydrotestosterone. The same group later showed that 200 mg of CPA, and even 100 mg/day, was sufficient to achieve a similar endocrine response, which was correlated to very favorable clinical responses in a Phase II situation (60,61). The approach has many potential advantages, and, from an endocrinological point of view, is very logical: this regimen combines the testosterone-reducing effects of two compounds, therefore, only small amounts of estrogen are required to bring down plasma testosterone to approximately castrate levels. Once castrate levels have been achieved, only low doses of CPA are necessary to counteract remaining androgens, mainly of adrenal origin. The regimen was shown to be associated with few side effects and a very low cost. The combination of low-dose CPA with low-dose DES was never studied in a Phase III situation in comparison to standard management. Considering the endocrine results and the observations in patients treated with this regimen (60), this combination treatment is very likely to be competitive with other standard forms of therapy.
A 2016 study of 50 mg/day CPA and 1 to 2 mg/day transdermal estradiol gel in transfeminine people showed that estradiol levels of about 45 pg/mL with CPA were insufficient to achieve female/castrate levels of testosterone, instead resulting in testosterone levels of about 120 to 190 ng/dL (Gava et al., 2016; Graph). Conversely, estradiol levels of about 85 pg/mL with CPA achieved complete suppression of gonadal testosterone production, with resulting testosterone levels of about 20 ng/dL. As such, a certain minimum level of estradiol with CPA appears to be required for complete testosterone suppression. A 2019 study of CPA and oral estradiol valerate in transfeminine people indicated that testosterone levels were still fully suppressed with median estradiol levels of 76 pg/mL and 25th percentile estradiol levels of 63 pg/mL (Angus et al., 2019; Graph).
Figures 5–7: Testosterone levels with CPA plus low doses/levels of estrogens in men and transfeminine people. Sources: Top-left: Goldenberg et al. (1988). Top-right: Gava et al. (2016). Bottom: Angus et al. (2019). See also on Wikipedia: Gallery. Note for the graph on the top right that the mean transdermal estradiol dosage increased between 6 and 12 months and this was likely responsible for the improvement in testosterone suppression.
Fung and colleagues showed that the combination of either 25 or 50 mg/day CPA with a moderate dosage of oral estradiol (~3.5 mg/day) or transdermal estradiol (~3.5 mg/day gel or ~100 μg/day patch) resulted in equivalent and complete suppression of gonadal testosterone production (~95% suppression of testosterone levels) in transfeminine people (Fung, Hellstern-Layefsky, & Lega, 2017). These dosages of estradiol would be expected to achieve estradiol levels of around 100 pg/mL on average (Aly, 2020; Wiki). This study was notably published 6 months before the 2017 second edition of the Endocrine Society guidelines were released (Hembree et al., 2017), and was probably responsible for the decrease in their recommended dosage of CPA from 50–100 mg/day to 25–50 mg/day.
Few studies to date have assessed testosterone suppression with low-dose CPA in combination with a low or moderate dosage of an estrogen. However, based on the fact that 5 to 10 mg/day CPA alone is probably maximal in terms of suppression of testosterone levels, it is likely that such dosages of CPA will be similarly effective as higher dosages. In accordance, studies of 5 to 12.5 mg/day CPA plus upper physiological replacement dosages of testosterone have demonstrated undetectable gonadotropin levels (<0.5 IU/L) and hence complete suppression of testicular function in healthy young men (Meriggiola et al., 1998; Meriggiola et al., 2002b). Estradiol is a more powerful antigonadotropin than testosterone (Wiki), so these findings probably apply to CPA in combination with physiological replacement levels of estradiol as well (e.g., mean estradiol levels of 100–200 pg/mL).
Accordingly, Meyer et al. (2020) assessed a dosage of CPA in combination with estradiol in 155 transfeminine people and found no difference in testosterone levels with 10, 25, or 50 mg/day CPA; testosterone levels were strongly suppressed with all three doses (to about 15–20 ng/dL on average, or into the lower end of the normal female range). The estradiol forms and doses used in this study were oral estradiol valerate (median 6 mg/day, range 3–10 mg/day), transdermal estradiol gel (median 2.25 mg/day, range 1.5–6 mg/day), and transdermal estradiol patches (100 μg/day in all cases). Estradiol levels were about 100 pg/mL on average, with an interquartile range (i.e., difference between 75th and 25th percentiles) of about 100 pg/mL. This study demonstrates that, provided estradiol levels are adequate, no more than 10 mg/day CPA is needed to fully suppress testosterone levels in transfeminine people. Another study likewise found no difference between <20 mg/day and >50 mg/day CPA in terms of testosterone suppression in transfeminine people (Even-Zohar et al., 2020).
Even doses of CPA lower than 5 mg/day (e.g., 2 mg/day) may be usefully effective for testosterone suppression if combined with sufficient levels of estradiol, although this has not been studied and remains to be validated. But there is certainly precedent for the notion when looking at studies with other progestogens. As an example, one study using 10 mg/day oral medroxyprogesterone acetate (which is roughly equivalent to 1 mg/day CPA in terms of ovulation inhibition in premenopausal women; Table) observed 63% lower testosterone levels (215 ng/dL vs. 79 ng/dL) when added to estradiol and spironolactone therapy in transfeminine people (Jain, Kwan, & Forcier, 2019). Analogous effects on testosterone levels would be anticipated for very-low-dose CPA. Moreover, such dosages of CPA would have the advantage of actually being physiological in terms of progestogenic exposure.
The androgen receptor antagonism of CPA is relatively weak in terms of potency; dosages of CPA of 50 to 300 mg/day seem to be necessary for meaningful or considerable androgen receptor antagonism. Unfortunately, such doses also result in extreme progestogenic overdosage and are associated with considerably greater risks and adverse effects. As a result, the use of such doses of CPA should no longer be considered advisable. Instead, CPA should be used at lower doses simply as a progestogen to suppress testosterone levels. As such, the highest effective dosage of CPA for testosterone suppression, which is probably about 10 mg/day or less (12.5 mg/day also being acceptable), should be around the maximal dosage of CPA that is used in transfeminine people.
It should be emphasized that since the combination of an estrogen and CPA can easily suppress testosterone levels well into the female/castrate range (typically to below average female levels), there isn’t necessarily a requirement for concomitant androgen receptor blockade. In any case, if androgen receptor antagonism to neutralize the remaining female/castrate levels of testosterone is still necessary or desired (e.g., to treat persisting acne or for some other purpose), a low dosage of a non-progestogenic androgen-receptor antagonist like spironolactone (e.g., 100–200 mg/day) or bicalutamide (e.g., 12.5–25 mg/day) can be added to CPA to more safely achieve this than use of higher CPA doses.
Recommended Dosages
Dosage for Testosterone Suppression
Estrogen Plus Cyproterone Acetate
The following recommended dosages of CPA in transfeminine people are for the combination of CPA with an estrogen and are specifically for achieving maximal suppression of testosterone levels:
Table 2: Recommended doses of CPA in combination with estrogen for maximal testosterone suppression in transfeminine people:
Form
Min. dosage
Max. dosage
Amount
10 mg tablets
5 mg/day
10 mg/day
1/2 of a tablet to 1 whole tablet per day
50 mg tablets
6.25 mg/day
12.5 mg/day
1/8th of a tablet to 1/4th of a tablet per day
Start with the minimum dosage of CPA for one month. After one month, have testosterone levels tested and confirm that they are in the normal female/castrate range (<50 ng/dL). Regardless of dosage, a concomitant minimum estradiol level of around 65 pg/mL needs to be attained in order to allow for complete suppression of testosterone levels with CPA. If testosterone levels aren’t sufficiently suppressed after a month and estradiol levels are adequate, increase to the maximum CPA dosage and re-check testosterone levels after another month. Alternatively, the dosage of estradiol can be increased instead; higher estradiol levels result in greater testosterone suppression as well.
Cyproterone Acetate Alone
The use of CPA alone (i.e., as a monotherapy for testosterone suppression) is not recommended due to the risk of decreased bone mineral density and other symptoms of sex-hormone deficiency (Wiki; Aly, 2019). In any case, the recommended dosages for CPA without an estrogen are essentially the same as those listed above of the combination of an estrogen with CPA for testosterone suppression. However, the higher CPA dose (10–12.5 mg/day) may be preferable for good measure in this scenario.
Dosage for Progestogenic Effects
The following recommended dosages of CPA in transfeminine people are for progestogenic effects similar to normal physiological exposure (equivalent of luteal-phase progesterone levels):
Table 3: Recommended doses of CPA for physiological progestogenic effects in transfeminine people:
Form
Dosage
Amount
10 mg tablets
2.5 mg/day
1/4th of a tablet per day
50 mg tablets
3.125 mg/day
1/16th of a tablet per day
Achieving Desired Dosages
CPA is available pharmaceutically most widely as 50-mg tablets. This can make achieving desired low doses of CPA more difficult. For splitting CPA tablets into small fractions, a pill cutter can be used. Additionally, CPA can be taken once every 2 or 3 days instead of once every day to help further divide doses. It is notable that CPA has a relatively long half-life in the body of about 1.5 to 2 days (but possibly up to 4 days) (Wiki; Graph). Hence, taking it once every other day instead of once per day, or even less frequently like once every 3 days, has sound basis and is likely to be entirely viable.
Updates
Update 1: GoLoCypro Study (In-Progress)
The GoLoCypro study (2019–2022) (more info) is being conducted by Dr. Judith Dean at the University of Queensland in Australia. It’s assessing the influence of estradiol plus CPA on testosterone levels at five different CPA dose levels (12.5 mg 2x/week, 12.5 mg/2 days, 12.5 mg/day, 25 mg/day, and 50 mg/day) in a total of 120 to 350 transfeminine people. CPA doses are being titrated to the minimum that maintain testosterone levels within the therapeutic goal range of 0.5 to 1.5 nmol/L (14–43 ng/dL). The study is among the first dose-ranging studies of CPA in transfeminine people to be conducted and is eagerly anticipated due to the valuable information that it should provide in terms of the minimum effective dosage of CPA for adequate testosterone suppression in transfeminine hormone therapy.
Update 2: Kuijpers et al. (2021) and Even Zohar et al. (2021)
Kuijpers, S. M., Wiepjes, C. M., Conemans, E. B., Fisher, A. D., T’Sjoen, G., & den Heijer, M. (2021). Toward a lowest effective dose of cyproterone acetate in trans women: Results from the ENIGI study. The Journal of Clinical Endocrinology & Metabolism, 106(10), e3936–e3945. [DOI:10.1210/clinem/dgab427]
The study employed estradiol (2–6 mg/day oral (as estradiol valerate), 50–150 μg/day patch, or gel) plus five different dose levels of CPA—0 mg/day (no CPA), 10 mg/day, 25 mg/day, 50 mg/day, and 100 mg/day. It found incompletely suppressed testosterone in the no CPA group but full and equivalent testosterone suppression with all doses of CPA. The results were as follows:
CPA dosage
0 mg/day
10 mg/day
25 mg/day
50 mg/day
100 mg/day
Initial subjects (n)
34
4
234
599
11
Dose increased (n)
16
1
11
2
0
Dose decreased (n)
0
0
4
40
7
T levels (nmol/L)
5.5
0.9
0.9
1.1
0.9
T levels (ng/dL)
~160
~26
~26
~32
~26
T <2 nmol/L [<~58 ng/dL] (%)
46.3
92.3
96.2
93.4
100.0
Abbreviations: T = testosterone.
The total numbers of subjects and blood tests after CPA dose increases/decreases were not provided. Hence, the exact total number of people and tests for the 10 mg/day group can’t be stated with certainty. The total number of tests for this group was at least 13 based on the testosterone suppression percentage provided however (92.3% or 12/13 but could potentially be 24/26, etc.). Regarding the small number of subjects/tests for the 10 mg/day group, the authors stated the following:
This study is part of the ENIGI initiative, a multicenter prospective cohort study. The main treatment protocol for trans women in this study was 50 mg of CPA daily combined with estrogens. In the first year of study inclusion, a few participants received a dose of 100 mg of CPA. Shortly thereafter, inhospital protocol changed to 50 mg of CPA. As more health concerns related to CPA use were raised over the years, the dose was further lowered from 50 mg to 25 mg and, finally, to 10 mg. However, due to the coronavirus (COVID-19) pandemic, limited results of participants with 10 mg of CPA were available for analysis.
Besides testosterone suppression, the study found that 10 mg/day CPA had less influence on prolactin and high-density lipoprotein (HDL) cholesterol levels than the higher doses of CPA. The study also assessed liver enzyme levels but found no differences between CPA doses.
The authors concluded with the following:
In conclusion, in this cohort of trans women, 10 mg of CPA was found to be effective in lowering testosterone concentrations to the range observed in cis women. A dose of 10 mg was equally effective as higher doses, was found to have less influence on prolactin concentrations and allows higher HDL-C concentrations to be maintained. While GnRH agonists are preferred over CPA due to the fewer associated long-term side effects, this study shows that CPA at a low dose is a viable option when GnRH agonists are contra-indicated, not available, or not reimbursed. Future research should focus on assessing the effectiveness of an even lower dose of CPA (e.g., 5 mg) and the potential long-term side effects.
Around the same that this study was published, Guy T’Sjoen (one of the authors of the study) and other colleagues in a review of optimal hormone therapy for transfeminine people recommended a dosage of no more than 10 or 12.5 mg/day CPA for no longer than 2 years (Glintborg et al., 2021). T’Sjoen is notable in being regarded as one of the foremost experts in transgender medicine and is a coauthor of the Endocrine Society transgender care guidelines (Hembree et al., 2017).
Shortly after the study of Kuijpers and colleagues and also in June 2021, Even Zohar and colleagues in Israel published the following study on low doses of CPA in transfeminine people:
Even Zohar, N., Sofer, Y., Yaish, I., Serebro, M., Tordjman, K., & Greenman, Y. (2021). Low-Dose Cyproterone Acetate Treatment for Transgender Women. The Journal of Sexual Medicine, 18(7), 1292–1298. [10.1016/j.jsxm.2021.04.008]
This study was initially reported as a conference abstract in May 2020 (Even-Zohar et al., 2020).
In the introduction section of the paper, the authors stated the following:
Treatment guidelines published by several organizations are available and assist clinicians in treating transgender women.4,7−9 A wide range of regimens for CPA administration have been proposed. By and large, the recommended doses have decreased over the years: doses of 50–100 mg/day were suggested in the 2009 Endocrine Society Guidelines,10 and amended to 25–50 mg/day in 2017.7 The proposed CPA doses were 12.5–25 mg/day in the 2019 guidelines of the Australian Professional Association for Transgender Health,4 and they were amended to 10–50 mg/day in the 2020 guidelines of the European Society for Sexual Medicine.8 There are no publications on data that compare different doses of CPA for efficacy or safety.
The researchers found that estradiol plus low-dose CPA (10–20 mg/day) suppressed testosterone levels to an equivalent extent as estradiol plus high-dose CPA (50–100 mg/day). Testosterone levels were suppressed into the female/castrate range or near so in both groups (generally ≤2 nmol/L or ≤58 pg/mL). Of the 38 transfeminine people on low-dose CPA, 32 (84%) were on 10 mg/day CPA and 6 (16%) were on 20 mg/day CPA (mean dose 11.6 ± 3.7 mg/day). Estradiol was given as transdermal estradiol patch (mean dose 83.7 ± 36.5 μg/day), transdermal estradiol gel (mean dose 3.8 ± 1.2 g/day), or oral estradiol (mean dose 4.1 ± 1.7 mg/day). Mean estradiol levels ranged from ~110 to 350 pmol/L (~30–95 pg/mL) in the low- and high-dose CPA groups over the follow-up period. Besides showing equivalent testosterone suppression, prolactin levels were significantly lower with low-dose CPA than with high-dose CPA (398 ± 69 mIU/mL vs. 804 ± 121 mIU/mL at 12 months of hormone therapy, respectively).
Based on their findings, the authors stated the following:
We suggest an adjustment of current clinical practice guidelines to recommend lower doses of CPA for the treatment of transgender women.
Both Kuijpers et al. (2021) and Even Zohar et al. (2021) claimed to be the first to demonstrate the efficacy of low-dose CPA in transfeminine people. However, that achievement actually appears to belong to Meyer et al. (2020), who in February 2020 found that estradiol plus 10, 25, or 50 mg/day CPA gave equivalent testosterone suppression across CPA doses in transfeminine people.
Although their study was not about CPA and testosterone suppression, Lim et al. (2020) reported in May/July 2020 that testosterone levels in transfeminine people were median (IQR) 0.6 (0.4–1.0) nmol/L for oral estradiol and 0.9 (0.7–1.6) nmol/L for transdermal estradiol in a mixed group of transfeminine people (n=26 total) on estradiol plus low-dose CPA (12.5 (12.5–18.8) mg/day) (n=14), estradiol alone post-gonadectomy (n=9), and estradiol plus spironolactone (n=3).
In December 2021, the following case report of fatal liver failure with low-dose CPA was published:
Kumar, P., Reddy, S., Kulkarni, A., Sharma, M., & Rao, P. N. (2021). Cyproterone acetate induced Acute liver failure: Case report and review of the literature. Journal of Clinical and Experimental Hepatology, 11(6), 739–741. [DOI:10.1016/j.jceh.2021.01.003]
The case report describes a 30-year-old cisgender woman who was on 25 mg/day CPA for treatment of hirsutism (excessive facial/body hair growth) for 6 months and developed acute liver failure. Four days following hospitalization, she died. This is the second published case report of liver toxicity with CPA at a dosage below 100 mg/day (the first and only other case was at 50 mg/day) (Wiki; Table). It is also the first report of liver failure in a cisgender woman taking CPA. The case indicates that CPA even at a relatively low dose of 25 mg/day is not fully safe in terms of liver toxicity. It further emphasizes the importance of using the lowest effective doses of CPA in transfeminine people (no more than 10–12.5 mg/day).
Update 4: Coleman et al. (2022) [WPATH SOC8 Guidelines]
In September 2022, the World Professional Association for Transgender Health (WPATH) Standards of Care for the Health of Transgender and Gender Diverse People Version 8 (SOC8) were published and made recommendations for transgender hormone therapy for the first time (Coleman et al., 2022). These guidelines recommended a dose of CPA of 10 mg/day in transfeminine people (Coleman et al., 2022). This dose is substantially lower than previous doses recommended by transgender care guidelines and is the first time that major guidelines have recommended a CPA dosage this low. The WPATH SOC8 cited Kuijpers et al. (2021) in support of this recommendation (though notably not Even Zohar et al. (2021) or Meyer et al. (2020)) and also discussed the dose-dependent risks of CPA such as meningiomas and high prolactin levels (Coleman et al., 2022). Considering the key position and importance of the WPATH SOC in transgender health, it is likely that lower CPA doses in transfeminine hormone therapy will now be widely adopted throughout the world. Continued use of higher CPA doses should be considered out of step with current accepted evidence-based practice.
Update 5: Collet et al. (2023)
In October 2022, a study more carefully assessing androgen suppression with estradiol plus CPA in transfeminine people was published:
Collet, S., Gieles, N., Wiepjes, C. M., Heijboer, A. C., Reyns, T., Fiers, T., Lapauw, B., den Heijer, M., & T’Sjoen, G. (2023). Changes in serum testosterone and adrenal androgen levels in transgender women with and without gonadectomy. The Journal of Clinical Endocrinology & Metabolism, 108(2), 331–338. [DOI:10.1210/clinem/dgac576]
In the study, 275 transfeminine people were treated with estradiol plus CPA, and levels of total testosterone, free testosterone, and the adrenal androgensdehydroepiandrosterone (DHEA), dehydroepiandrosterone sulfate (DHEA-S), and androstenedione (A4) were measured using liquid chromatography–mass spectrometry (LC–MS) at baseline and during follow-ups at 3 months, 12 months, 2 to 4 years, and after surgical gonadal removal (at which time CPA was discontinued). Estradiol was measured both with LC–MS (Amsterdam clinic) and with immunoassays (Ghent clinic). The forms and doses of estradiol used were most commonly oral estradiol valerate 4 mg/day or a transdermal estradiol patch 100 μg/day, while the dosage of CPA was usually 25 or 50 mg/day. About half of the transfeminine people eventually underwent surgical gonadal removal, usually after 2 years of hormone therapy.
Median estradiol levels ranged from 49 to 75 pg/mL (180–275 pmol/L) with LC–MS and from 63 to 69 pg/mL (232–255 pmol/L) with immunoassays at different follow-ups. After 3 months of hormone therapy, total testosterone decreased by 97.1%, from 536 ng/dL (18.6 nmol/L) to 12 ng/dL (0.40 nmol/L), and free testosterone decreased by 98.3%, from 109 pg/mL (378 pmol/L) to 2.0 pg/mL (7.1 pmol/L). Thereafter, total and free testosterone levels remained stable. Levels of DHEA, DHEA-S, and A4 decreased by 24.9 to 28.0%, 20.1 to 23.5%, and 36.5%, respectively, and likewise did not further change after the first 3 to 12 months of hormone therapy. No changes in androgen levels occurred upon surgical gonadal removal with discontinuation of CPA. The authors noted that testosterone levels in the transfeminine people on hormone therapy in the study were similar to or lower than those in cisgender women.
Update 6: Warzywoda et al. (2024) [GoLoCypro Study]
The GoLoCypro study, by Judith Dean and colleagues, was published online in February 2024:
Warzywoda, S., Fowler, J. A., Wood, P., Bisshop, F., Russell, D., Luu, H., Kelly, M., Featherstone, V., & Dean, J. A. (2024). How low can you go? Titrating the lowest effective dose of cyproterone acetate for transgender and gender diverse people who request feminizing hormones. International Journal of Transgender Health, advance online publication. [DOI:10.1080/26895269.2024.2317395]
The following are some noteworthy excerpts from the paper:
Of participants who completed the protocol, 74.0% (34/46) were able to achieve the target T-range (0.5–1.5 nmol/L) and 41.3% (19/46) were titrated to the lowest CPA level (12.5 mg cyproterone twice weekly).
Almost all participants who completed the protocol (91.3.0%, 42/46) recorded their CPA levels as level 3 (12.5 mg daily/25 [mg] alternate days) or lower, with 69.0% (29/42) of these being able to achieve the target T-range. Of those that completed, 41.3% (19/46) were able to achieve the lowest CPA level (12.5 mg cyproterone twice week) with 57.9% (11/19) being able to achieve the target T-range.
The study findings showed that for some patients, CPA doses as low as 12.5 mg on alternate days or less can successfully reduce testosterone to pre-menopausal ranges whilst ensuring testosterone was not over-suppressed.
Our study found that doses of CPA lower than the standard dose (12.5 mg CPA daily and/or 25 mg alternate days) were achievable for suppression of testosterone. Several studies have supported this finding that a lower dosage (10 mg CPA daily) is effective in testosterone reduction in individuals undergoing hormone feminization (Even Zohar et al., 2021; Kuijpers et al., 2021). While not all individuals within our study were able to titrate down CPA dosages, almost a quarter of participants who completed the protocol were achieving target T-ranges on 12.5 mg CPA twice weekly (equivalent to 3.5 mg/daily). To our knowledge ours is the first study to demonstrate that doses lower than 10 mg/daily as well as alternate days or twice weekly CPA are clinically effective in maintaining testosterone reduction within target ranges.
Update 7: More New Low-Dose CPA Studies (2023–2024)
Other new studies of low-dose CPA in transfeminine people have also been published in 2023 and 2024:
Angus, L. M., Leemaqz, S., Zajac, J. D., & Cheung, A. S. (November 2023). A randomised controlled trial of spironolactone versus cyproterone in trans people commencing estradiol. AusPATH 2023 Symposium. [URL] [PDF] [Trans Health Research Blog Post]
Angus, L. M., Leemaqz, S. Y., Zajac, J. D., & Cheung, A. S. (November 2023). The effect of cyproterone and spironolactone on breast development in transgender women: a randomised controlled trial. ESA/SRB/ENSA 2023 ASM 26-29 November, Brisbane, 54–55 (abstract no. 132). [URL] [PDF] [Full Abstract Book] [Trans Health Research Blog Post]
Flamant, T., Vervalcke, J., & T’Sjoen, G. (November 2023). Dose Reduction of Cyproterone Acetate in Trans Women and the Effect on Patient-reported Outcomes: Results from the ENIGI Study. Endocrine Abstracts, 97 [Belgian Endocrine Society 2023], 5–5 (abstract no. 007). [URL] [PDF]
Korpaisarn, S., Arunakul, J., Chaisuksombat, K., & Rattananukrom, T. (2023). A Low Dose Cyproterone Acetate In Feminizing Hormone Treatment. Journal of the Endocrine Society, 7(Suppl 1), A1098–A1099 (abstract no. SAT397/bvad114.2068). [DOI:10.1210/jendso/bvad114.2068]
Yang, W., Hong, T., Chang, X., Han, M., Gao, H., Pan, B., Zhao, Z., & Liu, Y. (2024). The efficacy of and user satisfaction with different antiandrogens in Chinese transgender women. International Journal of Transgender Health, advance online publication. [DOI:10.1080/26895269.2024.2323514]
References
Angus, L., Leemaqz, S., Ooi, O., Cundill, P., Silberstein, N., Locke, P., Zajac, J. D., & Cheung, A. S. (2019). Cyproterone acetate or spironolactone in lowering testosterone concentrations for transgender individuals receiving oestradiol therapy. Endocrine Connections, 8(7), 935–940. [DOI:10.1530/ec-19-0272]
Angus, L. M., Leemaqz, S., Zajac, J. D., & Cheung, A. S. (2023). A randomised controlled trial of spironolactone versus cyproterone in trans people commencing estradiol. AusPATH 2023 Symposium. [URL] [PDF] [Trans Health Research Blog Post]
Angus, L. M., Leemaqz, S. Y., Zajac, J. D., & Cheung, A. S. (2023). The effect of cyproterone and spironolactone on breast development in transgender women: a randomised controlled trial. ESA/SRB/ENSA 2023 ASM 26-29 November, Brisbane, 54–55 (abstract no. 132). [URL] [PDF] [Full Abstract Book] [Trans Health Research Blog Post]
Asscheman, H., & Gooren, L. J. (1992). Hormone Treatment in Transsexuals. In Bocking, W. O., Coleman, E. (Eds). Gender Dysphoria: Interdisciplinary Approaches in Clinical Management (pp. 39–54). Binghamton: Haworth Press. / Journal of Psychology & Human Sexuality, 5(4), 39–54. [Google Scholar] [Google Books] [DOI:10.1300/J056v05n04_03]
Athanasoulia-Kaspar, A. P., & Stalla, G. K. (2019). Endokrinologische Betreuung von Patienten mit Transsexualität. Geburtshilfe und Frauenheilkunde, 79(7), 672–675. [DOI:10.1055/a-0801-3319]
Bastianelli, C., Farris, M., Rosato, E., Brosens, I., & Benagiano, G. (2018). Pharmacodynamics of combined estrogen-progestin oral contraceptives 3. Inhibition of ovulation. Expert Review of Clinical Pharmacology, 11(11), 1085–1098. [DOI:10.1080/17512433.2018.1536544]
Bourns, A. (2019). Guidelines for Gender-Affirming Primary Care with Trans and Non-Binary Patients, 4th Edition. Toronto: Rainbow Health Ontario/Sherbourne Health. [URL] [PDF]
Bruchovsky, N., Larry Goldenberg, S., Akakura, K., & Rennie, P. S. (1993). Luteinizing hormone-releasing hormone agonists in prostate cancer. Elimination of flare reaction by pretreatment with cyproterone acetate and low-dose diethylstilbestrol. Cancer, 72(5), 1685–1691. [DOI:10.1002/1097-0142(19930901)72:5<1685::aid-cncr2820720532>3.0.co;2-3]
Bultynck, C., Pas, C., Defreyne, J., Cosyns, M., den Heijer, M., & T’Sjoen, G. (2017). Self-perception of voice in transgender persons during cross-sex hormone therapy. The Laryngoscope, 127(12), 2796–2804. [DOI:10.1002/lary.26716]
Chen, H., Wiepjes, C. M., van Schoor, N. M., Heijboer, A. C., de Jongh, R. T., den Heijer, M., & Lips, P. (2019). Changes of Vitamin D-Binding Protein, and Total, Bioavailable, and Free 25-Hydroxyvitamin D in Transgender People. The Journal of Clinical Endocrinology & Metabolism, 104(7), 2728–2734. [DOI:10.1210/jc.2018-02602]
Coleman, E., Radix, A. E., Bouman, W. P., Brown, G. R., de Vries, A. L., Deutsch, M. B., Ettner, R., Fraser, L., Goodman, M., Green, J., Hancock, A. B., Johnson, T. W., Karasic, D. H., Knudson, G. A., Leibowitz, S. F., Meyer-Bahlburg, H. F., Monstrey, S. J., Motmans, J., Nahata, L., … & Arcelus, J. (2022). [World Professional Association for Transgender Health (WPATH)] Standards of Care for the Health of Transgender and Gender Diverse People, Version 8. International Journal of Transgender Health, 23(Suppl 1), S1–S259. [DOI:10.1080/26895269.2022.2100644] [URL] [PDF]
Collet, S., Gieles, N., Wiepjes, C. M., Heijboer, A. C., Reyns, T., Fiers, T., Lapauw, B., den Heijer, M., & T’Sjoen, G. (2023). Changes in serum testosterone and adrenal androgen levels in transgender women with and without gonadectomy. The Journal of Clinical Endocrinology & Metabolism, 108(2), 331–338. [DOI:10.1210/clinem/dgac576]
Damgaard-Pedersen, F., & Føgh, M. (1980). The effect of cyproterone acetate on serum lipids in normal men. Acta Endocrinologica, 94(2), 280–283. [DOI:10.1530/acta.0.0940280]
de Blok, C. J., Klaver, M., Wiepjes, C. M., Nota, N. M., Heijboer, A. C., Fisher, A. D., Schreiner, T., T’Sjoen, G., & den Heijer, M. (2017). Breast Development in Transwomen After 1 Year of Cross-Sex Hormone Therapy: Results of a Prospective Multicenter Study. The Journal of Clinical Endocrinology & Metabolism, 103(2), 532–538. [DOI:10.1210/jc.2017-01927]
Defreyne, J., Vantomme, B., Van Caenegem, E., Wierckx, K., De Blok, C., Klaver, M., Nota, N. M., Van Dijk, D., Wiepjes, C. M., Den Heijer, M., & T’Sjoen, G. (2018). Prospective evaluation of hematocrit in gender-affirming hormone treatment: results from European Network for the Investigation of Gender Incongruence. Andrology, 6(3), 446–454. [DOI:10.1111/andr.12485]
Endrikat, J., Gerlinger, C., Richard, S., Rosenbaum, P., & Düsterberg, B. (2011). Ovulation inhibition doses of progestins: a systematic review of the available literature and of marketed preparations worldwide. Contraception, 84(6), 549–557. [DOI:10.1016/j.contraception.2011.04.009]
Even-Zohar, N., Sofer, Y., Yaish, I., Serebro, M., Tordjman, K., & Greenman, Y. (2020). SUN-042 Low Dose Cyproterone Acetate for the Treatment of Transgender Women - a Retrospective Study. Journal of the Endocrine Society, 4(Suppl 1), A715–A715. [DOI:10.1210/jendso/bvaa046.1412]
Even Zohar, N., Sofer, Y., Yaish, I., Serebro, M., Tordjman, K., & Greenman, Y. (2021). Low-Dose Cyproterone Acetate Treatment for Transgender Women. The Journal of Sexual Medicine, 18(7), 1292–1298. [DOI:10.1016/j.jsxm.2021.04.008]
Fink, G. (1979). Feedback Actions of Target Hormones on Hypothalamus and Pituitary With Special Reference to Gonadal Steroids. Annual Review of Physiology, 41(1), 571–585. [DOI:10.1146/annurev.ph.41.030179.003035]
Flamant, T., Vervalcke, J., & T’Sjoen, G. (2023). Dose Reduction of Cyproterone Acetate in Trans Women and the Effect on Patient-reported Outcomes: Results from the ENIGI Study. Endocrine Abstracts, 97 [Belgian Endocrine Society 2023], 5–5 (abstract no. 007). [URL] [PDF]
Føgh, M., Corker, C. S., Hunter, W. M., McLean, H., Philip, J., Schou, G., & Shakkebæk, N. E. (1979). The effects of low doses of cyproterone acetate on some functions of the reproductive system in normal men. Acta Endocrinologica, 91(3), 545–552. [DOI:10.1530/acta.0.0910545]
Føgh, M., Knudsen, J. B., & Gormsen, J. (1980). Effect of cyproterone acetate on platelet aggregability, fibrinolytic activity and fibrinolytic capacity in normal men. Acta Endocrinologica, 94(3), 430–432. [DOI:10.1530/acta.0.0940430]
Foegh, M. (1983). Evaluation of Steroids as COntraceptives in Men. Acta Endocrinologica, 104(3 Suppl b), S9–S48. [DOI:10.1530/acta.0.104s009]
Fredricsson, B., & Carlström, K. (2009). Effects of Low Doses of Cyproterone Acetate on Sperm Morphology and some other Parameters of Reproduction in Normal Men. Andrologia, 13(4), 369–375. [DOI:10.1111/j.1439-0272.1981.tb00067.x]
Fung, R., Hellstern-Layefsky, M., & Lega, I. (2017). Is a lower dose of cyproterone acetate as effective at testosterone suppression in transgender women as higher doses? International Journal of Transgenderism, 18(2), 123–128. [DOI:10.1080/15532739.2017.1290566]
Fuss, J., Hellweg, R., Van Caenegem, E., Briken, P., Stalla, G. K., T’Sjoen, G., & Auer, M. K. (2015). Cross-sex hormone treatment in male-to-female transsexual persons reduces serum brain-derived neurotrophic factor (BDNF). European Neuropsychopharmacology, 25(1), 95–99. [DOI:10.1016/j.euroneuro.2014.11.019]
Fuss, J., Claro, L., Ising, M., Biedermann, S. V., Wiedemann, K., Stalla, G. K., Briken, P., & Auer, M. K. (2019). Does sex hormone treatment reverse the sex-dependent stress regulation? A longitudinal study on hypothalamus-pituitary-adrenal (HPA) axis activity in transgender individuals. Psychoneuroendocrinology, 104, 228–237. [DOI:10.1016/j.psyneuen.2019.02.023]
Gava, G., Cerpolini, S., Martelli, V., Battista, G., Seracchioli, R., & Meriggiola, M. C. (2016). Cyproterone acetatevsleuprolide acetate in combination with transdermal oestradiol in transwomen: a comparison of safety and effectiveness. Clinical Endocrinology, 85(2), 239–246. [DOI:10.1111/cen.13050]
Gava, G., Mancini, I., Alvisi, S., Seracchioli, R., & Meriggiola, M. C. (2020). A comparison of 5-year administration of cyproterone acetate or leuprolide acetate in combination with estradiol in transwomen. European Journal of Endocrinology, 183(6), 561–569. [DOI:10.1530/eje-20-0370]
Geller, J., Albert, J., Yen, S. S., Geller, S., & Loza, D. (1981). Medical Castration of Males with Megestrol Acetate and Small Doses of Diethylstilbestrol*. The Journal of Clinical Endocrinology & Metabolism, 52(3), 576–580. [DOI:10.1210/jcem-52-3-576]
Geller, J., Albert, J., Yen, S. S., Geller, S., & Loza, D. (1981). Medical castration with megestrol acetate and minidose of diethylstilbestrol. Urology, 17(4 Suppl), 27–33. [Google Scholar] [PubMed]
Geller, J., & Albert, J. D. (1983). Comparison of various hormonal therapies for prostatic carcinoma. Seminars in Oncology, 10(4 Suppl 4), 34–41. [Google Scholar] [PubMed] [PDF]
Geller, J. (1988). Megestrol acetate and minidose estrogen in prostatic carcinoma. Urology, 32(3), 281–282. [DOI:10.1016/0090-4295(88)90402-5]
Geller J. (1991). Megestrol Acetate Plus Low-Dose Estrogen in the Management of Advanced Prostatic Carcinoma. The Urologic Clinics of North America, 18(1), 83–91. [DOI:10.1016/S0094-0143(21)01395-1] [Archive.org] [PDF]
Giltay, E. J., & Gooren, L. J. (2000). Effects of Sex Steroid Deprivation/Administration on Hair Growth and Skin Sebum Production in Transsexual Males and Females. The Journal of Clinical Endocrinology & Metabolism, 85(8), 2913–2921. [DOI:10.1210/jcem.85.8.6710]
Giltay, E. J., Gooren, L. J., Emeis, J. J., Kooistra, T., & Stehouwer, C. D. (2000). Oral, but Not Transdermal, Administration of Estrogens Lowers Tissue-Type Plasminogen Activator Levels in Humans Without Affecting Endothelial Synthesis. Arteriosclerosis, Thrombosis, and Vascular Biology, 20(5), 1396–1403. [DOI:10.1161/01.atv.20.5.1396]
Giltay, E. J., Verhoef, P., Gooren, L. J., Geleijnse, J. M., Schouten, E. G., & Stehouwer, C. D. (2003). Oral and transdermal estrogens both lower plasma total homocysteine in male-to-female transsexuals. Atherosclerosis, 168(1), 139–146. [DOI:10.1016/s0021-9150(03)00090-x]
Giltay, E. J., Gooren, L. J., Toorians, A. W., Katan, M. B., & Zock, P. L. (2004). Docosahexaenoic acid concentrations are higher in women than in men because of estrogenic effects. The American Journal of Clinical Nutrition, 80(5), 1167–1174. [DOI:10.1093/ajcn/80.5.1167]
Glintborg, D., T’Sjoen, G., Ravn, P., & Andersen, M. S. (2021). MANAGEMENT OF ENDOCRINE DISEASE: Optimal feminizing hormone treatment in transgender people. European Journal of Endocrinology, 185(2), R49–R63. [DOI:10.1530/eje-21-0059]
Goldenberg, S. L., Bruchovsky, N., Rennie, P. S., & Coppin, C. M. (1988). The Combination of Cyproterone Acetate and Low Dose Diethylstilbestrol in the Treatment of Advanced Prostatic Carcinoma. Journal of Urology, 140(6), 1460–1465. [DOI:10.1016/s0022-5347(17)42073-8]
Goldenberg, S. L., & Bruchovsky, N. (1991). Use of Cyproterone Acetate in Prostate Cancer. The Urologic Clinics of North America, 18(1), 111–122. [DOI:10.1016/S0094-0143(21)01398-7] [Archive.org] [PDF]
Goldenberg, S., Bruchovsky, N., Gleave, M., & Sullivan, L. (1996). Low-dose cyproterone acetate plus mini-dose diethylstilbestrol—A protocol for reversible medical castration. Urology, 47(6), 882–884. [DOI:10.1016/s0090-4295(96)00048-9]
Gooren, L. J., Giltay, E. J., & Bunck, M. C. (2008). Long-Term Treatment of Transsexuals with Cross-Sex Hormones: Extensive Personal Experience. The Journal of Clinical Endocrinology & Metabolism, 93(1), 19–25. [DOI:10.1210/jc.2007-1809]
Gräf, K., Brotherton, J., & Neumann, F. (1974). Clinical Uses of Antiandrogens. In Hughes, A., Hasan, S. H., Oertel, G. W., Voss, H. E., Bahner, F., Neumann, F., Steinbeck, H., Gräf, K.-J., Brotherton, J., Horn, H. J., & Wagner, R. K. (Eds.). Androgens II and Antiandrogens / Androgene II und Antiandrogene (Handbuch der experimentellen Pharmakologie/Handbook of Experimental Pharmacology, Volume 35, Part 2) (pp. 485–542). Berlin/Heidelberg: Springer. [DOI:10.1007/978-3-642-80859-3_7]
Hammerstein, J., Meckies, J., Leo-Rossberg, I., Moltz, L., & Zielske, F. (1975). Use of cyproterone acetate (CPA) in the treatment of acne, hirsutism and virilism. Journal of Steroid Biochemistry, 6(6), 827–836. [DOI:10.1016/0022-4731(75)90311-8]
Hammerstein, J. (1979). Cyproterone Acetate. In Jacobs, H. S. (Ed.). Advances in Gynaecological Endocrinology: Proceedings of the Sixth Study Group of the Royal College of Obstetricians and Gynaecologists, 18th and 19th October, 1978 (pp. 367–382). London: The College. [Google Scholar] [Google Books] [PDF]
Hammerstein, J. (1990). Antiandrogens: Clinical Aspects. In Orfanos, C. E., & Happle, R. (Eds.). Hair and Hair Diseases (pp. 827–886). Berlin/Heidelberg: Springer. [DOI:10.1007/978-3-642-74612-3_35]
Heath, R. A., & Wynne, K. (2019). A Guide to Transgender Health: State-of-the-art Information for Gender-Affirming People and Their Supporters (p. 122). Santa Barbara: Praeger/ABC-CLIO. [Google Books]
Hembree, W. C., Cohen-Kettenis, P., Delemarre-Van De Waal, H. A., Gooren, L. J., Meyer III, W. J., Spack, N. P., Tangpricha, V., & Montori, V. M. (2009). Endocrine treatment of transsexual persons: an Endocrine Society clinical practice guideline. The Journal of Clinical Endocrinology & Metabolism, 94(9), 3132–3154. [DOI:10.1210/jc.2009-0345]
Hembree, W. C., Cohen-Kettenis, P. T., Gooren, L., Hannema, S. E., Meyer, W. J., Murad, M. H., Rosenthal, S. M., Safer, J. D., Tangpricha, V., & T’Sjoen, G. G. (2017). Endocrine Treatment of Gender-Dysphoric/Gender-Incongruent Persons: An Endocrine Society* Clinical Practice Guideline [2nd Version]. The Journal of Clinical Endocrinology & Metabolism, 102(11), 3869–3903. [DOI:10.1210/jc.2017-01658] [PDF]
Jacobeit, J. W. (2019). Die hormonelle Behandlung von adulten Trans*Personen (in Deutschland). [Hormonal treatment of adult trans* persons (in Germany).] Journal für Klinische Endokrinologie und Stoffwechsel, 12(3), 102–110. [DOI:10.1007/s41969-019-00080-x]
Jacobi, G. H., Altwein, J. E., Kurth, K. H., Basting, R., & Hohenfellner, R. (1980). Treatment of Advanced Prostatic Cancer with Parenteral Cyproterone Acetate: A Phase III Randomised Trial*. British Journal of Urology, 52(3), 208–215. [DOI:10.1111/j.1464-410x.1980.tb02961.x]
Jacobi, G. H., Tunn, U., & Senge, T. (1982). Clinical experience with cyproterone acetate for palliation of inoperable prostate cancer. In Jacobi, G. H., & Hohenfellner, R. (Eds.). Prostate Cancer (International Perspectives in Urology, Volume 3) (pp. 305–319). Baltimore: Williams & Wilkins. [Google Scholar] [Google Books] [OpenLibrary] [WorldCat] [Archive.org] [PDF]
Jain, J., Kwan, D., & Forcier, M. (2019). Medroxyprogesterone Acetate in Gender-Affirming Therapy for Transwomen: Results From a Retrospective Study. The Journal of Clinical Endocrinology & Metabolism, 104(11), 5148–5156. [DOI:10.1210/jc.2018-02253]
Jequier, A. M., Bullimore, N. J., & Bishop, M. J. (2009). Cyproterone Acetate and a Small Dose of Oestrogen in the Pre-operative Management of Male Transsexuals. A Report of Three Cases. [Cyproteronacetat und kleine Östrogendosis in dem präoperativen Management männlicher Transsexueller. Bericht über drei Fälle.] Andrologia, 21(5), 456–461. [DOI:10.1111/j.1439-0272.1989.tb02447.x]
Johnson, D. E., Babaian, R. J., Swanson, D. A., Von Eschenbach, A. C., Wishnow, K. I., & Tenney, D. (1988). Medical castration using megestrol acetate and minidose estrogen. Urology, 31(5), 371–374. [DOI:10.1016/0090-4295(88)90726-1]
Knuth, U. A., Hano, R., & Nieschlag, E. (1984). Effect of Flutamide or Cyproterone Acetate on Pituitary and Testicular Hormones in Normal Men. The Journal of Clinical Endocrinology & Metabolism, 59(5), 963–969. [DOI:10.1210/jcem-59-5-963]
Koch, U. J., Lorenz, F., Danehl, K., & Hammerstein, J. (1975). Über die Verwendbarkeit von Cyproteronacetat zur Fertilitätshemmung beim Mann. Morphologische Veränderungen und Einflüsse auf die Spermienmotilität. Archiv für Gynäkologie, 219(1–4), 581–582. [DOI:10.1007/bf00669258]
Koch, U., Lorenz, F., Danehl, K., Ericsson, R., Hasan, S., Keyserlingk, D., Lübke, K., Mehring, M., Römmler, A., Schwartz, U., & Hammerstein, J. (1976). Continuous oral low-dosage cyproterone acetate for fertility regulation in the male? A trend analysis in 15 volunteers. Contraception, 14(2), 117–135. [DOI:10.1016/0010-7824(76)90081-0]
Korpaisarn, S., Arunakul, J., Chaisuksombat, K., & Rattananukrom, T. (2023). A Low Dose Cyproterone Acetate In Feminizing Hormone Treatment. Journal of the Endocrine Society, 7(Suppl 1), A1098–A1099 (abstract no. SAT397/bvad114.2068). [DOI:10.1210/jendso/bvad114.2068]
Kranz, G. S., Seiger, R., Kaufmann, U., Hummer, A., Hahn, A., Ganger, S., Tik, M., Windischberger, C., Kasper, S., & Lanzenberger, R. (2017). Effects of sex hormone treatment on white matter microstructure in individuals with gender dysphoria. NeuroImage, 150, 60–67. [DOI:10.1016/j.neuroimage.2017.02.027]
Kranz, G. S., Kaufmann, U., & Lanzenberger, R. (2019). Probing the Impact of Gender-Affirming Hormone Treatment on Odor Perception. Chemical Senses, 45(1), 37–44. [DOI:10.1093/chemse/bjz069]
Kuijpers, S. M., Wiepjes, C. M., Conemans, E. B., Fisher, A. D., T’Sjoen, G., & den Heijer, M. (2021). Toward a Lowest Effective Dose of Cyproterone Acetate in Trans Women: Results From the ENIGI Study. The Journal of Clinical Endocrinology & Metabolism, 106(10), e3936–e3945. [DOI:10.1210/clinem/dgab427]
Kumar, P., Reddy, S., Kulkarni, A., Sharma, M., & Rao, P. N. (2021). Cyproterone acetate induced acute liver failure: case report and review of the literature. Journal of Clinical and Experimental Hepatology, 11(6), 739–741. [DOI:10.1016/j.jceh.2021.01.003]
Lederbogen, S. (2009). Hormonbehandlung. PiD - Psychotherapie im Dialog, 10(1), 41–43. [DOI:10.1055/s-0028-1090190]
Lim, H. Y., Leemaqz, S. Y., Torkamani, N., Grossmann, M., Zajac, J. D., Nandurkar, H., Ho, P., & Cheung, A. S. (2020). Global Coagulation Assays in Transgender Women on Oral and Transdermal Estradiol Therapy. The Journal of Clinical Endocrinology & Metabolism, 105(7), e2369–e2377. [DOI:10.1210/clinem/dgaa262]
Liu, P. Y., Takahashi, P., & Veldhuis, J. D. (2017). An Ensemble Perspective of Aging-Related Hypoandrogenemia in Men. In Winters, S. J., & Huhtaniemi, I. T. (Eds.). Male Hypogonadism: Basic, Clinical and Therapeutic Principles, 2nd Edition (pp. 325–347). Cham: Springer. [DOI:10.1007/978-3-319-53298-1_16]
Mahfouda, S., Moore, J. K., Siafarikas, A., Hewitt, T., Ganti, U., Lin, A., & Zepf, F. D. (2019). Gender-affirming hormones and surgery in transgender children and adolescents. The Lancet Diabetes & Endocrinology, 7(6), 484–498. [DOI:10.1016/s2213-8587(18)30305-x]
Meriggiola, M. C., Bremner, W. J., Costantino, A., Di Cintio, G., & Flamigni, C. (1998). Low dose of cyproterone acetate and testosterone enanthate for contraception in men. Human Reproduction, 13(5), 1225–1229. [DOI:10.1093/humrep/13.5.1225]
Meriggiola, M. C., Bremner, W. J., Costantino, A., Bertaccini, A., Morselli-Labate, A. M., Huebler, D., Kaufmann, G., Oettel, M., & Flamigni, C. (2002). Twenty-One Day Administration of Dienogest Reversibly Suppresses Gonadotropins and Testosterone in Normal Men. The Journal of Clinical Endocrinology & Metabolism, 87(5), 2107–2113. [DOI:10.1210/jcem.87.5.8514]
Meriggiola, M. C., Costantino, A., Bremner, W. J., & Morselli-Labate, A. M. (2002). Higher Testosterone Dose Impairs Sperm Suppression Induced by a Combined Androgen‐Progestin Regimen. Journal of Andrology, 23(5), 684–690. [DOI:10.1002/j.1939-4640.2002.tb02311.x]
Meyer, G., Mayer, M., Mondorf, A., Flügel, A. K., Herrmann, E., & Bojunga, J. (2020). Safety and rapid efficacy of guideline-based gender-affirming hormone therapy: an analysis of 388 individuals diagnosed with gender dysphoria. European Journal of Endocrinology, 182(2), 149–156. [DOI:10.1530/eje-19-0463] [PDF]
Moltz, L., Römmler, A., Schwartz, U., & Hammerstein, J. (1978). Effects of Cyproterone Acetate (CPA) on Pituitary Gonadotrophin Release and on Androgen Secretion Before and After LH-RH Double Stimulation Tests in Men. International Journal of Andrology, 1(Suppl 2b) [5th Annual Workshop on the Testis, Geilo, Norway, April 1978, Endocrine Approach to Male Contraception], 713–719. [DOI:10.1111/j.1365-2605.1978.tb00518.x]
Moltz, L., Römmler, A., Schwartz, U., Post, K., & Hammerstein, J. (1978). Cyproterone acetate (CPA)—a potential male contraceptive: further studies on the interactions with endocrine parameters. Journal of Steroid Biochemistry, 9(9), 865–865 (abstract no. 252). [DOI:10.1016/0022-4731(78)90952-4]
Moltz, L., Römmler, A., Post, K., Schwartz, U., & Hammerstein, J. (1980). Medium dose cyproterone acetate (CPA): Effects on hormone secretion and on spermatogenesis in men. Contraception, 21(4), 393–413. [DOI:10.1016/s0010-7824(80)80017-5]
Moltz, L., Koch, U., Schwartz, U., Rommler, A., & Hammerstein, J. (1982). Male fertility regulation with cyproterone acetate (CPA). Contraceptive Delivery Systems, 3(3/4) [Retroproductive Health Care International Symposium, October 10-15 1982 Maui, Hawaii, USA, Expanded Abstracts], 298–298 (abstract no. 293). [Google Scholar] [PDF]
Moore, E., Wisniewski, A., & Dobs, A. (2003). Endocrine Treatment of Transsexual People: A Review of Treatment Regimens, Outcomes, and Adverse Effects. The Journal of Clinical Endocrinology & Metabolism, 88(8), 3467–3473. [DOI:10.1210/jc.2002-021967]
Nelson, J. B. (2012). Hormone Therapy for Prostate Cancer. In Wein, A. J., Kavoussi, L. R., Novick, A. C., Partin, A. W., & Peters, C. A. (Eds.). Campbell-Walsh Urology, 10th Edition, Volume 2 (pp. 2920–2953). Philadelphia: Elsevier/Saunders. [Google Scholar] [Google Books]
Nota, N. M., den Heijer, M., Gooren, L. J. (2019). Evaluation and Treatment of Gender-Dysphoric/Gender Incongruent Adults. [Updated 2019 Jul 21]. In Feingold, K. R., Anawalt, B., Blackman, M. R., et al. (Eds.). Endotext [Internet]. South Dartmouth, Massachusetts: MDText.com. [PubMed]
Oliphant, J., Veale, J., Macdonald, J., Carroll, R., Johnson, R., Harte, M., Stephenson, C. & Bullock, J. (2018). Guidelines for Gender Affirming Healthcare for Gender Diverse and Transgender Children, Young People and Adults in Aotearoa New Zealand. Waikato: Transgender Health Research Lab/University of Waikato. [URL] [PDF]
Ott, J., Aust, S., Promberger, R., Huber, J. C., & Kaufmann, U. (2011). Cross‐Sex Hormone Therapy Alters the Serum Lipid Profile: A Retrospective Cohort Study in 169 Transsexuals. The Journal of Sexual Medicine, 8(8), 2361–2369. [DOI:10.1111/j.1743-6109.2011.02311.x]
Petry, R., Mauss, J., Senge, T., & Rausch-Stroomann, J. (1970). Über den Einfluß von Cyproteronacetat, Norethisteronönanthat und Gestonoroncapronat auf die Hypophysen-Gonadenachse beim Mann. [Influence of Cyproterone-acetate, Norethisterone-enanthate and Gestonorone-capronate on the Hypophyseal-Gonadal-Axis in the Male.] In Kracht, J. (Ed.). Endokrinologie der Entwicklung und Reifung, 16. Symposion, Ulm, 26.-28. Februar 1970 (Symposion der Deutschen Gesellschaft für Endokrinologie, Volume 16) (pp. 428–430). Berlin: Springer. [Google Books] [DOI:10.1007/978-3-642-80591-2_118] [WorldCat] [PDF]
Petry, R., Rausch-Stroomann, J.-G., Berthold, K. Mauss, J., Ai, M., Senge, Th., & Vermeulen, A. (1970). Untersuchungen zum Wirkungsmechanismus der Antiandrogene Cyproteron und Cyproteronacetat beim Menschen (Gonadotropin-, Plasma-testosteron- und morphologische Keimdrüsenuntersuchungen). [Investigations on the mechanism of action of the antiandrogens cyproterone and cyproterone acetate in humans (gonadotropin, plasma testosterone, and morphological gonad investigations).] In Schlegel, B. (Ed.). Verhandlungen der Deutschen Gesellschaft für Innere Medizin: Sechsundsiebzigster Kongress Gehalten zu Wiesbaden vom 6. April – 9. April 1970 (Verhandlungen der Deutschen Gesellschaft für Innere Medizin, Volume 76) (pp. 873–876). München: Bergmann. [Google Scholar] [Google Books] [DOI:10.1007/978-3-642-85446-0] [WorldCat] [PDF]
Petry, R., Rausch-Stroomann, J. G., Mauss, J., Senge, Th., Ai, M., & Berthold, K. (1970). Investigations on the mode of action of the antiandrogens cyproterone and cyproterone acetate in man. / Investigations on the mechanism of action of anti androgenic cyproterone and cyproterone acetate in humans (gonadotropin, plasma testosterone, and morphological generative gland investigations). Medizinische Welt, 29, 1336–. [EurekaMag] [Cited by Koch et al. (1976)]
Petry, R., Mauss, J., Rausch-Stroomann, J. G., & Vermeulen, A. (1972). Reversible inhibition of spermatogenesis in men. Hormone and Metabolic Research, 4(5), 386–388. [DOI:10.1055/s-0028-1094040]
Roy, S., Chatterjee, S., Prasad, M., Poddar, A., Pandey, D., Pandey, H., & Jadhav, Y. (1976). Effects of cyproterone acetate on reproductive functions in normal human males. Contraception, 14(4), 403–423. [DOI:10.1016/s0010-7824(76)80055-8]
Roy, S., & Chatterjee, S. (1979). Studies with cyproterone acetate for male contraception. In James, V. H. T., & Pasqualini, J. R. (Eds.). Hormonal Steroids: Proceedings of the Fifth International Congress on Hormonal Steroids, New Delhi, India, October/November 1978 (pp. 675–680). Oxford: Pergamon Press. [DOI:10.1016/b978-0-08-023796-1.50099-2]
Roy, S., & Chatterjee, S. (1979). The Role of Antiandrogenic Action in Cyproterone Acetate-Induced Morphologic and Biochemical Changes in Human Semen. Fertility and Sterility, 32(1), 93–95. [DOI:10.1016/s0015-0282(16)44122-1]
Saborowski, K.-J. (1987). Konservative Therapie mit Cyproteronacetat und Estradiolundecylat beim Fortgeschrittenen Prostatacarcinom: Eine 5-Jahres-Studie. [Conservative Therapy with Cyproterone Acetate and Estradiol Undecylate in Advanced Prostate Cancer: A 5-Year Study.] (Doctoral dissertation, Ruhr-University Bochum.) [58 pages] [Google Scholar] [Google Books] [WorldCat] [PDF] [Translation]
Scharff, M., Wiepjes, C. M., Klaver, M., Schreiner, T., T’Sjoen, G., & den Heijer, M. (2019). Change in grip strength in trans people and its association with lean body mass and bone density. Endocrine Connections, 8(7), 1020–1028. [DOI:10.1530/ec-19-0196]
Schröder, F. H., & Radlmaier, A. (2002). Steroidal Antiandrogens. In Jordan, C. V., & Furr, B. J. A. (Eds.). Hormone Therapy in Breast and Prostate Cancer (pp. 325–346). Totowa, New Jersey: Humana Press. [DOI:10.1007/978-1-59259-152-7_15]
Slagter, M. H., Gooren, L. J., de Ronde, W., Soosaipillai, A., Scorilas, A., Giltay, E. J., Paliouras, M., & Diamandis, E. P. (2006). Serum and Urine Tissue Kallikrein Concentrations in Male-to-Female Transsexuals Treated with Antiandrogens and Estrogens. Clinical Chemistry, 52(7), 1356–1365. [DOI:10.1373/clinchem.2006.068932]
Sofer, Y., Yaish, I., Yaron, M., Bach, M. Y., Stern, N., & Greenman, Y. (2020). Differential Endocrine and Metabolic Effects of Testosterone Suppressive Agents in Transgender Women. Endocrine Practice, 26(8), 883–890. [DOI:10.4158/ep-2020-0032] [PDF]
T’Sjoen, G. G., Beguin, Y., Feyen, E., Rubens, R., Kaufman, J., & Gooren, L. (2005). Influence of exogenous oestrogen or (anti-) androgen administration on soluble transferrin receptor in human plasma. Journal of Endocrinology, 186(1), 61–67. [DOI:10.1677/joe.1.06112]
T’Sjoen, G., Weyers, S., Taes, Y., Lapauw, B., Toye, K., Goemaere, S., & Kaufman, J. (2009). Prevalence of Low Bone Mass in Relation to Estrogen Treatment and Body Composition in Male-to-Female Transsexual Persons. Journal of Clinical Densitometry, 12(3), 306–313. [DOI:10.1016/j.jocd.2008.11.002]
T’Sjoen, G., Arcelus, J., De Vries, A. L., Fisher, A. D., Nieder, T. O., Özer, M., & Motmans, J. (2020). European Society for Sexual Medicine Position Statement “Assessment and Hormonal Management in Adolescent and Adult Trans People, with Attention for Sexual Function and Satisfaction”. The Journal of Sexual Medicine, 17(4), 570–584. [DOI:10.1016/j.jsxm.2020.01.012]
Tack, L. J., Heyse, R., Craen, M., Dhondt, K., Bossche, H. V., Laridaen, J., & Cools, M. (2017). Consecutive Cyproterone Acetate and Estradiol Treatment in Late-Pubertal Transgender Female Adolescents. The Journal of Sexual Medicine, 14(5), 747–757. [DOI:10.1016/j.jsxm.2017.03.251]
Toorians, A. W., Thomassen, M. C., Zweegman, S., Magdeleyns, E. J., Tans, G., Gooren, L. J., & Rosing, J. (2003). Venous Thrombosis and Changes of Hemostatic Variables during Cross-Sex Hormone Treatment in Transsexual People. The Journal of Clinical Endocrinology & Metabolism, 88(12), 5723–5729. [DOI:10.1210/jc.2003-030520]
Torre, B. l., Norén, S., Hedman, M., & Diczfalusy, E. (1979). Effect of cyproterone acetate (CPA) on gonadal and adrenal function in men. Contraception, 20(4), 377–396. [DOI:10.1016/s0010-7824(79)80048-7]
Van Caenegem, E., Wierckx, K., Taes, Y., Schreiner, T., Vandewalle, S., Toye, K., Kaufman, J., & T’Sjoen, G. (2014). Preservation of volumetric bone density and geometry in trans women during cross-sex hormonal therapy: a prospective observational study. Osteoporosis International, 26(1), 35–47. [DOI:10.1007/s00198-014-2805-3]
van Dijk, D., Dekker, M. J., Conemans, E. B., Wiepjes, C. M., de Goeij, E. G., Overbeek, K. A., Fisher, A. D., den Heijer, M., & T’Sjoen, G. (2019). Explorative Prospective Evaluation of Short-Term Subjective Effects of Hormonal Treatment in Trans People—Results from the European Network for the Investigation of Gender Incongruence. The Journal of Sexual Medicine, 16(8), 1297–1309. [DOI:10.1016/j.jsxm.2019.05.009]
van Velzen, D. M., Paldino, A., Klaver, M., Nota, N. M., Defreyne, J., Hovingh, G. K., Thijs, A., Simsek, S., T’Sjoen, G., & den Heijer, M. (2019). Cardiometabolic Effects of Testosterone in Transmen and Estrogen Plus Cyproterone Acetate in Transwomen. The Journal of Clinical Endocrinology & Metabolism, 104(6), 1937–1947. [DOI:10.1210/jc.2018-02138]
Venner, P. M., Klotz, P. G., Klotz, L. H., Stewart, D. J., Davis, I. R., Orovan, W. L., & Ramsey, E. W. (1988). Megestrol acetate plus minidose diethylstilbestrol in the treatment of carcinoma of the prostate. Seminars in Oncology, 15(2 Suppl 1), 62–67. [Google Scholar] [PubMed]
Vereecke, G. (2019). Characterisation of testicular function and spermatogenesis in transgender women. (Master’s thesis, Ghent University.) [PDF]
Vereecke, G., Defreyne, J., Van Saen, D., Collet, S., Van Dorpe, J., T’Sjoen, G., & Goossens, E. (2020). Characterisation of testicular function and spermatogenesis in transgender women. Human Reproduction, 36(1), 5–15. [DOI:10.1093/humrep/deaa254]
Vita, R., Settineri, S., Liotta, M., Benvenga, S., & Trimarchi, F. (2018). Changes in hormonal and metabolic parameters in transgender subjects on cross-sex hormone therapy: A cohort study. Maturitas, 107, 92–96. [DOI:10.1016/j.maturitas.2017.10.012]
Vlot, M. C., Wiepjes, C. M., Jongh, R. T., T’Sjoen, G., Heijboer, A. C., & den Heijer, M. (2019). Gender‐Affirming Hormone Treatment Decreases Bone Turnover in Transwomen and Older Transmen. Journal of Bone and Mineral Research, 34(10), 1862–1872. [DOI:10.1002/jbmr.3762]
Wang, C., & Yeung, K. (1980). Use of low-dosage oral cyproterone acetate as a male contraceptive. Contraception, 21(3), 245–272. [DOI:10.1016/0010-7824(80)90005-0]
Warzywoda, S., Fowler, J. A., Wood, P., Bisshop, F., Russell, D., Luu, H., Kelly, M., Featherstone, V., & Dean, J. A. (2024). How low can you go? Titrating the lowest effective dose of cyproterone acetate for transgender and gender diverse people who request feminizing hormones. International Journal of Transgender Health, advance online publication. [DOI:10.1080/26895269.2024.2317395]
Wiepjes, C. M., Vlot, M. C., Klaver, M., Nota, N. M., de Blok, C. J., de Jongh, R. T., Lips, P., Heijboer, A. C., Fisher, A. D., Schreiner, T., T’Sjoen, G., & den Heijer, M. (2017). Bone Mineral Density Increases in Trans Persons After 1 Year of Hormonal Treatment: A Multicenter Prospective Observational Study. Journal of Bone and Mineral Research, 32(6), 1252–1260. [DOI:10.1002/jbmr.3102]
Wiepjes, C. M., Vlot, M. C., de Blok, C. J., Nota, N. M., de Jongh, R. T., & den Heijer, M. (2019). Bone geometry and trabecular bone score in transgender people before and after short- and long-term hormonal treatment. Bone, 127, 280–286. [DOI:10.1016/j.bone.2019.06.029]
Wierckx, K., Mueller, S., Weyers, S., Van Caenegem, E., Roef, G., Heylens, G., & T’Sjoen, G. (2012). Long‐Term Evaluation of Cross‐Sex Hormone Treatment in Transsexual Persons. The Journal of Sexual Medicine, 9(10), 2641–2651. [DOI:10.1111/j.1743-6109.2012.02876.x]
Wierckx, K., Van Caenegem, E., Schreiner, T., Haraldsen, I., Fisher, A., Toye, K., Kaufman, J. M., & T’Sjoen, G. (2014). Cross‐Sex Hormone Therapy in Trans Persons Is Safe and Effective at Short‐Time Follow‐Up: Results from the European Network for the Investigation of Gender Incongruence. The Journal of Sexual Medicine, 11(8), 1999–2011. [DOI:10.1111/jsm.12571]
Winkler-Crepaz, K., Müller, A., Böttcher, B., & Wildt, L. (2017). Hormonbehandlung bei Transgenderpatienten. [Hormone treatment of transgender patients.] Gynäkologische Endokrinologie, 15(1), 39–42. [DOI:10.1007/s10304-016-0116-9]
Winters, S. J., Wang, C., & (2009). LH and Non-SHBG Testosterone and Estradiol Levels During Testosterone Replacement of Hypogonadal Men: Further Evidence That Steroid Negative Feedback Increases as Men Grow Older. Journal of Andrology, 31(3), 281–287. [DOI:10.2164/jandrol.109.009035]
Yang, W., Hong, T., Chang, X., Han, M., Gao, H., Pan, B., Zhao, Z., & Liu, Y. (2024). The efficacy of and user satisfaction with different antiandrogens in Chinese transgender women. International Journal of Transgender Health, advance online publication. [DOI:10.1080/26895269.2024.2323514]
Zitzmann, M., Rohayem, J., Raidt, J., Kliesch, S., Kumar, N., Sitruk-Ware, R., & Nieschlag, E. (2017). Impact of various progestins with or without transdermal testosterone on gonadotropin levels for non-invasive hormonal male contraception: a randomized clinical trial. Andrology, 5(3), 516–526. [DOI:10.1111/andr.12328]
Zubiaurre-Elorza, L., Junque, C., Gómez-Gil, E., & Guillamon, A. (2014). Effects of Cross-Sex Hormone Treatment on Cortical Thickness in Transsexual Individuals. The Journal of Sexual Medicine, 11(5), 1248–1261. [DOI:10.1111/jsm.12491]
\ No newline at end of file
+Low Doses of Cyproterone Acetate Are Maximally Effective for Testosterone Suppression in Transfeminine People - Transfeminine Science
Low Doses of Cyproterone Acetate Are Maximally Effective for Testosterone Suppression in Transfeminine People
By Aly | First published July 1, 2019 | Last modified March 30, 2024
Abstract / TL;DR
Cyproterone acetate (CPA) is a progestogen and antiandrogen which is widely used in transfeminine hormone therapy. It is far more potent as a progestogen than as an androgen receptor antagonist. CPA has typically been used at doses of 1 to 2 mg/day as a progestogen in cisgender women and at doses of 50 to 300 mg/day as an antiandrogen. At typical antiandrogen doses of CPA, there is profound progestogenic overdosage as well as associated side effects and risks. CPA has antigonadotropic effects due to its progestogenic activity and thereby suppresses testosterone levels. By itself, CPA can maximally suppress testosterone levels by 50 to 70%, and in combination with even small amounts of estrogen, it can fully suppress gonadal testosterone production and thereby reduce testosterone levels by about 95%—or well into the female range. Although doses of CPA of 50 to 100 mg/day have been used in transfeminine people historically, it is now clear that 5 to 10 mg/day CPA has maximal or near-maximal effectiveness in terms of suppression of testosterone levels. CPA alone is most commonly available as 50-mg tablets. These tablets can be split with a pill cutter and taken once every day to once every other day to achieve an overall CPA dosage of 6.25 to 12.5 mg/day. These lower doses of CPA are not only much more cost-effective than traditional doses but are also likely to have better tolerability and safety. Due to the retained effectiveness of lower CPA doses and the known dose-dependent risks of CPA, doses of CPA used clinically in transfeminine people have been in a rapid decline.
Introduction
This article is about the dosage of cyproterone acetate (CPA), a progestin and antiandrogen, for use in hormone therapy for transfeminine people. It argues for the use of lower doses of CPA and goes fairly in-depth to justify these doses. If you are only interested in recommended doses of CPA for transfeminine people, they can be found in the Recommended Dosages section below.
Potency, Conventional Dosages, and Health Risks
CPA is a potent progestogen, with an ovulation-inhibiting dosage of about 1 mg/day and endometrial transformation dosage of about 1 to 3 mg/day in cisgender women (Wiki; Table; Endrikat et al., 2011). These dosages of CPA are similar in strength of progestogenic effect to those of normal progesterone production and levels during the luteal phase of the menstrual cycle in premenopausal women (which are about 25 mg/day and 15 ng/mL, respectively). In relation to the preceding, when CPA is used as a progestogen in cisgender women, for instance in birth control pills and menopausal hormone therapy preparations, it is formulated at a dose of 1 or 2 mg per tablet (Wiki).
In contrast to its progestogenic activity, CPA is far less potent as an androgen receptor antagonist (Wiki). When used as an antiandrogen, it is generally given at a dosage of 50 to 300 mg/day, both in cisgender women and men. A dosage of 50 to 100 mg/day is typical for androgen-dependent skin and hair conditions like acne and hirsutism in women and a dosage of 100 to 300 mg/day is typically used for prostate cancer in men (specifically 100–200 mg/day for CPA combined with castration and 200–300 mg/day for CPA monotherapy) (Wiki). As such, CPA is generally formulated at a dose of 50 or 100 mg per tablet for use in androgen-dependent conditions (Wiki). As an antiandrogen, CPA has a dual mechanism of action of both suppressing testosterone levels via its progestogenic activity at low doses and additionally blocking the actions of testosterone directly at the androgen receptor at higher doses.
Because CPA is so much more potent as a progestogen than as an androgen receptor antagonist, there is profound overdosage of progestogenic effect when CPA is used as an antiandrogen at typical clinical dosages. This is described in the following three literature excerpts by Jürgen Hammerstein, one of the scientists who developed CPA (Hammerstein et al., 1975; Hammerstein, 1990; Hammerstein, 1979):
Like chlormadinone acetate, its parent compound, CPA is also a strong progestogen with the endometrial transformation dose of both drugs being between 20 and 30 mg. […] To take full therapeutic advantage of its antiandrogenicity, CPA must be administered in doses per month that are 30 times the physiological equivalent of progesterone production in the cycle. CPA, although the most useful compound available in this field at the moment, cannot be considered therefore an ideal antiandrogen, all the more as some of the side effects may be related to the progestational overdosage rather than to the administered antiandrogenic activity. […] Adverse reactions like tiredness, lassitude, and increase in body weight are possibly due to the enormous overdose of progestational activity in the formula which is necessary to take full advantage of the antiandrogenicity of CPA.
Fixson (1963) tested CPA in ovariectomized women after pre-treatment with oestrogens; with a transformation dose of 20–30 mg this proved a powerful progestogen. The potency of CPA in the menses delay test is not exactly known, but has been estimated to be below 1 mg/day (Miller and Jacobs 1986). In relation to this progestational potency, its antiandrogenicity must be considered rather weak. Thus, in order to take full advantage of the latter, 100 mg CPA must be given daily, i.e. three times the cyclic transformation dose per day (Hammerstein and Cupceancu 1969); notably, this parameter is equivalent to the total progesterone production of a corpus luteum throughout its entire cyclic life span.
CPA may be characterized endocrinologically as possessing strong progestational [and] moderate anti-androgenic […] potencies. […] Its progestational activity, in terms of the transformation dose in the oestrogen-primed human endometrium, is 20–30 mg [per month/cycle] which is comparable to that of chlormadinone acetate and other strong progestogens. To take full clinical advantage of its anti-androgenicity not less than 50–100 mg CPA must be taken orally per day, which totals 2 to 3 times the progestational activity the female organism is exposed to throughout a complete ovulatory menstrual cycle. Thus unless much lower and less efficacious doses of CPA are used, a tremendous progestational overdosage must be accepted. […] As already pointed out CPA is endocrinologically not a well-balanced compound because of the strong preponderance of the progestational over the anti-androgenic potency. A way to avoid the heavy progestogen overdosage inherent with the high-dose reverse sequential therapy would be to combine the low-dose contraceptive formulation just mentioned with a pure anti-androgen such as free cyproterone. […] It must be emphasized that CPA is far from being an ideal drug for the anti-androgenic treatment of hirsutism because its progestational potency is much too strong and it is not effective when administered topically. Therefore it is worthwhile looking for better-balanced anti-androgenic compounds for the future.
The massive overdosage of progestogenic effect that occurs at such doses of CPA is likely responsible for the known adverse effects and risks of higher doses of CPA (Wiki). Examples of these side effects include fatigue, depression, weight gain, high prolactin levels (Wiki), benign brain tumors (Aly, 2020; Wiki; Table; Table), blood clots (Wiki), and cardiovascular problems (Wiki). Such risks are dose-dependent and have not been associated with 1 or 2 mg/day CPA (with the exception of an expected increase in the risk of blood clots in combination with oral estrogens for birth control or menopausal hormone therapy). The risk of liver toxicity with CPA is also dose-dependent, with elevated liver enzymes occurring mostly only at a dosage of 20 mg/day and above and rare cases of liver failure occurring almost exclusively at dosages of 100 mg/day and above (Wiki; Table). As such, there is good rationale for using the lowest possible effective dosage of CPA, an approach that is likely to minimize risks.
In transfeminine people, CPA has historically been used at a dosage of 50 to 100 mg/day (e.g., Moore, Wisniewski, & Dobs, 2003). Some earlier papers have recommended even higher doses of CPA, for instance 100 to 150 mg/day (Asscheman & Gooren, 1993). In 2017, the Endocrine Society published the latest edition of their clinical practice guidelines on hormone therapy for transgender people and reduced their recommended dosage of CPA from 50–100 mg/day to 25–50 mg/day (Hembree et al., 2017; Hembree et al., 2009). This was motivated in part by increasing knowledge and awareness of the risks of higher doses of CPA and by findings that these lower doses of CPA were still effective. However, it is likely that even these new lower dosages are still far in excess of what is really needed.
Testosterone Suppression with Low and High Doses
Progestogens by themselves, including CPA, are able to considerably suppress testosterone levels in gonadally intact people assigned male at birth. Around a dozen small and low-quality but nonetheless notable studies of low-dose CPA from the 1970s and early 1980s found that 5 to 10 mg/day CPA suppressed testosterone levels by about 40 to 70% in healthy young men (Table 1). A couple of individual studies notably reported virtually identical suppression of testosterone levels with 5 mg/day versus 10 mg/day CPA (both ~50% suppression) (Wang & Yeung, 1980; Graph) and with 10 mg/day versus 20 mg/day CPA (both ~60–70% suppression) (Koch et al., 1976; Koch et al., 1975; Graph). This lack of additional testosterone suppression with a doubling of dosage within studies suggests that testosterone suppression with CPA might have actually been maximal at a dosage of only 5 or 10 mg/day. A more modern study, which used a newer and more reliable analytic method for quantification of blood testosterone, found that 10 mg/day CPA suppressed testosterone levels by 66%, from about 600 ± 150 ng/dL to about 185 ng/dL (Meriggiola et al., 2002a; Graph). Similarly, another more modern study found that 10 to 20 mg/day CPA suppressed testosterone levels by 65%, from about 431 ng/dL to about 149 ng/dL, with no reported differences between doses (Zitzmann et al., 2017; Graph).
Table 1: Levels of testosterone and other sex hormones with CPA at low doses (5–30 mg/day):
Treatment and subjects
Findings
Source(s)
30 mg/day CPA in 5 normal males
T decreased “remarkably”. Exact values not given, but has graphs of T levels in a few individuals. After 30 mg/day, 5 mg/day was tried in one case and was not as effective in suppressing sperm production or T. Also reported decreases in gonadotropin excretion.
10 or 20 mg/day CPA in 15 normal healthy fertile males (age 25–35 years) (7 in 10 mg/day group and 8 in 20 mg/day group)
“Androgens (mainly T)” decreased by 60% for both 10 and 20 mg/day. Inconsistent changes in LH and slight decrease in FSH. Exact values not given, except in graphs.
10 mg/day CPA in 10 young healthy fertile men (age mean 27.2 ± 3.2 (range 21–35) years)
T decreased by 70%, DHT by 50%, LH by 30%, and FSH by 40%, while PRL increased by 75%. T was 495 ± 66 ng/dL before, 154 ± 23 ng/dL after 4 weeks, and 187 ± 38 ng/dL after 12 weeks. Also has values and graphs for other hormones.
20 mg/day CPA in 10 healthy males (age 26–55 years)
T decreased by 73% (range 71–75%), from 482 ng/dL (range 410–560 ng/dL) to 130 ng/dL (110–162 ng/dL). DHT decreased by 51% (range 47–55%), LH by 39% (range 34–45%), FSH by 66% (range 47–78%), 17-OH-P4 by 59%, A4 by 30%, TS by 34%, and DHTS by 35%. Also has exact values and graphs for other hormones.
5 or 10 mg/day CPA in 7 males (4 in each group; 1 received both 5 and 10 mg/day CPA at different times)
T change was “−40%” or “–50%”. At 5 mg/day, T was 745 ng/dL before, 460 ng/dL with treatment (–38%), and 668 ng/dL after discontinuation. At 10 mg/day, T was 708 ng/dL before, 398 ng/dL with t (reatment–44%), and 670 ng/dL after discontinuation. Also reported LH and FSH levels.
0, 5, or 10 mg/day CPA in 25 normal healthy males (age 20–51 years); 7 in 5 mg group (mean 37 ± 10 years), 8 in 10 mg group (mean 32 ± 8 years), 10 in 0 mg group (mean 32 ± 10 years)
At 5 mg/day, T decreased from 663 ± 120 ng/dL to 320 ± 160 ng/dL (−52%), and at 10 mg/day, T decreased from 692 ± 180 ng/dL to 340 ± 160 ng/dL (−51%). E2 decreased in parallel to T. At 5 mg/day, LH decreased from 2.1 ± 0.7 IU/L to 1.4 ± 0.5 IU/L (−33%), and at 10 mg/day, LH decreased from 2.3 ± 1.0 IU/L to 1.2 ± 0.5 IU/L (−48%). At 5 mg/day, FSH decreased from 3.1 ± 1.9 IU/L to 1.8 ± 0.9 IU/L (−42%), and at 10 mg/day, FSH decreased from 2.7 ± 1.0 IU/L to 1.5 ± 0.7 IU/L (−44%).
10 or 25 mg/day CPA in 4 healthy men (age 29–37 years); 3 in 10 mg group, 1 in 25 mg group
T “slightly reduced”. E “more significantly lowered”. LH not significantly changed. FSH “reduced” in “more or less all cases”. Exact hormone levels not given, but graphs provided with the values.
10 mg/day CPA (also placebo and 2, 5, and 10 mg/day dienogest) in 5 healthy men in each group
With CPA, T decreased from ~600 ± 150 ng/dL to ~185 ng/dL (–66 ± 4%). Also reported LH, FSH, and SHBG, as well as hormonal changes with placebo and dienogest (2, 5, and 10 mg/day).
10 or 20 mg/day CPA in 14 healthy young men (7 in each group)
T decreased from ~431 ng/dL at baseline to ~149 ng/dL with CPA (–65%) for the 10 and 20 mg/day doses combined. Values for dose subgroups not given. No significant differences between LH/FSH suppression between groups (which is indirectly suggestive of no differences in T suppression as well). Also reported hormone levels with other progestins.
Studies with other progestogens, such as desogestrel, dienogest, and medroxyprogesterone acetate, have consistently found that maximal suppression of testosterone levels in men occurs at a dosage that is between 5 and 10 times that of the ovulation-inhibiting dosage in cisgender women (Wiki; Wiki; Wiki). Another study is likewise suggestive of this for norethisterone acetate and levonorgestrel (Zitzmann et al., 2017; Graph). Along similar lines, doses of progestogens investigated for use in male hormonal contraception, in which the goal is antigonadotropic effects and the lowest fully effective dose is targeted, have been noted as being between 5 and 12 times the doses used in cisgender women (Foegh, 1983). Based on an ovulation-inhibiting dosage of CPA of 1 mg/day, these findings would imply that suppression of testosterone levels with CPA would likely be maximal at a dose of between 5 and 10 mg/day. In accordance, this dose range matches up with the findings of the studies above.
Although progestogens can considerably suppress testosterone levels at maximally effective dosages, it has been found that a “recovery” or “escape phenomenon”, in which testosterone levels eventually increase back to higher levels, occurs when progestogen monotherapy is used on a long-term basis. This has most notably been observed with the related progestogen megestrol acetate (Wiki), but has also been seen with CPA (Goldenberg & Bruchovsky, 1991; Saborowski, 1987; Jacobi, Tunn, & Senge, 1982). In one of these studies, testosterone levels were initially suppressed by CPA by about 70%, but increased back to about 50% of baseline between 6 and 12 months of therapy, remaining stable thereafter up to 24 months. The testosterone escape phenomenon should be kept in mind in the context of progestogen monotherapy for testosterone suppression. In contrast to progestogen monotherapy, this phenomenon has not been associated with combined estrogen and progestogen therapy.
Testosterone Suppression in Combination with Estrogen
CPA is generally used in combination with an estrogen in transfeminine people. Estrogens suppress testosterone levels similarly to progestogens. The combination of an estrogen and a progestogen is synergistic in terms of testosterone suppression and results in suppression of testosterone levels with lower doses than with either an estrogen or progestogen alone (Fink, 1979; Geller & Albert, 1983; Bastianelli et al., 2018). Although estrogens can suppress testosterone levels to an equivalent extent as surgical or medical castration (i.e., orchiectomy or GnRH agonists/antagonists), this usually requires relatively high estrogen levels, for instance in the range of 200 to 500 pg/mL (Wiki; Graphs). Because of the high and supraphysiological estradiol levels required for maximal or near-maximal suppression of testosterone levels, lower doses of estradiol are frequently combined with antiandrogens and/or progestogens to block or suppress remaining testosterone levels instead.
CPA, as mentioned earlier, leads to an incomplete suppression of plasma testosterone levels, which decrease by about 70% and remain at about three times castration values. In a very systematic approach to the problem, Rennie et al. (59) investigated and compared 12 different procedures of androgen deprivation. These authors found that the combination of CPA with an extremely low dose (0.1 mg/d) of [diethylstilbestrol (DES)] led to a very effective withdrawal of androgens in terms of plasma testosterone and tissue dihydrotestosterone. The same group later showed that 200 mg of CPA, and even 100 mg/day, was sufficient to achieve a similar endocrine response, which was correlated to very favorable clinical responses in a Phase II situation (60,61). The approach has many potential advantages, and, from an endocrinological point of view, is very logical: this regimen combines the testosterone-reducing effects of two compounds, therefore, only small amounts of estrogen are required to bring down plasma testosterone to approximately castrate levels. Once castrate levels have been achieved, only low doses of CPA are necessary to counteract remaining androgens, mainly of adrenal origin. The regimen was shown to be associated with few side effects and a very low cost. The combination of low-dose CPA with low-dose DES was never studied in a Phase III situation in comparison to standard management. Considering the endocrine results and the observations in patients treated with this regimen (60), this combination treatment is very likely to be competitive with other standard forms of therapy.
A 2016 study of 50 mg/day CPA and 1 to 2 mg/day transdermal estradiol gel in transfeminine people showed that estradiol levels of about 45 pg/mL with CPA were insufficient to achieve female/castrate levels of testosterone, instead resulting in testosterone levels of about 120 to 190 ng/dL (Gava et al., 2016; Graph). Conversely, estradiol levels of about 85 pg/mL with CPA achieved complete suppression of gonadal testosterone production, with resulting testosterone levels of about 20 ng/dL. As such, a certain minimum level of estradiol with CPA appears to be required for complete testosterone suppression. A 2019 study of CPA and oral estradiol valerate in transfeminine people indicated that testosterone levels were still fully suppressed with median estradiol levels of 76 pg/mL and 25th percentile estradiol levels of 63 pg/mL (Angus et al., 2019; Graph).
Figures 5–7: Testosterone levels with CPA plus low doses/levels of estrogens in men and transfeminine people. Sources: Top-left: Goldenberg et al. (1988). Top-right: Gava et al. (2016). Bottom: Angus et al. (2019). See also on Wikipedia: Gallery. Note for the graph on the top right that the mean transdermal estradiol dosage increased between 6 and 12 months and this was likely responsible for the improvement in testosterone suppression.
Fung and colleagues showed that the combination of either 25 or 50 mg/day CPA with a moderate dosage of oral estradiol (~3.5 mg/day) or transdermal estradiol (~3.5 mg/day gel or ~100 μg/day patch) resulted in equivalent and complete suppression of gonadal testosterone production (~95% suppression of testosterone levels) in transfeminine people (Fung, Hellstern-Layefsky, & Lega, 2017). These dosages of estradiol would be expected to achieve estradiol levels of around 100 pg/mL on average (Aly, 2020; Wiki). This study was notably published 6 months before the 2017 second edition of the Endocrine Society guidelines were released (Hembree et al., 2017), and was probably responsible for the decrease in their recommended dosage of CPA from 50–100 mg/day to 25–50 mg/day.
Few studies to date have assessed testosterone suppression with low-dose CPA in combination with a low or moderate dosage of an estrogen. However, based on the fact that 5 to 10 mg/day CPA alone is probably maximal in terms of suppression of testosterone levels, it is likely that such dosages of CPA will be similarly effective as higher dosages. In accordance, studies of 5 to 12.5 mg/day CPA plus upper physiological replacement dosages of testosterone have demonstrated undetectable gonadotropin levels (<0.5 IU/L) and hence complete suppression of testicular function in healthy young men (Meriggiola et al., 1998; Meriggiola et al., 2002b). Estradiol is a more powerful antigonadotropin than testosterone (Wiki), so these findings probably apply to CPA in combination with physiological replacement levels of estradiol as well (e.g., mean estradiol levels of 100–200 pg/mL).
Accordingly, Meyer et al. (2020) assessed a dosage of CPA in combination with estradiol in 155 transfeminine people and found no difference in testosterone levels with 10, 25, or 50 mg/day CPA; testosterone levels were strongly suppressed with all three doses (to about 15–20 ng/dL on average, or into the lower end of the normal female range). The estradiol forms and doses used in this study were oral estradiol valerate (median 6 mg/day, range 3–10 mg/day), transdermal estradiol gel (median 2.25 mg/day, range 1.5–6 mg/day), and transdermal estradiol patches (100 μg/day in all cases). Estradiol levels were about 100 pg/mL on average, with an interquartile range (i.e., difference between 75th and 25th percentiles) of about 100 pg/mL. This study demonstrates that, provided estradiol levels are adequate, no more than 10 mg/day CPA is needed to fully suppress testosterone levels in transfeminine people. Another study likewise found no difference between <20 mg/day and >50 mg/day CPA in terms of testosterone suppression in transfeminine people (Even-Zohar et al., 2020).
Even doses of CPA lower than 5 mg/day (e.g., 2 mg/day) may be usefully effective for testosterone suppression if combined with sufficient levels of estradiol, although this has not been studied and remains to be validated. But there is certainly precedent for the notion when looking at studies with other progestogens. As an example, one study using 10 mg/day oral medroxyprogesterone acetate (which is roughly equivalent to 1 mg/day CPA in terms of ovulation inhibition in premenopausal women; Table) observed 63% lower testosterone levels (215 ng/dL vs. 79 ng/dL) when added to estradiol and spironolactone therapy in transfeminine people (Jain, Kwan, & Forcier, 2019). Analogous effects on testosterone levels would be anticipated for very-low-dose CPA. Moreover, such dosages of CPA would have the advantage of actually being physiological in terms of progestogenic exposure.
The androgen receptor antagonism of CPA is relatively weak in terms of potency; dosages of CPA of 50 to 300 mg/day seem to be necessary for meaningful or considerable androgen receptor antagonism. Unfortunately, such doses also result in extreme progestogenic overdosage and are associated with considerably greater risks and adverse effects. As a result, the use of such doses of CPA should no longer be considered advisable. Instead, CPA should be used at lower doses simply as a progestogen to suppress testosterone levels. As such, the highest effective dosage of CPA for testosterone suppression, which is probably about 10 mg/day or less (12.5 mg/day also being acceptable), should be around the maximal dosage of CPA that is used in transfeminine people.
It should be emphasized that since the combination of an estrogen and CPA can easily suppress testosterone levels well into the female/castrate range (typically to below average female levels), there isn’t necessarily a requirement for concomitant androgen receptor blockade. In any case, if androgen receptor antagonism to neutralize the remaining female/castrate levels of testosterone is still necessary or desired (e.g., to treat persisting acne or for some other purpose), a low dosage of a non-progestogenic androgen-receptor antagonist like spironolactone (e.g., 100–200 mg/day) or bicalutamide (e.g., 12.5–25 mg/day) can be added to CPA to more safely achieve this than use of higher CPA doses.
Recommended Dosages
Dosage for Testosterone Suppression
Estrogen Plus Cyproterone Acetate
The following recommended dosages of CPA in transfeminine people are for the combination of CPA with an estrogen and are specifically for achieving maximal suppression of testosterone levels:
Table 2: Recommended doses of CPA in combination with estrogen for maximal testosterone suppression in transfeminine people:
Form
Min. dosage
Max. dosage
Amount
10 mg tablets
5 mg/day
10 mg/day
1/2 of a tablet to 1 whole tablet per day
50 mg tablets
6.25 mg/day
12.5 mg/day
1/8th of a tablet to 1/4th of a tablet per day
Start with the minimum dosage of CPA for one month. After one month, have testosterone levels tested and confirm that they are in the normal female/castrate range (<50 ng/dL). Regardless of dosage, a concomitant minimum estradiol level of around 65 pg/mL needs to be attained in order to allow for complete suppression of testosterone levels with CPA. If testosterone levels aren’t sufficiently suppressed after a month and estradiol levels are adequate, increase to the maximum CPA dosage and re-check testosterone levels after another month. Alternatively, the dosage of estradiol can be increased instead; higher estradiol levels result in greater testosterone suppression as well.
Cyproterone Acetate Alone
The use of CPA alone (i.e., as a monotherapy for testosterone suppression) is not recommended due to the risk of decreased bone mineral density and other symptoms of sex-hormone deficiency (Wiki; Aly, 2019). In any case, the recommended dosages for CPA without an estrogen are essentially the same as those listed above of the combination of an estrogen with CPA for testosterone suppression. However, the higher CPA dose (10–12.5 mg/day) may be preferable for good measure in this scenario.
Dosage for Progestogenic Effects
The following recommended dosages of CPA in transfeminine people are for progestogenic effects similar to normal physiological exposure (equivalent of luteal-phase progesterone levels):
Table 3: Recommended doses of CPA for physiological progestogenic effects in transfeminine people:
Form
Dosage
Amount
10 mg tablets
2.5 mg/day
1/4th of a tablet per day
50 mg tablets
3.125 mg/day
1/16th of a tablet per day
Achieving Desired Dosages
CPA is available pharmaceutically most widely as 50-mg tablets. This can make achieving desired low doses of CPA more difficult. For splitting CPA tablets into small fractions, a pill cutter can be used. Additionally, CPA can be taken once every 2 or 3 days instead of once every day to help further divide doses. It is notable that CPA has a relatively long half-life in the body of about 1.5 to 2 days (but possibly up to 4 days) (Wiki; Graph). Hence, taking it once every other day instead of once per day, or even less frequently like once every 3 days, has sound basis and is likely to be entirely viable.
Updates
Update 1: GoLoCypro Study (In-Progress)
The GoLoCypro study (2019–2022) (more info) is being conducted by Dr. Judith Dean at the University of Queensland in Australia. It’s assessing the influence of estradiol plus CPA on testosterone levels at five different CPA dose levels (12.5 mg 2x/week, 12.5 mg/2 days, 12.5 mg/day, 25 mg/day, and 50 mg/day) in a total of 120 to 350 transfeminine people. CPA doses are being titrated to the minimum that maintain testosterone levels within the therapeutic goal range of 0.5 to 1.5 nmol/L (14–43 ng/dL). The study is among the first dose-ranging studies of CPA in transfeminine people to be conducted and is eagerly anticipated due to the valuable information that it should provide in terms of the minimum effective dosage of CPA for adequate testosterone suppression in transfeminine hormone therapy.
Update 2: Kuijpers et al. (2021) and Even Zohar et al. (2021)
Kuijpers, S. M., Wiepjes, C. M., Conemans, E. B., Fisher, A. D., T’Sjoen, G., & den Heijer, M. (2021). Toward a lowest effective dose of cyproterone acetate in trans women: Results from the ENIGI study. The Journal of Clinical Endocrinology & Metabolism, 106(10), e3936–e3945. [DOI:10.1210/clinem/dgab427]
The study employed estradiol (2–6 mg/day oral (as estradiol valerate), 50–150 μg/day patch, or gel) plus five different dose levels of CPA—0 mg/day (no CPA), 10 mg/day, 25 mg/day, 50 mg/day, and 100 mg/day. It found incompletely suppressed testosterone in the no CPA group but full and equivalent testosterone suppression with all doses of CPA. The results were as follows:
CPA dosage
0 mg/day
10 mg/day
25 mg/day
50 mg/day
100 mg/day
Initial subjects (n)
34
4
234
599
11
Dose increased (n)
16
1
11
2
0
Dose decreased (n)
0
0
4
40
7
T levels (nmol/L)
5.5
0.9
0.9
1.1
0.9
T levels (ng/dL)
~160
~26
~26
~32
~26
T <2 nmol/L [<~58 ng/dL] (%)
46.3
92.3
96.2
93.4
100.0
Abbreviations: T = testosterone.
The total numbers of subjects and blood tests after CPA dose increases/decreases were not provided. Hence, the exact total number of people and tests for the 10 mg/day group can’t be stated with certainty. The total number of tests for this group was at least 13 based on the testosterone suppression percentage provided however (92.3% or 12/13 but could potentially be 24/26, etc.). Regarding the small number of subjects/tests for the 10 mg/day group, the authors stated the following:
This study is part of the ENIGI initiative, a multicenter prospective cohort study. The main treatment protocol for trans women in this study was 50 mg of CPA daily combined with estrogens. In the first year of study inclusion, a few participants received a dose of 100 mg of CPA. Shortly thereafter, inhospital protocol changed to 50 mg of CPA. As more health concerns related to CPA use were raised over the years, the dose was further lowered from 50 mg to 25 mg and, finally, to 10 mg. However, due to the coronavirus (COVID-19) pandemic, limited results of participants with 10 mg of CPA were available for analysis.
Besides testosterone suppression, the study found that 10 mg/day CPA had less influence on prolactin and high-density lipoprotein (HDL) cholesterol levels than the higher doses of CPA. The study also assessed liver enzyme levels but found no differences between CPA doses.
The authors concluded with the following:
In conclusion, in this cohort of trans women, 10 mg of CPA was found to be effective in lowering testosterone concentrations to the range observed in cis women. A dose of 10 mg was equally effective as higher doses, was found to have less influence on prolactin concentrations and allows higher HDL-C concentrations to be maintained. While GnRH agonists are preferred over CPA due to the fewer associated long-term side effects, this study shows that CPA at a low dose is a viable option when GnRH agonists are contra-indicated, not available, or not reimbursed. Future research should focus on assessing the effectiveness of an even lower dose of CPA (e.g., 5 mg) and the potential long-term side effects.
Around the same that this study was published, Guy T’Sjoen (one of the authors of the study) and other colleagues in a review of optimal hormone therapy for transfeminine people recommended a dosage of no more than 10 or 12.5 mg/day CPA for no longer than 2 years (Glintborg et al., 2021). T’Sjoen is notable in being regarded as one of the foremost experts in transgender medicine and is a coauthor of the Endocrine Society transgender care guidelines (Hembree et al., 2017).
Shortly after the study of Kuijpers and colleagues and also in June 2021, Even Zohar and colleagues in Israel published the following study on low doses of CPA in transfeminine people:
Even Zohar, N., Sofer, Y., Yaish, I., Serebro, M., Tordjman, K., & Greenman, Y. (2021). Low-Dose Cyproterone Acetate Treatment for Transgender Women. The Journal of Sexual Medicine, 18(7), 1292–1298. [10.1016/j.jsxm.2021.04.008]
This study was initially reported as a conference abstract in May 2020 (Even-Zohar et al., 2020).
In the introduction section of the paper, the authors stated the following:
Treatment guidelines published by several organizations are available and assist clinicians in treating transgender women.4,7−9 A wide range of regimens for CPA administration have been proposed. By and large, the recommended doses have decreased over the years: doses of 50–100 mg/day were suggested in the 2009 Endocrine Society Guidelines,10 and amended to 25–50 mg/day in 2017.7 The proposed CPA doses were 12.5–25 mg/day in the 2019 guidelines of the Australian Professional Association for Transgender Health,4 and they were amended to 10–50 mg/day in the 2020 guidelines of the European Society for Sexual Medicine.8 There are no publications on data that compare different doses of CPA for efficacy or safety.
The researchers found that estradiol plus low-dose CPA (10–20 mg/day) suppressed testosterone levels to an equivalent extent as estradiol plus high-dose CPA (50–100 mg/day). Testosterone levels were suppressed into the female/castrate range or near so in both groups (generally ≤2 nmol/L or ≤58 pg/mL). Of the 38 transfeminine people on low-dose CPA, 32 (84%) were on 10 mg/day CPA and 6 (16%) were on 20 mg/day CPA (mean dose 11.6 ± 3.7 mg/day). Estradiol was given as transdermal estradiol patch (mean dose 83.7 ± 36.5 μg/day), transdermal estradiol gel (mean dose 3.8 ± 1.2 g/day), or oral estradiol (mean dose 4.1 ± 1.7 mg/day). Mean estradiol levels ranged from ~110 to 350 pmol/L (~30–95 pg/mL) in the low- and high-dose CPA groups over the follow-up period. Besides showing equivalent testosterone suppression, prolactin levels were significantly lower with low-dose CPA than with high-dose CPA (398 ± 69 mIU/mL vs. 804 ± 121 mIU/mL at 12 months of hormone therapy, respectively).
Based on their findings, the authors stated the following:
We suggest an adjustment of current clinical practice guidelines to recommend lower doses of CPA for the treatment of transgender women.
Both Kuijpers et al. (2021) and Even Zohar et al. (2021) claimed to be the first to demonstrate the efficacy of low-dose CPA in transfeminine people. However, that achievement actually appears to belong to Meyer et al. (2020), who in February 2020 found that estradiol plus 10, 25, or 50 mg/day CPA gave equivalent testosterone suppression across CPA doses in transfeminine people.
Although their study was not about CPA and testosterone suppression, Lim et al. (2020) reported in May/July 2020 that testosterone levels in transfeminine people were median (IQR) 0.6 (0.4–1.0) nmol/L for oral estradiol and 0.9 (0.7–1.6) nmol/L for transdermal estradiol in a mixed group of transfeminine people (n=26 total) on estradiol plus low-dose CPA (12.5 (12.5–18.8) mg/day) (n=14), estradiol alone post-gonadectomy (n=9), and estradiol plus spironolactone (n=3).
In December 2021, the following case report of fatal liver failure with low-dose CPA was published:
Kumar, P., Reddy, S., Kulkarni, A., Sharma, M., & Rao, P. N. (2021). Cyproterone acetate induced Acute liver failure: Case report and review of the literature. Journal of Clinical and Experimental Hepatology, 11(6), 739–741. [DOI:10.1016/j.jceh.2021.01.003]
The case report describes a 30-year-old cisgender woman who was on 25 mg/day CPA for treatment of hirsutism (excessive facial/body hair growth) for 6 months and developed acute liver failure. Four days following hospitalization, she died. This is the second published case report of liver toxicity with CPA at a dosage below 100 mg/day (the first and only other case was at 50 mg/day) (Wiki; Table). It is also the first report of liver failure in a cisgender woman taking CPA. The case indicates that CPA even at a relatively low dose of 25 mg/day is not fully safe in terms of liver toxicity. It further emphasizes the importance of using the lowest effective doses of CPA in transfeminine people (no more than 10–12.5 mg/day).
Update 4: Coleman et al. (2022) [WPATH SOC8 Guidelines]
In September 2022, the World Professional Association for Transgender Health (WPATH) Standards of Care for the Health of Transgender and Gender Diverse People Version 8 (SOC8) were published and made recommendations for transgender hormone therapy for the first time (Coleman et al., 2022). These guidelines recommended a dose of CPA of 10 mg/day in transfeminine people (Coleman et al., 2022). This dose is substantially lower than previous doses recommended by transgender care guidelines and is the first time that major guidelines have recommended a CPA dosage this low. The WPATH SOC8 cited Kuijpers et al. (2021) in support of this recommendation (though notably not Even Zohar et al. (2021) or Meyer et al. (2020)) and also discussed the dose-dependent risks of CPA such as meningiomas and high prolactin levels (Coleman et al., 2022). Considering the key position and importance of the WPATH SOC in transgender health, it is likely that lower CPA doses in transfeminine hormone therapy will now be widely adopted throughout the world. Continued use of higher CPA doses should be considered out of step with current accepted evidence-based practice.
Update 5: Collet et al. (2023)
In October 2022, a study more carefully assessing androgen suppression with estradiol plus CPA in transfeminine people was published:
Collet, S., Gieles, N., Wiepjes, C. M., Heijboer, A. C., Reyns, T., Fiers, T., Lapauw, B., den Heijer, M., & T’Sjoen, G. (2023). Changes in serum testosterone and adrenal androgen levels in transgender women with and without gonadectomy. The Journal of Clinical Endocrinology & Metabolism, 108(2), 331–338. [DOI:10.1210/clinem/dgac576]
In the study, 275 transfeminine people were treated with estradiol plus CPA, and levels of total testosterone, free testosterone, and the adrenal androgensdehydroepiandrosterone (DHEA), dehydroepiandrosterone sulfate (DHEA-S), and androstenedione (A4) were measured using liquid chromatography–mass spectrometry (LC–MS) at baseline and during follow-ups at 3 months, 12 months, 2 to 4 years, and after surgical gonadal removal (at which time CPA was discontinued). Estradiol was measured both with LC–MS (Amsterdam clinic) and with immunoassays (Ghent clinic). The forms and doses of estradiol used were most commonly oral estradiol valerate 4 mg/day or a transdermal estradiol patch 100 μg/day, while the dosage of CPA was usually 25 or 50 mg/day. About half of the transfeminine people eventually underwent surgical gonadal removal, usually after 2 years of hormone therapy.
Median estradiol levels ranged from 49 to 75 pg/mL (180–275 pmol/L) with LC–MS and from 63 to 69 pg/mL (232–255 pmol/L) with immunoassays at different follow-ups. After 3 months of hormone therapy, total testosterone decreased by 97.1%, from 536 ng/dL (18.6 nmol/L) to 12 ng/dL (0.40 nmol/L), and free testosterone decreased by 98.3%, from 109 pg/mL (378 pmol/L) to 2.0 pg/mL (7.1 pmol/L). Thereafter, total and free testosterone levels remained stable. Levels of DHEA, DHEA-S, and A4 decreased by 24.9 to 28.0%, 20.1 to 23.5%, and 36.5%, respectively, and likewise did not further change after the first 3 to 12 months of hormone therapy. No changes in androgen levels occurred upon surgical gonadal removal with discontinuation of CPA. The authors noted that testosterone levels in the transfeminine people on hormone therapy in the study were similar to or lower than those in cisgender women.
Update 6: Warzywoda et al. (2024) [GoLoCypro Study]
The GoLoCypro study, by Judith Dean and colleagues, was published online in February 2024:
Warzywoda, S., Fowler, J. A., Wood, P., Bisshop, F., Russell, D., Luu, H., Kelly, M., Featherstone, V., & Dean, J. A. (2024). How low can you go? Titrating the lowest effective dose of cyproterone acetate for transgender and gender diverse people who request feminizing hormones. International Journal of Transgender Health, advance online publication. [DOI:10.1080/26895269.2024.2317395]
The following are some noteworthy excerpts from the paper:
Of participants who completed the protocol, 74.0% (34/46) were able to achieve the target T-range (0.5–1.5 nmol/L) and 41.3% (19/46) were titrated to the lowest CPA level (12.5 mg cyproterone twice weekly).
Almost all participants who completed the protocol (91.3.0%, 42/46) recorded their CPA levels as level 3 (12.5 mg daily/25 [mg] alternate days) or lower, with 69.0% (29/42) of these being able to achieve the target T-range. Of those that completed, 41.3% (19/46) were able to achieve the lowest CPA level (12.5 mg cyproterone twice week) with 57.9% (11/19) being able to achieve the target T-range.
The study findings showed that for some patients, CPA doses as low as 12.5 mg on alternate days or less can successfully reduce testosterone to pre-menopausal ranges whilst ensuring testosterone was not over-suppressed.
Our study found that doses of CPA lower than the standard dose (12.5 mg CPA daily and/or 25 mg alternate days) were achievable for suppression of testosterone. Several studies have supported this finding that a lower dosage (10 mg CPA daily) is effective in testosterone reduction in individuals undergoing hormone feminization (Even Zohar et al., 2021; Kuijpers et al., 2021). While not all individuals within our study were able to titrate down CPA dosages, almost a quarter of participants who completed the protocol were achieving target T-ranges on 12.5 mg CPA twice weekly (equivalent to 3.5 mg/daily). To our knowledge ours is the first study to demonstrate that doses lower than 10 mg/daily as well as alternate days or twice weekly CPA are clinically effective in maintaining testosterone reduction within target ranges.
Update 7: More New Low-Dose CPA Studies (2023–2024)
Other new studies of low-dose CPA in transfeminine people have also been published in 2023 and 2024:
Angus, L. M., Leemaqz, S., Zajac, J. D., & Cheung, A. S. (November 2023). A randomised controlled trial of spironolactone versus cyproterone in trans people commencing estradiol. AusPATH 2023 Symposium. [URL] [PDF] [Trans Health Research Blog Post]
Angus, L. M., Leemaqz, S. Y., Zajac, J. D., & Cheung, A. S. (November 2023). The effect of cyproterone and spironolactone on breast development in transgender women: a randomised controlled trial. ESA/SRB/ENSA 2023 ASM 26-29 November, Brisbane, 54–55 (abstract no. 132). [URL] [PDF] [Full Abstract Book] [Trans Health Research Blog Post]
Flamant, T., Vervalcke, J., & T’Sjoen, G. (November 2023). Dose Reduction of Cyproterone Acetate in Trans Women and the Effect on Patient-reported Outcomes: Results from the ENIGI Study. Endocrine Abstracts, 97 [Belgian Endocrine Society 2023], 5–5 (abstract no. 007). [URL] [PDF]
Korpaisarn, S., Arunakul, J., Chaisuksombat, K., & Rattananukrom, T. (2023). A Low Dose Cyproterone Acetate In Feminizing Hormone Treatment. Journal of the Endocrine Society, 7(Suppl 1), A1098–A1099 (abstract no. SAT397/bvad114.2068). [DOI:10.1210/jendso/bvad114.2068]
Yang, W., Hong, T., Chang, X., Han, M., Gao, H., Pan, B., Zhao, Z., & Liu, Y. (2024). The efficacy of and user satisfaction with different antiandrogens in Chinese transgender women. International Journal of Transgender Health, advance online publication. [DOI:10.1080/26895269.2024.2323514]
References
Angus, L., Leemaqz, S., Ooi, O., Cundill, P., Silberstein, N., Locke, P., Zajac, J. D., & Cheung, A. S. (2019). Cyproterone acetate or spironolactone in lowering testosterone concentrations for transgender individuals receiving oestradiol therapy. Endocrine Connections, 8(7), 935–940. [DOI:10.1530/ec-19-0272]
Angus, L. M., Leemaqz, S., Zajac, J. D., & Cheung, A. S. (2023). A randomised controlled trial of spironolactone versus cyproterone in trans people commencing estradiol. AusPATH 2023 Symposium. [URL] [PDF] [Trans Health Research Blog Post]
Angus, L. M., Leemaqz, S. Y., Zajac, J. D., & Cheung, A. S. (2023). The effect of cyproterone and spironolactone on breast development in transgender women: a randomised controlled trial. ESA/SRB/ENSA 2023 ASM 26-29 November, Brisbane, 54–55 (abstract no. 132). [URL] [PDF] [Full Abstract Book] [Trans Health Research Blog Post]
Asscheman, H., & Gooren, L. J. (1992). Hormone Treatment in Transsexuals. In Bocking, W. O., Coleman, E. (Eds). Gender Dysphoria: Interdisciplinary Approaches in Clinical Management (pp. 39–54). Binghamton: Haworth Press. / Journal of Psychology & Human Sexuality, 5(4), 39–54. [Google Scholar] [Google Books] [DOI:10.1300/J056v05n04_03]
Athanasoulia-Kaspar, A. P., & Stalla, G. K. (2019). Endokrinologische Betreuung von Patienten mit Transsexualität. Geburtshilfe und Frauenheilkunde, 79(7), 672–675. [DOI:10.1055/a-0801-3319]
Bastianelli, C., Farris, M., Rosato, E., Brosens, I., & Benagiano, G. (2018). Pharmacodynamics of combined estrogen-progestin oral contraceptives 3. Inhibition of ovulation. Expert Review of Clinical Pharmacology, 11(11), 1085–1098. [DOI:10.1080/17512433.2018.1536544]
Bourns, A. (2019). Guidelines for Gender-Affirming Primary Care with Trans and Non-Binary Patients, 4th Edition. Toronto: Rainbow Health Ontario/Sherbourne Health. [URL] [PDF]
Bruchovsky, N., Larry Goldenberg, S., Akakura, K., & Rennie, P. S. (1993). Luteinizing hormone-releasing hormone agonists in prostate cancer. Elimination of flare reaction by pretreatment with cyproterone acetate and low-dose diethylstilbestrol. Cancer, 72(5), 1685–1691. [DOI:10.1002/1097-0142(19930901)72:5<1685::aid-cncr2820720532>3.0.co;2-3]
Bultynck, C., Pas, C., Defreyne, J., Cosyns, M., den Heijer, M., & T’Sjoen, G. (2017). Self-perception of voice in transgender persons during cross-sex hormone therapy. The Laryngoscope, 127(12), 2796–2804. [DOI:10.1002/lary.26716]
Chen, H., Wiepjes, C. M., van Schoor, N. M., Heijboer, A. C., de Jongh, R. T., den Heijer, M., & Lips, P. (2019). Changes of Vitamin D-Binding Protein, and Total, Bioavailable, and Free 25-Hydroxyvitamin D in Transgender People. The Journal of Clinical Endocrinology & Metabolism, 104(7), 2728–2734. [DOI:10.1210/jc.2018-02602]
Coleman, E., Radix, A. E., Bouman, W. P., Brown, G. R., de Vries, A. L., Deutsch, M. B., Ettner, R., Fraser, L., Goodman, M., Green, J., Hancock, A. B., Johnson, T. W., Karasic, D. H., Knudson, G. A., Leibowitz, S. F., Meyer-Bahlburg, H. F., Monstrey, S. J., Motmans, J., Nahata, L., … & Arcelus, J. (2022). [World Professional Association for Transgender Health (WPATH)] Standards of Care for the Health of Transgender and Gender Diverse People, Version 8. International Journal of Transgender Health, 23(Suppl 1), S1–S259. [DOI:10.1080/26895269.2022.2100644] [URL] [PDF]
Collet, S., Gieles, N., Wiepjes, C. M., Heijboer, A. C., Reyns, T., Fiers, T., Lapauw, B., den Heijer, M., & T’Sjoen, G. (2023). Changes in serum testosterone and adrenal androgen levels in transgender women with and without gonadectomy. The Journal of Clinical Endocrinology & Metabolism, 108(2), 331–338. [DOI:10.1210/clinem/dgac576]
Damgaard-Pedersen, F., & Føgh, M. (1980). The effect of cyproterone acetate on serum lipids in normal men. Acta Endocrinologica, 94(2), 280–283. [DOI:10.1530/acta.0.0940280]
de Blok, C. J., Klaver, M., Wiepjes, C. M., Nota, N. M., Heijboer, A. C., Fisher, A. D., Schreiner, T., T’Sjoen, G., & den Heijer, M. (2017). Breast Development in Transwomen After 1 Year of Cross-Sex Hormone Therapy: Results of a Prospective Multicenter Study. The Journal of Clinical Endocrinology & Metabolism, 103(2), 532–538. [DOI:10.1210/jc.2017-01927]
Defreyne, J., Vantomme, B., Van Caenegem, E., Wierckx, K., De Blok, C., Klaver, M., Nota, N. M., Van Dijk, D., Wiepjes, C. M., Den Heijer, M., & T’Sjoen, G. (2018). Prospective evaluation of hematocrit in gender-affirming hormone treatment: results from European Network for the Investigation of Gender Incongruence. Andrology, 6(3), 446–454. [DOI:10.1111/andr.12485]
Endrikat, J., Gerlinger, C., Richard, S., Rosenbaum, P., & Düsterberg, B. (2011). Ovulation inhibition doses of progestins: a systematic review of the available literature and of marketed preparations worldwide. Contraception, 84(6), 549–557. [DOI:10.1016/j.contraception.2011.04.009]
Even-Zohar, N., Sofer, Y., Yaish, I., Serebro, M., Tordjman, K., & Greenman, Y. (2020). SUN-042 Low Dose Cyproterone Acetate for the Treatment of Transgender Women - a Retrospective Study. Journal of the Endocrine Society, 4(Suppl 1), A715–A715. [DOI:10.1210/jendso/bvaa046.1412]
Even Zohar, N., Sofer, Y., Yaish, I., Serebro, M., Tordjman, K., & Greenman, Y. (2021). Low-Dose Cyproterone Acetate Treatment for Transgender Women. The Journal of Sexual Medicine, 18(7), 1292–1298. [DOI:10.1016/j.jsxm.2021.04.008]
Fink, G. (1979). Feedback Actions of Target Hormones on Hypothalamus and Pituitary With Special Reference to Gonadal Steroids. Annual Review of Physiology, 41(1), 571–585. [DOI:10.1146/annurev.ph.41.030179.003035]
Flamant, T., Vervalcke, J., & T’Sjoen, G. (2023). Dose Reduction of Cyproterone Acetate in Trans Women and the Effect on Patient-reported Outcomes: Results from the ENIGI Study. Endocrine Abstracts, 97 [Belgian Endocrine Society 2023], 5–5 (abstract no. 007). [URL] [PDF]
Føgh, M., Corker, C. S., Hunter, W. M., McLean, H., Philip, J., Schou, G., & Shakkebæk, N. E. (1979). The effects of low doses of cyproterone acetate on some functions of the reproductive system in normal men. Acta Endocrinologica, 91(3), 545–552. [DOI:10.1530/acta.0.0910545]
Føgh, M., Knudsen, J. B., & Gormsen, J. (1980). Effect of cyproterone acetate on platelet aggregability, fibrinolytic activity and fibrinolytic capacity in normal men. Acta Endocrinologica, 94(3), 430–432. [DOI:10.1530/acta.0.0940430]
Foegh, M. (1983). Evaluation of Steroids as COntraceptives in Men. Acta Endocrinologica, 104(3 Suppl b), S9–S48. [DOI:10.1530/acta.0.104s009]
Fredricsson, B., & Carlström, K. (2009). Effects of Low Doses of Cyproterone Acetate on Sperm Morphology and some other Parameters of Reproduction in Normal Men. Andrologia, 13(4), 369–375. [DOI:10.1111/j.1439-0272.1981.tb00067.x]
Fung, R., Hellstern-Layefsky, M., & Lega, I. (2017). Is a lower dose of cyproterone acetate as effective at testosterone suppression in transgender women as higher doses? International Journal of Transgenderism, 18(2), 123–128. [DOI:10.1080/15532739.2017.1290566]
Fuss, J., Hellweg, R., Van Caenegem, E., Briken, P., Stalla, G. K., T’Sjoen, G., & Auer, M. K. (2015). Cross-sex hormone treatment in male-to-female transsexual persons reduces serum brain-derived neurotrophic factor (BDNF). European Neuropsychopharmacology, 25(1), 95–99. [DOI:10.1016/j.euroneuro.2014.11.019]
Fuss, J., Claro, L., Ising, M., Biedermann, S. V., Wiedemann, K., Stalla, G. K., Briken, P., & Auer, M. K. (2019). Does sex hormone treatment reverse the sex-dependent stress regulation? A longitudinal study on hypothalamus-pituitary-adrenal (HPA) axis activity in transgender individuals. Psychoneuroendocrinology, 104, 228–237. [DOI:10.1016/j.psyneuen.2019.02.023]
Gava, G., Cerpolini, S., Martelli, V., Battista, G., Seracchioli, R., & Meriggiola, M. C. (2016). Cyproterone acetatevsleuprolide acetate in combination with transdermal oestradiol in transwomen: a comparison of safety and effectiveness. Clinical Endocrinology, 85(2), 239–246. [DOI:10.1111/cen.13050]
Gava, G., Mancini, I., Alvisi, S., Seracchioli, R., & Meriggiola, M. C. (2020). A comparison of 5-year administration of cyproterone acetate or leuprolide acetate in combination with estradiol in transwomen. European Journal of Endocrinology, 183(6), 561–569. [DOI:10.1530/eje-20-0370]
Geller, J., Albert, J., Yen, S. S., Geller, S., & Loza, D. (1981). Medical Castration of Males with Megestrol Acetate and Small Doses of Diethylstilbestrol*. The Journal of Clinical Endocrinology & Metabolism, 52(3), 576–580. [DOI:10.1210/jcem-52-3-576]
Geller, J., Albert, J., Yen, S. S., Geller, S., & Loza, D. (1981). Medical castration with megestrol acetate and minidose of diethylstilbestrol. Urology, 17(4 Suppl), 27–33. [Google Scholar] [PubMed]
Geller, J., & Albert, J. D. (1983). Comparison of various hormonal therapies for prostatic carcinoma. Seminars in Oncology, 10(4 Suppl 4), 34–41. [Google Scholar] [PubMed] [PDF]
Geller, J. (1988). Megestrol acetate and minidose estrogen in prostatic carcinoma. Urology, 32(3), 281–282. [DOI:10.1016/0090-4295(88)90402-5]
Geller J. (1991). Megestrol Acetate Plus Low-Dose Estrogen in the Management of Advanced Prostatic Carcinoma. The Urologic Clinics of North America, 18(1), 83–91. [DOI:10.1016/S0094-0143(21)01395-1] [Archive.org]
Giltay, E. J., & Gooren, L. J. (2000). Effects of Sex Steroid Deprivation/Administration on Hair Growth and Skin Sebum Production in Transsexual Males and Females. The Journal of Clinical Endocrinology & Metabolism, 85(8), 2913–2921. [DOI:10.1210/jcem.85.8.6710]
Giltay, E. J., Gooren, L. J., Emeis, J. J., Kooistra, T., & Stehouwer, C. D. (2000). Oral, but Not Transdermal, Administration of Estrogens Lowers Tissue-Type Plasminogen Activator Levels in Humans Without Affecting Endothelial Synthesis. Arteriosclerosis, Thrombosis, and Vascular Biology, 20(5), 1396–1403. [DOI:10.1161/01.atv.20.5.1396]
Giltay, E. J., Verhoef, P., Gooren, L. J., Geleijnse, J. M., Schouten, E. G., & Stehouwer, C. D. (2003). Oral and transdermal estrogens both lower plasma total homocysteine in male-to-female transsexuals. Atherosclerosis, 168(1), 139–146. [DOI:10.1016/s0021-9150(03)00090-x]
Giltay, E. J., Gooren, L. J., Toorians, A. W., Katan, M. B., & Zock, P. L. (2004). Docosahexaenoic acid concentrations are higher in women than in men because of estrogenic effects. The American Journal of Clinical Nutrition, 80(5), 1167–1174. [DOI:10.1093/ajcn/80.5.1167]
Glintborg, D., T’Sjoen, G., Ravn, P., & Andersen, M. S. (2021). MANAGEMENT OF ENDOCRINE DISEASE: Optimal feminizing hormone treatment in transgender people. European Journal of Endocrinology, 185(2), R49–R63. [DOI:10.1530/eje-21-0059]
Goldenberg, S. L., Bruchovsky, N., Rennie, P. S., & Coppin, C. M. (1988). The Combination of Cyproterone Acetate and Low Dose Diethylstilbestrol in the Treatment of Advanced Prostatic Carcinoma. Journal of Urology, 140(6), 1460–1465. [DOI:10.1016/s0022-5347(17)42073-8]
Goldenberg, S. L., & Bruchovsky, N. (1991). Use of Cyproterone Acetate in Prostate Cancer. The Urologic Clinics of North America, 18(1), 111–122. [DOI:10.1016/S0094-0143(21)01398-7] [Archive.org]
Goldenberg, S., Bruchovsky, N., Gleave, M., & Sullivan, L. (1996). Low-dose cyproterone acetate plus mini-dose diethylstilbestrol—A protocol for reversible medical castration. Urology, 47(6), 882–884. [DOI:10.1016/s0090-4295(96)00048-9]
Gooren, L. J., Giltay, E. J., & Bunck, M. C. (2008). Long-Term Treatment of Transsexuals with Cross-Sex Hormones: Extensive Personal Experience. The Journal of Clinical Endocrinology & Metabolism, 93(1), 19–25. [DOI:10.1210/jc.2007-1809]
Gräf, K., Brotherton, J., & Neumann, F. (1974). Clinical Uses of Antiandrogens. In Hughes, A., Hasan, S. H., Oertel, G. W., Voss, H. E., Bahner, F., Neumann, F., Steinbeck, H., Gräf, K.-J., Brotherton, J., Horn, H. J., & Wagner, R. K. (Eds.). Androgens II and Antiandrogens / Androgene II und Antiandrogene (Handbuch der experimentellen Pharmakologie/Handbook of Experimental Pharmacology, Volume 35, Part 2) (pp. 485–542). Berlin/Heidelberg: Springer. [DOI:10.1007/978-3-642-80859-3_7]
Hammerstein, J., Meckies, J., Leo-Rossberg, I., Moltz, L., & Zielske, F. (1975). Use of cyproterone acetate (CPA) in the treatment of acne, hirsutism and virilism. Journal of Steroid Biochemistry, 6(6), 827–836. [DOI:10.1016/0022-4731(75)90311-8]
Hammerstein, J. (1979). Cyproterone Acetate. In Jacobs, H. S. (Ed.). Advances in Gynaecological Endocrinology: Proceedings of the Sixth Study Group of the Royal College of Obstetricians and Gynaecologists, 18th and 19th October, 1978 (pp. 367–382). London: The College. [Google Scholar] [Google Books] [PDF]
Hammerstein, J. (1990). Antiandrogens: Clinical Aspects. In Orfanos, C. E., & Happle, R. (Eds.). Hair and Hair Diseases (pp. 827–886). Berlin/Heidelberg: Springer. [DOI:10.1007/978-3-642-74612-3_35]
Heath, R. A., & Wynne, K. (2019). A Guide to Transgender Health: State-of-the-art Information for Gender-Affirming People and Their Supporters (p. 122). Santa Barbara: Praeger/ABC-CLIO. [Google Books]
Hembree, W. C., Cohen-Kettenis, P., Delemarre-Van De Waal, H. A., Gooren, L. J., Meyer III, W. J., Spack, N. P., Tangpricha, V., & Montori, V. M. (2009). Endocrine treatment of transsexual persons: an Endocrine Society clinical practice guideline. The Journal of Clinical Endocrinology & Metabolism, 94(9), 3132–3154. [DOI:10.1210/jc.2009-0345]
Hembree, W. C., Cohen-Kettenis, P. T., Gooren, L., Hannema, S. E., Meyer, W. J., Murad, M. H., Rosenthal, S. M., Safer, J. D., Tangpricha, V., & T’Sjoen, G. G. (2017). Endocrine Treatment of Gender-Dysphoric/Gender-Incongruent Persons: An Endocrine Society* Clinical Practice Guideline [2nd Version]. The Journal of Clinical Endocrinology & Metabolism, 102(11), 3869–3903. [DOI:10.1210/jc.2017-01658] [PDF]
Jacobeit, J. W. (2019). Die hormonelle Behandlung von adulten Trans*Personen (in Deutschland). [Hormonal treatment of adult trans* persons (in Germany).] Journal für Klinische Endokrinologie und Stoffwechsel, 12(3), 102–110. [DOI:10.1007/s41969-019-00080-x]
Jacobi, G. H., Altwein, J. E., Kurth, K. H., Basting, R., & Hohenfellner, R. (1980). Treatment of Advanced Prostatic Cancer with Parenteral Cyproterone Acetate: A Phase III Randomised Trial*. British Journal of Urology, 52(3), 208–215. [DOI:10.1111/j.1464-410x.1980.tb02961.x]
Jacobi, G. H., Tunn, U., & Senge, T. (1982). Clinical experience with cyproterone acetate for palliation of inoperable prostate cancer. In Jacobi, G. H., & Hohenfellner, R. (Eds.). Prostate Cancer (International Perspectives in Urology, Volume 3) (pp. 305–319). Baltimore: Williams & Wilkins. [Google Scholar] [Google Books] [OpenLibrary] [WorldCat] [Archive.org] [PDF]
Jain, J., Kwan, D., & Forcier, M. (2019). Medroxyprogesterone Acetate in Gender-Affirming Therapy for Transwomen: Results From a Retrospective Study. The Journal of Clinical Endocrinology & Metabolism, 104(11), 5148–5156. [DOI:10.1210/jc.2018-02253]
Jequier, A. M., Bullimore, N. J., & Bishop, M. J. (2009). Cyproterone Acetate and a Small Dose of Oestrogen in the Pre-operative Management of Male Transsexuals. A Report of Three Cases. [Cyproteronacetat und kleine Östrogendosis in dem präoperativen Management männlicher Transsexueller. Bericht über drei Fälle.] Andrologia, 21(5), 456–461. [DOI:10.1111/j.1439-0272.1989.tb02447.x]
Johnson, D. E., Babaian, R. J., Swanson, D. A., Von Eschenbach, A. C., Wishnow, K. I., & Tenney, D. (1988). Medical castration using megestrol acetate and minidose estrogen. Urology, 31(5), 371–374. [DOI:10.1016/0090-4295(88)90726-1]
Knuth, U. A., Hano, R., & Nieschlag, E. (1984). Effect of Flutamide or Cyproterone Acetate on Pituitary and Testicular Hormones in Normal Men. The Journal of Clinical Endocrinology & Metabolism, 59(5), 963–969. [DOI:10.1210/jcem-59-5-963]
Koch, U. J., Lorenz, F., Danehl, K., & Hammerstein, J. (1975). Über die Verwendbarkeit von Cyproteronacetat zur Fertilitätshemmung beim Mann. Morphologische Veränderungen und Einflüsse auf die Spermienmotilität. Archiv für Gynäkologie, 219(1–4), 581–582. [DOI:10.1007/bf00669258]
Koch, U., Lorenz, F., Danehl, K., Ericsson, R., Hasan, S., Keyserlingk, D., Lübke, K., Mehring, M., Römmler, A., Schwartz, U., & Hammerstein, J. (1976). Continuous oral low-dosage cyproterone acetate for fertility regulation in the male? A trend analysis in 15 volunteers. Contraception, 14(2), 117–135. [DOI:10.1016/0010-7824(76)90081-0]
Korpaisarn, S., Arunakul, J., Chaisuksombat, K., & Rattananukrom, T. (2023). A Low Dose Cyproterone Acetate In Feminizing Hormone Treatment. Journal of the Endocrine Society, 7(Suppl 1), A1098–A1099 (abstract no. SAT397/bvad114.2068). [DOI:10.1210/jendso/bvad114.2068]
Kranz, G. S., Seiger, R., Kaufmann, U., Hummer, A., Hahn, A., Ganger, S., Tik, M., Windischberger, C., Kasper, S., & Lanzenberger, R. (2017). Effects of sex hormone treatment on white matter microstructure in individuals with gender dysphoria. NeuroImage, 150, 60–67. [DOI:10.1016/j.neuroimage.2017.02.027]
Kranz, G. S., Kaufmann, U., & Lanzenberger, R. (2019). Probing the Impact of Gender-Affirming Hormone Treatment on Odor Perception. Chemical Senses, 45(1), 37–44. [DOI:10.1093/chemse/bjz069]
Kuijpers, S. M., Wiepjes, C. M., Conemans, E. B., Fisher, A. D., T’Sjoen, G., & den Heijer, M. (2021). Toward a Lowest Effective Dose of Cyproterone Acetate in Trans Women: Results From the ENIGI Study. The Journal of Clinical Endocrinology & Metabolism, 106(10), e3936–e3945. [DOI:10.1210/clinem/dgab427]
Kumar, P., Reddy, S., Kulkarni, A., Sharma, M., & Rao, P. N. (2021). Cyproterone acetate induced acute liver failure: case report and review of the literature. Journal of Clinical and Experimental Hepatology, 11(6), 739–741. [DOI:10.1016/j.jceh.2021.01.003]
Lederbogen, S. (2009). Hormonbehandlung. PiD - Psychotherapie im Dialog, 10(1), 41–43. [DOI:10.1055/s-0028-1090190]
Lim, H. Y., Leemaqz, S. Y., Torkamani, N., Grossmann, M., Zajac, J. D., Nandurkar, H., Ho, P., & Cheung, A. S. (2020). Global Coagulation Assays in Transgender Women on Oral and Transdermal Estradiol Therapy. The Journal of Clinical Endocrinology & Metabolism, 105(7), e2369–e2377. [DOI:10.1210/clinem/dgaa262]
Liu, P. Y., Takahashi, P., & Veldhuis, J. D. (2017). An Ensemble Perspective of Aging-Related Hypoandrogenemia in Men. In Winters, S. J., & Huhtaniemi, I. T. (Eds.). Male Hypogonadism: Basic, Clinical and Therapeutic Principles, 2nd Edition (pp. 325–347). Cham: Springer. [DOI:10.1007/978-3-319-53298-1_16]
Mahfouda, S., Moore, J. K., Siafarikas, A., Hewitt, T., Ganti, U., Lin, A., & Zepf, F. D. (2019). Gender-affirming hormones and surgery in transgender children and adolescents. The Lancet Diabetes & Endocrinology, 7(6), 484–498. [DOI:10.1016/s2213-8587(18)30305-x]
Meriggiola, M. C., Bremner, W. J., Costantino, A., Di Cintio, G., & Flamigni, C. (1998). Low dose of cyproterone acetate and testosterone enanthate for contraception in men. Human Reproduction, 13(5), 1225–1229. [DOI:10.1093/humrep/13.5.1225]
Meriggiola, M. C., Bremner, W. J., Costantino, A., Bertaccini, A., Morselli-Labate, A. M., Huebler, D., Kaufmann, G., Oettel, M., & Flamigni, C. (2002). Twenty-One Day Administration of Dienogest Reversibly Suppresses Gonadotropins and Testosterone in Normal Men. The Journal of Clinical Endocrinology & Metabolism, 87(5), 2107–2113. [DOI:10.1210/jcem.87.5.8514]
Meriggiola, M. C., Costantino, A., Bremner, W. J., & Morselli-Labate, A. M. (2002). Higher Testosterone Dose Impairs Sperm Suppression Induced by a Combined Androgen‐Progestin Regimen. Journal of Andrology, 23(5), 684–690. [DOI:10.1002/j.1939-4640.2002.tb02311.x]
Meyer, G., Mayer, M., Mondorf, A., Flügel, A. K., Herrmann, E., & Bojunga, J. (2020). Safety and rapid efficacy of guideline-based gender-affirming hormone therapy: an analysis of 388 individuals diagnosed with gender dysphoria. European Journal of Endocrinology, 182(2), 149–156. [DOI:10.1530/eje-19-0463] [PDF]
Moltz, L., Römmler, A., Schwartz, U., & Hammerstein, J. (1978). Effects of Cyproterone Acetate (CPA) on Pituitary Gonadotrophin Release and on Androgen Secretion Before and After LH-RH Double Stimulation Tests in Men. International Journal of Andrology, 1(Suppl 2b) [5th Annual Workshop on the Testis, Geilo, Norway, April 1978, Endocrine Approach to Male Contraception], 713–719. [DOI:10.1111/j.1365-2605.1978.tb00518.x]
Moltz, L., Römmler, A., Schwartz, U., Post, K., & Hammerstein, J. (1978). Cyproterone acetate (CPA)—a potential male contraceptive: further studies on the interactions with endocrine parameters. Journal of Steroid Biochemistry, 9(9), 865–865 (abstract no. 252). [DOI:10.1016/0022-4731(78)90952-4]
Moltz, L., Römmler, A., Post, K., Schwartz, U., & Hammerstein, J. (1980). Medium dose cyproterone acetate (CPA): Effects on hormone secretion and on spermatogenesis in men. Contraception, 21(4), 393–413. [DOI:10.1016/s0010-7824(80)80017-5]
Moltz, L., Koch, U., Schwartz, U., Rommler, A., & Hammerstein, J. (1982). Male fertility regulation with cyproterone acetate (CPA). Contraceptive Delivery Systems, 3(3/4) [Retroproductive Health Care International Symposium, October 10-15 1982 Maui, Hawaii, USA, Expanded Abstracts], 298–298 (abstract no. 293). [Google Scholar] [PDF]
Moore, E., Wisniewski, A., & Dobs, A. (2003). Endocrine Treatment of Transsexual People: A Review of Treatment Regimens, Outcomes, and Adverse Effects. The Journal of Clinical Endocrinology & Metabolism, 88(8), 3467–3473. [DOI:10.1210/jc.2002-021967]
Nelson, J. B. (2012). Hormone Therapy for Prostate Cancer. In Wein, A. J., Kavoussi, L. R., Novick, A. C., Partin, A. W., & Peters, C. A. (Eds.). Campbell-Walsh Urology, 10th Edition, Volume 2 (pp. 2920–2953). Philadelphia: Elsevier/Saunders. [Google Scholar] [Google Books]
Nota, N. M., den Heijer, M., Gooren, L. J. (2019). Evaluation and Treatment of Gender-Dysphoric/Gender Incongruent Adults. [Updated 2019 Jul 21]. In Feingold, K. R., Anawalt, B., Blackman, M. R., et al. (Eds.). Endotext [Internet]. South Dartmouth, Massachusetts: MDText.com. [PubMed]
Oliphant, J., Veale, J., Macdonald, J., Carroll, R., Johnson, R., Harte, M., Stephenson, C. & Bullock, J. (2018). Guidelines for Gender Affirming Healthcare for Gender Diverse and Transgender Children, Young People and Adults in Aotearoa New Zealand. Waikato: Transgender Health Research Lab/University of Waikato. [URL] [PDF]
Ott, J., Aust, S., Promberger, R., Huber, J. C., & Kaufmann, U. (2011). Cross‐Sex Hormone Therapy Alters the Serum Lipid Profile: A Retrospective Cohort Study in 169 Transsexuals. The Journal of Sexual Medicine, 8(8), 2361–2369. [DOI:10.1111/j.1743-6109.2011.02311.x]
Petry, R., Mauss, J., Senge, T., & Rausch-Stroomann, J. (1970). Über den Einfluß von Cyproteronacetat, Norethisteronönanthat und Gestonoroncapronat auf die Hypophysen-Gonadenachse beim Mann. [Influence of Cyproterone-acetate, Norethisterone-enanthate and Gestonorone-capronate on the Hypophyseal-Gonadal-Axis in the Male.] In Kracht, J. (Ed.). Endokrinologie der Entwicklung und Reifung, 16. Symposion, Ulm, 26.-28. Februar 1970 (Symposion der Deutschen Gesellschaft für Endokrinologie, Volume 16) (pp. 428–430). Berlin: Springer. [Google Books] [DOI:10.1007/978-3-642-80591-2_118] [WorldCat]
Petry, R., Rausch-Stroomann, J.-G., Berthold, K. Mauss, J., Ai, M., Senge, Th., & Vermeulen, A. (1970). Untersuchungen zum Wirkungsmechanismus der Antiandrogene Cyproteron und Cyproteronacetat beim Menschen (Gonadotropin-, Plasma-testosteron- und morphologische Keimdrüsenuntersuchungen). [Investigations on the mechanism of action of the antiandrogens cyproterone and cyproterone acetate in humans (gonadotropin, plasma testosterone, and morphological gonad investigations).] In Schlegel, B. (Ed.). Verhandlungen der Deutschen Gesellschaft für Innere Medizin: Sechsundsiebzigster Kongress Gehalten zu Wiesbaden vom 6. April – 9. April 1970 (Verhandlungen der Deutschen Gesellschaft für Innere Medizin, Volume 76) (pp. 873–876). München: Bergmann. [Google Scholar] [Google Books] [DOI:10.1007/978-3-642-85446-0] [WorldCat]
Petry, R., Rausch-Stroomann, J. G., Mauss, J., Senge, Th., Ai, M., & Berthold, K. (1970). Investigations on the mode of action of the antiandrogens cyproterone and cyproterone acetate in man. / Investigations on the mechanism of action of anti androgenic cyproterone and cyproterone acetate in humans (gonadotropin, plasma testosterone, and morphological generative gland investigations). Medizinische Welt, 29, 1336–. [EurekaMag] [Cited by Koch et al. (1976)]
Petry, R., Mauss, J., Rausch-Stroomann, J. G., & Vermeulen, A. (1972). Reversible inhibition of spermatogenesis in men. Hormone and Metabolic Research, 4(5), 386–388. [DOI:10.1055/s-0028-1094040]
Roy, S., Chatterjee, S., Prasad, M., Poddar, A., Pandey, D., Pandey, H., & Jadhav, Y. (1976). Effects of cyproterone acetate on reproductive functions in normal human males. Contraception, 14(4), 403–423. [DOI:10.1016/s0010-7824(76)80055-8]
Roy, S., & Chatterjee, S. (1979). Studies with cyproterone acetate for male contraception. In James, V. H. T., & Pasqualini, J. R. (Eds.). Hormonal Steroids: Proceedings of the Fifth International Congress on Hormonal Steroids, New Delhi, India, October/November 1978 (pp. 675–680). Oxford: Pergamon Press. [DOI:10.1016/b978-0-08-023796-1.50099-2]
Roy, S., & Chatterjee, S. (1979). The Role of Antiandrogenic Action in Cyproterone Acetate-Induced Morphologic and Biochemical Changes in Human Semen. Fertility and Sterility, 32(1), 93–95. [DOI:10.1016/s0015-0282(16)44122-1]
Saborowski, K.-J. (1987). Konservative Therapie mit Cyproteronacetat und Estradiolundecylat beim Fortgeschrittenen Prostatacarcinom: Eine 5-Jahres-Studie. [Conservative Therapy with Cyproterone Acetate and Estradiol Undecylate in Advanced Prostate Cancer: A 5-Year Study.] (Doctoral dissertation, Ruhr-University Bochum.) [58 pages] [Google Scholar] [Google Books] [WorldCat] [PDF] [Translation]
Scharff, M., Wiepjes, C. M., Klaver, M., Schreiner, T., T’Sjoen, G., & den Heijer, M. (2019). Change in grip strength in trans people and its association with lean body mass and bone density. Endocrine Connections, 8(7), 1020–1028. [DOI:10.1530/ec-19-0196]
Schröder, F. H., & Radlmaier, A. (2002). Steroidal Antiandrogens. In Jordan, C. V., & Furr, B. J. A. (Eds.). Hormone Therapy in Breast and Prostate Cancer (pp. 325–346). Totowa, New Jersey: Humana Press. [DOI:10.1007/978-1-59259-152-7_15]
Slagter, M. H., Gooren, L. J., de Ronde, W., Soosaipillai, A., Scorilas, A., Giltay, E. J., Paliouras, M., & Diamandis, E. P. (2006). Serum and Urine Tissue Kallikrein Concentrations in Male-to-Female Transsexuals Treated with Antiandrogens and Estrogens. Clinical Chemistry, 52(7), 1356–1365. [DOI:10.1373/clinchem.2006.068932]
Sofer, Y., Yaish, I., Yaron, M., Bach, M. Y., Stern, N., & Greenman, Y. (2020). Differential Endocrine and Metabolic Effects of Testosterone Suppressive Agents in Transgender Women. Endocrine Practice, 26(8), 883–890. [DOI:10.4158/ep-2020-0032]
T’Sjoen, G. G., Beguin, Y., Feyen, E., Rubens, R., Kaufman, J., & Gooren, L. (2005). Influence of exogenous oestrogen or (anti-) androgen administration on soluble transferrin receptor in human plasma. Journal of Endocrinology, 186(1), 61–67. [DOI:10.1677/joe.1.06112]
T’Sjoen, G., Weyers, S., Taes, Y., Lapauw, B., Toye, K., Goemaere, S., & Kaufman, J. (2009). Prevalence of Low Bone Mass in Relation to Estrogen Treatment and Body Composition in Male-to-Female Transsexual Persons. Journal of Clinical Densitometry, 12(3), 306–313. [DOI:10.1016/j.jocd.2008.11.002]
T’Sjoen, G., Arcelus, J., De Vries, A. L., Fisher, A. D., Nieder, T. O., Özer, M., & Motmans, J. (2020). European Society for Sexual Medicine Position Statement “Assessment and Hormonal Management in Adolescent and Adult Trans People, with Attention for Sexual Function and Satisfaction”. The Journal of Sexual Medicine, 17(4), 570–584. [DOI:10.1016/j.jsxm.2020.01.012]
Tack, L. J., Heyse, R., Craen, M., Dhondt, K., Bossche, H. V., Laridaen, J., & Cools, M. (2017). Consecutive Cyproterone Acetate and Estradiol Treatment in Late-Pubertal Transgender Female Adolescents. The Journal of Sexual Medicine, 14(5), 747–757. [DOI:10.1016/j.jsxm.2017.03.251]
Toorians, A. W., Thomassen, M. C., Zweegman, S., Magdeleyns, E. J., Tans, G., Gooren, L. J., & Rosing, J. (2003). Venous Thrombosis and Changes of Hemostatic Variables during Cross-Sex Hormone Treatment in Transsexual People. The Journal of Clinical Endocrinology & Metabolism, 88(12), 5723–5729. [DOI:10.1210/jc.2003-030520]
Torre, B. l., Norén, S., Hedman, M., & Diczfalusy, E. (1979). Effect of cyproterone acetate (CPA) on gonadal and adrenal function in men. Contraception, 20(4), 377–396. [DOI:10.1016/s0010-7824(79)80048-7]
Van Caenegem, E., Wierckx, K., Taes, Y., Schreiner, T., Vandewalle, S., Toye, K., Kaufman, J., & T’Sjoen, G. (2014). Preservation of volumetric bone density and geometry in trans women during cross-sex hormonal therapy: a prospective observational study. Osteoporosis International, 26(1), 35–47. [DOI:10.1007/s00198-014-2805-3]
van Dijk, D., Dekker, M. J., Conemans, E. B., Wiepjes, C. M., de Goeij, E. G., Overbeek, K. A., Fisher, A. D., den Heijer, M., & T’Sjoen, G. (2019). Explorative Prospective Evaluation of Short-Term Subjective Effects of Hormonal Treatment in Trans People—Results from the European Network for the Investigation of Gender Incongruence. The Journal of Sexual Medicine, 16(8), 1297–1309. [DOI:10.1016/j.jsxm.2019.05.009]
van Velzen, D. M., Paldino, A., Klaver, M., Nota, N. M., Defreyne, J., Hovingh, G. K., Thijs, A., Simsek, S., T’Sjoen, G., & den Heijer, M. (2019). Cardiometabolic Effects of Testosterone in Transmen and Estrogen Plus Cyproterone Acetate in Transwomen. The Journal of Clinical Endocrinology & Metabolism, 104(6), 1937–1947. [DOI:10.1210/jc.2018-02138]
Venner, P. M., Klotz, P. G., Klotz, L. H., Stewart, D. J., Davis, I. R., Orovan, W. L., & Ramsey, E. W. (1988). Megestrol acetate plus minidose diethylstilbestrol in the treatment of carcinoma of the prostate. Seminars in Oncology, 15(2 Suppl 1), 62–67. [Google Scholar] [PubMed]
Vereecke, G. (2019). Characterisation of testicular function and spermatogenesis in transgender women. (Master’s thesis, Ghent University.) [PDF]
Vereecke, G., Defreyne, J., Van Saen, D., Collet, S., Van Dorpe, J., T’Sjoen, G., & Goossens, E. (2020). Characterisation of testicular function and spermatogenesis in transgender women. Human Reproduction, 36(1), 5–15. [DOI:10.1093/humrep/deaa254]
Vita, R., Settineri, S., Liotta, M., Benvenga, S., & Trimarchi, F. (2018). Changes in hormonal and metabolic parameters in transgender subjects on cross-sex hormone therapy: A cohort study. Maturitas, 107, 92–96. [DOI:10.1016/j.maturitas.2017.10.012]
Vlot, M. C., Wiepjes, C. M., Jongh, R. T., T’Sjoen, G., Heijboer, A. C., & den Heijer, M. (2019). Gender‐Affirming Hormone Treatment Decreases Bone Turnover in Transwomen and Older Transmen. Journal of Bone and Mineral Research, 34(10), 1862–1872. [DOI:10.1002/jbmr.3762]
Wang, C., & Yeung, K. (1980). Use of low-dosage oral cyproterone acetate as a male contraceptive. Contraception, 21(3), 245–272. [DOI:10.1016/0010-7824(80)90005-0]
Warzywoda, S., Fowler, J. A., Wood, P., Bisshop, F., Russell, D., Luu, H., Kelly, M., Featherstone, V., & Dean, J. A. (2024). How low can you go? Titrating the lowest effective dose of cyproterone acetate for transgender and gender diverse people who request feminizing hormones. International Journal of Transgender Health, advance online publication. [DOI:10.1080/26895269.2024.2317395]
Wiepjes, C. M., Vlot, M. C., Klaver, M., Nota, N. M., de Blok, C. J., de Jongh, R. T., Lips, P., Heijboer, A. C., Fisher, A. D., Schreiner, T., T’Sjoen, G., & den Heijer, M. (2017). Bone Mineral Density Increases in Trans Persons After 1 Year of Hormonal Treatment: A Multicenter Prospective Observational Study. Journal of Bone and Mineral Research, 32(6), 1252–1260. [DOI:10.1002/jbmr.3102]
Wiepjes, C. M., Vlot, M. C., de Blok, C. J., Nota, N. M., de Jongh, R. T., & den Heijer, M. (2019). Bone geometry and trabecular bone score in transgender people before and after short- and long-term hormonal treatment. Bone, 127, 280–286. [DOI:10.1016/j.bone.2019.06.029]
Wierckx, K., Mueller, S., Weyers, S., Van Caenegem, E., Roef, G., Heylens, G., & T’Sjoen, G. (2012). Long‐Term Evaluation of Cross‐Sex Hormone Treatment in Transsexual Persons. The Journal of Sexual Medicine, 9(10), 2641–2651. [DOI:10.1111/j.1743-6109.2012.02876.x]
Wierckx, K., Van Caenegem, E., Schreiner, T., Haraldsen, I., Fisher, A., Toye, K., Kaufman, J. M., & T’Sjoen, G. (2014). Cross‐Sex Hormone Therapy in Trans Persons Is Safe and Effective at Short‐Time Follow‐Up: Results from the European Network for the Investigation of Gender Incongruence. The Journal of Sexual Medicine, 11(8), 1999–2011. [DOI:10.1111/jsm.12571]
Winkler-Crepaz, K., Müller, A., Böttcher, B., & Wildt, L. (2017). Hormonbehandlung bei Transgenderpatienten. [Hormone treatment of transgender patients.] Gynäkologische Endokrinologie, 15(1), 39–42. [DOI:10.1007/s10304-016-0116-9]
Winters, S. J., Wang, C., & (2009). LH and Non-SHBG Testosterone and Estradiol Levels During Testosterone Replacement of Hypogonadal Men: Further Evidence That Steroid Negative Feedback Increases as Men Grow Older. Journal of Andrology, 31(3), 281–287. [DOI:10.2164/jandrol.109.009035]
Yang, W., Hong, T., Chang, X., Han, M., Gao, H., Pan, B., Zhao, Z., & Liu, Y. (2024). The efficacy of and user satisfaction with different antiandrogens in Chinese transgender women. International Journal of Transgender Health, advance online publication. [DOI:10.1080/26895269.2024.2323514]
Zitzmann, M., Rohayem, J., Raidt, J., Kliesch, S., Kumar, N., Sitruk-Ware, R., & Nieschlag, E. (2017). Impact of various progestins with or without transdermal testosterone on gonadotropin levels for non-invasive hormonal male contraception: a randomized clinical trial. Andrology, 5(3), 516–526. [DOI:10.1111/andr.12328]
Zubiaurre-Elorza, L., Junque, C., Gómez-Gil, E., & Guillamon, A. (2014). Effects of Cross-Sex Hormone Treatment on Cortical Thickness in Transsexual Individuals. The Journal of Sexual Medicine, 11(5), 1248–1261. [DOI:10.1111/jsm.12491]
\ No newline at end of file
diff --git a/transfemscience.org/articles/e2-equivalent-doses/index.html b/transfemscience.org/articles/e2-equivalent-doses/index.html
index c9f5da7f..1c46aa1d 100644
--- a/transfemscience.org/articles/e2-equivalent-doses/index.html
+++ b/transfemscience.org/articles/e2-equivalent-doses/index.html
@@ -1 +1 @@
-Approximate Comparable Dosages of Estradiol by Different Routes - Transfeminine Science
Approximate Comparable Dosages of Estradiol by Different Routes
By Aly | First published April 19, 2020 | Last modified April 13, 2023
Preface
Transfeminine people often ask about equivalent dosages of estradiol by different routes of administration. This page was put together to help facilitate answering these questions.
Table of Comparable Estradiol Dosages
The following is a table of estimated equivalent dosages of estradiol by different routes:
a For oral estradiol. Oral estradiol 1.5 mg is equivalent to about 2 mg oral estradiol valerate (Wiki). b Based on sublingual estradiol having ~2- to 5-fold greater bioavailability than oral estradiol per studies (Wiki; Sam, 2021). c Much lower doses of transdermal estradiol can be used in the case of genital application relative to conventional skin sites (potentially e.g. 5-fold lower doses for similar estradiol levels) (Aly., 2019). d Different patch brands may result in differing estradiol levels (Rohr, Nauert, & Stehle, 1999; Langley et al., 2008; Farahmand & Maibach, 2009; Langley et al., 2015). e For i.m. or s.c. injection, total dose per week of an estradiol ester like estradiol valerate, estradiol cypionate, estradiol enanthate, or estradiol benzoate. Differences in molecular weight between these esters are minor (Table) and can be ignored for simplicity. Optimal injection intervals vary depending on the ester and doses should be scaled by injection interval to match the listed total dose per week (Aly, 2021).
Notes
These doses are not absolute and should be considered only a rough guideline. They represent a generalized model based on many different studies with often very different individual findings. There is also an assumption that estradiol levels scale linearly or proportionally with dose, which may or may not actually be the case. One study found lower bioavailability of oral estradiol at high doses for instance (Kuhnz, Gansau, & Mahler, 1993).
These doses are approximate equivalent or comparable doses and don’t necessarily correspond to typical or recommended clinical doses. Injectable estradiol formulations are generally used at higher doses than other routes and forms of estradiol for instance (Aly, 2021).
The comparable doses are based on total estradiol exposure rather than therapeutic estrogenic potency. Time-related variations in sex hormone levels have been reported to modify potency of sex hormone preparations (Aly, 2021). However, this has not been factored in to the table here due to a lack of available data and analysis on the influence. In any case, it may be relevant to routes with large fluctuations in estradiol levels like sublingual administration and shorter-acting injections.
A transdermal estradiol spray sold under the brand name Lenzetto is available. In a study in postmenopausal women, mean baseline-adjusted estradiol levels with Lenzetto over the course of a week following achievement of steady state were about 6 pg/mL pre-treatment, 13 pg/mL with 1 spray/day (1.53 mg/day), 19 pg/mL with 2 sprays/day (3.06 mg/day), and 26 pg/mL with 3 sprays/day (4.59 mg/day) (Morton et al., 2009; Graph). Hence, this form of estradiol appears to achieve relatively low estradiol levels that likely aren’t well-suited for transfeminine people. No data are available on higher doses (i.e., more sprays per day) and so this formulation has not been included in the table.
Discussion
For reference, mean integrated levels of estradiol during the normal menstrual cycle in premenopausal cisgender women are about 100 pg/mL and during the luteal phase (the latter half of the menstrual cycle) are around 150 pg/mL (Graph; Graph; Aly, 2018). The total production of estradiol over a single menstrual cycle (i.e., one month) is about 6 mg on average (Rosenfield et al., 2008; Aly, 2018). Slightly higher doses are required for injectable estradiol esters relative to endogenous production amounts since they contain less estradiol by weight due to the ester components (Table).
Note that there is high interindividual variability (i.e., variability between individuals) in terms of estradiol levels achieved with different forms and routes of estradiol. As an example, some people may get relatively low estradiol levels with the oral route and others may get relatively low levels with the transdermal route. Conversely, some people may get relatively high levels with the transdermal route or with injections. For data showing the substantial variability even with injections, see Aly (2021). Due to the variability in estradiol levels between individuals, the appropriate doses will often not be the same for different people. Doses should be adjusted as necessary based on blood work. It should also be noted that there are large time-dependent changes in estradiol levels with certain routes, namely sublingual or buccal administration (Graphs; Graph; Sam, 2021) and intramuscular or subcutaneous injection (Graphs; Aly, 2021). Due to these fluctuations, estradiol levels will be vastly different when measured at different time points with these routes (e.g., around peak versus around trough).
For transfeminine people who have not yet undergone or do not plan to undergo gonadectomy, a high to very high dose of estradiol can be used to achieve strong suppression of testosterone levels. On average, the high dose will suppress testosterone levels by about 90%, to around 50 ng/dL (Wiki; Aly, 2018). Hence, the high to very high doses are indicated for estradiol monotherapy (i.e., estradiol alone without an antiandrogen). After gonadectomy, testosterone suppression is no longer needed and lower doses of estradiol, such as the moderate doses, can be used instead. High doses of estradiol are not necessarily required if estradiol is used in combination with an adequately effective antiandrogen, for instance cyproterone acetate, bicalutamide, or a gonadotropin-releasing hormone agonist or antagonist. Spironolactone, on the other hand, may often not be fully effective for opposing androgens (Aly, 2018).
References
General Sources
Aly. (2019). Analysis of Estradiol and Testosterone Levels with Oral Estradiol in Transfeminine People Based on Leinung et al. (2018). Transfeminine Science, oral-e2-leinung-2018. [Google Scholar] [URL]
Aly. (2021). An Informal Meta-Analysis of Estradiol Curves with Injectable Estradiol Preparations. Transfeminine Science, injectable-e2-meta-analysis. [Google Scholar] [URL]
Armston, A., & Wood, P. (2002). Hormone replacement therapy (oestradiol-only preparations): can the laboratory recommend a concentration of plasma oestradiol to protect against osteoporosis? Annals of Clinical Biochemistry, 39(3), 184–193. [DOI:10.1258/0004563021902107]
Baker, V. L. (1994). Alternatives to Oral Estrogen Replacement: Transdermal Patches, Percutaneous Gels, Vaginal Creams and Rings, Implants, and Other Methods of Delivery. Obstetrics and Gynecology Clinics of North America, 21(2) [Primary Care of the Mature Woman], 271–297. [DOI:10.1016/S0889-8545(21)00629-X] [PDF]
Bruni, V., & Pampaloni, F. (2019). Hormone Replacement Therapy in Premature Ovarian Insufficiency. In Berga, S. L., Genazzani, A. R., Naftolin, F., & Petraglia, F. (Eds.). Menstrual Cycle Related Disorders (pp. 111–142). Cham: Springer. [DOI:10.1007/978-3-030-14358-9_10]
Farahmand, S., & Maibach, H. I. (2009). Transdermal drug pharmacokinetics in man: Interindividual variability and partial prediction. International Journal of Pharmaceutics, 367(1–2), 1–15. [DOI:10.1016/j.ijpharm.2008.11.020]
Herndon, J. S., Maheshwari, A. K., Nippoldt, T. B., Carlson, S. J., Davidge-Pitts, C. J., & Chang, A. Y. (2023). Comparison of Subcutaneous and Intramuscular Estradiol Regimens as part of Gender-Affirming Hormone Therapy. Endocrine Practice, 29(5), 356–361. [DOI:10.1016/j.eprac.2023.02.006] [URL] [PDF]
Kuhl, H. (2005). Pharmacology of estrogens and progestogens: influence of different routes of administration. Climacteric, 8(Suppl 1), 3–63. [DOI:10.1080/13697130500148875] [PDF]
Leinung, M. C., Feustel, P. J., & Joseph, J. (2018). Hormonal Treatment of Transgender Women with Oral Estradiol. Transgender Health, 3(1), 74–81. [DOI:10.1089/trgh.2017.0035]
Lobo, R. A., & Cassidenti, D. L. (1992). Pharmacokinetics of Oral 17 β-Estradiol. The Journal of Reproductive Medicine, 37(1), 77–84. [Google Scholar] [PubMed] [PDF]
Sam. (2021). An Exploration of Sublingual Estradiol as an Alternative to Oral Estradiol in Transfeminine People. Transfeminine Science, sublingual-e2-transfem. [Google Scholar] [URL]
Simon, J. A., & Snabes, M. C. (2007). Menopausal hormone therapy for vasomotor symptoms: balancing the risks and benefits with ultra-low doses of estrogen. Expert Opinion on Investigational Drugs, 16(12), 2005–2020. [DOI:10.1517/13543784.16.12.2005]
Taboada, M., Santen, R., Lima, J., Hossain, J., Singh, R., Klein, K. O., & Mauras, N. (2011). Pharmacokinetics and pharmacodynamics of oral and transdermal 17β estradiol in girls with Turner syndrome. The Journal of Clinical Endocrinology & Metabolism, 96(11), 3502–3510. [DOI:10.1210/jc.2011-1449]
Wikipedia. (2020, August 29). Pharmacokinetics of estradiol. Wikimedia Foundation. [URL]
Wikipedia. (2020, October 2). Template:Estrogen dosages for menopausal hormone therapy. Wikimedia Foundation. [URL]
Inline Citations
Farahmand, S., & Maibach, H. I. (2009). Transdermal drug pharmacokinetics in man: Interindividual variability and partial prediction. International Journal of Pharmaceutics, 367(1–2), 1–15. [DOI:10.1016/j.ijpharm.2008.11.020]
Kuhnz, W., Gansau, C., & Mahler, M. (1993). Pharmacokinetics of estradiol, free and total estrone, in young women following single intravenous and oral administration of 17β-estradiol. Arzneimittelforschung, 43(9), 966–973. [Google Scholar] [PubMed] [PDF]
Langley, R. E., Godsland, I. F., Kynaston, H., Clarke, N. W., Rosen, S. D., Morgan, R. C., Pollock, P., Kockelbergh, R., Lalani, E., Dearnaley, D., Parmar, M., & Abel, P. D. (2008). Early hormonal data from a multicentre phase II trial using transdermal oestrogen patches as first-line hormonal therapy in patients with locally advanced or metastatic prostate cancer. BJU International, 102(4), 442–445. [DOI:10.1111/j.1464-410x.2008.07583.x]
Langley, R. E., Duong, T., Godsland, I. F., Kynaston, H., Kockelbergh, R., Rosen, S. D., Alhasso, A. A., Dearnaley, D. P., Clarke, N. W., Jovic, G., Carpenter, R., Bara, A., Welland, A., Parmar, M. K., & Abel, P. D. (2015). Oestrogen patches (OP) to treat prostate cancer (PC) – Are different commercial brands interchangeable? Maturitas, 81(1), 210–211. [DOI:10.1016/j.maturitas.2015.02.320]
Morton, T. L., Gattermeir, D. J., Petersen, C. A., Day, W. W., & Schumacher, R. J. (2009). Steady-State Pharmacokinetics Following Application of a Novel Transdermal Estradiol Spray in Healthy Postmenopausal Women. The Journal of Clinical Pharmacology, 49(9), 1037–1046. [DOI:10.1177/0091270009339187]
Rohr, U. D., Nauert, C., & Stehle, B. (1999). 17β-Estradiol delivered by three different matrix patches 50 μg/day. Maturitas, 33(1), 45–58. [DOI:10.1016/s0378-5122(99)00039-0]
Rosenfield, R. L., Cooke, D. W., & Radovick, S. (2008). Puberty and Its Disorders in the Female. In Sperling, M. A. (Ed.). Pediatric Endocrinology, 3rd Edition (pp. 530–609). Philadelphia: Saunders/Elsevier. [Google Scholar] [Google Books] [DOI:10.1016/b978-141604090-3.50019-3] [Archive.org]
\ No newline at end of file
+Approximate Comparable Dosages of Estradiol by Different Routes - Transfeminine Science
Approximate Comparable Dosages of Estradiol by Different Routes
By Aly | First published April 19, 2020 | Last modified April 13, 2023
Preface
Transfeminine people often ask about equivalent dosages of estradiol by different routes of administration. This page was put together to help facilitate answering these questions.
Table of Comparable Estradiol Dosages
The following is a table of estimated equivalent dosages of estradiol by different routes:
a For oral estradiol. Oral estradiol 1.5 mg is equivalent to about 2 mg oral estradiol valerate (Wiki). b Based on sublingual estradiol having ~2- to 5-fold greater bioavailability than oral estradiol per studies (Wiki; Sam, 2021). c Much lower doses of transdermal estradiol can be used in the case of genital application relative to conventional skin sites (potentially e.g. 5-fold lower doses for similar estradiol levels) (Aly., 2019). d Different patch brands may result in differing estradiol levels (Rohr, Nauert, & Stehle, 1999; Langley et al., 2008; Farahmand & Maibach, 2009; Langley et al., 2015). e For i.m. or s.c. injection, total dose per week of an estradiol ester like estradiol valerate, estradiol cypionate, estradiol enanthate, or estradiol benzoate. Differences in molecular weight between these esters are minor (Table) and can be ignored for simplicity. Optimal injection intervals vary depending on the ester and doses should be scaled by injection interval to match the listed total dose per week (Aly, 2021).
Notes
These doses are not absolute and should be considered only a rough guideline. They represent a generalized model based on many different studies with often very different individual findings. There is also an assumption that estradiol levels scale linearly or proportionally with dose, which may or may not actually be the case. One study found lower bioavailability of oral estradiol at high doses for instance (Kuhnz, Gansau, & Mahler, 1993).
These doses are approximate equivalent or comparable doses and don’t necessarily correspond to typical or recommended clinical doses. Injectable estradiol formulations are generally used at higher doses than other routes and forms of estradiol for instance (Aly, 2021).
The comparable doses are based on total estradiol exposure rather than therapeutic estrogenic potency. Time-related variations in sex hormone levels have been reported to modify potency of sex hormone preparations (Aly, 2021). However, this has not been factored in to the table here due to a lack of available data and analysis on the influence. In any case, it may be relevant to routes with large fluctuations in estradiol levels like sublingual administration and shorter-acting injections.
A transdermal estradiol spray sold under the brand name Lenzetto is available. In a study in postmenopausal women, mean baseline-adjusted estradiol levels with Lenzetto over the course of a week following achievement of steady state were about 6 pg/mL pre-treatment, 13 pg/mL with 1 spray/day (1.53 mg/day), 19 pg/mL with 2 sprays/day (3.06 mg/day), and 26 pg/mL with 3 sprays/day (4.59 mg/day) (Morton et al., 2009; Graph). Hence, this form of estradiol appears to achieve relatively low estradiol levels that likely aren’t well-suited for transfeminine people. No data are available on higher doses (i.e., more sprays per day) and so this formulation has not been included in the table.
Discussion
For reference, mean integrated levels of estradiol during the normal menstrual cycle in premenopausal cisgender women are about 100 pg/mL and during the luteal phase (the latter half of the menstrual cycle) are around 150 pg/mL (Graph; Graph; Aly, 2018). The total production of estradiol over a single menstrual cycle (i.e., one month) is about 6 mg on average (Rosenfield et al., 2008; Aly, 2018). Slightly higher doses are required for injectable estradiol esters relative to endogenous production amounts since they contain less estradiol by weight due to the ester components (Table).
Note that there is high interindividual variability (i.e., variability between individuals) in terms of estradiol levels achieved with different forms and routes of estradiol. As an example, some people may get relatively low estradiol levels with the oral route and others may get relatively low levels with the transdermal route. Conversely, some people may get relatively high levels with the transdermal route or with injections. For data showing the substantial variability even with injections, see Aly (2021). Due to the variability in estradiol levels between individuals, the appropriate doses will often not be the same for different people. Doses should be adjusted as necessary based on blood work. It should also be noted that there are large time-dependent changes in estradiol levels with certain routes, namely sublingual or buccal administration (Graphs; Graph; Sam, 2021) and intramuscular or subcutaneous injection (Graphs; Aly, 2021). Due to these fluctuations, estradiol levels will be vastly different when measured at different time points with these routes (e.g., around peak versus around trough).
For transfeminine people who have not yet undergone or do not plan to undergo gonadectomy, a high to very high dose of estradiol can be used to achieve strong suppression of testosterone levels. On average, the high dose will suppress testosterone levels by about 90%, to around 50 ng/dL (Wiki; Aly, 2018). Hence, the high to very high doses are indicated for estradiol monotherapy (i.e., estradiol alone without an antiandrogen). After gonadectomy, testosterone suppression is no longer needed and lower doses of estradiol, such as the moderate doses, can be used instead. High doses of estradiol are not necessarily required if estradiol is used in combination with an adequately effective antiandrogen, for instance cyproterone acetate, bicalutamide, or a gonadotropin-releasing hormone agonist or antagonist. Spironolactone, on the other hand, may often not be fully effective for opposing androgens (Aly, 2018).
References
General Sources
Aly. (2019). Analysis of Estradiol and Testosterone Levels with Oral Estradiol in Transfeminine People Based on Leinung et al. (2018). Transfeminine Science, oral-e2-leinung-2018. [Google Scholar] [URL]
Aly. (2021). An Informal Meta-Analysis of Estradiol Curves with Injectable Estradiol Preparations. Transfeminine Science, injectable-e2-meta-analysis. [Google Scholar] [URL]
Armston, A., & Wood, P. (2002). Hormone replacement therapy (oestradiol-only preparations): can the laboratory recommend a concentration of plasma oestradiol to protect against osteoporosis? Annals of Clinical Biochemistry, 39(3), 184–193. [DOI:10.1258/0004563021902107]
Baker, V. L. (1994). Alternatives to Oral Estrogen Replacement: Transdermal Patches, Percutaneous Gels, Vaginal Creams and Rings, Implants, and Other Methods of Delivery. Obstetrics and Gynecology Clinics of North America, 21(2) [Primary Care of the Mature Woman], 271–297. [DOI:10.1016/S0889-8545(21)00629-X]
Bruni, V., & Pampaloni, F. (2019). Hormone Replacement Therapy in Premature Ovarian Insufficiency. In Berga, S. L., Genazzani, A. R., Naftolin, F., & Petraglia, F. (Eds.). Menstrual Cycle Related Disorders (pp. 111–142). Cham: Springer. [DOI:10.1007/978-3-030-14358-9_10]
Farahmand, S., & Maibach, H. I. (2009). Transdermal drug pharmacokinetics in man: Interindividual variability and partial prediction. International Journal of Pharmaceutics, 367(1–2), 1–15. [DOI:10.1016/j.ijpharm.2008.11.020]
Herndon, J. S., Maheshwari, A. K., Nippoldt, T. B., Carlson, S. J., Davidge-Pitts, C. J., & Chang, A. Y. (2023). Comparison of Subcutaneous and Intramuscular Estradiol Regimens as part of Gender-Affirming Hormone Therapy. Endocrine Practice, 29(5), 356–361. [DOI:10.1016/j.eprac.2023.02.006]
Kuhl, H. (2005). Pharmacology of estrogens and progestogens: influence of different routes of administration. Climacteric, 8(Suppl 1), 3–63. [DOI:10.1080/13697130500148875] [PDF]
Leinung, M. C., Feustel, P. J., & Joseph, J. (2018). Hormonal Treatment of Transgender Women with Oral Estradiol. Transgender Health, 3(1), 74–81. [DOI:10.1089/trgh.2017.0035]
Lobo, R. A., & Cassidenti, D. L. (1992). Pharmacokinetics of Oral 17 β-Estradiol. The Journal of Reproductive Medicine, 37(1), 77–84. [Google Scholar] [PubMed] [PDF]
Sam. (2021). An Exploration of Sublingual Estradiol as an Alternative to Oral Estradiol in Transfeminine People. Transfeminine Science, sublingual-e2-transfem. [Google Scholar] [URL]
Simon, J. A., & Snabes, M. C. (2007). Menopausal hormone therapy for vasomotor symptoms: balancing the risks and benefits with ultra-low doses of estrogen. Expert Opinion on Investigational Drugs, 16(12), 2005–2020. [DOI:10.1517/13543784.16.12.2005]
Taboada, M., Santen, R., Lima, J., Hossain, J., Singh, R., Klein, K. O., & Mauras, N. (2011). Pharmacokinetics and pharmacodynamics of oral and transdermal 17β estradiol in girls with Turner syndrome. The Journal of Clinical Endocrinology & Metabolism, 96(11), 3502–3510. [DOI:10.1210/jc.2011-1449]
Wikipedia. (2020, August 29). Pharmacokinetics of estradiol. Wikimedia Foundation. [URL]
Wikipedia. (2020, October 2). Template:Estrogen dosages for menopausal hormone therapy. Wikimedia Foundation. [URL]
Inline Citations
Farahmand, S., & Maibach, H. I. (2009). Transdermal drug pharmacokinetics in man: Interindividual variability and partial prediction. International Journal of Pharmaceutics, 367(1–2), 1–15. [DOI:10.1016/j.ijpharm.2008.11.020]
Kuhnz, W., Gansau, C., & Mahler, M. (1993). Pharmacokinetics of estradiol, free and total estrone, in young women following single intravenous and oral administration of 17β-estradiol. Arzneimittelforschung, 43(9), 966–973. [Google Scholar] [PubMed] [PDF]
Langley, R. E., Godsland, I. F., Kynaston, H., Clarke, N. W., Rosen, S. D., Morgan, R. C., Pollock, P., Kockelbergh, R., Lalani, E., Dearnaley, D., Parmar, M., & Abel, P. D. (2008). Early hormonal data from a multicentre phase II trial using transdermal oestrogen patches as first-line hormonal therapy in patients with locally advanced or metastatic prostate cancer. BJU International, 102(4), 442–445. [DOI:10.1111/j.1464-410x.2008.07583.x]
Langley, R. E., Duong, T., Godsland, I. F., Kynaston, H., Kockelbergh, R., Rosen, S. D., Alhasso, A. A., Dearnaley, D. P., Clarke, N. W., Jovic, G., Carpenter, R., Bara, A., Welland, A., Parmar, M. K., & Abel, P. D. (2015). Oestrogen patches (OP) to treat prostate cancer (PC) – Are different commercial brands interchangeable? Maturitas, 81(1), 210–211. [DOI:10.1016/j.maturitas.2015.02.320]
Morton, T. L., Gattermeir, D. J., Petersen, C. A., Day, W. W., & Schumacher, R. J. (2009). Steady-State Pharmacokinetics Following Application of a Novel Transdermal Estradiol Spray in Healthy Postmenopausal Women. The Journal of Clinical Pharmacology, 49(9), 1037–1046. [DOI:10.1177/0091270009339187]
Rohr, U. D., Nauert, C., & Stehle, B. (1999). 17β-Estradiol delivered by three different matrix patches 50 μg/day. Maturitas, 33(1), 45–58. [DOI:10.1016/s0378-5122(99)00039-0]
Rosenfield, R. L., Cooke, D. W., & Radovick, S. (2008). Puberty and Its Disorders in the Female. In Sperling, M. A. (Ed.). Pediatric Endocrinology, 3rd Edition (pp. 530–609). Philadelphia: Saunders/Elsevier. [Google Scholar] [Google Books] [DOI:10.1016/b978-141604090-3.50019-3] [Archive.org]
\ No newline at end of file
diff --git a/transfemscience.org/articles/estrogens-blood-clots/index.html b/transfemscience.org/articles/estrogens-blood-clots/index.html
index 479d3f4c..fe457c68 100644
--- a/transfemscience.org/articles/estrogens-blood-clots/index.html
+++ b/transfemscience.org/articles/estrogens-blood-clots/index.html
@@ -1 +1 @@
-Estrogens and Their Influences on Coagulation and Risk of Blood Clots - Transfeminine Science
Estrogens and Their Influences on Coagulation and Risk of Blood Clots
By Aly | First published October 20, 2020 | Last modified March 28, 2023
Abstract / TL;DR
Estrogens increase coagulation by activating estrogen receptors in the liver and thereby modulating the production of a variety of circulating coagulation factors. With sufficiently high exposure, this can result in an increase in the risk of blood clots as well as coagulation-associated cardiovascular complications like heart attack and stroke. However, the degrees of risk vary depending on the estrogen type, route, and dose. Non-bioidentical estrogens like ethinylestradiol have greater strength in the liver due to their relative resistance to metabolism and increase blood clot risk more readily than bioidentical estradiol, while oral administration of estradiol results in a first pass through the liver and has greater impact on blood clot risk than non-oral estradiol. Physiological estradiol levels with non-oral estradiol appear to have minimal to no risk of blood clots, whereas oral estradiol has significant risk and at high doses may have risk similar to that of the doses of ethinylestradiol in modern birth control pills. Higher estradiol levels with non-oral estradiol seem to have significant risk of blood clots and cardiovascular problems as well, although the risks appear to be lower than with ethinylestradiol-containing birth control pills. Absolute risks of blood clots are low but accumulate with time and add up on a population scale. In addition, a variety of risk factors, such as age, physical inactivity, concomitant progestogen use, and often-unknown thrombophilic abnormalities, can substantially augment risk. Due to their higher risks of blood clots, oral estradiol as well as excessive doses of non-oral estradiol should ideally be avoided in transfeminine people. This is particularly applicable in those with risk factors for blood clots. In any case, therapeutic considerations for transfeminine people include not only safety but also effectiveness, other factors like cost and convenience, and the natures of the alternative therapeutic options.
Introduction
Estrogens increase coagulation (blood clotting) and the risk of thrombosis, a cardiovascular event otherwise known as a blood clot. There are two major types of blood clots, which are categorized depending on whether they happen in a vein or in an artery: (1) venous thrombosis or venous thromboembolism (VTE); and (2) arterial thrombosis. VTE is a blood clot in a vein, a blood vessel that carries blood towards the heart. It comprises two different subtypes: (1) deep vein thrombosis (DVT), a clot in a vein of the leg or pelvic region; and (2) pulmonary embolism (PE), a clot that has broken free and blocked an artery in the lungs. Arterial thrombosis is a blood clot in an artery, a blood vessel that carries blood away from the heart. Arterial thrombosis can lead to myocardial infarction (MI; also known as heart attack) or cerebrovascular accident (CVA; also known as stroke). Blood clots are major health problems that can cause serious complications and even death. Estrogens, via increased coagulation with sufficiently high exposure, have the potential to heighten the risk of both venous and arterial thrombosis and hence to increase all of the aforementioned risks. The risk of blood clots with estrogens serves as a limiting factor in their use due to the potential health consequences.
Estrogens are selectiveagonists of the estrogen receptors (ERs). They are thought to increase coagulation and hence blood clot risk by activating ERs. However, the impact on coagulation and risk of blood clots with estrogens varies due to factors like estrogen type, route, and dose. In addition, other factors, like concomitant progestogen use and a variety of non-hormonal factors, are known to modify the risk. The purpose of this article is to review the risks of blood clots with estrogens, the mechanisms underlying increased coagulation and blood clot risk with estrogens, and the reasons for differences among estrogens in terms of risk. Exploring these topics can inform estrogen dosing considerations in transfeminine people and help to minimize risks and optimize safety. Moreover, higher levels of estrogens are therapeutically useful for suppressing testosterone production in transfeminine people but may increase blood clot risk, and risk–benefit analysis is warranted in this context.
Blood Clot Risks with Estrogens and Progestogens
A variety of estrogens have been used in medicine. These include bioidentical estrogens like estradiol as well as non-bioidentical estrogens like conjugated estrogens (CEEs; Premarin), ethinylestradiol (EE), and diethylstilbestrol (DES). Estradiol is the major natural estrogen in the human body. CEEs deliver primarily estradiol as the active estrogen, but also contain significant quantities of naturally occurring equine (horse) estrogens such as equilin (7-dehydroestrone) and 17β-dihydroequilin (7-dehydroestradiol). EE and DES are synthetic estrogens that were created by humans and do not occur naturally. DES was discontinued decades ago and is relatively little-known today, but has significant historical importance. Estradiol is used in both oral and non-oral forms (e.g., transdermal patches), while the non-bioidentical estrogens have typically been used orally. For context, the table below shows some approximate comparable doses of these estrogens in terms of general estrogenicity.
Table 1: Approximate or estimated comparable doses of estrogens in terms of general/systemic estrogenicity (Aly, 2020; Kuhl, 2005; Table; Table; Table):
Estrogen type/route
Very low dose a
Low dose a
Moderate dose b
High dose
Oral estradiol
1 mg/day
2 mg/day
4 mg/day
8 mg/day
Transdermal estradiolc
25 μg/day
50 μg/day
100 μg/day
200 μg/day
Oral conjugated estrogens
0.625 mg/day
1.25 mg/day
2.5 mg/day
5 mg/day
Oral ethinylestradiol
7.5 μg/day
15 μg/day
30 μg/day
60 μg/day
Oral diethylstilbestrol
0.375 mg/day
0.75 mg/day
1.5 mg/day
3 mg/day
Comparable estradiol level
~25 pg/mL
~50 pg/mL
~100 pg/mL
~200 pg/mL
a Menopausal replacement dosages. b Similar to normal mean/integrated estrogenic exposure during the menstrual cycle in premenopausal women (Aly, 2018). c Specifically transdermal patches.
Estrogens were first associated with blood clots and associated cardiovascular complications in the 1960s and 1970s. Significant to substantial increases in these risks were found in clinical trials of high-dose DES (5 mg/day) for prostate cancer in men (VACURG, 1967; Byar, 1973; Turo et al., 2014), trials of moderate-dose CEEs (2.5–5 mg/day) for prevention of heart disease in men (Coronary Drug Project Research Group, 1970; Coronary Drug Project Research Group, 1973; Luria, 1989; Sudhir & Komesaroff, 1999; Dutra et al., 2019), and studies of early high-dose EE-containing birth control pills (50–150 μg/day) in premenopausal women (Gerstman et al., 1991; PCASRM, 2017; Table). The increase in cardiovascular events with DES in men with prostate cancer was sufficiently great that it actually cancelled out the benefits of its effects against prostate cancer in terms of overall mortality. The large increases in blood clots and cardiovascular problems seen in these studies resulted in alarm and concern about the safety of estrogens. Consequent to these events, estrogen doses were lowered. DES for prostate cancer was decreased to 1 to 3 mg/day and EE in birth control pills was decreased to 20 to 35 μg/day. Estrogens were also reduced to lower doses for other indications, such as menopausal hormone therapy. The dose reductions helped to lower the risks, although it did not eliminate them.
Whereas the WHI demonstrated causation for oral CEEs alone in terms of blood clot risk, no adequately powered RCTs have been conducted with oral or transdermal estradiol alone to establish causation in terms of blood clot risk at this time. Only very large and expensive trials would be able to show this due to the rarity of blood clots, and these studies have not been conducted to date. For similar reasons, RCTs demonstrating increased risk of blood clots with EE-containing birth control pills have also not been conducted at this time (Moores, Bilello, & Murin, 2004). In any case, causation has clearly been demonstrated with estrogens in other contexts, and this can be assumed as likely in the case of oral estradiol similarly. In addition, the Estrogen in Venous Thromboembolism Trial (EVTET), an RCT of low-dose (2 mg/day) oral estradiol plus the progestogen norethisterone acetate (NETA) versus placebo in postmenopausal women with history of previous blood clots, found that this hormone therapy regimen significantly increased coagulation and the incidence of blood clots (10.7% incidence with hormone therapy and 2.3% with placebo; P = 0.04) (Høibraaten et al., 2000; Høibraaten et al., 2001).
Estradiol levels appear to not be associated with blood clot risk in premenopausal women (Holmegard et al., 2014). The fact that transdermal estradiol patches at 100 μg/day in menopausal women haven’t been associated with a greater risk of blood clots is notable as this dose achieves estradiol levels of around 100 pg/mL on average, which are similar to the mean integrated levels of estradiol during the normal menstrual cycle in premenopausal women (Aly, 2018; Wiki). Rates of blood clots are also similar between men—who have relatively low estradiol levels—and women after controlling for atypical hormonal states like pregnancy and use of birth control pills in women (Moores, Bilello, & Murin, 2004; Rosendaal, 2005; Montagnana et al., 2010; Roach et al., 2013). Interestingly however, men have a consistently higher incidence of recurrent blood clots than women (Roach et al., 2013). These findings suggest that physiological levels of estradiol and progesterone in premenopausal women may not meaningfully increase coagulation or blood clot risk. However, the available data are mixed, with some studies suggesting that estradiol and/or progesterone levels within physiological ranges may indeed influence coagulation (Chaireti et al., 2013) and blood clot risk in premenopausal and/or perimenopausal women (Simon et al., 2006; Canonico et al., 2014; Scheres et al., 2019).
Modern combined birth control pills contain EE at moderately estrogenic doses (20–35 μg/day) and a physiological dose of a progestogen. They increase the risk of blood clots by several-fold (Konkle & Sood, 2019; Vinogradova, Coupland, & Hippisley-Cox, 2015; Table). In addition, they are associated with about a 1.5- to 2-fold increase in risk of heart attack and stroke (Lidegaard, 2014; Konkle & Sood, 2019). However, overall mortality is not increased with birth control pills—at least in the relatively young women in whom they are used (Hannaford et al., 2010). Per studies of menopausal hormone therapy, it is likely that the progestogen in EE-containing birth control pills augments the risk of blood clots with EE. Early high-dose birth control pills (50–100 μg/day) had as much as twice the risk of blood clots of modern birth control pills (Gerstman et al., 1991; PCASRM, 2017; Table). In contrast to the different blood clot risks between oral and transdermal estradiol, non-oral birth control forms containing EE, for instance transdermal birth control patches and vaginal birth control rings, are associated with similar increases in blood clot risk as EE-containing birth control pills (Plu-Bureau et al., 2013; PCASRM, 2017; Konkle & Sood, 2019; Abou-Ismail, Sridhar, & Nayak, 2020). Hence, unlike with estradiol, route of administration does not appear to modify blood clot risk with EE based on available data.
High-dose estrogen therapy using oral synthetic estrogens like DES and EE in people with breast or prostate cancer has been found to strongly increase the risk of blood clots and associated cardiovascular complications (Phillips et al., 2014; Turo et al., 2014; Coelingh Bennink et al., 2017). This has also been the case with estramustine phosphate (EMP; estradiol normustine phosphate), an estradiol ester that is used at massive doses in prostate cancer (e.g., 140–1,400 mg/day orally) and that results in pregnancy levels of estradiol (Kitamura, 2001 [Graph]; Ravery et al., 2011). In the 1980s however, it was found that high-dose non-oral estradiol did not have the same cardiovascular risks as high-dose estrogen therapy with oral synthetic estrogens or EMP (von Schoultz et al., 1989; Ockrim & Abel, 2009). This included studies with polyestradiol phosphate (PEP), a long-lasting injectable prodrug of estradiol, and with high-dose transdermal estradiol gel (von Schoultz et al., 1989; Aly, 2019). However, subsequent larger and higher-quality studies found that although the cardiovascular risks with PEP were much lower than with high-dose oral synthetic estrogen therapy, they were nonetheless still increased (Hedlung et al., 2008; Ockrim & Abel, 2009; Hedlund et al., 2011; Sam, 2020). This includes an approximate 2-fold increase in the risk of blood clots with estradiol levels in the range of roughly 300 to 500 pg/mL (Sam, 2020). Studies using high-dose transdermal estradiol patches have not found significantly increased cardiovascular complications as of present (Langley et al., 2013; Sam, 2020). However, these studies have been relatively underpowered, which limits their interpretation. In any case, increased coagulation has been observed with high-dose transdermal estradiol patches (achieving estradiol levels of 350 to 500 pg/mL) (Bland et al., 2005) similarly to PEP (Mikkola et al., 1999). More data on the risk of blood clots and cardiovascular issues with high-dose transdermal estradiol patches should come in the future with PATCH and STAMPEDE—two large-scale clinical studies in the United Kingdom that are evaluating this form of estradiol for prostate cancer (Gilbert et al., 2018; Singla, Ghandour, & Raj, 2019).
Injections of short-acting estradiol esters like estradiol valerate and estradiol cypionate are notable in that they are often used by transfeminine people and are generally used at doses that achieve high estradiol levels. As with high-dose transdermal estradiol patches, little to no quality data on the risk of blood clots exists for these preparations at present. Pyra and colleagues found that the risk of blood clots with injectable estradiol valerate in transfeminine people was increased by around 2-fold, but the confidence intervals were very wide and statistical significance was not reached (Pyra et al., 2020). The doses used in the whole population for the study were not provided, but in the actual VTE cases, the doses of injectable estradiol valerate were described and ranged from 4 to 20 mg once per week and 10 to 40 mg once every 2 weeks (Pyra et al., 2020). Studies have also assessed and found increased coagulation with high doses of estradiol valerate by injection in the range of 10 to 40 mg once every 2 weeks in men with prostate cancer (Kohli & McClellan, 2001; Kohli et al., 2004; Kohli, 2005). Increased coagulation has additionally been observed with the combination of 5 mg estradiol valerate and a progestogen once per month as a combined injectable contraceptive in premenopausal women (Meng et al., 1990; UN/WHO et al., 2003). It is unclear whether the high peaks in estradiol levels associated with short-acting injectable forms of estradiol are harmful in terms of coagulation and blood clot risk (Hembree et al., 2017). However, the increased risk of polycythemia with short-acting injectable testosterone esters relative to other non-oral forms of testosterone (Ohlander, Varghese, & Pastuszak, 2018) is indirectly suggestive that this could be the case. Accordingly, a study found increased coagulation in premenopausal women with a combined injectable contraceptive containing estradiol valerate but not with one employing the more prolonged and stable estradiol cypionate at the same dose (UN/WHO et al., 2003).
Pregnancy is a time when estradiol and progesterone levels increase to extremely high concentrations (Graphs). Estradiol levels increase progressively throughout pregnancy to around 2,000 pg/mL on average at the end of the first trimester, to about 10,000 pg/mL on average at the end of the second trimester, and to around 20,000 pg/mL on average at the end of the third trimester (Kerlan et al., 1994 [Graph]; Schock et al., 2016). Coagulation is greatly increased during pregnancy, and the risk of blood clots is likewise strongly increased (Heit et al., 2000; Abdul Sultan et al., 2015; Heit, Spencer, & White, 2016; Table). Estradiol and progesterone levels are strongly correlated with the increases in coagulation during pregnancy (Bagot et al., 2019). The risk of blood clots with modern birth control pills is similar to that with pregnancy as a whole (Heit, Spencer, & White, 2016), while the increases in risk of blood clots with early high-dose EE-containing birth control pills and with high-dose oral synthetic estrogen therapy for breast and prostate cancer are comparable to the risk increase during late pregnancy. Estradiol levels also increase to very high concentrations during ovarian stimulation for in-vitro fertilization in premenopausal women, and this has been associated with increased coagulation and risk of blood clots as well (Westerlund et al., 2012; Rova, Passmark, & Lindqvist, 2012; Kasum et al., 2014).
Due to their greater risks of cardiovascular problems as well as other concerns, DES has been virtually abandoned while EE has been discontinued for almost all indications except birth control. EE continues to be used in birth control because it is resistant to metabolism in the uterus and controls menstrual bleeding better than oral estradiol does (Stanczyk, Archer, & Bhavnani, 2013). CEEs are also being increasingly superseded by estradiol in medicine, although significant use of CEEs for hormone therapy in cisgender women continues. Transdermal estradiol is gaining momentum over oral estradiol in menopausal hormone therapy as well. Major transgender hormone therapy guidelines (see also Aly, 2020) recommend against the use of EE and CEEs in transfeminine people due to their greater risks and the inability to accurately monitor blood estrogen levels with these preparations (Coleman et al., 2012; Deutsch, 2016; Hembree et al., 2017). Estradiol is the estrogen that is almost exclusively used in transfeminine people today. Besides estrogen type, it has been recommended that transdermal estradiol be used instead of oral estradiol in transfeminine people who are over 40 or 45 years of age or are otherwise at risk for blood clots (Deutsch, 2016; Iwamoto et al., 2019; Glintborg et al., 2021). Menopausal hormone therapy guidelines similarly recommend the use of transdermal estradiol over oral estrogens in cisgender women who are at higher risk for blood clots (e.g., Stuenkel et al., 2015).
In a historically notable study conducted by the Center of Expertise on Gender Dysphoria (CEGD) at the Vrije Universiteit Medical Center (VUMC) in Amsterdam, the Netherlands in the 1980s, it was reported that the risk of blood clots with high-dose EE and CPA in transfeminine people was increased by 45-fold relative to the expected incidence in the general population (Asscheman, Gooren, & Eklund, 1989; Asscheman et al., 2014). Mortality also appeared to be elevated and other health risks were increased as well (Asscheman, Gooren, & Eklund, 1989; Gooren & T’Sjoen, 2018). A subsequent study in transfeminine people by the CEGD confirmed strongly increased coagulation with EE but much lower increases with oral or transdermal estradiol (Toorians et al., 2003). Upon the CEGD switching transfeminine people from high-dose EE to physiological doses of oral or transdermal estradiol (also usually in combination with CPA), the risks decreased considerably (van Kesteren et al., 1997; Asscheman et al., 2011; Asscheman et al., 2014). These findings were of major importance in the replacement of EE with estradiol in transfeminine hormone therapy, and have surely contributed significantly to apprehension about the use of high doses of estrogens in transfeminine people.
Taken together, estrogens of all kinds have been shown to dose-dependently increase or be associated with increased risk of blood clots. These findings suggest that, provided of course sufficient exposure occurs, increased coagulation and blood clot risk are common properties of estrogens. However, synthetic and non-bioidentical estrogens have greater risk of blood clots than estradiol, and oral estradiol shows greater risk than non-oral estradiol. In fact, physiological estradiol levels in women and low to moderate doses of transdermal estradiol may have no significant risk of blood clots at all. Nonetheless, non-oral estradiol with sufficiently high exposure can increase blood clot risk just the same as other forms of estrogen. Concomitant therapy with progestogens appears to augment the risk of blood clots with estrogens and high doses may particularly amplify the risk.
Risks with Different Hormonal Exposures
The table below provides relative risk increases for blood clots with different types, routes, and doses of estrogens, as well as with SERMs, pregnancy, and high-dose CPA. It shows the greater risks of blood clots with (1) oral estradiol relative to non-oral estradiol; (2) estradiol compared to non-bioidentical estrogens; and (3) lower estrogen levels/doses relative to higher estrogen levels/doses.
Table 2: Relative risks of blood clots with different hormonal exposures (see also Machin & Ragni, 2020):
Footnotes:a At typical menopausal replacement doses (i.e., not very high—probably no more than double the given dose). b MPA, norethisterone, norgestrel, or drospirenone. c Modern EE + P birth control contains 20–35 μg/day EE, while high-dose EE + P birth control used in the 1960s and 1970s contained 50–150 μg/day EE. d Risk around twice as high as modern birth control pills. e Unpublished original research/analysis with borderline statistical significance (95% CI 0.99–4.22). f Excluding the postpartum period. With the postpartum period included, the risk of blood clots with pregnancy is 5–10× (McLintock, 2014). Abbreviations: E2 = Estradiol; CEEs = Conjugated estrogens; EE = Ethinylestradiol; DES = Diethylstilbestrol; EMP = Estramustine phosphate; PEP = Polyestradiol phosphate; SERMs = Selective estrogen receptor modulators; CPA = Cyproterone acetate; P = Progestogen.
Note that the values in the table are associations mostly from observational studies rather than from RCTs. Hence, in many cases, causation has not been definitively established. In addition, the values represent rough average values with often wide 95% confidence intervals. As a result, precision and accuracy of the estimates may in some cases be low. Also note that quantified blood clot risk will vary depending on the study and its definitions and methodology (including factors like sampling error, approach to control of confounding variables, and residual confounding influences).
Mechanisms of Increased Coagulation with Estrogens
Aside from coagulation factors, estrogens also modulate the synthesis of numerous other liver products (Kuhl, 1999; Kuhl, 2005; Table). Examples include sex hormone-binding globulin (SHBG), corticosteroid-binding globulin (CBG), various other circulating binding proteins, angiotensinogen, lipoproteins, and triglycerides, among others. In accordance with the mechanisms underlying increased coagulation and blood clot risk with estrogens, the differences in risk of blood clots with different types and routes of estrogens are mirrored in their influences on estrogen-sensitive liver products. Put another way, different estrogens have different relative potency in the liver when compared to their estrogenic potency elsewhere in the body. Synthetic and non-bioidentical estrogens have greater impact on liver synthesis than estradiol, while oral administration of estradiol has greater influence on liver synthesis than non-oral routes like transdermal administration or intramuscular injection, and this is likely to explain the observed differences in coagulation and blood clot risk with these different estrogens. The table below shows the liver potency of different estrogenic exposures as measured by influence specifically on SHBG levels, one of the most sensitive and well-characterized estrogen-modulated liver products.
Table 3: Relative increases in SHBG levels with different estrogenic exposures (see also Aly, 2020):
Footnotes:a Due to differences in molecular weight, estradiol valerate has about 75% of the amount of estradiol as regular estradiol. Hence, 6 mg/day estradiol valerate is approximately equivalent to 4.5 mg/day estradiol. b Modern EE + P birth control contains 20–35 μg/day EE, while high-dose EE + P birth control used in the 1960s and 1970s contained 50–150 μg/day EE. c In the form of 320 mg/month PEP (~700 pg/mL estradiol), 100 mg/month estradiol undecylate (~500–600 pg/mL estradiol), or 10 mg/10 days estradiol valerate (~500–1,200 pg/mL peak estradiol; Graphs). Abbreviations: E2 = Estradiol; EV = Estradiol valerate; CEEs = Conjugated estrogens; EE = Ethinylestradiol; DES = Diethylstilbestrol; EMP = Estramustine phosphate; PEP = Polyestradiol phosphate; P = Progestogen.
The increase in SHBG levels with estrogen therapy correlates with increases in coagulation and blood clot risk and can serve as a reliable surrogate indicator of these effects (Odlind et al., 2002; van Rooijen et al., 2004; van Vliet et al., 2005; Tchaikovski & Rosing, 2010; Raps et al., 2012; Stegeman et al., 2013; Hugon-Rodin et al., 2017; Eilertsen et al., 2019). The increases in SHBG levels and blood clot risk even appear quite similar to each other with modern birth control pills (both ~4-fold), high-dose oral synthetic estrogen therapy (both ~5–10-fold), and late pregnancy (both ~5–10-fold). When data on blood clot risk with a given estrogen route or dose are limited or unavailable—for instance with high-dose oral estradiol or high-dose estradiol ester injections—changes in SHBG levels can be used as a rough proxy or surrogate instead to estimate overall liver impact, magnitude of change in coagulation systems, and blood clot risk. It should be noted however that progestogens may augment the blood clot risk with estrogens without necessarily affecting SHBG levels or even while decreasing SHBG levels via concomitant androgenic activity (Kuhl, 2005; Vinogradova, Coupland, & Hippisley-Cox, 2019).
Physiological levels of estradiol appear to have relatively minimal influence on liver synthesis (Eisenfeld & Aten, 1979; Lax, 1987; Kuhl, 2005). This is in accordance with the limited influence or non-influence of physiological estradiol levels in women on blood clot risk. It is thought that under normal physiological circumstances, estradiol is only supposed to considerably affect liver synthesis at very high levels—namely during pregnancy. The changes in synthesis of liver products during pregnancy presumably have important biological roles at this time (Eisenfeld & Aten, 1979). One of these is considered to be increased coagulation, as coagulation limits blood loss with childbirth and hence has survival benefits. Conversely, there is no obvious benefit to increased coagulation outside of pregnancy.
Estradiol and the Liver First Pass with Oral Administration
The oralroute of administration is subject to a first pass through the liver via the hepatic portal vein which is not present with non-oral routes of administration (Pond & Tozer, 1984; Back & Rogers, 1987). As such, oral estradiol is subject to a hepatic first pass while this does not occur with non-oral forms of estradiol such as transdermal estradiol and injectable estradiol (Kuhl, 1998; Kuhl, 2005). This first pass results in disproportionate exposure of the liver to estradiol as well as disproportionate estrogenic impact on liver protein synthesis (Kuhl, 2005). Oral estradiol likewise has disproportionate estrogenic impact on the hepatic synthesis of coagulation factors (Kuhl, 1998; Kuhl, 2005). Due to the first pass, it is estimated that there is a 4- or 5-fold greater estrogenic impact of oral estradiol in the liver relative to non-oral estradiol (Kuhl, 2005). Due to the absence of the hepatic first pass with most non-oral routes, there is strong biological plausibility for the lower risk of blood clots that has been found with transdermal estradiol in comparison to oral estradiol in observational studies (Baber et al., 2016).
Although oral estradiol has a much higher relative potential for blood clots due to the liver first pass, sufficiently high levels of estradiol will diffuse into the liver from the blood to act on this tissue regardless of route of administration. Hence, high levels of estradiol via non-oral routes (or produced by the body itself) can increase coagulation and blood clot risk similarly to the oral route. This is clearly evidenced by hyperestrogenic situations like pregnancy and ovarian stimulation for in-vitro fertilization, when estradiol levels increase to very high concentrations and substantially influence liver protein synthesis.
Non-Bioidentical Estrogens and Resistance to Liver Metabolism
Non-bioidentical estrogens such as EE, DES, and CEEs have greater impact on liver protein synthesis and risk of blood clots than either oral estradiol or non-oral estradiol (Kuhl, 1998; Kuhl, 2005; Phillips et al., 2014; Turo et al., 2014; Table). This is because the liver strongly metabolizes and inactivates estradiol, whereas non-bioidentical estrogens have differences in their chemical structures relative to estradiol that result in them being much more resistant to liver metabolism (Kuhl, 1998; Kuhl, 2005; Connors & Middeldorp, 2019; Swee, Javaid, & Quinton, 2019).
EE can be considered as a case example. The oral bioavailability of EE is around 45%, while that of estradiol is only about 5% (Kuhl, 2005; Stanczyk, Archer, & Bhavnani, 2013). In addition, the blood half-life of EE is in the range of 5 to 30 hours, compared to less than 1 hour in the case of estradiol (White et al., 1998; Kuhl, 2005; Stanczyk, Archer, & Bhavnani, 2013). As a result of these and other differences, EE is approximately 120 times as potent as estradiol by weight in terms of general estrogenic effect (Kuhl, 2005; Table). Hence, EE is used clinically in μg doses whereas oral estradiol is used at over 100-fold higher mg doses. The pharmacokinetic differences between EE and estradiol reflect the strong resistance of EE to liver metabolism (Kuhl, 2005). EE, or 17α-ethynylestradiol, shows resistance to liver metabolism because of an ethynyl group at the C17α position which has been added to what is the otherwise unchanged structure of estradiol (Kuhl, 2005). This modification results in steric hindrance which blocks 17β-hydroxysteroid dehydrogenases (17β-HSDs) as well as conjugating enzymes like sulfotransferases and glucuronosyltransferases from metabolizing EE at the C17β hydroxyl group. 17β-HSDs normally convert estradiol into the weakly active estrone while the conjugating enzymes convert estradiol into inactive C17β estrogen sulfate and glucuronide conjugates like estrone sulfate (Kuhl, 2005). An “ethinylestrone” metabolite is in fact a structural impossibility due to the requirement of a double bond for a C17 ketone group—the needed C17α position is already occupied in EE by its ethynyl group. As such, the metabolism of estradiol into weakly active or inactive metabolites like estrone and estrone sulfate in the liver is protective against activation of hepatic ERs and procoagulation, and the lack of this with EE is responsible for its greater blood clot risk (Kuhl, 2005; Russell et al., 2017).
Figure 2: Chemical structures of selected estrogens. The C17 position in the case of the steroidal estrogens (E2, E1, and EE) is at the top right of the steroid nucleus.
Due to the marked resistance of EE to hepatic metabolism and inactivation, it persists for a long time in the liver—often cycling through it many times before finally being broken down. Moreover, EE shows several-fold disproportionate impact on liver protein synthesis at otherwise equivalent doses relative to oral estradiol (Kuhl, 2005; Table). Consequently, whereas EE has around 120-fold the general potency of oral estradiol, the liver potency of EE is around 350 to 1,500 times greater than that of oral estradiol (von Schoultz et al., 1989; Kuhl, 2005). A dose of EE of as little as 1 μg/day has been shown to impact liver metabolism (Speroff et al., 1996; Trémollieres, 2012). In addition, the fact that EE shows similar hepatic impact and risk of blood clots regardless of whether it is administered orally, transdermally, or vaginally indicates that unlike oral estradiol, the first pass through the liver with oral administration is not necessary for blood clot risk with EE (Plu-Bureau et al., 2013; PCASRM, 2017; Konkle & Sood, 2019). EE is so resistant to metabolism that it does not seem to matter how it is administered—the liver impact is substantial regardless of route. The greatly increased liver potency of EE results in its influence on coagulation and blood clot risk being much higher than that of estradiol at equivalent doses.
CEEs show a few-fold disproportionate estrogenic impact on liver protein synthesis relative to oral estradiol but less than that of EE (Kuhl, 2005; Table). This can be attributed to the equine (horse) estrogens in CEEs, which humans are presumably not adapted to and which show resistance to liver metabolism in humans. DES, on the other hand, shows even greater estrogenic influence on the liver than EE (Kuhl, 2005; Table). The more disproportionate impact on liver synthesis of DES relative to EE or CEEs may be attributable to the fact that it is a nonsteroidal estrogen and is far removed in structure from steroidal estrogens. This is relevant as steroidal estrogens are susceptible to varying extents to robust steroid-metabolizing enzymes in the liver (Kuhl, 2005). As with EE, 17β-HSDs have no affinity for DES and the hydroxyl groups of DES are not oxidized to form estrone-like ketone metabolites (Jensen et al., 2010). Consequent to their resistance to liver metabolism relative to estradiol, CEEs and nonsteroidal estrogens like DES have greater impacts on coagulation and blood clot risk than equivalent doses of estradiol similarly to EE although to varying extents.
When compared to transdermal estradiol rather than oral estradiol, the disproportionate influence of oral non-bioidentical estrogens on estrogen-modulated liver protein synthesis becomes extreme. With a little math, it quickly becomes apparent why high doses of these estrogens have influences on liver proteins and blood clot risks that are comparable to those during pregnancy. The table below shows some roughly calculated estimates for comparative liver strength of the different estrogens.
Table 4: Roughly calculated ratios of liver estrogenic potency to general/systemic estrogenic potency with estrogens based on a selection of liver products (e.g., SHBG, others) (Kuhl, 2005; Table):
Estrogen
Comparative liver potency
Relative to oral E2
Relative to transdermal E2
Transdermal E2
~0.25×a
1.0×a
Oral E2
1.0×
~4.0×
Oral CEEs
1.3–4.5×
~5.2–18×
Oral EE
2.9–5.0×
~12–20×
Oral DES
5.7–7.5×
~23–30×
a Based on a study that found oral estradiol to have 4-fold greater effect on SHBG levels than transdermal estradiol when used at doses that produced similar estradiol levels (Nachtigall et al., 2000).
Changes in liver protein synthesis induced by estrogens don’t scale linearly with dose or relative liver potency. There is progressive saturation in terms of changes in levels of SHBG and other liver products with estrogen dose—that is, higher doses have relatively diminished effect compared to lower doses (Kuhl, 1990; Kuhl, 1999). As an example, oral EE shows the following dose-dependent increases in SHBG levels: 2.0-fold at 5 μg/day, 3.0-fold at 10 μg/day, 3.4-fold at 20 μg/day, and 4.0-fold at 50 μg/day (Kuhl, 1998; Kuhl, 1999). These findings can be attributed to saturation of the competitive binding and/or activation of liver ERs by high estrogen concentrations (Kuhl, 1990). An implication of this dose-dependent saturation is that although for instance oral EE has much stronger potency in the liver than oral estradiol, oral estradiol can more quickly “catch up” to oral EE and other non-bioidentical estrogens in terms of liver impact than might be initially anticipated. Accordingly, oral estradiol has shown the following dose-dependent increases in SHBG levels: 1.6-fold at 1 mg/day, 2.2-fold at 2 mg/day, and 1.9- to 3.2-fold at 4 mg/day (Fåhraeus & Larsson-Cohn, 1982; Kuhl, 1998; Gibney et al., 2005; Ropponen et al., 2005). Hence, although oral EE may have roughly 3- to 5-fold higher liver potency than oral estradiol, a dose of oral estradiol near-equivalent to that of oral EE in terms of general estrogenic effect can increase SHBG levels to an extent that is only somewhat lower in comparison.
Selective Estrogen Receptor Modulators and Metabolism Resistance
SERMs like tamoxifen and raloxifene are essentially partial agonists of the ER. This is in contrast to estrogens—like estradiol, CEEs, EE, and DES—which act as full agonists of the ER. Similarly to nonsteroidal estrogens like DES, the clinically used SERMs are all nonsteroidal in structure and are strongly resistant to hepatic metabolism. In fact, certain SERMs, like tamoxifen and clomifene, are structurally related to and were derived from DES. SERMs show tissue differences in their ER-mediated effects, with estrogenic effects in some tissues (e.g., bone) and antiestrogenic effects in other tissues (e.g., breasts) (Lain, 2019; Table). Although there is variation between SERMs in terms of their effects in certain tissues (e.g., uterus), they are uniformly estrogenic in the liver. Consequently, SERMs show similar increases in blood clot risk as estrogens (Park & Jordan, 2002; Fabian & Kimler, 2005). As with non-bioidentical estrogens, the greater risk of blood clots with SERMs compared to oral estradiol can be attributed to their resistance to liver metabolism and hence to greater hepatic estrogenic potency. The SERMs that are used medically belong to diverse structural families (e.g., triphenylethylenes like tamoxifen and benzothiophenes like raloxifene). The only way in which SERMs of different structural classes are known to be related is in their shared interactions with the ERs.
Figure 3: Chemical structures of selected SERMs. They are nonsteroidal in structure and include tamoxifen (a triphenylethylene) and raloxifene (a benzothiophene).
Activation of the Estrogen Receptor is Specifically Responsible for Increased Coagulation with Estrogens and SERMs
Findings from preclinical and genetic research provide direct evidence for ER activation being responsible for the increased blood clot risk with estrogens. In an important animal study, EE was administered to mice and changes in procoagulant and anticoagulant biomarkers were measured (Cleuren et al., 2010). EE caused changes in levels of a variety of coagulation factors (Cleuren et al., 2010). The researchers also assessed estradiol and observed comparable changes (Cleuren et al., 2010). Co-administration of the selective ER full antagonist fulvestrant with EE neutralized all of the EE-induced coagulatory changes (Cleuren et al., 2010). Additionally, EE showed no effect on coagulation factors in ERα knockout mice (Cleuren et al., 2010). These findings are consistent with human and mouse genome-wide association studies which have found estrogen response elements (EREs)—DNA sequences that act as binding sites for genes regulated by the ER—embedded in a large number of genes involved in coagulatory pathways (Cleuren et al., 2010; Stanczyk, Mathews, & Cortessis, 2017).
The preceding findings are consistent with ER activation being responsible for increased coagulation and blood clot risk with estrogens and SERMs. This is in accordance with the fact that blood clot risk is a shared effect of selective ER agonists with highly diverse chemical structures, providing strong circumstantial support against a non-ER-mediated action of some sort being responsible (e.g., the weakly estrogenic metabolite estrone somehow mediating the blood clot risk with estradiol—Bagot et al., 2010). Increased coagulation and blood clot risk can thus be regarded as class effects of estrogens and SERMs—provided sufficiently high liver exposure. Due to differences in susceptibility to liver metabolism however, different ER agonists show differences in their relative impact on coagulation. Owing to estradiol’s lack of resistance to metabolism and its robust inactivation in the liver, the dosage requirements for increased coagulation and blood clot risk with estradiol—particularly in the case of non-oral estradiol—are greater than with non-bioidentical estrogens. Hence, estradiol, especially when administered via non-oral routes, is a safer form of estrogen therapy than other estrogens.
Absolute Incidences and Risk Factors
States of estrogen and/or progestogen exposure, such as exogenous hormone administration and pregnancy, are of course established risk factors for blood clots in women. In healthy young individuals without relevant risk factors for blood clots however, the incidence of blood clots is rare even in situations of considerably increased risk due to hormones (Rosendaal, 2005). The absolute incidence of VTE in non-pregnant women is only 1 to 5 of every 10,000 women each year (i.e., 0.01–0.05% per year) (PCASRM, 2017; Konkle & Sood, 2019). EE-containing birth control pills, which on average increase VTE risk by about 4-fold, are associated with an incidence of VTE of only 3 to 9 of every 10,000 women each year (i.e., 0.03–0.09% per year) (Konkle & Sood, 2019). Likewise, the absolute risk of blood clots during pregnancy, when estradiol and progesterone levels increase to extremely high concentrations and VTE risk is increased up to 7-fold (Abdul Sultan et al., 2015), is about 5 to 20 of every 10,000 women each year (i.e., 0.05–0.2% per year) (PCASRM, 2017; Konkle & Sood, 2019).
a 1–2/10,000 per year at <19 years of age, 2–3/10,000 per year at 20–29 years of age, 3–4/10,000 per year at 30–39 years of age, 5–7/10,000 per year at 40–49 years of age; roughly 3–4/10,000 per year for age 15–49 years overall (Rabe et al., 2011).
In addition to time and population considerations, there are, besides estrogen and progestogen exposure, a variety of other known risk factors for blood clots, and these risk factors can substantially augment blood clot risk (Heit et al., 2000; Rosendaal, 2005). Age is among the strongest of the known risk factors (Rosendaal, 2005; Montagnana et al., 2010). Moreover, age is uniquely notable as a risk factor in that it is one that eventually becomes relevant to everyone. The risk of blood clots increases on the order of 100-fold going from ≤15 years of age (incidence <0.005–0.01% per year) to ≥80 years of age (incidence ~0.5–1.0% per year) (Rosendaal, 2005; Montagnana et al., 2010; Rabe et al., 2011). The figure below provides a graphical representation of the influence of age on risk of blood clots.
Figure 4: Risk of first-incidence VTE (per 100,000 per year) by age group (in years) in men (black bars) and women (gray bars) (Oger, 2000; Rosendaal, 2005; Rosendaal, 2016).
Other established risk factors for blood clots and associated cardiovascular problems include physical inactivity (due to, e.g., bed rest, long-distance travel, etc.), obesity, smoking, thrombophilic abnormalities, cancer, surgery, and HIV, among many others (Baron et al., 1998; Heit et al., 2000; Rosendaal, 2005; Lijfering, Rosendaal, & Cannegieter, 2010; Timp et al., 2013). In addition to age, physical inactivity is one of the most important risk factors for blood clots and mediates the risk increases for many of the others (Rosendaal, 2005). Smoking on its own is not consistently associated with increased risk of VTE (Lijfering, Rosendaal, & Cannegieter, 2010), but in combination with EE-containing birth control pills has been associated with a synergistic increase in VTE risk (Pomp, Rosendaal, & Doggen, 2008) as well as large increases in risk of heart attack—for instance 20-fold higher risk in heavy smokers (Kuhl, 1999). The table below shows the influence of a selection of known risk factors for VTE:
Thrombophilias, heritable and acquired, exist in significant percentages of the population and can lead to large increases in blood clot risk (Lijfering, Rosendaal, & Cannegieter, 2010). Moreover, they are often if not usually unknown (Morimont, Dogné, & Douxfils, 2020). This is due to the fact that screening for heritable thrombophilias is mainly based on family history, which has low sensitivity and poor predictive value for identifying people with these abnormalities (Morimont, Dogné, & Douxfils, 2020). Hence, many people are at increased risk of blood clots without realizing it. The table below shows the prevalences of a variety of thrombophilic abnormalities and their impacts on blood clot risk.
Blood clots are considered to be a multicausal disease (Rosendaal, 2005). The risk of blood clots and associated cardiovascular complications with hormonal exposure is highest when multiple risk factors combine in a given individual. Under what are among the most extreme of circumstances in terms of risk—elderly people with cancer who are on high-dose oral synthetic estrogen therapy (e.g., DES)—blood clot incidence can be as high as 15 to 28% and overall incidence of cardiovascular complications as great as 35% (Phillips et al., 2014; Sciarria et al., 2014; Turo et al., 2014). These adverse effects contribute to substantial morbidity and incidence of death in these populations. Most people are however at nowhere near as great of risk. Risk factors like age are why pregnant women can have massive levels of estradiol and progesterone with relatively little issue whereas elderly cancer patients on high-dose oral synthetic estrogen therapy have a considerable risk of death.
In the VUMC studies that found 20- to 45-fold increased incidence of blood clots with high-dose EE and CPA over 5 to 10 years in transfeminine people, the absolute incidence of blood clots was approximately 6.3% (142/10,000 people per year) in the 1989 report and 5.5% (58/10,000 people per year) in the 1997 follow up (Asscheman, Gooren, & Eklund, 1989; van Kesteren et al., 1997; Asscheman et al., 2014; Goldstein et al., 2019; Min & Hopkins, 2021). In keeping with the known influence of age on blood clot risk, the absolute incidence was 2.1% in those under 40 years of age and 12% in those over 40 years of age in the 1989 study (Asscheman, Gooren, & Eklund, 1989; Asscheman et al., 2014). In about 70% of cases, there were—aside from age—no known risk factors for blood clots (Asscheman, Gooren, & Eklund, 1989; Asscheman et al., 2014). Following subsequent replacement of EE with low-to-moderate-dose transdermal estradiol in those over 40 years of age, the incidence of blood clots decreased substantially (with only one event occurring in the transdermal estradiol group) (van Kesteren et al., 1997; Asscheman et al., 2014; Min & Hopkins, 2021). A later study in 2013 by the Ghent University Hospital in Belgium observed a blood clot incidence of 5.1% in transfeminine people using mostly oral or transdermal estradiol with or without CPA over an average treatment period of 7.7 years (range 3 months to 35 years) (Wierckx et al., 2013; Min & Hopkins, 2021). Those who had blood clots often had other risk factors such as older age, smoking, immoblization due to surgery, or hypercoagulability (Wierckx et al., 2013; Min & Hopkins, 2021). In addition to cumulative exposure time, these studies further highlight the converging impact of multiple risk factors—with estrogen type, route, and dose, progestogen exposure, and age included among them—on the risk of blood clots.
Therapeutic Implications for Transfeminine People
Due to their greater risk of blood clots and cardiovascular problems, non-bioidentical estrogens like EE and CEEs are mostly no longer used in transfeminine people. Instead, estradiol, both in oral and non-oral forms, is used. Transgender clinical guidelines generally recommend keeping estradiol levels within normal physiological ranges for non-pregnant females of around 100 to 200 pg/mL regardless of whether the route of administration of estradiol is oral or non-oral (Aly, 2018). Higher estradiol levels are not currently known to have greater therapeutic benefit in terms of feminization or breast development (Nolan & Cheung, 2020). However, higher levels, in the range of 200 to 500 pg/mL, can provide additional therapeutic effect in the area of testosterone suppression—which can be indirectly beneficial to feminization if otherwise inadequate (Aly, 2018). Despite their recommendations for keeping estradiol levels in physiological ranges, transgender clinical guidelines notably recommend doses of estradiol ester injections that reach and even greatly exceed estradiol levels of 200 pg/mL (Aly, 2021).
Based on the available research (e.g., the risk of blood clots with lower doses, comparative SHBG increases), it would not be surprising if high-dose oral estradiol (e.g., 8 mg/day) had similar risk of blood clots as the relatively lower amounts of EE in birth control pills. The risk is likely to be particularly great in combination with progestogens (e.g., CPA). Due to its greater and unnecessary risk of blood clots relative to non-oral estradiol, oral estradiol should ideally be avoided in transfeminine people—particularly in those with risk factors for blood clots such as older age (e.g., >40 years) or concomitant progestogen use. However, the convenience of oral estradiol and its relative inexpensiveness (compared to e.g. transdermal forms) are significant advantages that will also be considered by transfeminine people and their clinicians. In contrast to oral estradiol, non-oral estradiol—with estradiol levels kept in physiological ranges of for instance 100 to 200 pg/mL—appears to have minimal to no risk of blood clots. Hence, non-oral estradiol at these levels can be used in transfeminine people with little concern.
In terms of higher estradiol levels delivered non-orally, the estimated 2-fold increase in risk of blood clots with estradiol levels of approximately 300 to 500 pg/mL (Sam, 2020) is notably lower than the average 4-fold increase in risk with widely used EE-containing birth control pills. Based on the usefulness of these levels for suppressing testosterone production and the widespread usage of EE-based birth control in cisgender women throughout the world, the degree of blood clot risk with high-dose non-oral estradiol, in reasonable amounts, could be considered therapeutically acceptable in transfeminine people (Haupt et al., 2020). This may be particularly true when high-dose non-oral estradiol monotherapy is compared to combination of estradiol with antiandrogens like spironolactone, CPA, or bicalutamide, which all have their own unique risks and drawbacks. In any case, as with oral estradiol, high estradiol levels with non-oral estradiol should ideally be avoided due to the additional risk they pose, and this is especially true in those with relevant risk factors for blood clots (e.g., older age). In addition, very high doses of non-oral estradiol resulting in estradiol levels above those required for testosterone suppression are difficult to justify as they pose further unnecessary risk and offer no clear additional therapeutic benefit.
Prevention of Blood Clots
The best way to prevent blood clots from happening is to avoid risk altogether. Avoiding use of oral estradiol, excessively high doses of non-oral estradiol, and progestogens when feasible and opting for safer therapeutic choices is recommended in this regard. In addition, avoiding use of such therapies in those with risk factors like older age (>40 years), known thrombophilic abnormalities, and sedentary lifestyle is advocated. Proactive behaviors like physical activity (e.g., walking, exercise), quitting smoking, and weight loss may help to reduce the risk of blood clots (Hibbs, 2008).
Certain anticoagulant and antiplatelet medications are used to help prevent blood clots in high-risk individuals. Examples include low-dose aspirin (Mekaj, Daci, & Mekaj, 2015; Matharu et al., 2020), direct factor Xa inhibitors like rivaroxaban (Xarelto) (Blondon, 2020), and direct thrombin inhibitors like dabigatran (Pradaxa), among others. Aspirin has been found to be effective in the prevention of blood clots (Mekaj, Daci, & Mekaj, 2015; Matharu et al., 2020) and has been recommended for use specifically in transfeminine people on hormone therapy (Feldman & Goldberg, 2006; Deutsch, 2016). However, evidence is limited and conflicting for prevention of blood clots related to hormone therapy (Grady et al., 2000; Cushman et al., 2004) and use of aspirin in transfeminine people for such purposes has been recommended against by others (Shatzel, Connelly, & DeLoughery, 2017). Rivaroxaban has been associated with more than completely offset risk of blood clots with oral menopausal hormonal therapy (Blondon, 2020). In any case, no anticoagulants are currently approved or well-supported for preventing risk of blood clots with hormone therapy. Accordingly, clinical guidelines state that there is insufficient evidence to guide decision-making in this area at this time (e.g., McLintock, 2014). It should also be cautioned that anticoagulants have side effects and risks of their own and should be used carefully.
Temporary discontinuation of estrogen therapy before surgery has traditionally been thought to help reduce the risk of blood clots during recovery based on theory and has been advised as well as mandated for transfeminine people undergoing surgical procedures (e.g., Asscheman et al., 2014). However, evidence is limited and inconclusive on this strategy at present and more research is needed to determine whether it is actually beneficial or not (Boskey, Taghinia, & Ganor, 2019; Nolan & Cheung, 2020; Haveles et al., 2021; Hontscharuk et al., 2021; Kozato et al., 2021; Nolan et al., 2021; Zucker, Reisman, & Safer, 2021). Recent studies have not found reduction in risk of blood clots with discontinuation of hormone therapy before surgery in transfeminine people but these studies have been underpowered and larger studies are needed (Blasdel et al., 2021). Temporarily stopping hormone therapy can be distressing for many transfeminine people and this should be weighed accordingly. A potential alternative to discontinuation of hormone therapy is temporary use of transdermal estradiol at physiological doses which has no known blood clot risk and is more likely to be safe.
Updates
Update 1: Langley et al. (2021) [PATCH Study Results]
In February 2021, a report on long-term cardiovascular outcomes for the Prostate Adenocarcinoma: TransCutaneous Hormones (PATCH) trial was published (Langley et al., 2021) [PDF; Supplementary appendix]. The PATCH trial is a large ongoing phase 2/3 randomized controlled trial of high-dose transdermal estradiol patches versus GnRH agonists for the treatment of prostate cancer in men (Langley et al., 2021). The estradiol patch dosage employed is specifically three to four 100 μg/day FemSeven or Progynova TS patches (Langley et al., 2021). In the February 2021 report of the study, 1,694 men were enrolled and randomized, with 790 included in the analysis for the GnRH agonist group and 904 included in the analysis for the estradiol patch group (Langley et al., 2021).
In those given estradiol, the median estradiol level was around 215 pg/mL (5%–95% range ~100–550 pg/mL) (Langley et al., 2021). About 93% of the men in this group achieved suppression of testosterone levels into the castrate range (<50 ng/dL), which was notably equal to the rate of suppression in the GnRH agonist group (~93%) (Langley et al., 2021). However, actual testosterone levels—as opposed to rates of testosterone suppression—were not provided in this report and hence comparison between groups is unavailable for this metric (Langley et al., 2021). After about 4 years median follow up, there were no significant differences on a variety of cardiovascular outcomes between the estradiol group and the GnRH agonist group (Langley et al., 2021). Among these outcomes included VTE, thromboembolic stroke, and other arterial embolic events (Langley et al., 2021). These results are in contrast to previous large clinical trials of PEP in prostate cancer, which found increased cardiovascular morbidity and risk of VTE but notably involved higher estradiol levels than employed in the PATCH trial (Ockrim & Abel, 2009; Sam, 2020). Based on their promising safety findings, the PATCH researchers stated that transdermal estrogen should be reconsidered for the treatment of prostate cancer (Langley et al., 2021).
These findings are reassuring and suggest that limitedly high levels of estradiol (e.g., 200–300 pg/mL perhaps) may likewise be acceptably safe in terms of blood clot and cardiovascular risk in transfeminine people. It should be noted however that the sample size of the trial, while large relative to previous clinical studies in this area, was underpowered for assessing risk of blood clots—which are relatively rare events that require very large samples to thoroughly quantify. Studies precisely assessing blood clot risk in peri- and postmenopausal women have included tens of thousands of individuals for instance. As such, while substantial increases in risk are not likely based on this trial, smaller increases in risk still cannot be ruled out at this time. It should additionally be noted that the robust testosterone suppression at the used doses in this study might not generalize to transfeminine people as a whole, as the men were mostly elderly and testosterone levels are known to decrease with age.
Update 2: Totaro et al. (2021) and Kotamarti et al. (2021)
Totaro, M., Palazzi, S., Castellini, C., Parisi, A., D’Amato, F., Tienforti, D., Baroni, M. G., Francavilla, S., & Barbonetti, A. (2021). Risk of Venous Thromboembolism in Transgender People Undergoing Hormone Feminizing Therapy: A Prevalence Meta-Analysis and Meta-Regression Study. Frontiers in Endocrinology, 12, 741866. [DOI:10.3389/fendo.2021.741866]
This study is the largest of its kind that has been conducted to date. The meta-analysis included 18 studies totaling 11,542 transfeminine people on hormone therapy. The pooled prevalence of VTE was 2% with a 95% confidence interval of 1 to 3%. However, there was large variability between studies. In the meta-regression analysis, older age and longer length of estrogen therapy were significantly positively associated with VTE prevalence. When analysis was restricted to those greater than or equal to 37.5 years of age, the prevalence of VTE was 3% (95% CI: 0–5%). Conversely, in those less than 37.5 years of age, the prevalence of VTE was 0% (95% CI: 0–2%). VTE prevalence was 1% (95% CI: 0–3%) with greater than or equal to 4.4 years of estrogen therapy and was 0% (95% CI: 0–3%) with less than 4.4 years of estrogen therapy. With regard to the 0% estimates, it is not the case that there is truly no risk of VTE in these instances but rather it can be assumed that the risks are sufficiently low that the meta-analysis was not powered well enough to detect and quantify them.
A limitation of the meta-analysis was that subgroup analyses based on estrogen type (i.e., estradiol vs. CEEs vs. EE) and route (e.g., oral estrogens or oral estradiol vs. transdermal estradiol) were said to not be possible due to insufficient data and hence were not performed. However, another recent meta-analysis published in July 2021, which analyzed much of the same literature as Totaro et al. (2021), did perform subgroup analyses by estrogen type and route. This publication is as follows:
Kotamarti, V. S., Greige, N., Heiman, A. J., Patel, A., & Ricci, J. A. (2021). Risk for Venous Thromboembolism in Transgender Patients Undergoing Cross-Sex Hormone Treatment: A Systematic Review. The Journal of Sexual Medicine, 18(7), 1280–1291. [DOI:10.1016/j.jsxm.2021.04.006]
And this is what they reported in terms of subgroup analyses for estrogen type and route:
Because varying VTE rates have been reported with different estrogen regimens, analyses of VTE incidence were performed comparing oral or transdermal delivery, or the specific estrogen formulation. As many studies reported populations using mixed estrogen formulations or did not report the type of estrogen regimen, further statistical analysis could not be performed.
Route of estrogen administration appeared to play a role in the AMAB population. [Oral] estrogens (7 studies; 34.0 VTE per 10,000 person-years) vs transdermal estrogens (3 studies, 11.2 VTE per 10,000 person-years). Additionally, estrogen formulation also appeared to have a difference VTE incidence. Ethinyl estradiol was also associated with increased VTE incidence (3 studies, 293.1 VTE per 10,000 person-years) followed by conjugated equine estrogens (1 study, 49.0 VTE per 10,000 person-years) and estradiol valerate (4 studies, 31.5 VTE per 10,000 person-years).
It is unclear how accurate these precise numbers are due to the quality limitations of the underlying data. Moreover, antiandrogens (e.g., CPA) were not controlled for and as discussed by this article are likely to additionally influence VTE risk. In any case, the reported numbers are interesting and are in accordance with different estrogen types and routes varying in terms of VTE risk.
References
Abdul Sultan, A., West, J., Stephansson, O., Grainge, M. J., Tata, L. J., Fleming, K. M., Humes, D., & Ludvigsson, J. F. (2015). Defining venous thromboembolism and measuring its incidence using Swedish health registries: a nationwide pregnancy cohort study. BMJ Open, 5(11), e008864. [DOI:10.1136/bmjopen-2015-008864]
Abou-Ismail, M. Y., Citla Sridhar, D., & Nayak, L. (2020). Estrogen and thrombosis: A bench to bedside review. Thrombosis Research, 192, 40–51. [DOI:10.1016/j.thromres.2020.05.008]
Amitrano, L., Guardascione, M. A., Brancaccio, V., & Balzano, A. (2002). Coagulation Disorders in Liver Disease. Seminars in Liver Disease, 22(1), 83–96. [DOI:10.1055/s-2002-23205]
Anderson, G. L., Limacher, M., Assaf, A. R., Bassford, T., Beresford, S. A., Black, H., Bonds, D., Brunner, R., Brzyski, R., Caan, B., Chlebowski, R., Curb, D., Gass, M., Hays, J., Heiss, G., Hendrix, S., Howard, B. V., Hsia, J., Hubbell, A., Jackson, R., … & Women’s Health Initiative Steering Committee. (2004). Effects of Conjugated Equine Estrogen in Postmenopausal Women With Hysterectomy: The Women’s Health Initiative Randomized Controlled Trial. JAMA, 291(14), 1701–1712. [DOI:10.1001/jama.291.14.1701]
Arnold, J. D., Sarkodie, E. P., Coleman, M. E., & Goldstein, D. A. (2016). Incidence of Venous Thromboembolism in Transgender Women Receiving Oral Estradiol. The Journal of Sexual Medicine, 13(11), 1773–1777. [DOI:10.1016/j.jsxm.2016.09.001]
Asscheman, H., Gooren, L., & Eklund, P. (1989). Mortality and morbidity in transsexual patients with cross-gender hormone treatment. Metabolism, 38(9), 869–873. [DOI:10.1016/0026-0495(89)90233-3]
Asscheman, H., Giltay, E. J., Megens, J. A., de Ronde, W. (Pim), van Trotsenburg, M. A., & Gooren, L. J. (2011). A long-term follow-up study of mortality in transsexuals receiving treatment with cross-sex hormones. European Journal of Endocrinology, 164(4), 635–642. [DOI:10.1530/eje-10-1038]
Asscheman, H., T’Sjoen, G., Lemaire, A., Mas, M., Meriggiola, M. C., Mueller, A., Kuhn, A., Dhejne, C., Morel-Journel, N., & Gooren, L. J. (2013). Venous thrombo-embolism as a complication of cross-sex hormone treatment of male-to-female transsexual subjects: a review. Andrologia, 46(7), 791–795. [DOI:10.1111/and.12150]
Baber, R. J., Panay, N., & Fenton, A. (2016). 2016 IMS Recommendations on women’s midlife health and menopause hormone therapy. Climacteric, 19(2), 109–150. [DOI:10.3109/13697137.2015.1129166]
Back, D. J., & Rogers, S. M. (2007). Review: first-pass metabolism by the gastrointestinal mucosa. Alimentary Pharmacology & Therapeutics, 1(5), 339–357. [DOI:10.1111/j.1365-2036.1987.tb00634.x]
Bagot, C., Marsh, M., Whitehead, M., Sherwood, R., Roberts, L., Patel, R., & Arya, R. (2010). The effect of estrone on thrombin generation may explain the different thrombotic risk between oral and transdermal hormone replacement therapy. Journal of Thrombosis and Haemostasis, 8(8), 1736–1744. [DOI:10.1111/j.1538-7836.2010.03953.x]
Bagot, C., Leishman, E., Onyiaodike, C., Jordan, F., Gibson, V., & Freeman, D. (2019). Changes in laboratory markers of thrombotic risk early in the first trimester of pregnancy may be linked to an increase in estradiol and progesterone. Thrombosis Research, 178, 47–53. [DOI:10.1016/j.thromres.2019.03.015]
Baron, J. A., Gridley, G., Weiderpass, E., Nyren, O., & Linet, M. (1998). Venous thromboembolism and cancer. The Lancet, 351(9109), 1077–1080. [DOI:10.1016/s0140-6736(97)10018-6]
Bezwada, P., Shaikh, A., & Misra, D. (2017). The Effect of Transdermal Estrogen Patch Use on Cardiovascular Outcomes: A Systematic Review. Journal of Women’s Health, 26(12), 1319–1325. [DOI:10.1089/jwh.2016.6151]
Blanco-Molina, M., Lozano, M., Cano, A., Cristobal, I., Pallardo, L., & Lete, I. (2012). Progestin-only contraception and venous thromboembolism. Thrombosis Research, 129(5), e257–e262. [DOI:10.1016/j.thromres.2012.02.042]
Bland, L. B., Garzotto, M., DeLoughery, T. G., Ryan, C. W., Schuff, K. G., Wersinger, E. M., Lemmon, D., & Beer, T. M. (2005). Phase II study of transdermal estradiol in androgen-independent prostate carcinoma. Cancer, 103(4), 717–723. [DOI:10.1002/cncr.20857]
Blasdel, G., Shakir, N., Parker, A., Bluebond-Langner, R., & Zhao, L. (2021). Letter to the Editor from Blasdel et al: “No Venous Thromboembolism Increase Among Transgender Female Patients Remaining on Estrogen for Gender-affirming Surgery”. The Journal of Clinical Endocrinology & Metabolism, 106(9), e3783–e3784. [DOI:10.1210/clinem/dgab243]
Blondon, M. (2020). Update On Oral Contraception And Venous Thromboembolism. HemaSphere Educational Updates in Hematology Book: 25th Congress of the European Hematology Association, Virtual Edition 2020, 4(S2). European Hematology Association. [Google Scholar] [DOI:10.1097/HS9.0000000000000444] [PDF]
Boskey, E. R., Taghinia, A. H., & Ganor, O. (2019). Association of Surgical Risk With Exogenous Hormone Use in Transgender Patients. JAMA Surgery, 154(2), 159–169. [DOI:10.1001/jamasurg.2018.4598]
Canonico, M., Plu-Bureau, G., Lowe, G. D., & Scarabin, P. (2008). Hormone replacement therapy and risk of venous thromboembolism in postmenopausal women: systematic review and meta-analysis. BMJ, 336(7655), 1227–1231. [DOI:10.1136/bmj.39555.441944.be]
Canonico, M., Plu-Bureau, G., O’Sullivan, M. J., Stefanick, M. L., Cochrane, B., Scarabin, P., & Manson, J. E. (2014). Age at menopause, reproductive history, and venous thromboembolism risk among postmenopausal women. Menopause, 21(3), 214–220. [DOI:10.1097/gme.0b013e31829752e0]
Cassidy, A., & Minihane, A. (2017). The role of metabolism (and the microbiome) in defining the clinical efficacy of dietary flavonoids. The American Journal of Clinical Nutrition, 105(1), 10–22. [DOI:10.3945/ajcn.116.136051]
Chaireti, R., Gustafsson, K. M., Bystrom, B., Bremme, K., & Lindahl, T. L. (2013). Endogenous thrombin potential is higher during the luteal phase than during the follicular phase of a normal menstrual cycle. Human Reproduction, 28(7), 1846–1852. [DOI:10.1093/humrep/det092]
Choi, J., Kim, D., Park, S., Lee, H., Kim, K., Kim, K., Kim, M., Kim, S., & Kim, S. (2015). Anti-thrombotic effect of rutin isolated from Dendropanax morbifera Leveille. Journal of Bioscience and Bioengineering, 120(2), 181–186. [DOI:10.1016/j.jbiosc.2014.12.012]
Cleuren, A., Van der Linden, I., de Visser, Y., Wagenaar, G., Reitsma, P., & van Vlijmen, B. (2010). 17α‐Ethinylestradiol rapidly alters transcript levels of murine coagulation genes via estrogen receptor α. Journal of Thrombosis and Haemostasis, 8(8), 1838–1846. [DOI:10.1111/j.1538-7836.2010.03930.x]
Coelingh Bennink, H. J., Verhoeven, C., Dutman, A. E., & Thijssen, J. (2017). The use of high-dose estrogens for the treatment of breast cancer. Maturitas, 95, 11–23. [DOI:10.1016/j.maturitas.2016.10.010]
Coleman, E., Bockting, W., Botzer, M., Cohen-Kettenis, P., DeCuypere, G., Feldman, J., Fraser, L., Green, J., Knudson, G., Meyer, W. J., Monstrey, S., Adler, R. K., Brown, G. R., Devor, A. H., Ehrbar, R., Ettner, R., Eyler, E., Garofalo, R., Karasic, D. H., … & Zucker, K. (2012). [World Professional Association for Transgender Health (WPATH)] Standards of Care for the Health of Transsexual, Transgender, and Gender-Nonconforming People, Version 7. International Journal of Transgenderism, 13(4), 165–232. [DOI:10.1080/15532739.2011.700873] [URL] [PDF]
Conard, J., Plu-Bureau, G., Bahi, N., Horellou, M., Pelissier, C., & Thalabard, J. (2004). Progestogen-only contraception in women at high risk of venous thromboembolism. Contraception, 70(6), 437–441. [DOI:10.1016/j.contraception.2004.07.009]
Connelly, P. J., Marie Freel, E., Perry, C., Ewan, J., Touyz, R. M., Currie, G., & Delles, C. (2019). Gender-Affirming Hormone Therapy, Vascular Health and Cardiovascular Disease in Transgender Adults. Hypertension, 74(6), 1266–1274. [DOI:10.1161/hypertensionaha.119.13080]
Connors, J. M., & Middeldorp, S. (2019). Transgender patients and the role of the coagulation clinician. Journal of Thrombosis and Haemostasis, 17(11), 1790–1797. [DOI:10.1111/jth.14626]
Curb, J. D., Prentice, R. L., Bray, P. F., Langer, R. D., Van Horn, L., Barnabei, V. M., Bloch, M. J., Cyr, M. G., Gass, M., Lepine, L., Rodabough, R. J., Sidney, S., Uwaifo, G. I., & Rosendaal, F. R. (2006). Venous Thrombosis and Conjugated Equine Estrogen in Women Without a Uterus. Archives of Internal Medicine, 166(7), 772–772. [DOI:10.1001/archinte.166.7.772]
Cushman, M. (2004). Estrogen Plus Progestin and Risk of Venous Thrombosis. JAMA, 292(13), 1573–1580. [DOI:10.1001/jama.292.13.1573]
Deitcher, S. R., & Gomes, M. P. (2004). The risk of venous thromboembolic disease associated with adjuvant hormone therapy for breast carcinoma. Cancer, 101(3), 439–449. [DOI:10.1002/cncr.20347]
DeLoughery, T. G. (2011). Estrogen and thrombosis: Controversies and common sense. Reviews in Endocrine and Metabolic Disorders, 12(2), 77–84. [DOI:10.1007/s11154-011-9178-0]
Deutsch, M. B. (2016). Overview of feminizing hormone therapy. In Deutsch, M. B. (Ed.). Guidelines for the Primary and Gender-Affirming Care of Transgender and Gender Nonbinary People, 2nd Edition (pp. 26–48). San Francisco: University of California, San Francisco/UCSF Transgender Care. [URL] [PDF]
Dinger, J., Do Minh, T., & Heinemann, K. (2016). Impact of estrogen type on cardiovascular safety of combined oral contraceptives. Contraception, 94(4), 328–339. [DOI:10.1016/j.contraception.2016.06.010]
Dittrich, R., Binder, H., Cupisti, S., Hoffmann, I., Beckmann, M., & Mueller, A. (2005). Endocrine Treatment of Male-to-Female Transsexuals Using Gonadotropin-Releasing Hormone Agonist. Experimental and Clinical Endocrinology & Diabetes, 113(10), 586–592. [DOI:10.1055/s-2005-865900]
Douxfils, J., Morimont, L., & Bouvy, C. (2020). Oral Contraceptives and Venous Thromboembolism: Focus on Testing that May Enable Prediction and Assessment of the Risk. Seminars in Thrombosis and Hemostasis, 46(8), 872–886. [DOI:10.1055/s-0040-1714140]
Douxfils, J., Klipping, C., Duijkers, I., Kinet, V., Mawet, M., Maillard, C., Jost, M., Rosing, J., & Foidart, J. (2020). Evaluation of the effect of a new oral contraceptive containing estetrol and drospirenone on hemostasis parameters. Contraception, 102(6), 396–402. [DOI:10.1016/j.contraception.2020.08.015]
Dutra, E., Lee, J., Torbati, T., Garcia, M., Merz, C. N., & Shufelt, C. (2019). Cardiovascular implications of gender-affirming hormone treatment in the transgender population. Maturitas, 129, 45–49. [DOI:10.1016/j.maturitas.2019.08.010]
Eilertsen, A. L., Dahm, A. E., Høibraaten, E., Lofthus, C. M., Mowinckel, M., & Sandset, P. M. (2019). Relationship between sex hormone binding globulin and blood coagulation in women on postmenopausal hormone treatment. Blood Coagulation & Fibrinolysis, 30(1), 17–23. [DOI:10.1097/mbc.0000000000000784]
Eisenfeld, A. J., & Aten, R. F. (1979). Estrogen receptor in the mammalian liver. In Briggs, M. H., & Corbin, A. (Eds.). Advances in Steroid Biochemistry and Pharmacology, 7, 91–117. London: Academic Press. [Google Scholar] [PubMed]
Eisenfeld, A. J., & Aten, R. F. (1987). Estrogen receptors and androgen receptors in the mammalian liver. Journal of Steroid Biochemistry, 27(4–6), 1109–1118. [DOI:10.1016/0022-4731(87)90197-x]
Fabian, C. J., & Kimler, B. F. (2005). Selective Estrogen-Receptor Modulators for Primary Prevention of Breast Cancer. Journal of Clinical Oncology, 23(8), 1644–1655. [DOI:10.1200/jco.2005.11.005]
Fåhraeus, L., & Larsson-Cohn, U. (1982). Oestrogens, gonadotrophins and SHBG during oral and cutaneous administration of oestradiol-17β to menopausal women. Acta Endocrinologica, 101(4), 592–596. [DOI:10.1530/acta.0.1010592]
Feldman, J. L., & Goldberg, J. (2006). Transgender Primary Medical Care: Suggested Guidelines for Clinicians in British Columbia. crhc/csac/Transcend Transgender Support & Education Society/Vancouver Coastal Health. [Google Scholar] [PDF]
Franchini, M., & Mannucci, P. M. (2015). Classic thrombophilic gene variants. Thrombosis and Haemostasis, 114(11), 885–889. [DOI:10.1160/th15-02-0141]
Fruzzetti, F., & Cagnacci, A. (2018). Venous thrombosis and hormonal contraception: what’s new with estradiol-based hormonal contraceptives? Open Access Journal of Contraception, 9, 75–79. [DOI:10.2147/oajc.s179673]
Gerstman, B. B., Piper, J. M., Tomita, D. K., Ferguson, W. J., Stadel, B. V., & Lundin, F. E. (1991). Oral Contraceptive Estrogen Dose and the Risk of Deep Venous Thromboembolic Disease. American Journal of Epidemiology, 133(1), 32–37. [DOI:10.1093/oxfordjournals.aje.a115799]
Getahun, D., Nash, R., Flanders, W. D., Baird, T. C., Becerra-Culqui, T. A., Cromwell, L., Hunkeler, E., Lash, T. L., Millman, A., Quinn, V. P., Robinson, B., Roblin, D., Silverberg, M. J., Safer, J., Slovis, J., Tangpricha, V., & Goodman, M. (2018). Cross-sex Hormones and Acute Cardiovascular Events in Transgender Persons. Annals of Internal Medicine, 169(4), 205. [DOI:10.7326/m17-2785]
Gibney, J., Johannsson, G., Leung, K., & Ho, K. K. (2005). Comparison of the Metabolic Effects of Raloxifene and Oral Estrogen in Postmenopausal and Growth Hormone-Deficient Women. The Journal of Clinical Endocrinology & Metabolism, 90(7), 3897–3903. [DOI:10.1210/jc.2005-0173]
Gilbert, D. C., Duong, T., Sydes, M., Bara, A., Clarke, N., Abel, P., James, N., Langley, R., Parmar, M., & (2018). Transdermal oestradiol as a method of androgen suppression for prostate cancer within the STAMPEDE trial platform. BJU International, 121(5), 680–683. [DOI:10.1111/bju.14153]
Glintborg, D., T’Sjoen, G., Ravn, P., & Andersen, M. S. (2021). MANAGEMENT OF ENDOCRINE DISEASE: Optimal feminizing hormone treatment in transgender people. European Journal of Endocrinology, 185(2), R49–R63. [DOI:10.1530/eje-21-0059]
Goldstein, Z., Khan, M., Reisman, T., & Safer, J. D. (2019). Managing the risk of venous thromboembolism in transgender adults undergoing hormone therapy. Journal of Blood Medicine, 10, 209–216. [DOI:10.2147/jbm.s166780]
Gooren, L. J., & T’Sjoen, G. (2018). Endocrine treatment of aging transgender people. Reviews in Endocrine and Metabolic Disorders, 19(3), 253–262. [DOI:10.1007/s11154-018-9449-0]
Gourdy, P., Bachelot, A., Catteau-Jonard, S., Chabbert-Buffet, N., Christin-Maître, S., Conard, J., Fredenrich, A., Gompel, A., Lamiche-Lorenzini, F., Moreau, C., Plu-Bureau, G., Vambergue, A., Vergès, B., & Kerlan, V. (2012). Hormonal contraception in women at risk of vascular and metabolic disorders: Guidelines of the French Society of Endocrinology. Annales d’Endocrinologie, 73(5), 469–487. [DOI:10.1016/j.ando.2012.09.001]
Grady, D., Wenger, N. K., Herrington, D., Khan, S., Furberg, C., Hunninghake, D., Vittinghoff, E., Hulley, S., & (2000). Postmenopausal Hormone Therapy Increases Risk for Venous Thromboembolic Disease: The Heart and Estrogen/progestin Replacement Study. Annals of Internal Medicine, 132(9), 689–696. [DOI:10.7326/0003-4819-132-9-200005020-00002]
Grandi, G., Facchinetti, F., & Bitzer, J. (2017). Estradiol in hormonal contraception: real evolution or just same old wine in a new bottle? The European Journal of Contraception & Reproductive Health Care, 22(4), 245–246. [DOI:10.1080/13625187.2017.1372571]
Grandi, G., Barra, F., Ferrero, S., & Facchinetti, F. (2019). Estradiol in non-oral hormonal contraception: a “long and winding road”. Expert Review of Endocrinology & Metabolism, 14(3), 153–155. [DOI:10.1080/17446651.2019.1604217]
Grandi, G., Del Savio, M. C., Lopes da Silva-Filho, A., & Facchinetti, F. (2020). Estetrol (E4): the new estrogenic component of combined oral contraceptives. Expert Review of Clinical Pharmacology, 13(4), 327–330. [DOI:10.1080/17512433.2020.1750365]
Grandi, G., Facchinetti, F., & Bitzer, J. (2022). Confirmation of the safety of combined oral contraceptives containing oestradiol on the risk of venous thromboembolism. The European Journal of Contraception & Reproductive Health Care, 27(2), 83–84. [DOI:10.1080/13625187.2022.2029397]
Grossmann, M., Wierman, M. E., Angus, P., & Handelsman, D. J. (2018). Reproductive Endocrinology of Nonalcoholic Fatty Liver Disease. Endocrine Reviews, 40(2), 417–446. [DOI:10.1210/er.2018-00158]
Hammond, G. L. (2017). Sex Hormone-Binding Globulin and the Metabolic Syndrome. In Winters, S. J., & Huhtaniemi, I. T. (Eds.). Male Hypogonadism: Basic, Clinical and Therapeutic Principles, 2nd Edition (pp. 305–324). Cham: Springer. [DOI:10.1007/978-3-319-53298-1_15]
Hannaford, P. C., Iversen, L., Macfarlane, T. V., Elliott, A. M., Angus, V., & Lee, A. J. (2010). Mortality among contraceptive pill users: cohort evidence from Royal College of General Practitioners’ Oral Contraception Study. BMJ, 340, c927. [DOI:10.1136/bmj.c927]
Haupt, C., Henke, M., Kutschmar, A., Hauser, B., Baldinger, S., Saenz, S. R., & Schreiber, G. (2020). Antiandrogen or estradiol treatment or both during hormone therapy in transitioning transgender women. Cochrane Database of Systematic Reviews, 2020(11), CD013138. [DOI:10.1002/14651858.cd013138.pub2]
Haveles, C. S., Wang, M. M., Arjun, A., Zaila, K. E., & Lee, J. C. (2020). Effect of Cross-Sex Hormone Therapy on Venous Thromboembolism Risk in Male-to-Female Gender-Affirming Surgery. Annals of Plastic Surgery, 86(1), 109–114. [DOI:10.1097/sap.0000000000002300]
Hedlund, P. O., Johansson, R., Damber, J. E., Hagerman, I., Henriksson, P., Iversen, P., Klarskov, P., Mogensen, P., Rasmussen, F., & Varenhorst, E. (2011). Significance of pretreatment cardiovascular morbidity as a risk factor during treatment with parenteral oestrogen or combined androgen deprivation of 915 patients with metastasized prostate cancer: Evaluation of cardiovascular events in a randomized trial. Scandinavian Journal of Urology and Nephrology, 45(5), 346–353. [DOI:10.3109/00365599.2011.585820]
Heit, J. A., Silverstein, M. D., Mohr, D. N., Petterson, T. M., O’Fallon, W. M., & Melton, L. J. (2000). Risk Factors for Deep Vein Thrombosis and Pulmonary Embolism. Archives of Internal Medicine, 160(6), 809–815. [DOI:10.1001/archinte.160.6.809]
Heit, J. A., Spencer, F. A., & White, R. H. (2016). The epidemiology of venous thromboembolism. Journal of Thrombosis and Thrombolysis, 41(1), 3–14. [DOI:10.1007/s11239-015-1311-6]
Hembree, W. C., Cohen-Kettenis, P. T., Gooren, L., Hannema, S. E., Meyer, W. J., Murad, M. H., Rosenthal, S. M., Safer, J. D., Tangpricha, V., & T’Sjoen, G. G. (2017). Endocrine Treatment of Gender-Dysphoric/Gender-Incongruent Persons: An Endocrine Society* Clinical Practice Guideline. The Journal of Clinical Endocrinology & Metabolism, 102(11), 3869–3903. [DOI:10.1210/jc.2017-01658]
Hemelaar, M., van der Mooren, M. J., Rad, M., Kluft, C., & Kenemans, P. (2008). Effects of non-oral postmenopausal hormone therapy on markers of cardiovascular risk: a systematic review. Fertility and Sterility, 90(3), 642–672. [DOI:10.1016/j.fertnstert.2007.07.1298]
Hibbs, D. (2008). Hormone replacement and the treatment of the transgender patient: A critical literature review. de Chesnay, M., & Anderson, B. (Eds.). Caring for the Vulnerable: Perspectives in Nursing Theory, Practice, and Research, 2nd Edition (pp. 351–362). Sudbury, Massachusetts: Jones & Barlett. [Google Scholar] [Google Books]
Higdon, J., Drake, V. J., Delage, B., & Crozier, A. (2016). Flavonoids. Corvallis, Oregon: Micronutrient Information Center, Linus Pauling Institute, Oregon State University. [URL]
Høibraaten, E., Qvigstad, E., Arnesen, H., Larsen, S., Wickstrøm, E., & Sandset, P. M. (2000). Increased Risk of Recurrent Venous Thromboembolism during Hormone Replacement Therapy. Thrombosis and Haemostasis, 84(12), 961–967. [DOI:10.1055/s-0037-1614156]
Høibraaten, E., Qvigstad, E., Andersen, T. O., Mowinckel, M., & Sandset, P. M. (2001). The Effects of Hormone Replacement Therapy (HRT) on Hemostatic Variables in Women with Previous Venous Thromboembolism – Results from a Randomized, Double-Blind, Clinical Trial. Thrombosis and Haemostasis, 85(5), 775–781. [DOI:10.1055/s-0037-1615717]
Holmegard, H., Nordestgaard, B., Schnohr, P., Tybjærg‐Hansen, A., & Benn, M. (2014). Endogenous sex hormones and risk of venous thromboembolism in women and men. Journal of Thrombosis and Haemostasis, 12(3), 297–305. [DOI:10.1111/jth.12484]
Hontscharuk, R., Alba, B., Manno, C., Pine, E., Deutsch, M. B., Coon, D., & Schechter, L. (2021). Perioperative Transgender Hormone Management: Avoiding Venous Thromboembolism and Other Complications. Plastic & Reconstructive Surgery, 147(4), 1008–1017. [DOI:10.1097/prs.0000000000007786]
Hugon-Rodin, J., Alhenc-Gelas, M., Hemker, H. C., Brailly-Tabard, S., Guiochon-Mantel, A., Plu-Bureau, G., & Scarabin, P. (2016). Sex hormone-binding globulin and thrombin generation in women using hormonal contraception. Biomarkers, 22(1), 81–85. [DOI:10.1080/1354750x.2016.1204010]
Hulley, S. (1998). Randomized Trial of Estrogen Plus Progestin for Secondary Prevention of Coronary Heart Disease in Postmenopausal Women. JAMA, 280(7), 605–613. [DOI:10.1001/jama.280.7.605]
Iqbal, J., Ginsburg, O. M., Wijeratne, T. D., Howell, A., Evans, G., Sestak, I., & Narod, S. A. (2012). Endometrial cancer and venous thromboembolism in women under age 50 who take tamoxifen for prevention of breast cancer: A systematic review. Cancer Treatment Reviews, 38(4), 318–328. [DOI:10.1016/j.ctrv.2011.06.009]
Irwig, M. S. (2018). Cardiovascular health in transgender people. Reviews in Endocrine and Metabolic Disorders, 19(3), 243–251. [DOI:10.1007/s11154-018-9454-3]
Iwamoto, S. J., Defreyne, J., Rothman, M. S., Van Schuylenbergh, J., Van de Bruaene, L., Motmans, J., & T’Sjoen, G. (2019). Health considerations for transgender women and remaining unknowns: a narrative review. Therapeutic Advances in Endocrinology and Metabolism, 10, 204201881987116. [DOI:10.1177/2042018819871166]
Jasuja, R., Passam, F. H., Kennedy, D. R., Kim, S. H., van Hessem, L., Lin, L., Bowley, S. R., Joshi, S. S., Dilks, J. R., Furie, B., Furie, B. C., & Flaumenhaft, R. (2012). Protein disulfide isomerase inhibitors constitute a new class of antithrombotic agents. Journal of Clinical Investigation, 122(6), 2104–2113. [DOI:10.1172/jci61228]
Jensen, E. V., Jacobson, H. I., Walf, A. A., & Frye, C. A. (2010). Estrogen action: A historic perspective on the implications of considering alternative approaches. Physiology & Behavior, 99(2), 151–162. [DOI:10.1016/j.physbeh.2009.08.013]
Kaemmle, L. M., Stadler, A., Janka, H., von Wolff, M., & Stute, P. (2022). The impact of micronized progesterone on cardiovascular events – a systematic review. Climacteric, 25(4), 327–336. [DOI:10.1080/13697137.2021.2022644]
Kasum, M., Danolić, D., Orešković, S., Ježek, D., Beketić-Orešković, L., & Pekez, M. (2014). Thrombosis following ovarian hyperstimulation syndrome. Gynecological Endocrinology, 30(11), 764–768. [DOI:10.3109/09513590.2014.927858]
Keenan, L., Kerr, T., Duane, M., & Van Gundy, K. (2018). Systematic Review of Hormonal Contraception and Risk of Venous Thrombosis. The Linacre Quarterly, 85(4), 470–477. [DOI:10.1177/0024363918816683]
Kerlan, V., Nahoul, K., Martelot, M., & Bercovici, J. (1994). Longitudinal study of maternal plasma bioavailable testosterone and androstanediol glucuronide levels during pregnancy. Clinical Endocrinology, 40(2), 263–267. [DOI:10.1111/j.1365-2265.1994.tb02478.x]
Khan, J., Schmidt, R. L., Spittal, M. J., Goldstein, Z., Smock, K. J., & Greene, D. N. (2019). Venous Thrombotic Risk in Transgender Women Undergoing Estrogen Therapy: A Systematic Review and Metaanalysis. Clinical Chemistry, 65(1), 57–66. [DOI:10.1373/clinchem.2018.288316]
Kitamura, T. (2001). Necessity of re‐evaluation of estramustine phosphate sodium (EMP) as a treatment option for first‐line monotherapy in advanced prostate cancer. International Journal of Urology, 8(2), 33–36. [DOI:10.1046/j.1442-2042.2001.00254.x]
Klil-Drori, A. J., Yin, H., Tagalakis, V., Aprikian, A., & Azoulay, L. (2016). Androgen Deprivation Therapy for Prostate Cancer and the Risk of Venous Thromboembolism. European Urology, 70(1), 56–61. [DOI:10.1016/j.eururo.2015.06.022]
Kohli, M., & McClellan, J. (2001). Parenteral Estrogen Therapy in Advanced Prostate Cancer: Retrospective Analysis of Intra-Muscular Estradiol Valerate in “Hormone Refractory” Prostate Disease. In Grunberg, S. M. (Ed.). Proceedings of the American Society of Clinical Oncology [Proc Am Soc Clin Oncol / Proceedings of ASCO], 20 [Thirty-Seventh Annual Meeting of the American Society of Clinical Oncology, May 12–15, 2001, San Francisco, California], 164b–164b (abstract no. 2407). Baltimore: Lippincott Williams & Wilkins. [ISSN:1081-0641] [ISBN-10:0-9664495-3-3] [Google Scholar] [WorldCat 1] [WorldCat 2] [WorldCat 3] [PDF]
Kohli, M., Alikhan, M. A., Spencer, H. J., & Carter, G. (2004). Phase I trial of intramuscular estradiol valerate (I/M-E) in hormone refractory prostate cancer. Journal of Clinical Oncology, 22(14 Suppl) [40th Annual Meeting of the American Society of Clinical Oncology: June 5–8, 2004, Ernest N. Morial Convention Center, New Orleans, Louisiana, Annual Meeting Proceedings], 436–436 (abstract no. 4726). [DOI:10.1200/jco.2004.22.90140.4726] [Google Books] [PDF]
Kohli, M. (2006). Phase II study of transdermal estradiol in androgen-independent prostate carcinoma. Cancer, 106(1), 234–235. [DOI:10.1002/cncr.21528]
Konkle, B. A., & Sood, S. L. (2019). Thrombotic Risk of Contraceptives and Other Hormonal Therapies. In Kitchens, C. S., Kessler, C. M., Konkle, B. A., Streiff, M. B., & Garcia, D. A. (Eds.). Consultative Hemostasis and Thrombosis, 4th Edition (pp. 637–650). Philadelphia: Elsevier. [DOI:10.1016/b978-0-323-46202-0.00031-5]
Kotamarti, V. S., Greige, N., Heiman, A. J., Patel, A., & Ricci, J. A. (2021). Risk for Venous Thromboembolism in Transgender Patients Undergoing Cross-Sex Hormone Treatment: A Systematic Review. The Journal of Sexual Medicine, 18(7), 1280–1291. [DOI:10.1016/j.jsxm.2021.04.006]
Kozato, A., Fox, G. W., Yong, P. C., Shin, S. J., Avanessian, B. K., Ting, J., Ling, Y., Karim, S., Safer, J. D., & Pang, J. H. (2021). No Venous Thromboembolism Increase Among Transgender Female Patients Remaining on Estrogen for Gender-Affirming Surgery. The Journal of Clinical Endocrinology & Metabolism, 106(4), 1586–1590. [DOI:10.1210/clinem/dgaa966]
Kronawitter, D., Gooren, L. J., Zollver, H., Oppelt, P. G., Beckmann, M. W., Dittrich, R., & Mueller, A. (2009). Effects of transdermal testosterone or oral dydrogesterone on hypoactive sexual desire disorder in transsexual women: results of a pilot study. European Journal of Endocrinology, 161(2), 363–368. [DOI:10.1530/eje-09-0265] [Table]
Kuhl, H. (1990). Ovulationshemmer: Die Bedeutung der Östrogendosis. [Ovulation Preventives: The Significance of the Estrogen Dose. / Ovulation Inhibitors: The Significance of Estrogen Dose.] Geburtshilfe und Frauenheilkunde, 50(12), 910–922. [Google Scholar 1] [Google Scholar 2] [PubMed] [DOI:10.1055/s-2008-1026392] [Translation]
Kuhl, H. (1996). Effects of progestogens on haemostasis. Maturitas, 24(1–2), 1–19. [DOI:10.1016/0378-5122(96)00994-2]
Kuhl, H. (1997). Metabolische Effekte der Östrogene und Gestagene. [Metabolic Effects of Estrogens and Progestogens.] Der Gynäkologe, 30(4), 357–369. [DOI:10.1007/pl00003042]
Kuhl, H. (1998). Adverse effects of estrogen treatment: natural vs. synthetic estrogens. In Lippert, T. H., Mueck, A. O., & Ginsburg, J. (Eds.). Sex Steroids and the Cardiovascular System: The Proceedings of the 1st Interdisciplinary Workshop, Tuebingen, Germany, October 1996. Parthenon Publishing Group, New York, London (pp. 201–210). London/New York: Parthenon. [Google Scholar] [Google Books] [PDF]
Kuhl, H. (1999). Hormonal contraception. In Oettel, M., & Schillinger, E. (Eds.). Estrogens and Antiestrogens II: Pharmacology and Clinical Application of Estrogens and Antiestrogen (Handbook of Experimental Pharmacology, Volume 135, Part 2) (pp. 363–407). Berlin/Heidelberg: Springer. [DOI:10.1007/978-3-642-60107-1_18] [PDF]
Kuhl, H. (2005). Pharmacology of Estrogens and Progestogens: Influence of Different Routes of Administration. Climacteric, 8(Suppl 1), 3–63. [DOI:10.1080/13697130500148875] [PDF]
Kuhl, H., & Stevenson, J. (2006). The effect of medroxyprogesterone acetate on estrogen-dependent risks and benefits – an attempt to interpret the Women’s Health Initiative results. Gynecological Endocrinology, 22(6), 303–317. [DOI:10.1080/09513590600717368]
Langley, R. E., Cafferty, F. H., Alhasso, A. A., Rosen, S. D., Sundaram, S. K., Freeman, S. C., Pollock, P., Jinks, R. C., Godsland, I. F., Kockelbergh, R., Clarke, N. W., Kynaston, H. G., Parmar, M. K., & Abel, P. D. (2013). Cardiovascular outcomes in patients with locally advanced and metastatic prostate cancer treated with luteinising-hormone-releasing-hormone agonists or transdermal oestrogen: the randomised, phase 2 MRC PATCH trial (PR09). The Lancet Oncology, 14(4), 306–316. [DOI:10.1016/s1470-2045(13)70025-1]
Langley, R. E., Gilbert, D. C., Duong, T., Clarke, N. W., Nankivell, M., Rosen, S. D., Mangar, S., Macnair, A., Sundaram, S. K., Laniado, M. E., Dixit, S., Madaan, S., Manetta, C., Pope, A., Scrase, C. D., Mckay, S., Muazzam, I. A., Collins, G. N., Worlding, J., Williams, S. T., Paez, E., Robinson, A., McFarlane, J., Deighan, J. V., Marshall, J., Forcat, S., Weiss, M., Kockelbergh, R., Alhasso, A., Kynaston, H., & Parmar, M. (2021). Transdermal oestradiol for androgen suppression in prostate cancer: long-term cardiovascular outcomes from the randomised Prostate Adenocarcinoma Transcutaneous Hormone (PATCH) trial programme. The Lancet, 397(10274), 581–591. [DOI:10.1016/s0140-6736(21)00100-8] [PDF] [Supplementary appendix]
Lax, E. (1987). Mechanisms of physiological and pharmacological sex hormone action on the mammalian liver. Journal of Steroid Biochemistry, 27(4–6), 1119–1128. [DOI:10.1016/0022-4731(87)90198-1]
Lidegaard, Ø. (2014). Hormonal contraception, thrombosis and age. Expert Opinion on Drug Safety, 13(10), 1353–1360. [DOI:10.1517/14740338.2014.950654]
Lijfering, W. M., Rosendaal, F. R., & Cannegieter, S. C. (2010). Risk factors for venous thrombosis - current understanding from an epidemiological point of view. British Journal of Haematology, 149(6), 824–833. [DOI:10.1111/j.1365-2141.2010.08206.x]
Lim, H. Y., Leemaqz, S. Y., Torkamani, N., Grossmann, M., Zajac, J. D., Nandurkar, H., Ho, P., & Cheung, A. S. (2020). Global Coagulation Assays in Transgender Women on Oral and Transdermal Estradiol Therapy. The Journal of Clinical Endocrinology & Metabolism, 105(7), e2369–e2377. [DOI:10.1210/clinem/dgaa262]
Luria, M. H. (1989). Estrogen and coronary arterial disease in men. International Journal of Cardiology, 25(2), 159–166. [DOI:10.1016/0167-5273(89)90102-2]
Ma, Y., Zeng, M., Sun, R., & Hu, M. (2015). Disposition of Flavonoids Impacts their Efficacy and Safety. Current Drug Metabolism, 15(9), 841–864. [DOI:10.2174/1389200216666150206123719]
Machin, N., & Ragni, M. V. (2020). Hormones and thrombosis: risk across the reproductive years and beyond. Translational Research, 225, 9–19. [DOI:10.1016/j.trsl.2020.06.011]
Mammen, E. F. (1992). Coagulation Abnormalities in Liver Disease. Hematology/Oncology Clinics of North America, 6(6), 1247–1257. [DOI:10.1016/s0889-8588(18)30273-9]
Mantha, S., Karp, R., Raghavan, V., Terrin, N., Bauer, K. A., & Zwicker, J. I. (2012). Assessing the risk of venous thromboembolic events in women taking progestin-only contraception: a meta-analysis. BMJ, 345, e4944. [DOI:10.1136/bmj.e4944]
Martinelli, I., Passamonti, S. M., & Bucciarelli, P. (2014). Thrombophilic states. In Biller, J., & Ferro, J. M. (Eds.). Neurologic Aspects of Systemic Disease Part II (Handbook of Clinical Neurology, Volume 120) (pp. 1061–1071). Philadelphia: Elsevier. [DOI:10.1016/b978-0-7020-4087-0.00071-1]
Martinez-Zapata, M. J., Vernooij, R. W., Uriona Tuma, S. M., Stein, A. T., Moreno, R. M., Vargas, E., Capellà, D., & Bonfill Cosp, X. (2016). Phlebotonics for venous insufficiency. Cochrane Database of Systematic Reviews, 2016(4), CD003229. [DOI:10.1002/14651858.cd003229.pub3]
Matharu, G. S., Kunutsor, S. K., Judge, A., Blom, A. W., & Whitehouse, M. R. (2020). Clinical Effectiveness and Safety of Aspirin for Venous Thromboembolism Prophylaxis After Total Hip and Knee Replacement. JAMA Internal Medicine, 180(3), 376–384. [DOI:10.1001/jamainternmed.2019.6108]
McLintock, C. (2014). Thromboembolism in pregnancy: Challenges and controversies in the prevention of pregnancy-associated venous thromboembolism and management of anticoagulation in women with mechanical prosthetic heart valves. Best Practice & Research Clinical Obstetrics & Gynaecology, 28(4), 519–536. [DOI:10.1016/j.bpobgyn.2014.03.001]
Mekaj, A., Mekaj, Y., & Daci, F. (2015). New insights into the mechanisms of action of aspirin and its use in the prevention and treatment of arterial and venous thromboembolism. Therapeutics and Clinical Risk Management, 11, 1449–1456. [DOI:10.2147/tcrm.s92222]
Mellinger, G. T., Bailar, J. C., Arduino, L. J., & the Veterans Administration Cooperative Urological Research Group. (1967). Treatment and survival of patients with cancer of the prostate. The Veterans Administration Co-operative Urological Research Group. Surgery Gynecology & Obstetrics, 124(5), 1011–1017. [Google Scholar] [PubMed]
Meng, Y., Jiang, H., Chen, A., Lu, F., Yang, H., Shen, M. Z., Sun, D., Shao, Q., & Fotherby, K. (1990). Hemostatic changes in women using a monthly injectable contraceptive for one year. Contraception, 42(4), 455–466. [DOI:10.1016/0010-7824(90)90052-w]
Mikkola, A., Ruutu, M., Aro, J., Rannikko, S., & Salo, J. (1999). The role of parenteral polyestradiol phosphate in the treatment of advanced prostatic cancer on the threshold of the new millennium. Annales Chirurgiae et Gynaecologiae, 88(1), 18–21. [Google Scholar] [PubMed] [PDF]
Min, L. L., & Hopkins, R. (2021). Endocrinological Care for Patients Undergoing Gender Affirmation (Including Risk of Thromboembolic Events). In Nikolavsky, D., & Blakely, S. A. (Eds.). Urological Care for the Transgender Patient: A Comprehensive Guide (pp. 23–36). Cham: Springer. [DOI:10.1007/978-3-030-18533-6_3]
Mohammed, K., Abu Dabrh, A. M., Benkhadra, K., Al Nofal, A., Carranza Leon, B. G., Prokop, L. J., Montori, V. M., Faubion, S. S., & Murad, M. H. (2015). Oral vs Transdermal Estrogen Therapy and Vascular Events: A Systematic Review and Meta-Analysis. The Journal of Clinical Endocrinology & Metabolism, 100(11), 4012–4020. [DOI:10.1210/jc.2015-2237]
Montagnana, M., Favaloro, E. J., Franchini, M., Guidi, G. C., & Lippi, G. (2009). The role of ethnicity, age and gender in venous thromboembolism. Journal of Thrombosis and Thrombolysis, 29(4), 489–496. [DOI:10.1007/s11239-009-0365-8]
Moores, L., Bilello, K. L., & Murin, S. (2004). Sex and gender issues and venous thromboembolism. Clinics in Chest Medicine, 25(2), 281–297. [DOI:10.1016/j.ccm.2004.01.013]
Morimont, L., Dogné, J., & Douxfils, J. (2020). Letter to the Editors-in-Chief in response to the article of Abou-Ismail, et al. entitled “Estrogen and thrombosis: A bench to bedside review” (Thrombosis Research 192 (2020) 40–51). Thrombosis Research, 193, 221–223. [DOI:10.1016/j.thromres.2020.08.006]
Morimont, L., Haguet, H., Dogné, J., Gaspard, U., & Douxfils, J. (2021). Combined Oral Contraceptives and Venous Thromboembolism: Review and Perspective to Mitigate the Risk. Frontiers in Endocrinology, 12, 769187. [DOI:10.3389/fendo.2021.769187]
Morling, J. R., Broderick, C., Yeoh, S. E., & Kolbach, D. N. (2018). Rutosides for treatment of post-thrombotic syndrome. Cochrane Database of Systematic Reviews, 2018(11), CD005625. [DOI:10.1002/14651858.cd005625.pub4]
Mueller, A., Dittrich, R., Binder, H., Kuehnel, W., Maltaris, T., Hoffmann, I., & Beckmann, M. W. (2005). High dose estrogen treatment increases bone mineral density in male-to-female transsexuals receiving gonadotropin-releasing hormone agonist in the absence of testosterone. European Journal of Endocrinology, 153(1), 107–113. [DOI:10.1530/eje.1.01943]
Mueller, A., Binder, H., Cupisti, S., Hoffmann, I., Beckmann, M., & Dittrich, R. (2006). Effects on the Male Endocrine System of Long-term Treatment with Gonadotropin-releasing Hormone Agonists and Estrogens in Male-to-Female Transsexuals. Hormone and Metabolic Research, 38(3), 183–187. [DOI:10.1055/s-2006-925198]
Mueller, A., Zollver, H., Kronawitter, D., Oppelt, P. G., Claassen, T., Hoffmann, I., Beckmann, M. W., & Dittrich, R. (2011). Body composition and bone mineral density in male-to-female transsexuals during cross-sex hormone therapy using gonadotrophin-releasing hormone agonist. Experimental and Clinical Endocrinology & Diabetes, 119(2), 95–100. [DOI:10.1055/s-0030-1255074] [Table]
Nachtigall, L. E., Raju, U., Banerjee, S., Wan, L., & Levitz, M. (2000). Serum Estradiol-Binding Profiles in Postmenopausal Women Undergoing Three Common Estrogen Replacement Therapies. Menopause, 7(4), 243–250. [DOI:10.1097/00042192-200007040-00006]
Nelson, M. D., Szczepaniak, L. S., Wei, J., Szczepaniak, E., Sánchez, F. J., Vilain, E., Stern, J. H., Bergman, R. N., Bairey Merz, C. N., & Clegg, D. J. (2016). Transwomen and the Metabolic Syndrome: Is Orchiectomy Protective? Transgender Health, 1(1), 165–171. [DOI:10.1089/trgh.2016.0016]
Nolan, B. J., & Cheung, A. S. (2020). Estradiol Therapy in the Perioperative Period: Implications for Transgender People Undergoing Feminizing Hormone Therapy. The Yale Journal of Biology and Medicine, 93(4), 539–548. [PubMed] [PubMed Central]
Nolan, B. J., & Cheung, A. S. (2021). Relationship Between Serum Estradiol Concentrations and Clinical Outcomes in Transgender Individuals Undergoing Feminizing Hormone Therapy: A Narrative Review. Transgender Health, 6(3), 125–131. [DOI:10.1089/trgh.2020.0077]
Nolan, I. T., Haley, C., Morrison, S. D., Pannucci, C. J., & Satterwhite, T. (2021). Estrogen Continuation and Venous Thromboembolism in Penile Inversion Vaginoplasty. The Journal of Sexual Medicine, 18(1), 193–200. [DOI:10.1016/j.jsxm.2020.10.018]
Ockrim, J., & Abel, P. D. (2009). Androgen deprivation therapy for prostate cancer – the potential of parenteral estrogen. Central European Journal of Urology, 62, 132–140. [DOI:10.5173/ceju.2009.03.art1]
Odlind, V., Milsom, I., Persson, I., & Victor, A. (2002). Can changes in sex hormone binding globulin predict the risk of venous thromboembolism with combined oral contraceptive pills?: A discussion based on recent recommendations from the European agency for evaluation of medicinal products regarding third generation oral contraceptive pills. Acta Obstetricia et Gynecologica Scandinavica, 81(6), 482–490. [DOI:10.1080/j.1600-0412.2002.810603.x] [URL]
Oger, E., & (2000). Incidence of Venous Thromboembolism: A Community-based Study in Western France. Thrombosis and Haemostasis, 83(5), 657–660. [DOI:10.1055/s-0037-1613887]
Ohlander, S. J., Varghese, B., & Pastuszak, A. W. (2018). Erythrocytosis Following Testosterone Therapy. Sexual Medicine Reviews, 6(1), 77–85. [DOI:10.1016/j.sxmr.2017.04.001]
Olié, V., Canonico, M., & Scarabin, P. (2010). Risk of venous thrombosis with oral versus transdermal estrogen therapy among postmenopausal women. Current Opinion in Hematology, 17(5), 457–463. [DOI:10.1097/moh.0b013e32833c07bc]
Olié, V., Plu-Bureau, G., Conard, J., Horellou, M., Canonico, M., & Scarabin, P. (2011). Hormone therapy and recurrence of venous thromboembolism among postmenopausal women. Menopause, 18(5), 488–493. [DOI:10.1097/gme.0b013e3181f9f7c3]
Oliver-Williams, C., Glisic, M., Shahzad, S., Brown, E., Pellegrino Baena, C., Chadni, M., Chowdhury, R., Franco, O. H., & Muka, T. (2018). The route of administration, timing, duration and dose of postmenopausal hormone therapy and cardiovascular outcomes in women: a systematic review. Human Reproduction Update, 25(2), 257–271. [DOI:10.1093/humupd/dmy039]
Olov Hedlund, P., Damber, J., Hagerman, I., Haukaas, S., Henriksson, P., Iversen, P., Johansson, R., Klarskov, P., Lundbeck, F., Rasmussen, F., Varenhorst, E., Viitanen, J., Olov Hedlund, P., Damber, J., Hagerman, I., Haukaas, S., Henriksson, P., Iversen, P., Johansson, R., Klarskov, P., Lundbeck, F., Rasmussen, F., Varenhorst, E., Viitanen, J., & The SPCG-5 Study Group. (2008). Parenteral estrogen versus combined androgen deprivation in the treatment of metastatic prostatic cancer: Part 2. Final evaluation of the Scandinavian Prostatic Cancer Group (SPCG) Study No. 5. Scandinavian Journal of Urology and Nephrology, 42(3), 220–229. [DOI:10.1080/00365590801943274]
Park, W. (2002). Selective estrogen receptor modulators (SERMS) and their roles in breast cancer prevention. Trends in Molecular Medicine, 8(2), 82–88. [DOI:10.1016/s1471-4914(02)02282-7]
Patel, K. T., Adeel, S., Rodrigues Miragaya, J., & Tangpricha, V. (2022). Progestogen Use in Gender-Affirming Hormone Therapy: A Systematic Review. Endocrine Practice, 28(12), 1244–1252. [DOI:10.1016/j.eprac.2022.08.012]
Peck-Radosavljevic, M. (2007). Review article: coagulation disorders in chronic liver disease. Alimentary Pharmacology & Therapeutics, 26, 21–28. [DOI:10.1111/j.1365-2036.2007.03509.x]
Pfeifer, S., Butts, S., Dumesic, D., Fossum, G., Gracia, C., La Barbera, A., Mersereau, J., Odem, R., Penzias, A., Pisarska, M., Rebar, R., Reindollar, R., Rosen, M., Sandlow, J., Sokol, R., Vernon, M., & Widra, E. (2017). Combined hormonal contraception and the risk of venous thromboembolism: a guideline. Fertility and Sterility, 107(1), 43–51. [DOI:10.1016/j.fertnstert.2016.09.027]
Phillips, I., Shah, S. I., Duong, T., Abel, P., & Langley, R. E. (2014). Androgen Deprivation Therapy and the Re-emergence of Parenteral Estrogen in Prostate Cancer. Oncology & Hematology Review, 10(1), 42–47. [PubMed Central] [DOI:10.17925/ohr.2014.10.1.42]
Plu-Bureau, G., Maitrot-Mantelet, L., Hugon-Rodin, J., & Canonico, M. (2013). Hormonal contraceptives and venous thromboembolism: An epidemiological update. Best Practice & Research Clinical Endocrinology & Metabolism, 27(1), 25–34. [DOI:10.1016/j.beem.2012.11.002]
Pomp, E. R., Rosendaal, F. R., & Doggen, C. J. (2008). Smoking increases the risk of venous thrombosis and acts synergistically with oral contraceptive use. American Journal of Hematology, 83(2), 97–102. [DOI:10.1002/ajh.21059]
Pond, S. M., & Tozer, T. N. (1984). First-Pass Elimination. Clinical Pharmacokinetics, 9(1), 1–25. [DOI:10.2165/00003088-198409010-00001]
Prentice, R. L., & Anderson, G. L. (2008). The Women’s Health Initiative: Lessons Learned. Annual Review of Public Health, 29(1), 131–150. [DOI:10.1146/annurev.publhealth.29.020907.090947]
Prentice, R. (2014). Postmenopausal Hormone Therapy and the Risks of Coronary Heart Disease, Breast Cancer, and Stroke. Seminars in Reproductive Medicine, 32(6), 419–425. [DOI:10.1055/s-0034-1384624]
Pyra, M., Casimiro, I., Rusie, L., Ross, N., Blum, C., Keglovitz Baker, K., Baker, A., & Schneider, J. (2020). An Observational Study of Hypertension and Thromboembolism Among Transgender Patients Using Gender-Affirming Hormone Therapy. Transgender Health, 5(1), 1–9. [DOI:10.1089/trgh.2019.0061]
Quinton, R., & Swee, D. S. (2019). Hormone replacement therapy: transgender studies show safety of estradiol. BMJ, 364, l600. [DOI:10.1136/bmj.l600]
Rabe, T., Luxembourg, B., Ludwig, M., Dinger, J. C., Bauersachs, R., Rott, H., Mueck, A. O., & Albring, C. (2011). Contraception and Thrombophilia - A statement from the German Society of Gynecological Endocrinology and Reproductive Medicine (DGGEF e. V.) and the Professional Association of the German Gynaecologists (BVF e. V.). Journal für Reproduktionsmedizin und Endokrinologie-Journal of Reproductive Medicine and Endocrinology, 8(Special Issue 1), 178–218. [URL]
Raps, M., Helmerhorst, F., Fleischer, K., Thomassen, S., Rosendaal, F., Rosing, J., Ballieux, B., & Van Vliet, H. (2012). Sex hormone‐binding globulin as a marker for the thrombotic risk of hormonal contraceptives. Journal of Thrombosis and Haemostasis, 10(6), 992–997. [DOI:10.1111/j.1538-7836.2012.04720.x]
Ravery, V., Fizazi, K., Oudard, S., Drouet, L., Eymard, J., Culine, S., Gravis, G., Hennequin, C., & Zerbib, M. (2011). The use of estramustine phosphate in the modern management of advanced prostate cancer. BJU International, 108(11), 1782–1786. [DOI:10.1111/j.1464-410x.2011.10201.x]
Reda, S., Morimont, L., Douxfils, J., & Rühl, H. (2020). Can We Measure the Individual Prothrombotic or Prohemorrhagic Tendency by Global Coagulation Tests? Hämostaseologie, 40(3), 364–378. [DOI:10.1055/a-1153-5824]
Renoux, C., Dell’Aniello, S., & Suissa, S. (2010). Hormone replacement therapy and the risk of venous thromboembolism: a population-based study. Journal of Thrombosis and Haemostasis, 8(5), 979–986. [DOI:10.1111/j.1538-7836.2010.03839.x]
Renoux, C., Dell’Aniello, S., Garbe, E., & Suissa, S. (2010). Transdermal and oral hormone replacement therapy and the risk of stroke: a nested case-control study. BMJ, 340, c2519. [DOI:10.1136/bmj.c2519]
Roach, R., Lijfering, W., Helmerhorst, F., Cannegieter, S., Rosendaal, F., & van Hylckama Vlieg, A. (2013). The risk of venous thrombosis in women over 50 years old using oral contraception or postmenopausal hormone therapy. Journal of Thrombosis and Haemostasis, 11(1), 124–131. [DOI:10.1111/jth.12060]
Roach, R. E., Lijfering, W. M., Rosendaal, F. R., Cannegieter, S. C., & le Cessie, S. (2014). Sex Difference in Risk of Second but Not of First Venous Thrombosis. Circulation, 129(1), 51–56. [DOI:10.1161/circulationaha.113.004768]
Rooijen, M., Silveira, A., Hamsten, A., & Bremme, K. (2004). Sex hormone–binding globulin—A surrogate marker for the prothrombotic effects of combined oral contraceptives. American Journal of Obstetrics and Gynecology, 190(2), 332–337. [DOI:10.1016/s0002-9378(03)00950-5]
Ropponen, A., Aittomäki, K., Vihma, V., Tikkanen, M. J., & Ylikorkala, O. (2005). Effects of Oral and Transdermal Estradiol Administration on Levels of Sex Hormone-Binding Globulin in Postmenopausal Women with and without a History of Intrahepatic Cholestasis of Pregnancy. The Journal of Clinical Endocrinology & Metabolism, 90(6), 3431–3434. [DOI:10.1210/jc.2005-0352]
Rosendaal, F. R. (2005). Venous thrombosis: the role of genes, environment, and behavior. Hematology American Society of Hematology Education Program, 2005(1), 1–12. [Google Scholar] [DOI:10.1182/asheducation-2005.1.1] [URL]
Rosendaal, F. R. (2016). Causes of venous thrombosis. Thrombosis Journal, 14(Suppl 1) [State of the Art 2016: Research and Review from the 9th Congress of the Asian-Pacific Society on Thrombosis and Hemostasis], 24. [DOI:10.1186/s12959-016-0108-y]
Rott, H. (2019). Birth Control Pills and Thrombotic Risks: Differences of Contraception Methods with and without Estrogen. Hämostaseologie, 39(1), 42–48. [DOI:10.1055/s-0039-1677806]
Rova, K., Passmark, H., & Lindqvist, P. G. (2012). Venous thromboembolism in relation to in vitro fertilization: an approach to determining the incidence and increase in risk in successful cycles. Fertility and Sterility, 97(1), 95–100. [DOI:10.1016/j.fertnstert.2011.10.038]
Rovinski, D., Ramos, R. B., Fighera, T. M., Casanova, G. K., & Spritzer, P. M. (2018). Risk of venous thromboembolism events in postmenopausal women using oral versus non-oral hormone therapy: A systematic review and meta-analysis. Thrombosis Research, 168, 83–95. [DOI:10.1016/j.thromres.2018.06.014]
Ruiz Garcia, V., López-Briz, E., Carbonell Sanchis, R., Gonzalvez Perales, J. L., & Bort-Martí, S. (2013). Megestrol acetate for treatment of anorexia-cachexia syndrome. Cochrane Database of Systematic Reviews, 2019(3), CD004310. [DOI:10.1002/14651858.cd004310.pub3]
Russell, N., Cheung, A., & Grossmann, M. (2017). Estradiol for the mitigation of adverse effects of androgen deprivation therapy. Endocrine-Related Cancer, 24(8), R297–R313. [DOI:10.1530/erc-17-0153]
Sahlin, L., & Schoultz, B. V. (1999). Liver Inclusive Protein, Lipid and Carbohydrate Metabolism. In Oettel, M., & Schillinger, E. (Eds.). Estrogens and Antiestrogens II: Pharmacology and Clinical Application of Estrogens and Antiestrogen (Handbook of Experimental Pharmacology, Volume 135, Part 2) (pp. 163–178). Berlin/Heidelberg: Springer. [DOI:10.1007/978-3-642-60107-1_8] [PDF]
Scarabin, P. (2018). Progestogens and venous thromboembolism in menopausal women: an updated oral versus transdermal estrogen meta-analysis. Climacteric, 21(4), 341–345. [DOI:10.1080/13697137.2018.1446931]
Scarabin, P., Canonico, M., Plu-Bureau, G., & Oger, E. (2020). Menopause and hormone therapy in the 21st century: why promote transdermal estradiol and progesterone? Heart, 106(16), 1278–1278. [DOI:10.1136/heartjnl-2020-316907]
Scheres, L. J., van Hylckama Vlieg, A., Ballieux, B. E., Fauser, B. C., Rosendaal, F. R., Middeldorp, S., & Cannegieter, S. C. (2019). Endogenous sex hormones and risk of venous thromboembolism in young women. Journal of Thrombosis and Haemostasis, 17(8), 1297–1304. [DOI:10.1111/jth.14474]
Scheres, L. J., Selier, N. L., Nota, N. M., van Diemen, J. J., Cannegieter, S. C., & den Heijer, M. (2021). Effect of gender‐affirming hormone use on coagulation profiles in transmen and transwomen. Journal of Thrombosis and Haemostasis, 19(4), 1029–1037. [DOI:10.1111/jth.15256]
Schindler, A. E. (2003). Differential effects of progestins on hemostasis. Maturitas, 46, 31–37. [DOI:10.1016/j.maturitas.2003.09.016]
Schock, H., Zeleniuch-Jacquotte, A., Lundin, E., Grankvist, K., Lakso, H., Idahl, A., Lehtinen, M., Surcel, H., & Fortner, R. T. (2016). Hormone concentrations throughout uncomplicated pregnancies: a longitudinal study. BMC Pregnancy and Childbirth, 16(1), 146. [DOI:10.1186/s12884-016-0937-5]
Schröder, F. H., & Radlmaier, A. (2002). Steroidal Antiandrogens. In Jordan, C. V., & Furr, B. J. A. (Eds.). Hormone Therapy in Breast and Prostate Cancer (pp. 325–346). Totowa, New Jersey: Humana Press. [DOI:10.1007/978-1-59259-152-7_15]
Sciarra, A., Gentile, V., Cattarino, S., Gentilucci, A., Alfarone, A., D’Eramo, G., & Salciccia, S. (2014). Oral ethinylestradiol in castration-resistant prostate cancer: A 10-year experience. International Journal of Urology, 22(1), 98–103. [DOI:10.1111/iju.12613]
Seaman, H. E., Langley, S. E., Farmer, R. D., & de Vries, C. S. (2007). Venous thromboembolism and cyproterone acetate in men with prostate cancer: a study using the General Practice Research Database. BJU International, 99(6), 1398–1403. [DOI:10.1111/j.1464-410x.2007.06859.x]
Shatzel, J. J., Connelly, K. J., & DeLoughery, T. G. (2017). Thrombotic issues in transgender medicine: A review. American Journal of Hematology, 92(2), 204–208. [DOI:10.1002/ajh.24593]
Shifren, J. L., Rifai, N., Desindes, S., McIlwain, M., Doros, G., & Mazer, N. A. (2008). A Comparison of the Short-Term Effects of Oral Conjugated Equine Estrogens Versus Transdermal Estradiol on C-Reactive Protein, Other Serum Markers of Inflammation, and Other Hepatic Proteins in Naturally Menopausal Women. The Journal of Clinical Endocrinology & Metabolism, 93(5), 1702–1710. [DOI:10.1210/jc.2007-2193]
Simon, T., De Jonage-Canonico, M. B., Oger, E., Wahl, D., Conard, J., Meyer, G., Emmerich, J., Barrellier, M., Guiraud, A., & Scarabin, P. (2006). Indicators of lifetime endogenous estrogen exposure and risk of venous thromboembolism. Journal of Thrombosis and Haemostasis, 4(1), 71–76. [DOI:10.1111/j.1538-7836.2005.01693.x]
Singla, N., Ghandour, R. A., & Raj, G. V. (2019). Investigational luteinizing hormone releasing hormone (LHRH) agonists and other hormonal agents in early stage clinical trials for prostate cancer. Expert Opinion on Investigational Drugs, 28(3), 249–259. [DOI:10.1080/13543784.2019.1570130]
Sitruk-Ware, R., & Nath, A. (2011). Metabolic effects of contraceptive steroids. Reviews in Endocrine and Metabolic Disorders, 12(2), 63–75. [DOI:10.1007/s11154-011-9182-4]
Sitruk-Ware, R., & Nath, A. (2013). Characteristics and metabolic effects of estrogen and progestins contained in oral contraceptive pills. Best Practice & Research Clinical Endocrinology & Metabolism, 27(1), 13–24. [DOI:10.1016/j.beem.2012.09.004]
Skouby, S. O., & Sidelmann, J. J. (2018). Impact of progestogens on hemostasis. Hormone Molecular Biology and Clinical Investigation, 37(2), 20180041. [DOI:10.1515/hmbci-2018-0041]
Smith, K., Galazi, M., Openshaw, M. R., Wilson, P., Sarker, S. J., O’Brien, N., Alifrangis, C., Stebbing, J., & Shamash, J. (2020). The Use of Transdermal Estrogen in Castrate-resistant, Steroid-refractory Prostate Cancer. Clinical Genitourinary Cancer, 18(3), e217–e223. [DOI:10.1016/j.clgc.2019.09.019]
Smith, N. L. (2004). Esterified Estrogens and Conjugated Equine Estrogens and the Risk of Venous Thrombosis. JAMA, 292(13), 1581–1587. [DOI:10.1001/jama.292.13.1581]
Smith, N. L., Blondon, M., Wiggins, K. L., Harrington, L. B., van Hylckama Vlieg, A., Floyd, J. S., Hwang, M., Bis, J. C., McKnight, B., Rice, K. M., Lumley, T., Rosendaal, F. R., Heckbert, S. R., & Psaty, B. M. (2014). Lower Risk of Cardiovascular Events in Postmenopausal Women Taking Oral Estradiol Compared With Oral Conjugated Equine Estrogens. JAMA Internal Medicine, 174(1), 25–34. [DOI:10.1001/jamainternmed.2013.11074]
Speroff, L. (1996). The Comparative Effect on Bone Density, Endometrium, and Lipids of Continuous Hormones as Replacement Therapy (CHART Study). JAMA, 276(17), 1397–1403. [DOI:10.1001/jama.1996.03540170041030]
Stanczyk, F. Z., Archer, D. F., & Bhavnani, B. R. (2013). Ethinyl estradiol and 17β-estradiol in combined oral contraceptives: pharmacokinetics, pharmacodynamics and risk assessment. Contraception, 87(6), 706–727. [DOI:10.1016/j.contraception.2012.12.011]
Stanczyk, F. Z., Mathews, B. W., & Cortessis, V. K. (2017). Does the type of progestin influence the production of clotting factors? Contraception, 95(2), 113–116. [DOI:10.1016/j.contraception.2016.07.007]
Stege, R., Carlström, K., Collste, L., Eriksson, A., Henriksson, P., & Pousette, A. (1988). Single drug polyestradiol phosphate therapy in prostatic cancer. American Journal of Clinical Oncology, 11(Suppl 2), S101–S103. [DOI:10.1097/00000421-198801102-00024] [PDF]
Stegeman, B., Raps, M., Helmerhorst, F., Vos, H., van Vliet, H., Rosendaal, F., & van Hylckama Vlieg, A. (2013). Effect of ethinylestradiol dose and progestagen in combined oral contraceptives on plasma sex hormone‐binding globulin levels in premenopausal women. Journal of Thrombosis and Haemostasis, 11(1), 203–205. [DOI:10.1111/jth.12054]
Stuenkel, C. A., Davis, S. R., Gompel, A., Lumsden, M. A., Murad, M. H., Pinkerton, J. V., & Santen, R. J. (2015). Treatment of Symptoms of the Menopause: An Endocrine Society Clinical Practice Guideline. The Journal of Clinical Endocrinology & Metabolism, 100(11), 3975–4011. [DOI:10.1210/jc.2015-2236]
Sudhir, K., & Komesaroff, P. A. (1999). Cardiovascular Actions of Estrogens in Men. The Journal of Clinical Endocrinology & Metabolism, 84(10), 3411–3415. [DOI:10.1210/jcem.84.10.5954]
Swee, D. S., Javaid, U., & Quinton, R. (2019). Estrogen Replacement in Young Hypogonadal Women—Transferrable Lessons From the Literature Related to the Care of Young Women With Premature Ovarian Failure and Transgender Women. Frontiers in Endocrinology, 10, 685. [DOI:10.3389/fendo.2019.00685]
Tadd, W., & Bayer, A. (2006). Dignity in health and social care for older Europeans: implications of a European project. Aging Health, 2(5), 771–779. [DOI:10.2217/1745509x.2.5.771]
Taylor, J. K., & Pendleton, N. (2016). Progesterone therapy for the treatment of non-cancer cachexia: a systematic review. BMJ Supportive & Palliative Care, 6(3), 276–286. [DOI:10.1136/bmjspcare-2015-001041]
Tchaikovski, S. N., & Rosing, J. (2010). Mechanisms of Estrogen-Induced Venous Thromboembolism. Thrombosis Research, 126(1), 5–11. [DOI:10.1016/j.thromres.2010.01.045]
Tepper, N. K., Whiteman, M. K., Marchbanks, P. A., James, A. H., & Curtis, K. M. (2016). Progestin-only contraception and thromboembolism: A systematic review. Contraception, 94(6), 678–700. [DOI:10.1016/j.contraception.2016.04.014]
Tepper, N. K., Jeng, G., Curtis, K. M., Boutot, M. E., Boulet, S. L., & Whiteman, M. K. (2019). Venous Thromboembolism Among Women Initiating Depot Medroxyprogesterone Acetate Immediately Postpartum. Obstetrics & Gynecology, 133(3), 533–540. [DOI:10.1097/aog.0000000000003135]
The Coronary Drug Project Research Group. (1970). The Coronary Drug Project. JAMA, 214(7), 1303–1313. [DOI:10.1001/jama.1970.03180070069012]
The Coronary Drug Project Research Group. (1973). The Coronary Drug Project. JAMA, 226(6), 652–657. [DOI:10.1001/jama.1973.03230060030009]
The Oral Contraceptive and Hemostasis Study Group. (1999). An open label, randomized study to evaluate the effects of seven monophasic oral contraceptive regimens on hemostatic variables. Contraception, 59(6), 345–355. [DOI:10.1016/s0010-7824(99)00044-x]
Timp, J. F., Braekkan, S. K., Versteeg, H. H., & Cannegieter, S. C. (2013). Epidemiology of cancer-associated venous thrombosis. Blood, 122(10), 1712–1723. [DOI:10.1182/blood-2013-04-460121]
Toorians, A. W., Thomassen, M. C., Zweegman, S., Magdeleyns, E. J., Tans, G., Gooren, L. J., & Rosing, J. (2003). Venous Thrombosis and Changes of Hemostatic Variables during Cross-Sex Hormone Treatment in Transsexual People. The Journal of Clinical Endocrinology & Metabolism, 88(12), 5723–5729. [DOI:10.1210/jc.2003-030520]
Totaro, M., Palazzi, S., Castellini, C., Parisi, A., D’Amato, F., Tienforti, D., Baroni, M. G., Francavilla, S., & Barbonetti, A. (2021). Risk of Venous Thromboembolism in Transgender People Undergoing Hormone Feminizing Therapy: A Prevalence Meta-Analysis and Meta-Regression Study. Frontiers in Endocrinology, 12, 741866. [DOI:10.3389/fendo.2021.741866]
Trémollieres, F. (2012). Contraception orale estro-progestative: quelle différence entre éthinylestradiol et estradiol? [Oral combined contraception: Is there any difference between ethinyl-estradiol and estradiol?] Gynécologie Obstétrique & Fertilité, 40(2), 109–115. [DOI:10.1016/j.gyobfe.2011.10.009]
Turo, R., Smolski, M., Esler, R., Kujawa, M. L., Bromage, S. J., Oakley, N., Adeyoju, A., Brown, S. C., Brough, R., Sinclair, A., & Collins, G. N. (2013). Diethylstilboestrol for the treatment of prostate cancer: past, present and future. Scandinavian Journal of Urology, 48(1), 4–14. [DOI:10.3109/21681805.2013.861508]
United Nations Development Programme/United Nations Population Fund/World Health Organization/World Bank Special Programme of Research, Development and Research Training in Human Reproduction, & Task Force on Long-acting Systemic Agents for Fertility Regulation. (2003). Comparative study of the effects of two once-a-month injectable contraceptives (Cyclofem® and Mesigyna®) and one oral contraceptive (Ortho-Novum 1/35®) on coagulation and fibrinolysis. Contraception, 68(3), 159–176. [DOI:10.1016/s0010-7824(03)00164-1]
van Hylckama Vlieg, A., Helmerhorst, F. M., & Rosendaal, F. R. (2010). The Risk of Deep Venous Thrombosis Associated With Injectable Depot–Medroxyprogesterone Acetate Contraceptives or a Levonorgestrel Intrauterine Device. Arteriosclerosis, Thrombosis, and Vascular Biology, 30(11), 2297–2300. [DOI:10.1161/atvbaha.110.211482]
Van Kesteren, P. J., Asscheman, H., Megens, J. A., & Gooren, L. J. (1997). Mortality and morbidity in transsexual subjects treated with cross-sex hormones. Clinical Endocrinology, 47(3), 337–343. [DOI:10.1046/j.1365-2265.1997.2601068.x]
van Vliet, H. A., Frolich, M., Christella, M., Thomassen, L., Doggen, C. J., Rosendaal, F. R., Rosing, J., & Helmerhorst, F. M. (2005). Association between sex hormone-binding globulin levels and activated protein C resistance in explaining the risk of thrombosis in users of oral contraceptives containing different progestogens. Human Reproduction, 20(2), 563–568. [DOI:10.1093/humrep/deh612]
Vinogradova, Y., Coupland, C., & Hippisley-Cox, J. (2015). Use of combined oral contraceptives and risk of venous thromboembolism: nested case-control studies using the QResearch and CPRD databases. BMJ, 350, h2135. [DOI:10.1136/bmj.h2135]
Vinogradova, Y., Coupland, C., & Hippisley-Cox, J. (2019). Use of hormone replacement therapy and risk of venous thromboembolism: nested case-control studies using the QResearch and CPRD databases. BMJ, 364, k4810. [DOI:10.1136/bmj.k4810]
von Schoultz, B., Carlström, K., Collste, L., Eriksson, A., Henriksson, P., Pousette, Å., & Stege, R. (1989). Estrogen therapy and liver function—metabolic effects of oral and parenteral administration. The Prostate, 14(4), 389–395. [DOI:10.1002/pros.2990140410]
Walker, I. D. (2010). Obstetrics, Contraception, and Estrogen Replacement. In Key, N., Makris, M., O’Shaughnessy, D., & Lillicrap, D. (Eds.). Practical Hemostasis and Thrombosis, 2nd Edition (pp. 247–257). Oxford: Wiley-Blackwell. [DOI:10.1002/9781444306286.ch24]
Weinand, J. D., & Safer, J. D. (2015). Hormone therapy in transgender adults is safe with provider supervision; A review of hormone therapy sequelae for transgender individuals. Journal of Clinical & Translational Endocrinology, 2(2), 55–60. [DOI:10.1016/j.jcte.2015.02.003]
Westerlund, E., Henriksson, P., Wallén, H., Hovatta, O., Wallberg, K. R., & Antovic, A. (2012). Detection of a procoagulable state during controlled ovarian hyperstimulation for in vitro fertilization with global assays of haemostasis. Thrombosis Research, 130(4), 649–653. [DOI:10.1016/j.thromres.2011.11.024]
White, C. M., Ferraro‐Borgida, M. J., Fossati, A. T., McGill, C. C., Ahlberg, A. W., Feng, Y. J., Heller, G. V., & Chow, M. S. (1998). The Pharmacokinetics of Intravenous Estradiol—A Preliminary Study. Pharmacotherapy: The Journal of Human Pharmacology and Drug Therapy, 18(6), 1343–1346. [DOI:10.1002/j.1875-9114.1998.tb03157.x]
Wiegratz, I., & Kuhl, H. (2006). Metabolic and clinical effects of progestogens. The European Journal of Contraception & Reproductive Health Care, 11(3), 153–161. [DOI:10.1080/13625180600772741]
Wierckx, K., Elaut, E., Declercq, E., Heylens, G., De Cuypere, G., Taes, Y., Kaufman, J. M., & T’Sjoen, G. (2013). Prevalence of cardiovascular disease and cancer during cross-sex hormone therapy in a large cohort of trans persons: a case–control study. European Journal of Endocrinology, 169(4), 471–478. [DOI:10.1530/eje-13-0493]
Writing Group for the Women’s Health Initiative Investigators. (2002). Risks and Benefits of Estrogen Plus Progestin in Healthy Postmenopausal Women: Principal Results From the Women’s Health Initiative Randomized Controlled Trial. JAMA, 288(3), 321–333. [DOI:10.1001/jama.288.3.321]
Zhang, M., Zhu, S., Yang, W., Huang, Q., & Ho, C. (2021). The biological fate and bioefficacy of citrus flavonoids: bioavailability, biotransformation, and delivery systems. Food & Function, 12(8), 3307–3323. [DOI:10.1039/d0fo03403g]
Zhao, J., Yang, J., & Xie, Y. (2019). Improvement strategies for the oral bioavailability of poorly water-soluble flavonoids: An overview. International Journal of Pharmaceutics, 570, 118642. [DOI:10.1016/j.ijpharm.2019.118642]
Zucker, R., Reisman, T., & Safer, J. D. (2021). Minimizing Venous Thromboembolism in Feminizing Hormone Therapy: Applying Lessons From Cisgender Women and Previous Data. Endocrine Practice, 27(6), 621–625. [DOI:10.1016/j.eprac.2021.03.010]
\ No newline at end of file
+Estrogens and Their Influences on Coagulation and Risk of Blood Clots - Transfeminine Science
Estrogens and Their Influences on Coagulation and Risk of Blood Clots
By Aly | First published October 20, 2020 | Last modified March 28, 2023
Abstract / TL;DR
Estrogens increase coagulation by activating estrogen receptors in the liver and thereby modulating the production of a variety of circulating coagulation factors. With sufficiently high exposure, this can result in an increase in the risk of blood clots as well as coagulation-associated cardiovascular complications like heart attack and stroke. However, the degrees of risk vary depending on the estrogen type, route, and dose. Non-bioidentical estrogens like ethinylestradiol have greater strength in the liver due to their relative resistance to metabolism and increase blood clot risk more readily than bioidentical estradiol, while oral administration of estradiol results in a first pass through the liver and has greater impact on blood clot risk than non-oral estradiol. Physiological estradiol levels with non-oral estradiol appear to have minimal to no risk of blood clots, whereas oral estradiol has significant risk and at high doses may have risk similar to that of the doses of ethinylestradiol in modern birth control pills. Higher estradiol levels with non-oral estradiol seem to have significant risk of blood clots and cardiovascular problems as well, although the risks appear to be lower than with ethinylestradiol-containing birth control pills. Absolute risks of blood clots are low but accumulate with time and add up on a population scale. In addition, a variety of risk factors, such as age, physical inactivity, concomitant progestogen use, and often-unknown thrombophilic abnormalities, can substantially augment risk. Due to their higher risks of blood clots, oral estradiol as well as excessive doses of non-oral estradiol should ideally be avoided in transfeminine people. This is particularly applicable in those with risk factors for blood clots. In any case, therapeutic considerations for transfeminine people include not only safety but also effectiveness, other factors like cost and convenience, and the natures of the alternative therapeutic options.
Introduction
Estrogens increase coagulation (blood clotting) and the risk of thrombosis, a cardiovascular event otherwise known as a blood clot. There are two major types of blood clots, which are categorized depending on whether they happen in a vein or in an artery: (1) venous thrombosis or venous thromboembolism (VTE); and (2) arterial thrombosis. VTE is a blood clot in a vein, a blood vessel that carries blood towards the heart. It comprises two different subtypes: (1) deep vein thrombosis (DVT), a clot in a vein of the leg or pelvic region; and (2) pulmonary embolism (PE), a clot that has broken free and blocked an artery in the lungs. Arterial thrombosis is a blood clot in an artery, a blood vessel that carries blood away from the heart. Arterial thrombosis can lead to myocardial infarction (MI; also known as heart attack) or cerebrovascular accident (CVA; also known as stroke). Blood clots are major health problems that can cause serious complications and even death. Estrogens, via increased coagulation with sufficiently high exposure, have the potential to heighten the risk of both venous and arterial thrombosis and hence to increase all of the aforementioned risks. The risk of blood clots with estrogens serves as a limiting factor in their use due to the potential health consequences.
Estrogens are selectiveagonists of the estrogen receptors (ERs). They are thought to increase coagulation and hence blood clot risk by activating ERs. However, the impact on coagulation and risk of blood clots with estrogens varies due to factors like estrogen type, route, and dose. In addition, other factors, like concomitant progestogen use and a variety of non-hormonal factors, are known to modify the risk. The purpose of this article is to review the risks of blood clots with estrogens, the mechanisms underlying increased coagulation and blood clot risk with estrogens, and the reasons for differences among estrogens in terms of risk. Exploring these topics can inform estrogen dosing considerations in transfeminine people and help to minimize risks and optimize safety. Moreover, higher levels of estrogens are therapeutically useful for suppressing testosterone production in transfeminine people but may increase blood clot risk, and risk–benefit analysis is warranted in this context.
Blood Clot Risks with Estrogens and Progestogens
A variety of estrogens have been used in medicine. These include bioidentical estrogens like estradiol as well as non-bioidentical estrogens like conjugated estrogens (CEEs; Premarin), ethinylestradiol (EE), and diethylstilbestrol (DES). Estradiol is the major natural estrogen in the human body. CEEs deliver primarily estradiol as the active estrogen, but also contain significant quantities of naturally occurring equine (horse) estrogens such as equilin (7-dehydroestrone) and 17β-dihydroequilin (7-dehydroestradiol). EE and DES are synthetic estrogens that were created by humans and do not occur naturally. DES was discontinued decades ago and is relatively little-known today, but has significant historical importance. Estradiol is used in both oral and non-oral forms (e.g., transdermal patches), while the non-bioidentical estrogens have typically been used orally. For context, the table below shows some approximate comparable doses of these estrogens in terms of general estrogenicity.
Table 1: Approximate or estimated comparable doses of estrogens in terms of general/systemic estrogenicity (Aly, 2020; Kuhl, 2005; Table; Table; Table):
Estrogen type/route
Very low dose a
Low dose a
Moderate dose b
High dose
Oral estradiol
1 mg/day
2 mg/day
4 mg/day
8 mg/day
Transdermal estradiolc
25 μg/day
50 μg/day
100 μg/day
200 μg/day
Oral conjugated estrogens
0.625 mg/day
1.25 mg/day
2.5 mg/day
5 mg/day
Oral ethinylestradiol
7.5 μg/day
15 μg/day
30 μg/day
60 μg/day
Oral diethylstilbestrol
0.375 mg/day
0.75 mg/day
1.5 mg/day
3 mg/day
Comparable estradiol level
~25 pg/mL
~50 pg/mL
~100 pg/mL
~200 pg/mL
a Menopausal replacement dosages. b Similar to normal mean/integrated estrogenic exposure during the menstrual cycle in premenopausal women (Aly, 2018). c Specifically transdermal patches.
Estrogens were first associated with blood clots and associated cardiovascular complications in the 1960s and 1970s. Significant to substantial increases in these risks were found in clinical trials of high-dose DES (5 mg/day) for prostate cancer in men (VACURG, 1967; Byar, 1973; Turo et al., 2014), trials of moderate-dose CEEs (2.5–5 mg/day) for prevention of heart disease in men (Coronary Drug Project Research Group, 1970; Coronary Drug Project Research Group, 1973; Luria, 1989; Sudhir & Komesaroff, 1999; Dutra et al., 2019), and studies of early high-dose EE-containing birth control pills (50–150 μg/day) in premenopausal women (Gerstman et al., 1991; PCASRM, 2017; Table). The increase in cardiovascular events with DES in men with prostate cancer was sufficiently great that it actually cancelled out the benefits of its effects against prostate cancer in terms of overall mortality. The large increases in blood clots and cardiovascular problems seen in these studies resulted in alarm and concern about the safety of estrogens. Consequent to these events, estrogen doses were lowered. DES for prostate cancer was decreased to 1 to 3 mg/day and EE in birth control pills was decreased to 20 to 35 μg/day. Estrogens were also reduced to lower doses for other indications, such as menopausal hormone therapy. The dose reductions helped to lower the risks, although it did not eliminate them.
Whereas the WHI demonstrated causation for oral CEEs alone in terms of blood clot risk, no adequately powered RCTs have been conducted with oral or transdermal estradiol alone to establish causation in terms of blood clot risk at this time. Only very large and expensive trials would be able to show this due to the rarity of blood clots, and these studies have not been conducted to date. For similar reasons, RCTs demonstrating increased risk of blood clots with EE-containing birth control pills have also not been conducted at this time (Moores, Bilello, & Murin, 2004). In any case, causation has clearly been demonstrated with estrogens in other contexts, and this can be assumed as likely in the case of oral estradiol similarly. In addition, the Estrogen in Venous Thromboembolism Trial (EVTET), an RCT of low-dose (2 mg/day) oral estradiol plus the progestogen norethisterone acetate (NETA) versus placebo in postmenopausal women with history of previous blood clots, found that this hormone therapy regimen significantly increased coagulation and the incidence of blood clots (10.7% incidence with hormone therapy and 2.3% with placebo; P = 0.04) (Høibraaten et al., 2000; Høibraaten et al., 2001).
Estradiol levels appear to not be associated with blood clot risk in premenopausal women (Holmegard et al., 2014). The fact that transdermal estradiol patches at 100 μg/day in menopausal women haven’t been associated with a greater risk of blood clots is notable as this dose achieves estradiol levels of around 100 pg/mL on average, which are similar to the mean integrated levels of estradiol during the normal menstrual cycle in premenopausal women (Aly, 2018; Wiki). Rates of blood clots are also similar between men—who have relatively low estradiol levels—and women after controlling for atypical hormonal states like pregnancy and use of birth control pills in women (Moores, Bilello, & Murin, 2004; Rosendaal, 2005; Montagnana et al., 2010; Roach et al., 2013). Interestingly however, men have a consistently higher incidence of recurrent blood clots than women (Roach et al., 2013). These findings suggest that physiological levels of estradiol and progesterone in premenopausal women may not meaningfully increase coagulation or blood clot risk. However, the available data are mixed, with some studies suggesting that estradiol and/or progesterone levels within physiological ranges may indeed influence coagulation (Chaireti et al., 2013) and blood clot risk in premenopausal and/or perimenopausal women (Simon et al., 2006; Canonico et al., 2014; Scheres et al., 2019).
Modern combined birth control pills contain EE at moderately estrogenic doses (20–35 μg/day) and a physiological dose of a progestogen. They increase the risk of blood clots by several-fold (Konkle & Sood, 2019; Vinogradova, Coupland, & Hippisley-Cox, 2015; Table). In addition, they are associated with about a 1.5- to 2-fold increase in risk of heart attack and stroke (Lidegaard, 2014; Konkle & Sood, 2019). However, overall mortality is not increased with birth control pills—at least in the relatively young women in whom they are used (Hannaford et al., 2010). Per studies of menopausal hormone therapy, it is likely that the progestogen in EE-containing birth control pills augments the risk of blood clots with EE. Early high-dose birth control pills (50–100 μg/day) had as much as twice the risk of blood clots of modern birth control pills (Gerstman et al., 1991; PCASRM, 2017; Table). In contrast to the different blood clot risks between oral and transdermal estradiol, non-oral birth control forms containing EE, for instance transdermal birth control patches and vaginal birth control rings, are associated with similar increases in blood clot risk as EE-containing birth control pills (Plu-Bureau et al., 2013; PCASRM, 2017; Konkle & Sood, 2019; Abou-Ismail, Sridhar, & Nayak, 2020). Hence, unlike with estradiol, route of administration does not appear to modify blood clot risk with EE based on available data.
High-dose estrogen therapy using oral synthetic estrogens like DES and EE in people with breast or prostate cancer has been found to strongly increase the risk of blood clots and associated cardiovascular complications (Phillips et al., 2014; Turo et al., 2014; Coelingh Bennink et al., 2017). This has also been the case with estramustine phosphate (EMP; estradiol normustine phosphate), an estradiol ester that is used at massive doses in prostate cancer (e.g., 140–1,400 mg/day orally) and that results in pregnancy levels of estradiol (Kitamura, 2001 [Graph]; Ravery et al., 2011). In the 1980s however, it was found that high-dose non-oral estradiol did not have the same cardiovascular risks as high-dose estrogen therapy with oral synthetic estrogens or EMP (von Schoultz et al., 1989; Ockrim & Abel, 2009). This included studies with polyestradiol phosphate (PEP), a long-lasting injectable prodrug of estradiol, and with high-dose transdermal estradiol gel (von Schoultz et al., 1989; Aly, 2019). However, subsequent larger and higher-quality studies found that although the cardiovascular risks with PEP were much lower than with high-dose oral synthetic estrogen therapy, they were nonetheless still increased (Hedlung et al., 2008; Ockrim & Abel, 2009; Hedlund et al., 2011; Sam, 2020). This includes an approximate 2-fold increase in the risk of blood clots with estradiol levels in the range of roughly 300 to 500 pg/mL (Sam, 2020). Studies using high-dose transdermal estradiol patches have not found significantly increased cardiovascular complications as of present (Langley et al., 2013; Sam, 2020). However, these studies have been relatively underpowered, which limits their interpretation. In any case, increased coagulation has been observed with high-dose transdermal estradiol patches (achieving estradiol levels of 350 to 500 pg/mL) (Bland et al., 2005) similarly to PEP (Mikkola et al., 1999). More data on the risk of blood clots and cardiovascular issues with high-dose transdermal estradiol patches should come in the future with PATCH and STAMPEDE—two large-scale clinical studies in the United Kingdom that are evaluating this form of estradiol for prostate cancer (Gilbert et al., 2018; Singla, Ghandour, & Raj, 2019).
Injections of short-acting estradiol esters like estradiol valerate and estradiol cypionate are notable in that they are often used by transfeminine people and are generally used at doses that achieve high estradiol levels. As with high-dose transdermal estradiol patches, little to no quality data on the risk of blood clots exists for these preparations at present. Pyra and colleagues found that the risk of blood clots with injectable estradiol valerate in transfeminine people was increased by around 2-fold, but the confidence intervals were very wide and statistical significance was not reached (Pyra et al., 2020). The doses used in the whole population for the study were not provided, but in the actual VTE cases, the doses of injectable estradiol valerate were described and ranged from 4 to 20 mg once per week and 10 to 40 mg once every 2 weeks (Pyra et al., 2020). Studies have also assessed and found increased coagulation with high doses of estradiol valerate by injection in the range of 10 to 40 mg once every 2 weeks in men with prostate cancer (Kohli & McClellan, 2001; Kohli et al., 2004; Kohli, 2005). Increased coagulation has additionally been observed with the combination of 5 mg estradiol valerate and a progestogen once per month as a combined injectable contraceptive in premenopausal women (Meng et al., 1990; UN/WHO et al., 2003). It is unclear whether the high peaks in estradiol levels associated with short-acting injectable forms of estradiol are harmful in terms of coagulation and blood clot risk (Hembree et al., 2017). However, the increased risk of polycythemia with short-acting injectable testosterone esters relative to other non-oral forms of testosterone (Ohlander, Varghese, & Pastuszak, 2018) is indirectly suggestive that this could be the case. Accordingly, a study found increased coagulation in premenopausal women with a combined injectable contraceptive containing estradiol valerate but not with one employing the more prolonged and stable estradiol cypionate at the same dose (UN/WHO et al., 2003).
Pregnancy is a time when estradiol and progesterone levels increase to extremely high concentrations (Graphs). Estradiol levels increase progressively throughout pregnancy to around 2,000 pg/mL on average at the end of the first trimester, to about 10,000 pg/mL on average at the end of the second trimester, and to around 20,000 pg/mL on average at the end of the third trimester (Kerlan et al., 1994 [Graph]; Schock et al., 2016). Coagulation is greatly increased during pregnancy, and the risk of blood clots is likewise strongly increased (Heit et al., 2000; Abdul Sultan et al., 2015; Heit, Spencer, & White, 2016; Table). Estradiol and progesterone levels are strongly correlated with the increases in coagulation during pregnancy (Bagot et al., 2019). The risk of blood clots with modern birth control pills is similar to that with pregnancy as a whole (Heit, Spencer, & White, 2016), while the increases in risk of blood clots with early high-dose EE-containing birth control pills and with high-dose oral synthetic estrogen therapy for breast and prostate cancer are comparable to the risk increase during late pregnancy. Estradiol levels also increase to very high concentrations during ovarian stimulation for in-vitro fertilization in premenopausal women, and this has been associated with increased coagulation and risk of blood clots as well (Westerlund et al., 2012; Rova, Passmark, & Lindqvist, 2012; Kasum et al., 2014).
Due to their greater risks of cardiovascular problems as well as other concerns, DES has been virtually abandoned while EE has been discontinued for almost all indications except birth control. EE continues to be used in birth control because it is resistant to metabolism in the uterus and controls menstrual bleeding better than oral estradiol does (Stanczyk, Archer, & Bhavnani, 2013). CEEs are also being increasingly superseded by estradiol in medicine, although significant use of CEEs for hormone therapy in cisgender women continues. Transdermal estradiol is gaining momentum over oral estradiol in menopausal hormone therapy as well. Major transgender hormone therapy guidelines (see also Aly, 2020) recommend against the use of EE and CEEs in transfeminine people due to their greater risks and the inability to accurately monitor blood estrogen levels with these preparations (Coleman et al., 2012; Deutsch, 2016; Hembree et al., 2017). Estradiol is the estrogen that is almost exclusively used in transfeminine people today. Besides estrogen type, it has been recommended that transdermal estradiol be used instead of oral estradiol in transfeminine people who are over 40 or 45 years of age or are otherwise at risk for blood clots (Deutsch, 2016; Iwamoto et al., 2019; Glintborg et al., 2021). Menopausal hormone therapy guidelines similarly recommend the use of transdermal estradiol over oral estrogens in cisgender women who are at higher risk for blood clots (e.g., Stuenkel et al., 2015).
In a historically notable study conducted by the Center of Expertise on Gender Dysphoria (CEGD) at the Vrije Universiteit Medical Center (VUMC) in Amsterdam, the Netherlands in the 1980s, it was reported that the risk of blood clots with high-dose EE and CPA in transfeminine people was increased by 45-fold relative to the expected incidence in the general population (Asscheman, Gooren, & Eklund, 1989; Asscheman et al., 2014). Mortality also appeared to be elevated and other health risks were increased as well (Asscheman, Gooren, & Eklund, 1989; Gooren & T’Sjoen, 2018). A subsequent study in transfeminine people by the CEGD confirmed strongly increased coagulation with EE but much lower increases with oral or transdermal estradiol (Toorians et al., 2003). Upon the CEGD switching transfeminine people from high-dose EE to physiological doses of oral or transdermal estradiol (also usually in combination with CPA), the risks decreased considerably (van Kesteren et al., 1997; Asscheman et al., 2011; Asscheman et al., 2014). These findings were of major importance in the replacement of EE with estradiol in transfeminine hormone therapy, and have surely contributed significantly to apprehension about the use of high doses of estrogens in transfeminine people.
Taken together, estrogens of all kinds have been shown to dose-dependently increase or be associated with increased risk of blood clots. These findings suggest that, provided of course sufficient exposure occurs, increased coagulation and blood clot risk are common properties of estrogens. However, synthetic and non-bioidentical estrogens have greater risk of blood clots than estradiol, and oral estradiol shows greater risk than non-oral estradiol. In fact, physiological estradiol levels in women and low to moderate doses of transdermal estradiol may have no significant risk of blood clots at all. Nonetheless, non-oral estradiol with sufficiently high exposure can increase blood clot risk just the same as other forms of estrogen. Concomitant therapy with progestogens appears to augment the risk of blood clots with estrogens and high doses may particularly amplify the risk.
Risks with Different Hormonal Exposures
The table below provides relative risk increases for blood clots with different types, routes, and doses of estrogens, as well as with SERMs, pregnancy, and high-dose CPA. It shows the greater risks of blood clots with (1) oral estradiol relative to non-oral estradiol; (2) estradiol compared to non-bioidentical estrogens; and (3) lower estrogen levels/doses relative to higher estrogen levels/doses.
Table 2: Relative risks of blood clots with different hormonal exposures (see also Machin & Ragni, 2020):
Footnotes:a At typical menopausal replacement doses (i.e., not very high—probably no more than double the given dose). b MPA, norethisterone, norgestrel, or drospirenone. c Modern EE + P birth control contains 20–35 μg/day EE, while high-dose EE + P birth control used in the 1960s and 1970s contained 50–150 μg/day EE. d Risk around twice as high as modern birth control pills. e Unpublished original research/analysis with borderline statistical significance (95% CI 0.99–4.22). f Excluding the postpartum period. With the postpartum period included, the risk of blood clots with pregnancy is 5–10× (McLintock, 2014). Abbreviations: E2 = Estradiol; CEEs = Conjugated estrogens; EE = Ethinylestradiol; DES = Diethylstilbestrol; EMP = Estramustine phosphate; PEP = Polyestradiol phosphate; SERMs = Selective estrogen receptor modulators; CPA = Cyproterone acetate; P = Progestogen.
Note that the values in the table are associations mostly from observational studies rather than from RCTs. Hence, in many cases, causation has not been definitively established. In addition, the values represent rough average values with often wide 95% confidence intervals. As a result, precision and accuracy of the estimates may in some cases be low. Also note that quantified blood clot risk will vary depending on the study and its definitions and methodology (including factors like sampling error, approach to control of confounding variables, and residual confounding influences).
Mechanisms of Increased Coagulation with Estrogens
Aside from coagulation factors, estrogens also modulate the synthesis of numerous other liver products (Kuhl, 1999; Kuhl, 2005; Table). Examples include sex hormone-binding globulin (SHBG), corticosteroid-binding globulin (CBG), various other circulating binding proteins, angiotensinogen, lipoproteins, and triglycerides, among others. In accordance with the mechanisms underlying increased coagulation and blood clot risk with estrogens, the differences in risk of blood clots with different types and routes of estrogens are mirrored in their influences on estrogen-sensitive liver products. Put another way, different estrogens have different relative potency in the liver when compared to their estrogenic potency elsewhere in the body. Synthetic and non-bioidentical estrogens have greater impact on liver synthesis than estradiol, while oral administration of estradiol has greater influence on liver synthesis than non-oral routes like transdermal administration or intramuscular injection, and this is likely to explain the observed differences in coagulation and blood clot risk with these different estrogens. The table below shows the liver potency of different estrogenic exposures as measured by influence specifically on SHBG levels, one of the most sensitive and well-characterized estrogen-modulated liver products.
Table 3: Relative increases in SHBG levels with different estrogenic exposures (see also Aly, 2020):
Footnotes:a Due to differences in molecular weight, estradiol valerate has about 75% of the amount of estradiol as regular estradiol. Hence, 6 mg/day estradiol valerate is approximately equivalent to 4.5 mg/day estradiol. b Modern EE + P birth control contains 20–35 μg/day EE, while high-dose EE + P birth control used in the 1960s and 1970s contained 50–150 μg/day EE. c In the form of 320 mg/month PEP (~700 pg/mL estradiol), 100 mg/month estradiol undecylate (~500–600 pg/mL estradiol), or 10 mg/10 days estradiol valerate (~500–1,200 pg/mL peak estradiol; Graphs). Abbreviations: E2 = Estradiol; EV = Estradiol valerate; CEEs = Conjugated estrogens; EE = Ethinylestradiol; DES = Diethylstilbestrol; EMP = Estramustine phosphate; PEP = Polyestradiol phosphate; P = Progestogen.
The increase in SHBG levels with estrogen therapy correlates with increases in coagulation and blood clot risk and can serve as a reliable surrogate indicator of these effects (Odlind et al., 2002; van Rooijen et al., 2004; van Vliet et al., 2005; Tchaikovski & Rosing, 2010; Raps et al., 2012; Stegeman et al., 2013; Hugon-Rodin et al., 2017; Eilertsen et al., 2019). The increases in SHBG levels and blood clot risk even appear quite similar to each other with modern birth control pills (both ~4-fold), high-dose oral synthetic estrogen therapy (both ~5–10-fold), and late pregnancy (both ~5–10-fold). When data on blood clot risk with a given estrogen route or dose are limited or unavailable—for instance with high-dose oral estradiol or high-dose estradiol ester injections—changes in SHBG levels can be used as a rough proxy or surrogate instead to estimate overall liver impact, magnitude of change in coagulation systems, and blood clot risk. It should be noted however that progestogens may augment the blood clot risk with estrogens without necessarily affecting SHBG levels or even while decreasing SHBG levels via concomitant androgenic activity (Kuhl, 2005; Vinogradova, Coupland, & Hippisley-Cox, 2019).
Physiological levels of estradiol appear to have relatively minimal influence on liver synthesis (Eisenfeld & Aten, 1979; Lax, 1987; Kuhl, 2005). This is in accordance with the limited influence or non-influence of physiological estradiol levels in women on blood clot risk. It is thought that under normal physiological circumstances, estradiol is only supposed to considerably affect liver synthesis at very high levels—namely during pregnancy. The changes in synthesis of liver products during pregnancy presumably have important biological roles at this time (Eisenfeld & Aten, 1979). One of these is considered to be increased coagulation, as coagulation limits blood loss with childbirth and hence has survival benefits. Conversely, there is no obvious benefit to increased coagulation outside of pregnancy.
Estradiol and the Liver First Pass with Oral Administration
The oralroute of administration is subject to a first pass through the liver via the hepatic portal vein which is not present with non-oral routes of administration (Pond & Tozer, 1984; Back & Rogers, 1987). As such, oral estradiol is subject to a hepatic first pass while this does not occur with non-oral forms of estradiol such as transdermal estradiol and injectable estradiol (Kuhl, 1998; Kuhl, 2005). This first pass results in disproportionate exposure of the liver to estradiol as well as disproportionate estrogenic impact on liver protein synthesis (Kuhl, 2005). Oral estradiol likewise has disproportionate estrogenic impact on the hepatic synthesis of coagulation factors (Kuhl, 1998; Kuhl, 2005). Due to the first pass, it is estimated that there is a 4- or 5-fold greater estrogenic impact of oral estradiol in the liver relative to non-oral estradiol (Kuhl, 2005). Due to the absence of the hepatic first pass with most non-oral routes, there is strong biological plausibility for the lower risk of blood clots that has been found with transdermal estradiol in comparison to oral estradiol in observational studies (Baber et al., 2016).
Although oral estradiol has a much higher relative potential for blood clots due to the liver first pass, sufficiently high levels of estradiol will diffuse into the liver from the blood to act on this tissue regardless of route of administration. Hence, high levels of estradiol via non-oral routes (or produced by the body itself) can increase coagulation and blood clot risk similarly to the oral route. This is clearly evidenced by hyperestrogenic situations like pregnancy and ovarian stimulation for in-vitro fertilization, when estradiol levels increase to very high concentrations and substantially influence liver protein synthesis.
Non-Bioidentical Estrogens and Resistance to Liver Metabolism
Non-bioidentical estrogens such as EE, DES, and CEEs have greater impact on liver protein synthesis and risk of blood clots than either oral estradiol or non-oral estradiol (Kuhl, 1998; Kuhl, 2005; Phillips et al., 2014; Turo et al., 2014; Table). This is because the liver strongly metabolizes and inactivates estradiol, whereas non-bioidentical estrogens have differences in their chemical structures relative to estradiol that result in them being much more resistant to liver metabolism (Kuhl, 1998; Kuhl, 2005; Connors & Middeldorp, 2019; Swee, Javaid, & Quinton, 2019).
EE can be considered as a case example. The oral bioavailability of EE is around 45%, while that of estradiol is only about 5% (Kuhl, 2005; Stanczyk, Archer, & Bhavnani, 2013). In addition, the blood half-life of EE is in the range of 5 to 30 hours, compared to less than 1 hour in the case of estradiol (White et al., 1998; Kuhl, 2005; Stanczyk, Archer, & Bhavnani, 2013). As a result of these and other differences, EE is approximately 120 times as potent as estradiol by weight in terms of general estrogenic effect (Kuhl, 2005; Table). Hence, EE is used clinically in μg doses whereas oral estradiol is used at over 100-fold higher mg doses. The pharmacokinetic differences between EE and estradiol reflect the strong resistance of EE to liver metabolism (Kuhl, 2005). EE, or 17α-ethynylestradiol, shows resistance to liver metabolism because of an ethynyl group at the C17α position which has been added to what is the otherwise unchanged structure of estradiol (Kuhl, 2005). This modification results in steric hindrance which blocks 17β-hydroxysteroid dehydrogenases (17β-HSDs) as well as conjugating enzymes like sulfotransferases and glucuronosyltransferases from metabolizing EE at the C17β hydroxyl group. 17β-HSDs normally convert estradiol into the weakly active estrone while the conjugating enzymes convert estradiol into inactive C17β estrogen sulfate and glucuronide conjugates like estrone sulfate (Kuhl, 2005). An “ethinylestrone” metabolite is in fact a structural impossibility due to the requirement of a double bond for a C17 ketone group—the needed C17α position is already occupied in EE by its ethynyl group. As such, the metabolism of estradiol into weakly active or inactive metabolites like estrone and estrone sulfate in the liver is protective against activation of hepatic ERs and procoagulation, and the lack of this with EE is responsible for its greater blood clot risk (Kuhl, 2005; Russell et al., 2017).
Figure 2: Chemical structures of selected estrogens. The C17 position in the case of the steroidal estrogens (E2, E1, and EE) is at the top right of the steroid nucleus.
Due to the marked resistance of EE to hepatic metabolism and inactivation, it persists for a long time in the liver—often cycling through it many times before finally being broken down. Moreover, EE shows several-fold disproportionate impact on liver protein synthesis at otherwise equivalent doses relative to oral estradiol (Kuhl, 2005; Table). Consequently, whereas EE has around 120-fold the general potency of oral estradiol, the liver potency of EE is around 350 to 1,500 times greater than that of oral estradiol (von Schoultz et al., 1989; Kuhl, 2005). A dose of EE of as little as 1 μg/day has been shown to impact liver metabolism (Speroff et al., 1996; Trémollieres, 2012). In addition, the fact that EE shows similar hepatic impact and risk of blood clots regardless of whether it is administered orally, transdermally, or vaginally indicates that unlike oral estradiol, the first pass through the liver with oral administration is not necessary for blood clot risk with EE (Plu-Bureau et al., 2013; PCASRM, 2017; Konkle & Sood, 2019). EE is so resistant to metabolism that it does not seem to matter how it is administered—the liver impact is substantial regardless of route. The greatly increased liver potency of EE results in its influence on coagulation and blood clot risk being much higher than that of estradiol at equivalent doses.
CEEs show a few-fold disproportionate estrogenic impact on liver protein synthesis relative to oral estradiol but less than that of EE (Kuhl, 2005; Table). This can be attributed to the equine (horse) estrogens in CEEs, which humans are presumably not adapted to and which show resistance to liver metabolism in humans. DES, on the other hand, shows even greater estrogenic influence on the liver than EE (Kuhl, 2005; Table). The more disproportionate impact on liver synthesis of DES relative to EE or CEEs may be attributable to the fact that it is a nonsteroidal estrogen and is far removed in structure from steroidal estrogens. This is relevant as steroidal estrogens are susceptible to varying extents to robust steroid-metabolizing enzymes in the liver (Kuhl, 2005). As with EE, 17β-HSDs have no affinity for DES and the hydroxyl groups of DES are not oxidized to form estrone-like ketone metabolites (Jensen et al., 2010). Consequent to their resistance to liver metabolism relative to estradiol, CEEs and nonsteroidal estrogens like DES have greater impacts on coagulation and blood clot risk than equivalent doses of estradiol similarly to EE although to varying extents.
When compared to transdermal estradiol rather than oral estradiol, the disproportionate influence of oral non-bioidentical estrogens on estrogen-modulated liver protein synthesis becomes extreme. With a little math, it quickly becomes apparent why high doses of these estrogens have influences on liver proteins and blood clot risks that are comparable to those during pregnancy. The table below shows some roughly calculated estimates for comparative liver strength of the different estrogens.
Table 4: Roughly calculated ratios of liver estrogenic potency to general/systemic estrogenic potency with estrogens based on a selection of liver products (e.g., SHBG, others) (Kuhl, 2005; Table):
Estrogen
Comparative liver potency
Relative to oral E2
Relative to transdermal E2
Transdermal E2
~0.25×a
1.0×a
Oral E2
1.0×
~4.0×
Oral CEEs
1.3–4.5×
~5.2–18×
Oral EE
2.9–5.0×
~12–20×
Oral DES
5.7–7.5×
~23–30×
a Based on a study that found oral estradiol to have 4-fold greater effect on SHBG levels than transdermal estradiol when used at doses that produced similar estradiol levels (Nachtigall et al., 2000).
Changes in liver protein synthesis induced by estrogens don’t scale linearly with dose or relative liver potency. There is progressive saturation in terms of changes in levels of SHBG and other liver products with estrogen dose—that is, higher doses have relatively diminished effect compared to lower doses (Kuhl, 1990; Kuhl, 1999). As an example, oral EE shows the following dose-dependent increases in SHBG levels: 2.0-fold at 5 μg/day, 3.0-fold at 10 μg/day, 3.4-fold at 20 μg/day, and 4.0-fold at 50 μg/day (Kuhl, 1998; Kuhl, 1999). These findings can be attributed to saturation of the competitive binding and/or activation of liver ERs by high estrogen concentrations (Kuhl, 1990). An implication of this dose-dependent saturation is that although for instance oral EE has much stronger potency in the liver than oral estradiol, oral estradiol can more quickly “catch up” to oral EE and other non-bioidentical estrogens in terms of liver impact than might be initially anticipated. Accordingly, oral estradiol has shown the following dose-dependent increases in SHBG levels: 1.6-fold at 1 mg/day, 2.2-fold at 2 mg/day, and 1.9- to 3.2-fold at 4 mg/day (Fåhraeus & Larsson-Cohn, 1982; Kuhl, 1998; Gibney et al., 2005; Ropponen et al., 2005). Hence, although oral EE may have roughly 3- to 5-fold higher liver potency than oral estradiol, a dose of oral estradiol near-equivalent to that of oral EE in terms of general estrogenic effect can increase SHBG levels to an extent that is only somewhat lower in comparison.
Selective Estrogen Receptor Modulators and Metabolism Resistance
SERMs like tamoxifen and raloxifene are essentially partial agonists of the ER. This is in contrast to estrogens—like estradiol, CEEs, EE, and DES—which act as full agonists of the ER. Similarly to nonsteroidal estrogens like DES, the clinically used SERMs are all nonsteroidal in structure and are strongly resistant to hepatic metabolism. In fact, certain SERMs, like tamoxifen and clomifene, are structurally related to and were derived from DES. SERMs show tissue differences in their ER-mediated effects, with estrogenic effects in some tissues (e.g., bone) and antiestrogenic effects in other tissues (e.g., breasts) (Lain, 2019; Table). Although there is variation between SERMs in terms of their effects in certain tissues (e.g., uterus), they are uniformly estrogenic in the liver. Consequently, SERMs show similar increases in blood clot risk as estrogens (Park & Jordan, 2002; Fabian & Kimler, 2005). As with non-bioidentical estrogens, the greater risk of blood clots with SERMs compared to oral estradiol can be attributed to their resistance to liver metabolism and hence to greater hepatic estrogenic potency. The SERMs that are used medically belong to diverse structural families (e.g., triphenylethylenes like tamoxifen and benzothiophenes like raloxifene). The only way in which SERMs of different structural classes are known to be related is in their shared interactions with the ERs.
Figure 3: Chemical structures of selected SERMs. They are nonsteroidal in structure and include tamoxifen (a triphenylethylene) and raloxifene (a benzothiophene).
Activation of the Estrogen Receptor is Specifically Responsible for Increased Coagulation with Estrogens and SERMs
Findings from preclinical and genetic research provide direct evidence for ER activation being responsible for the increased blood clot risk with estrogens. In an important animal study, EE was administered to mice and changes in procoagulant and anticoagulant biomarkers were measured (Cleuren et al., 2010). EE caused changes in levels of a variety of coagulation factors (Cleuren et al., 2010). The researchers also assessed estradiol and observed comparable changes (Cleuren et al., 2010). Co-administration of the selective ER full antagonist fulvestrant with EE neutralized all of the EE-induced coagulatory changes (Cleuren et al., 2010). Additionally, EE showed no effect on coagulation factors in ERα knockout mice (Cleuren et al., 2010). These findings are consistent with human and mouse genome-wide association studies which have found estrogen response elements (EREs)—DNA sequences that act as binding sites for genes regulated by the ER—embedded in a large number of genes involved in coagulatory pathways (Cleuren et al., 2010; Stanczyk, Mathews, & Cortessis, 2017).
The preceding findings are consistent with ER activation being responsible for increased coagulation and blood clot risk with estrogens and SERMs. This is in accordance with the fact that blood clot risk is a shared effect of selective ER agonists with highly diverse chemical structures, providing strong circumstantial support against a non-ER-mediated action of some sort being responsible (e.g., the weakly estrogenic metabolite estrone somehow mediating the blood clot risk with estradiol—Bagot et al., 2010). Increased coagulation and blood clot risk can thus be regarded as class effects of estrogens and SERMs—provided sufficiently high liver exposure. Due to differences in susceptibility to liver metabolism however, different ER agonists show differences in their relative impact on coagulation. Owing to estradiol’s lack of resistance to metabolism and its robust inactivation in the liver, the dosage requirements for increased coagulation and blood clot risk with estradiol—particularly in the case of non-oral estradiol—are greater than with non-bioidentical estrogens. Hence, estradiol, especially when administered via non-oral routes, is a safer form of estrogen therapy than other estrogens.
Absolute Incidences and Risk Factors
States of estrogen and/or progestogen exposure, such as exogenous hormone administration and pregnancy, are of course established risk factors for blood clots in women. In healthy young individuals without relevant risk factors for blood clots however, the incidence of blood clots is rare even in situations of considerably increased risk due to hormones (Rosendaal, 2005). The absolute incidence of VTE in non-pregnant women is only 1 to 5 of every 10,000 women each year (i.e., 0.01–0.05% per year) (PCASRM, 2017; Konkle & Sood, 2019). EE-containing birth control pills, which on average increase VTE risk by about 4-fold, are associated with an incidence of VTE of only 3 to 9 of every 10,000 women each year (i.e., 0.03–0.09% per year) (Konkle & Sood, 2019). Likewise, the absolute risk of blood clots during pregnancy, when estradiol and progesterone levels increase to extremely high concentrations and VTE risk is increased up to 7-fold (Abdul Sultan et al., 2015), is about 5 to 20 of every 10,000 women each year (i.e., 0.05–0.2% per year) (PCASRM, 2017; Konkle & Sood, 2019).
a 1–2/10,000 per year at <19 years of age, 2–3/10,000 per year at 20–29 years of age, 3–4/10,000 per year at 30–39 years of age, 5–7/10,000 per year at 40–49 years of age; roughly 3–4/10,000 per year for age 15–49 years overall (Rabe et al., 2011).
In addition to time and population considerations, there are, besides estrogen and progestogen exposure, a variety of other known risk factors for blood clots, and these risk factors can substantially augment blood clot risk (Heit et al., 2000; Rosendaal, 2005). Age is among the strongest of the known risk factors (Rosendaal, 2005; Montagnana et al., 2010). Moreover, age is uniquely notable as a risk factor in that it is one that eventually becomes relevant to everyone. The risk of blood clots increases on the order of 100-fold going from ≤15 years of age (incidence <0.005–0.01% per year) to ≥80 years of age (incidence ~0.5–1.0% per year) (Rosendaal, 2005; Montagnana et al., 2010; Rabe et al., 2011). The figure below provides a graphical representation of the influence of age on risk of blood clots.
Figure 4: Risk of first-incidence VTE (per 100,000 per year) by age group (in years) in men (black bars) and women (gray bars) (Oger, 2000; Rosendaal, 2005; Rosendaal, 2016).
Other established risk factors for blood clots and associated cardiovascular problems include physical inactivity (due to, e.g., bed rest, long-distance travel, etc.), obesity, smoking, thrombophilic abnormalities, cancer, surgery, and HIV, among many others (Baron et al., 1998; Heit et al., 2000; Rosendaal, 2005; Lijfering, Rosendaal, & Cannegieter, 2010; Timp et al., 2013). In addition to age, physical inactivity is one of the most important risk factors for blood clots and mediates the risk increases for many of the others (Rosendaal, 2005). Smoking on its own is not consistently associated with increased risk of VTE (Lijfering, Rosendaal, & Cannegieter, 2010), but in combination with EE-containing birth control pills has been associated with a synergistic increase in VTE risk (Pomp, Rosendaal, & Doggen, 2008) as well as large increases in risk of heart attack—for instance 20-fold higher risk in heavy smokers (Kuhl, 1999). The table below shows the influence of a selection of known risk factors for VTE:
Thrombophilias, heritable and acquired, exist in significant percentages of the population and can lead to large increases in blood clot risk (Lijfering, Rosendaal, & Cannegieter, 2010). Moreover, they are often if not usually unknown (Morimont, Dogné, & Douxfils, 2020). This is due to the fact that screening for heritable thrombophilias is mainly based on family history, which has low sensitivity and poor predictive value for identifying people with these abnormalities (Morimont, Dogné, & Douxfils, 2020). Hence, many people are at increased risk of blood clots without realizing it. The table below shows the prevalences of a variety of thrombophilic abnormalities and their impacts on blood clot risk.
Blood clots are considered to be a multicausal disease (Rosendaal, 2005). The risk of blood clots and associated cardiovascular complications with hormonal exposure is highest when multiple risk factors combine in a given individual. Under what are among the most extreme of circumstances in terms of risk—elderly people with cancer who are on high-dose oral synthetic estrogen therapy (e.g., DES)—blood clot incidence can be as high as 15 to 28% and overall incidence of cardiovascular complications as great as 35% (Phillips et al., 2014; Sciarria et al., 2014; Turo et al., 2014). These adverse effects contribute to substantial morbidity and incidence of death in these populations. Most people are however at nowhere near as great of risk. Risk factors like age are why pregnant women can have massive levels of estradiol and progesterone with relatively little issue whereas elderly cancer patients on high-dose oral synthetic estrogen therapy have a considerable risk of death.
In the VUMC studies that found 20- to 45-fold increased incidence of blood clots with high-dose EE and CPA over 5 to 10 years in transfeminine people, the absolute incidence of blood clots was approximately 6.3% (142/10,000 people per year) in the 1989 report and 5.5% (58/10,000 people per year) in the 1997 follow up (Asscheman, Gooren, & Eklund, 1989; van Kesteren et al., 1997; Asscheman et al., 2014; Goldstein et al., 2019; Min & Hopkins, 2021). In keeping with the known influence of age on blood clot risk, the absolute incidence was 2.1% in those under 40 years of age and 12% in those over 40 years of age in the 1989 study (Asscheman, Gooren, & Eklund, 1989; Asscheman et al., 2014). In about 70% of cases, there were—aside from age—no known risk factors for blood clots (Asscheman, Gooren, & Eklund, 1989; Asscheman et al., 2014). Following subsequent replacement of EE with low-to-moderate-dose transdermal estradiol in those over 40 years of age, the incidence of blood clots decreased substantially (with only one event occurring in the transdermal estradiol group) (van Kesteren et al., 1997; Asscheman et al., 2014; Min & Hopkins, 2021). A later study in 2013 by the Ghent University Hospital in Belgium observed a blood clot incidence of 5.1% in transfeminine people using mostly oral or transdermal estradiol with or without CPA over an average treatment period of 7.7 years (range 3 months to 35 years) (Wierckx et al., 2013; Min & Hopkins, 2021). Those who had blood clots often had other risk factors such as older age, smoking, immoblization due to surgery, or hypercoagulability (Wierckx et al., 2013; Min & Hopkins, 2021). In addition to cumulative exposure time, these studies further highlight the converging impact of multiple risk factors—with estrogen type, route, and dose, progestogen exposure, and age included among them—on the risk of blood clots.
Therapeutic Implications for Transfeminine People
Due to their greater risk of blood clots and cardiovascular problems, non-bioidentical estrogens like EE and CEEs are mostly no longer used in transfeminine people. Instead, estradiol, both in oral and non-oral forms, is used. Transgender clinical guidelines generally recommend keeping estradiol levels within normal physiological ranges for non-pregnant females of around 100 to 200 pg/mL regardless of whether the route of administration of estradiol is oral or non-oral (Aly, 2018). Higher estradiol levels are not currently known to have greater therapeutic benefit in terms of feminization or breast development (Nolan & Cheung, 2020). However, higher levels, in the range of 200 to 500 pg/mL, can provide additional therapeutic effect in the area of testosterone suppression—which can be indirectly beneficial to feminization if otherwise inadequate (Aly, 2018). Despite their recommendations for keeping estradiol levels in physiological ranges, transgender clinical guidelines notably recommend doses of estradiol ester injections that reach and even greatly exceed estradiol levels of 200 pg/mL (Aly, 2021).
Based on the available research (e.g., the risk of blood clots with lower doses, comparative SHBG increases), it would not be surprising if high-dose oral estradiol (e.g., 8 mg/day) had similar risk of blood clots as the relatively lower amounts of EE in birth control pills. The risk is likely to be particularly great in combination with progestogens (e.g., CPA). Due to its greater and unnecessary risk of blood clots relative to non-oral estradiol, oral estradiol should ideally be avoided in transfeminine people—particularly in those with risk factors for blood clots such as older age (e.g., >40 years) or concomitant progestogen use. However, the convenience of oral estradiol and its relative inexpensiveness (compared to e.g. transdermal forms) are significant advantages that will also be considered by transfeminine people and their clinicians. In contrast to oral estradiol, non-oral estradiol—with estradiol levels kept in physiological ranges of for instance 100 to 200 pg/mL—appears to have minimal to no risk of blood clots. Hence, non-oral estradiol at these levels can be used in transfeminine people with little concern.
In terms of higher estradiol levels delivered non-orally, the estimated 2-fold increase in risk of blood clots with estradiol levels of approximately 300 to 500 pg/mL (Sam, 2020) is notably lower than the average 4-fold increase in risk with widely used EE-containing birth control pills. Based on the usefulness of these levels for suppressing testosterone production and the widespread usage of EE-based birth control in cisgender women throughout the world, the degree of blood clot risk with high-dose non-oral estradiol, in reasonable amounts, could be considered therapeutically acceptable in transfeminine people (Haupt et al., 2020). This may be particularly true when high-dose non-oral estradiol monotherapy is compared to combination of estradiol with antiandrogens like spironolactone, CPA, or bicalutamide, which all have their own unique risks and drawbacks. In any case, as with oral estradiol, high estradiol levels with non-oral estradiol should ideally be avoided due to the additional risk they pose, and this is especially true in those with relevant risk factors for blood clots (e.g., older age). In addition, very high doses of non-oral estradiol resulting in estradiol levels above those required for testosterone suppression are difficult to justify as they pose further unnecessary risk and offer no clear additional therapeutic benefit.
Prevention of Blood Clots
The best way to prevent blood clots from happening is to avoid risk altogether. Avoiding use of oral estradiol, excessively high doses of non-oral estradiol, and progestogens when feasible and opting for safer therapeutic choices is recommended in this regard. In addition, avoiding use of such therapies in those with risk factors like older age (>40 years), known thrombophilic abnormalities, and sedentary lifestyle is advocated. Proactive behaviors like physical activity (e.g., walking, exercise), quitting smoking, and weight loss may help to reduce the risk of blood clots (Hibbs, 2008).
Certain anticoagulant and antiplatelet medications are used to help prevent blood clots in high-risk individuals. Examples include low-dose aspirin (Mekaj, Daci, & Mekaj, 2015; Matharu et al., 2020), direct factor Xa inhibitors like rivaroxaban (Xarelto) (Blondon, 2020), and direct thrombin inhibitors like dabigatran (Pradaxa), among others. Aspirin has been found to be effective in the prevention of blood clots (Mekaj, Daci, & Mekaj, 2015; Matharu et al., 2020) and has been recommended for use specifically in transfeminine people on hormone therapy (Feldman & Goldberg, 2006; Deutsch, 2016). However, evidence is limited and conflicting for prevention of blood clots related to hormone therapy (Grady et al., 2000; Cushman et al., 2004) and use of aspirin in transfeminine people for such purposes has been recommended against by others (Shatzel, Connelly, & DeLoughery, 2017). Rivaroxaban has been associated with more than completely offset risk of blood clots with oral menopausal hormonal therapy (Blondon, 2020). In any case, no anticoagulants are currently approved or well-supported for preventing risk of blood clots with hormone therapy. Accordingly, clinical guidelines state that there is insufficient evidence to guide decision-making in this area at this time (e.g., McLintock, 2014). It should also be cautioned that anticoagulants have side effects and risks of their own and should be used carefully.
Temporary discontinuation of estrogen therapy before surgery has traditionally been thought to help reduce the risk of blood clots during recovery based on theory and has been advised as well as mandated for transfeminine people undergoing surgical procedures (e.g., Asscheman et al., 2014). However, evidence is limited and inconclusive on this strategy at present and more research is needed to determine whether it is actually beneficial or not (Boskey, Taghinia, & Ganor, 2019; Nolan & Cheung, 2020; Haveles et al., 2021; Hontscharuk et al., 2021; Kozato et al., 2021; Nolan et al., 2021; Zucker, Reisman, & Safer, 2021). Recent studies have not found reduction in risk of blood clots with discontinuation of hormone therapy before surgery in transfeminine people but these studies have been underpowered and larger studies are needed (Blasdel et al., 2021). Temporarily stopping hormone therapy can be distressing for many transfeminine people and this should be weighed accordingly. A potential alternative to discontinuation of hormone therapy is temporary use of transdermal estradiol at physiological doses which has no known blood clot risk and is more likely to be safe.
Updates
Update 1: Langley et al. (2021) [PATCH Study Results]
In February 2021, a report on long-term cardiovascular outcomes for the Prostate Adenocarcinoma: TransCutaneous Hormones (PATCH) trial was published (Langley et al., 2021). The PATCH trial is a large ongoing phase 2/3 randomized controlled trial of high-dose transdermal estradiol patches versus GnRH agonists for the treatment of prostate cancer in men (Langley et al., 2021). The estradiol patch dosage employed is specifically three to four 100 μg/day FemSeven or Progynova TS patches (Langley et al., 2021). In the February 2021 report of the study, 1,694 men were enrolled and randomized, with 790 included in the analysis for the GnRH agonist group and 904 included in the analysis for the estradiol patch group (Langley et al., 2021).
In those given estradiol, the median estradiol level was around 215 pg/mL (5%–95% range ~100–550 pg/mL) (Langley et al., 2021). About 93% of the men in this group achieved suppression of testosterone levels into the castrate range (<50 ng/dL), which was notably equal to the rate of suppression in the GnRH agonist group (~93%) (Langley et al., 2021). However, actual testosterone levels—as opposed to rates of testosterone suppression—were not provided in this report and hence comparison between groups is unavailable for this metric (Langley et al., 2021). After about 4 years median follow up, there were no significant differences on a variety of cardiovascular outcomes between the estradiol group and the GnRH agonist group (Langley et al., 2021). Among these outcomes included VTE, thromboembolic stroke, and other arterial embolic events (Langley et al., 2021). These results are in contrast to previous large clinical trials of PEP in prostate cancer, which found increased cardiovascular morbidity and risk of VTE but notably involved higher estradiol levels than employed in the PATCH trial (Ockrim & Abel, 2009; Sam, 2020). Based on their promising safety findings, the PATCH researchers stated that transdermal estrogen should be reconsidered for the treatment of prostate cancer (Langley et al., 2021).
These findings are reassuring and suggest that limitedly high levels of estradiol (e.g., 200–300 pg/mL perhaps) may likewise be acceptably safe in terms of blood clot and cardiovascular risk in transfeminine people. It should be noted however that the sample size of the trial, while large relative to previous clinical studies in this area, was underpowered for assessing risk of blood clots—which are relatively rare events that require very large samples to thoroughly quantify. Studies precisely assessing blood clot risk in peri- and postmenopausal women have included tens of thousands of individuals for instance. As such, while substantial increases in risk are not likely based on this trial, smaller increases in risk still cannot be ruled out at this time. It should additionally be noted that the robust testosterone suppression at the used doses in this study might not generalize to transfeminine people as a whole, as the men were mostly elderly and testosterone levels are known to decrease with age.
Update 2: Totaro et al. (2021) and Kotamarti et al. (2021)
Totaro, M., Palazzi, S., Castellini, C., Parisi, A., D’Amato, F., Tienforti, D., Baroni, M. G., Francavilla, S., & Barbonetti, A. (2021). Risk of Venous Thromboembolism in Transgender People Undergoing Hormone Feminizing Therapy: A Prevalence Meta-Analysis and Meta-Regression Study. Frontiers in Endocrinology, 12, 741866. [DOI:10.3389/fendo.2021.741866]
This study is the largest of its kind that has been conducted to date. The meta-analysis included 18 studies totaling 11,542 transfeminine people on hormone therapy. The pooled prevalence of VTE was 2% with a 95% confidence interval of 1 to 3%. However, there was large variability between studies. In the meta-regression analysis, older age and longer length of estrogen therapy were significantly positively associated with VTE prevalence. When analysis was restricted to those greater than or equal to 37.5 years of age, the prevalence of VTE was 3% (95% CI: 0–5%). Conversely, in those less than 37.5 years of age, the prevalence of VTE was 0% (95% CI: 0–2%). VTE prevalence was 1% (95% CI: 0–3%) with greater than or equal to 4.4 years of estrogen therapy and was 0% (95% CI: 0–3%) with less than 4.4 years of estrogen therapy. With regard to the 0% estimates, it is not the case that there is truly no risk of VTE in these instances but rather it can be assumed that the risks are sufficiently low that the meta-analysis was not powered well enough to detect and quantify them.
A limitation of the meta-analysis was that subgroup analyses based on estrogen type (i.e., estradiol vs. CEEs vs. EE) and route (e.g., oral estrogens or oral estradiol vs. transdermal estradiol) were said to not be possible due to insufficient data and hence were not performed. However, another recent meta-analysis published in July 2021, which analyzed much of the same literature as Totaro et al. (2021), did perform subgroup analyses by estrogen type and route. This publication is as follows:
Kotamarti, V. S., Greige, N., Heiman, A. J., Patel, A., & Ricci, J. A. (2021). Risk for Venous Thromboembolism in Transgender Patients Undergoing Cross-Sex Hormone Treatment: A Systematic Review. The Journal of Sexual Medicine, 18(7), 1280–1291. [DOI:10.1016/j.jsxm.2021.04.006]
And this is what they reported in terms of subgroup analyses for estrogen type and route:
Because varying VTE rates have been reported with different estrogen regimens, analyses of VTE incidence were performed comparing oral or transdermal delivery, or the specific estrogen formulation. As many studies reported populations using mixed estrogen formulations or did not report the type of estrogen regimen, further statistical analysis could not be performed.
Route of estrogen administration appeared to play a role in the AMAB population. [Oral] estrogens (7 studies; 34.0 VTE per 10,000 person-years) vs transdermal estrogens (3 studies, 11.2 VTE per 10,000 person-years). Additionally, estrogen formulation also appeared to have a difference VTE incidence. Ethinyl estradiol was also associated with increased VTE incidence (3 studies, 293.1 VTE per 10,000 person-years) followed by conjugated equine estrogens (1 study, 49.0 VTE per 10,000 person-years) and estradiol valerate (4 studies, 31.5 VTE per 10,000 person-years).
It is unclear how accurate these precise numbers are due to the quality limitations of the underlying data. Moreover, antiandrogens (e.g., CPA) were not controlled for and as discussed by this article are likely to additionally influence VTE risk. In any case, the reported numbers are interesting and are in accordance with different estrogen types and routes varying in terms of VTE risk.
References
Abdul Sultan, A., West, J., Stephansson, O., Grainge, M. J., Tata, L. J., Fleming, K. M., Humes, D., & Ludvigsson, J. F. (2015). Defining venous thromboembolism and measuring its incidence using Swedish health registries: a nationwide pregnancy cohort study. BMJ Open, 5(11), e008864. [DOI:10.1136/bmjopen-2015-008864]
Abou-Ismail, M. Y., Citla Sridhar, D., & Nayak, L. (2020). Estrogen and thrombosis: A bench to bedside review. Thrombosis Research, 192, 40–51. [DOI:10.1016/j.thromres.2020.05.008]
Amitrano, L., Guardascione, M. A., Brancaccio, V., & Balzano, A. (2002). Coagulation Disorders in Liver Disease. Seminars in Liver Disease, 22(1), 83–96. [DOI:10.1055/s-2002-23205]
Anderson, G. L., Limacher, M., Assaf, A. R., Bassford, T., Beresford, S. A., Black, H., Bonds, D., Brunner, R., Brzyski, R., Caan, B., Chlebowski, R., Curb, D., Gass, M., Hays, J., Heiss, G., Hendrix, S., Howard, B. V., Hsia, J., Hubbell, A., Jackson, R., … & Women’s Health Initiative Steering Committee. (2004). Effects of Conjugated Equine Estrogen in Postmenopausal Women With Hysterectomy: The Women’s Health Initiative Randomized Controlled Trial. JAMA, 291(14), 1701–1712. [DOI:10.1001/jama.291.14.1701]
Arnold, J. D., Sarkodie, E. P., Coleman, M. E., & Goldstein, D. A. (2016). Incidence of Venous Thromboembolism in Transgender Women Receiving Oral Estradiol. The Journal of Sexual Medicine, 13(11), 1773–1777. [DOI:10.1016/j.jsxm.2016.09.001]
Asscheman, H., Gooren, L., & Eklund, P. (1989). Mortality and morbidity in transsexual patients with cross-gender hormone treatment. Metabolism, 38(9), 869–873. [DOI:10.1016/0026-0495(89)90233-3]
Asscheman, H., Giltay, E. J., Megens, J. A., de Ronde, W. (Pim), van Trotsenburg, M. A., & Gooren, L. J. (2011). A long-term follow-up study of mortality in transsexuals receiving treatment with cross-sex hormones. European Journal of Endocrinology, 164(4), 635–642. [DOI:10.1530/eje-10-1038]
Asscheman, H., T’Sjoen, G., Lemaire, A., Mas, M., Meriggiola, M. C., Mueller, A., Kuhn, A., Dhejne, C., Morel-Journel, N., & Gooren, L. J. (2013). Venous thrombo-embolism as a complication of cross-sex hormone treatment of male-to-female transsexual subjects: a review. Andrologia, 46(7), 791–795. [DOI:10.1111/and.12150]
Baber, R. J., Panay, N., & Fenton, A. (2016). 2016 IMS Recommendations on women’s midlife health and menopause hormone therapy. Climacteric, 19(2), 109–150. [DOI:10.3109/13697137.2015.1129166]
Back, D. J., & Rogers, S. M. (2007). Review: first-pass metabolism by the gastrointestinal mucosa. Alimentary Pharmacology & Therapeutics, 1(5), 339–357. [DOI:10.1111/j.1365-2036.1987.tb00634.x]
Bagot, C., Marsh, M., Whitehead, M., Sherwood, R., Roberts, L., Patel, R., & Arya, R. (2010). The effect of estrone on thrombin generation may explain the different thrombotic risk between oral and transdermal hormone replacement therapy. Journal of Thrombosis and Haemostasis, 8(8), 1736–1744. [DOI:10.1111/j.1538-7836.2010.03953.x]
Bagot, C., Leishman, E., Onyiaodike, C., Jordan, F., Gibson, V., & Freeman, D. (2019). Changes in laboratory markers of thrombotic risk early in the first trimester of pregnancy may be linked to an increase in estradiol and progesterone. Thrombosis Research, 178, 47–53. [DOI:10.1016/j.thromres.2019.03.015]
Baron, J. A., Gridley, G., Weiderpass, E., Nyren, O., & Linet, M. (1998). Venous thromboembolism and cancer. The Lancet, 351(9109), 1077–1080. [DOI:10.1016/s0140-6736(97)10018-6]
Bezwada, P., Shaikh, A., & Misra, D. (2017). The Effect of Transdermal Estrogen Patch Use on Cardiovascular Outcomes: A Systematic Review. Journal of Women’s Health, 26(12), 1319–1325. [DOI:10.1089/jwh.2016.6151]
Blanco-Molina, M., Lozano, M., Cano, A., Cristobal, I., Pallardo, L., & Lete, I. (2012). Progestin-only contraception and venous thromboembolism. Thrombosis Research, 129(5), e257–e262. [DOI:10.1016/j.thromres.2012.02.042]
Bland, L. B., Garzotto, M., DeLoughery, T. G., Ryan, C. W., Schuff, K. G., Wersinger, E. M., Lemmon, D., & Beer, T. M. (2005). Phase II study of transdermal estradiol in androgen-independent prostate carcinoma. Cancer, 103(4), 717–723. [DOI:10.1002/cncr.20857]
Blasdel, G., Shakir, N., Parker, A., Bluebond-Langner, R., & Zhao, L. (2021). Letter to the Editor from Blasdel et al: “No Venous Thromboembolism Increase Among Transgender Female Patients Remaining on Estrogen for Gender-affirming Surgery”. The Journal of Clinical Endocrinology & Metabolism, 106(9), e3783–e3784. [DOI:10.1210/clinem/dgab243]
Blondon, M. (2020). Update On Oral Contraception And Venous Thromboembolism. HemaSphere Educational Updates in Hematology Book: 25th Congress of the European Hematology Association, Virtual Edition 2020, 4(S2). European Hematology Association. [Google Scholar] [DOI:10.1097/HS9.0000000000000444] [PDF]
Boskey, E. R., Taghinia, A. H., & Ganor, O. (2019). Association of Surgical Risk With Exogenous Hormone Use in Transgender Patients. JAMA Surgery, 154(2), 159–169. [DOI:10.1001/jamasurg.2018.4598]
Canonico, M., Plu-Bureau, G., Lowe, G. D., & Scarabin, P. (2008). Hormone replacement therapy and risk of venous thromboembolism in postmenopausal women: systematic review and meta-analysis. BMJ, 336(7655), 1227–1231. [DOI:10.1136/bmj.39555.441944.be]
Canonico, M., Plu-Bureau, G., O’Sullivan, M. J., Stefanick, M. L., Cochrane, B., Scarabin, P., & Manson, J. E. (2014). Age at menopause, reproductive history, and venous thromboembolism risk among postmenopausal women. Menopause, 21(3), 214–220. [DOI:10.1097/gme.0b013e31829752e0]
Cassidy, A., & Minihane, A. (2017). The role of metabolism (and the microbiome) in defining the clinical efficacy of dietary flavonoids. The American Journal of Clinical Nutrition, 105(1), 10–22. [DOI:10.3945/ajcn.116.136051]
Chaireti, R., Gustafsson, K. M., Bystrom, B., Bremme, K., & Lindahl, T. L. (2013). Endogenous thrombin potential is higher during the luteal phase than during the follicular phase of a normal menstrual cycle. Human Reproduction, 28(7), 1846–1852. [DOI:10.1093/humrep/det092]
Choi, J., Kim, D., Park, S., Lee, H., Kim, K., Kim, K., Kim, M., Kim, S., & Kim, S. (2015). Anti-thrombotic effect of rutin isolated from Dendropanax morbifera Leveille. Journal of Bioscience and Bioengineering, 120(2), 181–186. [DOI:10.1016/j.jbiosc.2014.12.012]
Cleuren, A., Van der Linden, I., de Visser, Y., Wagenaar, G., Reitsma, P., & van Vlijmen, B. (2010). 17α‐Ethinylestradiol rapidly alters transcript levels of murine coagulation genes via estrogen receptor α. Journal of Thrombosis and Haemostasis, 8(8), 1838–1846. [DOI:10.1111/j.1538-7836.2010.03930.x]
Coelingh Bennink, H. J., Verhoeven, C., Dutman, A. E., & Thijssen, J. (2017). The use of high-dose estrogens for the treatment of breast cancer. Maturitas, 95, 11–23. [DOI:10.1016/j.maturitas.2016.10.010]
Coleman, E., Bockting, W., Botzer, M., Cohen-Kettenis, P., DeCuypere, G., Feldman, J., Fraser, L., Green, J., Knudson, G., Meyer, W. J., Monstrey, S., Adler, R. K., Brown, G. R., Devor, A. H., Ehrbar, R., Ettner, R., Eyler, E., Garofalo, R., Karasic, D. H., … & Zucker, K. (2012). [World Professional Association for Transgender Health (WPATH)] Standards of Care for the Health of Transsexual, Transgender, and Gender-Nonconforming People, Version 7. International Journal of Transgenderism, 13(4), 165–232. [DOI:10.1080/15532739.2011.700873] [URL] [PDF]
Conard, J., Plu-Bureau, G., Bahi, N., Horellou, M., Pelissier, C., & Thalabard, J. (2004). Progestogen-only contraception in women at high risk of venous thromboembolism. Contraception, 70(6), 437–441. [DOI:10.1016/j.contraception.2004.07.009]
Connelly, P. J., Marie Freel, E., Perry, C., Ewan, J., Touyz, R. M., Currie, G., & Delles, C. (2019). Gender-Affirming Hormone Therapy, Vascular Health and Cardiovascular Disease in Transgender Adults. Hypertension, 74(6), 1266–1274. [DOI:10.1161/hypertensionaha.119.13080]
Connors, J. M., & Middeldorp, S. (2019). Transgender patients and the role of the coagulation clinician. Journal of Thrombosis and Haemostasis, 17(11), 1790–1797. [DOI:10.1111/jth.14626]
Curb, J. D., Prentice, R. L., Bray, P. F., Langer, R. D., Van Horn, L., Barnabei, V. M., Bloch, M. J., Cyr, M. G., Gass, M., Lepine, L., Rodabough, R. J., Sidney, S., Uwaifo, G. I., & Rosendaal, F. R. (2006). Venous Thrombosis and Conjugated Equine Estrogen in Women Without a Uterus. Archives of Internal Medicine, 166(7), 772–772. [DOI:10.1001/archinte.166.7.772]
Cushman, M. (2004). Estrogen Plus Progestin and Risk of Venous Thrombosis. JAMA, 292(13), 1573–1580. [DOI:10.1001/jama.292.13.1573]
Deitcher, S. R., & Gomes, M. P. (2004). The risk of venous thromboembolic disease associated with adjuvant hormone therapy for breast carcinoma. Cancer, 101(3), 439–449. [DOI:10.1002/cncr.20347]
DeLoughery, T. G. (2011). Estrogen and thrombosis: Controversies and common sense. Reviews in Endocrine and Metabolic Disorders, 12(2), 77–84. [DOI:10.1007/s11154-011-9178-0]
Deutsch, M. B. (2016). Overview of feminizing hormone therapy. In Deutsch, M. B. (Ed.). Guidelines for the Primary and Gender-Affirming Care of Transgender and Gender Nonbinary People, 2nd Edition (pp. 26–48). San Francisco: University of California, San Francisco/UCSF Transgender Care. [URL] [PDF]
Dinger, J., Do Minh, T., & Heinemann, K. (2016). Impact of estrogen type on cardiovascular safety of combined oral contraceptives. Contraception, 94(4), 328–339. [DOI:10.1016/j.contraception.2016.06.010]
Dittrich, R., Binder, H., Cupisti, S., Hoffmann, I., Beckmann, M., & Mueller, A. (2005). Endocrine Treatment of Male-to-Female Transsexuals Using Gonadotropin-Releasing Hormone Agonist. Experimental and Clinical Endocrinology & Diabetes, 113(10), 586–592. [DOI:10.1055/s-2005-865900]
Douxfils, J., Morimont, L., & Bouvy, C. (2020). Oral Contraceptives and Venous Thromboembolism: Focus on Testing that May Enable Prediction and Assessment of the Risk. Seminars in Thrombosis and Hemostasis, 46(8), 872–886. [DOI:10.1055/s-0040-1714140]
Douxfils, J., Klipping, C., Duijkers, I., Kinet, V., Mawet, M., Maillard, C., Jost, M., Rosing, J., & Foidart, J. (2020). Evaluation of the effect of a new oral contraceptive containing estetrol and drospirenone on hemostasis parameters. Contraception, 102(6), 396–402. [DOI:10.1016/j.contraception.2020.08.015]
Dutra, E., Lee, J., Torbati, T., Garcia, M., Merz, C. N., & Shufelt, C. (2019). Cardiovascular implications of gender-affirming hormone treatment in the transgender population. Maturitas, 129, 45–49. [DOI:10.1016/j.maturitas.2019.08.010]
Eilertsen, A. L., Dahm, A. E., Høibraaten, E., Lofthus, C. M., Mowinckel, M., & Sandset, P. M. (2019). Relationship between sex hormone binding globulin and blood coagulation in women on postmenopausal hormone treatment. Blood Coagulation & Fibrinolysis, 30(1), 17–23. [DOI:10.1097/mbc.0000000000000784]
Eisenfeld, A. J., & Aten, R. F. (1979). Estrogen receptor in the mammalian liver. In Briggs, M. H., & Corbin, A. (Eds.). Advances in Steroid Biochemistry and Pharmacology, 7, 91–117. London: Academic Press. [Google Scholar] [PubMed]
Eisenfeld, A. J., & Aten, R. F. (1987). Estrogen receptors and androgen receptors in the mammalian liver. Journal of Steroid Biochemistry, 27(4–6), 1109–1118. [DOI:10.1016/0022-4731(87)90197-x]
Fabian, C. J., & Kimler, B. F. (2005). Selective Estrogen-Receptor Modulators for Primary Prevention of Breast Cancer. Journal of Clinical Oncology, 23(8), 1644–1655. [DOI:10.1200/jco.2005.11.005]
Fåhraeus, L., & Larsson-Cohn, U. (1982). Oestrogens, gonadotrophins and SHBG during oral and cutaneous administration of oestradiol-17β to menopausal women. Acta Endocrinologica, 101(4), 592–596. [DOI:10.1530/acta.0.1010592]
Feldman, J. L., & Goldberg, J. (2006). Transgender Primary Medical Care: Suggested Guidelines for Clinicians in British Columbia. crhc/csac/Transcend Transgender Support & Education Society/Vancouver Coastal Health. [Google Scholar] [PDF]
Franchini, M., & Mannucci, P. M. (2015). Classic thrombophilic gene variants. Thrombosis and Haemostasis, 114(11), 885–889. [DOI:10.1160/th15-02-0141]
Fruzzetti, F., & Cagnacci, A. (2018). Venous thrombosis and hormonal contraception: what’s new with estradiol-based hormonal contraceptives? Open Access Journal of Contraception, 9, 75–79. [DOI:10.2147/oajc.s179673]
Gerstman, B. B., Piper, J. M., Tomita, D. K., Ferguson, W. J., Stadel, B. V., & Lundin, F. E. (1991). Oral Contraceptive Estrogen Dose and the Risk of Deep Venous Thromboembolic Disease. American Journal of Epidemiology, 133(1), 32–37. [DOI:10.1093/oxfordjournals.aje.a115799]
Getahun, D., Nash, R., Flanders, W. D., Baird, T. C., Becerra-Culqui, T. A., Cromwell, L., Hunkeler, E., Lash, T. L., Millman, A., Quinn, V. P., Robinson, B., Roblin, D., Silverberg, M. J., Safer, J., Slovis, J., Tangpricha, V., & Goodman, M. (2018). Cross-sex Hormones and Acute Cardiovascular Events in Transgender Persons. Annals of Internal Medicine, 169(4), 205. [DOI:10.7326/m17-2785]
Gibney, J., Johannsson, G., Leung, K., & Ho, K. K. (2005). Comparison of the Metabolic Effects of Raloxifene and Oral Estrogen in Postmenopausal and Growth Hormone-Deficient Women. The Journal of Clinical Endocrinology & Metabolism, 90(7), 3897–3903. [DOI:10.1210/jc.2005-0173]
Gilbert, D. C., Duong, T., Sydes, M., Bara, A., Clarke, N., Abel, P., James, N., Langley, R., Parmar, M., & (2018). Transdermal oestradiol as a method of androgen suppression for prostate cancer within the STAMPEDE trial platform. BJU International, 121(5), 680–683. [DOI:10.1111/bju.14153]
Glintborg, D., T’Sjoen, G., Ravn, P., & Andersen, M. S. (2021). MANAGEMENT OF ENDOCRINE DISEASE: Optimal feminizing hormone treatment in transgender people. European Journal of Endocrinology, 185(2), R49–R63. [DOI:10.1530/eje-21-0059]
Goldstein, Z., Khan, M., Reisman, T., & Safer, J. D. (2019). Managing the risk of venous thromboembolism in transgender adults undergoing hormone therapy. Journal of Blood Medicine, 10, 209–216. [DOI:10.2147/jbm.s166780]
Gooren, L. J., & T’Sjoen, G. (2018). Endocrine treatment of aging transgender people. Reviews in Endocrine and Metabolic Disorders, 19(3), 253–262. [DOI:10.1007/s11154-018-9449-0]
Gourdy, P., Bachelot, A., Catteau-Jonard, S., Chabbert-Buffet, N., Christin-Maître, S., Conard, J., Fredenrich, A., Gompel, A., Lamiche-Lorenzini, F., Moreau, C., Plu-Bureau, G., Vambergue, A., Vergès, B., & Kerlan, V. (2012). Hormonal contraception in women at risk of vascular and metabolic disorders: Guidelines of the French Society of Endocrinology. Annales d’Endocrinologie, 73(5), 469–487. [DOI:10.1016/j.ando.2012.09.001]
Grady, D., Wenger, N. K., Herrington, D., Khan, S., Furberg, C., Hunninghake, D., Vittinghoff, E., Hulley, S., & (2000). Postmenopausal Hormone Therapy Increases Risk for Venous Thromboembolic Disease: The Heart and Estrogen/progestin Replacement Study. Annals of Internal Medicine, 132(9), 689–696. [DOI:10.7326/0003-4819-132-9-200005020-00002]
Grandi, G., Facchinetti, F., & Bitzer, J. (2017). Estradiol in hormonal contraception: real evolution or just same old wine in a new bottle? The European Journal of Contraception & Reproductive Health Care, 22(4), 245–246. [DOI:10.1080/13625187.2017.1372571]
Grandi, G., Barra, F., Ferrero, S., & Facchinetti, F. (2019). Estradiol in non-oral hormonal contraception: a “long and winding road”. Expert Review of Endocrinology & Metabolism, 14(3), 153–155. [DOI:10.1080/17446651.2019.1604217]
Grandi, G., Del Savio, M. C., Lopes da Silva-Filho, A., & Facchinetti, F. (2020). Estetrol (E4): the new estrogenic component of combined oral contraceptives. Expert Review of Clinical Pharmacology, 13(4), 327–330. [DOI:10.1080/17512433.2020.1750365]
Grandi, G., Facchinetti, F., & Bitzer, J. (2022). Confirmation of the safety of combined oral contraceptives containing oestradiol on the risk of venous thromboembolism. The European Journal of Contraception & Reproductive Health Care, 27(2), 83–84. [DOI:10.1080/13625187.2022.2029397]
Grossmann, M., Wierman, M. E., Angus, P., & Handelsman, D. J. (2018). Reproductive Endocrinology of Nonalcoholic Fatty Liver Disease. Endocrine Reviews, 40(2), 417–446. [DOI:10.1210/er.2018-00158]
Hammond, G. L. (2017). Sex Hormone-Binding Globulin and the Metabolic Syndrome. In Winters, S. J., & Huhtaniemi, I. T. (Eds.). Male Hypogonadism: Basic, Clinical and Therapeutic Principles, 2nd Edition (pp. 305–324). Cham: Springer. [DOI:10.1007/978-3-319-53298-1_15]
Hannaford, P. C., Iversen, L., Macfarlane, T. V., Elliott, A. M., Angus, V., & Lee, A. J. (2010). Mortality among contraceptive pill users: cohort evidence from Royal College of General Practitioners’ Oral Contraception Study. BMJ, 340, c927. [DOI:10.1136/bmj.c927]
Haupt, C., Henke, M., Kutschmar, A., Hauser, B., Baldinger, S., Saenz, S. R., & Schreiber, G. (2020). Antiandrogen or estradiol treatment or both during hormone therapy in transitioning transgender women. Cochrane Database of Systematic Reviews, 2020(11), CD013138. [DOI:10.1002/14651858.cd013138.pub2]
Haveles, C. S., Wang, M. M., Arjun, A., Zaila, K. E., & Lee, J. C. (2020). Effect of Cross-Sex Hormone Therapy on Venous Thromboembolism Risk in Male-to-Female Gender-Affirming Surgery. Annals of Plastic Surgery, 86(1), 109–114. [DOI:10.1097/sap.0000000000002300]
Hedlund, P. O., Johansson, R., Damber, J. E., Hagerman, I., Henriksson, P., Iversen, P., Klarskov, P., Mogensen, P., Rasmussen, F., & Varenhorst, E. (2011). Significance of pretreatment cardiovascular morbidity as a risk factor during treatment with parenteral oestrogen or combined androgen deprivation of 915 patients with metastasized prostate cancer: Evaluation of cardiovascular events in a randomized trial. Scandinavian Journal of Urology and Nephrology, 45(5), 346–353. [DOI:10.3109/00365599.2011.585820]
Heit, J. A., Silverstein, M. D., Mohr, D. N., Petterson, T. M., O’Fallon, W. M., & Melton, L. J. (2000). Risk Factors for Deep Vein Thrombosis and Pulmonary Embolism. Archives of Internal Medicine, 160(6), 809–815. [DOI:10.1001/archinte.160.6.809]
Heit, J. A., Spencer, F. A., & White, R. H. (2016). The epidemiology of venous thromboembolism. Journal of Thrombosis and Thrombolysis, 41(1), 3–14. [DOI:10.1007/s11239-015-1311-6]
Hembree, W. C., Cohen-Kettenis, P. T., Gooren, L., Hannema, S. E., Meyer, W. J., Murad, M. H., Rosenthal, S. M., Safer, J. D., Tangpricha, V., & T’Sjoen, G. G. (2017). Endocrine Treatment of Gender-Dysphoric/Gender-Incongruent Persons: An Endocrine Society* Clinical Practice Guideline. The Journal of Clinical Endocrinology & Metabolism, 102(11), 3869–3903. [DOI:10.1210/jc.2017-01658]
Hemelaar, M., van der Mooren, M. J., Rad, M., Kluft, C., & Kenemans, P. (2008). Effects of non-oral postmenopausal hormone therapy on markers of cardiovascular risk: a systematic review. Fertility and Sterility, 90(3), 642–672. [DOI:10.1016/j.fertnstert.2007.07.1298]
Hibbs, D. (2008). Hormone replacement and the treatment of the transgender patient: A critical literature review. de Chesnay, M., & Anderson, B. (Eds.). Caring for the Vulnerable: Perspectives in Nursing Theory, Practice, and Research, 2nd Edition (pp. 351–362). Sudbury, Massachusetts: Jones & Barlett. [Google Scholar] [Google Books]
Higdon, J., Drake, V. J., Delage, B., & Crozier, A. (2016). Flavonoids. Corvallis, Oregon: Micronutrient Information Center, Linus Pauling Institute, Oregon State University. [URL]
Høibraaten, E., Qvigstad, E., Arnesen, H., Larsen, S., Wickstrøm, E., & Sandset, P. M. (2000). Increased Risk of Recurrent Venous Thromboembolism during Hormone Replacement Therapy. Thrombosis and Haemostasis, 84(12), 961–967. [DOI:10.1055/s-0037-1614156]
Høibraaten, E., Qvigstad, E., Andersen, T. O., Mowinckel, M., & Sandset, P. M. (2001). The Effects of Hormone Replacement Therapy (HRT) on Hemostatic Variables in Women with Previous Venous Thromboembolism – Results from a Randomized, Double-Blind, Clinical Trial. Thrombosis and Haemostasis, 85(5), 775–781. [DOI:10.1055/s-0037-1615717]
Holmegard, H., Nordestgaard, B., Schnohr, P., Tybjærg‐Hansen, A., & Benn, M. (2014). Endogenous sex hormones and risk of venous thromboembolism in women and men. Journal of Thrombosis and Haemostasis, 12(3), 297–305. [DOI:10.1111/jth.12484]
Hontscharuk, R., Alba, B., Manno, C., Pine, E., Deutsch, M. B., Coon, D., & Schechter, L. (2021). Perioperative Transgender Hormone Management: Avoiding Venous Thromboembolism and Other Complications. Plastic & Reconstructive Surgery, 147(4), 1008–1017. [DOI:10.1097/prs.0000000000007786]
Hugon-Rodin, J., Alhenc-Gelas, M., Hemker, H. C., Brailly-Tabard, S., Guiochon-Mantel, A., Plu-Bureau, G., & Scarabin, P. (2016). Sex hormone-binding globulin and thrombin generation in women using hormonal contraception. Biomarkers, 22(1), 81–85. [DOI:10.1080/1354750x.2016.1204010]
Hulley, S. (1998). Randomized Trial of Estrogen Plus Progestin for Secondary Prevention of Coronary Heart Disease in Postmenopausal Women. JAMA, 280(7), 605–613. [DOI:10.1001/jama.280.7.605]
Iqbal, J., Ginsburg, O. M., Wijeratne, T. D., Howell, A., Evans, G., Sestak, I., & Narod, S. A. (2012). Endometrial cancer and venous thromboembolism in women under age 50 who take tamoxifen for prevention of breast cancer: A systematic review. Cancer Treatment Reviews, 38(4), 318–328. [DOI:10.1016/j.ctrv.2011.06.009]
Irwig, M. S. (2018). Cardiovascular health in transgender people. Reviews in Endocrine and Metabolic Disorders, 19(3), 243–251. [DOI:10.1007/s11154-018-9454-3]
Iwamoto, S. J., Defreyne, J., Rothman, M. S., Van Schuylenbergh, J., Van de Bruaene, L., Motmans, J., & T’Sjoen, G. (2019). Health considerations for transgender women and remaining unknowns: a narrative review. Therapeutic Advances in Endocrinology and Metabolism, 10, 204201881987116. [DOI:10.1177/2042018819871166]
Jasuja, R., Passam, F. H., Kennedy, D. R., Kim, S. H., van Hessem, L., Lin, L., Bowley, S. R., Joshi, S. S., Dilks, J. R., Furie, B., Furie, B. C., & Flaumenhaft, R. (2012). Protein disulfide isomerase inhibitors constitute a new class of antithrombotic agents. Journal of Clinical Investigation, 122(6), 2104–2113. [DOI:10.1172/jci61228]
Jensen, E. V., Jacobson, H. I., Walf, A. A., & Frye, C. A. (2010). Estrogen action: A historic perspective on the implications of considering alternative approaches. Physiology & Behavior, 99(2), 151–162. [DOI:10.1016/j.physbeh.2009.08.013]
Kaemmle, L. M., Stadler, A., Janka, H., von Wolff, M., & Stute, P. (2022). The impact of micronized progesterone on cardiovascular events – a systematic review. Climacteric, 25(4), 327–336. [DOI:10.1080/13697137.2021.2022644]
Kasum, M., Danolić, D., Orešković, S., Ježek, D., Beketić-Orešković, L., & Pekez, M. (2014). Thrombosis following ovarian hyperstimulation syndrome. Gynecological Endocrinology, 30(11), 764–768. [DOI:10.3109/09513590.2014.927858]
Keenan, L., Kerr, T., Duane, M., & Van Gundy, K. (2018). Systematic Review of Hormonal Contraception and Risk of Venous Thrombosis. The Linacre Quarterly, 85(4), 470–477. [DOI:10.1177/0024363918816683]
Kerlan, V., Nahoul, K., Martelot, M., & Bercovici, J. (1994). Longitudinal study of maternal plasma bioavailable testosterone and androstanediol glucuronide levels during pregnancy. Clinical Endocrinology, 40(2), 263–267. [DOI:10.1111/j.1365-2265.1994.tb02478.x]
Khan, J., Schmidt, R. L., Spittal, M. J., Goldstein, Z., Smock, K. J., & Greene, D. N. (2019). Venous Thrombotic Risk in Transgender Women Undergoing Estrogen Therapy: A Systematic Review and Metaanalysis. Clinical Chemistry, 65(1), 57–66. [DOI:10.1373/clinchem.2018.288316]
Kitamura, T. (2001). Necessity of re‐evaluation of estramustine phosphate sodium (EMP) as a treatment option for first‐line monotherapy in advanced prostate cancer. International Journal of Urology, 8(2), 33–36. [DOI:10.1046/j.1442-2042.2001.00254.x]
Klil-Drori, A. J., Yin, H., Tagalakis, V., Aprikian, A., & Azoulay, L. (2016). Androgen Deprivation Therapy for Prostate Cancer and the Risk of Venous Thromboembolism. European Urology, 70(1), 56–61. [DOI:10.1016/j.eururo.2015.06.022]
Kohli, M., & McClellan, J. (2001). Parenteral Estrogen Therapy in Advanced Prostate Cancer: Retrospective Analysis of Intra-Muscular Estradiol Valerate in “Hormone Refractory” Prostate Disease. In Grunberg, S. M. (Ed.). Proceedings of the American Society of Clinical Oncology [Proc Am Soc Clin Oncol / Proceedings of ASCO], 20 [Thirty-Seventh Annual Meeting of the American Society of Clinical Oncology, May 12–15, 2001, San Francisco, California], 164b–164b (abstract no. 2407). Baltimore: Lippincott Williams & Wilkins. [ISSN:1081-0641] [ISBN-10:0-9664495-3-3] [Google Scholar] [WorldCat 1] [WorldCat 2] [WorldCat 3] [PDF]
Kohli, M., Alikhan, M. A., Spencer, H. J., & Carter, G. (2004). Phase I trial of intramuscular estradiol valerate (I/M-E) in hormone refractory prostate cancer. Journal of Clinical Oncology, 22(14 Suppl) [40th Annual Meeting of the American Society of Clinical Oncology: June 5–8, 2004, Ernest N. Morial Convention Center, New Orleans, Louisiana, Annual Meeting Proceedings], 436–436 (abstract no. 4726). [DOI:10.1200/jco.2004.22.90140.4726] [Google Books] [PDF]
Kohli, M. (2006). Phase II study of transdermal estradiol in androgen-independent prostate carcinoma. Cancer, 106(1), 234–235. [DOI:10.1002/cncr.21528]
Konkle, B. A., & Sood, S. L. (2019). Thrombotic Risk of Contraceptives and Other Hormonal Therapies. In Kitchens, C. S., Kessler, C. M., Konkle, B. A., Streiff, M. B., & Garcia, D. A. (Eds.). Consultative Hemostasis and Thrombosis, 4th Edition (pp. 637–650). Philadelphia: Elsevier. [DOI:10.1016/b978-0-323-46202-0.00031-5]
Kotamarti, V. S., Greige, N., Heiman, A. J., Patel, A., & Ricci, J. A. (2021). Risk for Venous Thromboembolism in Transgender Patients Undergoing Cross-Sex Hormone Treatment: A Systematic Review. The Journal of Sexual Medicine, 18(7), 1280–1291. [DOI:10.1016/j.jsxm.2021.04.006]
Kozato, A., Fox, G. W., Yong, P. C., Shin, S. J., Avanessian, B. K., Ting, J., Ling, Y., Karim, S., Safer, J. D., & Pang, J. H. (2021). No Venous Thromboembolism Increase Among Transgender Female Patients Remaining on Estrogen for Gender-Affirming Surgery. The Journal of Clinical Endocrinology & Metabolism, 106(4), 1586–1590. [DOI:10.1210/clinem/dgaa966]
Kronawitter, D., Gooren, L. J., Zollver, H., Oppelt, P. G., Beckmann, M. W., Dittrich, R., & Mueller, A. (2009). Effects of transdermal testosterone or oral dydrogesterone on hypoactive sexual desire disorder in transsexual women: results of a pilot study. European Journal of Endocrinology, 161(2), 363–368. [DOI:10.1530/eje-09-0265] [Table]
Kuhl, H. (1990). Ovulationshemmer: Die Bedeutung der Östrogendosis. [Ovulation Preventives: The Significance of the Estrogen Dose. / Ovulation Inhibitors: The Significance of Estrogen Dose.] Geburtshilfe und Frauenheilkunde, 50(12), 910–922. [Google Scholar 1] [Google Scholar 2] [PubMed] [DOI:10.1055/s-2008-1026392] [Translation]
Kuhl, H. (1996). Effects of progestogens on haemostasis. Maturitas, 24(1–2), 1–19. [DOI:10.1016/0378-5122(96)00994-2]
Kuhl, H. (1997). Metabolische Effekte der Östrogene und Gestagene. [Metabolic Effects of Estrogens and Progestogens.] Der Gynäkologe, 30(4), 357–369. [DOI:10.1007/pl00003042]
Kuhl, H. (1998). Adverse effects of estrogen treatment: natural vs. synthetic estrogens. In Lippert, T. H., Mueck, A. O., & Ginsburg, J. (Eds.). Sex Steroids and the Cardiovascular System: The Proceedings of the 1st Interdisciplinary Workshop, Tuebingen, Germany, October 1996. Parthenon Publishing Group, New York, London (pp. 201–210). London/New York: Parthenon. [Google Scholar] [Google Books] [PDF]
Kuhl, H. (1999). Hormonal contraception. In Oettel, M., & Schillinger, E. (Eds.). Estrogens and Antiestrogens II: Pharmacology and Clinical Application of Estrogens and Antiestrogen (Handbook of Experimental Pharmacology, Volume 135, Part 2) (pp. 363–407). Berlin/Heidelberg: Springer. [DOI:10.1007/978-3-642-60107-1_18]
Kuhl, H. (2005). Pharmacology of Estrogens and Progestogens: Influence of Different Routes of Administration. Climacteric, 8(Suppl 1), 3–63. [DOI:10.1080/13697130500148875] [PDF]
Kuhl, H., & Stevenson, J. (2006). The effect of medroxyprogesterone acetate on estrogen-dependent risks and benefits – an attempt to interpret the Women’s Health Initiative results. Gynecological Endocrinology, 22(6), 303–317. [DOI:10.1080/09513590600717368]
Langley, R. E., Cafferty, F. H., Alhasso, A. A., Rosen, S. D., Sundaram, S. K., Freeman, S. C., Pollock, P., Jinks, R. C., Godsland, I. F., Kockelbergh, R., Clarke, N. W., Kynaston, H. G., Parmar, M. K., & Abel, P. D. (2013). Cardiovascular outcomes in patients with locally advanced and metastatic prostate cancer treated with luteinising-hormone-releasing-hormone agonists or transdermal oestrogen: the randomised, phase 2 MRC PATCH trial (PR09). The Lancet Oncology, 14(4), 306–316. [DOI:10.1016/s1470-2045(13)70025-1]
Langley, R. E., Gilbert, D. C., Duong, T., Clarke, N. W., Nankivell, M., Rosen, S. D., Mangar, S., Macnair, A., Sundaram, S. K., Laniado, M. E., Dixit, S., Madaan, S., Manetta, C., Pope, A., Scrase, C. D., Mckay, S., Muazzam, I. A., Collins, G. N., Worlding, J., Williams, S. T., Paez, E., Robinson, A., McFarlane, J., Deighan, J. V., Marshall, J., Forcat, S., Weiss, M., Kockelbergh, R., Alhasso, A., Kynaston, H., & Parmar, M. (2021). Transdermal oestradiol for androgen suppression in prostate cancer: long-term cardiovascular outcomes from the randomised Prostate Adenocarcinoma Transcutaneous Hormone (PATCH) trial programme. The Lancet, 397(10274), 581–591. [DOI:10.1016/s0140-6736(21)00100-8]
Lax, E. (1987). Mechanisms of physiological and pharmacological sex hormone action on the mammalian liver. Journal of Steroid Biochemistry, 27(4–6), 1119–1128. [DOI:10.1016/0022-4731(87)90198-1]
Lidegaard, Ø. (2014). Hormonal contraception, thrombosis and age. Expert Opinion on Drug Safety, 13(10), 1353–1360. [DOI:10.1517/14740338.2014.950654]
Lijfering, W. M., Rosendaal, F. R., & Cannegieter, S. C. (2010). Risk factors for venous thrombosis - current understanding from an epidemiological point of view. British Journal of Haematology, 149(6), 824–833. [DOI:10.1111/j.1365-2141.2010.08206.x]
Lim, H. Y., Leemaqz, S. Y., Torkamani, N., Grossmann, M., Zajac, J. D., Nandurkar, H., Ho, P., & Cheung, A. S. (2020). Global Coagulation Assays in Transgender Women on Oral and Transdermal Estradiol Therapy. The Journal of Clinical Endocrinology & Metabolism, 105(7), e2369–e2377. [DOI:10.1210/clinem/dgaa262]
Luria, M. H. (1989). Estrogen and coronary arterial disease in men. International Journal of Cardiology, 25(2), 159–166. [DOI:10.1016/0167-5273(89)90102-2]
Ma, Y., Zeng, M., Sun, R., & Hu, M. (2015). Disposition of Flavonoids Impacts their Efficacy and Safety. Current Drug Metabolism, 15(9), 841–864. [DOI:10.2174/1389200216666150206123719]
Machin, N., & Ragni, M. V. (2020). Hormones and thrombosis: risk across the reproductive years and beyond. Translational Research, 225, 9–19. [DOI:10.1016/j.trsl.2020.06.011]
Mammen, E. F. (1992). Coagulation Abnormalities in Liver Disease. Hematology/Oncology Clinics of North America, 6(6), 1247–1257. [DOI:10.1016/s0889-8588(18)30273-9]
Mantha, S., Karp, R., Raghavan, V., Terrin, N., Bauer, K. A., & Zwicker, J. I. (2012). Assessing the risk of venous thromboembolic events in women taking progestin-only contraception: a meta-analysis. BMJ, 345, e4944. [DOI:10.1136/bmj.e4944]
Martinelli, I., Passamonti, S. M., & Bucciarelli, P. (2014). Thrombophilic states. In Biller, J., & Ferro, J. M. (Eds.). Neurologic Aspects of Systemic Disease Part II (Handbook of Clinical Neurology, Volume 120) (pp. 1061–1071). Philadelphia: Elsevier. [DOI:10.1016/b978-0-7020-4087-0.00071-1]
Martinez-Zapata, M. J., Vernooij, R. W., Uriona Tuma, S. M., Stein, A. T., Moreno, R. M., Vargas, E., Capellà, D., & Bonfill Cosp, X. (2016). Phlebotonics for venous insufficiency. Cochrane Database of Systematic Reviews, 2016(4), CD003229. [DOI:10.1002/14651858.cd003229.pub3]
Matharu, G. S., Kunutsor, S. K., Judge, A., Blom, A. W., & Whitehouse, M. R. (2020). Clinical Effectiveness and Safety of Aspirin for Venous Thromboembolism Prophylaxis After Total Hip and Knee Replacement. JAMA Internal Medicine, 180(3), 376–384. [DOI:10.1001/jamainternmed.2019.6108]
McLintock, C. (2014). Thromboembolism in pregnancy: Challenges and controversies in the prevention of pregnancy-associated venous thromboembolism and management of anticoagulation in women with mechanical prosthetic heart valves. Best Practice & Research Clinical Obstetrics & Gynaecology, 28(4), 519–536. [DOI:10.1016/j.bpobgyn.2014.03.001]
Mekaj, A., Mekaj, Y., & Daci, F. (2015). New insights into the mechanisms of action of aspirin and its use in the prevention and treatment of arterial and venous thromboembolism. Therapeutics and Clinical Risk Management, 11, 1449–1456. [DOI:10.2147/tcrm.s92222]
Mellinger, G. T., Bailar, J. C., Arduino, L. J., & the Veterans Administration Cooperative Urological Research Group. (1967). Treatment and survival of patients with cancer of the prostate. The Veterans Administration Co-operative Urological Research Group. Surgery Gynecology & Obstetrics, 124(5), 1011–1017. [Google Scholar] [PubMed]
Meng, Y., Jiang, H., Chen, A., Lu, F., Yang, H., Shen, M. Z., Sun, D., Shao, Q., & Fotherby, K. (1990). Hemostatic changes in women using a monthly injectable contraceptive for one year. Contraception, 42(4), 455–466. [DOI:10.1016/0010-7824(90)90052-w]
Mikkola, A., Ruutu, M., Aro, J., Rannikko, S., & Salo, J. (1999). The role of parenteral polyestradiol phosphate in the treatment of advanced prostatic cancer on the threshold of the new millennium. Annales Chirurgiae et Gynaecologiae, 88(1), 18–21. [Google Scholar] [PubMed] [PDF]
Min, L. L., & Hopkins, R. (2021). Endocrinological Care for Patients Undergoing Gender Affirmation (Including Risk of Thromboembolic Events). In Nikolavsky, D., & Blakely, S. A. (Eds.). Urological Care for the Transgender Patient: A Comprehensive Guide (pp. 23–36). Cham: Springer. [DOI:10.1007/978-3-030-18533-6_3]
Mohammed, K., Abu Dabrh, A. M., Benkhadra, K., Al Nofal, A., Carranza Leon, B. G., Prokop, L. J., Montori, V. M., Faubion, S. S., & Murad, M. H. (2015). Oral vs Transdermal Estrogen Therapy and Vascular Events: A Systematic Review and Meta-Analysis. The Journal of Clinical Endocrinology & Metabolism, 100(11), 4012–4020. [DOI:10.1210/jc.2015-2237]
Montagnana, M., Favaloro, E. J., Franchini, M., Guidi, G. C., & Lippi, G. (2009). The role of ethnicity, age and gender in venous thromboembolism. Journal of Thrombosis and Thrombolysis, 29(4), 489–496. [DOI:10.1007/s11239-009-0365-8]
Moores, L., Bilello, K. L., & Murin, S. (2004). Sex and gender issues and venous thromboembolism. Clinics in Chest Medicine, 25(2), 281–297. [DOI:10.1016/j.ccm.2004.01.013]
Morimont, L., Dogné, J., & Douxfils, J. (2020). Letter to the Editors-in-Chief in response to the article of Abou-Ismail, et al. entitled “Estrogen and thrombosis: A bench to bedside review” (Thrombosis Research 192 (2020) 40–51). Thrombosis Research, 193, 221–223. [DOI:10.1016/j.thromres.2020.08.006]
Morimont, L., Haguet, H., Dogné, J., Gaspard, U., & Douxfils, J. (2021). Combined Oral Contraceptives and Venous Thromboembolism: Review and Perspective to Mitigate the Risk. Frontiers in Endocrinology, 12, 769187. [DOI:10.3389/fendo.2021.769187]
Morling, J. R., Broderick, C., Yeoh, S. E., & Kolbach, D. N. (2018). Rutosides for treatment of post-thrombotic syndrome. Cochrane Database of Systematic Reviews, 2018(11), CD005625. [DOI:10.1002/14651858.cd005625.pub4]
Mueller, A., Dittrich, R., Binder, H., Kuehnel, W., Maltaris, T., Hoffmann, I., & Beckmann, M. W. (2005). High dose estrogen treatment increases bone mineral density in male-to-female transsexuals receiving gonadotropin-releasing hormone agonist in the absence of testosterone. European Journal of Endocrinology, 153(1), 107–113. [DOI:10.1530/eje.1.01943]
Mueller, A., Binder, H., Cupisti, S., Hoffmann, I., Beckmann, M., & Dittrich, R. (2006). Effects on the Male Endocrine System of Long-term Treatment with Gonadotropin-releasing Hormone Agonists and Estrogens in Male-to-Female Transsexuals. Hormone and Metabolic Research, 38(3), 183–187. [DOI:10.1055/s-2006-925198]
Mueller, A., Zollver, H., Kronawitter, D., Oppelt, P. G., Claassen, T., Hoffmann, I., Beckmann, M. W., & Dittrich, R. (2011). Body composition and bone mineral density in male-to-female transsexuals during cross-sex hormone therapy using gonadotrophin-releasing hormone agonist. Experimental and Clinical Endocrinology & Diabetes, 119(2), 95–100. [DOI:10.1055/s-0030-1255074] [Table]
Nachtigall, L. E., Raju, U., Banerjee, S., Wan, L., & Levitz, M. (2000). Serum Estradiol-Binding Profiles in Postmenopausal Women Undergoing Three Common Estrogen Replacement Therapies. Menopause, 7(4), 243–250. [DOI:10.1097/00042192-200007040-00006]
Nelson, M. D., Szczepaniak, L. S., Wei, J., Szczepaniak, E., Sánchez, F. J., Vilain, E., Stern, J. H., Bergman, R. N., Bairey Merz, C. N., & Clegg, D. J. (2016). Transwomen and the Metabolic Syndrome: Is Orchiectomy Protective? Transgender Health, 1(1), 165–171. [DOI:10.1089/trgh.2016.0016]
Nolan, B. J., & Cheung, A. S. (2020). Estradiol Therapy in the Perioperative Period: Implications for Transgender People Undergoing Feminizing Hormone Therapy. The Yale Journal of Biology and Medicine, 93(4), 539–548. [PubMed] [PubMed Central]
Nolan, B. J., & Cheung, A. S. (2021). Relationship Between Serum Estradiol Concentrations and Clinical Outcomes in Transgender Individuals Undergoing Feminizing Hormone Therapy: A Narrative Review. Transgender Health, 6(3), 125–131. [DOI:10.1089/trgh.2020.0077]
Nolan, I. T., Haley, C., Morrison, S. D., Pannucci, C. J., & Satterwhite, T. (2021). Estrogen Continuation and Venous Thromboembolism in Penile Inversion Vaginoplasty. The Journal of Sexual Medicine, 18(1), 193–200. [DOI:10.1016/j.jsxm.2020.10.018]
Ockrim, J., & Abel, P. D. (2009). Androgen deprivation therapy for prostate cancer – the potential of parenteral estrogen. Central European Journal of Urology, 62, 132–140. [DOI:10.5173/ceju.2009.03.art1]
Odlind, V., Milsom, I., Persson, I., & Victor, A. (2002). Can changes in sex hormone binding globulin predict the risk of venous thromboembolism with combined oral contraceptive pills?: A discussion based on recent recommendations from the European agency for evaluation of medicinal products regarding third generation oral contraceptive pills. Acta Obstetricia et Gynecologica Scandinavica, 81(6), 482–490. [DOI:10.1080/j.1600-0412.2002.810603.x] [URL]
Oger, E., & (2000). Incidence of Venous Thromboembolism: A Community-based Study in Western France. Thrombosis and Haemostasis, 83(5), 657–660. [DOI:10.1055/s-0037-1613887]
Ohlander, S. J., Varghese, B., & Pastuszak, A. W. (2018). Erythrocytosis Following Testosterone Therapy. Sexual Medicine Reviews, 6(1), 77–85. [DOI:10.1016/j.sxmr.2017.04.001]
Olié, V., Canonico, M., & Scarabin, P. (2010). Risk of venous thrombosis with oral versus transdermal estrogen therapy among postmenopausal women. Current Opinion in Hematology, 17(5), 457–463. [DOI:10.1097/moh.0b013e32833c07bc]
Olié, V., Plu-Bureau, G., Conard, J., Horellou, M., Canonico, M., & Scarabin, P. (2011). Hormone therapy and recurrence of venous thromboembolism among postmenopausal women. Menopause, 18(5), 488–493. [DOI:10.1097/gme.0b013e3181f9f7c3]
Oliver-Williams, C., Glisic, M., Shahzad, S., Brown, E., Pellegrino Baena, C., Chadni, M., Chowdhury, R., Franco, O. H., & Muka, T. (2018). The route of administration, timing, duration and dose of postmenopausal hormone therapy and cardiovascular outcomes in women: a systematic review. Human Reproduction Update, 25(2), 257–271. [DOI:10.1093/humupd/dmy039]
Olov Hedlund, P., Damber, J., Hagerman, I., Haukaas, S., Henriksson, P., Iversen, P., Johansson, R., Klarskov, P., Lundbeck, F., Rasmussen, F., Varenhorst, E., Viitanen, J., Olov Hedlund, P., Damber, J., Hagerman, I., Haukaas, S., Henriksson, P., Iversen, P., Johansson, R., Klarskov, P., Lundbeck, F., Rasmussen, F., Varenhorst, E., Viitanen, J., & The SPCG-5 Study Group. (2008). Parenteral estrogen versus combined androgen deprivation in the treatment of metastatic prostatic cancer: Part 2. Final evaluation of the Scandinavian Prostatic Cancer Group (SPCG) Study No. 5. Scandinavian Journal of Urology and Nephrology, 42(3), 220–229. [DOI:10.1080/00365590801943274]
Park, W. (2002). Selective estrogen receptor modulators (SERMS) and their roles in breast cancer prevention. Trends in Molecular Medicine, 8(2), 82–88. [DOI:10.1016/s1471-4914(02)02282-7]
Patel, K. T., Adeel, S., Rodrigues Miragaya, J., & Tangpricha, V. (2022). Progestogen Use in Gender-Affirming Hormone Therapy: A Systematic Review. Endocrine Practice, 28(12), 1244–1252. [DOI:10.1016/j.eprac.2022.08.012]
Peck-Radosavljevic, M. (2007). Review article: coagulation disorders in chronic liver disease. Alimentary Pharmacology & Therapeutics, 26, 21–28. [DOI:10.1111/j.1365-2036.2007.03509.x]
Pfeifer, S., Butts, S., Dumesic, D., Fossum, G., Gracia, C., La Barbera, A., Mersereau, J., Odem, R., Penzias, A., Pisarska, M., Rebar, R., Reindollar, R., Rosen, M., Sandlow, J., Sokol, R., Vernon, M., & Widra, E. (2017). Combined hormonal contraception and the risk of venous thromboembolism: a guideline. Fertility and Sterility, 107(1), 43–51. [DOI:10.1016/j.fertnstert.2016.09.027]
Phillips, I., Shah, S. I., Duong, T., Abel, P., & Langley, R. E. (2014). Androgen Deprivation Therapy and the Re-emergence of Parenteral Estrogen in Prostate Cancer. Oncology & Hematology Review, 10(1), 42–47. [PubMed Central] [DOI:10.17925/ohr.2014.10.1.42]
Plu-Bureau, G., Maitrot-Mantelet, L., Hugon-Rodin, J., & Canonico, M. (2013). Hormonal contraceptives and venous thromboembolism: An epidemiological update. Best Practice & Research Clinical Endocrinology & Metabolism, 27(1), 25–34. [DOI:10.1016/j.beem.2012.11.002]
Pomp, E. R., Rosendaal, F. R., & Doggen, C. J. (2008). Smoking increases the risk of venous thrombosis and acts synergistically with oral contraceptive use. American Journal of Hematology, 83(2), 97–102. [DOI:10.1002/ajh.21059]
Pond, S. M., & Tozer, T. N. (1984). First-Pass Elimination. Clinical Pharmacokinetics, 9(1), 1–25. [DOI:10.2165/00003088-198409010-00001]
Prentice, R. L., & Anderson, G. L. (2008). The Women’s Health Initiative: Lessons Learned. Annual Review of Public Health, 29(1), 131–150. [DOI:10.1146/annurev.publhealth.29.020907.090947]
Prentice, R. (2014). Postmenopausal Hormone Therapy and the Risks of Coronary Heart Disease, Breast Cancer, and Stroke. Seminars in Reproductive Medicine, 32(6), 419–425. [DOI:10.1055/s-0034-1384624]
Pyra, M., Casimiro, I., Rusie, L., Ross, N., Blum, C., Keglovitz Baker, K., Baker, A., & Schneider, J. (2020). An Observational Study of Hypertension and Thromboembolism Among Transgender Patients Using Gender-Affirming Hormone Therapy. Transgender Health, 5(1), 1–9. [DOI:10.1089/trgh.2019.0061]
Quinton, R., & Swee, D. S. (2019). Hormone replacement therapy: transgender studies show safety of estradiol. BMJ, 364, l600. [DOI:10.1136/bmj.l600]
Rabe, T., Luxembourg, B., Ludwig, M., Dinger, J. C., Bauersachs, R., Rott, H., Mueck, A. O., & Albring, C. (2011). Contraception and Thrombophilia - A statement from the German Society of Gynecological Endocrinology and Reproductive Medicine (DGGEF e. V.) and the Professional Association of the German Gynaecologists (BVF e. V.). Journal für Reproduktionsmedizin und Endokrinologie-Journal of Reproductive Medicine and Endocrinology, 8(Special Issue 1), 178–218. [URL]
Raps, M., Helmerhorst, F., Fleischer, K., Thomassen, S., Rosendaal, F., Rosing, J., Ballieux, B., & Van Vliet, H. (2012). Sex hormone‐binding globulin as a marker for the thrombotic risk of hormonal contraceptives. Journal of Thrombosis and Haemostasis, 10(6), 992–997. [DOI:10.1111/j.1538-7836.2012.04720.x]
Ravery, V., Fizazi, K., Oudard, S., Drouet, L., Eymard, J., Culine, S., Gravis, G., Hennequin, C., & Zerbib, M. (2011). The use of estramustine phosphate in the modern management of advanced prostate cancer. BJU International, 108(11), 1782–1786. [DOI:10.1111/j.1464-410x.2011.10201.x]
Reda, S., Morimont, L., Douxfils, J., & Rühl, H. (2020). Can We Measure the Individual Prothrombotic or Prohemorrhagic Tendency by Global Coagulation Tests? Hämostaseologie, 40(3), 364–378. [DOI:10.1055/a-1153-5824]
Renoux, C., Dell’Aniello, S., & Suissa, S. (2010). Hormone replacement therapy and the risk of venous thromboembolism: a population-based study. Journal of Thrombosis and Haemostasis, 8(5), 979–986. [DOI:10.1111/j.1538-7836.2010.03839.x]
Renoux, C., Dell’Aniello, S., Garbe, E., & Suissa, S. (2010). Transdermal and oral hormone replacement therapy and the risk of stroke: a nested case-control study. BMJ, 340, c2519. [DOI:10.1136/bmj.c2519]
Roach, R., Lijfering, W., Helmerhorst, F., Cannegieter, S., Rosendaal, F., & van Hylckama Vlieg, A. (2013). The risk of venous thrombosis in women over 50 years old using oral contraception or postmenopausal hormone therapy. Journal of Thrombosis and Haemostasis, 11(1), 124–131. [DOI:10.1111/jth.12060]
Roach, R. E., Lijfering, W. M., Rosendaal, F. R., Cannegieter, S. C., & le Cessie, S. (2014). Sex Difference in Risk of Second but Not of First Venous Thrombosis. Circulation, 129(1), 51–56. [DOI:10.1161/circulationaha.113.004768]
Rooijen, M., Silveira, A., Hamsten, A., & Bremme, K. (2004). Sex hormone–binding globulin—A surrogate marker for the prothrombotic effects of combined oral contraceptives. American Journal of Obstetrics and Gynecology, 190(2), 332–337. [DOI:10.1016/s0002-9378(03)00950-5]
Ropponen, A., Aittomäki, K., Vihma, V., Tikkanen, M. J., & Ylikorkala, O. (2005). Effects of Oral and Transdermal Estradiol Administration on Levels of Sex Hormone-Binding Globulin in Postmenopausal Women with and without a History of Intrahepatic Cholestasis of Pregnancy. The Journal of Clinical Endocrinology & Metabolism, 90(6), 3431–3434. [DOI:10.1210/jc.2005-0352]
Rosendaal, F. R. (2005). Venous thrombosis: the role of genes, environment, and behavior. Hematology American Society of Hematology Education Program, 2005(1), 1–12. [Google Scholar] [DOI:10.1182/asheducation-2005.1.1] [URL]
Rosendaal, F. R. (2016). Causes of venous thrombosis. Thrombosis Journal, 14(Suppl 1) [State of the Art 2016: Research and Review from the 9th Congress of the Asian-Pacific Society on Thrombosis and Hemostasis], 24. [DOI:10.1186/s12959-016-0108-y]
Rott, H. (2019). Birth Control Pills and Thrombotic Risks: Differences of Contraception Methods with and without Estrogen. Hämostaseologie, 39(1), 42–48. [DOI:10.1055/s-0039-1677806]
Rova, K., Passmark, H., & Lindqvist, P. G. (2012). Venous thromboembolism in relation to in vitro fertilization: an approach to determining the incidence and increase in risk in successful cycles. Fertility and Sterility, 97(1), 95–100. [DOI:10.1016/j.fertnstert.2011.10.038]
Rovinski, D., Ramos, R. B., Fighera, T. M., Casanova, G. K., & Spritzer, P. M. (2018). Risk of venous thromboembolism events in postmenopausal women using oral versus non-oral hormone therapy: A systematic review and meta-analysis. Thrombosis Research, 168, 83–95. [DOI:10.1016/j.thromres.2018.06.014]
Ruiz Garcia, V., López-Briz, E., Carbonell Sanchis, R., Gonzalvez Perales, J. L., & Bort-Martí, S. (2013). Megestrol acetate for treatment of anorexia-cachexia syndrome. Cochrane Database of Systematic Reviews, 2019(3), CD004310. [DOI:10.1002/14651858.cd004310.pub3]
Russell, N., Cheung, A., & Grossmann, M. (2017). Estradiol for the mitigation of adverse effects of androgen deprivation therapy. Endocrine-Related Cancer, 24(8), R297–R313. [DOI:10.1530/erc-17-0153]
Sahlin, L., & Schoultz, B. V. (1999). Liver Inclusive Protein, Lipid and Carbohydrate Metabolism. In Oettel, M., & Schillinger, E. (Eds.). Estrogens and Antiestrogens II: Pharmacology and Clinical Application of Estrogens and Antiestrogen (Handbook of Experimental Pharmacology, Volume 135, Part 2) (pp. 163–178). Berlin/Heidelberg: Springer. [DOI:10.1007/978-3-642-60107-1_8]
Scarabin, P. (2018). Progestogens and venous thromboembolism in menopausal women: an updated oral versus transdermal estrogen meta-analysis. Climacteric, 21(4), 341–345. [DOI:10.1080/13697137.2018.1446931]
Scarabin, P., Canonico, M., Plu-Bureau, G., & Oger, E. (2020). Menopause and hormone therapy in the 21st century: why promote transdermal estradiol and progesterone? Heart, 106(16), 1278–1278. [DOI:10.1136/heartjnl-2020-316907]
Scheres, L. J., van Hylckama Vlieg, A., Ballieux, B. E., Fauser, B. C., Rosendaal, F. R., Middeldorp, S., & Cannegieter, S. C. (2019). Endogenous sex hormones and risk of venous thromboembolism in young women. Journal of Thrombosis and Haemostasis, 17(8), 1297–1304. [DOI:10.1111/jth.14474]
Scheres, L. J., Selier, N. L., Nota, N. M., van Diemen, J. J., Cannegieter, S. C., & den Heijer, M. (2021). Effect of gender‐affirming hormone use on coagulation profiles in transmen and transwomen. Journal of Thrombosis and Haemostasis, 19(4), 1029–1037. [DOI:10.1111/jth.15256]
Schindler, A. E. (2003). Differential effects of progestins on hemostasis. Maturitas, 46, 31–37. [DOI:10.1016/j.maturitas.2003.09.016]
Schock, H., Zeleniuch-Jacquotte, A., Lundin, E., Grankvist, K., Lakso, H., Idahl, A., Lehtinen, M., Surcel, H., & Fortner, R. T. (2016). Hormone concentrations throughout uncomplicated pregnancies: a longitudinal study. BMC Pregnancy and Childbirth, 16(1), 146. [DOI:10.1186/s12884-016-0937-5]
Schröder, F. H., & Radlmaier, A. (2002). Steroidal Antiandrogens. In Jordan, C. V., & Furr, B. J. A. (Eds.). Hormone Therapy in Breast and Prostate Cancer (pp. 325–346). Totowa, New Jersey: Humana Press. [DOI:10.1007/978-1-59259-152-7_15]
Sciarra, A., Gentile, V., Cattarino, S., Gentilucci, A., Alfarone, A., D’Eramo, G., & Salciccia, S. (2014). Oral ethinylestradiol in castration-resistant prostate cancer: A 10-year experience. International Journal of Urology, 22(1), 98–103. [DOI:10.1111/iju.12613]
Seaman, H. E., Langley, S. E., Farmer, R. D., & de Vries, C. S. (2007). Venous thromboembolism and cyproterone acetate in men with prostate cancer: a study using the General Practice Research Database. BJU International, 99(6), 1398–1403. [DOI:10.1111/j.1464-410x.2007.06859.x]
Shatzel, J. J., Connelly, K. J., & DeLoughery, T. G. (2017). Thrombotic issues in transgender medicine: A review. American Journal of Hematology, 92(2), 204–208. [DOI:10.1002/ajh.24593]
Shifren, J. L., Rifai, N., Desindes, S., McIlwain, M., Doros, G., & Mazer, N. A. (2008). A Comparison of the Short-Term Effects of Oral Conjugated Equine Estrogens Versus Transdermal Estradiol on C-Reactive Protein, Other Serum Markers of Inflammation, and Other Hepatic Proteins in Naturally Menopausal Women. The Journal of Clinical Endocrinology & Metabolism, 93(5), 1702–1710. [DOI:10.1210/jc.2007-2193]
Simon, T., De Jonage-Canonico, M. B., Oger, E., Wahl, D., Conard, J., Meyer, G., Emmerich, J., Barrellier, M., Guiraud, A., & Scarabin, P. (2006). Indicators of lifetime endogenous estrogen exposure and risk of venous thromboembolism. Journal of Thrombosis and Haemostasis, 4(1), 71–76. [DOI:10.1111/j.1538-7836.2005.01693.x]
Singla, N., Ghandour, R. A., & Raj, G. V. (2019). Investigational luteinizing hormone releasing hormone (LHRH) agonists and other hormonal agents in early stage clinical trials for prostate cancer. Expert Opinion on Investigational Drugs, 28(3), 249–259. [DOI:10.1080/13543784.2019.1570130]
Sitruk-Ware, R., & Nath, A. (2011). Metabolic effects of contraceptive steroids. Reviews in Endocrine and Metabolic Disorders, 12(2), 63–75. [DOI:10.1007/s11154-011-9182-4]
Sitruk-Ware, R., & Nath, A. (2013). Characteristics and metabolic effects of estrogen and progestins contained in oral contraceptive pills. Best Practice & Research Clinical Endocrinology & Metabolism, 27(1), 13–24. [DOI:10.1016/j.beem.2012.09.004]
Skouby, S. O., & Sidelmann, J. J. (2018). Impact of progestogens on hemostasis. Hormone Molecular Biology and Clinical Investigation, 37(2), 20180041. [DOI:10.1515/hmbci-2018-0041]
Smith, K., Galazi, M., Openshaw, M. R., Wilson, P., Sarker, S. J., O’Brien, N., Alifrangis, C., Stebbing, J., & Shamash, J. (2020). The Use of Transdermal Estrogen in Castrate-resistant, Steroid-refractory Prostate Cancer. Clinical Genitourinary Cancer, 18(3), e217–e223. [DOI:10.1016/j.clgc.2019.09.019]
Smith, N. L. (2004). Esterified Estrogens and Conjugated Equine Estrogens and the Risk of Venous Thrombosis. JAMA, 292(13), 1581–1587. [DOI:10.1001/jama.292.13.1581]
Smith, N. L., Blondon, M., Wiggins, K. L., Harrington, L. B., van Hylckama Vlieg, A., Floyd, J. S., Hwang, M., Bis, J. C., McKnight, B., Rice, K. M., Lumley, T., Rosendaal, F. R., Heckbert, S. R., & Psaty, B. M. (2014). Lower Risk of Cardiovascular Events in Postmenopausal Women Taking Oral Estradiol Compared With Oral Conjugated Equine Estrogens. JAMA Internal Medicine, 174(1), 25–34. [DOI:10.1001/jamainternmed.2013.11074]
Speroff, L. (1996). The Comparative Effect on Bone Density, Endometrium, and Lipids of Continuous Hormones as Replacement Therapy (CHART Study). JAMA, 276(17), 1397–1403. [DOI:10.1001/jama.1996.03540170041030]
Stanczyk, F. Z., Archer, D. F., & Bhavnani, B. R. (2013). Ethinyl estradiol and 17β-estradiol in combined oral contraceptives: pharmacokinetics, pharmacodynamics and risk assessment. Contraception, 87(6), 706–727. [DOI:10.1016/j.contraception.2012.12.011]
Stanczyk, F. Z., Mathews, B. W., & Cortessis, V. K. (2017). Does the type of progestin influence the production of clotting factors? Contraception, 95(2), 113–116. [DOI:10.1016/j.contraception.2016.07.007]
Stege, R., Carlström, K., Collste, L., Eriksson, A., Henriksson, P., & Pousette, A. (1988). Single drug polyestradiol phosphate therapy in prostatic cancer. American Journal of Clinical Oncology, 11(Suppl 2), S101–S103. [DOI:10.1097/00000421-198801102-00024] [PDF]
Stegeman, B., Raps, M., Helmerhorst, F., Vos, H., van Vliet, H., Rosendaal, F., & van Hylckama Vlieg, A. (2013). Effect of ethinylestradiol dose and progestagen in combined oral contraceptives on plasma sex hormone‐binding globulin levels in premenopausal women. Journal of Thrombosis and Haemostasis, 11(1), 203–205. [DOI:10.1111/jth.12054]
Stuenkel, C. A., Davis, S. R., Gompel, A., Lumsden, M. A., Murad, M. H., Pinkerton, J. V., & Santen, R. J. (2015). Treatment of Symptoms of the Menopause: An Endocrine Society Clinical Practice Guideline. The Journal of Clinical Endocrinology & Metabolism, 100(11), 3975–4011. [DOI:10.1210/jc.2015-2236]
Sudhir, K., & Komesaroff, P. A. (1999). Cardiovascular Actions of Estrogens in Men. The Journal of Clinical Endocrinology & Metabolism, 84(10), 3411–3415. [DOI:10.1210/jcem.84.10.5954]
Swee, D. S., Javaid, U., & Quinton, R. (2019). Estrogen Replacement in Young Hypogonadal Women—Transferrable Lessons From the Literature Related to the Care of Young Women With Premature Ovarian Failure and Transgender Women. Frontiers in Endocrinology, 10, 685. [DOI:10.3389/fendo.2019.00685]
Tadd, W., & Bayer, A. (2006). Dignity in health and social care for older Europeans: implications of a European project. Aging Health, 2(5), 771–779. [DOI:10.2217/1745509x.2.5.771]
Taylor, J. K., & Pendleton, N. (2016). Progesterone therapy for the treatment of non-cancer cachexia: a systematic review. BMJ Supportive & Palliative Care, 6(3), 276–286. [DOI:10.1136/bmjspcare-2015-001041]
Tchaikovski, S. N., & Rosing, J. (2010). Mechanisms of Estrogen-Induced Venous Thromboembolism. Thrombosis Research, 126(1), 5–11. [DOI:10.1016/j.thromres.2010.01.045]
Tepper, N. K., Whiteman, M. K., Marchbanks, P. A., James, A. H., & Curtis, K. M. (2016). Progestin-only contraception and thromboembolism: A systematic review. Contraception, 94(6), 678–700. [DOI:10.1016/j.contraception.2016.04.014]
Tepper, N. K., Jeng, G., Curtis, K. M., Boutot, M. E., Boulet, S. L., & Whiteman, M. K. (2019). Venous Thromboembolism Among Women Initiating Depot Medroxyprogesterone Acetate Immediately Postpartum. Obstetrics & Gynecology, 133(3), 533–540. [DOI:10.1097/aog.0000000000003135]
The Coronary Drug Project Research Group. (1970). The Coronary Drug Project. JAMA, 214(7), 1303–1313. [DOI:10.1001/jama.1970.03180070069012]
The Coronary Drug Project Research Group. (1973). The Coronary Drug Project. JAMA, 226(6), 652–657. [DOI:10.1001/jama.1973.03230060030009]
The Oral Contraceptive and Hemostasis Study Group. (1999). An open label, randomized study to evaluate the effects of seven monophasic oral contraceptive regimens on hemostatic variables. Contraception, 59(6), 345–355. [DOI:10.1016/s0010-7824(99)00044-x]
Timp, J. F., Braekkan, S. K., Versteeg, H. H., & Cannegieter, S. C. (2013). Epidemiology of cancer-associated venous thrombosis. Blood, 122(10), 1712–1723. [DOI:10.1182/blood-2013-04-460121]
Toorians, A. W., Thomassen, M. C., Zweegman, S., Magdeleyns, E. J., Tans, G., Gooren, L. J., & Rosing, J. (2003). Venous Thrombosis and Changes of Hemostatic Variables during Cross-Sex Hormone Treatment in Transsexual People. The Journal of Clinical Endocrinology & Metabolism, 88(12), 5723–5729. [DOI:10.1210/jc.2003-030520]
Totaro, M., Palazzi, S., Castellini, C., Parisi, A., D’Amato, F., Tienforti, D., Baroni, M. G., Francavilla, S., & Barbonetti, A. (2021). Risk of Venous Thromboembolism in Transgender People Undergoing Hormone Feminizing Therapy: A Prevalence Meta-Analysis and Meta-Regression Study. Frontiers in Endocrinology, 12, 741866. [DOI:10.3389/fendo.2021.741866]
Trémollieres, F. (2012). Contraception orale estro-progestative: quelle différence entre éthinylestradiol et estradiol? [Oral combined contraception: Is there any difference between ethinyl-estradiol and estradiol?] Gynécologie Obstétrique & Fertilité, 40(2), 109–115. [DOI:10.1016/j.gyobfe.2011.10.009]
Turo, R., Smolski, M., Esler, R., Kujawa, M. L., Bromage, S. J., Oakley, N., Adeyoju, A., Brown, S. C., Brough, R., Sinclair, A., & Collins, G. N. (2013). Diethylstilboestrol for the treatment of prostate cancer: past, present and future. Scandinavian Journal of Urology, 48(1), 4–14. [DOI:10.3109/21681805.2013.861508]
United Nations Development Programme/United Nations Population Fund/World Health Organization/World Bank Special Programme of Research, Development and Research Training in Human Reproduction, & Task Force on Long-acting Systemic Agents for Fertility Regulation. (2003). Comparative study of the effects of two once-a-month injectable contraceptives (Cyclofem® and Mesigyna®) and one oral contraceptive (Ortho-Novum 1/35®) on coagulation and fibrinolysis. Contraception, 68(3), 159–176. [DOI:10.1016/s0010-7824(03)00164-1]
van Hylckama Vlieg, A., Helmerhorst, F. M., & Rosendaal, F. R. (2010). The Risk of Deep Venous Thrombosis Associated With Injectable Depot–Medroxyprogesterone Acetate Contraceptives or a Levonorgestrel Intrauterine Device. Arteriosclerosis, Thrombosis, and Vascular Biology, 30(11), 2297–2300. [DOI:10.1161/atvbaha.110.211482]
Van Kesteren, P. J., Asscheman, H., Megens, J. A., & Gooren, L. J. (1997). Mortality and morbidity in transsexual subjects treated with cross-sex hormones. Clinical Endocrinology, 47(3), 337–343. [DOI:10.1046/j.1365-2265.1997.2601068.x]
van Vliet, H. A., Frolich, M., Christella, M., Thomassen, L., Doggen, C. J., Rosendaal, F. R., Rosing, J., & Helmerhorst, F. M. (2005). Association between sex hormone-binding globulin levels and activated protein C resistance in explaining the risk of thrombosis in users of oral contraceptives containing different progestogens. Human Reproduction, 20(2), 563–568. [DOI:10.1093/humrep/deh612]
Vinogradova, Y., Coupland, C., & Hippisley-Cox, J. (2015). Use of combined oral contraceptives and risk of venous thromboembolism: nested case-control studies using the QResearch and CPRD databases. BMJ, 350, h2135. [DOI:10.1136/bmj.h2135]
Vinogradova, Y., Coupland, C., & Hippisley-Cox, J. (2019). Use of hormone replacement therapy and risk of venous thromboembolism: nested case-control studies using the QResearch and CPRD databases. BMJ, 364, k4810. [DOI:10.1136/bmj.k4810]
von Schoultz, B., Carlström, K., Collste, L., Eriksson, A., Henriksson, P., Pousette, Å., & Stege, R. (1989). Estrogen therapy and liver function—metabolic effects of oral and parenteral administration. The Prostate, 14(4), 389–395. [DOI:10.1002/pros.2990140410]
Walker, I. D. (2010). Obstetrics, Contraception, and Estrogen Replacement. In Key, N., Makris, M., O’Shaughnessy, D., & Lillicrap, D. (Eds.). Practical Hemostasis and Thrombosis, 2nd Edition (pp. 247–257). Oxford: Wiley-Blackwell. [DOI:10.1002/9781444306286.ch24]
Weinand, J. D., & Safer, J. D. (2015). Hormone therapy in transgender adults is safe with provider supervision; A review of hormone therapy sequelae for transgender individuals. Journal of Clinical & Translational Endocrinology, 2(2), 55–60. [DOI:10.1016/j.jcte.2015.02.003]
Westerlund, E., Henriksson, P., Wallén, H., Hovatta, O., Wallberg, K. R., & Antovic, A. (2012). Detection of a procoagulable state during controlled ovarian hyperstimulation for in vitro fertilization with global assays of haemostasis. Thrombosis Research, 130(4), 649–653. [DOI:10.1016/j.thromres.2011.11.024]
White, C. M., Ferraro‐Borgida, M. J., Fossati, A. T., McGill, C. C., Ahlberg, A. W., Feng, Y. J., Heller, G. V., & Chow, M. S. (1998). The Pharmacokinetics of Intravenous Estradiol—A Preliminary Study. Pharmacotherapy: The Journal of Human Pharmacology and Drug Therapy, 18(6), 1343–1346. [DOI:10.1002/j.1875-9114.1998.tb03157.x]
Wiegratz, I., & Kuhl, H. (2006). Metabolic and clinical effects of progestogens. The European Journal of Contraception & Reproductive Health Care, 11(3), 153–161. [DOI:10.1080/13625180600772741]
Wierckx, K., Elaut, E., Declercq, E., Heylens, G., De Cuypere, G., Taes, Y., Kaufman, J. M., & T’Sjoen, G. (2013). Prevalence of cardiovascular disease and cancer during cross-sex hormone therapy in a large cohort of trans persons: a case–control study. European Journal of Endocrinology, 169(4), 471–478. [DOI:10.1530/eje-13-0493]
Writing Group for the Women’s Health Initiative Investigators. (2002). Risks and Benefits of Estrogen Plus Progestin in Healthy Postmenopausal Women: Principal Results From the Women’s Health Initiative Randomized Controlled Trial. JAMA, 288(3), 321–333. [DOI:10.1001/jama.288.3.321]
Zhang, M., Zhu, S., Yang, W., Huang, Q., & Ho, C. (2021). The biological fate and bioefficacy of citrus flavonoids: bioavailability, biotransformation, and delivery systems. Food & Function, 12(8), 3307–3323. [DOI:10.1039/d0fo03403g]
Zhao, J., Yang, J., & Xie, Y. (2019). Improvement strategies for the oral bioavailability of poorly water-soluble flavonoids: An overview. International Journal of Pharmaceutics, 570, 118642. [DOI:10.1016/j.ijpharm.2019.118642]
Zucker, R., Reisman, T., & Safer, J. D. (2021). Minimizing Venous Thromboembolism in Feminizing Hormone Therapy: Applying Lessons From Cisgender Women and Previous Data. Endocrine Practice, 27(6), 621–625. [DOI:10.1016/j.eprac.2021.03.010]
\ No newline at end of file
diff --git a/transfemscience.org/articles/high-dose-transdermal-e2/index.html b/transfemscience.org/articles/high-dose-transdermal-e2/index.html
index f1bffb2e..fcbef099 100644
--- a/transfemscience.org/articles/high-dose-transdermal-e2/index.html
+++ b/transfemscience.org/articles/high-dose-transdermal-e2/index.html
@@ -1 +1 @@
-A Review of Studies on Estradiol Levels and Testosterone Suppression with High-Dose Transdermal Estradiol Gel and Ointment in Cisgender Men with Prostate Cancer - Transfeminine Science
A Review of Studies on Estradiol Levels and Testosterone Suppression with High-Dose Transdermal Estradiol Gel and Ointment in Cisgender Men with Prostate Cancer
By Aly | First published June 30, 2019 | Last modified November 2, 2022
Abstract / TL;DR
High-dose estradiol monotherapy, generally used non-orally, is a therapeutic approach for testosterone suppression which is sometimes used in transfeminine people and men with prostate cancer. Limited data are available for this approach with certain forms of estradiol, so considering research in other patient populations besides transfeminine people can provide valuable information. In the 1970s and 1980s, studies were conducted on high-dose transdermal estradiol gel and ointment for the treatment of prostate cancer in men. Estradiol at 3 to 20 mg/day appeared to give 84 to 473 pg/mL estradiol and 105 to 260 ng/dL testosterone in these men. While informative, the findings of the studies are only so useful due to various unfortunate limitations. In any case, it’s apparent that transdermal estradiol gel and related forms don’t seem to be well-suited for achieving the high levels of estradiol that are needed for robust testosterone suppression with high-dose estradiol monotherapy in men with prostate cancer or transfeminine people. High-dose transdermal estradiol patches, or alternatively genital application of transdermal estradiol forms, may be more useful options for this approach on the other hand.
Introduction
High-dose estrogen monotherapy is a means of testosterone suppression which is sometimes used to treat prostate cancer in men. High-dose parenteral estradiol therapy is one particular approach used for this purpose which has less toxicity compared to use of oral and synthetic estrogens. In the late 1970s and early 1980s, high-dose transdermal estradiol gel/ointment was assessed by French researchers in three clinical studies for the treatment of prostate cancer (Steg & Benoit, 1979; Steg et al., 1979; Steg et al., 1980; Steg et al., 1983; Steg & Benoit, 1983; Benoit, 1985). The dosages used in the studies ranged from 3 to 20 mg/day. For comparison, typical doses of transdermal estradiol gel used in transfeminine hormone therapy to achieve physiological estradiol levels range from about 1 to 6 mg/day.
High-dose estradiol monotherapy, generally administered parenterally, is sometimes used as a means of suppressing testosterone levels in transfeminine hormone therapy similarly to the hormonal treatment of prostate cancer. This approach omits the use of antiandrogens and their costs, side effects, and risks, though at the same time incurs risks of higher estradiol exposure. There is limited information available on estradiol levels and testosterone suppression with high-dose estradiol gel and similar forms. Hence, a review of the relevant details from the studies of high-dose estradiol gel for prostate cancer is of value as it can be used to inform the use of high-dose estradiol monotherapy in transfeminine people.
The French studies in question appear to be the only clinical studies of high-dose transdermal estradiol gel/ointment for prostate cancer that have been published. This is in contrast to high-dose transdermal estradiol patches and injectable estradiol esters like polyestradiol phosphate (PEP) and estradiol undecylate (EU), which have been much more widely used in men with prostate cancer.
Data and Excerpts
A Note on Estradiol Delivery Rates
The authors use “γ” (“gamma”) as a unit in their papers. This is a now-deprecated non-SI unit of mass equal to 1 μg (Wiki). That is, “1 γ” means the same thing as “1 μg”. The researchers provided values using this unit as an estimate of the amount of estradiol actually absorbed into the body after taking into account the “cutaneous absorption coefficient” (i.e., transdermal bioavailability) of estradiol. However, when compared to established μg/day values for commercial transdermal estradiol patches and the estradiol levels associated with these patches, the values in the papers are very different from what would be expected. For this reason, and because estimates for transdermal estradiol patches were more rigorously determined and likely to be correct, the delivery rates reported by the authors are probably not accurate. It was important to include them in this article nonetheless however because the researchers modified their transdermal estradiol formulations between their studies, resulting in inconsistencies between the estradiol doses in gel/ointment and their estimated delivery values.
Study 1: Estradiol Gel 3 mg/day versus 6 mg/day
The following three papers pertain to the first study:
Steg, A., Benoit, G., Limouzin-Lamotte, A., Mahoudeau, J., Caillens, M., & Raichvarg, D. (1979). Cancer de la prostate: effets métaboliques des bêta-estradiol par voie percutanée. [Cancer of the prostate: metabolic effect of percutaneous beta-estradiol. / Prostatic carcinoma: metabolic effect of percutaneous beta-estradiol.] La Nouvelle Presse Medicale, 8(46), 3801–3802. [Google Scholar 1] [Google Scholar 2] [Pascal and Francis] [PubMed] [PDF]
Steg, A., Benoit, G., Limouzin-Lamotte, A., Mahoudeau, J., Caillens, M., & Raichvarg, D. (1980). Cancer de la prostate: Effets métaboliques du bêta-estradiol par voie percutanée. [Cancer of the prostate: metabolic effects of percutaneously administered beta-estradiol.] Revue Médicale de la Suisse Romande, 100(11), 895–897. [Google Scholar 1] [Google Scholar 2] [Pascal and Francis] [PubMed] [PDF]
In the study, 21 men with prostate cancer were divided into two groups and treated for 1 month with:
3 mg/day (“300 μg/day”) estradiol in 5 g/day gel applied to the abdomen in one daily dose
6 mg/day (“600 μg/day”) estradiol in 10 g/day gel applied to the abdomen in two daily divided doses
Hormone levels in the study were as follows:
Estradiol levels
Testosterone levels
Pre-treatment
23.2 ± 10.8 pg/mL
Pre-treatment
341 ± 180 ng/dL
E2 gel 3 mg/day
84.2 ± 54.3 pg/mL
E2 gel 3 mg/day
188 ± 125 ng/dL
E2 gel 6 mg/day
184.7 ± 98.46 pg/mL
E2 gel 6 mg/day
105 ± 113 ng/dL
Estrone levels
DHT levels
Pre-treatment
37.6 ± 16.2 pg/mL
Pre-treatment
36 ± 27 ng/dL
E2 gel 3 mg/day
86.7 ± 42.5 pg/mL
E2 gel 3 mg/day
23 ± 14 ng/dL
E2 gel 6 mg/day
150.9 ± 101.4 pg/mL
E2 gel 6 mg/day
12 ± 12 ng/dL
LH levels
FSH levels
Pre-treatment
6.21 ± 6.2 mIU/mL
Pre-treatment
7.56 ± 4.9 mIU/mL
E2 gel 3 mg/day
4.15 ± 3.3 mIU/mL
E2 gel 3 mg/day
6.44 ± 5.0 mIU/mL
E2 gel 6 mg/day
3.41 ± 3.2 mIU/mL
E2 gel 6 mg/day
4.13 ± 5.0 mIU/mL
The researchers stated that the testosterone levels resulting with 6 mg/day estradiol gel (105 ± 113 ng/) were similar to those that are known to occur with 3 mg/day oral diethylstilbestrol. However, this seems to be a somewhat inaccurate statement as 3 mg/day oral diethylstilbestrol has been found to consistently suppress testosterone levels into the castrate range (≤50 ng/dL) in studies (Wiki).
Study 2: Estradiol Ointment 10 mg/day versus Diethylstilbestrol Oral 3 mg/day
The following paper pertains to the second study:
Steg, A., Benoit, G., Maisonneuve, P., Tallet, F., Nahoul, K., Sultan, Y., Raichwarg, D., & Limouzin-Lamotte, M. A. (1983). Étude comparative du diéthylstilboestrol et du 17 bêta-oestradiol per-cutané dans le traitement du cancer de la prostate. [A comparative study of percutaneous 17 beta-estradiol and diethylstilbestrol in the treatment of prostatic cancer.] Annales d’Urologie, 17(4), 197–202. [Google Scholar] [PDF]
In the study, 56 men with prostate cancer were divided into two groups and treated for 3 months with:
10 mg/day (“600 μg/day”) estradiol in “ointment” applied to the abdomen in two daily divided doses
3 mg/day oral diethylstilbestrol in three daily divided doses
Hormone levels in the study were as follows:
Estradiol levels
Testosterone levels
Pre-treatment (E2 group)
30 pg/mL
Pre-treatment (E2 group)
450 ng/dL
E2 ointment 10 mg/day
107 ± 81 pg/mL
E2 ointment 10 mg/day
180 ± 160 ng/dL
Pre-treatment (DES group)
26 pg/mL
Pre-treatment (DES group)
420 ± 130 ng/dL
DES oral 3 mg/day
19 pg/mL
DES oral 3 mg/day
51 ± 0.9 ng/dL
LH levels
FSH levels
Pre-treatment (E2 group)
3.2 mIU/mL
Pre-treatment (E2 group)
4.7 mIU/mL
E2 ointment 10 mg/day
2.0 ± 0.9 mIU/mL
E2 ointment 10 mg/day
1.7 mIU/mL
Pre-treatment (DES group)
4.0 ± 3.2 mIU/mL
Pre-treatment (DES group)
5.8 mIU/mL
DES oral 3 mg/day
1.6 ± 1.2 mIU/mL
DES oral 3 mg/day
1.7 mIU/mL
Some SDs (±) are missing in the table above because not all were provided in the original paper. The SDs that were included above were actually reported in the paper for Study 3.
Some noteworthy translated excerpts from the paper:
This study shows that the clinical effects were more dramatic in the DES group, with a sharper drop in the free plasma testosterone level, than in the E2 group.
E2 has been administered too weakly because it is too low in the commercially used ointment and because application to the thick abdominal skin has a lower absorption coefficient than a thinner skin such as forearms for example. It is possible that a dose equivalent to 15 or 20 mg of gel, applied on the forearms, may allow to lower the testosterone below [100 ng/dL]. The marketing of a more concentrated ointment is therefore desirable, as well as the use of a more efficient absorption site.
The search for new estrogens and new routes of administration is therefore necessary: E2, a natural female hormone, induces no thromboembolic events. It seems to us, therefore, that a larger dose must be proposed to be as effective as 3 mg DES. A gel twice more concentrated is therefore currently under study.
The double-concentration estradiol gel was subsequently reported in Study 3 (see below).
It should be noted that the transdermal estradiol formulation in this study is different from that used in Study 1. Specifically, “6 mg/day estradiol gel” was stated to deliver “600 μg/day estradiol” in Study 1, whereas “10 mg/day estradiol ointment” was stated to deliver “600 μg/day estradiol” in Study 2. These apparent discrepancies might be of relevance to the unexpectedly lower estradiol levels and testosterone suppression in Study 2 compared to Study 1.
Study 3: Estradiol Ointment 20 mg/day versus Bilateral Orchiectomy
The following paper pertains to the third study:
Steg, A., & Benoit, G. (1983). Étude comparative de fortes doses d’oestradiol-17 β administrées par voie per-cutanée et de l’orchidectomie bilatérale dans le traitement du cancer de la prostate. [Prostatic carcinoma. Bilateral orchiectomy versus percutaneous administration of large doses of 17 β-estradiol. A comparative study. / Comparative study of percutaneous administration of large doses of 17β œstradiol and bilateral orchidectomy in prostatic carcinoma.] Annales d’Urologie, 17(5), 286–288. [Google Scholar] [Pascal and Francis] [PDF]
In the study, 38 men with prostate cancer were divided into two groups and treated for 1 month with:
20 mg/day (“1200 μg/day”) estradiol in an ointment applied to the skin in four daily divided doses
Bilateral orchiectomy (i.e., surgical removal of the testes)
Hormone levels in the study were as follows:
Condition
Estradiol levels
Testosterone levels
LH levels
Pre-treatment (E2 group)
52 ± 30 pg/mL
460 ± 230 ng/dL
2.6 ± 0.9 mIU/mL
E2 ointment 20 mg/day
473 ± 375 pg/mL
260 ± 160 ng/dL
1.7 ± 0.8 mIU/mL
Pre-treatment (orchi group)
Not reported
500 ± 160 ng/dL
5.5 ± 6 mIU/mL
Bilateral orchiectomy
Not reported
20 ± 10 ng/dL
19 ± 8 mIU/mL
Some noteworthy translated excerpts from the paper:
The purpose of this study was to determine whether hormonal efficacy [in the treatment of prostate cancer] was enhanced by the administration of large doses of E2. […] The study shows that, whereas orchiectomy lowers plasma testosterone levels dramatically, E2, at [the double dose used in this study compared to our previous study] (1200 [μg] versus 600 [μg]), surprisingly does not further lower it at all, but plasma E2 is substantially increased.
We have found that the administration of E2 causes significant biological changes; E2 is well-absorbed, testosterone is lowered, and LH and FSH are also lowered. But when comparing these effects with those obtained by castration, and with those also observed after administration of 3 mg of diethylstilbestrol (in our previous study), the results are much less brilliant. Indeed: the plasma testosterone is moderately lowered by E2 whereas the fall is much more pronounced with DES and is spectacular with castration; pituitary suppression is comparable with E2 and DES and of course orchiectomy increases LH; and if we compare the results obtained before and after treatment, it is clear that if before treatment the figures are comparable, after treatment the fall is pronounced only with DES and especially with orchiectomy.
The objective of this study was to determine whether doubling the dose of E2 enhances its antiandrogenic effect. [With both a lower dose and a higher dose], E2 is very well-absorbed. [With both doses], the pituitary suppression is identical, but on the other hand, not only is plasma testosterone not lower with [the higher dose], but it seems to be even [higher than with the lower dose]. This difference is also found clinically since with [the higher dose], 10% of patients were improved while with [the lower dose], 30% improvement was obtained.
How can this result be explained? Perhaps this is due to the contrary effects of E2 on androgens. Indeed: E2 on the one hand suppresses pituitary activity, which leads to a fall of testicular testosterone secretion, and at the same time E2 decreases 5α-reductase activity in the prostate; on the other hand, E2 causes an increase in SHBG and competes with free testosterone binding to SHBG and in this way increases the proportion of active free testosterone. In addition, testosterone also increases the level of cytoplasmic androgen receptors.
This work shows that E2 is well-absorbed percutaneously and causes practically no cardiovascular events. On the other hand, it appears that the antiandrogenic effect is significantly less by this route than that obtained by diethylstilbestrol and castration, and that in any case, we cannot improve the efficacy by increasing the dose of E2.
The finding that the 20 mg/day estradiol ointment resulted in less suppression of testosterone levels than the 10 mg/day estradiol ointment despite markedly higher estradiol levels is surprising. However, the researchers’ theoretical explanation of the result seems questionable. Abundant clinical research with high-dose estradiol for prostate cancer (e.g., transdermal patches, injectable polyestradiol phosphate injections, injectable estradiol undecylate) has shown stronger testosterone suppression with high estradiol levels in this range or below and seems to thoroughly contradict their results. Studies have consistently shown that estradiol levels of 200 to 500 pg/mL and above suppress testosterone levels by 90% and greater (to ~50 ng/dL and below) (Wiki; Graphs). Instead of the authors’ interpretation of their unexpected results, it seems possible that the testosterone assays for this study may have been inaccurate or perhaps some other methodological problem may have been responsible.
The concentration and dosage of estradiol ointment in this study were double those of Study 2, yet the estradiol levels measured in this study were almost 5-fold higher than those in Study 2. It’s possible that the higher concentration of ointment used may have resulted in disproportionately greater absorption, as one study found that the smaller the application area of estradiol gel (and hence higher the post-application concentration), the greater the resulting estradiol levels (Graph). On the other hand, it’s possible that the estradiol assays were inaccurate (as also suggested for testosterone above). Lastly, in contrast to the previous two papers, the authors don’t state where the ointment was applied in this study. It was probably the abdomen similarly, but this isn’t certain; they may have used one or more other locations with differing skin permeability (as they discussed the possibility of doing in Study 1). It’d be expected that they’d mention this change though, which perhaps makes the possibility unlikely.
Review Article
A review of hormone therapy for prostate cancer was also published by one of the researchers:
Benoit, G. (1985). Que Penser du Traitement Hormonal du Cancer de la Prostate / Hormonothérapie du Cancer de la Prostate. [Thoughts on the Hormonal Treatment of Prostate Cancer / Hormone Therapy of Prostate Cancer.] Gazette Médicale, 92(5), 33–39. [Google Scholar] [PDF] [Translation]
In the paper, she briefly mentioned her and her colleagues’ studies on high-dose transdermal estradiol gel/ointment for prostate cancer and provided some additional information pertaining to these studies. Here are the relevant translated excerpts from the paper:
In a study in Cochin (16), the efficacy of diethylstilbestrol was 50% of objective responses, but at a cost of 23% of thromboembolic events. These thromboembolic events are similar to the accidents that occur in women taking oral estrogen–progestogens. These are oral synthetic estrogens. In a series of diethylstilbestrol-treated prostate cancers, Steg (16) has shown that this treatment induces an increase in triglycerides and a decrease in coagulation factor VIII. Abbou (1) found, on his behalf, an increase in circulating immune complexes in patients with thrombosis under synthetic estrogen–progestogen therapy.
It therefore seems to us no longer possible to prescribe diethylstilbestrol as first intention. To reduce these cardiovascular events, most authors have tried to use natural estrogens administered intramuscularly, subcutaneously, or percutaneously. Cochin’s experience of using a natural estrogen (17-beta-estradiol) percutaneously has shown that this treatment may be effective, but that it is very difficult to administer: one in two patients is unable to apply the treatment correctly and regularly, which greatly reduces the use of such treatment (15).
As an indication, we report several studies made successively in Cochin (16, 17) with diethylstilbestrol, a natural estrogen (17-beta-estradiol), testicular pulpectomy, and an LHRH analogue administered subcutaneously.
The results confirm that diethylstilbestrol causes thromboembolic events. These different estrogenic treatments promote gynecomastia. Medical castration by LHRH analogues or surgical pulpectomy causes hot flushes. All these treatments reach, in a variable way, libido and sexual potency. This last effect is complex: it is known that castration, in young men, after puberty, does not regularly cause impotence, as shown by the history of castrates. However, it is necessary to warn the patient that each of these treatments can reach his manhood.
Synthetic estrogens, especially diethylstilbestrol, should no longer be used as first-line agents in the treatment of metastatic prostate cancer because of their thromboembolic risk. Natural estrogens do not seem efficient enough to be used regularly. Complete castration performs excessive mutilation. In our opinion, only testicular pulpectomy, LHRH analogues, and antiandrogens remain in competition.
The review also contains the following adapted summary table of data from their studies:
DES
E2 gel/ointment
Orchiectomy
GnRH analogue
Testosterone levels
50 ng/dL
100 ng/dL
20 ng/dL
50 ng/dL
50% partial remission
50%
30%
33%
41%
Cardiovascular events
23%
0%
0%
0%
The gonadotropin-releasing hormone (GnRH) analogue data were from other studies and papers by the same researchers (Steg et al., 1984; Steg et al., 1985a; Steg et al., 1985b). These studies did not assess transdermal estradiol and hence are not otherwise discussed in the present article.
The authors’ comments in this paper raise the additional question of whether inconsistent and suboptimal exposure to estradiol gel/ointment may have influenced the findings of their studies.
Summary and Discussion
In the reviewed clinical studies of high-dose transdermal estradiol gel/ointment in men with prostate cancer, the following results were obtained in terms of changes in measured hormone levels:
Estradiol dose
Estradiol levels
Testosterone levels
Before treatment
23–52 pg/mL
341–460 ng/dL
3 mg/day gel (“300 μg/day”)
84 pg/mL
188 ng/dL
6 mg/day gel (“600 μg/day”)
185 pg/mL
105 ng/dL
10 mg/day ointment (“600 μg/day”)
107 pg/mL
180 ng/dL
20 mg/day ointment (“1200 μg/day”)
473 pg/mL
260 ng/dL
Unfortunately, the data reported in these studies is not as useful as might have been hoped. This is due to inconsistencies with the transdermal estradiol formulations and doses used, reported issues with patient compliance in terms of consistent and correct administration, inconsistencies with the measured estradiol and testosterone levels, and omission of certain important details (e.g., ointment concentrations, gel/ointment compositions and differences, how the estimated estradiol delivery rates were determined, etc.). As a result of these limitations, there may be only so much that can be taken away from the studies.
In any case, these studies do contribute to an impression that transdermal estradiol gel achieves relatively low estradiol levels and is relatively weak in terms of estrogenic strength even when used at high doses. Other studies of high-dose transdermal estradiol gel/cream, for instance at doses of 3 to 8 mg/day, have reported relatively low estradiol levels similarly, for instance 100 to 200 pg/mL on average (e.g., Lauritzen, 1990; Wiki). Based on these studies, transdermal estradiol gel doesn’t seem to be a very effective or affordable way of achieving the estradiol levels that are needed for adequate suppression of testosterone levels with high-dose estradiol monotherapy in transfeminine people.
In contrast to transdermal estradiol gel, transdermal estradiol patches can consistently achieve much higher estradiol levels and testosterone suppression in comparison (Wiki). About 50 to 100 pg/mL estradiol per 100 μg/day estradiol patch appears to be achieved on average, and multiple 100 μg/day patches up to as high as eight at a time appear to result in approximately linear increases in estradiol levels (Aly, 2020; Wiki). The consistent and higher estradiol levels with estradiol patches makes them generally a more favorable form of estradiol for transdermal administration than estradiol gel and related formulations. Additionally, genital application of transdermal estradiol gel and other transdermal estradiol formulations can allow for dramatically higher estradiol levels (e.g., 5- to 8-fold) than application to conventional transdermal skin sites (e.g., forearm, abdomen) (Aly, 2019). This may also provide transdermal estradiol formulations with greater potential for high-dose estradiol monotherapy.
References
Benoit, G. (1985). Que Penser du Traitement Hormonal du Cancer de la Prostate / Hormonothérapie du Cancer de la Prostate. [Thoughts on the Hormonal Treatment of Prostate Cancer / Hormone Therapy of Prostate Cancer.] Gazette Médicale, 92(5), 33–39. [Google Scholar] [PDF] [Translation]
Lauritzen, C. (1990). Clinical use of oestrogens and progestogens. Maturitas, 12(3), 199–214. [DOI:10.1016/0378-5122(90)90004-P]
Steg, A., Benoit, G., Limouzin-Lamotte, A., Mahoudeau, J., Caillens, M., & Raichvarg, D. (1979). Cancer de la prostate: effets métaboliques des bêta-estradiol par voie percutanée. [Cancer of the prostate: metabolic effect of percutaneous beta-estradiol. / Prostatic carcinoma: metabolic effect of percutaneous beta-estradiol.] La Nouvelle Presse Medicale, 8(46), 3801–3802. [Google Scholar 1] [Google Scholar 2] [Pascal and Francis] [PubMed] [PDF]
Steg, A., Benoit, G., Limouzin-Lamotte, A., Mahoudeau, J., Caillens, M., & Raichvarg, D. (1980). Cancer de la prostate: Effets métaboliques du bêta-estradiol par voie percutanée. [Cancer of the prostate: metabolic effects of percutaneously administered beta-estradiol.] Revue Médicale de la Suisse Romande, 100(11), 895–897. [Google Scholar 1] [Google Scholar 2] [Pascal and Francis] [PubMed] [PDF]
Steg, A., Benoit, G., Maisonneuve, P., Tallet, F., Nahoul, K., Sultan, Y., Raichwarg, D., & Limouzin-Lamotte, M. A. (1983). Étude comparative du diéthylstilboestrol et du 17 bêta-oestradiol per-cutané dans le traitement du cancer de la prostate. [A comparative study of percutaneous 17 beta-estradiol and diethylstilbestrol in the treatment of prostatic cancer.] Annales d’Urologie, 17(4), 197–202. [Google Scholar] [PDF]
Steg, A., & Benoit, G. (1983). Étude comparative de fortes doses d’oestradiol-17 β administrées par voie per-cutanée et de l’orchidectomie bilatérale dans le traitement du cancer de la prostate. [Prostatic carcinoma. Bilateral orchiectomy versus percutaneous administration of large doses of 17 β-estradiol. A comparative study. / Comparative study of percutaneous administration of large doses of 17β œstradiol and bilateral orchidectomy in prostatic carcinoma.] Annales d’Urologie, 17(5), 286–288. [Google Scholar] [Pascal and Francis] [PDF]
Steg, A., Chiche, R., Boccon-Gibod, L., Debré, B., Duchier, J., & Schally, A. V. (1984). Traitement du cancer de la prostate par un agoniste de la LH-RH: le D Trp 6 LH-RH: Résultats préliminaires à propos de trente observations. [Treatment of prostatic cancer with an LH-RH agonist: the D Trp6 LH-RH. Preliminary results in 30 cases. / Treatment of prostate cancer with D Trp6 LH-RH, an LH-RH agonist. Preliminary results of thirty cases.] Annales d’Urologie, 18(6), 388–392. [Google Scholar 1] [Google Scholar 2] [PubMed]
Steg, A., Chiche, R., Boccon-Gibod, L., & Debre, B. (1985). Traitement du cancer de la prostate évolué par un agoniste de la gonadoréline, le DTrp6 LH-RH. Quarante et une observations. [Treatment of advanced prostatic cancer with a gonadorelin agonist, dTrp6 LHRH. 41 cases.] La Presse Médicale (Paris, France: 1983), 14(40), 2045–2048. [Google Scholar 1] [Google Scholar 2] [PubMed]
Steg, A., Chiche, R., Boccon-Gibod, L., Debre, B., & Duchier, J. (1985). Traitement du cancer de la prostate par un agoniste de la LH-RH: le D Trp6 LH-RH―résultats préliminaires à propos de trente observations. [Treatment of prostate cancer with D-TRP6 LH-RH, an LH-RH agonist—preliminary results in 30 cases.] La Semaine des Hôpitaux de Paris, 61(10), 615–618. [Google Scholar 1] [Google Scholar 2]
\ No newline at end of file
+A Review of Studies on Estradiol Levels and Testosterone Suppression with High-Dose Transdermal Estradiol Gel and Ointment in Cisgender Men with Prostate Cancer - Transfeminine Science
A Review of Studies on Estradiol Levels and Testosterone Suppression with High-Dose Transdermal Estradiol Gel and Ointment in Cisgender Men with Prostate Cancer
By Aly | First published June 30, 2019 | Last modified November 2, 2022
Abstract / TL;DR
High-dose estradiol monotherapy, generally used non-orally, is a therapeutic approach for testosterone suppression which is sometimes used in transfeminine people and men with prostate cancer. Limited data are available for this approach with certain forms of estradiol, so considering research in other patient populations besides transfeminine people can provide valuable information. In the 1970s and 1980s, studies were conducted on high-dose transdermal estradiol gel and ointment for the treatment of prostate cancer in men. Estradiol at 3 to 20 mg/day appeared to give 84 to 473 pg/mL estradiol and 105 to 260 ng/dL testosterone in these men. While informative, the findings of the studies are only so useful due to various unfortunate limitations. In any case, it’s apparent that transdermal estradiol gel and related forms don’t seem to be well-suited for achieving the high levels of estradiol that are needed for robust testosterone suppression with high-dose estradiol monotherapy in men with prostate cancer or transfeminine people. High-dose transdermal estradiol patches, or alternatively genital application of transdermal estradiol forms, may be more useful options for this approach on the other hand.
Introduction
High-dose estrogen monotherapy is a means of testosterone suppression which is sometimes used to treat prostate cancer in men. High-dose parenteral estradiol therapy is one particular approach used for this purpose which has less toxicity compared to use of oral and synthetic estrogens. In the late 1970s and early 1980s, high-dose transdermal estradiol gel/ointment was assessed by French researchers in three clinical studies for the treatment of prostate cancer (Steg & Benoit, 1979; Steg et al., 1979; Steg et al., 1980; Steg et al., 1983; Steg & Benoit, 1983; Benoit, 1985). The dosages used in the studies ranged from 3 to 20 mg/day. For comparison, typical doses of transdermal estradiol gel used in transfeminine hormone therapy to achieve physiological estradiol levels range from about 1 to 6 mg/day.
High-dose estradiol monotherapy, generally administered parenterally, is sometimes used as a means of suppressing testosterone levels in transfeminine hormone therapy similarly to the hormonal treatment of prostate cancer. This approach omits the use of antiandrogens and their costs, side effects, and risks, though at the same time incurs risks of higher estradiol exposure. There is limited information available on estradiol levels and testosterone suppression with high-dose estradiol gel and similar forms. Hence, a review of the relevant details from the studies of high-dose estradiol gel for prostate cancer is of value as it can be used to inform the use of high-dose estradiol monotherapy in transfeminine people.
The French studies in question appear to be the only clinical studies of high-dose transdermal estradiol gel/ointment for prostate cancer that have been published. This is in contrast to high-dose transdermal estradiol patches and injectable estradiol esters like polyestradiol phosphate (PEP) and estradiol undecylate (EU), which have been much more widely used in men with prostate cancer.
Data and Excerpts
A Note on Estradiol Delivery Rates
The authors use “γ” (“gamma”) as a unit in their papers. This is a now-deprecated non-SI unit of mass equal to 1 μg (Wiki). That is, “1 γ” means the same thing as “1 μg”. The researchers provided values using this unit as an estimate of the amount of estradiol actually absorbed into the body after taking into account the “cutaneous absorption coefficient” (i.e., transdermal bioavailability) of estradiol. However, when compared to established μg/day values for commercial transdermal estradiol patches and the estradiol levels associated with these patches, the values in the papers are very different from what would be expected. For this reason, and because estimates for transdermal estradiol patches were more rigorously determined and likely to be correct, the delivery rates reported by the authors are probably not accurate. It was important to include them in this article nonetheless however because the researchers modified their transdermal estradiol formulations between their studies, resulting in inconsistencies between the estradiol doses in gel/ointment and their estimated delivery values.
Study 1: Estradiol Gel 3 mg/day versus 6 mg/day
The following three papers pertain to the first study:
Steg, A., Benoit, G., Limouzin-Lamotte, A., Mahoudeau, J., Caillens, M., & Raichvarg, D. (1979). Cancer de la prostate: effets métaboliques des bêta-estradiol par voie percutanée. [Cancer of the prostate: metabolic effect of percutaneous beta-estradiol. / Prostatic carcinoma: metabolic effect of percutaneous beta-estradiol.] La Nouvelle Presse Medicale, 8(46), 3801–3802. [Google Scholar 1] [Google Scholar 2] [Pascal and Francis] [PubMed] [PDF]
Steg, A., Benoit, G., Limouzin-Lamotte, A., Mahoudeau, J., Caillens, M., & Raichvarg, D. (1980). Cancer de la prostate: Effets métaboliques du bêta-estradiol par voie percutanée. [Cancer of the prostate: metabolic effects of percutaneously administered beta-estradiol.] Revue Médicale de la Suisse Romande, 100(11), 895–897. [Google Scholar 1] [Google Scholar 2] [Pascal and Francis] [PubMed] [PDF]
In the study, 21 men with prostate cancer were divided into two groups and treated for 1 month with:
3 mg/day (“300 μg/day”) estradiol in 5 g/day gel applied to the abdomen in one daily dose
6 mg/day (“600 μg/day”) estradiol in 10 g/day gel applied to the abdomen in two daily divided doses
Hormone levels in the study were as follows:
Estradiol levels
Testosterone levels
Pre-treatment
23.2 ± 10.8 pg/mL
Pre-treatment
341 ± 180 ng/dL
E2 gel 3 mg/day
84.2 ± 54.3 pg/mL
E2 gel 3 mg/day
188 ± 125 ng/dL
E2 gel 6 mg/day
184.7 ± 98.46 pg/mL
E2 gel 6 mg/day
105 ± 113 ng/dL
Estrone levels
DHT levels
Pre-treatment
37.6 ± 16.2 pg/mL
Pre-treatment
36 ± 27 ng/dL
E2 gel 3 mg/day
86.7 ± 42.5 pg/mL
E2 gel 3 mg/day
23 ± 14 ng/dL
E2 gel 6 mg/day
150.9 ± 101.4 pg/mL
E2 gel 6 mg/day
12 ± 12 ng/dL
LH levels
FSH levels
Pre-treatment
6.21 ± 6.2 mIU/mL
Pre-treatment
7.56 ± 4.9 mIU/mL
E2 gel 3 mg/day
4.15 ± 3.3 mIU/mL
E2 gel 3 mg/day
6.44 ± 5.0 mIU/mL
E2 gel 6 mg/day
3.41 ± 3.2 mIU/mL
E2 gel 6 mg/day
4.13 ± 5.0 mIU/mL
The researchers stated that the testosterone levels resulting with 6 mg/day estradiol gel (105 ± 113 ng/) were similar to those that are known to occur with 3 mg/day oral diethylstilbestrol. However, this seems to be a somewhat inaccurate statement as 3 mg/day oral diethylstilbestrol has been found to consistently suppress testosterone levels into the castrate range (≤50 ng/dL) in studies (Wiki).
Study 2: Estradiol Ointment 10 mg/day versus Diethylstilbestrol Oral 3 mg/day
The following paper pertains to the second study:
Steg, A., Benoit, G., Maisonneuve, P., Tallet, F., Nahoul, K., Sultan, Y., Raichwarg, D., & Limouzin-Lamotte, M. A. (1983). Étude comparative du diéthylstilboestrol et du 17 bêta-oestradiol per-cutané dans le traitement du cancer de la prostate. [A comparative study of percutaneous 17 beta-estradiol and diethylstilbestrol in the treatment of prostatic cancer.] Annales d’Urologie, 17(4), 197–202. [Google Scholar] [PDF]
In the study, 56 men with prostate cancer were divided into two groups and treated for 3 months with:
10 mg/day (“600 μg/day”) estradiol in “ointment” applied to the abdomen in two daily divided doses
3 mg/day oral diethylstilbestrol in three daily divided doses
Hormone levels in the study were as follows:
Estradiol levels
Testosterone levels
Pre-treatment (E2 group)
30 pg/mL
Pre-treatment (E2 group)
450 ng/dL
E2 ointment 10 mg/day
107 ± 81 pg/mL
E2 ointment 10 mg/day
180 ± 160 ng/dL
Pre-treatment (DES group)
26 pg/mL
Pre-treatment (DES group)
420 ± 130 ng/dL
DES oral 3 mg/day
19 pg/mL
DES oral 3 mg/day
51 ± 0.9 ng/dL
LH levels
FSH levels
Pre-treatment (E2 group)
3.2 mIU/mL
Pre-treatment (E2 group)
4.7 mIU/mL
E2 ointment 10 mg/day
2.0 ± 0.9 mIU/mL
E2 ointment 10 mg/day
1.7 mIU/mL
Pre-treatment (DES group)
4.0 ± 3.2 mIU/mL
Pre-treatment (DES group)
5.8 mIU/mL
DES oral 3 mg/day
1.6 ± 1.2 mIU/mL
DES oral 3 mg/day
1.7 mIU/mL
Some SDs (±) are missing in the table above because not all were provided in the original paper. The SDs that were included above were actually reported in the paper for Study 3.
Some noteworthy translated excerpts from the paper:
This study shows that the clinical effects were more dramatic in the DES group, with a sharper drop in the free plasma testosterone level, than in the E2 group.
E2 has been administered too weakly because it is too low in the commercially used ointment and because application to the thick abdominal skin has a lower absorption coefficient than a thinner skin such as forearms for example. It is possible that a dose equivalent to 15 or 20 mg of gel, applied on the forearms, may allow to lower the testosterone below [100 ng/dL]. The marketing of a more concentrated ointment is therefore desirable, as well as the use of a more efficient absorption site.
The search for new estrogens and new routes of administration is therefore necessary: E2, a natural female hormone, induces no thromboembolic events. It seems to us, therefore, that a larger dose must be proposed to be as effective as 3 mg DES. A gel twice more concentrated is therefore currently under study.
The double-concentration estradiol gel was subsequently reported in Study 3 (see below).
It should be noted that the transdermal estradiol formulation in this study is different from that used in Study 1. Specifically, “6 mg/day estradiol gel” was stated to deliver “600 μg/day estradiol” in Study 1, whereas “10 mg/day estradiol ointment” was stated to deliver “600 μg/day estradiol” in Study 2. These apparent discrepancies might be of relevance to the unexpectedly lower estradiol levels and testosterone suppression in Study 2 compared to Study 1.
Study 3: Estradiol Ointment 20 mg/day versus Bilateral Orchiectomy
The following paper pertains to the third study:
Steg, A., & Benoit, G. (1983). Étude comparative de fortes doses d’oestradiol-17 β administrées par voie per-cutanée et de l’orchidectomie bilatérale dans le traitement du cancer de la prostate. [Prostatic carcinoma. Bilateral orchiectomy versus percutaneous administration of large doses of 17 β-estradiol. A comparative study. / Comparative study of percutaneous administration of large doses of 17β œstradiol and bilateral orchidectomy in prostatic carcinoma.] Annales d’Urologie, 17(5), 286–288. [Google Scholar] [Pascal and Francis] [PDF]
In the study, 38 men with prostate cancer were divided into two groups and treated for 1 month with:
20 mg/day (“1200 μg/day”) estradiol in an ointment applied to the skin in four daily divided doses
Bilateral orchiectomy (i.e., surgical removal of the testes)
Hormone levels in the study were as follows:
Condition
Estradiol levels
Testosterone levels
LH levels
Pre-treatment (E2 group)
52 ± 30 pg/mL
460 ± 230 ng/dL
2.6 ± 0.9 mIU/mL
E2 ointment 20 mg/day
473 ± 375 pg/mL
260 ± 160 ng/dL
1.7 ± 0.8 mIU/mL
Pre-treatment (orchi group)
Not reported
500 ± 160 ng/dL
5.5 ± 6 mIU/mL
Bilateral orchiectomy
Not reported
20 ± 10 ng/dL
19 ± 8 mIU/mL
Some noteworthy translated excerpts from the paper:
The purpose of this study was to determine whether hormonal efficacy [in the treatment of prostate cancer] was enhanced by the administration of large doses of E2. […] The study shows that, whereas orchiectomy lowers plasma testosterone levels dramatically, E2, at [the double dose used in this study compared to our previous study] (1200 [μg] versus 600 [μg]), surprisingly does not further lower it at all, but plasma E2 is substantially increased.
We have found that the administration of E2 causes significant biological changes; E2 is well-absorbed, testosterone is lowered, and LH and FSH are also lowered. But when comparing these effects with those obtained by castration, and with those also observed after administration of 3 mg of diethylstilbestrol (in our previous study), the results are much less brilliant. Indeed: the plasma testosterone is moderately lowered by E2 whereas the fall is much more pronounced with DES and is spectacular with castration; pituitary suppression is comparable with E2 and DES and of course orchiectomy increases LH; and if we compare the results obtained before and after treatment, it is clear that if before treatment the figures are comparable, after treatment the fall is pronounced only with DES and especially with orchiectomy.
The objective of this study was to determine whether doubling the dose of E2 enhances its antiandrogenic effect. [With both a lower dose and a higher dose], E2 is very well-absorbed. [With both doses], the pituitary suppression is identical, but on the other hand, not only is plasma testosterone not lower with [the higher dose], but it seems to be even [higher than with the lower dose]. This difference is also found clinically since with [the higher dose], 10% of patients were improved while with [the lower dose], 30% improvement was obtained.
How can this result be explained? Perhaps this is due to the contrary effects of E2 on androgens. Indeed: E2 on the one hand suppresses pituitary activity, which leads to a fall of testicular testosterone secretion, and at the same time E2 decreases 5α-reductase activity in the prostate; on the other hand, E2 causes an increase in SHBG and competes with free testosterone binding to SHBG and in this way increases the proportion of active free testosterone. In addition, testosterone also increases the level of cytoplasmic androgen receptors.
This work shows that E2 is well-absorbed percutaneously and causes practically no cardiovascular events. On the other hand, it appears that the antiandrogenic effect is significantly less by this route than that obtained by diethylstilbestrol and castration, and that in any case, we cannot improve the efficacy by increasing the dose of E2.
The finding that the 20 mg/day estradiol ointment resulted in less suppression of testosterone levels than the 10 mg/day estradiol ointment despite markedly higher estradiol levels is surprising. However, the researchers’ theoretical explanation of the result seems questionable. Abundant clinical research with high-dose estradiol for prostate cancer (e.g., transdermal patches, injectable polyestradiol phosphate injections, injectable estradiol undecylate) has shown stronger testosterone suppression with high estradiol levels in this range or below and seems to thoroughly contradict their results. Studies have consistently shown that estradiol levels of 200 to 500 pg/mL and above suppress testosterone levels by 90% and greater (to ~50 ng/dL and below) (Wiki; Graphs). Instead of the authors’ interpretation of their unexpected results, it seems possible that the testosterone assays for this study may have been inaccurate or perhaps some other methodological problem may have been responsible.
The concentration and dosage of estradiol ointment in this study were double those of Study 2, yet the estradiol levels measured in this study were almost 5-fold higher than those in Study 2. It’s possible that the higher concentration of ointment used may have resulted in disproportionately greater absorption, as one study found that the smaller the application area of estradiol gel (and hence higher the post-application concentration), the greater the resulting estradiol levels (Graph). On the other hand, it’s possible that the estradiol assays were inaccurate (as also suggested for testosterone above). Lastly, in contrast to the previous two papers, the authors don’t state where the ointment was applied in this study. It was probably the abdomen similarly, but this isn’t certain; they may have used one or more other locations with differing skin permeability (as they discussed the possibility of doing in Study 1). It’d be expected that they’d mention this change though, which perhaps makes the possibility unlikely.
Review Article
A review of hormone therapy for prostate cancer was also published by one of the researchers:
Benoit, G. (1985). Que Penser du Traitement Hormonal du Cancer de la Prostate / Hormonothérapie du Cancer de la Prostate. [Thoughts on the Hormonal Treatment of Prostate Cancer / Hormone Therapy of Prostate Cancer.] Gazette Médicale, 92(5), 33–39. [Google Scholar] [PDF] [Translation]
In the paper, she briefly mentioned her and her colleagues’ studies on high-dose transdermal estradiol gel/ointment for prostate cancer and provided some additional information pertaining to these studies. Here are the relevant translated excerpts from the paper:
In a study in Cochin (16), the efficacy of diethylstilbestrol was 50% of objective responses, but at a cost of 23% of thromboembolic events. These thromboembolic events are similar to the accidents that occur in women taking oral estrogen–progestogens. These are oral synthetic estrogens. In a series of diethylstilbestrol-treated prostate cancers, Steg (16) has shown that this treatment induces an increase in triglycerides and a decrease in coagulation factor VIII. Abbou (1) found, on his behalf, an increase in circulating immune complexes in patients with thrombosis under synthetic estrogen–progestogen therapy.
It therefore seems to us no longer possible to prescribe diethylstilbestrol as first intention. To reduce these cardiovascular events, most authors have tried to use natural estrogens administered intramuscularly, subcutaneously, or percutaneously. Cochin’s experience of using a natural estrogen (17-beta-estradiol) percutaneously has shown that this treatment may be effective, but that it is very difficult to administer: one in two patients is unable to apply the treatment correctly and regularly, which greatly reduces the use of such treatment (15).
As an indication, we report several studies made successively in Cochin (16, 17) with diethylstilbestrol, a natural estrogen (17-beta-estradiol), testicular pulpectomy, and an LHRH analogue administered subcutaneously.
The results confirm that diethylstilbestrol causes thromboembolic events. These different estrogenic treatments promote gynecomastia. Medical castration by LHRH analogues or surgical pulpectomy causes hot flushes. All these treatments reach, in a variable way, libido and sexual potency. This last effect is complex: it is known that castration, in young men, after puberty, does not regularly cause impotence, as shown by the history of castrates. However, it is necessary to warn the patient that each of these treatments can reach his manhood.
Synthetic estrogens, especially diethylstilbestrol, should no longer be used as first-line agents in the treatment of metastatic prostate cancer because of their thromboembolic risk. Natural estrogens do not seem efficient enough to be used regularly. Complete castration performs excessive mutilation. In our opinion, only testicular pulpectomy, LHRH analogues, and antiandrogens remain in competition.
The review also contains the following adapted summary table of data from their studies:
DES
E2 gel/ointment
Orchiectomy
GnRH analogue
Testosterone levels
50 ng/dL
100 ng/dL
20 ng/dL
50 ng/dL
50% partial remission
50%
30%
33%
41%
Cardiovascular events
23%
0%
0%
0%
The gonadotropin-releasing hormone (GnRH) analogue data were from other studies and papers by the same researchers (Steg et al., 1984; Steg et al., 1985a; Steg et al., 1985b). These studies did not assess transdermal estradiol and hence are not otherwise discussed in the present article.
The authors’ comments in this paper raise the additional question of whether inconsistent and suboptimal exposure to estradiol gel/ointment may have influenced the findings of their studies.
Summary and Discussion
In the reviewed clinical studies of high-dose transdermal estradiol gel/ointment in men with prostate cancer, the following results were obtained in terms of changes in measured hormone levels:
Estradiol dose
Estradiol levels
Testosterone levels
Before treatment
23–52 pg/mL
341–460 ng/dL
3 mg/day gel (“300 μg/day”)
84 pg/mL
188 ng/dL
6 mg/day gel (“600 μg/day”)
185 pg/mL
105 ng/dL
10 mg/day ointment (“600 μg/day”)
107 pg/mL
180 ng/dL
20 mg/day ointment (“1200 μg/day”)
473 pg/mL
260 ng/dL
Unfortunately, the data reported in these studies is not as useful as might have been hoped. This is due to inconsistencies with the transdermal estradiol formulations and doses used, reported issues with patient compliance in terms of consistent and correct administration, inconsistencies with the measured estradiol and testosterone levels, and omission of certain important details (e.g., ointment concentrations, gel/ointment compositions and differences, how the estimated estradiol delivery rates were determined, etc.). As a result of these limitations, there may be only so much that can be taken away from the studies.
In any case, these studies do contribute to an impression that transdermal estradiol gel achieves relatively low estradiol levels and is relatively weak in terms of estrogenic strength even when used at high doses. Other studies of high-dose transdermal estradiol gel/cream, for instance at doses of 3 to 8 mg/day, have reported relatively low estradiol levels similarly, for instance 100 to 200 pg/mL on average (e.g., Lauritzen, 1990; Wiki). Based on these studies, transdermal estradiol gel doesn’t seem to be a very effective or affordable way of achieving the estradiol levels that are needed for adequate suppression of testosterone levels with high-dose estradiol monotherapy in transfeminine people.
In contrast to transdermal estradiol gel, transdermal estradiol patches can consistently achieve much higher estradiol levels and testosterone suppression in comparison (Wiki). About 50 to 100 pg/mL estradiol per 100 μg/day estradiol patch appears to be achieved on average, and multiple 100 μg/day patches up to as high as eight at a time appear to result in approximately linear increases in estradiol levels (Aly, 2020; Wiki). The consistent and higher estradiol levels with estradiol patches makes them generally a more favorable form of estradiol for transdermal administration than estradiol gel and related formulations. Additionally, genital application of transdermal estradiol gel and other transdermal estradiol formulations can allow for dramatically higher estradiol levels (e.g., 5- to 8-fold) than application to conventional transdermal skin sites (e.g., forearm, abdomen) (Aly, 2019). This may also provide transdermal estradiol formulations with greater potential for high-dose estradiol monotherapy.
References
Benoit, G. (1985). Que Penser du Traitement Hormonal du Cancer de la Prostate / Hormonothérapie du Cancer de la Prostate. [Thoughts on the Hormonal Treatment of Prostate Cancer / Hormone Therapy of Prostate Cancer.] Gazette Médicale, 92(5), 33–39. [Google Scholar] [PDF] [Translation]
Lauritzen, C. (1990). Clinical use of oestrogens and progestogens. Maturitas, 12(3), 199–214. [DOI:10.1016/0378-5122(90)90004-P]
Steg, A., Benoit, G., Limouzin-Lamotte, A., Mahoudeau, J., Caillens, M., & Raichvarg, D. (1979). Cancer de la prostate: effets métaboliques des bêta-estradiol par voie percutanée. [Cancer of the prostate: metabolic effect of percutaneous beta-estradiol. / Prostatic carcinoma: metabolic effect of percutaneous beta-estradiol.] La Nouvelle Presse Medicale, 8(46), 3801–3802. [Google Scholar 1] [Google Scholar 2] [Pascal and Francis] [PubMed] [PDF]
Steg, A., Benoit, G., Limouzin-Lamotte, A., Mahoudeau, J., Caillens, M., & Raichvarg, D. (1980). Cancer de la prostate: Effets métaboliques du bêta-estradiol par voie percutanée. [Cancer of the prostate: metabolic effects of percutaneously administered beta-estradiol.] Revue Médicale de la Suisse Romande, 100(11), 895–897. [Google Scholar 1] [Google Scholar 2] [Pascal and Francis] [PubMed] [PDF]
Steg, A., Benoit, G., Maisonneuve, P., Tallet, F., Nahoul, K., Sultan, Y., Raichwarg, D., & Limouzin-Lamotte, M. A. (1983). Étude comparative du diéthylstilboestrol et du 17 bêta-oestradiol per-cutané dans le traitement du cancer de la prostate. [A comparative study of percutaneous 17 beta-estradiol and diethylstilbestrol in the treatment of prostatic cancer.] Annales d’Urologie, 17(4), 197–202. [Google Scholar] [PDF]
Steg, A., & Benoit, G. (1983). Étude comparative de fortes doses d’oestradiol-17 β administrées par voie per-cutanée et de l’orchidectomie bilatérale dans le traitement du cancer de la prostate. [Prostatic carcinoma. Bilateral orchiectomy versus percutaneous administration of large doses of 17 β-estradiol. A comparative study. / Comparative study of percutaneous administration of large doses of 17β œstradiol and bilateral orchidectomy in prostatic carcinoma.] Annales d’Urologie, 17(5), 286–288. [Google Scholar] [Pascal and Francis] [PDF]
Steg, A., Chiche, R., Boccon-Gibod, L., Debré, B., Duchier, J., & Schally, A. V. (1984). Traitement du cancer de la prostate par un agoniste de la LH-RH: le D Trp 6 LH-RH: Résultats préliminaires à propos de trente observations. [Treatment of prostatic cancer with an LH-RH agonist: the D Trp6 LH-RH. Preliminary results in 30 cases. / Treatment of prostate cancer with D Trp6 LH-RH, an LH-RH agonist. Preliminary results of thirty cases.] Annales d’Urologie, 18(6), 388–392. [Google Scholar 1] [Google Scholar 2] [PubMed]
Steg, A., Chiche, R., Boccon-Gibod, L., & Debre, B. (1985). Traitement du cancer de la prostate évolué par un agoniste de la gonadoréline, le DTrp6 LH-RH. Quarante et une observations. [Treatment of advanced prostatic cancer with a gonadorelin agonist, dTrp6 LHRH. 41 cases.] La Presse Médicale (Paris, France: 1983), 14(40), 2045–2048. [Google Scholar 1] [Google Scholar 2] [PubMed]
Steg, A., Chiche, R., Boccon-Gibod, L., Debre, B., & Duchier, J. (1985). Traitement du cancer de la prostate par un agoniste de la LH-RH: le D Trp6 LH-RH―résultats préliminaires à propos de trente observations. [Treatment of prostate cancer with D-TRP6 LH-RH, an LH-RH agonist—preliminary results in 30 cases.] La Semaine des Hôpitaux de Paris, 61(10), 615–618. [Google Scholar 1] [Google Scholar 2]
\ No newline at end of file
diff --git a/transfemscience.org/articles/injectable-e2-meta-analysis/index.html b/transfemscience.org/articles/injectable-e2-meta-analysis/index.html
index 27844039..2c88b1d7 100644
--- a/transfemscience.org/articles/injectable-e2-meta-analysis/index.html
+++ b/transfemscience.org/articles/injectable-e2-meta-analysis/index.html
@@ -1 +1 @@
-An Informal Meta-Analysis of Estradiol Curves with Injectable Estradiol Preparations - Transfeminine Science
An Informal Meta-Analysis of Estradiol Curves with Injectable Estradiol Preparations
By Aly | First published July 16, 2021 | Last modified June 27, 2024
Abstract / TL;DR
Injectable estradiol preparations such as estradiol valerate and estradiol cypionate in oil are frequently used as estrogens in transfeminine hormone therapy. However, there is little characterization of these preparations in transfeminine people and dosing recommendations by transgender health guidelines appear to be based on expert opinion rather than on clinical data. To help shed light on the properties of injectable estradiol and to better inform dosing considerations in transfeminine people, an informal meta-analysis of available clinical data on estradiol concentration–time curves with major injectable estradiol formulations was conducted. The included preparations were injectable estradiol benzoate in oil, estradiol valerate in oil, estradiol cypionate both in oil and as a suspension, estradiol enanthate in oil, estradiol undecylate in oil, and polyestradiol phosphate. The literature was searched for clinical concentration–time data with these injectable estradiol esters and these data were collected and analyzed. Meta-analysis consisted of data for each injectable estradiol preparation being processed and fit with pharmacokinetic models. Selected pharmacokinetic parameters were additionally determined and reported. The results of this work were discussed with regard to characteristics of injectable estradiol preparations like curve shapes, durations, estrogenic exposure, and variability between people and studies. Recommendations for injectable estradiol preparations by transgender health guidelines were also explored in light of the present results. Current guidelines recommend doses of these preparations that appear to be highly excessive with injection intervals that are too widely spaced. Based on the findings of the present meta-analysis, recommendations by guidelines should be reassessed. Finally, the fitted curves in this work were incorporated into an interactive web-based injectable estradiol simulator intended for use by transfeminine people and their medical providers to help guide therapeutic decisions.
Introduction
Estradiol is the main estrogen used in transfeminine hormone therapy and is available in a variety of different forms for use by different routes of administration. The most commonly employed forms are oral, sublingual, transdermal, and injectable preparations. Injectable estradiol preparations have been discontinued in many countries and hence are unavailable for use in transfeminine hormone therapy in many parts of the world, for instance in most of Europe (Glintborg et al., 2021). However, they are still used by many transfeminine people particularly in the United States and in the do-it-yourself (DIY) community. The most commonly used forms include estradiol valerate, estradiol cypionate, and estradiol enanthate all in oil. Injectable estradiol preparations have certain advantages over other estradiol forms that make them a popular choice for use in transfeminine hormone therapy. These include often lower cost, capacity to easily achieve higher estradiol levels that can be useful for testosterone suppression, less frequent administration, and theoretically reduced health risks relative to oral estradiol at equivalent doses due to the lack of the first pass with this route (Aly, 2020). The higher estradiol levels with injections are particularly useful for estradiol monotherapy, in which an antiandrogen is not used.
Clinically used injectable estradiol preparations are formulated not as estradiol but as estradiol esters. When injected into muscle or fat in oil solutions or crystalline aqueous suspensions, these estradiol esters form depots at the injection site from which they are slowly released. Subsequent to release, estradiol esters are rapidly metabolized into estradiol and hence act as prodrugs. When estradiol itself is given by intramuscular injection in an aqueous solution or oil solution, it is rapidly absorbed and has a very short duration. Due to having lipophilic esters, most clinically used injectable estradiol esters are more fat-soluble than estradiol (as measured by oil–water partition coefficient (P)) (Table). When these esters are administered as oil solutions by intramuscular or subcutaneous injection, their increased lipophilicity causes them to be released from the injection-site depot more slowly than estradiol and to therefore have longer durations. In the case of fatty acid esters, the longer the chain length of the ester—as in e.g. estradiol valerate (5 carbons) vs. estradiol enanthate (7 carbons) vs. estradiol undecylate (10 carbons)—the greater the fat solubility, the slower the rate of release from the depot, and the longer the time to peak levels and duration (Edkins, 1959; Sinkula, 1978; Chien, 1981; Kuhl, 2005; Kalicharan, 2017; Vhora et al., 2019). The durations of both injectable oil solutions and aqueous suspensions depend on the ester and its particular physicochemical properties, but the characteristics of these preparations are different and they work in distinct ways to produce their depot effects (Enever et al., 1983; Aly, 2019). The durations of oil solutions are dependent on the lipophilicity of the ester as well as oil vehicle, whereas the durations of aqueous suspensions depend on the properties of the ester crystal lattice as well as crystal sizes (Chien, 1981; Enever et al., 1983; Aly, 2019). The polymeric estradiol ester polyestradiol phosphate is more hydrophilic (water-soluble) than estradiol and works differently than other injectable estradiol preparations. Ιt is composed of many estradiol molecules linked together via phosphate esters (on average 13 molecules of estradiol per one molecule of polyestradiol phosphate) and has a prolonged duration due to slow cleavage into estradiol following injection. Estradiol esters are able to substantially prolong the duration of estradiol when used as injectables and these preparations have durations ranging from days to months depending on the ester and how it is formulated (Table).
In order to aid understanding of concentration–time profiles with injectable estradiol preparations, I’ve developed an interactive web-based injectable estradiol simulator for transfeminine people and their medical providers. During work on this simulator, it became apparent that there is substantial variability in estradiol levels and curve shapes between different studies even with the same injectable estradiol ester. The injectable estradiol simulator was originally designed to simulate curves from only a single well-known pharmacokinetic study that directly compared estradiol benzoate, estradiol valerate, and estradiol cypionate in oil (Oriowo et al., 1980 [Graph]). However, due to the considerable differences in estradiol levels and curves across studies, it was decided that relying on only one study for such a project would be untenable. Instead, for the simulations to be reasonably accurate to the available data, many studies would need to be incorporated. Including additional studies would also allow for inclusion of other injectable estradiol esters in the simulator. As a result, the present work—an informal meta-analysis of estradiol curves with injectable estradiol formulations—was conducted for the simulator project.
Methods
A literature search was performed to identify studies reporting clinical estradiol concentration–time data with major injectable estradiol formulations (Table 1). All of these preparations have been used in transfeminine hormone therapy at one time or another in different parts of the world, although only estradiol valerate in oil and estradiol cypionate in oil are widely used today. Some of the injectable preparations included have notably been discontinued. Acceptable data for the search included mean and individual estradiol concentration data and Cmax estradiol levels (mean peak estradiol levels of individual subjects at time Tmax). Databases like PubMed, Google Scholar, and WorldCat were searched using relevant keywords (e.g., estradiol ester names and variations thereof as well as major brand names). Publications with relevant information were catalogued for data collection. Only single-dose data and multi-dose data that allowed estradiol levels to return to baseline between doses (as in e.g. repeated once-monthly combined injectable contraceptives) were included. Studies were included regardless of the hypothalamic–pituitary–gonadal axis (HPG axis) status of the participants. The study selection criteria aimed to maximize data inclusion due to scarcity of data for several preparations. If however there were many studies for a specific preparation, studies with only 1 or 2 subjects were generally skipped due to the limited additional value that they would provide. When data were in figures in papers—as was generally the case—they were extracted from the graphs using WebPlotDigitizer.
Table 1: Major injectable estradiol formulations (ordered roughly from shortest- to longest-acting):
Following their collection, data were processed, aggregated, and modeled. Data were adjusted for endogenous estradiol production and were normalized by dose. Adjustment for endogenous estradiol production was generally done via subtraction of baseline estradiol levels. In a number of cases however, subtraction of trough estradiol levels or of estradiol levels from a control group was required instead. Data were also weighted by sample size. In a handful of instances, certain missing information (e.g., time to peak levels, baseline levels, subject body weights) was filled in with reasonable assumptions to help maximize data inclusion. Data were processed in the form of mean estradiol curve data rather than individual-subject data (except for rare n=1 studies). The combined processed data from all studies for each injectable estradiol preparation were fit via least squares regression to one-, two-, and three-compartmentpharmacokinetic models with first-order absorption and elimination that were obtained from the literature and other sources (e.g., Colburn, 1981; Wagner, 1993; Fisher & Shafer, 2007; Lixoft, 2008; Abuhelwa, Foster, & Upton, 2015; Certara, 2020). These models fit most curves from individual studies very well. Fitting the combined curve fits of all individual studies (as opposed to fitting all of the combined processed data directly) was additionally evaluated for each injectable estradiol preparation, and if it was feasible for the preparation and allowed for better fitting results, was employed instead. Fitting directly to the combined processed data has the effect of weighting individual studies by quantity of time points, whereas fitting the combined curve fits of studies eliminates this. The Akaike information criterion (AIC) was used to help guide model selection for fitting of the preparations. Curve fitting was performed using the Python library Lmfit with the Levenberg–Marquardt algorithm. Cmax concentrations are a different form of data than mean curve estradiol concentration–time data, and for this reason, were not included in the fitting unless data were very limited for a given injectable estradiol preparation. Outlying data were also excluded from fitting in a number of instances and this allowed for improved curve fits with more uniform area-under-the-curve levels. The main criterion used for excluding curves was fit area-under-the-curve levels that deviated considerably from what was typical for the injectable estradiol preparations (generally less than about 50% of the average or greater than about 150% of the average).
A selection of pharmacokinetic parameters were calculated for each injectable estradiol preparation using the single-dose fit curves and compartmental pharmacokinetic analyses. These parameters included maximal or peak concentrations of estradiol after a single dose scaled to 5 mg (Cmax), time to maximal concentrations of estradiol after a single dose (Tmax), total area-under-the-curve concentrations of estradiol after a single dose (AUC0–∞), terminal elimination half-life after a single dose (t1/2), and the terminal 90% life after a single dose (t90%) (calculated as t1/2 × 3.322). In addition, selected pharmacokinetic parameters were calculated for simulated repeated administration of each injectable preparation at steady state with a dose and dose interval of 5 mg once every 7 days using the single-dose fit curves and compartmental pharmacokinetic analyses. These parameters included time to peak concentrations of estradiol (Tmax), peak and trough concentrations of estradiol (Cmax and Cmin, respectively), peak–trough difference (PTD; Cmax – Cmin), peak–trough ratio (PTR; Cmax ÷ Cmin), and integratedmean concentrations of estradiol (Cavg). Simulation of repeated administration was performed by stacking estradiol levels for multiple injections. Cmax and Tmax were defined and calculated in general as peak estradiol level and time to peak level of the fit mean curve as opposed to the mean peak level and mean time to peak level of individual subjects. This is because the latter would not be possible to compute as most studies reported only estradiol mean curve data. Pharmacokinetic parameters were calculated using relevant pharmacokinetic equations and, as a sanity check, were compared against those computed by PKSolver, a Microsoft Excel pharmacokinetics add-in program (Zhang et al., 2010).
Results
The figures in the subsequent sections show the original data from studies adjusted for endogenous estradiol levels and normalized to a common dose as well as the curve fits to the data (or alternatively the curve fits of the fits of the data depending on the preparation) for the included injectable estradiol preparations. Estradiol benzoate, estradiol cypionate in oil, and estradiol cypionate suspension were fit to the fits of all individual studies for these preparations, whereas estradiol enanthate, estradiol undecylate, and polyestradiol phosphate were fit directly to the combined processed data for these esters. In the case of estradiol valerate, the two fitting approaches gave nearly identical curves, and so fitting the combined processed original data was done for simplicity for this preparation. Cmax studies were excluded in the fitting for all preparations except estradiol enanthate, for which available estradiol concentration–time data were otherwise very limited. The data for the injectable estradiol preparations were generally fit best by a three-compartment pharmacokinetic model (Desmos). As a result, and for consistency, this model was used in the fitting of all preparations.
Estradiol Benzoate
Injectable estradiol benzoate has been extensively used in the past in scientific research, most notably in studies elucidating the function and dynamics of the HPG axis. One such use of estradiol benzoate has been the estrogen provocation test, a diagnostic test of HPG axis function. Due to its use in research, substantial estradiol concentration–time data with injectable estradiol benzoate exists. A total of 26 publications and concentration–time data for 355 individual injections were identified (Table 2).
Table 2: Studies of injectable estradiol benzoate (Spreadsheet; Plotly):
a Total number of injections, not total number of subjects.
A number of studies were excluded from fitting due to much higher or lower area-under-the-curve levels than average. A couple of studies were omitted from the meta-analysis as they only reported total estrogen levels rather than estradiol levels with estradiol benzoate (Akande, 1974; Weiss, Nachtigall, & Ganguly, 1976). Two studies were omitted due partly to being very old and using very early and inaccurate blood tests (Varangot & Cedard, 1957; Ittrich & Pots, 1965 [Graph]). The processed original data and fit of fits curve for estradiol benzoate are shown in Figure 1.
Figure 1: Published estradiol concentration–time curves and fit of fit curves (thick black or white line) with a single intramuscular injection of estradiol benzoate in oil solution over a period of 7 days. Each curve was adjusted for endogenous estradiol levels, normalized to a dose of 5 mg, and fit with a compartmental pharmacokinetic model. Following this, the combined fit curves of the individual studies were fit using the same pharmacokinetic model. The original data from the studies for estradiol benzoate are also provided elsewhere (Spreadsheet; Plotly).
Estradiol Valerate
Studies with curve data on injectable estradiol valerate come from its use in menopausal hormone therapy and other therapeutic indications for estrogens, its use in combined injectable contraceptives, and use in scientific research. A total of 28 publications and concentration–time data for 309 individual injections were identified for estradiol valerate (Table 3).
Table 3: Studies of injectable estradiol valerate (Spreadsheet; Plotly):
Study
na
Subjects
Dose
Reference(s)
S7175
12
Premenopausal women with menstrual migraine (n=10) and amenorrheic/postmenopausal women with history of menstrual migraine (n=2)
Normally cycling transmasculine people not on hormone therapy (n=31), transfeminine people not on hormone therapy (n=14), and gonadally intact transfeminine people on oral estrogen therapy (n=9)
a Total number of injections, not total number of subjects.
A few of these studies were excluded from fitting due generally to much higher or lower area-under-the-curve levels than average or due to being Cmax data. One study was omitted as it only reported estrone levels rather than estradiol levels (Ibrahim, 1996). Another study was not included due to being in pregnant women with concomitant pregnancy termination (Garner & Armstrong, 1977). One last study was omitted due partly to being very old and using very early and inaccurate blood tests (Ittrich & Pots, 1965 [Graph]). The processed original data and fit curve for estradiol valerate are shown in Figure 2.
Figure 2: Published estradiol concentration–time curves and fit curve (thick black or white line) with a single intramuscular injection of estradiol valerate in oil solution over a period of 30 days. Curves were adjusted for endogenous estradiol levels, normalized to a dose of 10 mg, and fit with a compartmental pharmacokinetic model. Fitting of the combined fits of individual studies for this preparation was explored but gave a nearly identical overall curve, so the overall fit curve for the combined processed original data was used for simplicity for this preparation. The original data from the studies for estradiol valerate are also provided elsewhere (Spreadsheet; Plotly).
Estradiol Cypionate Oil
Estradiol cypionate in oil is used in menopausal hormone therapy and for other estrogen indications. However, its use has been more limited relative to other injectable estradiol preparations, like estradiol valerate. Only a handful of studies with relevant data were identified for estradiol cypionate in oil. This included 4 publications and estradiol concentration–time data for 49 individual injections (Table 4).
Table 4: Studies of injectable estradiol cypionate in oil (Spreadsheet; Plotly):
a Total number of injections, not total number of subjects.
No curves were excluded from fitting in the case of this preparation. The processed original data and fit of fit curves for estradiol cypionate in oil are shown in Figure 3.
Figure 3: Published estradiol concentration–time curves and fit of fit curves (thick black or white line) with a single intramuscular injection of estradiol cypionate in oil solution over a period of 30 days. Each curve was adjusted for endogenous estradiol levels, normalized to a dose of 5 mg, and fit with a compartmental pharmacokinetic model. Following this, the combined fit curves of the individual studies were fit using the same pharmacokinetic model. The original data from the studies for estradiol cypionate in oil are also provided elsewhere (Spreadsheet; Plotly).
Estradiol Cypionate Suspension
Estradiol cypionate suspension has been used exclusively in combined injectable contraceptives. For this reason, many relatively high quality pharmacokinetic studies with this injectable preparation have been conducted. A total of 9 publications and estradiol concentration–time data for 131 individual injections were identified for estradiol cypionate suspension (Table 5).
Table 5: Studies of injectable estradiol cypionate suspension (Spreadsheet; Plotly):
a Total number of injections, not total number of subjects. b By subcutaneous injection rather than intramuscular injection.
One of these studies used subcutaneous injection instead of the usual intramuscular injection but the resulting curve was very similar to the curve for intramuscular injection in the same study (Sierra-Ramírez et al., 2011 [Graph]). Several Cmax studies were excluded from fitting for this preparation. One pharmacokinetic study only measured estradiol cypionate levels rather than estradiol levels and hence was not included (Martins et al., 2019 [Graph]). The processed original data and fit of fit curves for estradiol cypionate suspension are shown in Figure 4.
Figure 4: Published estradiol concentration–time curves and fit of fits curve (thick black or white line) with a single intramuscular (or in one case subcutaneous) injection of a microcrystalline aqueous suspension of estradiol cypionate over a period of 30 days. Each curve was adjusted for endogenous estradiol levels, normalized to a dose of 5 mg, and fit with a compartmental pharmacokinetic model. Following this, the combined fit curves of the individual studies were fit using the same pharmacokinetic model. The original data from the studies for estradiol cypionate suspension are also provided elsewhere (Spreadsheet; Plotly).
Estradiol Enanthate
Estradiol enanthate has been used exclusively in combined injectable contraceptives. Several pharmacokinetic studies have been conducted with it because of this. A total of 7 publications and concentration–time data for 270 individual injections were identified for estradiol enanthate (Table 6).
Table 6: Studies of injectable estradiol enanthate (Spreadsheet; Plotly):
a Total number of injections, not total number of subjects.
Of the available data, 216 of the injections were from a single study and mainly included only Cmax levels. Wiemeyer et al. (1986) was excluded from fitting due to having unusually high area-under-the-curve levels with a small sample size (n=3). Because of the scarcity of estradiol concentration–time data available for estradiol enanthate, Cmax studies were included in the fitting for this preparation. The processed original data and fit curve for estradiol enanthate are shown in Figure 5.
Figure 5: Published estradiol concentration–time curves and fit curve (thick black or white line) with a single intramuscular injection of estradiol enanthate in oil solution over a period of 30 days. Curves were adjusted for endogenous estradiol levels, normalized to a dose of 10 mg, and fit with a compartmental pharmacokinetic model. The original data from the studies for estradiol enanthate are also provided elsewhere (Spreadsheet; Plotly).
Estradiol Undecylate
Estradiol undecylate was formerly used in the treatment of prostate cancer and in menopausal hormone therapy as well as for other estrogen therapeutic indications. However, it was discontinued many years ago and is no longer used today. Nonetheless, estradiol undecylate is of significant historical interest as an injectable estradiol preparation. A total of 4 publications and estradiol concentration–time data for 7 individual injections were identified for estradiol undecylate (Table 7).
Table 7: Studies of injectable estradiol undecylate (Spreadsheet; Plotly):
a Total number of injections, not total number of subjects.
Unfortunately, the identified data were of very low quality, with small sample sizes and considerable variations in estradiol levels. Moreover, estradiol undecylate is a very long-acting injectable estradiol ester with a duration measured in months, and the follow up in these studies only went to about 2 weeks post-injection. For these reasons, it was not possible to fit the data for estradiol undecylate in a reasonably accurate way—as suggested by area-under-the-curve estradiol levels that were only around one-third those of the other non-polymeric injectable estradiol esters. Limited multi-dose hormone concentration–time data also exist for estradiol undecylate, but these data could not be incorporated (Jacobi & Altwein, 1979 [Graph]; Jacobi et al., 1980 [Graph]; Derra, 1981 [Graph]). The processed original data and fit curve for estradiol undecylate are shown in Figure 6.
Figure 6: Published estradiol concentration–time curves and fit curve (thick black or white line) with a single intramuscular injection of estradiol undecylate in oil solution over a period of 90 days. Curves were adjusted for endogenous estradiol levels, normalized to a dose of 50 mg, and fit with a compartmental pharmacokinetic model. The original data from the studies for estradiol undecylate are also provided elsewhere (Spreadsheet; Plotly).
Polyestradiol Phosphate
Polyestradiol phosphate has been used primarily in the treatment of prostate cancer but has also been used for estrogen therapeutic indications like treatment of breast cancer and menopausal hormone therapy. While this injectable estradiol preparation has been used widely in the past, it appears to have recently been discontinued. All of the identified studies with estradiol concentration–time data on polyestradiol phosphate were in men with prostate cancer. A total of 11 publications and concentration–time data for 114 individual injections were identified for polyestradiol phosphate (Table 8).
Table 8: Studies of injectable polyestradiol phosphate (Spreadsheet; Plotly):
a Total number of injections, not total number of subjects.
A few older and strongly outlying studies were excluded from the fitting. The processed original data and fit curve for polyestradiol phosphate are shown in Figure 7.
Figure 7: Published estradiol concentration–time curves and fit curve (thick black or white line) with a single intramuscular injection of an aqueous solution of polyestradiol phosphate over a period of 90 days. The graph was clipped to maximum estradiol levels of 600 pg/mL (~2,200 pmol/L) for better viewability. Curves were adjusted for endogenous estradiol levels, normalized to a dose of 160 mg, and fit with a compartmental pharmacokinetic model. The original data from the studies for polyestradiol phosphate are also provided elsewhere (Spreadsheet; Plotly).
Other Injectable Estradiol Preparations
A number of clinical studies with estradiol concentration–time data for other injectable estradiol preparations were also identified during literature search:
Estradiol (unesterified) in an “aqueous” preparation (type of aqueous preparation unspecified but probably a microcrystalline aqueous suspension) (Jones et al., 1978 [Graph])
These preparations were not included in the present meta-analysis due to their relative obscurity and the limited data available for them. In addition, there were concerns about fitting the used pharmacokinetic models to the formulations with multiple estradiol components and to the microsphere formulations.
No estradiol concentration–time data were identified for certain other injectable estradiol forms of interest, like unesterified estradiol in aqueous solution, estradiol benzoate as a microcrystalline aqueous suspension (Agofollin Depot; Ovocyclin M), or estradiol benzoate butyrate/dihydroxyprogesterone acetophenide in oil (Redimen, Soluna, Unijab) (another lesser-known combined injectable contraceptive).
All Injectable Estradiol Preparations Together
Figure 8 shows the curve fits for all of the injectable estradiol preparations scaled to a single dose of 5 mg (or equivalent) together in the same figure. The dose for polyestradiol phosphate was scaled to be about 6.5 times higher than the other injectable estradiol preparations in order to make it roughly equivalent to them in terms of total estradiol exposure. This was because polyestradiol phosphate was found to produce much lower area-under-the-curve estradiol levels than the other injectable estradiol preparations (see the Discussion section). Estradiol undecylate was not included in Figure 8 as a decent fit curve could not be obtained for it due to the very limited data available for this preparation.
Figure 8: Curve fits of published estradiol concentration–time data with different injectable estradiol preparations by intramuscular injection scaled to equivalent doses and plotted over a period of 20 days in a single combined graph. Polyestradiol phosphate is scaled to a 6.5-fold higher dose that is roughly equivalent to that for the other esters as it gave total estradiol levels that were around 6 or 7 times lower than the other esters at the same dose. An alternative version of this figure without estradiol benzoate and with the x-axis spanning 30 days is also provided (Graph).
Figure 9 shows simulated curves at steady state for repeated administration of all of the injectable estradiol preparations scaled to a dose of 5 mg (or equivalent) once every 7 days. As with the previous figure, the dose for polyestradiol phosphate was scaled to be about 6.5 times higher than the other injectable estradiol preparations and estradiol undecylate was not included in the figure.
Figure 9: Simulated curves at steady state for repeated administration of different injectable estradiol preparations by intramuscular injection scaled to equivalent doses and plotted over three injection cycles. This simulation was based on the fit curves of the published single-dose estradiol concentration–time data reported in this meta-analysis. Polyestradiol phosphate is scaled to a 6.5-fold higher dose that is roughly equivalent to that for the other esters as it gave total estradiol levels that were around 6 or 7 times lower than the other esters at the same dose. An alternative version of this figure without estradiol benzoate is also provided (Graph).
For more simulated estradiol concentration–time curves with repeated injections of these injectable estradiol preparations, please see the accompanying interactive web simulator.
Selected Pharmacokinetic Parameters
The table below shows selected pharmacokinetic parameters for the fit curves of the included injectable estradiol preparations (Table 9). Estradiol undecylate was not included in the table due to the lack of data needed to achieve a decent curve fit for this preparation and the uncertainty of its parameters.
Table 9: Selected pharmacokinetic parameters for estradiol with injectable estradiol preparations following a single 5 mg dose by intramuscular injection:
Estradiol preparation
Tmax (d)
Cmax (pg/mL)
t1/2 (d)
t90% (d)
AUC0–∞ (pg•d/mL)
Estradiol benzoate in oil
0.65
971
1.2
3.9
2410
Estradiol valerate in oil
2.1
295
3.0
9.9
1886
Estradiol cypionate oil
4.3
155
6.7
22.3
2150
Estradiol cypionate suspension
1.2
241
5.1
16.9
2096
Estradiol enanthate in oil
6.5
160
4.6
15.1
2183
Polyestradiol phosphate a
18.0
34
28.4
94.2
2117
a Scaled instead to a single 32.5 mg injection (6.5 times higher dose than with the other esters).
The table below shows selected pharmacokinetic parameters for simulated curves at steady state with repeated administration of the included injectable estradiol preparations (Table 10). As with the previous table, estradiol undecylate was not included.
Table 10: Selected pharmacokinetic parameters for estradiol with injectable estradiol preparations with simulated repeated administration of 5 mg once every 7 days by intramuscular injection:
Estradiol preparation
Tmax (d)
Cmax (pg/mL)
Cmin (pg/mL)
Peak–trough diff. (pg/mL)
Peak–trough ratio
Cavg (pg/mL)
Estradiol benzoate in oil
0.64
990
29
962
35
344
Estradiol valerate in oil
1.9
384
142
242
2.7
269
Estradiol cypionate oil
3.1
339
262
77
1.3
307
Estradiol cypionate suspension
1.0
404
189
214
2.1
299
Estradiol enanthate in oil
4.0
329
288
41
1.1
312
Polyestradiol phosphate a
3.2
304
299
5
1.0
302
a Scaled instead to repeated injections of 32.5 mg every 7 days (6.5 times higher dose than with the other esters).
Terminal half-life (t1/2) is the time for the concentration of estradiol to decrease by 50% after pseudo-equilibrium of distribution has been reached—not the time required for half of an administered dose of the estradiol ester to be eliminated (Toutain & Bousquet-Mélou, 2004). It is calculated using only the terminal portion of a concentration–time curve, without the absorption or distribution phases influencing it (Toutain & Bousquet-Mélou, 2004). Due to flip–flop kinetics with depot injectables and the very short blood half-life of estradiol (~0.5–2 hours), what is being described by the terminal half-life in the case of depot estradiol injectables is not actually elimination of estradiol from blood but rather is the absorption of estradiol from the injection-site depot (Toutain & Bousquet-Mélou, 2004; Yáñez et al., 2011).
Discussion
Data Quality, Limitations, and Variability Between Studies
The accuracies of the curve fits for the different included injectable estradiol preparations are limited by the available data for these preparations. The quantity and quality of data are variable among these preparations. In some cases, such as with estradiol valerate in oil and estradiol cypionate in suspension, the data are overall quite good. In other instances, such as with estradiol cypionate in oil and estradiol enanthate in oil, the available data are more limited. There was undersampling of certain parts of the concentration–time curve with some preparations, for instance estradiol benzoate in oil (the early curve), estradiol enanthate in oil (much of the curve), and polyestradiol phosphate (the late curve). In the case of estradiol undecylate in oil, the available data for this preparation weren’t adequate to achieve a decent curve fit at all. The fit curves and calculated pharmacokinetic parameters of the included injectable estradiol preparations should be interpreted with the imperfect data in mind. For example, the curve shapes and pharmacokinetic parameters for the different preparations should not be taken as precise determinations in most cases but instead as rough estimates that would no doubt change with more and better data. Indeed, the fits and pharmacokinetic parameters were often noticeably sensitive to the influences of individual studies. Modeling decisions, such as the choice of pharmacokinetic model, or whether to fit directly to the combined processed data versus to the fits of individual studies, also yielded significantly different curve fits as well as calculated pharmacokinetic parameters.
Due to scarcity of data for several injectable estradiol preparations, the study selection criteria maximized data inclusion in order to allow for better curve fits at the risk of including potentially less reliable data. As examples, studies were included regardless of the status of the HPG axis of the participants, and Cmax data were included in the fitting if data were very limited. In the case of HPG axis state, studies with cycling women may result in greater error due to more variable levels of endogenous estradiol. Moreover, acute high levels of estradiol can induce a surge in luteinizing hormone levels after several days in gonadally intact women, and this may cause a delayed bump in estradiol levels (Wiki). One of the more overt instances of this can be seen in a study of estradiol benzoate in such women (Shaw, 1978 [Graph]). Many if not most of the included studies with estradiol benzoate involved women with intact HPG axes, whereas studies of this sort were uncommon with the other preparations. In the case of Cmax data, these data when Cmax corresponds to the mean of individual peaks are a different type of data than the peak of the mean curve of all individuals. Cmax levels can differ in both magnitude and timing compared to the mean curve peak (e.g., Oriowo et al., 1980 [Graph]; Rahimy, Ryan, & Hopkins, 1999). This is because for instance not all individuals peak at the same time and this variability in time to peak normally serves to dilute peak levels for the mean curve when compared to individual maximal concentrations. However, Cmax levels are in any case generally in the vicinity of the mean curve peak. While Cmax levels were excluded in the fitting for most injectable estradiol preparations, they were included in the case of estradiol enanthate. This was because the available mean and individual estradiol curve data were very limited for this specific preparation, and inclusion of Cmax data allowed for improved fitting in spite of its limitations. Lastly, some of the included data was once-monthly multi-dose, and research with once-monthly estradiol enanthate-containing combined injectable contraceptives has found that the time to peak levels may shift with repeated long-term use (Schiavon et al., 1988; Garza-Flores, 1994).
There was considerable variability between studies in terms of estradiol levels and concentration–time curve shapes with the same injectable estradiol preparation. The reasons for the large variability across studies are not fully clear. In any case, there are many potential factors that may contribute to this variability. These include preparation- and injection-related factors like formulation (e.g., oil vehicle, other components and excipients, concentration, particle size), injection volume, site of injection (e.g., buttocks, thigh, upper arm), injection technique (e.g., force of injection—and resulting depot droplet dimensions), and syringe dead space. They additionally include various subject- and research-related variables like differing blood-testing methodology, differing sample characteristics (e.g., age, weight, gender, ethnicity, physical activity, HPG axis state), and sampling error (Sinkula, 1978; Chien, 1981; Minto et al., 1997; Larsen & Larsen, 2009; Larsen et al., 2009; Florence, 2010; Larsen, Thing, & Larsen, 2012; Kalicharan, 2017). Older studies, which used potentially less accurate blood tests and tended to have smaller numbers of subjects, seemed to particularly add to the variability between studies. These studies may represent less reliable data than more recent research with larger sample sizes. The exclusion criteria helped to remove outliers for the different injectable estradiol preparations however. This meta-analysis does not take into account the potential factors underlying the variability between studies. To do so would be difficult, as in many cases information on these variables is not provided in individual studies and research quantifying their precise influences and relative importances is limited.
It is in any case known from other studies that different oil vehicles are absorbed at different rates from the injection site (Svendsen & Aaes‐Jørgensen, 1979; Schultz et al., 1998; Larsen et al., 2001) and can result in different concentration–time curve shapes (Ballard, 1978 [Excerpt]; Knudsen, Hansen, & Larsen, 1985). This is thought to be due to differences in oil lipophilicity and depot release rates. Viscosity of oils has also been hypothesized to potentially influence rate of depot escape (Schug, Donath, & Blume, 2012). However, research so far has not supported this hypothesis (Larsen & Larsen, 2009; Larsen, Thing, & Larsen, 2012). Oil vehicles can vary with injectable estradiol preparations even for the same estradiol ester. For instance, pharmaceutical estradiol valerate is formulated in sesame oil, castor oil, or sunflower oil depending on the preparation (Table). It is notable however that these three oils have similar lipophilicities (Table). On the other hand, homebrewed injectable estradiol preparations used by DIY transfeminine people often employ medium-chain triglyceride (MCT) oil as the oil vehicle. This oil (in the proprietary form of Viscoleo) has notably been found to be much more rapidly absorbed than conventional oils like sesame oil and castor oil in animals (Svendsen & Aaes‐Jørgensen, 1979; Schultz et al., 1998; Larsen et al., 2001). In addition, although based on very limited data, MCT oil has been found to give spikier and shorter-lasting depot injectable curves in humans (Knudsen, Hansen, & Larsen, 1985). As such, injectable estradiol preparations using MCT oil as the vehicle may have differing and less favorable concentration–time curve shapes than pharmaceutical injectable estradiol products. Other excipients, like benzyl alcohol, as well as factors like injection site and volume, have additionally been found to influence pharmacokinetic properties with depot injectables (Minto et al., 1997; Kalicharan, Schot, & Vromans, 2016). Excipients besides oil vehicle also vary by formulation (Table).
An implication of the variability between studies is that there is not a single estradiol concentration–time curve for a given injectable estradiol preparation but rather there are many, with these curves determined by variables such as formulation, dose/administration, and subject characteristics, among others. Hence, the curve fits determined in this meta-analysis represent only an estimation of the most typical and hence likely case, but the true curve for a preparation in a given context may be quite different.
Fitting all studies for a given injectable estradiol preparation individually first, and then fitting the fits of these studies, allowed for improved curve fits relative to directly fitting all of the combined processed original data for the preparation. The latter approach has limitations in that it has the effect of inherently weighting individual studies by quantity of time points (resulting in studies with greater time sampling having greater influence on the fit). Additionally, and more problematically, this approach can lead to distortions in curve shape due to different studies sampling different portions of the curve to differing extents in conjunction with systematic differences in curves between these studies. These are problems that fitting the fits of individual studies instead can solve. However, it is not possible to fit all individual studies, as some studies have limited time sampling and curve characterization which precludes fitting them appropriately. Cmax data are an example of this, which on their own cannot be fit properly. As such, it was not possible to fit the fits of the individual studies for all injectable estradiol preparations. Consequently, the fitting approach in this regard was not the same across esters, with some fit instead directly to the combined processed original data (e.g., estradiol enanthate, polyestradiol phosphate).
In spite of the various limitations of this work, aggregated analysis and modeling with injectable estradiol preparations has not previously been done. This informal meta-analysis provides among the most detailed insight into estradiol levels and curve shapes with these preparations available to date.
Durations and Curve Shapes
The curve shapes of non-polymeric injectable estradiol esters in oil relate strongly to lipophilicity. The more lipophilic the ester, the lower the peak levels and the more protracted the estradiol concentration–time curve. Accordingly, estradiol benzoate, one of the least lipophilic estradiol esters, has one of the spikiest curves and shortest durations, whereas more lipophilic estradiol esters, like estradiol cypionate in oil and estradiol enanthate, have comparatively flatter curves with delayed peaks and longer durations.
Duration of Estradiol Valerate
The estradiol concentration–time curve for injectable estradiol valerate in the well-known Oriowo et al. (1980) [Graph] study is notably spikier and shorter-lasting than the overall curve for estradiol valerate in this meta-analysis. On the other hand, the overall curve for injectable estradiol valerate in this meta-analysis was similar to (and considerably influenced by) the curves from several relatively recent and presumably better-quality studies of this injectable estradiol ester (e.g., Göretzlehner et al., 2002; Valle Alvarez, 2011; Schug, Donath, & Blume, 2012). It’s noteworthy that Oriowo et al. (1980) used a peanut oil-based formulation of estradiol valerate that differed from pharmaceutical injectable estradiol valerate preparations, which generally use sesame oil or castor oil as the carrier (as well as other excipients) (Table). This may have influenced the curve shape of estradiol valerate in Oriowo et al. (1980). The study also had a small sample size relative to the more recent studies (n=9 versus n=17, n=32, and n=24×2, respectively). Based on the newer and overall data, estradiol valerate appears to have a curve that is noticeably flatter and more prolonged than that suggested by Oriowo et al. (1980).
Duration of Estradiol Cypionate in Oil versus Estradiol Enanthate
Available estradiol concentration–time data for injectable estradiol cypionate in oil and estradiol enanthate in oil are more limited than with several of the other injectable estradiol preparations, and no direct comparisons of these two preparations exist at present. Based on some of the available literature on these injectable estradiol esters, most notably discussion by Oriowo et al. (1980) and a review of the pharmacokinetics of combined injectable contraceptives (Garza-Flores, 1994 [Graph]), it seemed that the duration of estradiol enanthate in oil was longer than that of estradiol cypionate in oil. However, this was based on limited research from separate and hence indirectly comparative studies of these esters. The estradiol cypionate in oil data from the relevant Garza-Flores (1994) figure was based on Oriowo et al. (1980) [Graph], and there are reasons to be cautious about relying on these data alone. The main concern is that curve shapes with the same injectable estradiol preparation can vary considerably across studies, as the present meta-analysis has shown. The reasons for this have yet to be fully clarified as already discussed, but among other factors may include varying formulations across studies of the same injectable estradiol ester. It is notable in this regard that Oriowo et al. (1980) used a formulation of estradiol cypionate that differs from conventional pharmaceutical estradiol cypionate in oil preparations—specifically, the study used a peanut oil-based formulation (with few other specifics) rather than the cottonseed oil-based preparation employed in marketed pharmaceutical formulations (Table). The study also had a somewhat small sample size (n=10) and may have had significant sampling error. Hence, single studies, perhaps particularly Oriowo et al. (1980), should be interpreted cautiously.
A small but interesting pharmacokinetic study which directly compared injectable testosterone cypionate (n=6) and testosterone enanthate (n=6) both in oil is relevant to the topic in question. This study found that equivalent doses of these testosterone esters using otherwise identical formulations produced virtually identical testosterone concentration–time curves (Schulte-Beerbühl & Nieschlag, 1980 [Graph]). The findings of this study are consistent with the fact that the lipophilicities of testosterone cypionate and testosterone enanthate (as measured by predicted log P) are very similar when directly compared (e.g., 5.1 vs. 5.11 with ALOGPS, 6.29 vs. 6.11 with ChemAxon logP, and 6.4 vs. 6.3 with XLogP3, respectively (Table). This of course is of importance as lipophilicity is thought to be the key factor determining the release kinetics of oil-based depot injectables (Sinkula, 1978; Shah, 2007; Larsen & Larsen, 2009; Larsen, Thing, & Larsen, 2012; Shahiwala, Mehta, & Momin, 2018). Analogously similar lipophilicities can be seen when comparing estradiol cypionate and estradiol enanthate, which employ the same ester moieties (e.g., predicted log P values of 6.47 vs. 6.45 with ALOGPS and 7.1 vs. 7.0 with XLogP3, respectively) (Table). Hence, on a theoretical level, injectable estradiol cypionate and estradiol enanthate, like injectable testosterone cypionate and testosterone enanthate, might be expected to produce very similar curves—at least provided all other variables, such as formulation, are held constant.
The present meta-analysis found that the overall estradiol curve for estradiol cypionate in oil was significantly less spikey and more prolonged than that observed in Oriowo et al. (1980). It is noteworthy in this regard that all of the other studies included for estradiol cypionate in oil specifically employed pharmaceutical Depo-Estradiol and that the overall curve for this preparation appears to be more consistent with its licensed injection interval for use in menopausal hormone therapy (1–5 mg once every 3–4 weeks) (Depo-Estradiol Label). Moreover, this meta-analysis found that injectable estradiol cypionate in oil and estradiol enanthate in oil had fairly similar and comparably flat and prolonged estradiol concentration–time curves. However, estradiol cypionate in oil appeared to peak earlier than estradiol enanthate, while estradiol enanthate was eliminated more rapidly than estradiol cypionate in oil in the terminal portion of the curve. In any case, the available concentration–time data for these preparations are limited, and the present work is not able to determine whether these estradiol esters have truly differing pharmacokinetic properties, as the apparent differences between the curves for these preparations may simply be due to statistical error. Taken together, estradiol cypionate in oil may have a less spikey and longer-lasting curve than that implied by Oriowo et al. (1980), and estradiol cypionate in oil and estradiol enanthate may have more similar curves than has been previously assumed.
Curve Shape of Estradiol Cypionate Suspension
While estradiol cypionate as an aqueous suspension is a relatively long-lasting injectable estradiol preparation similarly to estradiol cypionate in oil and estradiol enanthate in oil, it seems to differ in the shape of its estradiol concentration–time curve from these preparations. Estradiol cypionate as a suspension has a curve that appears to peak significantly earlier than estradiol cypionate in oil and other longer-acting oil-based injectable estradiol preparations. This might relate to the differing mechanisms of depot action and unique properties of injectable aqueous suspensions (Aly, 2019). In line with this notion, injectable medroxyprogesterone acetate suspension (Depo-Provera) also appears to peak rapidly despite having a very long duration (longer durations tending to be associated with delayed peaks in the case of oil-based depot injectables) (Graphs). Although aqueous suspensions generally last longer than oil solutions as injectables (Enever et al., 1983; Aly, 2019), this is not always the case, and estradiol cypionate suspension interestingly seems to be shorter-acting than estradiol cypionate in oil.
Estradiol Exposure and Potency
The average estradiol levels with the non-polymeric injectable estradiol esters when scaled to a dose and dosing interval of 5 mg every 7 days were around 300 pg/mL (~1,100 pmol/L). For comparison, in premenopausal cisgender women, estradiol production is on average about 200 μg/day (or 6 mg per month/cycle) and mean estradiol levels are around 100 pg/mL (~370 pmol/L) (Aly, 2019). After adjusting for the molecular weight of the ester, the estradiol levels for a given dose of non-polymeric injectable estradiol esters are in fairly close agreement with the estradiol levels for an equal quantity of estradiol produced endogenously by the ovaries in premenopausal cisgender women (very roughly around 1.2 mg estradiol per 7 days for injectable estradiol esters and 1.4 mg estradiol per 7 days for ovarian production to achieve average integrated estradiol levels of around 100 pg/mL). The preceding is in accordance with the fact that injectable estradiol valerate has been reported to have approximately 100% bioavailability (with this being less characterized but likely also the case for the other non-polymeric injectable estradiol esters) (Düsterberg & Nishino, 1982; Seibert & Günzel, 1994).
Although non-polymeric injectable estradiol esters have differing estradiol concentration–time curve shapes, they all appear to achieve fairly similar area-under-the-curve levels of estradiol when compared to one another. This is in accordance with the fact that differences in molecular weight and hence estradiol content with the different estradiol esters are fairly minor (all of the assessed non-polymeric esters range from 62 to 76% of that of estradiol in terms of estradiol content, and all but estradiol undecylate are in the range of 69 to 76%) (Table). The appearance of differences in area-under-the-curve levels of estradiol in the present meta-analysis is probably just due to statistical error, and true differences cannot be established by this meta-analysis. An implication of the similar area-under-the-curve estradiol levels with the different non-polymeric injectable estradiol esters is that these preparations can all be expected to deliver a roughly comparable amount of estradiol for the same dose.
On the other hand, the polymeric ester polyestradiol phosphate appears to produce around 6- to 7-fold lower area-under-the-curve and average estradiol levels than non-polymeric estradiol esters. This suggests that the estradiol in polyestradiol phosphate is not 100% bioavailable, and is supported by the fact that this ester is used clinically at substantially higher dosages than other injectable estradiol esters (40–320 mg/month), even for the same indications such as menopausal hormone therapy and treatment of prostate cancer (Wiki; Estradurin Labels). This does not seem to have been previously described in the literature, and the reasons for it are unknown. It seems possible that polyestradiol phosphate may be partially excreted before it can be cleaved into estradiol and thereby rendered partly inactive, in turn necessitating the use of higher doses to achieve the same estradiol levels and therapeutic effect.
Although two given injectable estradiol preparations may produce equivalent total estradiol levels, this does not necessarily mean that they will always have the same estrogenic potency (i.e., strength of effect at a given dose). It is plausible that spikier estradiol concentration–time curves, like with estradiol benzoate, may have overall lower estrogenic potency than more steady curves, like with estradiol enanthate. This is because estrogen receptors for a given tissue should become saturated at a certain point due to the finite quantity of available receptors in the tissue. As a result, high peak estradiol levels with spikier curves may effectively be “wasted” to varying extents in different tissues. On the other hand, more spikey estradiol curves, due to higher peak estradiol levels, might have greater influence on tissues that require high estradiol levels for effect such as the liver (and by extension on coagulation and associated health risks) (Aly, 2020). However, these possibilities are speculative and theoretical. Although some literature exists that is relevant to this issue (e.g., Parkes, 1937; Bradbury, Long, & Durham, 1953), there is very little research in this area. Consequently, it is not currently possible to take into account time-related variations in estradiol levels or differing estradiol curve shapes when assessing the comparative estrogenic potency between injectable estradiol preparations (or between other estradiol forms/routes). It is also noteworthy that these variations depend on injection interval and may be reduced with shorter injection intervals that maintain steadier estradiol levels, which must also be considered.
Variability Between Individuals
There is substantial variation in total estradiol levels and curve shapes between people with the same injectable estradiol preparation. Indicators of interindividual variability such as standard deviation or 95% range have not been included in this meta-analysis at this time due to the large amount of additional time and work this would require (e.g., additional extraction of error bars from all studies and analysis). In any case, individual studies that were included show this marked interindividual variation (e.g., Oriowo et al., 1980; Derra, 1981 [Graph]; Aedo et al., 1985 [Graphs]; Sang et al., 1987 [Graphs]; Rahimy & Ryan, 1999 [Graph]; Valle Alvarez, 2011 [Graph]; Schug, Donath, & Blume, 2012 [Graphs]). Highly variable estradiol levels are already well-established with oral and transdermal estradiol (Kuhl, 2005; Wiki). Less variability might be expected with non-polymeric injectable estradiol esters since these preparations appear to have approximately complete bioavailability. However, it seems that even with injectable forms of estradiol, the variability between people is still quite substantial. An implication of this is that the appropriate dose and dosing interval of an injectable estradiol formulation for a given person will vary considerably. This emphasizes the importance of blood work to ensure that injectable estradiol preparations are neither overdosed—which can increase health risks such as blood clots (Aly, 2020)—nor underdosed—which may result in suboptimal testosterone suppression and therapeutic efficacy.
Insights for Clinical Guidelines and Dosing Recommendations
Clinical guidelines for transgender health (see also Aly (2020)) provide recommendations on doses and dosing intervals of injectable estradiol valerate in oil and estradiol cypionate in oil (Table 11). Dosing recommendations are not given for other injectable estradiol preparations, which are much less commonly used in transgender medicine. The recommended doses for estradiol valerate and estradiol cypionate vary widely depending on the guidelines, whereas the recommended intervals are consistently once every 1 to 2 weeks. The doses for estradiol valerate range from 2 to 20 mg/week or 5 to 80 mg/2 weeks and the doses for estradiol cypionate range from <1 to 10 mg/week or <2 to 80 mg/2 weeks. For reference, the Endocrine Society guidelines and the University of California, San Francisco (UCSF) guidelines are the most major clinical guidelines for transgender hormone therapy at present (Aly, 2020). The Endocrine Society guidelines recommend 5 to 30 mg/2 weeks or 2 to 10 mg/week for either estradiol valerate or estradiol cypionate (Hembree et al., 2017). Conversely, the UCSF guidelines recommend <20 to 40 mg/2 weeks for estradiol valerate and <2 to 5 mg/2 weeks for estradiol cypionate (with the option to divide dose into weekly injections if cyclical side effects occur) (Deutsch, 2016a).
Table 11: Recommended doses and injection intervals of injectable estradiol preparations (specifically estradiol valerate and estradiol cypionate) in transgender medicine clinical guidelinesa:
a Several other guidelines recommend doses and intervals that appear to be taken directly from the Endocrine Society or UCSF guidelines and thus are not listed here but can be found elsewhere (Aly, 2020).
A number of concerns arise when the doses and intervals of injectable estradiol valerate and estradiol cypionate recommended by the major transgender clinical guidelines are considered in the context of the present informal meta-analysis and when they are compared between guidelines. Based on the present work, dosages of injectable preparations recommended by the major transgender clinical guidelines appear to result in estradiol exposure that is markedly higher than that with the recommended dosages for other routes and forms of estradiol (e.g., oral or transdermal). Whereas a dosage of 5 mg/week of any non-polymeric injectable estradiol ester appears to give average estradiol levels of around 300 pg/mL (~1,100 pmol/L), which are already supraphysiological, doses of injectable estradiol valerate or estradiol cypionate recommended by guidelines are as high as 15 to 20 mg per week. The average estradiol concentrations that would be expected to result from such doses per this meta-analysis (e.g., ~600–1,200 pg/mL or 2,200–4,400 pmol/L at 10–20 mg/week) (Figure 10) would vastly exceed the ranges for estradiol levels in transfeminine people advised by the same guidelines (generally about 50–200 pg/mL or ~180–730 pmol/L) (Table). This is not merely theoretical; for example, a study that used 40 mg/week estradiol valerate by intramuscular injection in cisgender women with estrogen deficiency to produce “pseudopregnancy” reported measured estradiol levels of about 2,500 pg/mL (~9,200 pmol/L) at 3 months and 3,100 pg/mL (~11,400 pmol/L) at 6 months of treatment (Ulrich, Pfeifer, & Lauritzen, 1994). Moreover, highly supraphysiological estradiol levels with guideline-based injectable estradiol doses are not unexpected when normal production of estradiol in premenopausal cisgender women is considered (~1.4 mg per week or 6 mg per month/cycle giving mean estradiol levels of ~100 pg/mL or 370 pmol/L) (Aly, 2019). Clinical safety data on high doses of injectable estradiol esters like estradiol valerate and estradiol cypionate are lacking at present, but excessive estrogenic exposure is known to increase the risk of health complications such as blood clots (Aly, 2020). The very high doses of these preparations that are recommended by guidelines should raise considerable reservations about their safety.
Figure 10: Simulated estradiol levels with injectable estradiol valerate at the doses and interval (5–40 mg/2 weeks) preferentially recommended by current major transgender care guidelines. Steady-state estradiol levels are reached by about the second or third injection with this injection interval and levels do not further accumulate. An alternative version of this figure with half-doses at a once-weekly interval (i.e., 2.5–20 mg/week) is also provided (Graph).
The present author elsewhere has listed doses of injectable estradiol preparations that are roughly comparable in terms of total estradiol exposure to doses for other estradiol forms and routes used in transfeminine people (Aly, 2020). These doses range from about 1 to 6 mg per week for “low dose” to “very high dose” therapy with non-polymeric injectable estradiol esters (Graph). This dose range for injectable estradiol is likely to be more appropriate for use in transfeminine people than current recommendations by many guidelines. Although high estradiol levels can be useful in transfeminine hormone therapy when antiandrogens are not used due to their greater efficacy than physiological levels in terms of testosterone suppression, only modestly supraphysiological estradiol levels (e.g., ~200–300 pg/mL or 730–1,100 pmol/L) appear to be required for strong testosterone suppression (Aly, 2019; Langley et al., 2021; Aly, 2020). In relation to this, doses of injectable estradiol need not be excessive.
Some guidelines, such as the Endocrine Society guidelines, recommend the same doses and intervals for both estradiol valerate and estradiol cypionate, whereas other guidelines, such as the UCSF guidelines, recommend different doses for these two injectable estradiol esters. Concerningly, the doses for estradiol valerate and estradiol cypionate recommended by the UCSF guidelines differ by roughly an order of magnitude (<20 to 40 mg/2 weeks for estradiol valerate and <2 to 5 mg/2 weeks for estradiol cypionate). These estradiol esters appear to produce similar average estradiol levels (e.g., around 300 pg/mL or 1,100 pmol/L at a dosage of 5 mg/week) and have concentration–time curve shapes that are not extremely different, with estradiol cypionate being only somewhat flatter and more prolonged than estradiol valerate. As such, it would appear that similar doses should be appropriate for these esters. This is supported by the fact that the same doses of estradiol valerate and estradiol cypionate are used in combined injectable contraceptives in cisgender women (both 5 mg once per month) and that these doses were carefully determined during an intensive clinical development programme for these preparations (Garza-Flores, 1994; Newton, d’Arcangues, & Hall, 1994; Sang, 1994; Toppozada, 1994). This programme notably included dose-ranging and direct-comparison studies. Based on the present analysis, the current recommendations by the UCSF guidelines may result in marked overdosage in the case of estradiol valerate and potential underdosage in the case of estradiol cypionate.
Transgender health guidelines recommend an injection interval for estradiol valerate and estradiol cypionate in oil of once every 1 to 2 weeks. Although an injection interval of 2 weeks seems technically feasible in the case of both of these preparations, such an interval would appear to result in substantial fluctuations in estradiol levels, with high peak levels and low troughs. This is particularly true in the case of the shorter-acting estradiol valerate (Figures 10, 11). Considering the wide fluctuations and unknown effects of this variability, as well as the fact that testosterone suppression when applicable may depend on sustained higher estradiol levels, it may be advisable that a once-weekly interval be preferentially recommended for these preparations. This would achieve steadier estradiol levels and would reduce potential problems due to high or low estradiol levels (Figure 11). Alternatively, a shorter interval of once every 5 days may be used with estradiol valerate to further reduce the variability in estradiol levels that occurs with this preparation (Figure 11). On the other hand, an injection interval of once every 10 days to 2 weeks may be practical and allowable in the case of the longer-acting estradiol cypionate in oil (as well as estradiol enanthate) (Figure 11)—provided that the injection cycles are well-tolerated and testosterone suppression remains adequate. When selecting different injection intervals, doses should be scaled by the interval to maintain equivalent total estradiol exposure (e.g., 3.5 mg/5 days, 5 mg/7 days, 7 mg/10 days, or 10 mg/14 days for high-dose non-polymeric injectable estradiol esters).
Figure 11: Simulated estradiol levels with a high dosage of injectable estradiol valerate or estradiol cypionate in oil at different injection intervals (doses scaled by interval to be equivalent in total estradiol exposure).
With the preceding concerns about the doses and intervals of injectable estradiol preparations recommended by transgender care guidelines considered, the question of how these recommendations were determined arises. Unfortunately, current guidelines do not generally describe how they arrived at their recommendations nor do they usually cite sources to support them. It is notable that the UCSF guidelines recommend doses and intervals for injectable estradiol preparations that are nearly identical to those advised by Christian Hamburger and Harry Benjamin in the late 1960s in the first medical textbook on transgender people (Hamburger & Benjamin, 1969). These authors recommended a dose of 10–40 mg/2 weeks for estradiol valerate and of 2–5 mg/2 weeks for estradiol cypionate (although Benjamin additionally stated that after 4–8 months, the same doses could be used at a longer injection interval of once every 4 weeks). These recommendations were notably made before estradiol blood tests became practicably available and were prior to the advent of modern pharmacokinetic studies. Hence, the recommendations for at least these guidelines appear to be based mainly on past expert opinion and long-standing historical precedent rather than on pharmacokinetic or clinical data. The same is likely to also be true for most other guidelines. High doses with certain injectable estradiol preparations (namely estradiol valerate) were probably originally employed for the purpose of achieving longer durations and more convenient injection intervals. This was notably prior to the risks of excessive estrogenic exposure like blood clots becoming known, and these doses may simply have never been revised.
Among the surveyed guidelines for transgender hormone therapy, only the UCSF guidelines (Deutsch, 2016b) and the Sherbourne Health/Rainbow Health Ontario guidelines (Bourns, 2019) referenced pharmacokinetic literature in their discussion of injectable estradiol. The specific publications cited by these guidelines were Düsterberg & Nishino (1982), Sierra-Ramírez et al. (2011), and Thurman et al. (2013). Although it is favorable to see guidelines considering published pharmacokinetic data for informing use of these preparations, there are a few concerns about the studies that were cited. Düsterberg & Nishino (1982) in its study of injectable estradiol valerate had a very small sample size (n=2), and this study was excluded as an outlier in the present meta-analysis due to unusually high estradiol levels. The findings of Düsterberg & Nishino (1982) also do not seem to have actually been used to guide dosing recommendations in the case of the UCSF guidelines, since if this were the case, the recommended doses should have been much lower. On the other hand, Bourns (2019) cited the same study and recommended injectable estradiol valerate at doses of 3–4 mg/week or 6–8 mg/2 weeks. These doses are well below those recommended by other transgender care guidelines and appear to be more appropriate for use in transfeminine people in light of the present meta-analysis. Sierra-Ramírez et al. (2011) and Thurman et al. (2013), although better-quality studies than Düsterberg & Nishino (1982), described injectable estradiol cypionate suspension rather than estradiol cypionate in oil. The oil-based version of estradiol cypionate is the form normally used in transfeminine hormone therapy, and there are important differences between these estradiol cypionate preparations such that pharmacokinetic studies for the suspension can’t necessarily be generalized to the oil solution. These preparations do in any case produce similar total estradiol levels however and hence doses should be comparable for them.
This meta-analysis is only informal and unpublished research. Nonetheless, based on the results of this work and the preceding discussion, current dosing recommendations for injectable estradiol preparations by most transgender clinical guidelines appear to be highly excessive and likely unsafe, with injection intervals that may additionally be too widely spaced. Transgender care guidelines should consider reassessing these recommendations, and the transgender medical community should make an effort to better characterize the pharmacokinetics and optimal dosing schemes of injectable estradiol preparations in transfeminine people in the future. Since clinical data on these preparations are scarce and will probably remain so in the near-term, use of published pharmacokinetic data may be further considered for guiding dosing recommendations for injectable estradiol. As identified and catalogued by this meta-analysis, there is a wealth of existing data that could be used to better inform transgender care guidelines in terms of the use of injectable estradiol preparations in transfeminine people.
Interactive Web Simulator
This informal meta-analysis of estradiol concentration–time data with injectable estradiol preparations was conducted for the purpose of deriving accurate and representative estradiol curves for incorporation into a web-based injectable estradiol simulator intended for use by transfeminine people and their clinicians. This web app is able to simulate both single-injection curves and repeated-injection curves with these preparations. An informational page for this simulator can be found at the following location:
There are various possibilities for further work on this project in the future. For example, assessment of interindividual variability for estradiol levels with injectable estradiol preparations could be included in the meta-analysis. As another example, it would be fairly straightforward and valuable to expand the meta-analysis as well as simulator to other hormonal preparations such as injectable testosterone preparations and other estradiol routes and forms like oral estradiol, sublingual estradiol, and estradiol pellets. Pharmacokinetic literature for some of these preparations has already been collected by this author. However, these future possibilities would require much additional time and effort to complete.
Special Thanks
A special thank you to Violet and Lila for their indispensable input and guidance on modeling topics during the work on this project. An additional thanks to Violet for deriving a special three-compartment pharmacokinetic model that was used in this work. Please also check out Violet’s own projects Tilia—an effort to empower trans people with tools to manage their hormonal transitions—and TransKit—a work-in-progress pharmacokinetic simulation library specifically tailored for transgender hormone therapy. Lastly, thank you to all the peer reviewers who carefully reviewed this article prior to it being posted.
Updates
Update 1: WPATH SOC8 Guidelines
In September 2022, the World Professional Association for Transgender Health (WPATH) Standards of Care for the Health of Transgender and Gender Diverse People Version 8 (SOC8) were published and made recommendations on transgender hormone therapy for the first time (Coleman et al., 2022). These guidelines are among the most highly regarded and consulted transgender care guidelines. In terms of the recommended doses of hormonal medications for transgender people, the WPATH SOC8 appear to have largely copied the Endocrine Society’s 2017 guidelines on transgender hormone therapy (Hembree et al., 2017). More specifically, in the case of injectable estradiol preparations for transfeminine people, doses of 5–30 mg/2 weeks or 2–10 mg/week estradiol valerate or estradiol cypionate were recommended. There was no discussion of injectable estradiol in the guidelines besides the preceding doses and intervals being included in a table, and no literature citations were included to support these doses. As described in the present work, these recommendations include doses and intervals that appear to be highly excessive, too widely spaced, and are likely unsafe. As such, major transgender care guidelines unfortunately continue to make uncited recommendations for injectable estradiol that are out of step with insights available from abundant published pharmacokinetic data. These recommendations are likely inadvisable, with the possibility of substantial health risks.
Update 2: Literature Mentions
The following publications in the literature have cited or mentioned Transfeminine Science’s injectable estradiol simulator and/or meta-analysis since the project was published in mid-2021:
Hughes et al. (2022)
Hughes, J. H., Woo, K. H., Keizer, R. J., & Goswami, S. (2022). Clinical Decision Support for Precision Dosing: Opportunities for Enhanced Equity and Inclusion in Health Care. Clinical Pharmacology & Therapeutics, 113(3), 565–574. [DOI:10.1002/cpt.2799]:
Lastly, we recommend that developers of [clinical decision support software (CDSS)] for dosing take an iterative and participatory approach to designing systems. By involving stakeholders in the design process, they will develop solutions that best suit users’ needs and are more likely to be adopted and used correctly. This participatory approach should involve interviews and usability testing with clinicians. Formal usability testing and analysis with real end users can improve the quality and usefulness of a system.88 Though patients themselves are not typically the end users of CDSS, their expertise (especially that of marginalized groups and organized patient advocacy organizations) can also inform CDSS developers. As an example, transgender people have compiled their own resources to understanding dosing regimens in the absence of clear clinical guidelines.89 Developers of CDSS could provide a great deal of value to these patient populations, and improve their software’s utility, by working with them to understand their needs from a dosing tool.
89. Aly, W. An interactive web simulator for estradiol levels with injectable estradiol esters. Transfeminine Science <https://transfemscience.org/articles/injectable-e2-simulator-release/> (2021) Accessed November 1, 2022.
Jaafar et al. (2022)
Jaafar, S., Torres-Leguizamon, M., Duplessy, C., & Stambolis-Ruhstorfer, M. (2022). Hormonothérapie injectable et réduction des risques: pratiques, difficultés, santé des personnes trans en France. [Hormone replacement therapy injections and harm reduction: practices, difficulties, and transgender people’s health in France.] Sante Publique, 34(HS2), 109–122. [Google Scholar] [PubMed] [DOI:10.3917/spub.hs2.0109] [Translated]:
With regard to feminizing [substitutive hormone therapy (HS)], there are no specialty injectables based on estrogens in the French pharmacopoeia. This makes it impossible to set up estrogen monotherapies which require high dosages that are more difficult to obtain with specialties with other galenic forms [5]. Faced with this lack of care, some trans women and transfeminine people obtain estradiol-based injectable solutions on the Internet or through other sources [6]. […]
5. Aly. An informal meta-analysis of estradiol curves with injectable estradiol preparations [Internet]. Transfem Sci. 2021 July 16. [Visited on 29/12/2022]. Online : https://transfemscience.org/articles/injectable-e2-meta-analysis/.
Linet (2023)
Linet, T. (2023). Prise en charge endocrinologique d’une personne trans. [Endocrinological care of a trans person.] In Faucher, P., Hassoun, D., & Linet, T. (Eds.). Santé sexuelle et reproductive des personnes LGBT [Sexual and Reproductive Health of LGBT People] (pp. 109–124). Issy-les-Moulineaux, France: Elsevier Masson. [Google Books] [URL] [WorldCat] [Excerpt] [Translated]:
Choice of estrogen.
Estradiol is generally the most prescribed estrogen. It is given orally or sublingually in transfeminine people with no significant cardiovascular risk factors. For others, the percutaneous form (patches, gel) is recommended.
The starting dose is 2 mg of estradiol orally with a step increase of 2 mg every 2 to 3 months until the optimal dose is reached [1]. For the patches, the initial dosage and the increments are 50 or 100 μg, and for the gel 2.5 g. This means that the optimal dose is generally 6 to 8 mg per day for the oral route, 3 to 4 mg for the sublingual route, and 300 to 400 μg for the patches (see table 11.1).
It may happen in consultation that the person does not wish to use the prescribed estrogens and wishes to continue the self-prescription of injectable estrogens. It is then possible to evaluate with them the most suitable dosage using the Transfem Science Injection Simulator (https://transfemscience.org/misc/injectable-e2-simulator/). Risk prevention related to injections (needles) can be done. Associations can help the person find 25 G needles of 40 mm useful this type of treatment.
Rothman et al. (2024)
Rothman, M. S., Ariel, D., Kelley, C., Hamnvik, O. R., Abramowitz, J., Irwig, M. S., Soe, K., Davidge-Pitts, C., Misakian, A. L., Safer, J. D., & Iwamoto, S. J. (2024). The Use of Injectable Estradiol in Transgender and Gender Diverse Adults: A Scoping Review of Dose and Serum Estradiol Levels. Endocrine Practice, ahead of print. [DOI:10.1016/j.eprac.2024.05.008]:
In recent years, we have noted trends in our clinical practices with TGD adults requesting injectable estradiol, particularly in the United States. The reasons given can vary; it may be due to ease of weekly or every two weeks administration, fatigue of taking daily oral medications and skin reactions to or cost of transdermal preparations. There have been discussions as to the roles of estrone/estradiol ratios in feminization and whether injectable estradiol might lead to more favorable results, however research has not supported a role for estrone in optimizing feminizing outcomes [13]. There is also a belief that higher levels can be attained with 82 injections and may lead to faster and more complete feminization; however, there is a lack of data in the literature to support these conclusions. Such conversations occurring on reddit.com and even some hormone provider websites, are perhaps related to the historical use of high dose injectable estradiol noted above [14]. However, there is a paucity of data to guide clinicians on what dose, type and at what interval estradiol esters should be injected and when levels should be measured to ensure physiologic range estradiol levels. In fact, recent reports and clinical observations have raised concerns that the dosing suggested in guidelines may result in supraphysiological estradiol levels and that higher doses and levels may put patients at elevated risk of thromboembolic events [15-18]. This scoping review examines the available data on levels achieved with various dosages of estradiol injections in TGD adults. We also report on testosterone suppression, route (i.e., SC vs. IM), and type of estradiol ester as well as timing of blood draw relative to dose, where available.
Acknowledgment
[…] [We] thank Aly from Transfemscience for community representation and correspondence.
In March 2023, the following study on injectable estradiol in transfeminine people was published online:
Herndon, J. S., Maheshwari, A. K., Nippoldt, T. B., Carlson, S. J., Davidge-Pitts, C. J., & Chang, A. Y. (2023). Comparison of Subcutaneous and Intramuscular Estradiol Regimens as part of Gender-Affirming Hormone Therapy. Endocrine Practice, 29(5), 356–361. [DOI:10.1016/j.eprac.2023.02.006] [URL]
The study was a retrospective analysis of individualized injectable estradiol in adult transfeminine people who received hormone therapy at the Mayo Clinic. Doses of injectable estradiol were adjusted by clinical providers based on estradiol levels, testosterone suppression, and feminization goals, and subsequently these clinical data were retrospectively studied by Mayo Clinic researchers. The primary aim of the study was to compare injectable estradiol by intramuscular versus subcutaneous routes. However, other general considerations for injectable estradiol, such as dosing, estradiol levels, testosterone suppression, type of injectable estradiol ester (estradiol valerate vs. estradiol cypionate), and estradiol monotherapy versus concomitant use of antiandrogens, were also assessed. The paper noted that the study was the largest to assess injectable estradiol in transfeminine people to date and was the first to directly compare intramuscular and subcutaneous injectable estradiol routes in transfeminine people.
Injectable estradiol doses were adjusted to achieve estradiol and testosterone levels within therapeutic ranges defined by the Endocrine Society 2017 guidelines (>100 pg/mL [367 pg/mL] for estradiol and <50 ng/dL [<1.7 nmol/L] for testosterone). Estradiol levels were measured exclusively using liquid chromatography–tandem mass spectrometry (LC–MS/MS), while the assay method for measuring testosterone levels was not specified. In terms of when in the injection cycle estradiol levels were measured, the authors stated the following: (1) “Timing of estradiol blood draw in relation to injection was not protocolized” and (2) “In our practice, although estradiol concentrations were generally checked midway through the injection cycle, we were unable to document with certainty the timing of the estradiol lab testing which may have influenced the results and/or the outliers”. Only the most recent blood test for each individual was analyzed, with the results of earlier tests discarded. Doses were analyzed in per-week amounts, regardless of dosing frequency (either once weekly or once every two weeks).
There were a total of 130 transfeminine people on injectable estradiol who were analyzed in the study. Of these individuals, 56 received intramuscular (i.m.) injections and 74 received subcutaneous (s.c.) injections. The median duration of therapy for injectable estradiol was 3.0 years for both routes. The vast majority of people used weekly injections (91.1% for i.m., 98.6% for s.c.), whereas the small remainder (n=6) injected once every 2 weeks. Similarly, the great majority used injectable estradiol valerate (89.3% for i.m., 86.5% for s.c.), while a small subset (n=16) used injectable estradiol cypionate. The authors did not state the injectable vehicles, but they can be confidently assumed to have both been in oil. The treatment-individualized doses per week of injectable estradiol were median 4 mg (interquartile range (IQR) 3–5.15 mg; range 1–8 mg) for the i.m. route and median 3.75 mg (IQR 3–4 mg; range 1–8 mg) for the s.c. route, with the differences in doses between groups being slightly but significantly different (p = 0.005). For the small number of people on two-week injection cycles, the doses for the combined i.m. and s.c. groups were median 8.5 mg (range 6–16 mg) every 2 weeks. Estradiol levels with injectable estradiol were median 189.5 pg/mL (IQR 126.8–252.5 or 122.5–257 pg/mL; range ~33–575 pg/mL] for i.m. and median 196 pg/mL (IQR 125.3–298.5 pg/mL; range ~23–581 pg/mL) for s.c., with the differences between groups not being significantly different (p = 0.70). The percentages of individuals with estradiol levels in target range (>100 pg/mL) were 78.6% for i.m. and 82.4% for s.c. The estradiol doses and levels of individual patients for each route were also provided in the paper (Graph). It can be seen that more individuals clustered into the higher range of doses with i.m. than with s.c. injections.
In the case of estradiol valerate versus estradiol cypionate, dose per week for i.m. with estradiol valerate was median 4 mg (IQR 3–5.45 mg) and with estradiol cypionate was median 4 mg (IQR 2.25–5 mg). In the case of s.c., dose per week with estradiol valerate was median 4 mg (IQR 3–4 mg) and with estradiol cypionate was median 3 mg (IQR 2–3 mg). The doses between estradiol valerate and estradiol cypionate were not significantly different in the case of i.m. (p = 0.51), but were significantly different in the case of s.c. (p = 0.025). Estradiol levels with the two different injectable estradiol esters were not provided.
On multiple regression analysis, injectable estradiol dose was significantly positively associated with estradiol levels (p < 0.001) following adjustment for several variables (injection route, body mass index (BMI), antiandrogen use, gonadectomy status). Each 1 mg per week in dose was associated with estradiol levels that were increased by (estimate ± standard error) 57.42 ± 10.46 pg/mL. No other variable, including notably BMI, was significantly associated with estradiol levels. According to the authors, the dose-dependently higher estradiol levels with injectable estradiol suggested the need to start at lower doses that are gradually increased in conjunction with close monitoring of hormone levels.
Testosterone levels in those with gonads were 11 ng/dL (IQR 0–19.8 ng/dL) for i.m. and 11 ng/dL (0–20 ng/dL) for s.c., with levels not significantly different between groups (p = 0.92). Adequate testosterone suppression (<50 ng/dL) in those with gonads was achieved in 84.6% with i.m. and 86.6% with s.c. In the small subset of individuals on injections every two weeks (n=6), 100% of individuals achieved target estradiol and testosterone levels. A majority of individuals on injectable estradiol in the study concomitantly used an antiandrogen, with this usually being spironolactone or finasteride. In a minority of individuals, injectable estradiol monotherapy, without concomitant use of an antiandrogen, was employed and hormone levels were measured (n=17). In this subgroup, estradiol levels were median 220 pg/mL (IQR 180–264 pg/mL) at a dose per week of median 4 mg (IQR 3–6 mg), with estradiol levels noticeably higher than in the overall group. In terms of hormone levels for those on injectable estradiol monotherapy, 100% achieved therapeutic estradiol levels (>100 pg/mL) and 88.2% achieved target testosterone levels (<50 ng/dL). The authors noted that most individuals on injectable estradiol monotherapy were able to adequately suppress testosterone, but that higher doses and levels of estradiol may be needed for testosterone suppression in this context.
Herndon et al. (2023) noted that existing recommendations for injectable estradiol in transfeminine people suggest doses of 2 to 10 mg per week or 5 to 30 mg every 2 weeks, referencing the Endocrine Society 2017 guidelines (Hembree et al., 2017) and UCSF 2016 guidelines (Deutsch, 2016a). They also noted that the UCSF 2016 guidelines recommended lower doses of estradiol cypionate than estradiol valerate, which they attributed to pharmacokinetic differences between the esters (citing Oriowo et al. (1980) for this claim). However, the authors noted that the differences between estradiol valerate and estradiol cypionate doses they observed were small, and questioned the clinical relevance of the differences. The authors also tactfully critiqued dosing recommendations by existing guidelines, and suggested their own data to guide dosing instead, with the following relevant excerpts:
Prior studies used for development of guidelines for parenteral doses are suboptimal given their small sample sizes or pre-specificized [gender-affirming hormone therapy (GAHT)] protocols with no adjustment of estradiol doses or no information on hormone concentrations achieved. [Discussion of Deutsch, Bhakri, & Kubicek (2015) and Mueller et al. (2011) …]
Overall, the studies used to support the current dosing recommendation guidelines for parenteral estradiol dosing are limited, incomplete with regards to hormone concentrations achieved, and do not provide SC as an available option. The doses of estradiol used in this study (with either SC or IM approach), were successful in achieving serum estradiol concentrations at the cisgender female range. Most importantly, as compared to current available guidelines and consensus statements [1, 2], these doses of estradiol valerate are less than half of what is recommended for both initial and maintenance dosing and achieved suppression of testosterone.
Lower doses of parenteral injections than previously described in clinical practice guidelines achieved therapeutic estradiol concentrations. Our data can serve as a dosing guide for initial and maintenance use of parenteral estradiol, which is different than what has been previously described.
Herndon et al. (2023) concluded that injectable estradiol by both i.m. and s.c. routes is effective in achieving therapeutic estradiol levels in transfeminine people. They noted that there were not meaningful differences between i.m. and s.c. in terms of dose, although i.m. may require slightly higher doses than s.c. to achieve therapeutic estradiol levels. The authors stated that doses of injectable estradiol to achieve therapeutic estradiol levels in transfeminine people were lower than previously recommended by guidelines and other publications. They concluded that clinical use of injectable estradiol in transfeminine people should include discussion of both i.m. and s.c. routes and invidiualization by patient. Finally, they called for more clinical studies on injectable estradiol in transfeminine people to evaluate clinical outcomes, feminization, and additional risks and benefits of this route compared to other routes.
The findings of Herndon et al. (2023) are pleasingly consistent with the results of the present meta-analysis. Based on the findings of this meta-analysis, assuming a linear relationship between dose and estradiol levels, estradiol levels with non-polymeric injectable estradiol esters, like estradiol valerate and estradiol cypionate in oil via intramuscular injection, increase by around 60 pg/mL on average for each 1 mg per week in dose (with Herndon et al. (2023) finding a value of 57 pg/mL per 1 mg using a multiple linear regression model). In relation to this, mean integrated estradiol levels of around 250 pg/mL on average would be expected at a dosage of 4 mg once per week. Accordingly, Herndon et al. (2023) found median estradiol levels of 190 to 196 pg/mL at per-week median doses of 3.75 to 4 mg. Similarly, the present work recommended injectable estradiol doses with non-polymeric esters of 1 to 6 mg per week (to achieve mean integrated estradiol levels of roughly 50–300 pg/mL), which is comparable to the range of about 2 to 6 mg per week used in most transfeminine people in Herndon et al. (2023) (to achieve estradiol levels of at least 100 pg/mL, along with adequate testosterone suppression). Additionally, it was noted in this meta-analysis—based on clinical research in cisgender men with prostate cancer—that only modestly supraphysiological estradiol levels, of no more than approximately 200 to 300 pg/mL, are likely to be needed for strong testosterone suppression in transfeminine people. This has likewise been confirmed with solid clinical data in transfeminine people by Herndon et al. (2023), with 88% of those on injectable estradiol monotherapy having testosterone levels of <50 ng/dL at a median injectable estradiol dose of 4 mg/week and with median estradiol levels of 220 pg/mL. It is the opinion of the present author that Herndon et al. (2023) is a very important and formative study, with clinical implications that go far beyond merely supporting the s.c. use of injectable estradiol. The study represents the first major step in the published literature to correcting the dosing and intervals of injectable estradiol in transgender care guidelines and in transgender health generally. I commend the researchers for their work.
Update 4: Rothman et al. (2024a) and Rothman et al. (2024b)
In February 2024, the following short review on injectable estradiol dosing in transfeminine people by Micol Rothman and colleagues was published online:
Rothman, M. S., Hamnvik, O. P. R., Davidge-Pitts, C., Safer, J. D., Ariel, D., Tangpricha, V., Abramowitz, J., Soe, K., Sarvaideo, J., Kelley, C., Irwig, M. S., & Iwamoto, S. J. (2024). Revisiting Injectable Estrogen Dosing Recommendations for Gender-Affirming Hormone Therapy. Transgender Health, ahead of print. [DOI:10.1089/trgh.2023.0209]
Here is the abstract of the paper:
Injectable estrogens are options for gender-affirming hormone therapy per guidelines, which suggest intramuscular dosages of 5–30 mg every 2 weeks or 2–10 mg weekly with estradiol cypionate or valerate interchangeably. Data among transgender and gender-diverse patients are limited due to local unavailability and concerns around laboratory assay variability and estradiol (E2) level fluctuation. We note a concerning trend where patients are prescribed high-dose injections based on the guidelines leading to serum E2 levels well above the range recommended in the same guidelines. Our review indicates that 5 mg weekly or lower should be prescribed when initiating injectable estrogens to avoid supraphysiologic E2 levels.
Then, in May 2024, the following longer and more comprehensive review on injectable estradiol dosing in transfeminine people by Rothman and most of the same other academics was published online:
Rothman, M. S., Ariel, D., Kelley, C., Hamnvik, O. R., Abramowitz, J., Irwig, M. S., Soe, K., Davidge-Pitts, C., Misakian, A. L., Safer, J. D., & Iwamoto, S. J. (2024). The Use of Injectable Estradiol in Transgender and Gender Diverse Adults: A Scoping Review of Dose and Serum Estradiol Levels. Endocrine Practice, ahead of print. [DOI:10.1016/j.eprac.2024.05.008]
Here is the abstract of this paper:
Objective: Feminizing gender-affirming hormone therapy is the mainstay of treatment for many transgender and gender diverse people. Injectable estradiol preparations are recommended by the World Professional Association for Transgender Health Standards of Care 8 and the Endocrine Society guidelines. Many patients prefer this route of administration, but few studies have rigorously assessed optimal dosing or route.
Methods: We performed a scoping review of the available data on estradiol levels achieved with various dosages of estradiol injections in transgender and gender diverse adults on feminizing gender-affirming hormone therapy. We also report on testosterone suppression, route (ie, subcutaneous vs intramuscular), and type of injectable estradiol ester as well as timing of blood draw relative to the most recent dose, where available.
Results: The data we reviewed suggest that the current guidelines, which recommend starting doses 2 to 10 mg weekly or 5 to 30 mg every 2 weeks of estradiol cypionate or valerate, are too high and likely lead to patients having supraphysiologic levels across much of their injection cycle.
Conclusions: The optimal starting dose for injectable estradiol remains unclear and whether it should differ for cypionate and valerate. Based on the data available, we suggest that clinicians start injectable estradiol cypionate or valerate via subcutaneous or intramuscular injections at a dose ≤5 mg weekly and then titrate accordingly to keep levels within guideline-recommended range. Future studies should assess timing of injections and subsequent levels more precisely across the injection cycle and between esters.
This paper notably also cited the present Transfeminine Science article as raising concerns about guideline-based dosing for injectable estradiol and potential health complications from these doses.
Aside from Micol Rothman herself, these reviews were also authored by other well-known experts in transgender health. For instance, two of the coauthors, Joshua Safer and Michael Irwig, were authors for the WPATH SOC8 hormone therapy chapter (WPATH SOC8 Full Contributor List). Additionally, Safer was one of the authors for the Endocrine Society’s transgender hormone therapy guidelines (Hembree et al., 2017). As such, it would appear that transgender medicine has finally started to seriously correct injectable estradiol dosing. This is a very important development. Now, the appropriate dosing and intervals of injectable estradiol will need to be more precisely established and the corrections will need to make their way into updated transgender hormone therapy guidelines and general clinical practice.
Update 5: Kariyawasam et al. (2024)
In March 2024, the following study of estradiol levels with different routes of estradiol in transfeminine people, including injectable estradiol, was published:
Kariyawasam, N. M., Ahmad, T., Sarma, S., & Fung, R. (2024). Comparison of Estrone/Estradiol Ratio and Levels in Transfeminine Individuals on Different Routes of Estradiol. Transgender Health, ahead of print. [DOI:10.1089/trgh.2023.0138]
The study stratified injectable estradiol doses into different dosing levels, accounted for timing of blood draws, and compared injectable estradiol to other estradiol routes. The other routes included oral estradiol, sublingual estradiol, and transdermal estradiol. The form of injectable estradiol used was estradiol valerate in dose groups including ≤4 mg/week (“low-dose”), >4 mg/week to ≤8 mg/week (“medium-dose”), and >8 mg/week (“high-dose”). In the study, this injectable estradiol regimen resulted in supraphysiological estradiol levels in the medium- to high-dose groups (>4 mg/week) and dramatically higher estradiol levels than with the other estradiol routes (Data). Median estradiol levels were reported in a subsequent paper as follows: “Figure 2 from the paper shows estradiol levels across the 3 groups. Although exact numbers are not given in this figure, we learned through correspondence with the authors that the low dose injection group [n=8] had a median level of 202.7 ± SD 232.6 pg/mL, the medium group [n=22] 465.2 ± SD 466.3 pg/mL, and the high group [n=3] 574.4 ± SD147.3 pg/mL (converted from SI units)” (Rothman et al., 2024b). Although the sample sizes for the different dose groups were small, this study, along with Herndon et al. (2023), provides some of the best clinical data on estradiol levels with injectable estradiol in transfeminine people that have so far been published.
Update 6: Patel et al. (2024)
In June 2024, the following open-access review discussing injectable estradiol in transfeminine people and calling for updated transgender health guidelines was published:
Patel, R., Korenman, S., Weimer, A., & Grock, S. (2024). A Call for Updates to Hormone Therapy Guidelines for Gender-Diverse Adults Assigned Male at Birth. Cureus, 16(6), e62262. [DOI:10.7759/cureus.62262] [PDF]
The following quote is the relevant excerpt on injectable estradiol from the review:
The current guideline-based dosing recommendations for estradiol vary considerably, which is problematic for clinicians and patients who rely on guidelines to initiate treatment. Most notably, the conversion rates between parenteral estradiol valerate and estradiol cypionate vary drastically between the UCSF Guidelines for the Primary and Gender-Affirming Care of Transgender and Gender Nonbinary People (UCSF Guidelines) and The Endocrine Society Clinical Practice Guidelines for Endocrine Treatment of Gender-Dysphoric/Gender-Incongruent Persons (the Endocrine Society Guidelines). The UCSF Guidelines indicate the conversion between estradiol valerate and cypionate to be as high as a 4:1 ratio [2], while the Endocrine Society Guidelines provide no dosing differentiations [1]. Herndon and colleagues demonstrated that the conversion between estradiol cypionate and estradiol valerate is closer to 1:1 [4]. Further equivalence studies are needed to clarify ideal dosing conversions.
The Endocrine Society Guidelines recommend titrating estradiol to 100-200 pg/mL [1]. The UCSF Guidelines recommend 2-4 mg daily as the starting dose for oral estradiol and 5 mg weekly for parenteral estradiol valerate [2]. The Endocrine Society Guidelines suggest oral estradiol 2-6 mg daily and parenteral estradiol 2- 10 mg weekly [1]. However, Chantrapanichkul et al. found that intramuscular injections of estradiol valerate greater than 5 mg weekly led to mean estradiol concentrations well above 200 pg/mL, while 4-5 mg of oral estradiol daily only led to minimum desired concentrations [5]. Similarly, Herndon et al. found that subcutaneous estradiol at a median dose of 3.75 mg per week led to a median estradiol level of 196 pg/mL [4]. Thus, current guideline-based dosing may lead providers to choose doses of injectable estradiol that would result in supratherapeutic serum estradiol levels. In light of these recent publications, it is clear that guideline-based dosing for estradiol needs updating. In our clinical experience, parenteral estradiol valerate at doses of 2-4 mg weekly typically leads to physiologic estradiol levels. Estradiol cypionate should likely be dosed in a 1:1 ratio with estradiol valerate until future data are obtained.
Lastly, while estradiol valerate and cypionate are only FDA-approved for intramuscular administration, many patients prefer subcutaneous administration. There are small studies that suggest the pharmacokinetics of intramuscular and subcutaneous estradiol are similar [4]. While the UCSF Guidelines comment on the use of subcutaneous estradiol, other guidelines should be updated to include this option for patients [2].
Abuhelwa, A. Y., Foster, D. J., & Upton, R. N. (2015). ADVAN-style analytical solutions for common pharmacokinetic models. Journal of Pharmacological and Toxicological Methods, 73, 42–48. [DOI:10.1016/j.vascn.2015.03.004]
Aedo, A. R., Landgren, B. M., Johannisson, E., & Diczfalusy, E. (1985). Pharmacokinetic and pharmacodynamic investigations with monthly injectable contraceptive preparations. Contraception, 31(5), 453–469. [DOI:10.1016/0010-7824(85)90081-2]
Aisaka, K., Ando, S., Kokubo, K., Yoshida, K., & Mori, H. (1986). いわゆる潜在性高prolactin血症患者におけるprolactin分泌予備能の検討. [Studies on Prolactin Secreting Capacity in the Ovulatory Infertile Patients with Transient Hyperprolactinemia.] 日本内分泌学会雑誌 / Nihon Naibunpi Gakkai Zasshi / Folia Endocrinologica Japonica, 62(5), 662–671. [DOI:10.1507/endocrine1927.62.5_662]
Akande, E. O. (1974). The effect of oestrogen on plasma levels of luteinizing hormone in euthyroid and thyrotoxic postmenopausal women. The Journal of Obstetrics and Gynaecology of the British Commonwealth / BJOG, 81(10), 795–803. [DOI:10.1111/j.1471-0528.1974.tb00383.x]
Ballard, B. E. (1978). An Overview of Prolonged Action Drug Dosage Forms. In Robinson, J. R. (Ed.). Sustained and Controlled Release Drug Delivery Systems (pp. 1–69). New York/Basel: Marcel Dekker. [Google Scholar] [Google Books]
Behre, H. M., Oberpenning, F., & Nieschlag, E. (1990). Comparative pharmacokinetics of androgen preparations: application of computer analysis and simulation. In Nieschlag, E., & Behre, H. M. (Eds.). Testosterone: Action · Deficiency · Substitution, 1st Edition (pp. 115–135). Berlin/Heidelberg: Springer. [DOI:10.1007/978-3-662-00814-0_6]
Behre, H. M., & Nieschlag, E. (1998). Comparative pharmacokinetics of testosterone esters. In Nieschlag, E., & Behre, H. M. (Eds.). Testosterone: Action · Deficiency · Substitution, 2nd Edition (pp. 329–348). Berlin/Heidelberg: Springer. [DOI:10.1007/978-3-642-72185-4_11]
Behre, H. M., Wang, C., Handelsman, D. J., & Nieschlag, E. (2004). Pharmacology of testosterone preparations. Testosterone: Action · Deficiency · Substitution, 3rd Edition (pp. 405–444). Cambridge/New York: Cambridge University Press. [DOI:10.1017/CBO9780511545221.015] [PDF]
Behre, H. M., & Nieschlag, E. (2012). Testosterone preparations for clinical use in males. In Nieschlag, E., Behre, H. M., & Nieschlag, S. (Eds.). Testosterone: Action · Deficiency · Substitution, 4th Edition (pp. 309–335). Cambridge/New York: Cambridge University Press. [DOI:10.1017/CBO9781139003353.016]
Bider, D., Ben-Rafael, Z., Shalev, J., Goldenberg, M., Mashiach, S., & Blankstein, J. (1989). Pituitary and ovarian suppression rate after high dosage of gonadotropin-releasing hormone agonist. Fertility and Sterility, 51(4), 578–581. [DOI:10.1016/S0015-0282(16)60602-7]
Blackwell, R. E., Boots, L. R., & Potter Jr, H. D. (1982). Evaluation of Delestrogen and Parlodel as a luteolytic agent in humans. Fertility and Sterility, 37(2), 213–217. [DOI:10.1016/S0015-0282(16)46042-5]
Bourns, A. (2019). Guidelines for Gender-Affirming Primary Care with Trans and Non-Binary Patients, 4th Edition. Toronto: Rainbow Health Ontario/Sherbourne Health. [URL] [PDF]
Bradbury, J. T., Long, R. C., & Durham, W. C. (1953). Progesterone and estrogen requirements to induce and maintain decidua. Fertility and Sterility, 4(1), 63–75. [DOI:10.1016/S0015-0282(16)31145-1]
Braun, P., Wildt, L., & Leyendecker, G. (1983). The effect of danazol on gonadotropin secretion during the follicular phase of the menstrual cycle. Fertility and Sterility, 40(1), 37–44. [DOI:10.1016/S0015-0282(16)47174-8]
Buckman, M. T., Johnson, J., Ellis, H., Srivastava, L., & Peake, G. T. (1980). Differential lipemic and proteinemic response to oral ethinyl estradiol and parenteral estradiol cypionate. Metabolism, 29(9), 803–805. [DOI:10.1016/0026-0495(80)90117-1]
Callen-Lorde Community Health Center. (2018). Protocols for the Provision of Hormone Therapy. New York City: Callen-Lorde Community Health Center. [URL] [PDF]
Canales, E. S., Cabezas, A., Vázquez-Matute, L., & Zárate, A. (1978). Induction of ovulation with clomiphene and estradiol benzoate in anovulatory women refractory to clomiphene alone. Fertility and Sterility, 29(5), 496–499. [DOI:10.1016/S0015-0282(16)43271-1]
Canales, E. S., Fonseca, M. E., Mason, M., & Zárate, A. (1981). Feedback effect of estradiol on follicle-stimulating hormone and prolactin secretion during the puerperium. International Journal of Gynecology & Obstetrics, 19(1), 79–81. [DOI:10.1016/0020-7292(81)90043-6]
Cano, A., Gimeno, F., Fuente, T., Parrilla, J. J., & Abad, L. (1986). The positive feedback of estradiol on gonadotropin secretion in women with perimenopausal dysfunctional uterine bleeding. European Journal of Obstetrics & Gynecology and Reproductive Biology, 22(5–6), 353–358. [DOI:10.1016/0028-2243(86)90125-5]
Cavanaugh, T., Hopwood, R., Gonzalez, A., & Thompson, J. (2015). The Medical Care of Transgender Persons. Boston: Fenway Health. [URL] [PDF]
Chantrapanichkul, P., Stevenson, M. O., Suppakitjanusant, P., Goodman, M., & Tangpricha, V. (2021). Serum Hormone Concentrations in Transgender Individuals Receiving Gender-Affirming Hormone Therapy: A Longitudinal Retrospective Cohort Study. Endocrine Practice, 27(1), 27–33. [DOI:10.4158/EP-2020-0414] [PDF] [Table]
Chien, Y. W. (1981). Long-acting parenteral drug formulations. Journal of Parenteral Science and Technology / PDA Journal of Pharmaceutical Science and Technology, 35(3), 106–139. [Google Scholar] [URL] [PDF]
Cirrincione, L. R., Winston McPherson, G., Rongitsch, J., Sadilkova, K., Drees, J. C., Krasowski, M. D., Dickerson, J. A., & Greene, D. N. (2021). Sublingual estradiol is associated with higher estrone concentrations than transdermal or injectable preparations in transgender women and gender nonbinary adults. LGBT Health, 8(2), 125–132. [DOI:10.1089/lgbt.2020.0249] [PDF] [Table]
Colburn, W. A. (1981). Simultaneous pharmacokinetic and pharmacodynamic modeling. Journal of Pharmacokinetics and Biopharmaceutics, 9(3), 367–388. [DOI:10.1007/BF01059272]
Coleman, E., Radix, A. E., Bouman, W. P., Brown, G. R., de Vries, A. L., Deutsch, M. B., Ettner, R., Fraser, L., Goodman, M., Green, J., Hancock, A. B., Johnson, T. W., Karasic, D. H., Knudson, G. A., Leibowitz, S. F., Meyer-Bahlburg, H. F., Monstrey, S. J., Motmans, J., Nahata, L., … & Arcelus, J. (2022). [World Professional Association for Transgender Health (WPATH)] Standards of Care for the Health of Transgender and Gender Diverse People, Version 8. International Journal of Transgender Health, 23(Suppl 1), S1–S259. [DOI:10.1080/26895269.2022.2100644] [URL] [PDF]
Dahl, M., Feldman, J. L., Goldberg, J., & Jaberi, A. (2015). Endocrine Therapy for Transgender Adults in British Columbia: Suggested Guidelines. Physical Aspects of Transgender Endocrine Therapy. Vancouver: Vancouver Coastal Health. [Google Scholar] [PDF]
Davidson, A., Franicevich, J., Freeman, M., Lin, R., Martinez, L., Monihan, M., Porch, M., Samuel, L., Stukalin, R., Vormohr, J., & Zevin, B. (2013). Protocols for Hormonal Reassignment of Gender. San Francisco: San Francisco Department of Public Health/Tom Waddell Health Center. [Google Scholar] [PDF]
Depo®-Estradiol Estradiol Cypionate Label. U.S. Food and Drug Administration/Pharmacia & Upjohn (Pfizer). [URL] [PDF]
Derra, C. (1981). Hormonprofile unter Östrogen- und Antiandrogentherapie bei Patienten mit Prostatakarzinom: Östradiolundecylat versus Cyproteronacetat. [Hormone Profiles under Estrogen and Antiandrogen Therapy in Patients with Prostate Cancer: Estradiol Undecylate versus Cyproterone Acetate.] (Doctoral dissertation, University of Mainz.) [Google Scholar] [WorldCat] [PDF] [Translation]
Deutsch, M. (2014). Medical Transition. In Erickson-Schroth, L. (Ed.). Trans Bodies, Trans Selves: A Resource for the Transgender Community, 1st Edition (pp. 241–264). Oxford: Oxford University Press. [Google Scholar] [Google Books] [OpenLibrary] [WorldCat] [Archive.org] [PDF]
Deutsch, M. B., Bhakri, V., & Kubicek, K. (2015). Effects of Cross-Sex Hormone Treatment on Transgender Women and Men. Obstetrics & Gynecology, 125(3), 605–610. [DOI:10.1097/AOG.0000000000000692]
Deutsch, M. B. (Ed.). (2016). Guidelines for the Primary and Gender-Affirming Care of Transgender and Gender Nonbinary People, 2nd Edition. San Francisco: University of California, San Francisco/UCSF Transgender Care. [URL] [PDF]
Deutsch, M. B. (2016). Overview of feminizing hormone therapy. In Deutsch, M. B. (Ed.). Guidelines for the Primary and Gender-Affirming Care of Transgender and Gender Nonbinary People, 2nd Edition (pp. 26–48). San Francisco: University of California, San Francisco/UCSF Transgender Care. [URL] [PDF]
Düsterberg, B., & Nishino, Y. (1982). Pharmacokinetic and pharmacological features of oestradiol valerate. Maturitas, 4(4), 315–324. [DOI:10.1016/0378-5122(82)90064-0]
Düsterberg, B., & Wendt, H. (1983). Plasma levels of dehydroepiandrosterone and 17β-estradiol after intramuscular administration of Gynodian-Depot® in 3 women. Hormones, 17(2), 84–89. [DOI:10.1159/000179680]
Düsterberg, B., Schmidt-Gollwitzer, M., & Hümpel, M. (1985). Pharmacokinetics and biotransformation of estradiol valerate in ovariectomized women. Hormone Research in Paediatrics, 21(3), 145–154. [DOI:10.1159/000180039]
Edkins, R. P. (1959). The Modification of the Duration of Drug Action: Pharmaceutical Considerations. Journal of Pharmacy and Pharmacology, 11(Suppl 1), 54T–66T. [DOI:10.1111/j.2042-7158.1959.tb10412.x]
Enever, R. P., Fotherby, K., Naderi, S., & Lewis, G. A. (1983). Long-acting contraceptive agents: The influence of physicochemical properties of some esters of norethisterone upon the plasma levels of free norethisterone. Steroids, 41(3), 381–396. [DOI:10.1016/0039-128X(83)90109-5]
Eriksson, O., Bäckström, T., Stridsberg, M., Hammarlund-Udenaes, M., & Naessén, T. (2006). Differential response to estrogen challenge test in women with and without premenstrual dysphoria. Psychoneuroendocrinology, 31(4), 415–427. [DOI:10.1016/j.psyneuen.2005.10.004]
Espino y Sosa, S., Cortés Fuentes, M., Gómez Rico, J. A., & Cortés Bonilla, M. (2019). Non-polymeric Microspheres for the Therapeutic Use of Estrogens: An Innovative Technology. In Khan, W. A. (Ed.). Estrogen. London: IntechOpen. [DOI:10.5772/intechopen.82553]
Fisher, D., & Shafer, S. (2007). Fisher/Shafer NONMEM Workshop Pharmacokinetic and Pharmacodynamic Analysis with NONMEM. Basic Concepts. [PDF]
Florence, A. T. (2010). Looking at Formulations. In Florence, A. T. An Introduction to Clinical Pharmaceutics (pp. 69–100). London/Chicago: Pharmaceutical Press. [Google Scholar] [Google Books]
Fotherby, K., Benagiano, G., Toppozada, H. K., Abdel-Rahman, A., Navaroli, F., Arce, B., Ramos-Cordero, R., Gual, C., Landgren, B. M., & Johannisson, E. (1982). A preliminary pharmacological trial of the monthly injectable contraceptive Cycloprovera. Contraception, 25(3), 261–272. [DOI:10.1016/0010-7824(82)90049-X]
Futterweit, W., Gabrilove, J., & Smith, H. (1984). Testicular steroidogenic response to human chorionic gonadotropin of fifteen male transsexuals on chronic estrogen treatment. Metabolism, 33(10), 936–942. [DOI:10.1016/0026-0495(84)90248-8] [Figure]
Garner, P. R., & Armstrong, D. T. (1977). The effect of human chorionic gonadotropin and estradiol-17β on the maintenance of the human corpus luteum of early pregnancy. American Journal of Obstetrics and Gynecology, 128(5), 469–475. [DOI:10.1016/0002-9378(77)90026-6]
Garza-Flores, J., Rodriguez, V., Perez-Palacios, G., Virutamasen, P., Tang-Keow, P., Konsayreepong, R., Kovacs, L., Koloszar, S., & Hall, P. E. (1987). A multicentered pharmacokinetic, pharmacodynamic study of once-a-month injectable contraceptives. I. Different doses of HRP112 and of DepoProvera. Contraception, 36(4), 441–457. [DOI:10.1016/0010-7824(87)90093-X]
Garza-Flores, J., Alba, V. M., Cravioto, M. C., Hernandez, L., Perez-Palacios, G., Alvarado, G., Rivera, R., Recio, R., & Bassol, S. (1989). Estrogen-progestogen once-a-month injectable contraceptives and serum prolactin. Contraception, 39(5), 519–529. [DOI:10.1016/0010-7824(89)90107-8]
Garza-Flores, J., Fatinikun, T., Hernandez, L., Ramos, I., Cardenas, M., & Menjivar, M. (1991). A pilot study on the assessment of a progesterone/estradiol sustained release as once-a-month-injectable contraceptive. Contraception, 44(1), 45–59. [DOI:10.1016/0010-7824(91)90105-O]
Garza-Flores, J. (1994). Pharmacokinetics of once-a-month injectable contraceptives. Contraception, 49(4), 347–359. [DOI:10.1016/0010-7824(94)90032-9]
Geppert, G. (1975). Untersuchungen zur Pharmakokinetik von Östradiol-17β, Östradiol-Benzoat, Östradiol-Valerianat und Östradiol-Undezylat bei der Frau: Der Verlauf der Konzentrationen von Östradiol-17β, Östron, LH und FSH im Serum. [Studies on the Pharmacokinetics of Estradiol-17β, Estradiol Benzoate, Estradiol Valerate, and Estradiol Undecylate in Women: The Course of the Relationships Between Estradiol-17β, Estrone, LH, and FSH in Serum.] (Doctoral dissertation, University of Bonn.) [Google Scholar] [WorldCat] [PDF] [Translation]
Glintborg, D., T’Sjoen, G., Ravn, P., & Andersen, M. S. (2021). Management of endocrine disease: Optimal feminizing hormone treatment in transgender people. European Journal of Endocrinology, 185(2), R49–R63. [DOI:10.1530/EJE-21-0059]
Goh, H. H., & Ratnam, S. S. (1988). The LH surge in humans: its mechanism and sex difference. Gynecological Endocrinology, 2(2), 165–182. [DOI:10.3109/09513598809023624]
Goh, H. H., & Ratnam, S. S. (1990). Effect of estrogens on prolactin secretion in transsexual subjects. Archives of Sexual Behavior, 19(5), 507–516. [DOI:10.1007/BF02442351]
Goh, V. H. H., & Lee, K. O. (1998). Does a positive oestrogen feedback on the hypothalamic-pituitary axis exist concurrently with a defective testosterone feedback in Klinefelter’s syndrome? Hormone Research in Paediatrics, 50(3), 160–165. [DOI:10.1159/000023266]
Goodman, R. E., Anderson, D. C., Bu’Lock, D. E., Sheffield, B., Lynch, S. S., & Butt, W. R. (1985). Study of the effect of estradiol on gonadotrophin levels in untreated male-to-female transsexuals. Archives of Sexual Behavior, 14(2), 141–146. [DOI:10.1007/BF01541659]
Gooren, L. J. G., Rao, B. R., Van Kessel, H., & Harmsen-Louman, W. (1984). Estrogen positive feedback on LH secretion in transsexuality. Psychoneuroendocrinology, 9(3), 249–259. [DOI:10.1016/0306-4530(84)90004-0]
Gooren, L. (2005). Hormone treatment of the adult transsexual patient. Hormone Research in Paediatrics, 64(Suppl 2), 31–36. [DOI:10.1159/000087751]
Göretzlehner, G., Ackermann, W., Angelow, K., Bergmann, G., Bieck, E., Golbs, S., & Kliem, O. (2002). Pharmakokinetik von Estron, Estradiol, FSH, LH und Prolaktin nach intramuskulärer Applikation von 5 mg Estradiolvalerat. [Pharmacokinetics of estradiol valerate in postmenopausal women after intramuscular administration.] Journal für Menopause, 9(2), 46–49. [Google Scholar] [URL] [PDF] [Translation]
Gorton, N., Jaffe, J. M., Thompson, J., Menkin, D., Nesteby, A., Dunn, D., Baker, K. K., Harbatkin, D., Do, T., Radix, A., Meacher, P., Goldstein, Z., Carpenter, W., Caine, M., Henn, S., Murayama, R., Feldmann, J., & Zayas, S. (2019). TransLine Gender Affirming Hormone Therapy Prescriber Guidelines. San Francisco: Lyon-Martin Health Services/TransLine. [URL] [PDF]
Gunnarsson, P. O., & Norlén, B. J. (1988). Clinical pharmacology of polyestradiol phosphate. The Prostate, 13(4), 299–304. [DOI:10.1002/pros.2990130405]
Hamburger, C., & Benjamin, H. (1969). Endocrine Treatment of Male and Female Transsexualism / Appendix for the Practicing Physician: Suggestions and Guidelines for the Management of Transsexuals. In Green, R., & Money, J. (Eds.). Transsexualism and Sex Reassignment (pp. 291–307). Baltimore: John Hopkins University Press. [Google Scholar] [Google Books] [PDF]
Hembree, W. C., Cohen-Kettenis, P. T., Gooren, L., Hannema, S. E., Meyer, W. J., Murad, M. H., Rosenthal, S. M., Safer, J. D., Tangpricha, V., & T’Sjoen, G. G. (2017). Endocrine Treatment of Gender-Dysphoric/Gender-Incongruent Persons: An Endocrine Society Clinical Practice Guideline. The Journal of Clinical Endocrinology and Metabolism, 102(11), 3869–3903. [DOI:10.1210/jc.2017-01658]
Henriksson, P., Carlström, K., Pousette, A., Gunnarsson, P. O., Johansson, C. J., Eriksson, B., Altersgård-Brorsson, A. K., Nordle, O., & Stege, R. (1999). Time for revival of estrogens in the treatment of advanced prostatic carcinoma? Pharmacokinetics, and endocrine and clinical effects, of a parenteral estrogen regimen. The Prostate, 40(2), 76–82. [DOI:10.1002/(SICI)1097-0045(19990701)40:2<76::AID-PROS2>3.0.CO;2-Q]
Herndon, J. S., Maheshwari, A. K., Nippoldt, T. B., Carlson, S. J., Davidge-Pitts, C. J., & Chang, A. Y. (2023). Comparison of Subcutaneous and Intramuscular Estradiol Regimens as part of Gender-Affirming Hormone Therapy. Endocrine Practice, 29(5), 356–361. [DOI:10.1016/j.eprac.2023.02.006] [URL] [PDF]
Hughes, J. H., Woo, K. H., Keizer, R. J., & Goswami, S. (2022). Clinical Decision Support for Precision Dosing: Opportunities for Enhanced Equity and Inclusion in Health Care. Clinical Pharmacology & Therapeutics, 113(3), 565–574. [DOI:10.1002/cpt.2799]:
Ibrahim, S. (1996/1998). Pharmakokinetische Untersuchungen mit Östradiolvalerat und Hydroxyprogesteroncaproat in Depotform nach einmaliger Applikation bei 24 postmenopausalen Frauen. [Pharmacokinetic studies with estradiol valerate and hydroxyprogesterone caproate in depot form after a single application in 24 postmenopausal women.] (Doctoral dissertation, Dresden University of Technology.) [Google Scholar] [WorldCat] [Partial PDF]
Ittrich, G., & Pots, P. (1965). Östrogenbestimmungen in Blut und Urin nach Verabreichung von Östrogenen. [Estrogen determinations in blood and urine after administration of estrogens.] In Kraatz, H. (Ed.). International Symposium der Gynäkologischen Endokrinologie vom 15. bis 18. Mai 1963. / Abhandlungen der Deutschen Akademie der Wissenschaften zu Berlin, Klasse für Medizin, 1965(1), 53–56. [ISSN:0568-4250] [WorldCat 1] [WorldCat 2] [WorldCat 3] [PDF] [Translation]
Jaafar, S., Torres-Leguizamon, M., Duplessy, C., & Stambolis-Ruhstorfer, M. (2022). Hormonothérapie injectable et réduction des risques: pratiques, difficultés, santé des personnes trans en France. [Hormone replacement therapy injections and harm reduction: practices, difficulties, and transgender people’s health in France.] Sante Publique, 34(HS2), 109–122. [Google Scholar] [PubMed] [DOI:10.3917/spub.hs2.0109]
Jacobi, G. H., & Altwein, J. E. (1979). Bromocriptin als Palliativtherapie beim fortgeschrittenen Prostatakarzinom. [Bromocriptine for palliation of advanced prostatic carcinoma. Experimental and clinical profile of a drug.] Urologia Internationalis, 34(4), 266–290. [DOI:10.1159/000280272]
Jacobi, G. H., Altwein, J. E., Kurth, K. H., Basting, R., & Hohenfellner, R. (1980). Treatment of advanced prostatic cancer with parenteral cyproterone acetate: a phase III randomised trial. British Journal of Urology, 52(3), 208–215. [DOI:10.1111/j.1464-410X.1980.tb02961.x]
Jacobi, G. R. (1982). Experimental Rationale for the Investigation of Antiprolactins as Palliative Treatment for Prostate Cancer. In Jacobi, G. H., & Hohenfellner, R. (Eds.). Prostate Cancer (International Perspectives in Urology, Volume 3) (pp. 419–431). Baltimore/London: Williams & Wilkins. [Google Scholar] [Google Books]
Jilma, B., Eichler, H. G., Breiteneder, H., Wolzt, M., Aringer, M., Graninger, W., Röhrer, C., Veitl, M., & Wagner, O. F. (1994). Effects of 17β-estradiol on circulating adhesion molecules. The Journal of Clinical Endocrinology and Metabolism, 79(6), 1619–1624. [DOI:10.1210/jcem.79.6.7527406]
Johansson, C. J., & Gunnarsson, P. O. (2000). Pharmacodynamic model of testosterone suppression after intramuscular depot estrogen therapy in prostate cancer. The Prostate, 44(1), 26–30. [DOI:10.1002/1097-0045(20000615)44:1<26::AID-PROS4>3.0.CO;2-P]
Jones, T. M., Fang, V. S., Landau, R. L., & Rosenfield, R. (1978). Direct inhibition of Leydig cell function by estradiol. The Journal of Clinical Endocrinology and Metabolism, 47(6), 1368–1373. [DOI:10.1210/jcem-47-6-1368]
Jönsson, G., Olsson, A. M., Luttrop, W., Cekan, Z., Purvis, K., & Diczfalusy, E. (1976). Treatment of prostatic carcinoma with various types of estrogen derivatives. In Munson, P. L., Diczfalusy, E., Glover, J., Olson, R. E., Harris, R. S., Thimann, K. V., Loraine, J. A., & Wool, I. G. (Eds.). Vitamins & Hormones, Volume 33 (pp. 351–376). New York/San Francisco/London: Academic Press. [DOI:10.1016/S0083-6729(08)60965-6]
Kalicharan, R. W., Schot, P., & Vromans, H. (2016). Fundamental understanding of drug absorption from a parenteral oil depot. European Journal of Pharmaceutical Sciences, 83, 19–27. [DOI:10.1016/j.ejps.2015.12.011]
Kalicharan, R. W. (2017). New Insights into Drug Absorption from Oil Depots. (Doctoral dissertation, Utrecht University.) [Google Scholar] [URL] [PDF]
Kariyawasam, N. M., Ahmad, T., Sarma, S., & Fung, R. (2024). Comparison of Estrone/Estradiol Ratio and Levels in Transfeminine Individuals on Different Routes of Estradiol. Transgender Health, ahead of print. [DOI:10.1089/trgh.2023.0138] [Data]
Kemeter, P., Bernaschek, G., Altmann, G., & Feichtinger, W. (1984). The effect of 2 mg estradiol-17β plus 1 mg estriol, sequentially combined with 1 mg norethisteroneacetate, on LH, FSH, estradiol-17β, progesterone, testosterone and prolactin after ovarectomy. Archives of Gynecology, 234(3), 219–229. [DOI:10.1007/BF00570759]
Kerdelhué, B., Andrews, M. C., Zhao, Y., Scholler, R., & Jones Jr, H. W. (2006). Short term changes in melatonin and cortisol serum levels after a single administration of estrogen to menopausal women. Neuroendocrinology Letters, 27(5), 659–664. [Google Scholar] [URL] [PDF]
Keye, W. R., & Jaffe, R. B. (1975). Strength-duration characteristics of estrogen effects on gonadotropin response to gonadotropin-releasing hormone in women. I. Effects of varying duration of estradiol administration. The Journal of Clinical Endocrinology and Metabolism, 41(6), 1003–1008. [DOI:10.1210/jcem-41-6-1003]
Knudsen, P., Hansen, L. B., & Larsen, N. E. (1985). Pharmacokinetic implications of different oil vehicles used in depot neuroleptic treatment. Acta Psychiatrica Scandinavica, 72(S322), 7–10. [DOI:10.1111/j.1600-0447.1985.tb08535.x]
Kronawitter, D., Gooren, L. J., Zollver, H., Oppelt, P. G., Beckmann, M. W., Dittrich, R., & Mueller, A. (2009). Effects of transdermal testosterone or oral dydrogesterone on hypoactive sexual desire disorder in transsexual women: results of a pilot study. European Journal of Endocrinology, 161(2), 363–368. [DOI:10.1530/eje-09-0265] [Table]
Kuhl, H. (1986). Hormonsubstitution durch Injektionspräparate und Hautimplantate. [Hormone substitution by injectable preparations and skin implants.] Der Gynäkologe, 19(4), 241–247. [Google Scholar] [PubMed] [PDF] [Translation]
Kuhl, H. (1990). Pharmacokinetics of oestrogens and progestogens. Maturitas, 12(3), 171–197. [DOI:10.1016/0378-5122(90)90003-O]
Kuhl, H. (2005). Pharmacology of estrogens and progestogens: influence of different routes of administration. Climacteric, 8(Suppl 1), 3–63. [DOI:10.1080/13697130500148875] [PDF]
LaBudde, J. A., Craig, W. Y., & Spratt, D. I. (2020). Initial Evaluation of Safety and Efficacy of Administration of Estradiol (E2) by Subcutaneous (SC) Injections to Male-to-Female (MTF) Transgender Patients. Fertility and Sterility, 114(3), e91–e91. [DOI:10.1016/j.fertnstert.2020.08.277]
Langley, R. E., Gilbert, D. C., Duong, T., Clarke, N. W., Nankivell, M., Rosen, S. D., Mangar, S., Macnair, A., Sundaram, S. K., Laniado, M. E., Dixit, S., Madaan, S., Manetta, C., Pope, A., Scrase, C. D., Mckay, S., Muazzam, I. A., Collins, G. N., Worlding, J., Williams, S. T., … & Parmar, M. (2021). Transdermal oestradiol for androgen suppression in prostate cancer: long-term cardiovascular outcomes from the randomised Prostate Adenocarcinoma Transcutaneous Hormone (PATCH) trial programme. The Lancet, 397(10274), 581–591. [DOI:10.1016/S0140-6736(21)00100-8]
Larsen, S. W., Rinvar, E., Svendsen, O., Lykkesfeldt, J., Friis, G. J., & Larsen, C. (2001). Determination of the disappearance rate of iodine-125 labelled oils from the injection site after intramuscular and subcutaneous administration to pigs. International Journal of Pharmaceutics, 230(1–2), 67–75. [DOI:10.1016/S0378-5173(01)00860-2]
Larsen, S. W., & Larsen, C. (2009). Critical factors influencing the in vivo performance of long-acting lipophilic solutions—impact on in vitro release method design. The AAPS Journal, 11(4), 762–770. [DOI:10.1208/s12248-009-9153-9]
Larsen, C., Larsen, S. W., Jensen, H., Yaghmur, A., & Østergaard, J. (2009). Role of in vitro release models in formulation development and quality control of parenteral depots. Expert Opinion on Drug Delivery, 6(12), 1283–1295. [DOI:10.1517/17425240903307431]
Larsen, S. W., Thing, M. A., & Larsen, C. (2012). Oily (lipophilic) solutions and suspensions. In Wright, J. C., & Burgess, D. J. (Eds.). Long Acting Injections and Implants (Advances in Delivery Science and Technology) (pp. 113–135). Boston: Springer. [DOI:10.1007/978-1-4614-0554-2_7]
Le, A., Huang, K. J., & Cirrincione, L. R. (2022). Regulation of drug-metabolizing enzymes by sex-related hormones: clinical implications for transgender medicine. Trends in Pharmacological Sciences, 43(7), 582–592. [DOI:10.1016/j.tips.2022.03.006]
Leinonen, P., Hammond, G. L., Lukkarinen, O., & Vihko, R. (1979). Serum sex hormone binding globulin and testosterone binding after estradiol administration, castration, and their combination in men with prostatic carcinoma. Investigative Urology, 17(1), 24–27. [Google Scholar] [PubMed]
Leinonen, P. (1980). Estrone and estradiol concentrations in the testis and spermatic and peripheral venous blood of elderly men: the influence of estrogen treatment. Journal of Steroid Biochemistry, 13(7), 737–742. [DOI:10.1016/0022-4731(80)90225-3]
Leyendecker, G., Geppert, G., Nocke, W., & Ufer, J. (1975). Untersuchungen zur Pharmakokinetik von Östradiol-17β, Östradiol-Benzoat, Östradiol-Valerianat und Östradiol-Undezylat bei der Frau: Der Verlauf der Konzentrationen von Östradiol-17β, Östron, LH und FSH im Serum. [Estradiol-17β, Estrone, LH and FSH in Serum After Administration of Estradiol-17β, Estradiol-Benzoate, Estradiol-Valeriate and Estradiol-Undecylate in the Female.] Geburtshilfe und Frauenheilkunde, 35(5), 370–374. [Google Scholar] [PubMed] [PDF] [Translation]
Leyendecker, G., Wildt, L., Gips, H., Nocke, W., & Plotz, E. J. (1976). Experimental studies on the positive feedback effect of progesterone, 17α-hydroxyprogesterone and 20α-dihydroprogesterone on the pituitary release of LH and FSH in the human female. Archiv für Gynäkologie, 221(1), 29–45. [DOI:10.1007/BF00667679]
Lichten, E. M., Lichten, J. B., Whitty, A., & Pieper, D. (1996). The confirmation of a biochemical marker for women’s hormonal migraine: The depo‐estradiol challenge test. Headache: The Journal of Head and Face Pain, 36(6), 367–371. [DOI:10.1046/j.1526-4610.1996.3606367.x]
Linet, T. (2023). Prise en charge endocrinologique d’une personne trans. [Endocrinological care of a trans person.] In Faucher, P., Hassoun, D., & Linet, T. (Eds.). Santé sexuelle et reproductive des personnes LGBT [Sexual and Reproductive Health of LGBT People] (pp. 109–124). Issy-les-Moulineaux, France: Elsevier Masson. [Google Books] [URL] [WorldCat] [Excerpt]
Lixsoft. (2008). Mathematical Expressions of the Pharmacokinetic and Pharmacodynamic Models Implemented in the Monolix Software. [PDF]
Martinez, G. (1995). Estradiol and Progesterone Serum Levels in Women Using the Once-a-month Injectable Contraceptive Perlutal. / Benagiano, G., Bianchi, P., von Kesserü, E., Castañeda, A., Correa, J. E., & Martínez, G. (1995). Session 19 what is new about injectable contraceptives? Advances in Contraception, 11(1), 39–42. [DOI:10.1007/BF02436100]
Martins, R. S., Antunes, N. J., Comerlatti, G., Caraccio, G., Moreno, R. A., Frecentese, F., Caliendo, G., & De Nucci, G. (2019). Quantification of estradiol cypionate in plasma by liquid chromatography coupled with tandem mass spectrometry: Application in a pharmacokinetic study in healthy female volunteers. Journal of Pharmaceutical and Biomedical Analysis, 170, 273–278. [DOI:10.1016/j.jpba.2019.03.053]
Messinis, I. E., & Templeton, A. (1987). Effect of high dose exogenous oestrogen on midcycle luteinizing hormone surge in human spontaneous cycles. Clinical Endocrinology, 27(4), 453–459. [DOI:10.1111/j.1365-2265.1987.tb01173.x]
Messinis, I. E., & Templeton, A. A. (1987). Disparate effects of endogenous and exogenous oestradiol on luteal phase function in women. Reproduction, 79(2), 549–554. [DOI:10.1530/jrf.0.0790549]
Minto, C. F., Howe, C., Wishart, S., Conway, A. J., & Handelsman, D. J. (1997). Pharmacokinetics and pharmacodynamics of nandrolone esters in oil vehicle: effects of ester, injection site and injection volume. Journal of Pharmacology and Experimental Therapeutics, 281(1), 93–102. [URL]
Mueller, A., Zollver, H., Kronawitter, D., Oppelt, P. G., Claassen, T., Hoffmann, I., Beckmann, M. W., & Dittrich, R. (2011). Body composition and bone mineral density in male-to-female transsexuals during cross-sex hormone therapy using gonadotrophin-releasing hormone agonist. Experimental and Clinical Endocrinology & Diabetes, 119(2), 95–100. [DOI:10.1055/s-0030-1255074] [Table]
Newton, J. R., d’Arcangues, C., & Hall, P. E. (1994). A review of ‘once-a-month’ combined injectable contraceptives. Journal of Obstetrics and Gynaecology, 14(Suppl 1), S1–S34. [DOI:10.3109/01443619409027641]
Nelson, M. D., Szczepaniak, L. S., Wei, J., Szczepaniak, E., Sánchez, F. J., Vilain, E., Stern, J. H., Bergman, R. N., Bairey Merz, C. N., & Clegg, D. J. (2016). Transwomen and the Metabolic Syndrome: Is Orchiectomy Protective? Transgender Health, 1(1), 165–171. [DOI:10.1089/trgh.2016.0016] [Table]
Nieschlag, E., & Behre, H. M. (2010). Testosterone therapy. In Nieschlag, E., Behre, H. M., & Nieschlag, S. (Eds.). Andrology (pp. 437–455). Berlin/Heidelberg: Springer. [DOI:10.1007/978-3-540-78355-8_21] [PDF]
Norlén, B. J., Fritjofsson, Å., Grönquist, L., Gunnarsson, P. O., Johansson, S. Å., & Plym-Forshell, G. (1987). Plasma concentrations of estradiol and testosterone in single-drug polyestradiol phosphate therapy for prostatic cancer. European Urology, 13, 193–197. [DOI:10.1159/000472772]
Olson-Kennedy, J., Rosenthal, S. M., Hastings, J., & Wesp, L. (2016). Health considerations for gender non-conforming children and transgender adolescents. In Deutsch, M. B. (Ed.). Guidelines for the Primary and Gender-Affirming Care of Transgender and Gender Nonbinary People, 2nd Edition (pp. 186–199). San Francisco: University of California, San Francisco/UCSF Transgender Care. [URL] [PDF]
Oriowo, M. A., Landgren, B. M., Stenström, B., & Diczfalusy, E. (1980). A comparison of the pharmacokinetic properties of three estradiol esters. Contraception, 21(4), 415–424. [DOI:10.1016/S0010-7824(80)80018-7]
Parkes, A. S. (1937). Relative duration of action of various esters of oestrone, oestradiol and oestriol. Biochemical Journal, 31(4), 579–585. [DOI:10.1042/bj0310579]
Patel, R., Korenman, S., Weimer, A., & Grock, S. (2024). A Call for Updates to Hormone Therapy Guidelines for Gender-Diverse Adults Assigned Male at Birth. Cureus, 16(6), e62262. [DOI:10.7759/cureus.62262] [PDF]:
Presl, J., Horejsi, J., Štroufová, A., & Herzmann, J. (1976). Sexual maturation in girls and the development of estrogen-induced gonadotropic hormone release. Annales de Biologie Animale, Biochimie, Biophysique, 16(3), 377–383. [DOI:10.1051/rnd:19760314]
Rahimy, M. H., & Ryan, K. K. (1999). Lunelle monthly contraceptive injection (medroxyprogesterone acetate and estradiol cypionate injectable suspension): assessment of return of ovulation after three monthly injections in surgically sterile women. Contraception, 60(4), 189–200. [DOI:10.1016/s0010-7824(99)00081-5]
Rahimy, M. H., Ryan, K. K., & Hopkins, N. K. (1999). Lunelle™ monthly contraceptive injection (medroxyprogesterone acetate and estradiol cypionate injectable suspension): steady-state pharmacokinetics of MPA and E2 in surgically sterile women. Contraception, 60(4), 209–214. [DOI:10.1016/S0010-7824(99)00086-4]
Rauramo, L., Punnonen, R., Kaihola, H. L., & Grönroos, M. (1980). Serum oestrone, oestradiol and oestriol concentrations in castrated women during intramuscular oestradiolvalerate and oestradiolbenzoate-oestradiolphenylpropionate therapy. Maturitas, 2(1), 53–58. [DOI:10.1016/0378-5122(80)90060-2]
Rauramo, L., Punnonen, R., & Grönroos, M. (1981). Serum concentrations of oestrone, oestradiol and oestriol during various oestrogen treatments. Maturitas, 3(2), 183–186. [DOI:10.1016/0378-5122(81)90010-4]
Recio, R., Garza-Flores, J., Schiavon, R., Reyes, A., Diaz-Sanchez, V., Valles, V., Luz de la Cruz, D., Oropeza, G., & Perez-Palacios, G. (1986). Pharmacodynamic assessment of dihydroxyprogesterone acetophenide plus estradiol enanthate as a monthly injectable contraceptive. Contraception, 33(6), 579–589. [DOI:10.1016/0010-7824(86)90046-6]
Reimann, I. W., Britzelmeier, C., Haber, P., Wollmann, H., Antonin, K. H., & Bieck, P. R. (1987). Influence of Oestradiol on Alpha2-Adrenoceptor Binding Sites on Intact Platelets of Young Male Volunteers. European Journal of Clinical Pharmacology, 33(2), 147–150. [DOI:10.1007/BF00544558]
Rosenfield, R. L., Fang, V. S., Dupon, C., Kim, M. H., & Refetoff, S. (1973). The effects of low doses of depot estradiol and testosterone in teenagers with ovarian failure and Turner’s syndrome. The Journal of Clinical Endocrinology and Metabolism, 37(4), 574–580. [DOI:10.1210/jcem-37-4-574]
Rosenfield, R. L., & Fang, V. S. (1974). The effects of prolonged physiologic estradiol therapy on the maturation of hypogonadal teen-agers. The Journal of Pediatrics, 85(6), 830–837. [DOI:10.1016/S0022-3476(74)80355-0]
Rothman, M. S., Ariel, D., Kelley, C., Hamnvik, O. R., Abramowitz, J., Irwig, M. S., Soe, K., Davidge-Pitts, C., Misakian, A. L., Safer, J. D., & Iwamoto, S. J. (2024). The Use of Injectable Estradiol in Transgender and Gender Diverse Adults: A Scoping Review of Dose and Serum Estradiol Levels. Endocrine Practice, ahead of print. [DOI:10.1016/j.eprac.2024.05.008]
Rothman, M. S., Hamnvik, O. P. R., Davidge-Pitts, C., Safer, J. D., Ariel, D., Tangpricha, V., Abramowitz, J., Soe, K., Sarvaideo, J., Kelley, C., Irwig, M. S., & Iwamoto, S. J. (2024). Revisiting Injectable Estrogen Dosing Recommendations for Gender-Affirming Hormone Therapy. Transgender Health, ahead of print. [DOI:10.1089/trgh.2023.0209]
Sang, G. W., Ge, J. L., Liu, X. H., Shao, Q. X., Zhao, X. J., & Mao, S. M. (1987). 不同剂量庚炔诺酮单独或配伍戊酸雌二醇后的药代动力学及药效学. [Pharmacokinetics and pharmacodynamics of different doses of norethisterone enanthate alone and in combination with estradiol valerate.] 中国 临 床药理 学杂志 / Chinese Journal of Clinical Pharmacology, 3(1), 7–18. [Google Scholar] [CNKI] [DOI:10.13699/j.cnki.1001-6821.1987.01.002] [PDF]
Sang, G. W. (1994). Pharmacodynamic effects of once-a-month combined injectable contraceptives. Contraception, 49(4), 361–385. [DOI:10.1016/0010-7824(94)90033-7]
Schiavon, R., Benavides, S., Oropeza, G., Garza-Flores, J., Recio, R., Díaz-Sanchez, V., & Pérez-Palacios, G. (1988). Serum estrogens and ovulation return in chronic users of a once-a-month injectable contraceptive. Contraception, 37(6), 591–598. [DOI:10.1016/0010-7824(88)90005-4]
Schug, B. S., Donath, F., & Blume, H. H. (2012). Bioavailability and pharmacodynamics of two 10-mg estradiol valerate depot formulations following IM single dose administration in healthy postmenopausal volunteers. International Journal of Clinical Pharmacology and Therapeutics, 50(2), 100–117. [Google Scholar] [DOI:10.5414/cp201589] [PDF]
Schulte-Beerbühl, M., & Nieschlag, E. (1980). Comparison of testosterone, dihydrotestosterone, luteinizing hormone, and follicle-stimulating hormone in serum after injection of testosterone enanthate or testosterone cypionate. Fertility and Sterility, 33(2), 201–203. [DOI:10.1016/S0015-0282(16)44543-7]
Schultz, K., Møllgaard, B., Fisher, A. N., Illum, L., & Larsen, C. (1998). Intramuscular rate of disappearance of oily vehicles in rabbits investigated by gamma-scintigraphy. International Journal of Pharmaceutics, 169(1), 121–126. [DOI:10.1016/S0378-5173(98)00121-5]
Schweikert, H. U., Weissbach, L., Leyendecker, G., Schwinger, E., Wartenberg, H., & Krück, F. (1982). Clinical, endocrinological, and cytological characterization of two 46, XX males. The Journal of Clinical Endocrinology & Metabolism, 54(4), 745–752. [DOI:10.1210/jcem-54-4-745]
Seibert, B., & Günzel, P. (1994). Animal toxicity studies performed for risk assessment of the once-a-month injectable contraceptive Mesigyna®. Contraception, 49(4), 303–333. [DOI:10.1016/0010-7824(94)90030-2]
Shah, J. C. (2007). Controlled Release – Small Molecules. In Stella, V. J., Borchardt, R. T., Hageman, M. J., Oliyai, R., Maag, H., & Tilley, J. W. (Eds.). Prodrugs: Challenges and Rewards, Part 1 (Biotechnology: Pharmaceutical Aspects, Volume V) (pp. 357–377). New York: Springer. [DOI:10.1007/978-0-387-49785-3_9]
Sharula, Chekir, C., Emi, Y., Arai, F., Kikuchi, Y., Sasaki, A., Matsuda, M., Shimizu, K., Tabuchi, K., Kamada, Y., Hiramatsu, Y., & Nakatsuka, M. (2012). Altered arterial stiffness in male‐to‐female transsexuals undergoing hormonal treatment. Journal of Obstetrics and Gynaecology Research, 38(6), 932–940. [DOI:10.1111/j.1447-0756.2011.01815.x] [Data]
Shaw, R. W., Butt, W. R., London, D. R., & Marshall, J. C. (1975). The oestrogen provocation test: a method of assessing the hypothalamic‐pituitary axis in patients with amenorrhoea. Clinical Endocrinology, 4(3), 267–276. [DOI:10.1111/j.1365-2265.1975.tb01534.x]
Shaw, R. W., Butt, W. R., & London, D. R. (1975). The effect of oestrogen pretreatment on subsequent response to luteinizing hormone releasing hormone in normal women. Clinical Endocrinology, 4(3), 297–304. [DOI:10.1111/j.1365-2265.1975.tb01537.x]
Shaw, R. W. (1978). Neuroendocrinology of the menstrual cycle in humans. Clinics in Endocrinology and Metabolism, 7(3), 531–559. [DOI:10.1016/S0300-595X(78)80008-5]
Shahiwala, A., Mehta, T. A., & Momin, M. M. (2018). Parenteral drug delivery systems. In Misra, A., & Shahiwala, A. (Eds.). In-Vitro and In-Vivo Tools in Drug Delivery Research for Optimum Clinical Outcomes (pp. 283–318). Boca Raton: CRC Press. [DOI:10.1201/b22448-9] [Google Books]
Sherwin, B. B., & Gelfand, M. M. (1987). Individual differences in mood with menopausal replacement therapy: Possible role of sex hormone-binding globulin. Journal of Psychosomatic Obstetrics & Gynecology, 6(2), 121–131. [DOI:10.3109/01674828709016773]
Sherwin, B. B., Gelfand, M. M., Schucher, R., & Gabor, J. (1987). Postmenopausal estrogen and androgen replacement and lipoprotein lipid concentrations. American Journal of Obstetrics and Gynecology, 156(2), 414–419. [DOI:10.1016/0002-9378(87)90295-X]
Sherwin, B. B. (1988). Affective changes with estrogen and androgen replacement therapy in surgically menopausal women. Journal of Affective Disorders, 14(2), 177–187. [DOI:10.1016/0165-0327(88)90061-4]
Sierra-Ramírez, J. A., Lara-Ricalde, R., Lujan, M., Velázquez-Ramírez, N., Godínez-Victoria, M., Hernádez-Munguía, I. A., Padilla, A., & Garza-Flores, J. (2011). Comparative pharmacokinetics and pharmacodynamics after subcutaneous and intramuscular administration of medroxyprogesterone acetate (25 mg) and estradiol cypionate (5 mg). Contraception, 84(6), 565–570. [DOI:10.1016/j.contraception.2011.03.014]
Sinkula, A. A. (1978). Methods to Achieve Sustained Drug Delivery. The Chemical Approach. In Robinson, J. R. (Ed.). Sustained and Controlled Release Drug Delivery Systems (pp. 411–555). New York/Basel: Marcel Dekker. [Google Scholar] [Google Books] [PDF]
Somerville, B. W. (1971). The Role of Oestradiol in Menstrual Migraine. In Somerville, B. W. The Influence of Progesterone and Oestradiol on Migraine (Doctoral dissertation, University of New South Wales) (pp. 93–104). [Google Scholar] [URL] [WorldCat] [PDF]
Somerville, B. W. (1972). The Role of Estradiol Withdrawal in the Etiology of Menstrual Migraine. Neurology, 22(4), 355–365. [DOI:10.1212/WNL.22.4.355]
Somerville, B. W. (1972). The influence of progesterone and estradiol upon migraine. Headache: The Journal of Head and Face Pain, 12(3), 93–102. [DOI:10.1111/j.1526-4610.1972.hed1203093.x]
Somerville, B. W. (1972). The Influence of Hormones Upon Migraine in Women. Medical Journal of Australia, 2(S2), 6–11. [DOI:10.5694/j.1326-5377.1972.tb93039.x]
Somerville, B. W. (1975). Estrogen‐withdrawal migraine: I. Duration of exposure required and attempted prophylaxis by premenstrual estrogen administration. Neurology, 25(3), 239–244. [DOI:10.1212/wnl.25.3.239]
Spack, N. P. (2013). Management of transgenderism. JAMA, 309(5), 478–484. [DOI:10.1001/jama.2012.165234]
Stege, R., Carlström, K., Collste, L., Eriksson, A., Henriksson, P., & Pousette, A. (1988). Single drug polyestradiol phosphate therapy in prostatic cancer. American Journal of Clinical Oncology, 11(Suppl 2), S101–S103. [DOI:10.1097/00000421-198801102-00024] [PDF]
Stege, R., Carlström, K., Collste, L., Eriksson, A., Henriksson, P., Pousette, Å., & von Schoultz, B. (1989). Single‐drug parenteral estrogen treatment in prostatic cancer: A study of two maintenance‐dose regimens. The Prostate, 14(2), 183–188. [DOI:10.1002/pros.2990140211]
Stege, R., Gunnarsson, P. O., Johansson, C. J., Olsson, P., Pousette, Å., & Carlström, K. (1996). Pharmacokinetics and testosterone suppression of a single dose of polyestradiol phosphate (Estradurin®) in prostatic cancer patients. The Prostate, 28(5), 307–310. [DOI:10.1002/(SICI)1097-0045(199605)28:5<307::AID-PROS6>3.0.CO;2-8]
Sumioki, H. (1987). ヒト排卵機構とGonadotropin分泌調節における “β-Endorphinおよびβ-Lipotropin” の役割に関する研究. [The Role of “β-Endorphin & β-Lipotropin” on the Gonadotropin Regulation in the Mechanism of Human Ovulation.] Folia Endocrinologica Japonica, 63(10), 1289–1307. [DOI:10.1507/endocrine1927.63.10_1289]
Svendsen, O., & Aaes‐Jørgensen, T. (1979). Studies on the fate of vegetable oil after intramuscular injection into experimental animals. Acta Pharmacologica et Toxicologica, 45(5), 352–378. [DOI:10.1111/j.1600-0773.1979.tb02404.x]
Tassinari, R., & Maranghi, F. (2021). Rodent Model of Gender-Affirming Hormone Therapies as Specific Tool for Identifying Susceptibility and Vulnerability of Transgender People and Future Applications for Risk Assessment. International Journal of Environmental Research and Public Health, 18(23), 12640. [DOI:10.3390/ijerph182312640]
Thurman, A., Kimble, T., Hall, P., Schwartz, J. L., & Archer, D. F. (2013). Medroxyprogesterone acetate and estradiol cypionate injectable suspension (Cyclofem) monthly contraceptive injection: steady-state pharmacokinetics. Contraception, 87(6), 738–743. [DOI:10.1016/j.contraception.2012.11.010]
Toppozada, M. K. (1994). Existing once-a-month combined injectable contraceptives. Contraception, 49(4), 293–301. [DOI:10.1016/0010-7824(94)90029-9]
Toutain, P. L., & Bousquet-Mélou, A. (2004). Plasma terminal half-life. Journal of Veterinary Pharmacology and Therapeutics, 27(6), 427–439. [DOI:10.1111/j.1365-2885.2004.00600.x]
Trans Care BC. (2021). Gender-affirming Care for Trans, Two-Spirit, and Gender Diverse Patients in BC: A Primary Care Toolkit. Vancouver: Provincial Health Services Authority/Trans Care BC. [URL] [PDF]
Travaglini, P., Ambrosi, B., Beck-Peccoz, P., Elli, R., Rondena, M., Bara, R., & Weber, G. (1978). Hypothalamic-pituitary-ovarian function in hyperprolactinemic women. Journal of Endocrinological Investigation, 1(1), 39–45. [DOI:10.1007/BF03346769]
Travaglini, P., Elli, R., Ambrosi, B., Ballabio, M., Moriondo, P., & Faglia, G. (1979). Serum LH increase after estradiol and progesterone administration in hyperprolactinemic women. Journal of Endocrinological Investigation, 2(4), 407–411. [DOI:10.1007/BF03349341]
T’Sjoen, G., Arcelus, J., De Vries, A. L., Fisher, A. D., Nieder, T. O., Özer, M., & Motmans, J. (2020). European Society for Sexual Medicine position statement “assessment and hormonal management in adolescent and adult trans people, with attention for sexual function and satisfaction”. The Journal of Sexual Medicine, 17(4), 570–584. [DOI:10.1016/j.jsxm.2020.01.012]
Ulrich, U., Pfeifer, T., & Lauritzen, C. (1994). Rapid Increase in Lumbar Spine Bone Density in Osteopenic Women by High-Dose Intramuscular Estrogen-Progestogen Injections. Hormone and Metabolic Research, 26(9), 428–431. [DOI:10.1055/s-2007-1001723]
Välimäki, M., Pelkonen, R., Salaspuro, M., Härkönen, M., Hirvonen, E., & Ylikahri, R. (1984). Sex hormones in amenorrheic women with alcoholic liver disease. The Journal of Clinical Endocrinology and Metabolism, 59(1), 133–138. [DOI:10.1210/jcem-59-1-133]
Valle Alvarez, D. C. (2011). Efecto de una Dosis de 50 mg de Enantato de Noretisterona y 5 mg de Valerato de Estradiol en los Niveles de Testosterona Total en Hombres Mexicanos Sanos. [Effect of a Dose of 50 mg of Norethisterone Enanthate and 5 mg of Estradiol Valerate on Total Testosterone Levels in Healthy Mexican Men.] (Masters thesis, National Polytechnic Institute of Mexico.) [Google Scholar] [URL] [PDF] [Translation]
Varangot, J., & Cedard, L. (1957). Modifications des Œstrogènes Sanguins Après Administration Intramusculaire de Benzoate d’Œstradiol. [Changes in Serum Estrogens After Intramuscular Administration of Estradiol Benzoate.] Comptes Rendus des Séances de la Société de Biologie et de ses Filiales, 151(10), 1707–1712. [Google Scholar 1] [Google Scholar 2] [PubMed] [PDF] [Translation]
Vermeulen, A. (1977). Transport and Distribution of Androgens at Different Ages. In Martini, L., & Motta, M. (Eds.). Androgens and Antiandrogens (pp. 53–65). New York: Raven Press. [Google Scholar] [Google Books] [OpenLibrary] [WorldCat] [Archive.org] [Excerpt]
Vhora, I., Bardoliwala, D., Ranamalla, S. R., & Javia, A. (2019). Parenteral controlled and prolonged drug delivery systems: therapeutic needs and formulation strategies. In Misra A., & Shahiwala, A. (Eds.). Novel Drug Delivery Technologies (pp. 183–260). Singapore: Springer. [DOI:10.1007/978-981-13-3642-3_7]
Vizziello, G., D’Amato, G., Trentadue, R., & Fanizza, G. (1993). Studio dinamico del blocco ipofisario indotto dalla triptorelina, mediante test all’estradiolo benzoato. [Estradiol benzoate test in the study of pituitary block induced by triptorelin.] Minerva Ginecologica, 45(4), 185–189. [Google Scholar] [PubMed] [PDF] [Translation]
Wagner, J. G. (1993). Pharmacokinetics for the Pharmaceutical Scientist. Lancaster/Basel: Technomic. [DOI:10.1201/9780203743652] [Google Books]
Weiss, G., Nachtigall, L. E., & Ganguly, M. (1976). Induction of an LH surge with estradiol benzoate. A clinical test of pituitary-hypothalamic axis competence. Obstetrics and Gynecology, 47(4), 415–418. [URL]
White, M. C., Rosenstock, J., Anapliotou, M., Mashiter, K., & Joplin, G. F. (1981). Heterogeneity of prolactin responses to oestradiol benzoate in women with prolactinomas. The Lancet, 317(8235), 1394–1396. [DOI:10.1016/S0140-6736(81)92571-X]
Wiemeyer, J. C., Fernandez, M., Moguilevsky, J. A., & Sagasta, C. L. (1986). Pharmacokinetic Studies of Estradiol Enantate in Menopausic Women. Arzneimittel-Forschung, 36(11), 1674–1677. [Google Scholar] [PubMed] [PDF]
Wiemeyer, J. C., Fernandez, M., Sagasta, C. L., & Moguilevsky, J. A. (1987). Estudos farmacocinéticos do enantato de estradiol em mulheres na menopausa. [Pharmacokinetic studies of estradiol enantate in menopausic women.] Jornal Brasileiro de Ginecologia, 97(9), 497–501. [Google Scholar] [LILACS] [PDF]
Yan, J., Pan, J., Chang, Y., & Kang, J. (1987). The effect of monthly injectable contraceptive megestrol acetate compound on pituitary-ovarian function. 上海第二医科大学学报(英文版) / Journal of Shanghai Second Medical University / Medical Bulletin of Shanghai Jiaotong University, 1(2), 7–12. [Google Scholar] [CNKI] [PDF]
Yáñez, J. A., Remsberg, C. M., Sayre, C. L., Forrest, M. L., & Davies, N. M. (2011). Flip-flop pharmacokinetics–delivering a reversal of disposition: challenges and opportunities during drug development. Therapeutic Delivery, 2(5), 643–672. [DOI:10.4155/tde.11.19]
Zhang, Y., Huo, M., Zhou, J., & Xie, S. (2010). PKSolver: An add-in program for pharmacokinetic and pharmacodynamic data analysis in Microsoft Excel. Computer Methods and Programs in Biomedicine, 99(3), 306–314. [DOI:10.1016/j.cmpb.2010.01.007]
Zhou, X. F., Shao, Q. X., Han, X. J., Weng, L. J., & Sang, G. W. (1998). Pharmacokinetics of medroxyprogesterone acetate after single and multiple injection of Cyclofem® in Chinese women. Contraception, 57(6), 405–411. [DOI:10.1016/S0010-7824(98)00048-1]
\ No newline at end of file
+An Informal Meta-Analysis of Estradiol Curves with Injectable Estradiol Preparations - Transfeminine Science
An Informal Meta-Analysis of Estradiol Curves with Injectable Estradiol Preparations
By Aly | First published July 16, 2021 | Last modified May 8, 2025
Abstract / TL;DR
Injectable estradiol preparations such as estradiol valerate and estradiol cypionate in oil are frequently used as estrogens in transfeminine hormone therapy. However, there is little characterization of these preparations in transfeminine people and dosing recommendations by transgender health guidelines appear to be based on expert opinion rather than on clinical data. To help shed light on the properties of injectable estradiol and to better inform dosing considerations in transfeminine people, an informal meta-analysis of available clinical data on estradiol concentration–time curves with major injectable estradiol formulations was conducted. The included preparations were injectable estradiol benzoate in oil, estradiol valerate in oil, estradiol cypionate both in oil and as a suspension, estradiol enanthate in oil, estradiol undecylate in oil, and polyestradiol phosphate. The literature was searched for clinical concentration–time data with these injectable estradiol esters and these data were collected and analyzed. Meta-analysis consisted of data for each injectable estradiol preparation being processed and fit with pharmacokinetic models. Selected pharmacokinetic parameters were additionally determined and reported. The results of this work were discussed with regard to characteristics of injectable estradiol preparations like curve shapes, durations, estrogenic exposure, and variability between people and studies. Recommendations for injectable estradiol preparations by transgender health guidelines were also explored in light of the present results. Current guidelines recommend doses of these preparations that appear to be highly excessive with injection intervals that are too widely spaced. Based on the findings of the present meta-analysis, recommendations by guidelines should be reassessed. Finally, the fitted curves in this work were incorporated into an interactive web-based injectable estradiol simulator intended for use by transfeminine people and their medical providers to help guide therapeutic decisions.
Introduction
Estradiol is the main estrogen used in transfeminine hormone therapy and is available in a variety of different forms for use by different routes of administration. The most commonly employed forms are oral, sublingual, transdermal, and injectable preparations. Injectable estradiol preparations have been discontinued in many countries and hence are unavailable for use in transfeminine hormone therapy in many parts of the world, for instance in most of Europe (Glintborg et al., 2021). However, they are still used by many transfeminine people particularly in the United States and in the do-it-yourself (DIY) community. The most commonly used forms include estradiol valerate, estradiol cypionate, and estradiol enanthate all in oil. Injectable estradiol preparations have certain advantages over other estradiol forms that make them a popular choice for use in transfeminine hormone therapy. These include often lower cost, capacity to easily achieve higher estradiol levels that can be useful for testosterone suppression, less frequent administration, and theoretically reduced health risks relative to oral estradiol at equivalent doses due to the lack of the first pass with this route (Aly, 2020). The higher estradiol levels with injections are particularly useful for estradiol monotherapy, in which an antiandrogen is not used.
Clinically used injectable estradiol preparations are formulated not as estradiol but as estradiol esters. When injected into muscle or fat in oil solutions or crystalline aqueous suspensions, these estradiol esters form depots at the injection site from which they are slowly released. Subsequent to release, estradiol esters are rapidly metabolized into estradiol and hence act as prodrugs. When estradiol itself is given by intramuscular injection in an aqueous solution or oil solution, it is rapidly absorbed and has a very short duration. Due to having lipophilic esters, most clinically used injectable estradiol esters are more fat-soluble than estradiol (as measured by oil–water partition coefficient (P)) (Table). When these esters are administered as oil solutions by intramuscular or subcutaneous injection, their increased lipophilicity causes them to be released from the injection-site depot more slowly than estradiol and to therefore have longer durations. In the case of fatty acid esters, the longer the chain length of the ester—as in e.g. estradiol valerate (5 carbons) vs. estradiol enanthate (7 carbons) vs. estradiol undecylate (10 carbons)—the greater the fat solubility, the slower the rate of release from the depot, and the longer the time to peak levels and duration (Edkins, 1959; Sinkula, 1978; Chien, 1981; Kuhl, 2005; Kalicharan, 2017; Vhora et al., 2019). The durations of both injectable oil solutions and aqueous suspensions depend on the ester and its particular physicochemical properties, but the characteristics of these preparations are different and they work in distinct ways to produce their depot effects (Enever et al., 1983; Aly, 2019). The durations of oil solutions are dependent on the lipophilicity of the ester as well as oil vehicle, whereas the durations of aqueous suspensions depend on the properties of the ester crystal lattice as well as crystal sizes (Chien, 1981; Enever et al., 1983; Aly, 2019). The polymeric estradiol ester polyestradiol phosphate is more hydrophilic (water-soluble) than estradiol and works differently than other injectable estradiol preparations. Ιt is composed of many estradiol molecules linked together via phosphate esters (on average 13 molecules of estradiol per one molecule of polyestradiol phosphate) and has a prolonged duration due to slow cleavage into estradiol following injection. Estradiol esters are able to substantially prolong the duration of estradiol when used as injectables and these preparations have durations ranging from days to months depending on the ester and how it is formulated (Table).
In order to aid understanding of concentration–time profiles with injectable estradiol preparations, I’ve developed an interactive web-based injectable estradiol simulator for transfeminine people and their medical providers. During work on this simulator, it became apparent that there is substantial variability in estradiol levels and curve shapes between different studies even with the same injectable estradiol ester. The injectable estradiol simulator was originally designed to simulate curves from only a single well-known pharmacokinetic study that directly compared estradiol benzoate, estradiol valerate, and estradiol cypionate in oil (Oriowo et al., 1980 [Graph]). However, due to the considerable differences in estradiol levels and curves across studies, it was decided that relying on only one study for such a project would be untenable. Instead, for the simulations to be reasonably accurate to the available data, many studies would need to be incorporated. Including additional studies would also allow for inclusion of other injectable estradiol esters in the simulator. As a result, the present work—an informal meta-analysis of estradiol curves with injectable estradiol formulations—was conducted for the simulator project.
Methods
A literature search was performed to identify studies reporting clinical estradiol concentration–time data with major injectable estradiol formulations (Table 1). All of these preparations have been used in transfeminine hormone therapy at one time or another in different parts of the world, although only estradiol valerate in oil and estradiol cypionate in oil are widely used today. Some of the injectable preparations included have notably been discontinued. Acceptable data for the search included mean and individual estradiol concentration data and Cmax estradiol levels (mean peak estradiol levels of individual subjects at time Tmax). Databases like PubMed, Google Scholar, and WorldCat were searched using relevant keywords (e.g., estradiol ester names and variations thereof as well as major brand names). Publications with relevant information were catalogued for data collection. Only single-dose data and multi-dose data that allowed estradiol levels to return to baseline between doses (as in e.g. repeated once-monthly combined injectable contraceptives) were included. Studies were included regardless of the hypothalamic–pituitary–gonadal axis (HPG axis) status of the participants. The study selection criteria aimed to maximize data inclusion due to scarcity of data for several preparations. If however there were many studies for a specific preparation, studies with only 1 or 2 subjects were generally skipped due to the limited additional value that they would provide. When data were in figures in papers—as was generally the case—they were extracted from the graphs using WebPlotDigitizer.
Table 1: Major injectable estradiol formulations (ordered roughly from shortest- to longest-acting):
Following their collection, data were processed, aggregated, and modeled. Data were adjusted for endogenous estradiol production and were normalized by dose. Adjustment for endogenous estradiol production was generally done via subtraction of baseline estradiol levels. In a number of cases however, subtraction of trough estradiol levels or of estradiol levels from a control group was required instead. Data were also weighted by sample size. In a handful of instances, certain missing information (e.g., time to peak levels, baseline levels, subject body weights) was filled in with reasonable assumptions to help maximize data inclusion. Data were processed in the form of mean estradiol curve data rather than individual-subject data (except for rare n=1 studies). The combined processed data from all studies for each injectable estradiol preparation were fit via least squares regression to one-, two-, and three-compartmentpharmacokinetic models with first-order absorption and elimination that were obtained from the literature and other sources (e.g., Colburn, 1981; Wagner, 1993; Fisher & Shafer, 2007; Lixoft, 2008; Abuhelwa, Foster, & Upton, 2015; Certara, 2020). These models fit most curves from individual studies very well. Fitting the combined curve fits of all individual studies (as opposed to fitting all of the combined processed data directly) was additionally evaluated for each injectable estradiol preparation, and if it was feasible for the preparation and allowed for better fitting results, was employed instead. Fitting directly to the combined processed data has the effect of weighting individual studies by quantity of time points, whereas fitting the combined curve fits of studies eliminates this. The Akaike information criterion (AIC) was used to help guide model selection for fitting of the preparations. Curve fitting was performed using the Python library Lmfit with the Levenberg–Marquardt algorithm. Cmax concentrations are a different form of data than mean curve estradiol concentration–time data, and for this reason, were not included in the fitting unless data were very limited for a given injectable estradiol preparation. Outlying data were also excluded from fitting in a number of instances and this allowed for improved curve fits with more uniform area-under-the-curve levels. The main criterion used for excluding curves was fit area-under-the-curve levels that deviated considerably from what was typical for the injectable estradiol preparations (generally less than about 50% of the average or greater than about 150% of the average).
A selection of pharmacokinetic parameters were calculated for each injectable estradiol preparation using the single-dose fit curves and compartmental pharmacokinetic analyses. These parameters included maximal or peak concentrations of estradiol after a single dose scaled to 5 mg (Cmax), time to maximal concentrations of estradiol after a single dose (Tmax), total area-under-the-curve concentrations of estradiol after a single dose (AUC0–∞), terminal elimination half-life after a single dose (t1/2), and the terminal 90% life after a single dose (t90%) (calculated as t1/2 × 3.322). In addition, selected pharmacokinetic parameters were calculated for simulated repeated administration of each injectable preparation at steady state with a dose and dose interval of 5 mg once every 7 days using the single-dose fit curves and compartmental pharmacokinetic analyses. These parameters included time to peak concentrations of estradiol (Tmax), peak and trough concentrations of estradiol (Cmax and Cmin, respectively), peak–trough difference (PTD; Cmax – Cmin), peak–trough ratio (PTR; Cmax ÷ Cmin), and integratedmean concentrations of estradiol (Cavg). Simulation of repeated administration was performed by stacking estradiol levels for multiple injections. Cmax and Tmax were defined and calculated in general as peak estradiol level and time to peak level of the fit mean curve as opposed to the mean peak level and mean time to peak level of individual subjects. This is because the latter would not be possible to compute as most studies reported only estradiol mean curve data. Pharmacokinetic parameters were calculated using relevant pharmacokinetic equations and, as a sanity check, were compared against those computed by PKSolver, a Microsoft Excel pharmacokinetics add-in program (Zhang et al., 2010).
Results
The figures in the subsequent sections show the original data from studies adjusted for endogenous estradiol levels and normalized to a common dose as well as the curve fits to the data (or alternatively the curve fits of the fits of the data depending on the preparation) for the included injectable estradiol preparations. Estradiol benzoate, estradiol cypionate in oil, and estradiol cypionate suspension were fit to the fits of all individual studies for these preparations, whereas estradiol enanthate, estradiol undecylate, and polyestradiol phosphate were fit directly to the combined processed data for these esters. In the case of estradiol valerate, the two fitting approaches gave nearly identical curves, and so fitting the combined processed original data was done for simplicity for this preparation. Cmax studies were excluded in the fitting for all preparations except estradiol enanthate, for which available estradiol concentration–time data were otherwise very limited. The data for the injectable estradiol preparations were generally fit best by a three-compartment pharmacokinetic model (Desmos). As a result, and for consistency, this model was used in the fitting of all preparations.
Estradiol Benzoate
Injectable estradiol benzoate has been extensively used in the past in scientific research, most notably in studies elucidating the function and dynamics of the HPG axis. One such use of estradiol benzoate has been the estrogen provocation test, a diagnostic test of HPG axis function. Due to its use in research, substantial estradiol concentration–time data with injectable estradiol benzoate exists. A total of 26 publications and concentration–time data for 355 individual injections were identified (Table 2).
Table 2: Studies of injectable estradiol benzoate (Spreadsheet; Plotly):
a Total number of injections, not total number of subjects.
A number of studies were excluded from fitting due to much higher or lower area-under-the-curve levels than average. A couple of studies were omitted from the meta-analysis as they only reported total estrogen levels rather than estradiol levels with estradiol benzoate (Akande, 1974; Weiss, Nachtigall, & Ganguly, 1976). Two studies were omitted due partly to being very old and using very early and inaccurate blood tests (Varangot & Cedard, 1957; Ittrich & Pots, 1965 [Graph]). The processed original data and fit of fits curve for estradiol benzoate are shown in Figure 1.
Figure 1: Published estradiol concentration–time curves and fit of fit curves (thick black or white line) with a single intramuscular injection of estradiol benzoate in oil solution over a period of 7 days. Each curve was adjusted for endogenous estradiol levels, normalized to a dose of 5 mg, and fit with a compartmental pharmacokinetic model. Following this, the combined fit curves of the individual studies were fit using the same pharmacokinetic model. The original data from the studies for estradiol benzoate are also provided elsewhere (Spreadsheet; Plotly).
Estradiol Valerate
Studies with curve data on injectable estradiol valerate come from its use in menopausal hormone therapy and other therapeutic indications for estrogens, its use in combined injectable contraceptives, and use in scientific research. A total of 28 publications and concentration–time data for 309 individual injections were identified for estradiol valerate (Table 3).
Table 3: Studies of injectable estradiol valerate (Spreadsheet; Plotly):
Study
na
Subjects
Dose
Reference(s)
S7175
12
Premenopausal women with menstrual migraine (n=10) and amenorrheic/postmenopausal women with history of menstrual migraine (n=2)
Normally cycling transmasculine people not on hormone therapy (n=31), transfeminine people not on hormone therapy (n=14), and gonadally intact transfeminine people on oral estrogen therapy (n=9)
a Total number of injections, not total number of subjects.
A few of these studies were excluded from fitting due generally to much higher or lower area-under-the-curve levels than average or due to being Cmax data. One study was omitted as it only reported estrone levels rather than estradiol levels (Ibrahim, 1996). Another study was not included due to being in pregnant women with concomitant pregnancy termination (Garner & Armstrong, 1977). One last study was omitted due partly to being very old and using very early and inaccurate blood tests (Ittrich & Pots, 1965 [Graph]). The processed original data and fit curve for estradiol valerate are shown in Figure 2.
Figure 2: Published estradiol concentration–time curves and fit curve (thick black or white line) with a single intramuscular injection of estradiol valerate in oil solution over a period of 30 days. Curves were adjusted for endogenous estradiol levels, normalized to a dose of 10 mg, and fit with a compartmental pharmacokinetic model. Fitting of the combined fits of individual studies for this preparation was explored but gave a nearly identical overall curve, so the overall fit curve for the combined processed original data was used for simplicity for this preparation. The original data from the studies for estradiol valerate are also provided elsewhere (Spreadsheet; Plotly).
Estradiol Cypionate Oil
Estradiol cypionate in oil is used in menopausal hormone therapy and for other estrogen indications. However, its use has been more limited relative to other injectable estradiol preparations, like estradiol valerate. Only a handful of studies with relevant data were identified for estradiol cypionate in oil. This included 4 publications and estradiol concentration–time data for 49 individual injections (Table 4).
Table 4: Studies of injectable estradiol cypionate in oil (Spreadsheet; Plotly):
a Total number of injections, not total number of subjects.
No curves were excluded from fitting in the case of this preparation. The processed original data and fit of fit curves for estradiol cypionate in oil are shown in Figure 3.
Figure 3: Published estradiol concentration–time curves and fit of fit curves (thick black or white line) with a single intramuscular injection of estradiol cypionate in oil solution over a period of 30 days. Each curve was adjusted for endogenous estradiol levels, normalized to a dose of 5 mg, and fit with a compartmental pharmacokinetic model. Following this, the combined fit curves of the individual studies were fit using the same pharmacokinetic model. The original data from the studies for estradiol cypionate in oil are also provided elsewhere (Spreadsheet; Plotly).
Estradiol Cypionate Suspension
Estradiol cypionate suspension has been used exclusively in combined injectable contraceptives. For this reason, many relatively high quality pharmacokinetic studies with this injectable preparation have been conducted. A total of 9 publications and estradiol concentration–time data for 131 individual injections were identified for estradiol cypionate suspension (Table 5).
Table 5: Studies of injectable estradiol cypionate suspension (Spreadsheet; Plotly):
a Total number of injections, not total number of subjects. b By subcutaneous injection rather than intramuscular injection.
One of these studies used subcutaneous injection instead of the usual intramuscular injection but the resulting curve was very similar to the curve for intramuscular injection in the same study (Sierra-Ramírez et al., 2011 [Graph]). Several Cmax studies were excluded from fitting for this preparation. One pharmacokinetic study only measured estradiol cypionate levels rather than estradiol levels and hence was not included (Martins et al., 2019 [Graph]). The processed original data and fit of fit curves for estradiol cypionate suspension are shown in Figure 4.
Figure 4: Published estradiol concentration–time curves and fit of fits curve (thick black or white line) with a single intramuscular (or in one case subcutaneous) injection of a microcrystalline aqueous suspension of estradiol cypionate over a period of 30 days. Each curve was adjusted for endogenous estradiol levels, normalized to a dose of 5 mg, and fit with a compartmental pharmacokinetic model. Following this, the combined fit curves of the individual studies were fit using the same pharmacokinetic model. The original data from the studies for estradiol cypionate suspension are also provided elsewhere (Spreadsheet; Plotly).
Estradiol Enanthate
Estradiol enanthate has been used exclusively in combined injectable contraceptives. Several pharmacokinetic studies have been conducted with it because of this. A total of 7 publications and concentration–time data for 270 individual injections were identified for estradiol enanthate (Table 6).
Table 6: Studies of injectable estradiol enanthate (Spreadsheet; Plotly):
a Total number of injections, not total number of subjects.
Of the available data, 216 of the injections were from a single study and mainly included only Cmax levels. Wiemeyer et al. (1986) was excluded from fitting due to having unusually high area-under-the-curve levels with a small sample size (n=3). Because of the scarcity of estradiol concentration–time data available for estradiol enanthate, Cmax studies were included in the fitting for this preparation. The processed original data and fit curve for estradiol enanthate are shown in Figure 5.
Figure 5: Published estradiol concentration–time curves and fit curve (thick black or white line) with a single intramuscular injection of estradiol enanthate in oil solution over a period of 30 days. Curves were adjusted for endogenous estradiol levels, normalized to a dose of 10 mg, and fit with a compartmental pharmacokinetic model. The original data from the studies for estradiol enanthate are also provided elsewhere (Spreadsheet; Plotly).
Estradiol Undecylate
Estradiol undecylate was formerly used in the treatment of prostate cancer and in menopausal hormone therapy as well as for other estrogen therapeutic indications. However, it was discontinued many years ago and is no longer used today. Nonetheless, estradiol undecylate is of significant historical interest as an injectable estradiol preparation. A total of 4 publications and estradiol concentration–time data for 7 individual injections were identified for estradiol undecylate (Table 7).
Table 7: Studies of injectable estradiol undecylate (Spreadsheet; Plotly):
a Total number of injections, not total number of subjects.
Unfortunately, the identified data were of very low quality, with small sample sizes and considerable variations in estradiol levels. Moreover, estradiol undecylate is a very long-acting injectable estradiol ester with a duration measured in months, and the follow up in these studies only went to about 2 weeks post-injection. For these reasons, it was not possible to fit the data for estradiol undecylate in a reasonably accurate way—as suggested by area-under-the-curve estradiol levels that were only around one-third those of the other non-polymeric injectable estradiol esters. Limited multi-dose hormone concentration–time data also exist for estradiol undecylate, but these data could not be incorporated (Jacobi & Altwein, 1979 [Graph]; Jacobi et al., 1980 [Graph]; Derra, 1981 [Graph]). The processed original data and fit curve for estradiol undecylate are shown in Figure 6.
Figure 6: Published estradiol concentration–time curves and fit curve (thick black or white line) with a single intramuscular injection of estradiol undecylate in oil solution over a period of 90 days. Curves were adjusted for endogenous estradiol levels, normalized to a dose of 50 mg, and fit with a compartmental pharmacokinetic model. The original data from the studies for estradiol undecylate are also provided elsewhere (Spreadsheet; Plotly).
Polyestradiol Phosphate
Polyestradiol phosphate has been used primarily in the treatment of prostate cancer but has also been used for estrogen therapeutic indications like treatment of breast cancer and menopausal hormone therapy. While this injectable estradiol preparation has been used widely in the past, it appears to have recently been discontinued. All of the identified studies with estradiol concentration–time data on polyestradiol phosphate were in men with prostate cancer. A total of 11 publications and concentration–time data for 114 individual injections were identified for polyestradiol phosphate (Table 8).
Table 8: Studies of injectable polyestradiol phosphate (Spreadsheet; Plotly):
a Total number of injections, not total number of subjects.
A few older and strongly outlying studies were excluded from the fitting. The processed original data and fit curve for polyestradiol phosphate are shown in Figure 7.
Figure 7: Published estradiol concentration–time curves and fit curve (thick black or white line) with a single intramuscular injection of an aqueous solution of polyestradiol phosphate over a period of 90 days. The graph was clipped to maximum estradiol levels of 600 pg/mL (~2,200 pmol/L) for better viewability. Curves were adjusted for endogenous estradiol levels, normalized to a dose of 160 mg, and fit with a compartmental pharmacokinetic model. The original data from the studies for polyestradiol phosphate are also provided elsewhere (Spreadsheet; Plotly).
Other Injectable Estradiol Preparations
A number of clinical studies with estradiol concentration–time data for other injectable estradiol preparations were also identified during literature search:
Estradiol (unesterified) in an “aqueous” preparation (type of aqueous preparation unspecified but probably a microcrystalline aqueous suspension) (Jones et al., 1978 [Graph])
These preparations were not included in the present meta-analysis due to their relative obscurity and the limited data available for them. In addition, there were concerns about fitting the used pharmacokinetic models to the formulations with multiple estradiol components and to the microsphere formulations.
No estradiol concentration–time data were identified for certain other injectable estradiol forms of interest, like unesterified estradiol in aqueous solution, estradiol benzoate as a microcrystalline aqueous suspension (Agofollin Depot; Ovocyclin M), or estradiol benzoate butyrate/dihydroxyprogesterone acetophenide in oil (Redimen, Soluna, Unijab) (another lesser-known combined injectable contraceptive).
All Injectable Estradiol Preparations Together
Figure 8 shows the curve fits for all of the injectable estradiol preparations scaled to a single dose of 5 mg (or equivalent) together in the same figure. The dose for polyestradiol phosphate was scaled to be about 6.5 times higher than the other injectable estradiol preparations in order to make it roughly equivalent to them in terms of total estradiol exposure. This was because polyestradiol phosphate was found to produce much lower area-under-the-curve estradiol levels than the other injectable estradiol preparations (see the Discussion section). Estradiol undecylate was not included in Figure 8 as a decent fit curve could not be obtained for it due to the very limited data available for this preparation.
Figure 8: Curve fits of published estradiol concentration–time data with different injectable estradiol preparations by intramuscular injection scaled to equivalent doses and plotted over a period of 20 days in a single combined graph. Polyestradiol phosphate is scaled to a 6.5-fold higher dose that is roughly equivalent to that for the other esters as it gave total estradiol levels that were around 6 or 7 times lower than the other esters at the same dose. An alternative version of this figure without estradiol benzoate and with the x-axis spanning 30 days is also provided (Graph).
Figure 9 shows simulated curves at steady state for repeated administration of all of the injectable estradiol preparations scaled to a dose of 5 mg (or equivalent) once every 7 days. As with the previous figure, the dose for polyestradiol phosphate was scaled to be about 6.5 times higher than the other injectable estradiol preparations and estradiol undecylate was not included in the figure.
Figure 9: Simulated curves at steady state for repeated administration of different injectable estradiol preparations by intramuscular injection scaled to equivalent doses and plotted over three injection cycles. This simulation was based on the fit curves of the published single-dose estradiol concentration–time data reported in this meta-analysis. Polyestradiol phosphate is scaled to a 6.5-fold higher dose that is roughly equivalent to that for the other esters as it gave total estradiol levels that were around 6 or 7 times lower than the other esters at the same dose. An alternative version of this figure without estradiol benzoate is also provided (Graph).
For more simulated estradiol concentration–time curves with repeated injections of these injectable estradiol preparations, please see the accompanying interactive web simulator.
Selected Pharmacokinetic Parameters
The table below shows selected pharmacokinetic parameters for the fit curves of the included injectable estradiol preparations (Table 9). Estradiol undecylate was not included in the table due to the lack of data needed to achieve a decent curve fit for this preparation and the uncertainty of its parameters.
Table 9: Selected pharmacokinetic parameters for estradiol with injectable estradiol preparations following a single 5 mg dose by intramuscular injection:
Estradiol preparation
Tmax (d)
Cmax (pg/mL)
t1/2 (d)
t90% (d)
AUC0–∞ (pg•d/mL)
Estradiol benzoate in oil
0.65
971
1.2
3.9
2410
Estradiol valerate in oil
2.1
295
3.0
9.9
1886
Estradiol cypionate oil
4.3
155
6.7
22.3
2150
Estradiol cypionate suspension
1.2
241
5.1
16.9
2096
Estradiol enanthate in oil
6.5
160
4.6
15.1
2183
Polyestradiol phosphate a
18.0
34
28.4
94.2
2117
a Scaled instead to a single 32.5 mg injection (6.5 times higher dose than with the other esters).
The table below shows selected pharmacokinetic parameters for simulated curves at steady state with repeated administration of the included injectable estradiol preparations (Table 10). As with the previous table, estradiol undecylate was not included.
Table 10: Selected pharmacokinetic parameters for estradiol with injectable estradiol preparations with simulated repeated administration of 5 mg once every 7 days by intramuscular injection:
Estradiol preparation
Tmax (d)
Cmax (pg/mL)
Cmin (pg/mL)
Peak–trough diff. (pg/mL)
Peak–trough ratio
Cavg (pg/mL)
Estradiol benzoate in oil
0.64
990
29
962
35
344
Estradiol valerate in oil
1.9
384
142
242
2.7
269
Estradiol cypionate oil
3.1
339
262
77
1.3
307
Estradiol cypionate suspension
1.0
404
189
214
2.1
299
Estradiol enanthate in oil
4.0
329
288
41
1.1
312
Polyestradiol phosphate a
3.2
304
299
5
1.0
302
a Scaled instead to repeated injections of 32.5 mg every 7 days (6.5 times higher dose than with the other esters).
Terminal half-life (t1/2) is the time for the concentration of estradiol to decrease by 50% after pseudo-equilibrium of distribution has been reached—not the time required for half of an administered dose of the estradiol ester to be eliminated (Toutain & Bousquet-Mélou, 2004). It is calculated using only the terminal portion of a concentration–time curve, without the absorption or distribution phases influencing it (Toutain & Bousquet-Mélou, 2004). Due to flip–flop kinetics with depot injectables and the very short blood half-life of estradiol (~0.5–2 hours), what is being described by the terminal half-life in the case of depot estradiol injectables is not actually elimination of estradiol from blood but rather is the absorption of estradiol from the injection-site depot (Toutain & Bousquet-Mélou, 2004; Yáñez et al., 2011).
Discussion
Data Quality, Limitations, and Variability Between Studies
The accuracies of the curve fits for the different included injectable estradiol preparations are limited by the available data for these preparations. The quantity and quality of data are variable among these preparations. In some cases, such as with estradiol valerate in oil and estradiol cypionate in suspension, the data are overall quite good. In other instances, such as with estradiol cypionate in oil and estradiol enanthate in oil, the available data are more limited. There was undersampling of certain parts of the concentration–time curve with some preparations, for instance estradiol benzoate in oil (the early curve), estradiol enanthate in oil (much of the curve), and polyestradiol phosphate (the late curve). In the case of estradiol undecylate in oil, the available data for this preparation weren’t adequate to achieve a decent curve fit at all. The fit curves and calculated pharmacokinetic parameters of the included injectable estradiol preparations should be interpreted with the imperfect data in mind. For example, the curve shapes and pharmacokinetic parameters for the different preparations should not be taken as precise determinations in most cases but instead as rough estimates that would no doubt change with more and better data. Indeed, the fits and pharmacokinetic parameters were often noticeably sensitive to the influences of individual studies. Modeling decisions, such as the choice of pharmacokinetic model, or whether to fit directly to the combined processed data versus to the fits of individual studies, also yielded significantly different curve fits as well as calculated pharmacokinetic parameters.
Due to scarcity of data for several injectable estradiol preparations, the study selection criteria maximized data inclusion in order to allow for better curve fits at the risk of including potentially less reliable data. As examples, studies were included regardless of the status of the HPG axis of the participants, and Cmax data were included in the fitting if data were very limited. In the case of HPG axis state, studies with cycling women may result in greater error due to more variable levels of endogenous estradiol. Moreover, acute high levels of estradiol can induce a surge in luteinizing hormone levels after several days in gonadally intact women, and this may cause a delayed bump in estradiol levels (Wiki). One of the more overt instances of this can be seen in a study of estradiol benzoate in such women (Shaw, 1978 [Graph]). Many if not most of the included studies with estradiol benzoate involved women with intact HPG axes, whereas studies of this sort were uncommon with the other preparations. In the case of Cmax data, these data when Cmax corresponds to the mean of individual peaks are a different type of data than the peak of the mean curve of all individuals. Cmax levels can differ in both magnitude and timing compared to the mean curve peak (e.g., Oriowo et al., 1980 [Graph]; Rahimy, Ryan, & Hopkins, 1999). This is because for instance not all individuals peak at the same time and this variability in time to peak normally serves to dilute peak levels for the mean curve when compared to individual maximal concentrations. However, Cmax levels are in any case generally in the vicinity of the mean curve peak. While Cmax levels were excluded in the fitting for most injectable estradiol preparations, they were included in the case of estradiol enanthate. This was because the available mean and individual estradiol curve data were very limited for this specific preparation, and inclusion of Cmax data allowed for improved fitting in spite of its limitations. Lastly, some of the included data was once-monthly multi-dose, and research with once-monthly estradiol enanthate-containing combined injectable contraceptives has found that the time to peak levels may shift with repeated long-term use (Schiavon et al., 1988; Garza-Flores, 1994).
There was considerable variability between studies in terms of estradiol levels and concentration–time curve shapes with the same injectable estradiol preparation. The reasons for the large variability across studies are not fully clear. In any case, there are many potential factors that may contribute to this variability. These include preparation- and injection-related factors like formulation (e.g., oil vehicle, other components and excipients, concentration, particle size), injection volume, site of injection (e.g., buttocks, thigh, upper arm), injection technique (e.g., force of injection—and resulting depot droplet dimensions), and syringe dead space. They additionally include various subject- and research-related variables like differing blood-testing methodology, differing sample characteristics (e.g., age, weight, gender, ethnicity, physical activity, HPG axis state), and sampling error (Sinkula, 1978; Chien, 1981; Minto et al., 1997; Larsen & Larsen, 2009; Larsen et al., 2009; Florence, 2010; Larsen, Thing, & Larsen, 2012; Kalicharan, 2017). Older studies, which used potentially less accurate blood tests and tended to have smaller numbers of subjects, seemed to particularly add to the variability between studies. These studies may represent less reliable data than more recent research with larger sample sizes. The exclusion criteria helped to remove outliers for the different injectable estradiol preparations however. This meta-analysis does not take into account the potential factors underlying the variability between studies. To do so would be difficult, as in many cases information on these variables is not provided in individual studies and research quantifying their precise influences and relative importances is limited.
It is in any case known from other studies that different oil vehicles are absorbed at different rates from the injection site (Svendsen & Aaes‐Jørgensen, 1979; Schultz et al., 1998; Larsen et al., 2001) and can result in different concentration–time curve shapes (Ballard, 1978 [Excerpt]; Knudsen, Hansen, & Larsen, 1985). This is thought to be due to differences in oil lipophilicity and depot release rates. Viscosity of oils has also been hypothesized to potentially influence rate of depot escape (Schug, Donath, & Blume, 2012). However, research so far has not supported this hypothesis (Larsen & Larsen, 2009; Larsen, Thing, & Larsen, 2012). Oil vehicles can vary with injectable estradiol preparations even for the same estradiol ester. For instance, pharmaceutical estradiol valerate is formulated in sesame oil, castor oil, or sunflower oil depending on the preparation (Table). It is notable however that these three oils have similar lipophilicities (Table). On the other hand, homebrewed injectable estradiol preparations used by DIY transfeminine people often employ medium-chain triglyceride (MCT) oil as the oil vehicle. This oil (in the proprietary form of Viscoleo) has notably been found to be much more rapidly absorbed than conventional oils like sesame oil and castor oil in animals (Svendsen & Aaes‐Jørgensen, 1979; Schultz et al., 1998; Larsen et al., 2001). In addition, although based on very limited data, MCT oil has been found to give spikier and shorter-lasting depot injectable curves in humans (Knudsen, Hansen, & Larsen, 1985). As such, injectable estradiol preparations using MCT oil as the vehicle may have differing and less favorable concentration–time curve shapes than pharmaceutical injectable estradiol products. Other excipients, like benzyl alcohol, as well as factors like injection site and volume, have additionally been found to influence pharmacokinetic properties with depot injectables (Minto et al., 1997; Kalicharan, Schot, & Vromans, 2016). Excipients besides oil vehicle also vary by formulation (Table).
An implication of the variability between studies is that there is not a single estradiol concentration–time curve for a given injectable estradiol preparation but rather there are many, with these curves determined by variables such as formulation, dose/administration, and subject characteristics, among others. Hence, the curve fits determined in this meta-analysis represent only an estimation of the most typical and hence likely case, but the true curve for a preparation in a given context may be quite different.
Fitting all studies for a given injectable estradiol preparation individually first, and then fitting the fits of these studies, allowed for improved curve fits relative to directly fitting all of the combined processed original data for the preparation. The latter approach has limitations in that it has the effect of inherently weighting individual studies by quantity of time points (resulting in studies with greater time sampling having greater influence on the fit). Additionally, and more problematically, this approach can lead to distortions in curve shape due to different studies sampling different portions of the curve to differing extents in conjunction with systematic differences in curves between these studies. These are problems that fitting the fits of individual studies instead can solve. However, it is not possible to fit all individual studies, as some studies have limited time sampling and curve characterization which precludes fitting them appropriately. Cmax data are an example of this, which on their own cannot be fit properly. As such, it was not possible to fit the fits of the individual studies for all injectable estradiol preparations. Consequently, the fitting approach in this regard was not the same across esters, with some fit instead directly to the combined processed original data (e.g., estradiol enanthate, polyestradiol phosphate).
In spite of the various limitations of this work, aggregated analysis and modeling with injectable estradiol preparations has not previously been done. This informal meta-analysis provides among the most detailed insight into estradiol levels and curve shapes with these preparations available to date.
Durations and Curve Shapes
The curve shapes of non-polymeric injectable estradiol esters in oil relate strongly to lipophilicity. The more lipophilic the ester, the lower the peak levels and the more protracted the estradiol concentration–time curve. Accordingly, estradiol benzoate, one of the least lipophilic estradiol esters, has one of the spikiest curves and shortest durations, whereas more lipophilic estradiol esters, like estradiol cypionate in oil and estradiol enanthate, have comparatively flatter curves with delayed peaks and longer durations.
Duration of Estradiol Valerate
The estradiol concentration–time curve for injectable estradiol valerate in the well-known Oriowo et al. (1980) [Graph] study is notably spikier and shorter-lasting than the overall curve for estradiol valerate in this meta-analysis. On the other hand, the overall curve for injectable estradiol valerate in this meta-analysis was similar to (and considerably influenced by) the curves from several relatively recent and presumably better-quality studies of this injectable estradiol ester (e.g., Göretzlehner et al., 2002; Valle Alvarez, 2011; Schug, Donath, & Blume, 2012). It’s noteworthy that Oriowo et al. (1980) used a peanut oil-based formulation of estradiol valerate that differed from pharmaceutical injectable estradiol valerate preparations, which generally use sesame oil or castor oil as the carrier (as well as other excipients) (Table). This may have influenced the curve shape of estradiol valerate in Oriowo et al. (1980). The study also had a small sample size relative to the more recent studies (n=9 versus n=17, n=32, and n=24×2, respectively). Based on the newer and overall data, estradiol valerate appears to have a curve that is noticeably flatter and more prolonged than that suggested by Oriowo et al. (1980).
Duration of Estradiol Cypionate in Oil versus Estradiol Enanthate
Available estradiol concentration–time data for injectable estradiol cypionate in oil and estradiol enanthate in oil are more limited than with several of the other injectable estradiol preparations, and no direct comparisons of these two preparations exist at present. Based on some of the available literature on these injectable estradiol esters, most notably discussion by Oriowo et al. (1980) and a review of the pharmacokinetics of combined injectable contraceptives (Garza-Flores, 1994 [Graph]), it seemed that the duration of estradiol enanthate in oil was longer than that of estradiol cypionate in oil. However, this was based on limited research from separate and hence indirectly comparative studies of these esters. The estradiol cypionate in oil data from the relevant Garza-Flores (1994) figure was based on Oriowo et al. (1980) [Graph], and there are reasons to be cautious about relying on these data alone. The main concern is that curve shapes with the same injectable estradiol preparation can vary considerably across studies, as the present meta-analysis has shown. The reasons for this have yet to be fully clarified as already discussed, but among other factors may include varying formulations across studies of the same injectable estradiol ester. It is notable in this regard that Oriowo et al. (1980) used a formulation of estradiol cypionate that differs from conventional pharmaceutical estradiol cypionate in oil preparations—specifically, the study used a peanut oil-based formulation (with few other specifics) rather than the cottonseed oil-based preparation employed in marketed pharmaceutical formulations (Table). The study also had a somewhat small sample size (n=10) and may have had significant sampling error. Hence, single studies, perhaps particularly Oriowo et al. (1980), should be interpreted cautiously.
A small but interesting pharmacokinetic study which directly compared injectable testosterone cypionate (n=6) and testosterone enanthate (n=6) both in oil is relevant to the topic in question. This study found that equivalent doses of these testosterone esters using otherwise identical formulations produced virtually identical testosterone concentration–time curves (Schulte-Beerbühl & Nieschlag, 1980 [Graph]). The findings of this study are consistent with the fact that the lipophilicities of testosterone cypionate and testosterone enanthate (as measured by predicted log P) are very similar when directly compared (e.g., 5.1 vs. 5.11 with ALOGPS, 6.29 vs. 6.11 with ChemAxon logP, and 6.4 vs. 6.3 with XLogP3, respectively (Table). This of course is of importance as lipophilicity is thought to be the key factor determining the release kinetics of oil-based depot injectables (Sinkula, 1978; Shah, 2007; Larsen & Larsen, 2009; Larsen, Thing, & Larsen, 2012; Shahiwala, Mehta, & Momin, 2018). Analogously similar lipophilicities can be seen when comparing estradiol cypionate and estradiol enanthate, which employ the same ester moieties (e.g., predicted log P values of 6.47 vs. 6.45 with ALOGPS and 7.1 vs. 7.0 with XLogP3, respectively) (Table). Hence, on a theoretical level, injectable estradiol cypionate and estradiol enanthate, like injectable testosterone cypionate and testosterone enanthate, might be expected to produce very similar curves—at least provided all other variables, such as formulation, are held constant.
The present meta-analysis found that the overall estradiol curve for estradiol cypionate in oil was significantly less spikey and more prolonged than that observed in Oriowo et al. (1980). It is noteworthy in this regard that all of the other studies included for estradiol cypionate in oil specifically employed pharmaceutical Depo-Estradiol and that the overall curve for this preparation appears to be more consistent with its licensed injection interval for use in menopausal hormone therapy (1–5 mg once every 3–4 weeks) (Depo-Estradiol Label). Moreover, this meta-analysis found that injectable estradiol cypionate in oil and estradiol enanthate in oil had fairly similar and comparably flat and prolonged estradiol concentration–time curves. However, estradiol cypionate in oil appeared to peak earlier than estradiol enanthate, while estradiol enanthate was eliminated more rapidly than estradiol cypionate in oil in the terminal portion of the curve. In any case, the available concentration–time data for these preparations are limited, and the present work is not able to determine whether these estradiol esters have truly differing pharmacokinetic properties, as the apparent differences between the curves for these preparations may simply be due to statistical error. Taken together, estradiol cypionate in oil may have a less spikey and longer-lasting curve than that implied by Oriowo et al. (1980), and estradiol cypionate in oil and estradiol enanthate may have more similar curves than has been previously assumed.
Curve Shape of Estradiol Cypionate Suspension
While estradiol cypionate as an aqueous suspension is a relatively long-lasting injectable estradiol preparation similarly to estradiol cypionate in oil and estradiol enanthate in oil, it seems to differ in the shape of its estradiol concentration–time curve from these preparations. Estradiol cypionate as a suspension has a curve that appears to peak significantly earlier than estradiol cypionate in oil and other longer-acting oil-based injectable estradiol preparations. This might relate to the differing mechanisms of depot action and unique properties of injectable aqueous suspensions (Aly, 2019). In line with this notion, injectable medroxyprogesterone acetate suspension (Depo-Provera) also appears to peak rapidly despite having a very long duration (longer durations tending to be associated with delayed peaks in the case of oil-based depot injectables) (Graphs). Although aqueous suspensions generally last longer than oil solutions as injectables (Enever et al., 1983; Aly, 2019), this is not always the case, and estradiol cypionate suspension interestingly seems to be shorter-acting than estradiol cypionate in oil.
Estradiol Exposure and Potency
The average estradiol levels with the non-polymeric injectable estradiol esters when scaled to a dose and dosing interval of 5 mg every 7 days were around 300 pg/mL (~1,100 pmol/L). For comparison, in premenopausal cisgender women, estradiol production is on average about 200 μg/day (or 6 mg per month/cycle) and mean estradiol levels are around 100 pg/mL (~370 pmol/L) (Aly, 2019). After adjusting for the molecular weight of the ester, the estradiol levels for a given dose of non-polymeric injectable estradiol esters are in fairly close agreement with the estradiol levels for an equal quantity of estradiol produced endogenously by the ovaries in premenopausal cisgender women (very roughly around 1.2 mg estradiol per 7 days for injectable estradiol esters and 1.4 mg estradiol per 7 days for ovarian production to achieve average integrated estradiol levels of around 100 pg/mL). The preceding is in accordance with the fact that injectable estradiol valerate has been reported to have approximately 100% bioavailability (with this being less characterized but likely also the case for the other non-polymeric injectable estradiol esters) (Düsterberg & Nishino, 1982; Seibert & Günzel, 1994).
Although non-polymeric injectable estradiol esters have differing estradiol concentration–time curve shapes, they all appear to achieve fairly similar area-under-the-curve levels of estradiol when compared to one another. This is in accordance with the fact that differences in molecular weight and hence estradiol content with the different estradiol esters are fairly minor (all of the assessed non-polymeric esters range from 62 to 76% of that of estradiol in terms of estradiol content, and all but estradiol undecylate are in the range of 69 to 76%) (Table). The appearance of differences in area-under-the-curve levels of estradiol in the present meta-analysis is probably just due to statistical error, and true differences cannot be established by this meta-analysis. An implication of the similar area-under-the-curve estradiol levels with the different non-polymeric injectable estradiol esters is that these preparations can all be expected to deliver a roughly comparable amount of estradiol for the same dose.
On the other hand, the polymeric ester polyestradiol phosphate appears to produce around 6- to 7-fold lower area-under-the-curve and average estradiol levels than non-polymeric estradiol esters. This suggests that the estradiol in polyestradiol phosphate is not 100% bioavailable, and is supported by the fact that this ester is used clinically at substantially higher dosages than other injectable estradiol esters (40–320 mg/month), even for the same indications such as menopausal hormone therapy and treatment of prostate cancer (Wiki; Estradurin Labels). This does not seem to have been previously described in the literature, and the reasons for it are unknown. It seems possible that polyestradiol phosphate may be partially excreted before it can be cleaved into estradiol and thereby rendered partly inactive, in turn necessitating the use of higher doses to achieve the same estradiol levels and therapeutic effect.
Although two given injectable estradiol preparations may produce equivalent total estradiol levels, this does not necessarily mean that they will always have the same estrogenic potency (i.e., strength of effect at a given dose). It is plausible that spikier estradiol concentration–time curves, like with estradiol benzoate, may have overall lower estrogenic potency than more steady curves, like with estradiol enanthate. This is because estrogen receptors for a given tissue should become saturated at a certain point due to the finite quantity of available receptors in the tissue. As a result, high peak estradiol levels with spikier curves may effectively be “wasted” to varying extents in different tissues. On the other hand, more spikey estradiol curves, due to higher peak estradiol levels, might have greater influence on tissues that require high estradiol levels for effect such as the liver (and by extension on coagulation and associated health risks) (Aly, 2020). However, these possibilities are speculative and theoretical. Although some literature exists that is relevant to this issue (e.g., Parkes, 1937; Bradbury, Long, & Durham, 1953), there is very little research in this area. Consequently, it is not currently possible to take into account time-related variations in estradiol levels or differing estradiol curve shapes when assessing the comparative estrogenic potency between injectable estradiol preparations (or between other estradiol forms/routes). It is also noteworthy that these variations depend on injection interval and may be reduced with shorter injection intervals that maintain steadier estradiol levels, which must also be considered.
Variability Between Individuals
There is substantial variation in total estradiol levels and curve shapes between people with the same injectable estradiol preparation. Indicators of interindividual variability such as standard deviation or 95% range have not been included in this meta-analysis at this time due to the large amount of additional time and work this would require (e.g., additional extraction of error bars from all studies and analysis). In any case, individual studies that were included show this marked interindividual variation (e.g., Oriowo et al., 1980; Derra, 1981 [Graph]; Aedo et al., 1985 [Graphs]; Sang et al., 1987 [Graphs]; Rahimy & Ryan, 1999 [Graph]; Valle Alvarez, 2011 [Graph]; Schug, Donath, & Blume, 2012 [Graphs]). Highly variable estradiol levels are already well-established with oral and transdermal estradiol (Kuhl, 2005; Wiki). Less variability might be expected with non-polymeric injectable estradiol esters since these preparations appear to have approximately complete bioavailability. However, it seems that even with injectable forms of estradiol, the variability between people is still quite substantial. An implication of this is that the appropriate dose and dosing interval of an injectable estradiol formulation for a given person will vary considerably. This emphasizes the importance of blood work to ensure that injectable estradiol preparations are neither overdosed—which can increase health risks such as blood clots (Aly, 2020)—nor underdosed—which may result in suboptimal testosterone suppression and therapeutic efficacy.
Insights for Clinical Guidelines and Dosing Recommendations
Clinical guidelines for transgender health (see also Aly (2020)) provide recommendations on doses and dosing intervals of injectable estradiol valerate in oil and estradiol cypionate in oil (Table 11). Dosing recommendations are not given for other injectable estradiol preparations, which are much less commonly used in transgender medicine. The recommended doses for estradiol valerate and estradiol cypionate vary widely depending on the guidelines, whereas the recommended intervals are consistently once every 1 to 2 weeks. The doses for estradiol valerate range from 2 to 20 mg/week or 5 to 80 mg/2 weeks and the doses for estradiol cypionate range from <1 to 10 mg/week or <2 to 80 mg/2 weeks. For reference, the Endocrine Society guidelines and the University of California, San Francisco (UCSF) guidelines are the most major clinical guidelines for transgender hormone therapy at present (Aly, 2020). The Endocrine Society guidelines recommend 5 to 30 mg/2 weeks or 2 to 10 mg/week for either estradiol valerate or estradiol cypionate (Hembree et al., 2017). Conversely, the UCSF guidelines recommend <20 to 40 mg/2 weeks for estradiol valerate and <2 to 5 mg/2 weeks for estradiol cypionate (with the option to divide dose into weekly injections if cyclical side effects occur) (Deutsch, 2016a).
Table 11: Recommended doses and injection intervals of injectable estradiol preparations (specifically estradiol valerate and estradiol cypionate) in transgender medicine clinical guidelinesa:
a Several other guidelines recommend doses and intervals that appear to be taken directly from the Endocrine Society or UCSF guidelines and thus are not listed here but can be found elsewhere (Aly, 2020).
A number of concerns arise when the doses and intervals of injectable estradiol valerate and estradiol cypionate recommended by the major transgender clinical guidelines are considered in the context of the present informal meta-analysis and when they are compared between guidelines. Based on the present work, dosages of injectable preparations recommended by the major transgender clinical guidelines appear to result in estradiol exposure that is markedly higher than that with the recommended dosages for other routes and forms of estradiol (e.g., oral or transdermal). Whereas a dosage of 5 mg/week of any non-polymeric injectable estradiol ester appears to give average estradiol levels of around 300 pg/mL (~1,100 pmol/L), which are already supraphysiological, doses of injectable estradiol valerate or estradiol cypionate recommended by guidelines are as high as 15 to 20 mg per week. The average estradiol concentrations that would be expected to result from such doses per this meta-analysis (e.g., ~600–1,200 pg/mL or 2,200–4,400 pmol/L at 10–20 mg/week) (Figure 10) would vastly exceed the ranges for estradiol levels in transfeminine people advised by the same guidelines (generally about 50–200 pg/mL or ~180–730 pmol/L) (Table). This is not merely theoretical; for example, a study that used 40 mg/week estradiol valerate by intramuscular injection in cisgender women with estrogen deficiency to produce “pseudopregnancy” reported measured estradiol levels of about 2,500 pg/mL (~9,200 pmol/L) at 3 months and 3,100 pg/mL (~11,400 pmol/L) at 6 months of treatment (Ulrich, Pfeifer, & Lauritzen, 1994). Moreover, highly supraphysiological estradiol levels with guideline-based injectable estradiol doses are not unexpected when normal production of estradiol in premenopausal cisgender women is considered (~1.4 mg per week or 6 mg per month/cycle giving mean estradiol levels of ~100 pg/mL or 370 pmol/L) (Aly, 2019). Clinical safety data on high doses of injectable estradiol esters like estradiol valerate and estradiol cypionate are lacking at present, but excessive estrogenic exposure is known to increase the risk of health complications such as blood clots (Aly, 2020). The very high doses of these preparations that are recommended by guidelines should raise considerable reservations about their safety.
Figure 10: Simulated estradiol levels with injectable estradiol valerate at the doses and interval (5–40 mg/2 weeks) preferentially recommended by current major transgender care guidelines. Steady-state estradiol levels are reached by about the second or third injection with this injection interval and levels do not further accumulate. An alternative version of this figure with half-doses at a once-weekly interval (i.e., 2.5–20 mg/week) is also provided (Graph).
The present author elsewhere has listed doses of injectable estradiol preparations that are roughly comparable in terms of total estradiol exposure to doses for other estradiol forms and routes used in transfeminine people (Aly, 2020). These doses range from about 1 to 6 mg per week for “low dose” to “very high dose” therapy with non-polymeric injectable estradiol esters (Graph). This dose range for injectable estradiol is likely to be more appropriate for use in transfeminine people than current recommendations by many guidelines. Although high estradiol levels can be useful in transfeminine hormone therapy when antiandrogens are not used due to their greater efficacy than physiological levels in terms of testosterone suppression, only modestly supraphysiological estradiol levels (e.g., ~200–300 pg/mL or 730–1,100 pmol/L) appear to be required for strong testosterone suppression (Aly, 2019; Langley et al., 2021; Aly, 2020). In relation to this, doses of injectable estradiol need not be excessive.
Some guidelines, such as the Endocrine Society guidelines, recommend the same doses and intervals for both estradiol valerate and estradiol cypionate, whereas other guidelines, such as the UCSF guidelines, recommend different doses for these two injectable estradiol esters. Concerningly, the doses for estradiol valerate and estradiol cypionate recommended by the UCSF guidelines differ by roughly an order of magnitude (<20 to 40 mg/2 weeks for estradiol valerate and <2 to 5 mg/2 weeks for estradiol cypionate). These estradiol esters appear to produce similar average estradiol levels (e.g., around 300 pg/mL or 1,100 pmol/L at a dosage of 5 mg/week) and have concentration–time curve shapes that are not extremely different, with estradiol cypionate being only somewhat flatter and more prolonged than estradiol valerate. As such, it would appear that similar doses should be appropriate for these esters. This is supported by the fact that the same doses of estradiol valerate and estradiol cypionate are used in combined injectable contraceptives in cisgender women (both 5 mg once per month) and that these doses were carefully determined during an intensive clinical development programme for these preparations (Garza-Flores, 1994; Newton, d’Arcangues, & Hall, 1994; Sang, 1994; Toppozada, 1994). This programme notably included dose-ranging and direct-comparison studies. Based on the present analysis, the current recommendations by the UCSF guidelines may result in marked overdosage in the case of estradiol valerate and potential underdosage in the case of estradiol cypionate.
Transgender health guidelines recommend an injection interval for estradiol valerate and estradiol cypionate in oil of once every 1 to 2 weeks. Although an injection interval of 2 weeks seems technically feasible in the case of both of these preparations, such an interval would appear to result in substantial fluctuations in estradiol levels, with high peak levels and low troughs. This is particularly true in the case of the shorter-acting estradiol valerate (Figures 10, 11). Considering the wide fluctuations and unknown effects of this variability, as well as the fact that testosterone suppression when applicable may depend on sustained higher estradiol levels, it may be advisable that a once-weekly interval be preferentially recommended for these preparations. This would achieve steadier estradiol levels and would reduce potential problems due to high or low estradiol levels (Figure 11). Alternatively, a shorter interval of once every 5 days may be used with estradiol valerate to further reduce the variability in estradiol levels that occurs with this preparation (Figure 11). On the other hand, an injection interval of once every 10 days to 2 weeks may be practical and allowable in the case of the longer-acting estradiol cypionate in oil (as well as estradiol enanthate) (Figure 11)—provided that the injection cycles are well-tolerated and testosterone suppression remains adequate. When selecting different injection intervals, doses should be scaled by the interval to maintain equivalent total estradiol exposure (e.g., 3.5 mg/5 days, 5 mg/7 days, 7 mg/10 days, or 10 mg/14 days for high-dose non-polymeric injectable estradiol esters).
Figure 11: Simulated estradiol levels with a high dosage of injectable estradiol valerate or estradiol cypionate in oil at different injection intervals (doses scaled by interval to be equivalent in total estradiol exposure).
With the preceding concerns about the doses and intervals of injectable estradiol preparations recommended by transgender care guidelines considered, the question of how these recommendations were determined arises. Unfortunately, current guidelines do not generally describe how they arrived at their recommendations nor do they usually cite sources to support them. It is notable that the UCSF guidelines recommend doses and intervals for injectable estradiol preparations that are nearly identical to those advised by Christian Hamburger and Harry Benjamin in the late 1960s in the first medical textbook on transgender people (Hamburger & Benjamin, 1969). These authors recommended a dose of 10–40 mg/2 weeks for estradiol valerate and of 2–5 mg/2 weeks for estradiol cypionate (although Benjamin additionally stated that after 4–8 months, the same doses could be used at a longer injection interval of once every 4 weeks). These recommendations were notably made before estradiol blood tests became practicably available and were prior to the advent of modern pharmacokinetic studies. Hence, the recommendations for at least these guidelines appear to be based mainly on past expert opinion and long-standing historical precedent rather than on pharmacokinetic or clinical data. The same is likely to also be true for most other guidelines. High doses with certain injectable estradiol preparations (namely estradiol valerate) were probably originally employed for the purpose of achieving longer durations and more convenient injection intervals. This was notably prior to the risks of excessive estrogenic exposure like blood clots becoming known, and these doses may simply have never been revised.
Among the surveyed guidelines for transgender hormone therapy, only the UCSF guidelines (Deutsch, 2016b) and the Sherbourne Health/Rainbow Health Ontario guidelines (Bourns, 2019) referenced pharmacokinetic literature in their discussion of injectable estradiol. The specific publications cited by these guidelines were Düsterberg & Nishino (1982), Sierra-Ramírez et al. (2011), and Thurman et al. (2013). Although it is favorable to see guidelines considering published pharmacokinetic data for informing use of these preparations, there are a few concerns about the studies that were cited. Düsterberg & Nishino (1982) in its study of injectable estradiol valerate had a very small sample size (n=2), and this study was excluded as an outlier in the present meta-analysis due to unusually high estradiol levels. The findings of Düsterberg & Nishino (1982) also do not seem to have actually been used to guide dosing recommendations in the case of the UCSF guidelines, since if this were the case, the recommended doses should have been much lower. On the other hand, Bourns (2019) cited the same study and recommended injectable estradiol valerate at doses of 3–4 mg/week or 6–8 mg/2 weeks. These doses are well below those recommended by other transgender care guidelines and appear to be more appropriate for use in transfeminine people in light of the present meta-analysis. Sierra-Ramírez et al. (2011) and Thurman et al. (2013), although better-quality studies than Düsterberg & Nishino (1982), described injectable estradiol cypionate suspension rather than estradiol cypionate in oil. The oil-based version of estradiol cypionate is the form normally used in transfeminine hormone therapy, and there are important differences between these estradiol cypionate preparations such that pharmacokinetic studies for the suspension can’t necessarily be generalized to the oil solution. These preparations do in any case produce similar total estradiol levels however and hence doses should be comparable for them.
This meta-analysis is only informal and unpublished research. Nonetheless, based on the results of this work and the preceding discussion, current dosing recommendations for injectable estradiol preparations by most transgender clinical guidelines appear to be highly excessive and likely unsafe, with injection intervals that may additionally be too widely spaced. Transgender care guidelines should consider reassessing these recommendations, and the transgender medical community should make an effort to better characterize the pharmacokinetics and optimal dosing schemes of injectable estradiol preparations in transfeminine people in the future. Since clinical data on these preparations are scarce and will probably remain so in the near-term, use of published pharmacokinetic data may be further considered for guiding dosing recommendations for injectable estradiol. As identified and catalogued by this meta-analysis, there is a wealth of existing data that could be used to better inform transgender care guidelines in terms of the use of injectable estradiol preparations in transfeminine people.
Interactive Web Simulator
This informal meta-analysis of estradiol concentration–time data with injectable estradiol preparations was conducted for the purpose of deriving accurate and representative estradiol curves for incorporation into a web-based injectable estradiol simulator intended for use by transfeminine people and their clinicians. This web app is able to simulate both single-injection curves and repeated-injection curves with these preparations. An informational page for this simulator can be found at the following location:
There are various possibilities for further work on this project in the future. For example, assessment of interindividual variability for estradiol levels with injectable estradiol preparations could be included in the meta-analysis. As another example, it would be fairly straightforward and valuable to expand the meta-analysis as well as simulator to other hormonal preparations such as injectable testosterone preparations and other estradiol routes and forms like oral estradiol, sublingual estradiol, and estradiol pellets. Pharmacokinetic literature for some of these preparations has already been collected by this author. However, these future possibilities would require much additional time and effort to complete.
Special Thanks
A special thank you to Violet and Lila for their indispensable input and guidance on modeling topics during the work on this project. An additional thanks to Violet for deriving a special three-compartment pharmacokinetic model that was used in this work. Please also check out Violet’s own projects Tilia—an effort to empower trans people with tools to manage their hormonal transitions—and TransKit—a work-in-progress pharmacokinetic simulation library specifically tailored for transgender hormone therapy. Lastly, thank you to all the peer reviewers who carefully reviewed this article prior to it being posted.
Updates
Update 1: WPATH SOC8 Guidelines
In September 2022, the World Professional Association for Transgender Health (WPATH) Standards of Care for the Health of Transgender and Gender Diverse People Version 8 (SOC8) were published and made recommendations on transgender hormone therapy for the first time (Coleman et al., 2022). These guidelines are among the most highly regarded and consulted transgender care guidelines. In terms of the recommended doses of hormonal medications for transgender people, the WPATH SOC8 appear to have largely copied the Endocrine Society’s 2017 guidelines on transgender hormone therapy (Hembree et al., 2017). More specifically, in the case of injectable estradiol preparations for transfeminine people, doses of 5–30 mg/2 weeks or 2–10 mg/week estradiol valerate or estradiol cypionate were recommended. There was no discussion of injectable estradiol in the guidelines besides the preceding doses and intervals being included in a table, and no literature citations were included to support these doses. As described in the present work, these recommendations include doses and intervals that appear to be highly excessive, too widely spaced, and are likely unsafe. As such, major transgender care guidelines unfortunately continue to make uncited recommendations for injectable estradiol that are out of step with insights available from abundant published pharmacokinetic data. These recommendations are likely inadvisable, with the possibility of substantial health risks.
Update 2: Literature Mentions
The following publications in the literature have cited or mentioned Transfeminine Science’s injectable estradiol simulator and/or meta-analysis since the project was published in mid-2021:
Hughes et al. (2022)
Hughes, J. H., Woo, K. H., Keizer, R. J., & Goswami, S. (2022). Clinical Decision Support for Precision Dosing: Opportunities for Enhanced Equity and Inclusion in Health Care. Clinical Pharmacology & Therapeutics, 113(3), 565–574. [DOI:10.1002/cpt.2799]:
Lastly, we recommend that developers of [clinical decision support software (CDSS)] for dosing take an iterative and participatory approach to designing systems. By involving stakeholders in the design process, they will develop solutions that best suit users’ needs and are more likely to be adopted and used correctly. This participatory approach should involve interviews and usability testing with clinicians. Formal usability testing and analysis with real end users can improve the quality and usefulness of a system.88 Though patients themselves are not typically the end users of CDSS, their expertise (especially that of marginalized groups and organized patient advocacy organizations) can also inform CDSS developers. As an example, transgender people have compiled their own resources to understanding dosing regimens in the absence of clear clinical guidelines.89 Developers of CDSS could provide a great deal of value to these patient populations, and improve their software’s utility, by working with them to understand their needs from a dosing tool.
89. Aly, W. An interactive web simulator for estradiol levels with injectable estradiol esters. Transfeminine Science <https://transfemscience.org/articles/injectable-e2-simulator-release/> (2021) Accessed November 1, 2022.
Jaafar et al. (2022)
Jaafar, S., Torres-Leguizamon, M., Duplessy, C., & Stambolis-Ruhstorfer, M. (2022). Hormonothérapie injectable et réduction des risques: pratiques, difficultés, santé des personnes trans en France. [Hormone replacement therapy injections and harm reduction: practices, difficulties, and transgender people’s health in France.] Sante Publique, 34(HS2), 109–122. [Google Scholar] [PubMed] [DOI:10.3917/spub.hs2.0109] [Translated]:
With regard to feminizing [substitutive hormone therapy (HS)], there are no specialty injectables based on estrogens in the French pharmacopoeia. This makes it impossible to set up estrogen monotherapies which require high dosages that are more difficult to obtain with specialties with other galenic forms [5]. Faced with this lack of care, some trans women and transfeminine people obtain estradiol-based injectable solutions on the Internet or through other sources [6]. […]
5. Aly. An informal meta-analysis of estradiol curves with injectable estradiol preparations [Internet]. Transfem Sci. 2021 July 16. [Visited on 29/12/2022]. Online : https://transfemscience.org/articles/injectable-e2-meta-analysis/.
Linet (2023)
Linet, T. (2023). Prise en charge endocrinologique d’une personne trans. [Endocrinological care of a trans person.] In Faucher, P., Hassoun, D., & Linet, T. (Eds.). Santé sexuelle et reproductive des personnes LGBT [Sexual and Reproductive Health of LGBT People] (pp. 109–124). Issy-les-Moulineaux, France: Elsevier Masson. [Google Books] [URL] [WorldCat] [Excerpt] [Translated]:
Choice of estrogen.
Estradiol is generally the most prescribed estrogen. It is given orally or sublingually in transfeminine people with no significant cardiovascular risk factors. For others, the percutaneous form (patches, gel) is recommended.
The starting dose is 2 mg of estradiol orally with a step increase of 2 mg every 2 to 3 months until the optimal dose is reached [1]. For the patches, the initial dosage and the increments are 50 or 100 μg, and for the gel 2.5 g. This means that the optimal dose is generally 6 to 8 mg per day for the oral route, 3 to 4 mg for the sublingual route, and 300 to 400 μg for the patches (see table 11.1).
It may happen in consultation that the person does not wish to use the prescribed estrogens and wishes to continue the self-prescription of injectable estrogens. It is then possible to evaluate with them the most suitable dosage using the Transfem Science Injection Simulator (https://transfemscience.org/misc/injectable-e2-simulator/). Risk prevention related to injections (needles) can be done. Associations can help the person find 25 G needles of 40 mm useful this type of treatment.
Rothman et al. (2024)
Rothman, M. S., Ariel, D., Kelley, C., Hamnvik, O. R., Abramowitz, J., Irwig, M. S., Soe, K., Davidge-Pitts, C., Misakian, A. L., Safer, J. D., & Iwamoto, S. J. (2024). The Use of Injectable Estradiol in Transgender and Gender Diverse Adults: A Scoping Review of Dose and Serum Estradiol Levels. Endocrine Practice, 30(9), 870–878. [DOI:10.1016/j.eprac.2024.05.008]:
In recent years, we have noted trends in our clinical practices with TGD adults requesting injectable estradiol, particularly in the United States. The reasons given can vary; it may be due to ease of weekly or every two weeks administration, fatigue of taking daily oral medications and skin reactions to or cost of transdermal preparations. There have been discussions as to the roles of estrone/estradiol ratios in feminization and whether injectable estradiol might lead to more favorable results, however research has not supported a role for estrone in optimizing feminizing outcomes [13]. There is also a belief that higher levels can be attained with injections and may lead to faster and more complete feminization; however, there is a lack of data in the literature to support these conclusions. Such conversations occurring on reddit.com and even some hormone provider websites, are perhaps related to the historical use of high dose injectable estradiol noted above [14]. However, there is a paucity of data to guide clinicians on what dose, type and at what interval estradiol esters should be injected and when levels should be measured to ensure physiologic range estradiol levels. In fact, recent reports and clinical observations have raised concerns that the dosing suggested in guidelines may result in supraphysiological estradiol levels and that higher doses and levels may put patients at elevated risk of thromboembolic events [15-18]. This scoping review examines the available data on levels achieved with various dosages of estradiol injections in TGD adults. We also report on testosterone suppression, route (i.e., SC vs. IM), and type of estradiol ester as well as timing of blood draw relative to dose, where available.
Acknowledgment
[…] [We] thank Aly from Transfemscience for community representation and correspondence.
Toffoli Ribeiro, C., Gois, Í., da Rosa Borges, M., Ferreira, L. G. A., Brandão Vasco, M., Ferreira, J. G., Maia, T. C., & Dias-da-Silva, M. R. (2024). Assessment of parenteral estradiol and dihydroxyprogesterone use among other feminizing regimens for transgender women: insights on satisfaction with breast development from community-based healthcare services. Annals of Medicine, 56(1), 2406458. [DOI:10.1080/07853890.2024.2406458]:
Utilizing a previously published meta-analysis method of estradiol concentration-time data from publicly available information on cisgender women who had used EEn or EEn/DHPA [17], we reanalyzed and integrated data from various studies. […]
[…] The V3C Fitter and Desmos tools, accessible online at https://alyw234237.github.io/injectable-e2-simulator/v3c-fitter/ and https://www.desmos.com/calculator/ndgvp2avhj?lang=pt-BR respectively, were utilized for fitting the three-compartment pharmacokinetic model. […]
Pharmacokinetics of injectable estradiol enanthate
[…] The boxplot graph (Figure 5) illustrates that the median estradiol levels in trans women using EEn/DHPA fell within this population’s expected average range values (100–200pg/mL).
Figure 5. Meta-analysis of estradiol concentration-time data from cisgender women under EEn alone or EEn/DHPA. Fitted data curves from various studies individually and combined into a single-dose curve over 30 days were generated based on an informal meta-analysis of published estradiol concentration-time data from cisgender women under EEn or EEn/DHPA [17]. […]
References
[17] Aly. 2021. An informal meta-analysis of estradiol curves with injectable estradiol preparations. Transfeminine Sci. https:// transfemscience.org/articles/injectable-e2-meta-analysis/
Update 3: Herndon et al. (2023)
In March 2023, the following study on injectable estradiol in transfeminine people was published online:
Herndon, J. S., Maheshwari, A. K., Nippoldt, T. B., Carlson, S. J., Davidge-Pitts, C. J., & Chang, A. Y. (2023). Comparison of Subcutaneous and Intramuscular Estradiol Regimens as part of Gender-Affirming Hormone Therapy. Endocrine Practice, 29(5), 356–361. [DOI:10.1016/j.eprac.2023.02.006]
The study was a retrospective analysis of individualized injectable estradiol in adult transfeminine people who received hormone therapy at the Mayo Clinic. Doses of injectable estradiol were adjusted by clinical providers based on estradiol levels, testosterone suppression, and feminization goals, and subsequently these clinical data were retrospectively studied by Mayo Clinic researchers. The primary aim of the study was to compare injectable estradiol by intramuscular versus subcutaneous routes. However, other general considerations for injectable estradiol, such as dosing, estradiol levels, testosterone suppression, type of injectable estradiol ester (estradiol valerate vs. estradiol cypionate), and estradiol monotherapy versus concomitant use of antiandrogens, were also assessed. The paper noted that the study was the largest to assess injectable estradiol in transfeminine people to date and was the first to directly compare intramuscular and subcutaneous injectable estradiol routes in transfeminine people.
Injectable estradiol doses were adjusted to achieve estradiol and testosterone levels within therapeutic ranges defined by the Endocrine Society 2017 guidelines (>100 pg/mL [367 pg/mL] for estradiol and <50 ng/dL [<1.7 nmol/L] for testosterone). Estradiol levels were measured exclusively using liquid chromatography–tandem mass spectrometry (LC–MS/MS), while the assay method for measuring testosterone levels was not specified. In terms of when in the injection cycle estradiol levels were measured, the authors stated the following: (1) “Timing of estradiol blood draw in relation to injection was not protocolized” and (2) “In our practice, although estradiol concentrations were generally checked midway through the injection cycle, we were unable to document with certainty the timing of the estradiol lab testing which may have influenced the results and/or the outliers”. Only the most recent blood test for each individual was analyzed, with the results of earlier tests discarded. Doses were analyzed in per-week amounts, regardless of dosing frequency (either once weekly or once every two weeks).
There were a total of 130 transfeminine people on injectable estradiol who were analyzed in the study. Of these individuals, 56 received intramuscular (i.m.) injections and 74 received subcutaneous (s.c.) injections. The median duration of therapy for injectable estradiol was 3.0 years for both routes. The vast majority of people used weekly injections (91.1% for i.m., 98.6% for s.c.), whereas the small remainder (n=6) injected once every 2 weeks. Similarly, the great majority used injectable estradiol valerate (89.3% for i.m., 86.5% for s.c.), while a small subset (n=16) used injectable estradiol cypionate. The authors did not state the injectable vehicles, but they can be confidently assumed to have both been in oil. The treatment-individualized doses per week of injectable estradiol were median 4 mg (interquartile range (IQR) 3–5.15 mg; range 1–8 mg) for the i.m. route and median 3.75 mg (IQR 3–4 mg; range 1–8 mg) for the s.c. route, with the differences in doses between groups being slightly but significantly different (p = 0.005). For the small number of people on two-week injection cycles, the doses for the combined i.m. and s.c. groups were median 8.5 mg (range 6–16 mg) every 2 weeks. Estradiol levels with injectable estradiol were median 189.5 pg/mL (IQR 126.8–252.5 or 122.5–257 pg/mL; range ~33–575 pg/mL] for i.m. and median 196 pg/mL (IQR 125.3–298.5 pg/mL; range ~23–581 pg/mL) for s.c., with the differences between groups not being significantly different (p = 0.70). The percentages of individuals with estradiol levels in target range (>100 pg/mL) were 78.6% for i.m. and 82.4% for s.c. The estradiol doses and levels of individual patients for each route were also provided in the paper (Graph). It can be seen that more individuals clustered into the higher range of doses with i.m. than with s.c. injections.
In the case of estradiol valerate versus estradiol cypionate, dose per week for i.m. with estradiol valerate was median 4 mg (IQR 3–5.45 mg) and with estradiol cypionate was median 4 mg (IQR 2.25–5 mg). In the case of s.c., dose per week with estradiol valerate was median 4 mg (IQR 3–4 mg) and with estradiol cypionate was median 3 mg (IQR 2–3 mg). The doses between estradiol valerate and estradiol cypionate were not significantly different in the case of i.m. (p = 0.51), but were significantly different in the case of s.c. (p = 0.025). Estradiol levels with the two different injectable estradiol esters were not provided.
On multiple regression analysis, injectable estradiol dose was significantly positively associated with estradiol levels (p < 0.001) following adjustment for several variables (injection route, body mass index (BMI), antiandrogen use, gonadectomy status). Each 1 mg per week in dose was associated with estradiol levels that were increased by (estimate ± standard error) 57.42 ± 10.46 pg/mL. No other variable, including notably BMI, was significantly associated with estradiol levels. According to the authors, the dose-dependently higher estradiol levels with injectable estradiol suggested the need to start at lower doses that are gradually increased in conjunction with close monitoring of hormone levels.
Testosterone levels in those with gonads were 11 ng/dL (IQR 0–19.8 ng/dL) for i.m. and 11 ng/dL (0–20 ng/dL) for s.c., with levels not significantly different between groups (p = 0.92). Adequate testosterone suppression (<50 ng/dL) in those with gonads was achieved in 84.6% with i.m. and 86.6% with s.c. In the small subset of individuals on injections every two weeks (n=6), 100% of individuals achieved target estradiol and testosterone levels. A majority of individuals on injectable estradiol in the study concomitantly used an antiandrogen, with this usually being spironolactone or finasteride. In a minority of individuals, injectable estradiol monotherapy, without concomitant use of an antiandrogen, was employed and hormone levels were measured (n=17). In this subgroup, estradiol levels were median 220 pg/mL (IQR 180–264 pg/mL) at a dose per week of median 4 mg (IQR 3–6 mg), with estradiol levels noticeably higher than in the overall group. In terms of hormone levels for those on injectable estradiol monotherapy, 100% achieved therapeutic estradiol levels (>100 pg/mL) and 88.2% achieved target testosterone levels (<50 ng/dL). The authors noted that most individuals on injectable estradiol monotherapy were able to adequately suppress testosterone, but that higher doses and levels of estradiol may be needed for testosterone suppression in this context.
Herndon et al. (2023) noted that existing recommendations for injectable estradiol in transfeminine people suggest doses of 2 to 10 mg per week or 5 to 30 mg every 2 weeks, referencing the Endocrine Society 2017 guidelines (Hembree et al., 2017) and UCSF 2016 guidelines (Deutsch, 2016a). They also noted that the UCSF 2016 guidelines recommended lower doses of estradiol cypionate than estradiol valerate, which they attributed to pharmacokinetic differences between the esters (citing Oriowo et al. (1980) for this claim). However, the authors noted that the differences between estradiol valerate and estradiol cypionate doses they observed were small, and questioned the clinical relevance of the differences. The authors also tactfully critiqued dosing recommendations by existing guidelines, and suggested their own data to guide dosing instead, with the following relevant excerpts:
Prior studies used for development of guidelines for parenteral doses are suboptimal given their small sample sizes or pre-specificized [gender-affirming hormone therapy (GAHT)] protocols with no adjustment of estradiol doses or no information on hormone concentrations achieved. [Discussion of Deutsch, Bhakri, & Kubicek (2015) and Mueller et al. (2011) …]
Overall, the studies used to support the current dosing recommendation guidelines for parenteral estradiol dosing are limited, incomplete with regards to hormone concentrations achieved, and do not provide SC as an available option. The doses of estradiol used in this study (with either SC or IM approach), were successful in achieving serum estradiol concentrations at the cisgender female range. Most importantly, as compared to current available guidelines and consensus statements [1, 2], these doses of estradiol valerate are less than half of what is recommended for both initial and maintenance dosing and achieved suppression of testosterone.
Lower doses of parenteral injections than previously described in clinical practice guidelines achieved therapeutic estradiol concentrations. Our data can serve as a dosing guide for initial and maintenance use of parenteral estradiol, which is different than what has been previously described.
Herndon et al. (2023) concluded that injectable estradiol by both i.m. and s.c. routes is effective in achieving therapeutic estradiol levels in transfeminine people. They noted that there were not meaningful differences between i.m. and s.c. in terms of dose, although i.m. may require slightly higher doses than s.c. to achieve therapeutic estradiol levels. The authors stated that doses of injectable estradiol to achieve therapeutic estradiol levels in transfeminine people were lower than previously recommended by guidelines and other publications. They concluded that clinical use of injectable estradiol in transfeminine people should include discussion of both i.m. and s.c. routes and invidiualization by patient. Finally, they called for more clinical studies on injectable estradiol in transfeminine people to evaluate clinical outcomes, feminization, and additional risks and benefits of this route compared to other routes.
The findings of Herndon et al. (2023) are pleasingly consistent with the results of the present meta-analysis. Based on the findings of this meta-analysis, assuming a linear relationship between dose and estradiol levels, estradiol levels with non-polymeric injectable estradiol esters, like estradiol valerate and estradiol cypionate in oil via intramuscular injection, increase by around 60 pg/mL on average for each 1 mg per week in dose (with Herndon et al. (2023) finding a value of 57 pg/mL per 1 mg using a multiple linear regression model). In relation to this, mean integrated estradiol levels of around 250 pg/mL on average would be expected at a dosage of 4 mg once per week. Accordingly, Herndon et al. (2023) found median estradiol levels of 190 to 196 pg/mL at per-week median doses of 3.75 to 4 mg. Similarly, the present work recommended injectable estradiol doses with non-polymeric esters of 1 to 6 mg per week (to achieve mean integrated estradiol levels of roughly 50–300 pg/mL), which is comparable to the range of about 2 to 6 mg per week used in most transfeminine people in Herndon et al. (2023) (to achieve estradiol levels of at least 100 pg/mL, along with adequate testosterone suppression). Additionally, it was noted in this meta-analysis—based on clinical research in cisgender men with prostate cancer—that only modestly supraphysiological estradiol levels, of no more than approximately 200 to 300 pg/mL, are likely to be needed for strong testosterone suppression in transfeminine people. This has likewise been confirmed with solid clinical data in transfeminine people by Herndon et al. (2023), with 88% of those on injectable estradiol monotherapy having testosterone levels of <50 ng/dL at a median injectable estradiol dose of 4 mg/week and with median estradiol levels of 220 pg/mL. It is the opinion of the present author that Herndon et al. (2023) is a very important and formative study, with clinical implications that go far beyond merely supporting the s.c. use of injectable estradiol. The study represents the first major step in the published literature to correcting the dosing and intervals of injectable estradiol in transgender care guidelines and in transgender health generally. I commend the researchers for their work.
Update 4: Rothman et al. (2024a) and Rothman et al. (2024b)
In February 2024, the following short review on injectable estradiol dosing in transfeminine people by Micol Rothman and colleagues was published online:
Rothman, M. S., Hamnvik, O. P. R., Davidge-Pitts, C., Safer, J. D., Ariel, D., Tangpricha, V., Abramowitz, J., Soe, K., Sarvaideo, J., Kelley, C., Irwig, M. S., & Iwamoto, S. J. (2024). Revisiting Injectable Estrogen Dosing Recommendations for Gender-Affirming Hormone Therapy. Transgender Health, 9(6), 463–465. [DOI:10.1089/trgh.2023.0209]
Here is the abstract of the paper:
Injectable estrogens are options for gender-affirming hormone therapy per guidelines, which suggest intramuscular dosages of 5–30 mg every 2 weeks or 2–10 mg weekly with estradiol cypionate or valerate interchangeably. Data among transgender and gender-diverse patients are limited due to local unavailability and concerns around laboratory assay variability and estradiol (E2) level fluctuation. We note a concerning trend where patients are prescribed high-dose injections based on the guidelines leading to serum E2 levels well above the range recommended in the same guidelines. Our review indicates that 5 mg weekly or lower should be prescribed when initiating injectable estrogens to avoid supraphysiologic E2 levels.
Then, in May 2024, the following longer and more comprehensive review on injectable estradiol dosing in transfeminine people by Rothman and most of the same other academics was published online:
Rothman, M. S., Ariel, D., Kelley, C., Hamnvik, O. R., Abramowitz, J., Irwig, M. S., Soe, K., Davidge-Pitts, C., Misakian, A. L., Safer, J. D., & Iwamoto, S. J. (2024). The Use of Injectable Estradiol in Transgender and Gender Diverse Adults: A Scoping Review of Dose and Serum Estradiol Levels. Endocrine Practice, 30(9), 870–878. [DOI:10.1016/j.eprac.2024.05.008]
Here is the abstract of this paper:
Objective: Feminizing gender-affirming hormone therapy is the mainstay of treatment for many transgender and gender diverse people. Injectable estradiol preparations are recommended by the World Professional Association for Transgender Health Standards of Care 8 and the Endocrine Society guidelines. Many patients prefer this route of administration, but few studies have rigorously assessed optimal dosing or route.
Methods: We performed a scoping review of the available data on estradiol levels achieved with various dosages of estradiol injections in transgender and gender diverse adults on feminizing gender-affirming hormone therapy. We also report on testosterone suppression, route (ie, subcutaneous vs intramuscular), and type of injectable estradiol ester as well as timing of blood draw relative to the most recent dose, where available.
Results: The data we reviewed suggest that the current guidelines, which recommend starting doses 2 to 10 mg weekly or 5 to 30 mg every 2 weeks of estradiol cypionate or valerate, are too high and likely lead to patients having supraphysiologic levels across much of their injection cycle.
Conclusions: The optimal starting dose for injectable estradiol remains unclear and whether it should differ for cypionate and valerate. Based on the data available, we suggest that clinicians start injectable estradiol cypionate or valerate via subcutaneous or intramuscular injections at a dose ≤5 mg weekly and then titrate accordingly to keep levels within guideline-recommended range. Future studies should assess timing of injections and subsequent levels more precisely across the injection cycle and between esters.
This paper notably also cited the present Transfeminine Science article as raising concerns about guideline-based dosing for injectable estradiol and potential health complications from these doses.
Aside from Micol Rothman herself, these reviews were also authored by other well-known experts in transgender health. For instance, two of the coauthors, Joshua Safer and Michael Irwig, were authors for the WPATH SOC8 hormone therapy chapter (WPATH SOC8 Full Contributor List). Additionally, Safer was one of the authors for the Endocrine Society’s transgender hormone therapy guidelines (Hembree et al., 2017). As such, it would appear that transgender medicine has finally started to seriously correct injectable estradiol dosing. This is a very important development. Now, the appropriate dosing and intervals of injectable estradiol will need to be more precisely established and the corrections will need to make their way into updated transgender hormone therapy guidelines and general clinical practice.
A letter to the editor commented on and concorded with Rothman and colleagues’ second literature review:
Patel, K. T., & Tangpricha, V. (2024). Parenteral Estradiol for Transgender Women: Time to adjust the dose. Endocrine Practice, 30(9), 893–894. [DOI:10.1016/j.eprac.2024.07.005]
Update 5: Kariyawasam et al. (2024)
In March 2024, the following study of estradiol levels with different routes of estradiol in transfeminine people, including injectable estradiol, was published:
Kariyawasam, N. M., Ahmad, T., Sarma, S., & Fung, R. (2024). Comparison of Estrone/Estradiol Ratio and Levels in Transfeminine Individuals on Different Routes of Estradiol. Transgender Health, ahead of print. [DOI:10.1089/trgh.2023.0138]
The study stratified injectable estradiol doses into different dosing levels, accounted for timing of blood draws, and compared injectable estradiol to other estradiol routes. The other routes included oral estradiol, sublingual estradiol, and transdermal estradiol. The form of injectable estradiol used was estradiol valerate in dose groups including ≤4 mg/week (“low-dose”), >4 mg/week to ≤8 mg/week (“medium-dose”), and >8 mg/week (“high-dose”). In the study, this injectable estradiol regimen resulted in supraphysiological estradiol levels in the medium- to high-dose groups (>4 mg/week) and dramatically higher estradiol levels than with the other estradiol routes (Data). Median estradiol levels were reported in a subsequent paper as follows: “Figure 2 from the paper shows estradiol levels across the 3 groups. Although exact numbers are not given in this figure, we learned through correspondence with the authors that the low dose injection group [n=8] had a median level of 202.7 ± SD 232.6 pg/mL, the medium group [n=22] 465.2 ± SD 466.3 pg/mL, and the high group [n=3] 574.4 ± SD147.3 pg/mL (converted from SI units)” (Rothman et al., 2024b). Although the sample sizes for the different dose groups were small, this study, along with Herndon et al. (2023), provides some of the best clinical data on estradiol levels with injectable estradiol in transfeminine people that have so far been published.
Update 6: Patel et al. (2024)
In June 2024, the following open-access review discussing injectable estradiol in transfeminine people and calling for updated transgender health guidelines was published:
Patel, R., Korenman, S., Weimer, A., & Grock, S. (2024). A Call for Updates to Hormone Therapy Guidelines for Gender-Diverse Adults Assigned Male at Birth. Cureus, 16(6), e62262. [DOI:10.7759/cureus.62262] [PDF]
The following quote is the relevant excerpt on injectable estradiol from the review:
The current guideline-based dosing recommendations for estradiol vary considerably, which is problematic for clinicians and patients who rely on guidelines to initiate treatment. Most notably, the conversion rates between parenteral estradiol valerate and estradiol cypionate vary drastically between the UCSF Guidelines for the Primary and Gender-Affirming Care of Transgender and Gender Nonbinary People (UCSF Guidelines) and The Endocrine Society Clinical Practice Guidelines for Endocrine Treatment of Gender-Dysphoric/Gender-Incongruent Persons (the Endocrine Society Guidelines). The UCSF Guidelines indicate the conversion between estradiol valerate and cypionate to be as high as a 4:1 ratio [2], while the Endocrine Society Guidelines provide no dosing differentiations [1]. Herndon and colleagues demonstrated that the conversion between estradiol cypionate and estradiol valerate is closer to 1:1 [4]. Further equivalence studies are needed to clarify ideal dosing conversions.
The Endocrine Society Guidelines recommend titrating estradiol to 100-200 pg/mL [1]. The UCSF Guidelines recommend 2-4 mg daily as the starting dose for oral estradiol and 5 mg weekly for parenteral estradiol valerate [2]. The Endocrine Society Guidelines suggest oral estradiol 2-6 mg daily and parenteral estradiol 2- 10 mg weekly [1]. However, Chantrapanichkul et al. found that intramuscular injections of estradiol valerate greater than 5 mg weekly led to mean estradiol concentrations well above 200 pg/mL, while 4-5 mg of oral estradiol daily only led to minimum desired concentrations [5]. Similarly, Herndon et al. found that subcutaneous estradiol at a median dose of 3.75 mg per week led to a median estradiol level of 196 pg/mL [4]. Thus, current guideline-based dosing may lead providers to choose doses of injectable estradiol that would result in supratherapeutic serum estradiol levels. In light of these recent publications, it is clear that guideline-based dosing for estradiol needs updating. In our clinical experience, parenteral estradiol valerate at doses of 2-4 mg weekly typically leads to physiologic estradiol levels. Estradiol cypionate should likely be dosed in a 1:1 ratio with estradiol valerate until future data are obtained.
Lastly, while estradiol valerate and cypionate are only FDA-approved for intramuscular administration, many patients prefer subcutaneous administration. There are small studies that suggest the pharmacokinetics of intramuscular and subcutaneous estradiol are similar [4]. While the UCSF Guidelines comment on the use of subcutaneous estradiol, other guidelines should be updated to include this option for patients [2].
Update 7: Toffoli Ribeiro et al. (2024)
Toffoli Ribeiro, C., Gois, Í., da Rosa Borges, M., Ferreira, L. G. A., Brandão Vasco, M., Ferreira, J. G., Maia, T. C., & Dias-da-Silva, M. R. (2024). Assessment of parenteral estradiol and dihydroxyprogesterone use among other feminizing regimens for transgender women: insights on satisfaction with breast development from community-based healthcare services. Annals of Medicine, 56(1), 2406458. [DOI:10.1080/07853890.2024.2406458]:
This study examines the effects of a commonly used injectable hormone combination, specifically estradiol enanthate with dihydroxyprogesterone acetophenide (EEn/DHPA), […] Our research focused on a retrospective longitudinal study involving a large cohort of transwomen evaluated between 2020 and 2022, comprising 101 participants. We assessed serum levels of estradiol (E2), testosterone (T), luteinizing hormone (LH), and follicle-stimulating hormone (FSH), comparing the EEn/DHPA hormonal regimen with other combined estrogen-progestogen (CEP) therapies. […] Our findings indicated that participants using the EEn/DHPA regimen exhibited significantly higher serum E2 levels (mean: 186 pg/mL ± 32 pg/mL) than those using other therapies (62 ± 7 pg/mL), along with lower FSH levels, but no significant differences in T and LH levels. […] These results suggest that an injectable, low-cost EEn/DHPA administered every three weeks could serve as an alternative feminizing regimen, particularly considering the extensive long-term experience of the local transgender community. Further longitudinal studies on the efficacy of feminizing-body effects and endovascular risks of various parenteral CEP types are warranted to improve primary healthcare provision for transgender persons.
Introduction
Injectable combined estrogens with progestogens (CEP) have long been widely used in Brazil and other Latin American countries, predominantly among ciswomen as an injectable contraceptive and by Brazilian transgender women and travestis as GAHT [8]. Despite the absence of recognition by the Endocrine Society as an alternative hormonal regimen due to concerns regarding thrombogenicity and challenges in routine monitoring through blood testing, the prevalent use of CEP necessitates evaluating its regimen recommendations. This has led our research to delve deeper into understanding CEP regimens, considering the experiences of travestis amidst distinct sociocultural lifestyles and limited access to public endocrinological care services [15,16]. Hence, our objective is to elucidate our observations in monitoring trans individuals utilizing CEP regimens by evaluating hormone levels […] within a cohort of transwomen employing the most common injectable CEP, namely estradiol enanthate with dihydroxyprogesterone acetophenide (EEn/DHPA) and comparing these observations with other GAHT regimens.
Subjects and methods
Estradiol enanthate pharmacokinetics curve
Utilizing a previously published meta-analysis method of estradiol concentration-time data from publicly available information on cisgender women who had used EEn or EEn/DHPA [17], we reanalyzed and integrated data from various studies. A unified single-dose curve for 30 days was created. We employed least squares regression for studies with four or more concentration-time data points (solid lines). We manually adjusted other studies with three data points to fit into a single-dose curve.
Each study’s data were adjusted for baseline estradiol levels or endogenous estradiol production and then normalized by 10 mg. The V3C Fitter and Desmos tools, accessible online at https://alyw234237.github.io/injectable-e2-simulator/v3c-fitter/ and https://www.desmos.com/calculator/ndgvp2avhj?lang=pt-BR respectively, were utilized for fitting the three-compartment pharmacokinetic model. Estradiol levels from transgender women on EEn/DHPA in this study were presented using a box plot graph featuring percentiles at 10, 25, 50, 75, and 90.
Results
Hormonal levels during the follow-up of feminizing regimens
Scatter plot graphs depicted the measurement of sex hormones (Figure 2). Serum estradiol levels in the EEn/ DHPA group (mean: 186.4pg/mL ± 32.8pg/mL) were significantly higher than those in the group using other therapies (62.2±6.9pg/mL) (Figure 2(A)). Within the EEn/DHPA group, serum FSH levels were significantly lower compared to the other group (Others) (Figure 2(B)). However, no significant difference was found between the groups concerning testosterone (Figure 2(C)) and LH (Figure 2(D)) levels.
Pharmacokinetics of injectable estradiol enanthate
Serum estradiol levels in trans women using EEn/DHPA reached the target levels for this population during hormone therapy, a trend not observed in participants using other feminizing hormone therapies (Table 1). The boxplot graph (Figure 5) illustrates that the median estradiol levels in trans women using EEn/DHPA fell within this population’s expected average range values (100–200pg/mL).
Figure 5. Meta-analysis of estradiol concentration-time data from cisgender women under EEn alone or EEn/DHPA. Fitted data curves from various studies individually and combined into a single-dose curve over 30 days were generated based on an informal meta-analysis of published estradiol concentration-time data from cisgender women under EEn or EEn/DHPA [17]. For studies with four or more concentration-time data points (solid lines) and the fit of combined data (thick black line), least squares regression to a three-compartment pharmacokinetic model was employed. A single-dose curve was manually adjusted for studies with three data points (dashed lines). Data from each study were adjusted for endogenous estradiol production via baseline or trough estradiol levels subtraction and normalized by 10mg. The graph illustrates estradiol levels from the transwoman cohort in a boxplot. The shaded area represents the optimal target range for estradiol levels in transwomen under hormone therapy. The boxplot graph displays the percentiles 10, 25, 50, 75, and 90 for estradiol levels of transwomen under EEn/DHPA in this study (N=53).
Discussion
Our study represents a pioneering contribution to the literature by demonstrating that Brazilian trans women undergoing EEn/DHPA therapy achieved estradiol levels comparable to those observed during the follicular phase in cisgender women. […]
Our study further noted that DHPA demonstrates comparable efficacy to cyproterone or other anti-androgens in achieving optimal LH pituitary suppression and reducing testosterone levels. EEn/ DHPA, an affordable injectable contraceptive widely accessible in South American countries, presents a promising avenue for attaining target hormone levels among transfeminine individuals.
Additionally, our investigation, which reviewed pharmacokinetic data, supports the potential implementation of EEn/DHPA in a 21-day regimen to sustain optimal estradiol levels. While alternative medications exist to inhibit testosterone production and action, their availability varies based on regional healthcare provider systems. […]
EEn/DHPA, commonly used as a long-lasting injectable contraceptive [21–23], has found application in feminizing hormone therapy for transfeminine people, notably in travestis in Brazil [7,8,24,25]. […]
In conclusion, our long-term cohort study suggests that administering parenteral estradiol enanthate with dihydroxyprogesterone acetophenide every three weeks could serve as a practical option for feminizing hormone regimens in transgender women. Nonetheless, adopting an individualized approach that takes into account each individual’s goals, response to prior hormone therapies, and medical history is crucial. This personalized approach is central to improving healthcare provision and ensuring optimal outcomes in bodily changes. By continuing to explore and refine hormone therapy regimens, we can better support the health and well-being of transgender individuals on their gender-affirming journey.
References
[17] Aly. 2021. An informal meta-analysis of estradiol curves with injectable estradiol preparations. Transfeminine Sci. https:// transfemscience.org/articles/injectable-e2-meta-analysis/
Update 8: Misakian et al. (2025)
Misakian, A. L., Kelley, C. E., Sullivan, E. A., Chang, J. J., Singh, G., Kokosa, S., Avila, J., Cooper, H., Liang, J. W., Botzheim, B., Quint, M., Jeevananthan, A., Chi, E., Harmer, M., Hiatt, L., Kowalewski, M., Steinberg, B., Tausinga, T., Tanner, H., Ho, T. F., … Ariel, D. (2025). Injectable Estradiol Use in Transgender and Gender-Diverse Individuals throughout the United States. The Journal of Clinical Endocrinology & Metabolism, dgaf015. [DOI:10.1210/clinem/dgaf015]:
Context: Guidelines for use of injectable estradiol esters (valerate [EV] and cypionate [EC]) among transgender and gender-diverse (TGD) individuals designated male at birth vary considerably, with many providers noting supraphysiologic serum estradiol concentrations based on current dosing recommendations.
Objectives: This work aimed to 1. determine the dose of injectable estradiol (subcutaneous [SC] and intramuscular [IM]) needed to reach guideline-recommended estradiol concentrations for TGD adults using EC/EV; 2. describe the relationship between estradiol concentration relative to timing/dose of last estradiol injection and other covariates; and 3. determine dosing differences between IM/SC EV/EC.
Methods: A cross-sectional retrospective study was conducted across 6 US medical centers including TGD adults on same-dose injectable estradiol for more than 75 days, with confirmed timing of estradiol concentration relative to last injection, from January 1, 2019 to December 31, 2023. Descriptive statistics were used to describe patient characteristics and weighted linear mixed models to evaluate relationship between various covariates and estradiol concentration.
Results: Data from 562 patients were included. Among those injecting every 7 days who reached the guideline-recommended estradiol concentration (n = 131, 27.5%), the median estradiol dose was 4.0 mg (interquartile range, 3.0-5.0 mg). Among all patients, the majority reached supraphysiologic estradiol concentrations (>200 pg/mL [>734 pmol/L]) while dose and timing in the injection cycle were significant covariates for the estradiol concentration. There were no significant dosing differences between IM/SC EV/EC.
Conclusion: Injectable estradiol esters effectively reach guideline-recommended estradiol concentrations but at lower doses than previously recommended. Estradiol concentrations are best interpreted relative to timing of last injection. Route of administration and type of ester do not significantly affect estradiol concentrations.
[…]
And a letter to the editor commenting on the paper:
Milano, C., & Harper, J. (2025). Comments on Injectable Estradiol Use in Transgender and Gender-Diverse Individuals in the US. The Journal of Clinical Endocrinology & Metabolism, dgaf134. [DOI:10.1210/clinem/dgaf134]
Update 9: Slack et al. (2025)
Slack, D. J., Di Via Ioschpe, A., Saturno, M., Kihuwa-Mani, S., Amakiri, U. O., Guerra, D., Karim, S., & Safer, J. D. (2025). Examining the Influence of the Route of Administration and Dose of Estradiol on Serum Estradiol and Testosterone Levels in Feminizing Gender-Affirming Hormone Therapy. Endocrine Practice, 31(1), 19–27. [DOI:10.1016/j.eprac.2024.10.002]:
Introduction: […] This study investigates the effect of route of administration (ROA) and dose of estradiol on estradiol (E2) and testosterone (T) levels in transfeminine individuals.
Methods: We conducted a chart review of 573 patients with an active prescription for estradiol for feminizing GAHT and serum hormone levels available.
Results: […] Intramuscular estradiol was associated with lower T and higher E2 compared to oral and transdermal ROAs (P < .001), with many achieving target hormone levels even at low doses.
Conclusions: […] The intramuscular ROA appears to be the most potent delivery of estradiol with impact on serum hormone levels with doses on the low end of guideline-suggested ranges.
[…]
Update 10: Carlson et al. (2025)
Carlson, S. M., Dominguez, C., Jeevananthan, A., & Crowley, M. J. (2025). Follow-Up Estradiol Levels Based on Regimen Formulation With Guideline-Concordant Gender-Affirming Hormone Therapy. Journal of the Endocrine Society, 9(3), bvae205. [DOI:10.1210/jendso/bvae205]:
Context: Endocrine Society guidelines for dosing of feminizing gender-affirming hormone therapy (GAHT) have remained essentially unchanged since 2009. The Endocrine Society recommends periodic monitoring of serum estradiol levels, with the goal of maintaining levels in the premenopausal cisgender female range (100-200 pg/mL). However, it is not clear whether guideline-concordant dosing consistently produces guideline-recommended levels across common estradiol formulation types (oral pills, parenteral injections, transdermal patches).
Objective: All transgender and nonbinary patients receiving estradiol-based GAHT between October 2015 and March 2023 were reviewed at a single center, with the goal of determining the frequency with which guideline-concordant dosing with different estradiol formulations led to guideline-recommended estradiol levels.
Methods: Demographics, GAHT regimen, and estradiol levels were obtained via chart review, and data were analyzed descriptively.
Results: The analytic population included n = 35 individuals, including n = 9 prescribed oral estradiol pills, n = 11 prescribed parenteral injections, and n = 15 prescribed transdermal patches. With guideline-concordant doses of oral estradiol (mean 2.8 mg daily), the mean follow-up level was 168 pg/mL; 32% of follow-up levels were subtherapeutic and 14% were supratherapeutic. With guideline-concordant doses of parenteral estradiol (mean 5.8 mg weekly), the mean midpoint follow-up level was 342 pg/mL; 91% of midpoint follow-up levels were supratherapeutic. With guideline-concordant doses of transdermal estradiol (mean 0.09 mg/day), the mean follow-up level was 81.5 pg/mL; 70% of follow-up levels were subtherapeutic.
Conclusion: Supratherapeutic follow-up estradiol levels were common with guideline-concordant parenteral estradiol doses, as were subtherapeutic follow-up levels with guideline-concordant transdermal doses. These findings may suggest the need for revision of guideline-recommended estradiol doses for these formulations
[…]
Update 11: Kanin et al. (2025)
Kanin, M., Slack, M., Patel, R., Chen, K. T., Jackson, N., Williams, K. C., & Grock, S. (2025). Injectable Estradiol Dosing Regimens in Transgender and Nonbinary Adults Listed as Male at Birth. Journal of the Endocrine Society, bvaf004. [DOI:10.1210/jendso/bvaf004]:
Context: Many transgender and nonbinary (TGNB) individuals assigned male at birth (AMAB) seek hormone therapy to achieve physical and emotional changes. Standard therapy includes estradiol, with or without an antiandrogen. Our clinical observations suggest that currently recommended injectable estradiol dosing may lead to supratherapeutic estradiol levels.
Objective: We sought to evaluate whether lower-than-recommended doses of injectable estradiol were effective in achieving serum estradiol and testosterone goals.
Methods: We conducted a retrospective cohort study to evaluate injectable estradiol dosing in treatment-naive AMAB individuals initiating hormone therapy. Data from a single provider at an academic center from January 2017 to March 2023 were analyzed. A total of 29 patients were eligible for inclusion. The primary variables of estradiol dosage, serum estradiol, and testosterone levels were analyzed over 15 months.
Results: The average estradiol dose decreased from 4.3 to 3.7 mg weekly (P < .001) during the study period with a final on-treatment estradiol level of 248 pg/mL. All individuals achieved a testosterone level of less than 50 ng/dL during the study period. The average initial on-treatment testosterone level was not significantly different from average final on-treatment measurement of 24.0 mg/dL (P = .95). […]
Conclusion: Lower doses of injectable estradiol can achieve therapeutic estradiol levels with excellent testosterone suppression. […]
[…]
This study had been previously published as a conference abstract:
Kanin, M., Slack, M., Patel, R., Chen, K. T., Jackson, N., Williams, K., & Grock, S. (2024). 8309 Injectable Estradiol Dosing Regimens; A Retrospective Review of Hormone Therapy for Gender-Diverse Adults Assigned Male at Birth. Journal of the Endocrine Society, 8(Suppl 1), bvae163-1706. [DOI:10.1210/jendso/bvae163.1706]
Abuhelwa, A. Y., Foster, D. J., & Upton, R. N. (2015). ADVAN-style analytical solutions for common pharmacokinetic models. Journal of Pharmacological and Toxicological Methods, 73, 42–48. [DOI:10.1016/j.vascn.2015.03.004]
Aedo, A. R., Landgren, B. M., Johannisson, E., & Diczfalusy, E. (1985). Pharmacokinetic and pharmacodynamic investigations with monthly injectable contraceptive preparations. Contraception, 31(5), 453–469. [DOI:10.1016/0010-7824(85)90081-2]
Aisaka, K., Ando, S., Kokubo, K., Yoshida, K., & Mori, H. (1986). いわゆる潜在性高prolactin血症患者におけるprolactin分泌予備能の検討. [Studies on Prolactin Secreting Capacity in the Ovulatory Infertile Patients with Transient Hyperprolactinemia.] 日本内分泌学会雑誌 / Nihon Naibunpi Gakkai Zasshi / Folia Endocrinologica Japonica, 62(5), 662–671. [DOI:10.1507/endocrine1927.62.5_662]
Akande, E. O. (1974). The effect of oestrogen on plasma levels of luteinizing hormone in euthyroid and thyrotoxic postmenopausal women. The Journal of Obstetrics and Gynaecology of the British Commonwealth / BJOG, 81(10), 795–803. [DOI:10.1111/j.1471-0528.1974.tb00383.x]
Ballard, B. E. (1978). An Overview of Prolonged Action Drug Dosage Forms. In Robinson, J. R. (Ed.). Sustained and Controlled Release Drug Delivery Systems (pp. 1–69). New York/Basel: Marcel Dekker. [Google Scholar] [Google Books]
Behre, H. M., Oberpenning, F., & Nieschlag, E. (1990). Comparative pharmacokinetics of androgen preparations: application of computer analysis and simulation. In Nieschlag, E., & Behre, H. M. (Eds.). Testosterone: Action · Deficiency · Substitution, 1st Edition (pp. 115–135). Berlin/Heidelberg: Springer. [DOI:10.1007/978-3-662-00814-0_6]
Behre, H. M., & Nieschlag, E. (1998). Comparative pharmacokinetics of testosterone esters. In Nieschlag, E., & Behre, H. M. (Eds.). Testosterone: Action · Deficiency · Substitution, 2nd Edition (pp. 329–348). Berlin/Heidelberg: Springer. [DOI:10.1007/978-3-642-72185-4_11]
Behre, H. M., Wang, C., Handelsman, D. J., & Nieschlag, E. (2004). Pharmacology of testosterone preparations. Testosterone: Action · Deficiency · Substitution, 3rd Edition (pp. 405–444). Cambridge/New York: Cambridge University Press. [DOI:10.1017/CBO9780511545221.015] [PDF]
Behre, H. M., & Nieschlag, E. (2012). Testosterone preparations for clinical use in males. In Nieschlag, E., Behre, H. M., & Nieschlag, S. (Eds.). Testosterone: Action · Deficiency · Substitution, 4th Edition (pp. 309–335). Cambridge/New York: Cambridge University Press. [DOI:10.1017/CBO9781139003353.016]
Bider, D., Ben-Rafael, Z., Shalev, J., Goldenberg, M., Mashiach, S., & Blankstein, J. (1989). Pituitary and ovarian suppression rate after high dosage of gonadotropin-releasing hormone agonist. Fertility and Sterility, 51(4), 578–581. [DOI:10.1016/S0015-0282(16)60602-7]
Blackwell, R. E., Boots, L. R., & Potter Jr, H. D. (1982). Evaluation of Delestrogen and Parlodel as a luteolytic agent in humans. Fertility and Sterility, 37(2), 213–217. [DOI:10.1016/S0015-0282(16)46042-5]
Bourns, A. (2019). Guidelines for Gender-Affirming Primary Care with Trans and Non-Binary Patients, 4th Edition. Toronto: Rainbow Health Ontario/Sherbourne Health. [URL] [PDF]
Bradbury, J. T., Long, R. C., & Durham, W. C. (1953). Progesterone and estrogen requirements to induce and maintain decidua. Fertility and Sterility, 4(1), 63–75. [DOI:10.1016/S0015-0282(16)31145-1]
Braun, P., Wildt, L., & Leyendecker, G. (1983). The effect of danazol on gonadotropin secretion during the follicular phase of the menstrual cycle. Fertility and Sterility, 40(1), 37–44. [DOI:10.1016/S0015-0282(16)47174-8]
Buckman, M. T., Johnson, J., Ellis, H., Srivastava, L., & Peake, G. T. (1980). Differential lipemic and proteinemic response to oral ethinyl estradiol and parenteral estradiol cypionate. Metabolism, 29(9), 803–805. [DOI:10.1016/0026-0495(80)90117-1]
Callen-Lorde Community Health Center. (2018). Protocols for the Provision of Hormone Therapy. New York City: Callen-Lorde Community Health Center. [URL] [PDF]
Canales, E. S., Cabezas, A., Vázquez-Matute, L., & Zárate, A. (1978). Induction of ovulation with clomiphene and estradiol benzoate in anovulatory women refractory to clomiphene alone. Fertility and Sterility, 29(5), 496–499. [DOI:10.1016/S0015-0282(16)43271-1]
Canales, E. S., Fonseca, M. E., Mason, M., & Zárate, A. (1981). Feedback effect of estradiol on follicle-stimulating hormone and prolactin secretion during the puerperium. International Journal of Gynecology & Obstetrics, 19(1), 79–81. [DOI:10.1016/0020-7292(81)90043-6]
Cano, A., Gimeno, F., Fuente, T., Parrilla, J. J., & Abad, L. (1986). The positive feedback of estradiol on gonadotropin secretion in women with perimenopausal dysfunctional uterine bleeding. European Journal of Obstetrics & Gynecology and Reproductive Biology, 22(5–6), 353–358. [DOI:10.1016/0028-2243(86)90125-5]
Carlson, S. M., Dominguez, C., Jeevananthan, A., & Crowley, M. J. (2025). Follow-Up Estradiol Levels Based on Regimen Formulation With Guideline-Concordant Gender-Affirming Hormone Therapy. Journal of the Endocrine Society, 9(3), bvae205. [DOI:10.1210/jendso/bvae205]
Cavanaugh, T., Hopwood, R., Gonzalez, A., & Thompson, J. (2015). The Medical Care of Transgender Persons. Boston: Fenway Health. [URL] [PDF]
Chantrapanichkul, P., Stevenson, M. O., Suppakitjanusant, P., Goodman, M., & Tangpricha, V. (2021). Serum Hormone Concentrations in Transgender Individuals Receiving Gender-Affirming Hormone Therapy: A Longitudinal Retrospective Cohort Study. Endocrine Practice, 27(1), 27–33. [DOI:10.4158/EP-2020-0414] [Table]
Chien, Y. W. (1981). Long-acting parenteral drug formulations. Journal of Parenteral Science and Technology / PDA Journal of Pharmaceutical Science and Technology, 35(3), 106–139. [Google Scholar] [URL] [PDF]
Cirrincione, L. R., Winston McPherson, G., Rongitsch, J., Sadilkova, K., Drees, J. C., Krasowski, M. D., Dickerson, J. A., & Greene, D. N. (2021). Sublingual estradiol is associated with higher estrone concentrations than transdermal or injectable preparations in transgender women and gender nonbinary adults. LGBT Health, 8(2), 125–132. [DOI:10.1089/lgbt.2020.0249] [Table]
Colburn, W. A. (1981). Simultaneous pharmacokinetic and pharmacodynamic modeling. Journal of Pharmacokinetics and Biopharmaceutics, 9(3), 367–388. [DOI:10.1007/BF01059272]
Coleman, E., Radix, A. E., Bouman, W. P., Brown, G. R., de Vries, A. L., Deutsch, M. B., Ettner, R., Fraser, L., Goodman, M., Green, J., Hancock, A. B., Johnson, T. W., Karasic, D. H., Knudson, G. A., Leibowitz, S. F., Meyer-Bahlburg, H. F., Monstrey, S. J., Motmans, J., Nahata, L., … & Arcelus, J. (2022). [World Professional Association for Transgender Health (WPATH)] Standards of Care for the Health of Transgender and Gender Diverse People, Version 8. International Journal of Transgender Health, 23(Suppl 1), S1–S259. [DOI:10.1080/26895269.2022.2100644] [URL] [PDF]
Dahl, M., Feldman, J. L., Goldberg, J., & Jaberi, A. (2015). Endocrine Therapy for Transgender Adults in British Columbia: Suggested Guidelines. Physical Aspects of Transgender Endocrine Therapy. Vancouver: Vancouver Coastal Health. [Google Scholar] [PDF]
Davidson, A., Franicevich, J., Freeman, M., Lin, R., Martinez, L., Monihan, M., Porch, M., Samuel, L., Stukalin, R., Vormohr, J., & Zevin, B. (2013). Protocols for Hormonal Reassignment of Gender. San Francisco: San Francisco Department of Public Health/Tom Waddell Health Center. [Google Scholar] [PDF]
Depo®-Estradiol Estradiol Cypionate Label. U.S. Food and Drug Administration/Pharmacia & Upjohn (Pfizer). [URL] [PDF]
Derra, C. (1981). Hormonprofile unter Östrogen- und Antiandrogentherapie bei Patienten mit Prostatakarzinom: Östradiolundecylat versus Cyproteronacetat. [Hormone Profiles under Estrogen and Antiandrogen Therapy in Patients with Prostate Cancer: Estradiol Undecylate versus Cyproterone Acetate.] (Doctoral dissertation, University of Mainz.) [Google Scholar] [WorldCat] [PDF] [Translation]
Deutsch, M. (2014). Medical Transition. In Erickson-Schroth, L. (Ed.). Trans Bodies, Trans Selves: A Resource for the Transgender Community, 1st Edition (pp. 241–264). Oxford: Oxford University Press. [Google Scholar] [Google Books] [OpenLibrary] [WorldCat] [Archive.org] [PDF]
Deutsch, M. B., Bhakri, V., & Kubicek, K. (2015). Effects of Cross-Sex Hormone Treatment on Transgender Women and Men. Obstetrics & Gynecology, 125(3), 605–610. [DOI:10.1097/AOG.0000000000000692]
Deutsch, M. B. (Ed.). (2016). Guidelines for the Primary and Gender-Affirming Care of Transgender and Gender Nonbinary People, 2nd Edition. San Francisco: University of California, San Francisco/UCSF Transgender Care. [URL] [PDF]
Deutsch, M. B. (2016). Overview of feminizing hormone therapy. In Deutsch, M. B. (Ed.). Guidelines for the Primary and Gender-Affirming Care of Transgender and Gender Nonbinary People, 2nd Edition (pp. 26–48). San Francisco: University of California, San Francisco/UCSF Transgender Care. [URL] [PDF]
Düsterberg, B., & Nishino, Y. (1982). Pharmacokinetic and pharmacological features of oestradiol valerate. Maturitas, 4(4), 315–324. [DOI:10.1016/0378-5122(82)90064-0]
Düsterberg, B., & Wendt, H. (1983). Plasma levels of dehydroepiandrosterone and 17β-estradiol after intramuscular administration of Gynodian-Depot® in 3 women. Hormones, 17(2), 84–89. [DOI:10.1159/000179680]
Düsterberg, B., Schmidt-Gollwitzer, M., & Hümpel, M. (1985). Pharmacokinetics and biotransformation of estradiol valerate in ovariectomized women. Hormone Research in Paediatrics, 21(3), 145–154. [DOI:10.1159/000180039]
Edkins, R. P. (1959). The Modification of the Duration of Drug Action: Pharmaceutical Considerations. Journal of Pharmacy and Pharmacology, 11(Suppl 1), 54T–66T. [DOI:10.1111/j.2042-7158.1959.tb10412.x]
Enever, R. P., Fotherby, K., Naderi, S., & Lewis, G. A. (1983). Long-acting contraceptive agents: The influence of physicochemical properties of some esters of norethisterone upon the plasma levels of free norethisterone. Steroids, 41(3), 381–396. [DOI:10.1016/0039-128X(83)90109-5]
Eriksson, O., Bäckström, T., Stridsberg, M., Hammarlund-Udenaes, M., & Naessén, T. (2006). Differential response to estrogen challenge test in women with and without premenstrual dysphoria. Psychoneuroendocrinology, 31(4), 415–427. [DOI:10.1016/j.psyneuen.2005.10.004]
Espino y Sosa, S., Cortés Fuentes, M., Gómez Rico, J. A., & Cortés Bonilla, M. (2019). Non-polymeric Microspheres for the Therapeutic Use of Estrogens: An Innovative Technology. In Khan, W. A. (Ed.). Estrogen. London: IntechOpen. [DOI:10.5772/intechopen.82553]
Fisher, D., & Shafer, S. (2007). Fisher/Shafer NONMEM Workshop Pharmacokinetic and Pharmacodynamic Analysis with NONMEM. Basic Concepts. [PDF]
Florence, A. T. (2010). Looking at Formulations. In Florence, A. T. An Introduction to Clinical Pharmaceutics (pp. 69–100). London/Chicago: Pharmaceutical Press. [Google Scholar] [Google Books]
Fotherby, K., Benagiano, G., Toppozada, H. K., Abdel-Rahman, A., Navaroli, F., Arce, B., Ramos-Cordero, R., Gual, C., Landgren, B. M., & Johannisson, E. (1982). A preliminary pharmacological trial of the monthly injectable contraceptive Cycloprovera. Contraception, 25(3), 261–272. [DOI:10.1016/0010-7824(82)90049-X]
Futterweit, W., Gabrilove, J., & Smith, H. (1984). Testicular steroidogenic response to human chorionic gonadotropin of fifteen male transsexuals on chronic estrogen treatment. Metabolism, 33(10), 936–942. [DOI:10.1016/0026-0495(84)90248-8] [Figure]
Garner, P. R., & Armstrong, D. T. (1977). The effect of human chorionic gonadotropin and estradiol-17β on the maintenance of the human corpus luteum of early pregnancy. American Journal of Obstetrics and Gynecology, 128(5), 469–475. [DOI:10.1016/0002-9378(77)90026-6]
Garza-Flores, J., Rodriguez, V., Perez-Palacios, G., Virutamasen, P., Tang-Keow, P., Konsayreepong, R., Kovacs, L., Koloszar, S., & Hall, P. E. (1987). A multicentered pharmacokinetic, pharmacodynamic study of once-a-month injectable contraceptives. I. Different doses of HRP112 and of DepoProvera. Contraception, 36(4), 441–457. [DOI:10.1016/0010-7824(87)90093-X]
Garza-Flores, J., Alba, V. M., Cravioto, M. C., Hernandez, L., Perez-Palacios, G., Alvarado, G., Rivera, R., Recio, R., & Bassol, S. (1989). Estrogen-progestogen once-a-month injectable contraceptives and serum prolactin. Contraception, 39(5), 519–529. [DOI:10.1016/0010-7824(89)90107-8]
Garza-Flores, J., Fatinikun, T., Hernandez, L., Ramos, I., Cardenas, M., & Menjivar, M. (1991). A pilot study on the assessment of a progesterone/estradiol sustained release as once-a-month-injectable contraceptive. Contraception, 44(1), 45–59. [DOI:10.1016/0010-7824(91)90105-O]
Garza-Flores, J. (1994). Pharmacokinetics of once-a-month injectable contraceptives. Contraception, 49(4), 347–359. [DOI:10.1016/0010-7824(94)90032-9]
Geppert, G. (1975). Untersuchungen zur Pharmakokinetik von Östradiol-17β, Östradiol-Benzoat, Östradiol-Valerianat und Östradiol-Undezylat bei der Frau: Der Verlauf der Konzentrationen von Östradiol-17β, Östron, LH und FSH im Serum. [Studies on the Pharmacokinetics of Estradiol-17β, Estradiol Benzoate, Estradiol Valerate, and Estradiol Undecylate in Women: The Course of the Relationships Between Estradiol-17β, Estrone, LH, and FSH in Serum.] (Doctoral dissertation, University of Bonn.) [Google Scholar] [WorldCat] [PDF] [Translation]
Glintborg, D., T’Sjoen, G., Ravn, P., & Andersen, M. S. (2021). Management of endocrine disease: Optimal feminizing hormone treatment in transgender people. European Journal of Endocrinology, 185(2), R49–R63. [DOI:10.1530/EJE-21-0059]
Goh, H. H., & Ratnam, S. S. (1988). The LH surge in humans: its mechanism and sex difference. Gynecological Endocrinology, 2(2), 165–182. [DOI:10.3109/09513598809023624]
Goh, H. H., & Ratnam, S. S. (1990). Effect of estrogens on prolactin secretion in transsexual subjects. Archives of Sexual Behavior, 19(5), 507–516. [DOI:10.1007/BF02442351]
Goh, V. H. H., & Lee, K. O. (1998). Does a positive oestrogen feedback on the hypothalamic-pituitary axis exist concurrently with a defective testosterone feedback in Klinefelter’s syndrome? Hormone Research in Paediatrics, 50(3), 160–165. [DOI:10.1159/000023266]
Goodman, R. E., Anderson, D. C., Bu’Lock, D. E., Sheffield, B., Lynch, S. S., & Butt, W. R. (1985). Study of the effect of estradiol on gonadotrophin levels in untreated male-to-female transsexuals. Archives of Sexual Behavior, 14(2), 141–146. [DOI:10.1007/BF01541659]
Gooren, L. J. G., Rao, B. R., Van Kessel, H., & Harmsen-Louman, W. (1984). Estrogen positive feedback on LH secretion in transsexuality. Psychoneuroendocrinology, 9(3), 249–259. [DOI:10.1016/0306-4530(84)90004-0]
Gooren, L. (2005). Hormone treatment of the adult transsexual patient. Hormone Research in Paediatrics, 64(Suppl 2), 31–36. [DOI:10.1159/000087751]
Göretzlehner, G., Ackermann, W., Angelow, K., Bergmann, G., Bieck, E., Golbs, S., & Kliem, O. (2002). Pharmakokinetik von Estron, Estradiol, FSH, LH und Prolaktin nach intramuskulärer Applikation von 5 mg Estradiolvalerat. [Pharmacokinetics of estradiol valerate in postmenopausal women after intramuscular administration.] Journal für Menopause, 9(2), 46–49. [Google Scholar] [URL] [PDF] [Translation]
Gorton, N., Jaffe, J. M., Thompson, J., Menkin, D., Nesteby, A., Dunn, D., Baker, K. K., Harbatkin, D., Do, T., Radix, A., Meacher, P., Goldstein, Z., Carpenter, W., Caine, M., Henn, S., Murayama, R., Feldmann, J., & Zayas, S. (2019). TransLine Gender Affirming Hormone Therapy Prescriber Guidelines. San Francisco: Lyon-Martin Health Services/TransLine. [URL] [PDF]
Gunnarsson, P. O., & Norlén, B. J. (1988). Clinical pharmacology of polyestradiol phosphate. The Prostate, 13(4), 299–304. [DOI:10.1002/pros.2990130405]
Hamburger, C., & Benjamin, H. (1969). Endocrine Treatment of Male and Female Transsexualism / Appendix for the Practicing Physician: Suggestions and Guidelines for the Management of Transsexuals. In Green, R., & Money, J. (Eds.). Transsexualism and Sex Reassignment (pp. 291–307). Baltimore: John Hopkins University Press. [Google Scholar] [Google Books] [PDF]
Hembree, W. C., Cohen-Kettenis, P. T., Gooren, L., Hannema, S. E., Meyer, W. J., Murad, M. H., Rosenthal, S. M., Safer, J. D., Tangpricha, V., & T’Sjoen, G. G. (2017). Endocrine Treatment of Gender-Dysphoric/Gender-Incongruent Persons: An Endocrine Society Clinical Practice Guideline. The Journal of Clinical Endocrinology and Metabolism, 102(11), 3869–3903. [DOI:10.1210/jc.2017-01658]
Henriksson, P., Carlström, K., Pousette, A., Gunnarsson, P. O., Johansson, C. J., Eriksson, B., Altersgård-Brorsson, A. K., Nordle, O., & Stege, R. (1999). Time for revival of estrogens in the treatment of advanced prostatic carcinoma? Pharmacokinetics, and endocrine and clinical effects, of a parenteral estrogen regimen. The Prostate, 40(2), 76–82. [DOI:10.1002/(SICI)1097-0045(19990701)40:2<76::AID-PROS2>3.0.CO;2-Q]
Herndon, J. S., Maheshwari, A. K., Nippoldt, T. B., Carlson, S. J., Davidge-Pitts, C. J., & Chang, A. Y. (2023). Comparison of Subcutaneous and Intramuscular Estradiol Regimens as part of Gender-Affirming Hormone Therapy. Endocrine Practice, 29(5), 356–361. [DOI:10.1016/j.eprac.2023.02.006]
Hughes, J. H., Woo, K. H., Keizer, R. J., & Goswami, S. (2022). Clinical Decision Support for Precision Dosing: Opportunities for Enhanced Equity and Inclusion in Health Care. Clinical Pharmacology & Therapeutics, 113(3), 565–574. [DOI:10.1002/cpt.2799]:
Ibrahim, S. (1996/1998). Pharmakokinetische Untersuchungen mit Östradiolvalerat und Hydroxyprogesteroncaproat in Depotform nach einmaliger Applikation bei 24 postmenopausalen Frauen. [Pharmacokinetic studies with estradiol valerate and hydroxyprogesterone caproate in depot form after a single application in 24 postmenopausal women.] (Doctoral dissertation, Dresden University of Technology.) [Google Scholar] [WorldCat] [Partial PDF]
Ittrich, G., & Pots, P. (1965). Östrogenbestimmungen in Blut und Urin nach Verabreichung von Östrogenen. [Estrogen determinations in blood and urine after administration of estrogens.] In Kraatz, H. (Ed.). International Symposium der Gynäkologischen Endokrinologie vom 15. bis 18. Mai 1963. / Abhandlungen der Deutschen Akademie der Wissenschaften zu Berlin, Klasse für Medizin, 1965(1), 53–56. [ISSN:0568-4250] [WorldCat 1] [WorldCat 2] [WorldCat 3] [PDF] [Translation]
Jaafar, S., Torres-Leguizamon, M., Duplessy, C., & Stambolis-Ruhstorfer, M. (2022). Hormonothérapie injectable et réduction des risques: pratiques, difficultés, santé des personnes trans en France. [Hormone replacement therapy injections and harm reduction: practices, difficulties, and transgender people’s health in France.] Sante Publique, 34(HS2), 109–122. [Google Scholar] [PubMed] [DOI:10.3917/spub.hs2.0109]
Jacobi, G. H., & Altwein, J. E. (1979). Bromocriptin als Palliativtherapie beim fortgeschrittenen Prostatakarzinom. [Bromocriptine for palliation of advanced prostatic carcinoma. Experimental and clinical profile of a drug.] Urologia Internationalis, 34(4), 266–290. [DOI:10.1159/000280272]
Jacobi, G. H., Altwein, J. E., Kurth, K. H., Basting, R., & Hohenfellner, R. (1980). Treatment of advanced prostatic cancer with parenteral cyproterone acetate: a phase III randomised trial. British Journal of Urology, 52(3), 208–215. [DOI:10.1111/j.1464-410X.1980.tb02961.x]
Jacobi, G. R. (1982). Experimental Rationale for the Investigation of Antiprolactins as Palliative Treatment for Prostate Cancer. In Jacobi, G. H., & Hohenfellner, R. (Eds.). Prostate Cancer (International Perspectives in Urology, Volume 3) (pp. 419–431). Baltimore/London: Williams & Wilkins. [Google Scholar] [Google Books]
Jilma, B., Eichler, H. G., Breiteneder, H., Wolzt, M., Aringer, M., Graninger, W., Röhrer, C., Veitl, M., & Wagner, O. F. (1994). Effects of 17β-estradiol on circulating adhesion molecules. The Journal of Clinical Endocrinology and Metabolism, 79(6), 1619–1624. [DOI:10.1210/jcem.79.6.7527406]
Johansson, C. J., & Gunnarsson, P. O. (2000). Pharmacodynamic model of testosterone suppression after intramuscular depot estrogen therapy in prostate cancer. The Prostate, 44(1), 26–30. [DOI:10.1002/1097-0045(20000615)44:1<26::AID-PROS4>3.0.CO;2-P]
Jones, T. M., Fang, V. S., Landau, R. L., & Rosenfield, R. (1978). Direct inhibition of Leydig cell function by estradiol. The Journal of Clinical Endocrinology and Metabolism, 47(6), 1368–1373. [DOI:10.1210/jcem-47-6-1368]
Jönsson, G., Olsson, A. M., Luttrop, W., Cekan, Z., Purvis, K., & Diczfalusy, E. (1976). Treatment of prostatic carcinoma with various types of estrogen derivatives. In Munson, P. L., Diczfalusy, E., Glover, J., Olson, R. E., Harris, R. S., Thimann, K. V., Loraine, J. A., & Wool, I. G. (Eds.). Vitamins & Hormones, Volume 33 (pp. 351–376). New York/San Francisco/London: Academic Press. [DOI:10.1016/S0083-6729(08)60965-6]
Kalicharan, R. W., Schot, P., & Vromans, H. (2016). Fundamental understanding of drug absorption from a parenteral oil depot. European Journal of Pharmaceutical Sciences, 83, 19–27. [DOI:10.1016/j.ejps.2015.12.011]
Kalicharan, R. W. (2017). New Insights into Drug Absorption from Oil Depots. (Doctoral dissertation, Utrecht University.) [Google Scholar] [URL] [PDF]
Kanin, M., Slack, M., Patel, R., Chen, K. T., Jackson, N., Williams, K., & Grock, S. (2024). 8309 Injectable Estradiol Dosing Regimens; A Retrospective Review of Hormone Therapy for Gender-Diverse Adults Assigned Male at Birth. Journal of the Endocrine Society, 8(Suppl 1), bvae163-1706. [DOI:10.1210/jendso/bvae163.1706]
Kanin, M., Slack, M., Patel, R., Chen, K. T., Jackson, N., Williams, K. C., & Grock, S. (2025). Injectable Estradiol Dosing Regimens in Transgender and Nonbinary Adults Listed as Male at Birth. Journal of the Endocrine Society, bvaf004. [DOI:10.1210/jendso/bvaf004]
Kariyawasam, N. M., Ahmad, T., Sarma, S., & Fung, R. (2024). Comparison of Estrone/Estradiol Ratio and Levels in Transfeminine Individuals on Different Routes of Estradiol. Transgender Health, ahead of print. [DOI:10.1089/trgh.2023.0138] [Data]
Kemeter, P., Bernaschek, G., Altmann, G., & Feichtinger, W. (1984). The effect of 2 mg estradiol-17β plus 1 mg estriol, sequentially combined with 1 mg norethisteroneacetate, on LH, FSH, estradiol-17β, progesterone, testosterone and prolactin after ovarectomy. Archives of Gynecology, 234(3), 219–229. [DOI:10.1007/BF00570759]
Kerdelhué, B., Andrews, M. C., Zhao, Y., Scholler, R., & Jones Jr, H. W. (2006). Short term changes in melatonin and cortisol serum levels after a single administration of estrogen to menopausal women. Neuroendocrinology Letters, 27(5), 659–664. [Google Scholar] [URL] [PDF]
Keye, W. R., & Jaffe, R. B. (1975). Strength-duration characteristics of estrogen effects on gonadotropin response to gonadotropin-releasing hormone in women. I. Effects of varying duration of estradiol administration. The Journal of Clinical Endocrinology and Metabolism, 41(6), 1003–1008. [DOI:10.1210/jcem-41-6-1003]
Knudsen, P., Hansen, L. B., & Larsen, N. E. (1985). Pharmacokinetic implications of different oil vehicles used in depot neuroleptic treatment. Acta Psychiatrica Scandinavica, 72(S322), 7–10. [DOI:10.1111/j.1600-0447.1985.tb08535.x]
Kronawitter, D., Gooren, L. J., Zollver, H., Oppelt, P. G., Beckmann, M. W., Dittrich, R., & Mueller, A. (2009). Effects of transdermal testosterone or oral dydrogesterone on hypoactive sexual desire disorder in transsexual women: results of a pilot study. European Journal of Endocrinology, 161(2), 363–368. [DOI:10.1530/eje-09-0265] [Table]
Kuhl, H. (1986). Hormonsubstitution durch Injektionspräparate und Hautimplantate. [Hormone substitution by injectable preparations and skin implants.] Der Gynäkologe, 19(4), 241–247. [Google Scholar] [PubMed] [PDF] [Translation]
Kuhl, H. (1990). Pharmacokinetics of oestrogens and progestogens. Maturitas, 12(3), 171–197. [DOI:10.1016/0378-5122(90)90003-O]
Kuhl, H. (2005). Pharmacology of estrogens and progestogens: influence of different routes of administration. Climacteric, 8(Suppl 1), 3–63. [DOI:10.1080/13697130500148875] [PDF]
LaBudde, J. A., Craig, W. Y., & Spratt, D. I. (2020). Initial Evaluation of Safety and Efficacy of Administration of Estradiol (E2) by Subcutaneous (SC) Injections to Male-to-Female (MTF) Transgender Patients. Fertility and Sterility, 114(3), e91–e91. [DOI:10.1016/j.fertnstert.2020.08.277]
Langley, R. E., Gilbert, D. C., Duong, T., Clarke, N. W., Nankivell, M., Rosen, S. D., Mangar, S., Macnair, A., Sundaram, S. K., Laniado, M. E., Dixit, S., Madaan, S., Manetta, C., Pope, A., Scrase, C. D., Mckay, S., Muazzam, I. A., Collins, G. N., Worlding, J., Williams, S. T., … & Parmar, M. (2021). Transdermal oestradiol for androgen suppression in prostate cancer: long-term cardiovascular outcomes from the randomised Prostate Adenocarcinoma Transcutaneous Hormone (PATCH) trial programme. The Lancet, 397(10274), 581–591. [DOI:10.1016/S0140-6736(21)00100-8]
Larsen, S. W., Rinvar, E., Svendsen, O., Lykkesfeldt, J., Friis, G. J., & Larsen, C. (2001). Determination of the disappearance rate of iodine-125 labelled oils from the injection site after intramuscular and subcutaneous administration to pigs. International Journal of Pharmaceutics, 230(1–2), 67–75. [DOI:10.1016/S0378-5173(01)00860-2]
Larsen, S. W., & Larsen, C. (2009). Critical factors influencing the in vivo performance of long-acting lipophilic solutions—impact on in vitro release method design. The AAPS Journal, 11(4), 762–770. [DOI:10.1208/s12248-009-9153-9]
Larsen, C., Larsen, S. W., Jensen, H., Yaghmur, A., & Østergaard, J. (2009). Role of in vitro release models in formulation development and quality control of parenteral depots. Expert Opinion on Drug Delivery, 6(12), 1283–1295. [DOI:10.1517/17425240903307431]
Larsen, S. W., Thing, M. A., & Larsen, C. (2012). Oily (lipophilic) solutions and suspensions. In Wright, J. C., & Burgess, D. J. (Eds.). Long Acting Injections and Implants (Advances in Delivery Science and Technology) (pp. 113–135). Boston: Springer. [DOI:10.1007/978-1-4614-0554-2_7]
Le, A., Huang, K. J., & Cirrincione, L. R. (2022). Regulation of drug-metabolizing enzymes by sex-related hormones: clinical implications for transgender medicine. Trends in Pharmacological Sciences, 43(7), 582–592. [DOI:10.1016/j.tips.2022.03.006]
Leinonen, P., Hammond, G. L., Lukkarinen, O., & Vihko, R. (1979). Serum sex hormone binding globulin and testosterone binding after estradiol administration, castration, and their combination in men with prostatic carcinoma. Investigative Urology, 17(1), 24–27. [Google Scholar] [PubMed]
Leinonen, P. (1980). Estrone and estradiol concentrations in the testis and spermatic and peripheral venous blood of elderly men: the influence of estrogen treatment. Journal of Steroid Biochemistry, 13(7), 737–742. [DOI:10.1016/0022-4731(80)90225-3]
Leyendecker, G., Geppert, G., Nocke, W., & Ufer, J. (1975). Untersuchungen zur Pharmakokinetik von Östradiol-17β, Östradiol-Benzoat, Östradiol-Valerianat und Östradiol-Undezylat bei der Frau: Der Verlauf der Konzentrationen von Östradiol-17β, Östron, LH und FSH im Serum. [Estradiol-17β, Estrone, LH and FSH in Serum After Administration of Estradiol-17β, Estradiol-Benzoate, Estradiol-Valeriate and Estradiol-Undecylate in the Female.] Geburtshilfe und Frauenheilkunde, 35(5), 370–374. [Google Scholar] [PubMed] [PDF] [Translation]
Leyendecker, G., Wildt, L., Gips, H., Nocke, W., & Plotz, E. J. (1976). Experimental studies on the positive feedback effect of progesterone, 17α-hydroxyprogesterone and 20α-dihydroprogesterone on the pituitary release of LH and FSH in the human female. Archiv für Gynäkologie, 221(1), 29–45. [DOI:10.1007/BF00667679]
Lichten, E. M., Lichten, J. B., Whitty, A., & Pieper, D. (1996). The confirmation of a biochemical marker for women’s hormonal migraine: The depo‐estradiol challenge test. Headache: The Journal of Head and Face Pain, 36(6), 367–371. [DOI:10.1046/j.1526-4610.1996.3606367.x]
Linet, T. (2023). Prise en charge endocrinologique d’une personne trans. [Endocrinological care of a trans person.] In Faucher, P., Hassoun, D., & Linet, T. (Eds.). Santé sexuelle et reproductive des personnes LGBT [Sexual and Reproductive Health of LGBT People] (pp. 109–124). Issy-les-Moulineaux, France: Elsevier Masson. [Google Books] [URL] [WorldCat] [Excerpt]
Lixsoft. (2008). Mathematical Expressions of the Pharmacokinetic and Pharmacodynamic Models Implemented in the Monolix Software. [PDF]
Martinez, G. (1995). Estradiol and Progesterone Serum Levels in Women Using the Once-a-month Injectable Contraceptive Perlutal. / Benagiano, G., Bianchi, P., von Kesserü, E., Castañeda, A., Correa, J. E., & Martínez, G. (1995). Session 19 what is new about injectable contraceptives? Advances in Contraception, 11(1), 39–42. [DOI:10.1007/BF02436100]
Martins, R. S., Antunes, N. J., Comerlatti, G., Caraccio, G., Moreno, R. A., Frecentese, F., Caliendo, G., & De Nucci, G. (2019). Quantification of estradiol cypionate in plasma by liquid chromatography coupled with tandem mass spectrometry: Application in a pharmacokinetic study in healthy female volunteers. Journal of Pharmaceutical and Biomedical Analysis, 170, 273–278. [DOI:10.1016/j.jpba.2019.03.053]
Messinis, I. E., & Templeton, A. (1987). Effect of high dose exogenous oestrogen on midcycle luteinizing hormone surge in human spontaneous cycles. Clinical Endocrinology, 27(4), 453–459. [DOI:10.1111/j.1365-2265.1987.tb01173.x]
Messinis, I. E., & Templeton, A. A. (1987). Disparate effects of endogenous and exogenous oestradiol on luteal phase function in women. Reproduction, 79(2), 549–554. [DOI:10.1530/jrf.0.0790549]
Milano, C., & Harper, J. (2025). Comments on Injectable Estradiol Use in Transgender and Gender-Diverse Individuals in the US. The Journal of Clinical Endocrinology & Metabolism, dgaf134. [DOI:10.1210/clinem/dgaf134]
Minto, C. F., Howe, C., Wishart, S., Conway, A. J., & Handelsman, D. J. (1997). Pharmacokinetics and pharmacodynamics of nandrolone esters in oil vehicle: effects of ester, injection site and injection volume. Journal of Pharmacology and Experimental Therapeutics, 281(1), 93–102. [URL]
Misakian, A. L., Kelley, C. E., Sullivan, E. A., Chang, J. J., Singh, G., Kokosa, S., Avila, J., Cooper, H., Liang, J. W., Botzheim, B., Quint, M., Jeevananthan, A., Chi, E., Harmer, M., Hiatt, L., Kowalewski, M., Steinberg, B., Tausinga, T., Tanner, H., Ho, T. F., … Ariel, D. (2025). Injectable Estradiol Use in Transgender and Gender-Diverse Individuals throughout the United States. The Journal of Clinical Endocrinology & Metabolism, dgaf015. [DOI:10.1210/clinem/dgaf015]
Mueller, A., Zollver, H., Kronawitter, D., Oppelt, P. G., Claassen, T., Hoffmann, I., Beckmann, M. W., & Dittrich, R. (2011). Body composition and bone mineral density in male-to-female transsexuals during cross-sex hormone therapy using gonadotrophin-releasing hormone agonist. Experimental and Clinical Endocrinology & Diabetes, 119(2), 95–100. [DOI:10.1055/s-0030-1255074] [Table]
Newton, J. R., d’Arcangues, C., & Hall, P. E. (1994). A review of ‘once-a-month’ combined injectable contraceptives. Journal of Obstetrics and Gynaecology, 14(Suppl 1), S1–S34. [DOI:10.3109/01443619409027641]
Nelson, M. D., Szczepaniak, L. S., Wei, J., Szczepaniak, E., Sánchez, F. J., Vilain, E., Stern, J. H., Bergman, R. N., Bairey Merz, C. N., & Clegg, D. J. (2016). Transwomen and the Metabolic Syndrome: Is Orchiectomy Protective? Transgender Health, 1(1), 165–171. [DOI:10.1089/trgh.2016.0016] [Table]
Nieschlag, E., & Behre, H. M. (2010). Testosterone therapy. In Nieschlag, E., Behre, H. M., & Nieschlag, S. (Eds.). Andrology (pp. 437–455). Berlin/Heidelberg: Springer. [DOI:10.1007/978-3-540-78355-8_21] [PDF]
Norlén, B. J., Fritjofsson, Å., Grönquist, L., Gunnarsson, P. O., Johansson, S. Å., & Plym-Forshell, G. (1987). Plasma concentrations of estradiol and testosterone in single-drug polyestradiol phosphate therapy for prostatic cancer. European Urology, 13, 193–197. [DOI:10.1159/000472772]
Olson-Kennedy, J., Rosenthal, S. M., Hastings, J., & Wesp, L. (2016). Health considerations for gender non-conforming children and transgender adolescents. In Deutsch, M. B. (Ed.). Guidelines for the Primary and Gender-Affirming Care of Transgender and Gender Nonbinary People, 2nd Edition (pp. 186–199). San Francisco: University of California, San Francisco/UCSF Transgender Care. [URL] [PDF]
Oriowo, M. A., Landgren, B. M., Stenström, B., & Diczfalusy, E. (1980). A comparison of the pharmacokinetic properties of three estradiol esters. Contraception, 21(4), 415–424. [DOI:10.1016/S0010-7824(80)80018-7]
Parkes, A. S. (1937). Relative duration of action of various esters of oestrone, oestradiol and oestriol. Biochemical Journal, 31(4), 579–585. [DOI:10.1042/bj0310579]
Patel, R., Korenman, S., Weimer, A., & Grock, S. (2024). A Call for Updates to Hormone Therapy Guidelines for Gender-Diverse Adults Assigned Male at Birth. Cureus, 16(6), e62262. [DOI:10.7759/cureus.62262] [PDF]
Patel, K. T., & Tangpricha, V. (2024). Parenteral Estradiol for Transgender Women: Time to adjust the dose. Endocrine Practice, 30(9), 893–894. [DOI:10.1016/j.eprac.2024.07.005]
Presl, J., Horejsi, J., Štroufová, A., & Herzmann, J. (1976). Sexual maturation in girls and the development of estrogen-induced gonadotropic hormone release. Annales de Biologie Animale, Biochimie, Biophysique, 16(3), 377–383. [DOI:10.1051/rnd:19760314]
Rahimy, M. H., & Ryan, K. K. (1999). Lunelle monthly contraceptive injection (medroxyprogesterone acetate and estradiol cypionate injectable suspension): assessment of return of ovulation after three monthly injections in surgically sterile women. Contraception, 60(4), 189–200. [DOI:10.1016/s0010-7824(99)00081-5]
Rahimy, M. H., Ryan, K. K., & Hopkins, N. K. (1999). Lunelle™ monthly contraceptive injection (medroxyprogesterone acetate and estradiol cypionate injectable suspension): steady-state pharmacokinetics of MPA and E2 in surgically sterile women. Contraception, 60(4), 209–214. [DOI:10.1016/S0010-7824(99)00086-4]
Rauramo, L., Punnonen, R., Kaihola, H. L., & Grönroos, M. (1980). Serum oestrone, oestradiol and oestriol concentrations in castrated women during intramuscular oestradiolvalerate and oestradiolbenzoate-oestradiolphenylpropionate therapy. Maturitas, 2(1), 53–58. [DOI:10.1016/0378-5122(80)90060-2]
Rauramo, L., Punnonen, R., & Grönroos, M. (1981). Serum concentrations of oestrone, oestradiol and oestriol during various oestrogen treatments. Maturitas, 3(2), 183–186. [DOI:10.1016/0378-5122(81)90010-4]
Recio, R., Garza-Flores, J., Schiavon, R., Reyes, A., Diaz-Sanchez, V., Valles, V., Luz de la Cruz, D., Oropeza, G., & Perez-Palacios, G. (1986). Pharmacodynamic assessment of dihydroxyprogesterone acetophenide plus estradiol enanthate as a monthly injectable contraceptive. Contraception, 33(6), 579–589. [DOI:10.1016/0010-7824(86)90046-6]
Reimann, I. W., Britzelmeier, C., Haber, P., Wollmann, H., Antonin, K. H., & Bieck, P. R. (1987). Influence of Oestradiol on Alpha2-Adrenoceptor Binding Sites on Intact Platelets of Young Male Volunteers. European Journal of Clinical Pharmacology, 33(2), 147–150. [DOI:10.1007/BF00544558]
Rosenfield, R. L., Fang, V. S., Dupon, C., Kim, M. H., & Refetoff, S. (1973). The effects of low doses of depot estradiol and testosterone in teenagers with ovarian failure and Turner’s syndrome. The Journal of Clinical Endocrinology and Metabolism, 37(4), 574–580. [DOI:10.1210/jcem-37-4-574]
Rosenfield, R. L., & Fang, V. S. (1974). The effects of prolonged physiologic estradiol therapy on the maturation of hypogonadal teen-agers. The Journal of Pediatrics, 85(6), 830–837. [DOI:10.1016/S0022-3476(74)80355-0]
Rothman, M. S., Ariel, D., Kelley, C., Hamnvik, O. R., Abramowitz, J., Irwig, M. S., Soe, K., Davidge-Pitts, C., Misakian, A. L., Safer, J. D., & Iwamoto, S. J. (2024). The Use of Injectable Estradiol in Transgender and Gender Diverse Adults: A Scoping Review of Dose and Serum Estradiol Levels. Endocrine Practice, 30(9), 870–878. [DOI:10.1016/j.eprac.2024.05.008]
Rothman, M. S., Hamnvik, O. P. R., Davidge-Pitts, C., Safer, J. D., Ariel, D., Tangpricha, V., Abramowitz, J., Soe, K., Sarvaideo, J., Kelley, C., Irwig, M. S., & Iwamoto, S. J. (2024). Revisiting Injectable Estrogen Dosing Recommendations for Gender-Affirming Hormone Therapy. Transgender Health, 9(6), 463–465. [DOI:10.1089/trgh.2023.0209]
Sang, G. W., Ge, J. L., Liu, X. H., Shao, Q. X., Zhao, X. J., & Mao, S. M. (1987). 不同剂量庚炔诺酮单独或配伍戊酸雌二醇后的药代动力学及药效学. [Pharmacokinetics and pharmacodynamics of different doses of norethisterone enanthate alone and in combination with estradiol valerate.] 中国 临 床药理 学杂志 / Chinese Journal of Clinical Pharmacology, 3(1), 7–18. [Google Scholar] [CNKI] [DOI:10.13699/j.cnki.1001-6821.1987.01.002] [PDF]
Sang, G. W. (1994). Pharmacodynamic effects of once-a-month combined injectable contraceptives. Contraception, 49(4), 361–385. [DOI:10.1016/0010-7824(94)90033-7]
Schiavon, R., Benavides, S., Oropeza, G., Garza-Flores, J., Recio, R., Díaz-Sanchez, V., & Pérez-Palacios, G. (1988). Serum estrogens and ovulation return in chronic users of a once-a-month injectable contraceptive. Contraception, 37(6), 591–598. [DOI:10.1016/0010-7824(88)90005-4]
Schug, B. S., Donath, F., & Blume, H. H. (2012). Bioavailability and pharmacodynamics of two 10-mg estradiol valerate depot formulations following IM single dose administration in healthy postmenopausal volunteers. International Journal of Clinical Pharmacology and Therapeutics, 50(2), 100–117. [Google Scholar] [DOI:10.5414/cp201589] [PDF]
Schulte-Beerbühl, M., & Nieschlag, E. (1980). Comparison of testosterone, dihydrotestosterone, luteinizing hormone, and follicle-stimulating hormone in serum after injection of testosterone enanthate or testosterone cypionate. Fertility and Sterility, 33(2), 201–203. [DOI:10.1016/S0015-0282(16)44543-7]
Schultz, K., Møllgaard, B., Fisher, A. N., Illum, L., & Larsen, C. (1998). Intramuscular rate of disappearance of oily vehicles in rabbits investigated by gamma-scintigraphy. International Journal of Pharmaceutics, 169(1), 121–126. [DOI:10.1016/S0378-5173(98)00121-5]
Schweikert, H. U., Weissbach, L., Leyendecker, G., Schwinger, E., Wartenberg, H., & Krück, F. (1982). Clinical, endocrinological, and cytological characterization of two 46, XX males. The Journal of Clinical Endocrinology & Metabolism, 54(4), 745–752. [DOI:10.1210/jcem-54-4-745]
Seibert, B., & Günzel, P. (1994). Animal toxicity studies performed for risk assessment of the once-a-month injectable contraceptive Mesigyna®. Contraception, 49(4), 303–333. [DOI:10.1016/0010-7824(94)90030-2]
Shah, J. C. (2007). Controlled Release – Small Molecules. In Stella, V. J., Borchardt, R. T., Hageman, M. J., Oliyai, R., Maag, H., & Tilley, J. W. (Eds.). Prodrugs: Challenges and Rewards, Part 1 (Biotechnology: Pharmaceutical Aspects, Volume V) (pp. 357–377). New York: Springer. [DOI:10.1007/978-0-387-49785-3_9]
Sharula, Chekir, C., Emi, Y., Arai, F., Kikuchi, Y., Sasaki, A., Matsuda, M., Shimizu, K., Tabuchi, K., Kamada, Y., Hiramatsu, Y., & Nakatsuka, M. (2012). Altered arterial stiffness in male‐to‐female transsexuals undergoing hormonal treatment. Journal of Obstetrics and Gynaecology Research, 38(6), 932–940. [DOI:10.1111/j.1447-0756.2011.01815.x] [Data]
Shaw, R. W., Butt, W. R., London, D. R., & Marshall, J. C. (1975). The oestrogen provocation test: a method of assessing the hypothalamic‐pituitary axis in patients with amenorrhoea. Clinical Endocrinology, 4(3), 267–276. [DOI:10.1111/j.1365-2265.1975.tb01534.x]
Shaw, R. W., Butt, W. R., & London, D. R. (1975). The effect of oestrogen pretreatment on subsequent response to luteinizing hormone releasing hormone in normal women. Clinical Endocrinology, 4(3), 297–304. [DOI:10.1111/j.1365-2265.1975.tb01537.x]
Shaw, R. W. (1978). Neuroendocrinology of the menstrual cycle in humans. Clinics in Endocrinology and Metabolism, 7(3), 531–559. [DOI:10.1016/S0300-595X(78)80008-5]
Shahiwala, A., Mehta, T. A., & Momin, M. M. (2018). Parenteral drug delivery systems. In Misra, A., & Shahiwala, A. (Eds.). In-Vitro and In-Vivo Tools in Drug Delivery Research for Optimum Clinical Outcomes (pp. 283–318). Boca Raton: CRC Press. [DOI:10.1201/b22448-9] [Google Books]
Sherwin, B. B., & Gelfand, M. M. (1987). Individual differences in mood with menopausal replacement therapy: Possible role of sex hormone-binding globulin. Journal of Psychosomatic Obstetrics & Gynecology, 6(2), 121–131. [DOI:10.3109/01674828709016773]
Sherwin, B. B., Gelfand, M. M., Schucher, R., & Gabor, J. (1987). Postmenopausal estrogen and androgen replacement and lipoprotein lipid concentrations. American Journal of Obstetrics and Gynecology, 156(2), 414–419. [DOI:10.1016/0002-9378(87)90295-X]
Sherwin, B. B. (1988). Affective changes with estrogen and androgen replacement therapy in surgically menopausal women. Journal of Affective Disorders, 14(2), 177–187. [DOI:10.1016/0165-0327(88)90061-4]
Sierra-Ramírez, J. A., Lara-Ricalde, R., Lujan, M., Velázquez-Ramírez, N., Godínez-Victoria, M., Hernádez-Munguía, I. A., Padilla, A., & Garza-Flores, J. (2011). Comparative pharmacokinetics and pharmacodynamics after subcutaneous and intramuscular administration of medroxyprogesterone acetate (25 mg) and estradiol cypionate (5 mg). Contraception, 84(6), 565–570. [DOI:10.1016/j.contraception.2011.03.014]
Sinkula, A. A. (1978). Methods to Achieve Sustained Drug Delivery. The Chemical Approach. In Robinson, J. R. (Ed.). Sustained and Controlled Release Drug Delivery Systems (pp. 411–555). New York/Basel: Marcel Dekker. [Google Scholar] [Google Books] [PDF]
Slack, D. J., Di Via Ioschpe, A., Saturno, M., Kihuwa-Mani, S., Amakiri, U. O., Guerra, D., Karim, S., & Safer, J. D. (2025). Examining the Influence of the Route of Administration and Dose of Estradiol on Serum Estradiol and Testosterone Levels in Feminizing Gender-Affirming Hormone Therapy. Endocrine Practice, 31(1), 19–27. [DOI:10.1016/j.eprac.2024.10.002]
Somerville, B. W. (1971). The Role of Oestradiol in Menstrual Migraine. In Somerville, B. W. The Influence of Progesterone and Oestradiol on Migraine (Doctoral dissertation, University of New South Wales) (pp. 93–104). [Google Scholar] [URL] [WorldCat] [PDF]
Somerville, B. W. (1972). The Role of Estradiol Withdrawal in the Etiology of Menstrual Migraine. Neurology, 22(4), 355–365. [DOI:10.1212/WNL.22.4.355]
Somerville, B. W. (1972). The influence of progesterone and estradiol upon migraine. Headache: The Journal of Head and Face Pain, 12(3), 93–102. [DOI:10.1111/j.1526-4610.1972.hed1203093.x]
Somerville, B. W. (1972). The Influence of Hormones Upon Migraine in Women. Medical Journal of Australia, 2(S2), 6–11. [DOI:10.5694/j.1326-5377.1972.tb93039.x]
Somerville, B. W. (1975). Estrogen‐withdrawal migraine: I. Duration of exposure required and attempted prophylaxis by premenstrual estrogen administration. Neurology, 25(3), 239–244. [DOI:10.1212/wnl.25.3.239]
Spack, N. P. (2013). Management of transgenderism. JAMA, 309(5), 478–484. [DOI:10.1001/jama.2012.165234]
Stege, R., Carlström, K., Collste, L., Eriksson, A., Henriksson, P., & Pousette, A. (1988). Single drug polyestradiol phosphate therapy in prostatic cancer. American Journal of Clinical Oncology, 11(Suppl 2), S101–S103. [DOI:10.1097/00000421-198801102-00024] [PDF]
Stege, R., Carlström, K., Collste, L., Eriksson, A., Henriksson, P., Pousette, Å., & von Schoultz, B. (1989). Single‐drug parenteral estrogen treatment in prostatic cancer: A study of two maintenance‐dose regimens. The Prostate, 14(2), 183–188. [DOI:10.1002/pros.2990140211]
Stege, R., Gunnarsson, P. O., Johansson, C. J., Olsson, P., Pousette, Å., & Carlström, K. (1996). Pharmacokinetics and testosterone suppression of a single dose of polyestradiol phosphate (Estradurin®) in prostatic cancer patients. The Prostate, 28(5), 307–310. [DOI:10.1002/(SICI)1097-0045(199605)28:5<307::AID-PROS6>3.0.CO;2-8]
Sumioki, H. (1987). ヒト排卵機構とGonadotropin分泌調節における “β-Endorphinおよびβ-Lipotropin” の役割に関する研究. [The Role of “β-Endorphin & β-Lipotropin” on the Gonadotropin Regulation in the Mechanism of Human Ovulation.] Folia Endocrinologica Japonica, 63(10), 1289–1307. [DOI:10.1507/endocrine1927.63.10_1289]
Svendsen, O., & Aaes‐Jørgensen, T. (1979). Studies on the fate of vegetable oil after intramuscular injection into experimental animals. Acta Pharmacologica et Toxicologica, 45(5), 352–378. [DOI:10.1111/j.1600-0773.1979.tb02404.x]
Tassinari, R., & Maranghi, F. (2021). Rodent Model of Gender-Affirming Hormone Therapies as Specific Tool for Identifying Susceptibility and Vulnerability of Transgender People and Future Applications for Risk Assessment. International Journal of Environmental Research and Public Health, 18(23), 12640. [DOI:10.3390/ijerph182312640]
Thurman, A., Kimble, T., Hall, P., Schwartz, J. L., & Archer, D. F. (2013). Medroxyprogesterone acetate and estradiol cypionate injectable suspension (Cyclofem) monthly contraceptive injection: steady-state pharmacokinetics. Contraception, 87(6), 738–743. [DOI:10.1016/j.contraception.2012.11.010]
Toffoli Ribeiro, C., Gois, Í., da Rosa Borges, M., Ferreira, L. G. A., Brandão Vasco, M., Ferreira, J. G., Maia, T. C., & Dias-da-Silva, M. R. (2024). Assessment of parenteral estradiol and dihydroxyprogesterone use among other feminizing regimens for transgender women: insights on satisfaction with breast development from community-based healthcare services. Annals of Medicine, 56(1), 2406458. [DOI:10.1080/07853890.2024.2406458]
Toppozada, M. K. (1994). Existing once-a-month combined injectable contraceptives. Contraception, 49(4), 293–301. [DOI:10.1016/0010-7824(94)90029-9]
Toutain, P. L., & Bousquet-Mélou, A. (2004). Plasma terminal half-life. Journal of Veterinary Pharmacology and Therapeutics, 27(6), 427–439. [DOI:10.1111/j.1365-2885.2004.00600.x]
Trans Care BC. (2021). Gender-affirming Care for Trans, Two-Spirit, and Gender Diverse Patients in BC: A Primary Care Toolkit. Vancouver: Provincial Health Services Authority/Trans Care BC. [URL] [PDF]
Travaglini, P., Ambrosi, B., Beck-Peccoz, P., Elli, R., Rondena, M., Bara, R., & Weber, G. (1978). Hypothalamic-pituitary-ovarian function in hyperprolactinemic women. Journal of Endocrinological Investigation, 1(1), 39–45. [DOI:10.1007/BF03346769]
Travaglini, P., Elli, R., Ambrosi, B., Ballabio, M., Moriondo, P., & Faglia, G. (1979). Serum LH increase after estradiol and progesterone administration in hyperprolactinemic women. Journal of Endocrinological Investigation, 2(4), 407–411. [DOI:10.1007/BF03349341]
T’Sjoen, G., Arcelus, J., De Vries, A. L., Fisher, A. D., Nieder, T. O., Özer, M., & Motmans, J. (2020). European Society for Sexual Medicine position statement “assessment and hormonal management in adolescent and adult trans people, with attention for sexual function and satisfaction”. The Journal of Sexual Medicine, 17(4), 570–584. [DOI:10.1016/j.jsxm.2020.01.012]
Ulrich, U., Pfeifer, T., & Lauritzen, C. (1994). Rapid Increase in Lumbar Spine Bone Density in Osteopenic Women by High-Dose Intramuscular Estrogen-Progestogen Injections. Hormone and Metabolic Research, 26(9), 428–431. [DOI:10.1055/s-2007-1001723]
Välimäki, M., Pelkonen, R., Salaspuro, M., Härkönen, M., Hirvonen, E., & Ylikahri, R. (1984). Sex hormones in amenorrheic women with alcoholic liver disease. The Journal of Clinical Endocrinology and Metabolism, 59(1), 133–138. [DOI:10.1210/jcem-59-1-133]
Valle Alvarez, D. C. (2011). Efecto de una Dosis de 50 mg de Enantato de Noretisterona y 5 mg de Valerato de Estradiol en los Niveles de Testosterona Total en Hombres Mexicanos Sanos. [Effect of a Dose of 50 mg of Norethisterone Enanthate and 5 mg of Estradiol Valerate on Total Testosterone Levels in Healthy Mexican Men.] (Masters thesis, National Polytechnic Institute of Mexico.) [Google Scholar] [URL] [PDF] [Translation]
Varangot, J., & Cedard, L. (1957). Modifications des Œstrogènes Sanguins Après Administration Intramusculaire de Benzoate d’Œstradiol. [Changes in Serum Estrogens After Intramuscular Administration of Estradiol Benzoate.] Comptes Rendus des Séances de la Société de Biologie et de ses Filiales, 151(10), 1707–1712. [Google Scholar 1] [Google Scholar 2] [PubMed] [PDF] [Translation]
Vermeulen, A. (1977). Transport and Distribution of Androgens at Different Ages. In Martini, L., & Motta, M. (Eds.). Androgens and Antiandrogens (pp. 53–65). New York: Raven Press. [Google Scholar] [Google Books] [OpenLibrary] [WorldCat] [Archive.org] [Excerpt]
Vhora, I., Bardoliwala, D., Ranamalla, S. R., & Javia, A. (2019). Parenteral controlled and prolonged drug delivery systems: therapeutic needs and formulation strategies. In Misra A., & Shahiwala, A. (Eds.). Novel Drug Delivery Technologies (pp. 183–260). Singapore: Springer. [DOI:10.1007/978-981-13-3642-3_7]
Vizziello, G., D’Amato, G., Trentadue, R., & Fanizza, G. (1993). Studio dinamico del blocco ipofisario indotto dalla triptorelina, mediante test all’estradiolo benzoato. [Estradiol benzoate test in the study of pituitary block induced by triptorelin.] Minerva Ginecologica, 45(4), 185–189. [Google Scholar] [PubMed] [PDF] [Translation]
Wagner, J. G. (1993). Pharmacokinetics for the Pharmaceutical Scientist. Lancaster/Basel: Technomic. [DOI:10.1201/9780203743652] [Google Books]
Weiss, G., Nachtigall, L. E., & Ganguly, M. (1976). Induction of an LH surge with estradiol benzoate. A clinical test of pituitary-hypothalamic axis competence. Obstetrics and Gynecology, 47(4), 415–418. [URL]
White, M. C., Rosenstock, J., Anapliotou, M., Mashiter, K., & Joplin, G. F. (1981). Heterogeneity of prolactin responses to oestradiol benzoate in women with prolactinomas. The Lancet, 317(8235), 1394–1396. [DOI:10.1016/S0140-6736(81)92571-X]
Wiemeyer, J. C., Fernandez, M., Moguilevsky, J. A., & Sagasta, C. L. (1986). Pharmacokinetic Studies of Estradiol Enantate in Menopausic Women. Arzneimittel-Forschung, 36(11), 1674–1677. [Google Scholar] [PubMed] [PDF]
Wiemeyer, J. C., Fernandez, M., Sagasta, C. L., & Moguilevsky, J. A. (1987). Estudos farmacocinéticos do enantato de estradiol em mulheres na menopausa. [Pharmacokinetic studies of estradiol enantate in menopausic women.] Jornal Brasileiro de Ginecologia, 97(9), 497–501. [Google Scholar] [LILACS] [PDF]
Yan, J., Pan, J., Chang, Y., & Kang, J. (1987). The effect of monthly injectable contraceptive megestrol acetate compound on pituitary-ovarian function. 上海第二医科大学学报(英文版) / Journal of Shanghai Second Medical University / Medical Bulletin of Shanghai Jiaotong University, 1(2), 7–12. [Google Scholar] [CNKI] [PDF]
Yáñez, J. A., Remsberg, C. M., Sayre, C. L., Forrest, M. L., & Davies, N. M. (2011). Flip-flop pharmacokinetics–delivering a reversal of disposition: challenges and opportunities during drug development. Therapeutic Delivery, 2(5), 643–672. [DOI:10.4155/tde.11.19]
Zhang, Y., Huo, M., Zhou, J., & Xie, S. (2010). PKSolver: An add-in program for pharmacokinetic and pharmacodynamic data analysis in Microsoft Excel. Computer Methods and Programs in Biomedicine, 99(3), 306–314. [DOI:10.1016/j.cmpb.2010.01.007]
Zhou, X. F., Shao, Q. X., Han, X. J., Weng, L. J., & Sang, G. W. (1998). Pharmacokinetics of medroxyprogesterone acetate after single and multiple injection of Cyclofem® in Chinese women. Contraception, 57(6), 405–411. [DOI:10.1016/S0010-7824(98)00048-1]
\ No newline at end of file
diff --git a/transfemscience.org/articles/nandrolone/index.html b/transfemscience.org/articles/nandrolone/index.html
index 317ca0b3..01a58717 100644
--- a/transfemscience.org/articles/nandrolone/index.html
+++ b/transfemscience.org/articles/nandrolone/index.html
@@ -1 +1 @@
-Nandrolone as a Potential Alternative Androgen with Reduced Androgenic Side Effects for Transfeminine and Transmasculine People - Transfeminine Science
Nandrolone as a Potential Alternative Androgen with Reduced Androgenic Side Effects for Transfeminine and Transmasculine People
By Aly | First published March 20, 2020 | Last modified March 23, 2023
Abstract / TL;DR
Nandrolone, or 19-nortestosterone, is a unique androgen and anabolic steroid which is used in the form of injectable ester prodrugs like nandrolone decanoate. It is closely related to testosterone structurally but has a number of important pharmacological differences in comparison. These differences include inactivation by 5α-reductase rather than potentiation, less or no conversion into estradiol, and much greater progestogenic activity. The inactivation of nandrolone by 5α-reductase results in nandrolone theoretically having much lower androgenic strength than testosterone in skin, hair follicles, and the prostate, among other tissues. Consequently, nandrolone may have less propensity for oily skin, acne, facial/body hair growth, scalp hair loss, and prostate problems than testosterone. On the other hand, nandrolone is theoretically expected to have full androgenic efficacy in most other tissues, including bone, fat, and muscle (and hence of masculine skeletal, fat, and muscular changes). This is also likely to be the case when it comes to voice, bottom growth, and sexual function. The reduced androgenic impact of nandrolone in skin and hair follicles relative to testosterone make it a favorable potential alternative option for androgen therapy both for transfeminine people and for some transmasculine people.
Introduction
Nandrolone, also known chemically as 19-nortestosterone (19-NT), is an androgen and anabolic steroid (AAS) similarly to testosterone (T). It is used as a medication by intramuscular or subcutaneous injection in the form of longer-acting esters like nandrolone decanoate (ND; Deca-Durabolin) and nandrolone phenylpropionate (NPP; Durabolin), which are converted into nandrolone in the body. This is analogous to longer-acting testosterone esters like testosterone enanthate (TE) and testosterone undecanoate (TU) and their conversion in the body into testosterone. Nandrolone is used in medicine for a variety of indications that benefit from anabolic effects in tissues like muscle, bone, and kidneys. Examples include wasting syndromes, osteoporosis, kidney disease, and anemia. It is used not only in men but also in women, for instance to prevent and treat postmenopausal osteoporosis in women who can’t tolerate estrogens or in whom estrogens can’t be taken. Nandrolone has additionally been advocated for use in androgen replacement therapy for women (Davis, 1999).
Nandrolone is closely related to testosterone in terms of chemical structure, pharmacodynamic actions, and disposition in the body. At the same time however, nandrolone has a key difference from testosterone that makes it a very favorable alternative option for use as an androgen in transgender hormone therapy. This is the case not only for transfeminine people but also for transmasculine people. This property of nandrolone is that it is inactivated by 5α-reductase in tissues that express this enzyme. This is in contrast to testosterone, which is potentiated in such tissues via conversion into dihydrotestosterone (DHT). Because of this difference, nandrolone has normal androgenic effects in most of the body but a greatly reduced potential for androgenic effects in skin and hair follicles relative to testosterone. As a result, nandrolone has a variably reduced potential for androgenic skin and hair side effects such as oily skin, acne, facial and body hair growth, and scalp hair loss.
Because of its favorable profile relative to testosterone, nandrolone has been advocated for use in androgen replacement therapy in cisgender men (Wu & Kovac, 2016; Pan & Kovac, 2016). It has also been studied for use in male hormonal contraception as an alternative and replacement for testosterone (Knuth et al., 1986; Nieschlag, 2010; Nieschlag & Behre, 2012). Nandrolone is advantageous for cisgender men not only due to preservation of scalp hair but also due to its lower stimulation of the prostate gland. As a result of its more favorable profile in terms of skin and hair follicles, nandrolone is an underappreciated alternative possibility relative to testosterone for use not only in cisgender people but also in transfeminine and transmasculine people.
Chemistry of Nandrolone
Nandrolone is chemically known as 19-nortestosterone. It is very close to testosterone in terms of chemical structure, the only difference between the two compounds being that the C19 methyl group of testosterone has been removed in the case of nandrolone. Nandrolone is not a synthetic compound; it occurs naturally in the human body in trace amounts as an intermediate in the conversion of testosterone to estradiol by the enzyme aromatase (Bricout & White, 2004). As such, although nandrolone couldn’t be said to be “bioidentical”, it’s quite similar to testosterone.
Figure: Chemical structures of testosterone and nandrolone (19-nortestosterone). The structural difference between testosterone and nandrolone is at the C19 position and is highlighted by the circled areas.
Nandrolone is an agonist of the androgen receptor (AR) similarly to testosterone. It shows higher affinity for the AR than does testosterone and has almost no binding affinity for sex hormone-binding globulin (SHBG) however. For these reasons, nandrolone has about 2.5- to 5-fold higher potency than testosterone in rats on measures of general AR agonistic strength, such as stimulation of muscle growth (Sundaram et al., 1995; Tóth & Zakár, 1986; Wiki; Winters, 1976). It is likewise a more potent AAS than testosterone in humans, and is used medically at lower doses in comparison (Wiki).
Testosterone is a substrate for 5α-reductase in tissues that express this enzyme like skin, hair follicles, prostate gland, and seminal vesicles, among others. It is converted by 5α-reductase into dihydrotestosterone (DHT), an androgen with much higher AR affinity and AR agonistic potency than that of testosterone (Wiki). Consequently, it is estimated that the effects of testosterone are potentiated by 2- to 3-fold via conversion into DHT in tissues that express 5α-reductase (Sundaram et al., 1995). The role of DHT in the effects of testosterone is demonstrated by a rare intersex condition known as 5α-reductase type 2 deficiency, as well as by 5α-reductase inhibitors (5α-RIs) like finasteride and dutasteride (Wiki; Wiki). Men with 5α-reductase type 2 deficiency are reported to have reduced facial hair, a female-like pattern of body hair (with terminal hair largely restricted to the underarms and lower pubic triangle), and no scalp hair recession in the temples nor scalp hair loss in general. Conversely, other aspects of male secondary sexual development, like voice deepening, muscle growth, bone changes, and pubertal penile enlargement, are all normal in the condition. In addition, no feminization or gynecomastia occurs. Hence, adults with 5α-reductase type 2 deficiency have a masculine appearance (Imperato-McGinley & Peterson, 1976; Peterson et al., 1977; Photos). In published photographs of individuals with the condition however, features like lack of body hair and rounded feminine hairlines can be noted.
5α-Reductase inhibitors have similar effects relative to the profile of 5α-reductase type 2 deficiency. For this reason, they are used in the treatment and prevention of scalp hair loss in men and off-label for hirsutism (excessive facial/body hair growth) in women. They greatly slow the rate of scalp hair loss over time in men. For example, a large 5-year randomized controlled trial showed that in men with diagnosed scalp hair loss, 100% of those who received placebo had significant further scalp hair loss whereas only 35% of those who received finasteride had further scalp hair loss (Propecia label). Low-quality evidence suggests that finasteride has similar effectiveness to antiandrogens like spironolactone and flutamide in the treatment of hirsutism in women (Barrionuevo et al., 2018; van Zuuren et al., 2015). Dutasteride has similar or greater effectiveness than finasteride for scalp hair loss in men (Arif et al., 2017), whereas it hasn’t yet been studied in the treatment of hirsutism (Wiki).
5α-Reductase is the key to the favorable differences between testosterone and nandrolone. Both testosterone and nandrolone are substrates for 5α-reductase and have similar affinity for this enzyme (Tóth & Zakár, 1986). But whereas testosterone is potentiated via conversion into DHT in tissues that express 5α-reductase, nandrolone is inactivated by 5α-reductase in these tissues (Kicman, 2008; Tóth, 2009). This is because the 5α-reduced metabolite of nandrolone, 5α-dihydronandrolone (DHN), is a weaker AR agonist with much lower affinity for the AR than nandrolone (Tóth & Zakár, 1986; Kumar et al., 1999). The following table shows AR and SHBG relative binding affinities (RBA) of testosterone, nandrolone, trestolone, and their 5α-reduced forms (Kumar et al., 1999):
Steroid
AR RBA
SHBG RBA
Testosterone
100%
100%
5α-Dihydrotestosterone
290%
340%
Nandrolone
230%
5%
5α-Dihydronandrolone
10%
5%
Trestolone
380%
6%
5α-Dihydrotrestolone
30%
2%
In rodents, although nandrolone has about 3-fold higher anabolic or muscle-stimulating potency than testosterone, its androgenic potency in the prostate gland and seminal vesicles is only about 20 to 40% of that of testosterone (Sundaram et al., 1995; Tóth & Zakár, 1986; Wiki). This works out to an approximate 11:1 dissociation between the effects of nandrolone in tissues with little or no 5α-reductase (muscle) versus with high 5α-reductase (prostate gland, seminal vesicles) in rodents (Wiki). The exact ratio of potency between these tissues in humans is unknown, and extrapolation from rodents should be cautioned against. In any case, an analogous dissociation of some level can be anticipated. As such, nandrolone can be expected to have high AR agonistic strength in most of the body, where 5α-reductase has minimal expression (e.g., fat, muscle, bone), but much lower potency in tissues with high 5α-reductase expression, like skin, hair follicles, the prostate gland, and the seminal vesicles.
It’s important to be clear that nandrolone is not simply akin to taking testosterone with a 5α-reductase inhibitor like dutasteride to block 5α-reductase. This is because nandrolone isn’t merely not potentiated by 5α-reductase, it’s weakened by 5α-reductase. For this reason, 5α-reductase inhibitors actually increase the androgenic strength of nandrolone in tissues that express 5α-reductase like the prostate gland in rodents (Sundaram et al., 1995). (And, for this reason, nandrolone should not be taken with a 5α-reductase inhibitor, in contrast to testosterone.) In other words, nandrolone goes beyond testosterone plus a 5α-reductase inhibitor in terms of the dissociation of its potency between tissues that express 5α-reductase and tissues that do not. As a result, nandrolone has much lower androgenic strength in such tissues than does the combination of testosterone plus a 5α-reductase inhibitor. Nandrolone also appears to have lower strength in tissues that express 5α-reductase than do most other AAS, for instance synthetic DHT derivatives like oxandrolone and stanozolol (Tóth & Zakár, 1986). This is because these AAS are not substrates for 5α-reductase and hence are neither potentiated nor weakened by 5α-reductase, similarly to testosterone with a 5α-reductase inhibitor. The inactivation of nandrolone by 5α-reductase makes it very unique among AAS and AR agonists. Only nandrolone and a few of its derivatives like normethandrone and norethandrolone have this very special property.
Testosterone and nandrolone may also be non-identical in their androgenic actions and effects for reasons other than metabolism. This is because different AR agonists including strong androgens like testosterone and DHT, weak androgens like dehydroepiandrosterone (DHEA) and androstenedione (A4), and predominantly anabolic androgens like nandrolone, oxandrolone, and stanozolol, have been shown to produce differential AR-mediated changes in gene expression (Holterhus, Piefke, & Hiort, 2002; Kicman, 2008; Hiort, 2013). However, nandrolone was more similar in its profile to testosterone than the synthetic AAS. In any case, the clinical implications of these differences in relation to therapeutic use of testosterone versus nandrolone, if any, are unknown.
In relation to the fact that nandrolone is an intermediate in the aromatase-mediated reaction that converts testosterone into estradiol, both testosterone and nandrolone are transformed into estradiol, and hence estradiol is their specific estrogen metabolite. Paradoxically however, whereas it has the same potential for 5α-reduction as testosterone, nandrolone as a medication is aromatized into estradiol virtually not at all (Handelsman, 2016). In accordance, nandrolone suppresses estradiol levels in men and results in low estradiol levels even at very high doses (Friedl, 1991; Hobbs et al., 1993; Hobbs, Jones, & Plymate, 1996; Behre et al., 2001). The following table gives an example of estradiol (E2) levels in men with high-dose testosterone versus high-dose nandrolone (Friedl, 1991):
Drug and dose
E2 before
E2 after
Change
Testosterone enanthate 300 mg/week i.m.
32 ± 4.6 pg/mL
79 ± 9.3 pg/mL
+147%
Nandrolone decanoate 300 mg/week i.m.
40 ± 6.0 pg/mL
14 ± 1.6 pg/mL
–65%
Testosterone and nandrolone themselves don’t have significant affinity for the estrogen receptors nor intrinsic estrogenic activity outside of aromatization to estradiol (Kuiper et al., 1997; Table). Although androgens also help to maintain bone mineral density and AAS like nandrolone are used to treat osteoporosis in postmenopausal women (Geusens, 1995; Ebeling, 2010), estrogens are comparatively much more important for maintenance of bone mineral density and prevention of osteoporosis in both men and women (Wiki). Studies of high-dose nandrolone and androstanolone (DHT) have shown that these non-aromatizable AAS are not adequate for maintenance of bone mineral density in men, whereas the aromatizable testosterone is effective for such purposes (Ronald et al., 1998; Crawford et al., 2003; Lemmey et al., 2013; Sartorius, Ly, & Handelsman, 2014; Čeponis et al., 2017). Non-aromatizable AAS are likewise inferior to estrogen and estrogen–progestogen therapy for maintaining bone mineral density in postmenopausal women (Lauritzen, 1984 [Graph]; Hassager et al., 1991).
Because of its minimal conversion into estradiol, nandrolone should be used as an androgen in transmasculine people only in combination with low-dose estradiol to replace the lost estradiol that would otherwise be provided by testosterone. Estradiol levels in men are on average around 30 pg/mL, and estradiol levels of at least 20 to 30 pg/mL appear to be necessary for maintenance of bone density in men (Doran et al., 2001). A low-dose transdermal estradiol patch, for instance 14 to 25 μg/day, is likely to be adequate for achieving such levels. Alternatively, another option like transdermal estradiol gel (e.g., 0.75–1 mg/day) or low-dose oral estradiol (e.g., 0.5–1 mg/day) may be used instead.
Nandrolone likewise has progestogenic activity. However, the progestogenic activity of nandrolone is greatly enhanced relative to that of testosterone. The affinity of nandrolone for the PR is 5- to 20-fold higher than that of testosterone and its progestogenic potency is correspondingly improved (Wiki; Wiki; Bardin & Janne, 1986). Despite this however, the progestogenic potency of nandrolone is still relatively low. For instance, its affinity for the PR is only about 10 to 20% of that of progesterone and the nandrolone-derived progestin norethisterone (also known as 17α-ethynyl-19-nortestosterone). At the same time however, nandrolone is used at relatively large doses compared to norethisterone. This may help to compensate for its lower progestogenic potency and may allow for significant progestogenic effects at typical clinical doses (Camerino & Sciaky, 1975).
The following table shows human and rabbit PR RBAs and relative progestogenic activity (as measured by in-vivo induction of uteroglobin synthesis in rabbit uterus) of progesterone and several AAS including testosterone and nandrolone (Jänne et al., 1978; Bardin & Janne, 1986):
Steroid
hPR RBA
rbPR RBA
Progestogenic activity (rabbit)
Progesterone
100%
100%
100%
Testosterone
1.6%
1.6%
0.9%
Dihydrotestosterone
3.3%
3.3%
1.9%
Nandrolone
8.9%
12%
5.2%
Methyltestosterone
4.6%
3.4%
0.6%
Norethandrolone
130%
70%
115%
The development of nandrolone was an intermediate step in the eventual development of the 19-nortestosterone group of progestins, which are widely used in hormonal birth control. These include progestins like norethisterone and levonorgestrel, among many others.
Advantages of Nandrolone Over Testosterone
Because of its substantially lower androgenic strength in tissues that have high 5α-reductase expression relative to tissues that have minimal or no 5α-reductase expression, nandrolone is likely to have normal androgenic effects in muscle, bone, fat, and most other tissues but much weaker androgenic strength in skin and hair follicles than equivalent doses of testosterone. As a result of this, although nandrolone has high capacity for producing most aspects of masculinization, it has a lower potential for many of the undesirable androgenic skin and hair side effects of testosterone, including oily skin, acne, facial and body hair growth, and scalp hair loss. This may allow for unique advantages of nandrolone over testosterone in transfeminine and transmasculine hormone therapy.
The benefits of nandrolone are expected to partially differ in transfeminine people relative to transmasculine people however. This is due to the different doses of nandrolone used in these individuals, namely low, female replacement doses in transfeminine people and full, male replacement doses in transmasculine people. As an example, transmasculine people taking full male androgen replacement doses should probably expect no less oily skin or acne with nandrolone than with testosterone. This is because very low levels of testosterone are necessary for such effects, as evidenced by the fact that acne prevalence and severity is similar in females compared to males (Skroza et al., 2018) despite the fact that testosterone levels are 20-fold lower in women than in men (Styne & Grumbach, 2016). Conversely, transfeminine people taking nandrolone at doses equivalent to the effect of testosterone levels in the normal female range may experience less or possibly no oily skin or acne with nandrolone compared to use of testosterone instead. This is due to the equivalent testosterone levels being far closer to the biological threshold for manifestation of such effects.
Nandrolone can be anticipated to have far less potential for scalp hair loss relative to testosterone in transmasculine people (Wu & Kovac, 2016; Pan & Kovac, 2016). This is related to the lack of scalp hair loss in men with 5α-reductase type 2 deficiency and the high effectiveness of 5α-reductase inhibitors for scalp hair loss. However, nandrolone is theoretically even better than testosterone plus a 5α-reductase inhibitor when it comes to preservation of scalp hair. This is because again, nandrolone is not simply not potentiated, but is inactivated in tissues that express 5α-reductase. Nandrolone replacement of testosterone represents a highly promising treatment for scalp hair loss in men that offers potentially superior effectiveness to 5α-reductase inhibitors. Moreover, since nandrolone isn’t an inhibitor of 5α-reductase, it doesn’t interfere with 5α-reduced neurosteroid synthesis. Hence, nandrolone doesn’t have the possible psychiatric side effects that have been associated with 5α-reductase inhibitors, for instance depression (Irwig, 2015; Kuhl & Wiegratz, 2017; Wiki).
On the basis of 5α-reductase type 2 deficiency, nandrolone may be expected to produce reduced facial and particularly body hair growth relative to testosterone in transmasculine people. Essentially no body or facial hair growth is likely to occur with nandrolone at doses equivalent to female-range testosterone levels in transfeminine people, and even at supraphysiological levels, facial and body hair growth is likely to be less than with testosterone. However, facial and body hirsutism have nonetheless been reported with nandrolone at postmenopausal osteoporosis doses (Need et al., 1989; Passeri et al., 1993; Geusens, 1995; Flicker et al., 1997).
For transmasculine people who want the benefits of nandrolone except the lesser facial hair growth, topical testosterone to the beard area can potentially be used in conjunction with nandrolone injections to restore full facial hair growth. Another possibility for achieving effects of both testosterone and nandrolone in transmasculine people could be to start on testosterone and use it for a few years, allowing for facial/body hair growth and hairline masculinization, and then switch from testosterone to nandrolone for long-term therapy, allowing for preservation of scalp hair.
One of the reasons that nandrolone is attractive for androgen replacement therapy in cisgender men is that it has very weak relative effects in the prostate gland compared to testosterone. This is due to inactivation of nandrolone in the prostate gland by 5α-reductase similarly to other tissues that express this enzyme. It is anticipated that long-term androgen replacement therapy with nandrolone might allow for a reduced risk of enlarged prostate and prostate cancer compared to testosterone in men (Wu & Kovac, 2016; Pan & Kovac, 2016). As transfeminine people also have prostate glands, the weak effects of nandrolone in the prostate are potentially of relevance to us as well. However, due to estrogen therapy and androgen deprivation, the prostate is atrophied in transfeminine people and prostate cancer is very rare (Wiki). In relation to this, the favorable prostate profile of nandrolone may be of little significance for transfeminine people.
Although nandrolone is quite promising for transgender hormone therapy, it is important to be clear that there are currently no quality clinical studies comparing it to testosterone and showing that it is less androgenic in terms of skin and hair effects (even if there is strong theoretical basis for this notion, particularly in the case of scalp hair loss). Nor are there any studies demonstrating with certainty that it is as effective as testosterone in terms of inducing general masculinization. Moreover, the appropriate dosages of nandrolone for use in androgen replacement in women and men are uncertain. Finally, nandrolone has been little-studied for androgen replacement and its long-term tolerability and health safety for this use haven’t been properly characterized. For these reasons, androgen replacement with nandrolone in cisgender men and transmasculine people is an experimental therapy. Additional research is needed to properly characterize nandrolone for this indication.
Androgen Replacement in Transfeminine People
Some believe that testosterone is important in women for mood, well-being, energy, sexual desire and function, general health, and for other reasons. Androgen levels and activity may be low in many transfeminine people due to hormone therapy and/or gonadectomy, raising concerns about androgen deficiency. However, there is little or no change in androgen levels with natural menopause in cisgender women and only a small decrease in androgen levels with ovariectomy in women (Liu & Handelsman, 1998). Moreover, there is inadequate evidence to support claims of benefit with androgen replacement therapy in women at present, and there are no well-supported benefits of female-range doses of testosterone (Wiki). For these reasons, androgen replacement therapy in women is controversial (Liu & Handelsman, 1998).
Testosterone does stimulate sexual desire in women, but only at levels that are above the normal female range (>50 ng/dL) (Cappelletti & Wallen, 2016; Wiki). And even with high testosterone levels of 80 to 150 ng/dL, stimulation of sexual desire in women is modest (Cappelletti & Wallen, 2016; Wiki). It is likely that estradiol rather than testosterone (or progesterone) is the key sex hormone for sexual desire in women (Cappelletti & Wallen, 2016; Aly, 2020).
Androgens can have detrimental effects in transfeminine people. They can cause androgenic and masculinizing effects like oily skin, acne, seborrhea, facial/body hair growth, scalp hair loss, and voice deepening, among others. In addition, androgens oppose the effects of estrogens in the breasts, and may inhibit breast development even with low-level exposure or physiological levels in females (Dimitrakakis et al., 2003; Peters et al., 2011; Sas et al., 2014; Barbieri, 2017).
For these reasons, transfeminine people don’t necessarily require androgen replacement, and it shouldn’t be routinely used out of concern of androgen deficiency. In any case, some transfeminine people insist on androgen replacement, and others desire supraphysiological levels of androgens for purposes like stimulating libido or helping to build and maintain muscle mass. There is some evidence that even physiological levels of testosterone may help to support muscle mass in women (Huang & Basaria, 2017). Moreover, in transfeminine people who are fully hormonally transitioned, breast development is complete, and hence inhibition of the breasts by androgens is no longer a concern. Another potentially useful indication of androgens in transfeminine people is to counteract cellulite (Wiki; Gruber et al., 2002; Avram, 2004). Since nandrolone has full androgenic potential in fat tissue, it may be similarly effective as testosterone for this purpose. However, there are no good studies of androgens for treatment of cellulite at this time.
Although androgen replacement therapy isn’t recommended for cisgender women or transfeminine people because of a lack of evidence of benefit and potential adverse effects, nandrolone is a very favorable alternative to testosterone for such purposes in those who nonetheless opt for such therapy. This is due to its improved skin and hair profile and hence a probable lower risk of undesirable effects.
Additional Topics on Nandrolone
This section is for additional topics on nandrolone as an androgen in transfeminine and transmasculine people, including its availability, dosage, androgenic/masculinizing effects besides skin and hair (e.g., voice deepening, bottom growth/clitoral enlargement, sexual effects), and liver safety.
Availability of Nandrolone
Nandrolone esters remain widely available for medical use throughout the world (Drugs.com). However, the availability of AAS, including nandrolone esters, has become increasingly limited over time. The shorter-acting ester nandrolone phenylpropionate is no longer available in the United States or many other countries, and the more favorable longer-acting nandrolone decanoate was discontinued in the United States in 2019. However, nandrolone decanoate remains available from compounding pharmacies in the United States, for instance AnazaoHealth. It is only available from this particular pharmacy at a very high concentration of 200 mg/mL however, which although a potentially workable concentration for use in transmasculine people, is likely completely impractical for use in transfeminine people. Compounding pharmacies might be able to do custom concentrations upon request though.
Another potential means of delivering nandrolone is via an orally active nandrolone androgen prohormone like 19-nordehydroepiandrosterone (19-nor-DHEA). This compound is converted into nandrolone analogously to the use of DHEA as a prohormone of testosterone (Wiki). It is sold as an over-the-counter supplement from certain online vendors, similarly to DHEA. 19-Nor-DHEA may be a more suitable option for transfeminine people due to the lower doses needed and less suitable for transmasculine people due to the much higher doses required.
Dosage of Nandrolone
The dosage of nandrolone for use in androgen replacement therapy in women and men hasn’t been established. Hence, we don’t completely know what the appropriate dose is for use in transfeminine and transmasculine hormone therapy. In any case, it is possible for us to estimate.
One review recommended a clinical dose range in males of 50–400 mg/2–4 weeks for testosterone enanthate or cypionate but 50–100/3–4 weeks for nandrolone decanoate (Hickson et al., 1989). This is also in line with several-fold higher potency of nandrolone relative to testosterone.
Dosage for Transmasculine People
A typical dosage of testosterone enanthate for use in androgen replacement therapy in cisgender and transgender men is 50 to 100 mg once per week by intramuscular injection (Wiki; Wiki). Hence, an appropriate dosage of nandrolone decanoate, assuming 3-fold greater potency than testosterone, might be about 16.7 to 33.3 mg once per week by intramuscular injection (ignoring the small differences in molecular weight between testosterone enanthate and nandrolone decanoate). However, it must be emphasized that these doses are merely educated guesses. It’s notable that these doses are quite similar to those used in postmenopausal osteoporosis in women (about 12.5 to 25 mg per week total). Hence, although such doses have certainly been associated with masculinizing effects in women, they might be suboptimal in terms of masculinization for transmasculine people. Consequently, it’s possible that a higher dose, like 50 mg once per week, might be more appropriate. In addition to weekly use, nandrolone decanoate has a duration suitable for use once every 2 weeks (Graphs).
Nandrolone hexyloxyphenylpropionate (NHPP; brand name Anadur) was studied as a male hormonal contraceptive by the World Health Organization and others at a dose of 200 mg/3 weeks i.m. in combination with depot medroxyprogesterone acetate (Knuth et al., 1986; Nieschlag, 2010; Nieschlag & Behre, 2012). It was used as a replacement and alternative for testosterone and was given at a dosage of about 66.7 mg once per week. However, this was an intentionally supraphysiological dosage which was selected to achieve a male contraceptive effect, as suggested by suppression of gonadotropins to undetectable levels (Knuth et al., 1985). Hence, although safe and well-tolerated in limited studies, it might be a high dosage for transmasculine hormone therapy. Very high doses of nandrolone can reproduce the full spectrum of androgenic effects of testosterone, and hence doses of nandrolone that are too high may serve to nullify its advantages over testosterone (van der Vies, 1985).
Dosage for Transfeminine People
In postmenopausal women, nandrolone decanoate has been used for general androgen replacement at a dose of 25 to 50 mg once every 6 to 12 weeks (about 2–8 mg/week or 0.29–1.14 mg/day), and for prevention and treatment of osteoporosis at a dose of 50 mg once every 2 to 4 weeks (about 12.5–25 mg/week or 1.8–3.6 mg/day) (Wiki; Table). However, these doses of nandrolone decanoate are likely to be highly excessive for physiological androgen replacement in women and transfeminine people and are probably also spaced too widely in terms of dosing interval. This is based on the following: (1) normal production of testosterone in premenopausal women is about 150 μg/day; (2) nandrolone is more potent as an androgen receptor agonist than testosterone; and (3) pharmacokinetic concentration–time curves for nandrolone decanoate suggest that an appropriate dosing interval is once every 1 to 2 weeks (Graphs). Indeed, nandrolone decanoate at 50 mg/2–4 weeks has been found to produce significant masculinizing effects in women with long-term use (Geusens, 1995; Wiki). Since nandrolone has high theoretical masculinizing potential in most tissues in the body, like muscle, bone, fat, and vocal tissue, it’s very important that transfeminine people don’t take doses that are too large.
Androgenic and Masculinizing Effects Besides Skin and Hair
Nandrolone has sometimes been described as “non-masculinizing” or “minimally virilizing”, but this is misleading and inaccurate. Nandrolone has high theoretical potential to produce masculinizing skeletal, fat, and muscular effects, like growth of muscles, widening of shoulders, masculine enlargement, elongation, and shaping of bones, and masculine distribution of fat. It also has high capacity to produce voice deepening (the vocal tissue notably being part muscle). The only clear differences in masculinizing effect between nandrolone and testosterone are that nandrolone has a greatly reduced theoretical potential for androgenic effect in skin and hair follicles. Succinctly, nandrolone could be thought of as testosterone with minimization of the undesirable skin and hair effects.
Voice Deepening with Nandrolone
The vocal tissue, consisting of the vocal cords and the larynx, are part muscle, and 5α-reductase is expressed minimally or not at all in this tissue (Bhagavan, 2002; Kicman, 2008). Accordingly, voice deepening is normal in individuals with 5α-reductase type 2 deficiency (Imperato-McGinley & Zhu, 2002). As such, nandrolone would be expected to produce voice deepening similarly to testosterone. In accordance, voice deepening has been reported with nandrolone in women at doses used in postmenopausal osteoporosis (Gerritsma et al., 1994; Geusens, 1995; Frisoli et al., 2005). There are case reports of severe and complete masculinization of the voice in women treated with excessive doses of nandrolone (Damsté, 1964; Brodnitz, 1971; Baker, 1999). Voice changes have also been seen with nandrolone derivatives like normethandrone (Feldman et al., 1960).
Bottom Growth with Nandrolone
DHT is required for normal male sexual differentiation of the genitals during prenatal development. This is evidenced by 5α-reductase type 2 deficiency, in which the genitals are ambiguous but overall more female-like at birth and in childhood (Wiki). Although DHT is critical for prenatal genital masculinization, the same may not be true for pubertal development of the penis (Hiort, 2013). Individuals with 5α-reductase type 2 deficiency undergo masculinization of the genitals at puberty such that a small and near-functional penis develops (Peterson et al., 1977; Marks, 2004; Hiort, 2013; Photos). This is so striking that males with 5α-reductase type 2 deficiency in the Dominican Republic are referred to as “guevedoces”, which is said to literally mean “penis at 12”.
As 5α-reductase may not be critical for penile enlargement at puberty, nandrolone may allow for no less bottom growth (clitoral enlargement) in transmasculine people than does testosterone. Indeed, nandrolone has been reported to produce clitoral enlargement as a side effect in women and penile growth in prepubertal boys (Camerino & Sala, 1960; Camerino & Sciaky, 1975). Similar findings have been made for derivatives of nandrolone like normethandrone and norethandrolone (Feldman et al., 1960; Roche, Towns, & Wettenhall, 1963; Kirschvink et al., 1963; Prunty et al., 1958).
Since this article was published, a review suggesting nandrolone as a potential component of transgender hormone therapy for non-binary individuals has been published:
Cocchetti, C., Ristori, J., Romani, A., Maggi, M., & Fisher, A. D. (2020). Hormonal Treatment Strategies Tailored to Non-Binary Transgender Individuals. Journal of Clinical Medicine, 9(6), 1609. [DOI:10.3390/jcm9061609]
The review includes the following excerpts on nandrolone:
Other options may include nandrolone, an anabolic steroid administered via intramuscular injection, which is not as optimal a substrate for 5α-reductase as testosterone, but it has a stronger effect compared to the testosterone on target tissues devoid of 5α-reductase activity (e.g., muscular tissue) [15]. Indeed, nandrolone can be theoretically used in non-binary [assigned female at birth (AFAB)] individuals requesting masculinization of body shape (i.e., increased muscle mass) with a limited increase in facial and body hair. Regarding the safety profile of this compound, data are limited by the fact that most observations come from the setting of androgenic-anabolic steroid (AAS) abuse [16,17], thus their applicability to appropriate medical therapy is limited [18]. In this setting, concerns about cardiomyopathy and coronary artery disease risk emerged [19], although associated with the administration of nandrolone at extremely higher dosages [20]. Furthermore, nandrolone use does not seem associated to hepatotoxicity, since, as an injectable oil, it is not subject to first-pass hepatic metabolism.
Moreover, some AFAB transgender individuals can benefit from testosterone therapy combined with 5α-reductase inhibitors or from treatment with nandrolone (an androgenic compound less prone to 5α reduction) in case they wish only a partial virilization (i.e., voice deepening and lean mass increase without facial and body hair increase).
In addition to the above review, a second review suggesting nandrolone as a potential option for hormone therapy in non-binary individuals has been published (as a preprint):
Vetri, M., Cataldi, A., Naselli, A., & Vetri, A. (2021). Transsexualism Ethiology and Medical Management: Between Scientific Evidence and Personal Experiences. Preprints, 2021030172. [DOI:10.20944/preprints202103.0172.v1]:
With the following relevant excerpt:
In [female-to-males] (FtMs) requesting partial masculinization, it may be possible to reduce the dose of testosterone or substitute it with nandrolone, an anabolic steroid administered via intramuscular injection. So, we must accept alternative hormonal treatment regimens, other than those reported in current guidelines, for such nonbinary transgender individuals, to try to improve their psychological well-being and quality of life [40].
However, this preprint article appears to have never ended up being accepted for publication.
Update 3: Cocchetti et al. (2020) and Iuliano et al. (2021)
Further articles have mentioned nandrolone as a hypothetical option for transgender people, for instance Cocchetti et al. (2020):
Another hypothetic option [for management of hypoactive sexual desire disorder in transgender women] may include nandrolone, an androgenic compound administered via intramuscular injection, less prone to 5-alpha reduction anabolic steroid leading to limited virilizing dermatological undesired effects [72]. However, data on its efficacy on sexual desire are not yet available.
Actually, the classic view of gender binarism and [gender-affirming hormone therapy (GAHT)] should be reconsidered because of the increasing prevalence of non-binary individuals experiencing [gender dysphoria (GD)]. Therefore, new therapeutic strategies should be also considered [17]. Since there is a lack in standardized hormonal treatment protocols for non-binary [assigned female at birth (AFAB)], GAHT goals should be adjusted according to patients’ needs in order to improve the self-perception and the quality of life [18]. For instance, different testosterone doses and/or other androgen preparations (i.e., nandrolone) are suggested to modulate the requested body changes [18], even if serious ethical concerns on some drugs exist.
References
Anderson, R. A., Martin, C. W., Kung, A. W., Everington, D., Pun, T. C., Tan, K. C., Bancroft, J., Sundaram, K., Moo-Young, A. J., & Baird, D. T. (1999). 7α-Methyl-19-Nortestosterone Maintains Sexual Behavior and Mood in Hypogonadal Men. The Journal of Clinical Endocrinology & Metabolism, 84(10), 3556–3562. [DOI:10.1210/jcem.84.10.6028]
Anderson, R. A., Wallace, A. M., Sattar, N., Kumar, N., & Sundaram, K. (2003). Evidence for Tissue Selectivity of the Synthetic Androgen 7α-Methyl-19-Nortestosterone in Hypogonadal Men. The Journal of Clinical Endocrinology & Metabolism, 88(6), 2784–2793. [DOI:10.1210/jc.2002-021960]
Arif, T., Dorjay, K., Adil, M., & Sami, M. (2017). Dutasteride in Androgenetic Alopecia: An Update. Current Clinical Pharmacology, 12(1), 31–35. [DOI:10.2174/1574884712666170310111125]
Avram, M. M. (2004). Cellulite: a review of its physiology and treatment. Journal of Cosmetic and Laser Therapy, 6(4), 181–185. [DOI:10.1080/14764170410003057]
Azzouni, F., Godoy, A., Li, Y., & Mohler, J. (2012). The 5 Alpha-Reductase Isozyme Family: A Review of Basic Biology and Their Role in Human Diseases. Advances in Urology, 2012 (Personalized Cancer Therapy for Urological Cancers: From Bench to Bedside and Back), 530121. [DOI:10.1155/2012/530121]
Baker, J. (1999). A report on alterations to the speaking and singing voices of four women following hormonal therapy with virilizing agents. Journal of Voice, 13(4), 496–507. [DOI:10.1016/s0892-1997(99)80005-8]
Barbieri, R. L. (2019). Breast. In Strauss, J. F., & Barbieri, R. L. (Eds.). Yen and Jaffe’s Reproductive Endocrinology: Physiology, Pathophysiology, and Clinical Management, 8th Edition (pp. 248–255.e3). Philadelphia: Elsevier. [Google Books] [DOI:10.1016/B978-0-323-47912-7.00010-X]
Bardin, C. W., & Janne, O. A. (1986). Steroids of One Class Can Mimic, Inhibit and Potentiate the Biological Effects of Other Steroid Classes When Administered at High Doses. In Gregoire, A. T., & Blye, R. P. (Eds.). Contraceptive Steroids: Pharmacology and Safety (pp. 123–143). Boston, MA: Springer US. [DOI:10.1007/978-1-4613-2241-2_6]
Barrionuevo, P., Nabhan, M., Altayar, O., Wang, Z., Erwin, P. J., Asi, N., Martin, K. A., & Murad, M. H. (2018). Treatment Options for Hirsutism: A Systematic Review and Network Meta-Analysis. The Journal of Clinical Endocrinology & Metabolism, 103(4), 1258–1264. [DOI:10.1210/jc.2017-02052]
Bässler, R. (1970). The Morphology of Hormone Induced Structural Changes in the Female Breast. In Altmann, H.-W., et al. (Eds.). Current Topics in Pathology: Ergebnisse der Pathology, Volume 53 (pp. 1–89). Heidelberg: Springer Berlin. [DOI:10.1007/978-3-662-30514-0_1] [PDF]
Behre, H. M., Nashan, D., Hubert, W., & Nieschlag, E. (1992). Depot gonadotropin-releasing hormone agonist blunts the androgen-induced suppression of spermatogenesis in a clinical trial of male contraception. The Journal of Clinical Endocrinology & Metabolism, 74(1), 84–90. [DOI:10.1210/jcem.74.1.1727833]
Behre, H., Kliesch, S., Lemcke, B., von Eckardstein, S., & Nieschlag, E. (2001). Suppression of spermatogenesis to azoospermia by combined administration of GnRH antagonist and 19-nortestosterone cannot be maintained by this non-aromatizable androgen alone. Human Reproduction, 16(12), 2570–2577. [DOI:10.1093/humrep/16.12.2570]
Bhagavan, N. V. (2002). Endocrine Metabolism V: Reproductive System. In Bhagavan, N. V. Medical Biochemistry, 4th Edition (pp. 781–801). San Diego: Harcourt/Academic Press. [Google Books] [WorldCat]
Bourg, R. (1950). Activité sécrétrice des glandes mammaires; consécutive a des doses massives de testostérone chez la femme après castration. [Secretory activity of the mammary glands; sequellae of massive testosterone doses in women following castration.] Annales d’Endocrinologie, 11(3), 254–260. [Google Scholar] [PubMed] [PDF]
Bricout, V., & Wright, F. (2004). Update on nandrolone and norsteroids: how endogenous or xenobiotic are these substances? European Journal of Applied Physiology, 92(1–2), 1–12. [DOI:10.1007/s00421-004-1051-3]
Brodnitz, F. S. (1971). Hormones and the human voice. Bulletin of the New York Academy of Medicine, 47(2), 183–191. [Google Scholar] [PubMed] [PubMed Central]
Buvat, J., Maggi, M., Guay, A., & Torres, L. O. (2013). Testosterone Deficiency in Men: Systematic Review and Standard Operating Procedures for Diagnosis and Treatment. The Journal of Sexual Medicine, 10(1), 245–284. [DOI:10.1111/j.1743-6109.2012.02783.x]
Camerino, B., & Sala, G. (1960). Anabolic Steroids. In Jucker, E. (Ed.). Fortschritte der Arzneimittelforschung / Progress in Drug Research / Progrès des Recherches Pharmaceutiques, Volume 2 (pp. 71–134). Basel: Birkhäuser Basel. [DOI:10.1007/978-3-0348-7038-2_2]
Camerino, B., & Sciaky, R. (1975). Structure and effects of anabolic steroids. Pharmacology & Therapeutics. Part B: General and Systematic Pharmacology, 1(2), 233–275. [DOI:10.1016/0306-039x(75)90007-0]
Cappelletti, M., & Wallen, K. (2016). Increasing women’s sexual desire: The comparative effectiveness of estrogens and androgens. Hormones and Behavior, 78, 178–193. [DOI:10.1016/j.yhbeh.2015.11.003]
Čeponis, J., Wang, C., Swerdloff, R. S., & Liu, P. Y. (2017). Anabolic and Metabolic Effects of Testosterone and Other Androgens: Direct Effects and Role of Testosterone Metabolic Products. In Simoni, M., & Huhtaniemi, I. T. (Eds.). Endocrinology of the Testis and Male Reproduction (pp. 373–394). Cham: Springer International Publishing. [DOI:10.1007/978-3-319-44441-3_11]
Cocchetti, C., Ristori, J., Romani, A., Maggi, M., & Fisher, A. D. (2020). Hormonal Treatment Strategies Tailored to Non-Binary Transgender Individuals. Journal of Clinical Medicine, 9(6), 1609. [DOI:10.3390/jcm9061609]
Cocchetti, C., Ristori, J., Mazzoli, F., Vignozzi, L., Maggi, M., & Fisher, A. D. (2020). Management of hypoactive sexual desire disorder in transgender women: a guide for clinicians. International journal of Impotence Research, 33(7), 703–709. [DOI:10.1038/s41443-021-00409-8]
Cooke, P. S., Nanjappa, M. K., Ko, C., Prins, G. S., & Hess, R. A. (2017). Estrogens in Male Physiology. Physiological Reviews, 97(3), 995–1043. [DOI:10.1152/physrev.00018.2016]
Crawford, B. A., Liu, P. Y., Kean, M. T., Bleasel, J. F., & Handelsman, D. J. (2003). Randomized Placebo-Controlled Trial of Androgen Effects on Muscle and Bone in Men Requiring Long-Term Systemic Glucocorticoid Treatment. The Journal of Clinical Endocrinology & Metabolism, 88(7), 3167–3176. [DOI:10.1210/jc.2002-021827]
Damsté, P. (1964). Virilization of the Voice due to Anabolic Stereoids. Folia Phoniatrica et Logopaedica, 16(1), 10–18. [DOI:10.1159/000262980]
Davis, S. (1999). The therapeutic use of androgens in women. The Journal of Steroid Biochemistry and Molecular Biology, 69(1–6), 177–184. [DOI:10.1016/s0960-0760(99)00054-0]
Dimitrakakis, C., Zhou, J., Wang, J., Belanger, A., LaBrie, F., Cheng, C., Powell, D., & Bondy, C. (2003). A physiologic role for testosterone in limiting estrogenic stimulation of the breast. Menopause, 10(4), 292–298. [DOI:10.1097/01.gme.0000055522.67459.89]
Doran, P. M., Riggs, B. L., Atkinson, E. J., & Khosla, S. (2001). Effects of Raloxifene, a Selective Estrogen Receptor Modulator, on Bone Turnover Markers and Serum Sex Steroid and Lipid Levels in Elderly Men. Journal of Bone and Mineral Research, 16(11), 2118–2125. [DOI:10.1359/jbmr.2001.16.11.2118]
Drugs.com. International > Nandrolone. Drugs.com. [URL]
Ebeling, P. R. (2010). Androgens and osteoporosis. Current Opinion in Endocrinology, Diabetes & Obesity, 17(3), 284–292. [DOI:10.1097/med.0b013e328339658c]
Feldman, E. B., Carter, A. C., Kossa, J. L., McCarrick, J. F., & Schwartz, H. L. (1960). Endocrinologic and Metabolic Effects of 17α-Methyl-19-nortestosterone in Women. The Journal of Clinical Endocrinology & Metabolism, 20(6), 842–857. [DOI:10.1210/jcem-20-6-842]
Flicker, L., Hopper, J. L., Larkins, R. G., Lichtenstein, M., Buirski, G., & Wark, J. D. (1997). Nandrolone decanoate and intranasal calcitonin as therapy in established osteoporosis. Osteoporosis International, 7(1), 29–35. [DOI:10.1007/bf01623456]
Friedl, K. E., Jones, R. E., Hannan, C. J., & Plymate, S. R. (1989). The Administration of Pharmacological Doses of Testosterone or 19-Nortestosterone to Normal Men is Not Associated with Increased Insulin Secretion or Impaired Glucose Tolerance. The Journal of Clinical Endocrinology & Metabolism, 68(5), 971–975. [DOI:10.1210/jcem-68-5-971]
Friedl, K. E., Dettori, J. R., Hannan, C. J., Patience, T. H., & Plymate, S. R. (1991). Comparison of the effects of high dose testosterone and 19-nortestosterone to a replacement dose of testosterone on strength and body composition in normal men. The Journal of Steroid Biochemistry and Molecular Biology, 40(4–6), 607–612, IN5–IN6. [DOI:10.1016/0960-0760(91)90283-b]
Frisoli, A., Chaves, P. H., Pinheiro, M. M., & Szejnfeld, V. L. (2005). The Effect of Nandrolone Decanoate on Bone Mineral Density, Muscle Mass, and Hemoglobin Levels in Elderly Women With Osteoporosis: A Double-Blind, Randomized, Placebo-Controlled Clinical Trial. The Journals of Gerontology Series A: Biological Sciences and Medical Sciences, 60(5), 648–653. [DOI:10.1093/gerona/60.5.648]
Gerritsma, E. J., Brocaar, M. P., Hakkesteegt, M. M., & Birkenhäger, J. C. (1994). Virilization of the voice in post-menopausal women due to the anabolic steroid nandrolone decanoate (Decadurabolin). The effects of medication for one year. Clinical Otolaryngology, 19(1), 79–84. [DOI:10.1111/j.1365-2273.1994.tb01153.x]
Geusens, P. (1995). Nandrolone decanoate: Pharmacological properties and therapeutic use in osteoporosis. Clinical Rheumatology, 14(S3), 32–39. [DOI:10.1007/bf02210686]
Gold, J., Batterham, M., Rekers, H., Harms, M., Geurts, T., Helmyr, P., Silva de Mendonca, J., Falleiros Carvalho, L., Panos, G., Pinchera, A., Aiuti, F., Lee, C., Horban, A., Gatell, J., Phanuphak, P., Prasithsirikul, W., Gazzard, B., Bloch, M., & Danner, S. (2006). Effects of nandrolone decanoate compared with placebo or testosterone on HIV-associated wasting. HIV Medicine, 7(3), 146–155. [DOI:10.1111/j.1468-1293.2006.00358.x]
Gruber, C. J., Wieser, F., Gruber, I. M., Ferlitsch, K., Gruber, D. M., & Huber, J. C. (2002). Current concepts in aesthetic endocrinology. Gynecological Endocrinology, 16(6), 431–441. [DOI:10.1080/gye.16.6.431.441]
Hamdy, R. C., Moore, S. W., Whalen, K. E., & Landy, C. (1998). Nandrolone Decanoate for Men With Osteoporosis. American Journal of Therapeutics, 5(2), 89–96. [DOI:10.1097/00045391-199803000-00006]
Handelsman, D. J. (2016). Androgen Physiology, Pharmacology, and Abuse. In Jameson, J. L., & De Groot, L. J. (Eds.). Endocrinology: Adult and Pediatric, 7th Edition, Volume 2 (pp. 2368–2393.e16). Philadelphia: Saunders/Elsevier. [Google Books] [DOI:10.1016/B978-0-323-18907-1.00138-4]
Hassager, C., Jensen, L., Johansen, J., Riis, B., Melkko, J., Pødenphant, J., Risteli, L., Christiansen, C., & Risteli, J. (1991). The carboxy-terminal propeptide of type I procollagen in serum as a marker of bone formation: The effect of nandrolone decanoate and female sex hormones. Metabolism, 40(2), 205–208. [DOI:10.1016/0026-0495(91)90176-w]
Hickson, R. C., Ball, K. L., & Falduto, M. T. (1989). Adverse Effects of Anabolic Steroids. Medical Toxicology and Adverse Drug Experience, 4(4), 254–271. [DOI:10.1007/bf03259912]
Hiort, O. (2013). The differential role of androgens in early human sex development. BMC Medicine, 11(1), 152. [DOI:10.1186/1741-7015-11-152]
Hirshburg, J. M., Kelsey, P. A., Therrien, C. A., Gavino, A. C., & Reichenberg, J. S. (2016). Adverse Effects and Safety of 5-alpha Reductase Inhibitors (Finasteride, Dutasteride): A Systematic Review. The Journal of Clinical and Aesthetic Dermatology, 9(7), 56–62. [Google Scholar] [PubMed] [PubMed Central]
Hobbs, C. J., Plymate, S. R., Rosen, C. J., & Adler, R. A. (1993). Testosterone administration increases insulin-like growth factor-I levels in normal men. The Journal of Clinical Endocrinology & Metabolism, 77(3), 776–779. [DOI:10.1210/jcem.77.3.7690364]
Hobbs, C. J., Jones, R. E., & Plymate, S. R. (1996). Nandrolone, a 19-nortestosterone, enhances insulin-independent glucose uptake in normal men. The Journal of Clinical Endocrinology & Metabolism, 81(4), 1582–1585. [DOI:10.1210/jcem.81.4.8636371]
Holterhus, P., Piefke, S., & Hiort, O. (2002). Anabolic steroids, testosterone-precursors and virilizing androgens induce distinct activation profiles of androgen responsive promoter constructs. The Journal of Steroid Biochemistry and Molecular Biology, 82(4–5), 269–275. [DOI:10.1016/s0960-0760(02)00220-0]
Huang, G., & Basaria, S. (2017). The Case for Androgens in Menopausal Women: When and How? In Pal, L., & Sayegh, R. A. (Eds.). Essentials of Menopause Management: A Case-Based Approach (pp. 173–196). Cham: Springer International Publishing. [DOI:10.1007/978-3-319-42451-4_10]
Imperato-McGinley, J., & Peterson, R. E. (1976). Male pseudohermaphroditism: The complexities of male phenotypic development. The American Journal of Medicine, 61(2), 251–272. [DOI:10.1016/0002-9343(76)90175-3]
Imperato-McGinley, J., & Zhu, Y. (2002). Androgens and male physiology the syndrome of 5α-reductase-2 deficiency. Molecular and Cellular Endocrinology, 198(1–2), 51–59. [DOI:10.1016/s0303-7207(02)00368-4]
Irwig, M. S. (2015). Safety concerns regarding 5α reductase inhibitors for the treatment of androgenetic alopecia. Current Opinion in Endocrinology, Diabetes & Obesity, 22(3), 248–253. [DOI:10.1097/med.0000000000000158]
Iuliano, S., Izzo, G., Zagari, M. C., Vergine, M., Brunetti, F. S., Brunetti, A., Di Luigi, L., & Aversa, A. (2021). Endocrine management of transgender adults: a clinical approach. Sexes, 2(1), 104–118. [DOI:10.3390/sexes2010009]
Jänne, O., Hemminki, S., Isomaa, V., Kokko, E., Torkkeli, H., Torkkeli, T., & Vierikko, P. (1978). Progestational Activity of Natural and Synthetic Androgens. International Journal of Andrology, 1(s2a) [Endocrine Approach to Male Contraception: Transactions of the Fifth Annual Workshop on the Testis, Held at Geilo, Norway on April 2-5, 1978], 162–174. [DOI:10.1111/j.1365-2605.1978.tb00015.x]
Kicman, A. T. (2008). Pharmacology of anabolic steroids. British Journal of Pharmacology, 154(3), 502–521. [DOI:10.1038/bjp.2008.165]
Kirschvink, J. F. (1963). Studies of Anabolic Steroids. American Journal of Diseases of Children, 106(4), 368–368. [DOI:10.1001/archpedi.1963.02080050370005]
Knuth, U. A., Behre, H., Belkien, L., Bents, H., & Nieschlag, E. (1985). Clinical trial of 19-nortestosterone-hexoxyphenylpropionate (Anadur) for male fertility regulation. Fertility and Sterility, 44(6), 814–821. [DOI:10.1016/s0015-0282(16)49043-6]
Knuth, U. A., Behre, H., Belkien, L., Bents, H., & Nieschlag, E. (1986). 19-Nortestosterone for male fertility regulation. In Zatuchni, G. I., Goldsmith, A., Spieler, J. M., & Sciarra, J. J. (Eds.). Male Contraception: Advances and Future Prospects: Proceedings of an International Workshop on Male Contraception, Advances and Future Prospects, May 28-31, 1985, Geneva, Switzerland (pp. 320–328). Philadelphia: Harper and Row. [Google Scholar] [Google Books] [WorldCat] [PDF]
Knuth, U. A., Yeung, C., & Nieschlag, E. (1989). Combination of 19-nortestosterone-hexyloxyphenylpropionate (Anadur) and depot-medroxyprogesterone-acetate (Clinovir) for male contraception. Fertility and Sterility, 51(6), 1011–1018. [DOI:10.1016/s0015-0282(16)60735-5]
Kuhl, H., & Wiegratz, I. (2017). Das Post-Finasterid-Syndrom. [Post Finasteride Syndrome.] Gynäkologische Endokrinologie, 15(2), 153–163. [DOI:10.1007/s10304-017-0126-2]
Kuiper, G. G., Carlsson, B., Grandien, K., Enmark, E., Häggblad, J., Nilsson, S., & Gustafsson, J. (1997). Comparison of the Ligand Binding Specificity and Transcript Tissue Distribution of Estrogen Receptors α and β. Endocrinology, 138(3), 863–870. [DOI:10.1210/endo.138.3.4979]
Kumar, N., Crozat, A., Li, F., Catterall, J., Bardin, C., & Sundaram, K. (1999). 7α-methyl-19-nortestosterone, a synthetic androgen with high potency: structure-activity comparisons with other androgens. The Journal of Steroid Biochemistry and Molecular Biology, 71(5–6), 213–222. [DOI:10.1016/s0960-0760(99)00143-0]
Lauritzen, C. (1984). Pre- and Postmenopause. In Platt, D. (Ed.). Geriatrics 3: Gynecology · Orthopaedics · Anesthesiology · Surgery · Otorhinolaryngology · Ophthalmology · Dermatology (pp. 2–45). Berlin/Heidelberg: Springer Berlin Heidelberg. [DOI:10.1007/978-3-642-68976-5_1]
Lemmey, A. B., Elamanchi, S. R., Marcora, S. M., Casanova, F., & Maddison, P. J. (2013). Efficacy of nandrolone decanoate in treating rheumatoid cachexia in male rheumatoid arthritis patients. In Matsuno, H. (Ed.). Innovative Rheumatology (pp. 271–285). Rijeka, Croatia: InTech. [DOI:10.5772/53236]
Liu, P. Y., & Handelsman, D. J. (1998). Androgen therapy in non-gonadal disease. In Nieschlag, E., & Behre, H. M. (Eds.). Testosterone: Action · Deficiency · Substitution, 2nd Edition (pp. 473–512). Berlin/Heidelberg: Springer. [DOI:10.1007/978-3-642-72185-4_17]
Marks, L. S. (2004). 5α-reductase: history and clinical importance. Reviews in Urology, 6(Suppl 9), S11–S21. [Google Scholar] [PubMed] [PubMed Central]
Mella, J. M., Perret, M. C., Manzotti, M., Catalano, H. N., & Guyatt, G. (2010). Efficacy and Safety of Finasteride Therapy for Androgenetic Alopecia. Archives of Dermatology, 146(10), 1141–1150. [DOI:10.1001/archdermatol.2010.256]
Need, A. (1989). Cross-over study of fat-corrected forearm mineral content during nandrolone decanoate therapy for osteoporosis. Bone, 10(1), 3–6. [DOI:10.1016/8756-3282(89)90139-7]
Neff, M. S., Goldberg, J., Slifkin, R. F., Eiser, A. R., Calamia, V., Kaplan, M., Baez, A., Gupta, S., & Mattoo, N. (1981). A Comparison of Androgens for Anemia in Patients on Hemodialysis. New England Journal of Medicine, 304(15), 871–875. [DOI:10.1056/nejm198104093041504]
Nieschlag, E. (2010). Clinical trials in male hormonal contraception. Contraception, 82(5), 457–470. [DOI:10.1016/j.contraception.2010.03.020]
Nieschlag, E., & Behre, H. M. (2012). The essential role of testosterone in hormonal male contraception. In Nieschlag, E., Behre, H. M., & Nieschlag, S. (Eds.). Testosterone: Action · Deficiency · Substitution, 4th Edition (pp. 470–493). Cambridge/New York: Cambridge University Press. [DOI:10.1017/cbo9781139003353.023]
Nieschlag, E., Kumar, N., & Sitruk-Ware, R. (2013). 7α-Methyl-19-nortestosterone (MENTR): the Population Council’s contribution to research on male contraception and treatment of hypogonadism. Contraception, 87(3), 288–295. [DOI:10.1016/j.contraception.2012.08.036]
Pan, M. M., & Kovac, J. R. (2016). Beyond testosterone cypionate: evidence behind the use of nandrolone in male health and wellness. Translational Andrology and Urology, 5(2), 213–219. [DOI:10.21037/tau.2016.03.03]
Passeri, M., Pedrazzoni, M., Pioli, G., Butturini, L., Ruys, A., & Cortenraad, M. (1993). Effects of nandrolone decanoate on bone mass in established osteoporosis. Maturitas, 17(3), 211–219. [DOI:10.1016/0378-5122(93)90049-n]
Peters, A. A., Ingman, W. V., Tilley, W. D., & Butler, L. M. (2011). Differential Effects of Exogenous Androgen and an Androgen Receptor Antagonist in the Peri- and Postpubertal Murine Mammary Gland. Endocrinology, 152(10), 3728–3737. [DOI:10.1210/en.2011-1133]
Peterson, R. E., Imperato-McGinley, J., Gautier, T., & Sturla, E. (1977). Male pseudohermaphroditism due to steroid 5α-reductase deficiency. The American Journal of Medicine, 62(2), 170–191. [DOI:10.1016/0002-9343(77)90313-8]
Propecia Finasteride Label. U.S. Food and Drug Administration. [URL] [PDF]
Prunty, F. T., Brooks, R. V., Clayton, B. E., & McSwiney, R. R. (1958). Some Effects of 17α-Ethyl-19-Nortestosterone in Man. Proceedings of the Royal Society of Medicine, 51(7), 557–558. [Google Scholar] [PubMed] [PubMed Central]
Roche, A., Towns, J. W., & Wettenhall, H. (1963). Influence of norethandrolone on the stature of short children. The Journal of Pediatrics, 63(5), 967–976. [DOI:10.1016/s0022-3476(63)80228-0]
Russell, N., & Grossmann, M. (2019). MECHANISMS IN ENDOCRINOLOGY: Estradiol as a male hormone. European Journal of Endocrinology, 181(1), R23–R43. [DOI:10.1530/eje-18-1000]
Sardar, P., Jha, A., Roy, D., Majumdar, U., Guha, P., Roy, S., Banerjee, R., Banerjee, A. K., & Bandyopadhyay, D. (2010). Therapeutic Effects of Nandrolone and Testosterone in Adult Male HIV Patients With AIDS Wasting Syndrome (AWS): A Randomized, Double-Blind, Placebo-Controlled Trial. HIV Clinical Trials, 11(4), 220–229. [DOI:10.1310/hct1104-220]
Sartorius, G. A., Ly, L. P., & Handelsman, D. J. (2014). Male Sexual Function Can Be Maintained Without Aromatization: Randomized Placebo‐Controlled Trial of Dihydrotestosterone (DHT) in Healthy, Older Men for 24 Months. The Journal of Sexual Medicine, 11(10), 2562–2570. [DOI:10.1111/jsm.12550]
Sas, T., Gault, E., Zeger Bardsley, M., Menke, L., Freriks, K., Perry, R., Otten, B., de Muinck Keizer-Schrama, S., Timmers, H., Wit, J., Ross, J., & Donaldson, M. (2014). Safety and Efficacy of Oxandrolone in Growth Hormone-Treated Girls with Turner Syndrome: Evidence from Recent Studies and Recommendations for Use. Hormone Research in Paediatrics, 81(5), 289–297. [DOI:10.1159/000358195]
Schürmeyer, T., Belkien, L., Knuth, U., & Nieschlag, E. (1984). Reversible azoospermia induced by the anabolic steroid 19-nortestosterone. The Lancet, 323(8374), 417–420. [DOI:10.1016/s0140-6736(84)91752-5]
Simpson, E. R., & Jones, M. E. (2007). Of Mice and Men: The Many Guises of Estrogens. In Korach, K. S., & Wintermantel, T. (Eds.). Tissue-Specific Estrogen Action: Novel Mechanisms, Novel Ligands, Novel Therapies (Ernst Schering Foundation Symposium Proceedings, Volume 2006/1) (pp. 45–68). Berlin/Heidelberg: Springer. [DOI:10.1007/2789_2006_016]
Skroza, N., Tolino, E., Mambrin, A., Zuber, S., Balduzzi, V., Marchesiello, A., Bernardini, N., Proietti, I., & Potenza, C. (2018). Adult Acne Versus Adolescent Acne: A Retrospective Study of 1,167 Patients. The Journal of Clinical and Aesthetic Dermatology, 11(1), 21–25. [Google Scholar] [PubMed] [PubMed Central] [URL]
Styne, D. M., & Grumbach, M. M. (2016). Physiology and Disorders of Puberty. In Melmed, S., Polonsky, K. S., Larsen, P. R., Kronenberg, & H. M. (Eds.). Williams Textbook of Endocrinology, 13th Edition (pp. 1074–1218). Philadelphia: Elsevier. [DOI:10.1016/b978-0-323-29738-7.00025-3]
Sundaram, K., & Kumar, N. (2000). 7alpha-Methyl-19-nortestosterone (MENT): the optimal androgen for male contraception and replacement therapy. International Journal of Andrology, 23(S2), 13–15. [DOI:10.1046/j.1365-2605.2000.00004.x]
Sundaram, K., Kumar, N., & Bardin, C. W. (1994). 7α-Methyl-19-nortestosterone: An Ideal Androgen for Replacement Therapy. In Bardin, W. C. (Ed.). Proceedings of the 1992 Laurentian Hormone Conference (Recent Progress in Hormone Research, Volume 49) (pp. 373–376). San Diego: Academic Press. [DOI:10.1016/b978-0-12-571149-4.50027-1]
Sundaram, K., Kumar, N., Monder, C., & Bardin, C. (1995). Different patterns of metabolism determine the relative anabolic activity of 19-norandrogens. The Journal of Steroid Biochemistry and Molecular Biology, 53(1–6), 253–257. [DOI:10.1016/0960-0760(95)00056-6]
Suvisaari, J. (2000). 7α-Methyl-19-Nortestosterone (MENT): Pharmacokinetics and Antigonadotropic Effects in Men. (Doctoral dissertation, University of Helsinki.) Helsinki: University of Helsinki. [Google Scholar] [URL] [PDF]
Thirumalai, A., Ceponis, J., Amory, J. K., Swerdloff, R., Surampudi, V., Liu, P. Y., Bremner, W. J., Harvey, E., Blithe, D. L., Lee, M. S., Hull, L., Wang, C., & Page, S. T. (2018). Effects of 28 Days of Oral Dimethandrolone Undecanoate in Healthy Men: A Prototype Male Pill. The Journal of Clinical Endocrinology & Metabolism, 104(2), 423–432. [DOI:10.1210/jc.2018-01452]
Tóth, M. (2009). Mioanabolikus Szteroidok és Szelektív Androgénreceptormodulátorok: Hatásmechanizmus és Terápiás Perspektívák. [Myoanabolic Steroids and Selective Androgen Receptor Modulators: Mechanism of Action and Perspectives. Orvosi Hetilap, 150(45), 2051–2059. [DOI:10.1556/oh.2009.28739] [Translation]
Tóth, M., & Zakár, T. (1986). Classification of Anabolic Steroids Using the Method of Competitive Metabolism. Experimental and Clinical Endocrinology & Diabetes, 87(2), 125–132. [DOI:10.1055/s-0029-1210533]
Trost, L., Saitz, T. R., & Hellstrom, W. J. (2013). Side Effects of 5‐Alpha Reductase Inhibitors: A Comprehensive Review. Sexual Medicine Reviews, 1(1), 24–41. [DOI:10.1002/smrj.3]
van der Vies, J. (1985). Implications of basic pharmacology in the therapy with esters of nandrolone. Acta Endocrinologica, 110(3 Suppl a), S38–S44. [DOI:10.1530/acta.0.109s0038]
van Zuuren, E. J., Fedorowicz, Z., Carter, B., & Pandis, N. (2015). Interventions for hirsutism (excluding laser and photoepilation therapy alone). Cochrane Database of Systematic Reviews, 2015, CD010334. [DOI:10.1002/14651858.cd010334.pub2]
Vetri, M., Cataldi, A., Naselli, A., & Vetri, A. (2021). Transsexualism Ethiology and Medical Management: Between Scientific Evidence and Personal Experiences. Preprints, 2021030172. [DOI:10.20944/preprints202103.0172.v1]
Wibowo, E., Schellhammer, P., & Wassersug, R. J. (2011). Role of Estrogen in Normal Male Function: Clinical Implications for Patients With Prostate Cancer on Androgen Deprivation Therapy. Journal of Urology, 185(1), 17–23. [DOI:10.1016/j.juro.2010.08.094]
Wibowo, E., & Wassersug, R. J. (2013). The effect of estrogen on the sexual interest of castrated males: Implications to prostate cancer patients on androgen-deprivation therapy. Critical Reviews in Oncology/Hematology, 87(3), 224–238. [DOI:10.1016/j.critrevonc.2013.01.006]
Winters, S. J. (1990). Androgens: Endocrine Physiology and Pharmacology. In Lin, G. C., & Erinoff, L. (Eds.). Anabolic Steroid Abuse (National Institute on Drug Abuse Research Monograph Series, Volume 102) (pp. 113–130). Rockville, Maryland: National Institute on Drug Abuse/U.S. Department of Health and Human Services. [Google Scholar] [PubMed] [Google Books] [PDF]
World Health Organization & Task Force on Methods for the Regulation of Male Fertility. (1993). Comparison of two androgens plus depot-medroxyprogesterone acetate for suppression to azoospermia in Indonesian men. Fertility and Sterility, 60(6), 1062–1068. [DOI:10.1016/s0015-0282(16)56411-5]
Wu, C., & Kovac, J. R. (2016). Novel Uses for the Anabolic Androgenic Steroids Nandrolone and Oxandrolone in the Management of Male Health. Current Urology Reports, 17(10), 72. [DOI:10.1007/s11934-016-0629-8]
Wu, S., Yuen, F., Swerdloff, R. S., Pak, Y., Thirumalai, A., Liu, P. Y., Amory, J. K., Bai, F., Hull, L., Blithe, D. L., Anawalt, B. D., Parman, T., Kim, K., Lee, M. S., Bremner, W. J., Page, S. T., & Wang, C. (2018). Safety and Pharmacokinetics of Single-Dose Novel Oral Androgen 11β-Methyl-19-Nortestosterone-17β-Dodecylcarbonate in Men. The Journal of Clinical Endocrinology & Metabolism, 104(3), 629–638. [DOI:10.1210/jc.2018-01528]
Yuen, F., Thirumalai, A., Pham, C., Swerdloff, R. S., Anawalt, B. D., Liu, P. Y., Amory, J. K., Bremner, W. J., Dart, C., Wu, H., Hull, L., Blithe, D. L., Long, J., Wang, C., & Page, S. T. (2020). Daily Oral Administration of the Novel Androgen 11β-MNTDC Markedly Suppresses Serum Gonadotropins in Healthy Men. The Journal of Clinical Endocrinology & Metabolism, 105(3), e835–e847. [DOI:10.1210/clinem/dgaa032]
\ No newline at end of file
+Nandrolone as a Potential Alternative Androgen with Reduced Androgenic Side Effects for Transfeminine and Transmasculine People - Transfeminine Science
Nandrolone as a Potential Alternative Androgen with Reduced Androgenic Side Effects for Transfeminine and Transmasculine People
By Aly | First published March 20, 2020 | Last modified March 23, 2023
Abstract / TL;DR
Nandrolone, or 19-nortestosterone, is a unique androgen and anabolic steroid which is used in the form of injectable ester prodrugs like nandrolone decanoate. It is closely related to testosterone structurally but has a number of important pharmacological differences in comparison. These differences include inactivation by 5α-reductase rather than potentiation, less or no conversion into estradiol, and much greater progestogenic activity. The inactivation of nandrolone by 5α-reductase results in nandrolone theoretically having much lower androgenic strength than testosterone in skin, hair follicles, and the prostate, among other tissues. Consequently, nandrolone may have less propensity for oily skin, acne, facial/body hair growth, scalp hair loss, and prostate problems than testosterone. On the other hand, nandrolone is theoretically expected to have full androgenic efficacy in most other tissues, including bone, fat, and muscle (and hence of masculine skeletal, fat, and muscular changes). This is also likely to be the case when it comes to voice, bottom growth, and sexual function. The reduced androgenic impact of nandrolone in skin and hair follicles relative to testosterone make it a favorable potential alternative option for androgen therapy both for transfeminine people and for some transmasculine people.
Introduction
Nandrolone, also known chemically as 19-nortestosterone (19-NT), is an androgen and anabolic steroid (AAS) similarly to testosterone (T). It is used as a medication by intramuscular or subcutaneous injection in the form of longer-acting esters like nandrolone decanoate (ND; Deca-Durabolin) and nandrolone phenylpropionate (NPP; Durabolin), which are converted into nandrolone in the body. This is analogous to longer-acting testosterone esters like testosterone enanthate (TE) and testosterone undecanoate (TU) and their conversion in the body into testosterone. Nandrolone is used in medicine for a variety of indications that benefit from anabolic effects in tissues like muscle, bone, and kidneys. Examples include wasting syndromes, osteoporosis, kidney disease, and anemia. It is used not only in men but also in women, for instance to prevent and treat postmenopausal osteoporosis in women who can’t tolerate estrogens or in whom estrogens can’t be taken. Nandrolone has additionally been advocated for use in androgen replacement therapy for women (Davis, 1999).
Nandrolone is closely related to testosterone in terms of chemical structure, pharmacodynamic actions, and disposition in the body. At the same time however, nandrolone has a key difference from testosterone that makes it a very favorable alternative option for use as an androgen in transgender hormone therapy. This is the case not only for transfeminine people but also for transmasculine people. This property of nandrolone is that it is inactivated by 5α-reductase in tissues that express this enzyme. This is in contrast to testosterone, which is potentiated in such tissues via conversion into dihydrotestosterone (DHT). Because of this difference, nandrolone has normal androgenic effects in most of the body but a greatly reduced potential for androgenic effects in skin and hair follicles relative to testosterone. As a result, nandrolone has a variably reduced potential for androgenic skin and hair side effects such as oily skin, acne, facial and body hair growth, and scalp hair loss.
Because of its favorable profile relative to testosterone, nandrolone has been advocated for use in androgen replacement therapy in cisgender men (Wu & Kovac, 2016; Pan & Kovac, 2016). It has also been studied for use in male hormonal contraception as an alternative and replacement for testosterone (Knuth et al., 1986; Nieschlag, 2010; Nieschlag & Behre, 2012). Nandrolone is advantageous for cisgender men not only due to preservation of scalp hair but also due to its lower stimulation of the prostate gland. As a result of its more favorable profile in terms of skin and hair follicles, nandrolone is an underappreciated alternative possibility relative to testosterone for use not only in cisgender people but also in transfeminine and transmasculine people.
Chemistry of Nandrolone
Nandrolone is chemically known as 19-nortestosterone. It is very close to testosterone in terms of chemical structure, the only difference between the two compounds being that the C19 methyl group of testosterone has been removed in the case of nandrolone. Nandrolone is not a synthetic compound; it occurs naturally in the human body in trace amounts as an intermediate in the conversion of testosterone to estradiol by the enzyme aromatase (Bricout & White, 2004). As such, although nandrolone couldn’t be said to be “bioidentical”, it’s quite similar to testosterone.
Figure: Chemical structures of testosterone and nandrolone (19-nortestosterone). The structural difference between testosterone and nandrolone is at the C19 position and is highlighted by the circled areas.
Nandrolone is an agonist of the androgen receptor (AR) similarly to testosterone. It shows higher affinity for the AR than does testosterone and has almost no binding affinity for sex hormone-binding globulin (SHBG) however. For these reasons, nandrolone has about 2.5- to 5-fold higher potency than testosterone in rats on measures of general AR agonistic strength, such as stimulation of muscle growth (Sundaram et al., 1995; Tóth & Zakár, 1986; Wiki; Winters, 1976). It is likewise a more potent AAS than testosterone in humans, and is used medically at lower doses in comparison (Wiki).
Testosterone is a substrate for 5α-reductase in tissues that express this enzyme like skin, hair follicles, prostate gland, and seminal vesicles, among others. It is converted by 5α-reductase into dihydrotestosterone (DHT), an androgen with much higher AR affinity and AR agonistic potency than that of testosterone (Wiki). Consequently, it is estimated that the effects of testosterone are potentiated by 2- to 3-fold via conversion into DHT in tissues that express 5α-reductase (Sundaram et al., 1995). The role of DHT in the effects of testosterone is demonstrated by a rare intersex condition known as 5α-reductase type 2 deficiency, as well as by 5α-reductase inhibitors (5α-RIs) like finasteride and dutasteride (Wiki; Wiki). Men with 5α-reductase type 2 deficiency are reported to have reduced facial hair, a female-like pattern of body hair (with terminal hair largely restricted to the underarms and lower pubic triangle), and no scalp hair recession in the temples nor scalp hair loss in general. Conversely, other aspects of male secondary sexual development, like voice deepening, muscle growth, bone changes, and pubertal penile enlargement, are all normal in the condition. In addition, no feminization or gynecomastia occurs. Hence, adults with 5α-reductase type 2 deficiency have a masculine appearance (Imperato-McGinley & Peterson, 1976; Peterson et al., 1977; Photos). In published photographs of individuals with the condition however, features like lack of body hair and rounded feminine hairlines can be noted.
5α-Reductase inhibitors have similar effects relative to the profile of 5α-reductase type 2 deficiency. For this reason, they are used in the treatment and prevention of scalp hair loss in men and off-label for hirsutism (excessive facial/body hair growth) in women. They greatly slow the rate of scalp hair loss over time in men. For example, a large 5-year randomized controlled trial showed that in men with diagnosed scalp hair loss, 100% of those who received placebo had significant further scalp hair loss whereas only 35% of those who received finasteride had further scalp hair loss (Propecia label). Low-quality evidence suggests that finasteride has similar effectiveness to antiandrogens like spironolactone and flutamide in the treatment of hirsutism in women (Barrionuevo et al., 2018; van Zuuren et al., 2015). Dutasteride has similar or greater effectiveness than finasteride for scalp hair loss in men (Arif et al., 2017), whereas it hasn’t yet been studied in the treatment of hirsutism (Wiki).
5α-Reductase is the key to the favorable differences between testosterone and nandrolone. Both testosterone and nandrolone are substrates for 5α-reductase and have similar affinity for this enzyme (Tóth & Zakár, 1986). But whereas testosterone is potentiated via conversion into DHT in tissues that express 5α-reductase, nandrolone is inactivated by 5α-reductase in these tissues (Kicman, 2008; Tóth, 2009). This is because the 5α-reduced metabolite of nandrolone, 5α-dihydronandrolone (DHN), is a weaker AR agonist with much lower affinity for the AR than nandrolone (Tóth & Zakár, 1986; Kumar et al., 1999). The following table shows AR and SHBG relative binding affinities (RBA) of testosterone, nandrolone, trestolone, and their 5α-reduced forms (Kumar et al., 1999):
Steroid
AR RBA
SHBG RBA
Testosterone
100%
100%
5α-Dihydrotestosterone
290%
340%
Nandrolone
230%
5%
5α-Dihydronandrolone
10%
5%
Trestolone
380%
6%
5α-Dihydrotrestolone
30%
2%
In rodents, although nandrolone has about 3-fold higher anabolic or muscle-stimulating potency than testosterone, its androgenic potency in the prostate gland and seminal vesicles is only about 20 to 40% of that of testosterone (Sundaram et al., 1995; Tóth & Zakár, 1986; Wiki). This works out to an approximate 11:1 dissociation between the effects of nandrolone in tissues with little or no 5α-reductase (muscle) versus with high 5α-reductase (prostate gland, seminal vesicles) in rodents (Wiki). The exact ratio of potency between these tissues in humans is unknown, and extrapolation from rodents should be cautioned against. In any case, an analogous dissociation of some level can be anticipated. As such, nandrolone can be expected to have high AR agonistic strength in most of the body, where 5α-reductase has minimal expression (e.g., fat, muscle, bone), but much lower potency in tissues with high 5α-reductase expression, like skin, hair follicles, the prostate gland, and the seminal vesicles.
It’s important to be clear that nandrolone is not simply akin to taking testosterone with a 5α-reductase inhibitor like dutasteride to block 5α-reductase. This is because nandrolone isn’t merely not potentiated by 5α-reductase, it’s weakened by 5α-reductase. For this reason, 5α-reductase inhibitors actually increase the androgenic strength of nandrolone in tissues that express 5α-reductase like the prostate gland in rodents (Sundaram et al., 1995). (And, for this reason, nandrolone should not be taken with a 5α-reductase inhibitor, in contrast to testosterone.) In other words, nandrolone goes beyond testosterone plus a 5α-reductase inhibitor in terms of the dissociation of its potency between tissues that express 5α-reductase and tissues that do not. As a result, nandrolone has much lower androgenic strength in such tissues than does the combination of testosterone plus a 5α-reductase inhibitor. Nandrolone also appears to have lower strength in tissues that express 5α-reductase than do most other AAS, for instance synthetic DHT derivatives like oxandrolone and stanozolol (Tóth & Zakár, 1986). This is because these AAS are not substrates for 5α-reductase and hence are neither potentiated nor weakened by 5α-reductase, similarly to testosterone with a 5α-reductase inhibitor. The inactivation of nandrolone by 5α-reductase makes it very unique among AAS and AR agonists. Only nandrolone and a few of its derivatives like normethandrone and norethandrolone have this very special property.
Testosterone and nandrolone may also be non-identical in their androgenic actions and effects for reasons other than metabolism. This is because different AR agonists including strong androgens like testosterone and DHT, weak androgens like dehydroepiandrosterone (DHEA) and androstenedione (A4), and predominantly anabolic androgens like nandrolone, oxandrolone, and stanozolol, have been shown to produce differential AR-mediated changes in gene expression (Holterhus, Piefke, & Hiort, 2002; Kicman, 2008; Hiort, 2013). However, nandrolone was more similar in its profile to testosterone than the synthetic AAS. In any case, the clinical implications of these differences in relation to therapeutic use of testosterone versus nandrolone, if any, are unknown.
In relation to the fact that nandrolone is an intermediate in the aromatase-mediated reaction that converts testosterone into estradiol, both testosterone and nandrolone are transformed into estradiol, and hence estradiol is their specific estrogen metabolite. Paradoxically however, whereas it has the same potential for 5α-reduction as testosterone, nandrolone as a medication is aromatized into estradiol virtually not at all (Handelsman, 2016). In accordance, nandrolone suppresses estradiol levels in men and results in low estradiol levels even at very high doses (Friedl, 1991; Hobbs et al., 1993; Hobbs, Jones, & Plymate, 1996; Behre et al., 2001). The following table gives an example of estradiol (E2) levels in men with high-dose testosterone versus high-dose nandrolone (Friedl, 1991):
Drug and dose
E2 before
E2 after
Change
Testosterone enanthate 300 mg/week i.m.
32 ± 4.6 pg/mL
79 ± 9.3 pg/mL
+147%
Nandrolone decanoate 300 mg/week i.m.
40 ± 6.0 pg/mL
14 ± 1.6 pg/mL
–65%
Testosterone and nandrolone themselves don’t have significant affinity for the estrogen receptors nor intrinsic estrogenic activity outside of aromatization to estradiol (Kuiper et al., 1997; Table). Although androgens also help to maintain bone mineral density and AAS like nandrolone are used to treat osteoporosis in postmenopausal women (Geusens, 1995; Ebeling, 2010), estrogens are comparatively much more important for maintenance of bone mineral density and prevention of osteoporosis in both men and women (Wiki). Studies of high-dose nandrolone and androstanolone (DHT) have shown that these non-aromatizable AAS are not adequate for maintenance of bone mineral density in men, whereas the aromatizable testosterone is effective for such purposes (Ronald et al., 1998; Crawford et al., 2003; Lemmey et al., 2013; Sartorius, Ly, & Handelsman, 2014; Čeponis et al., 2017). Non-aromatizable AAS are likewise inferior to estrogen and estrogen–progestogen therapy for maintaining bone mineral density in postmenopausal women (Lauritzen, 1984 [Graph]; Hassager et al., 1991).
Because of its minimal conversion into estradiol, nandrolone should be used as an androgen in transmasculine people only in combination with low-dose estradiol to replace the lost estradiol that would otherwise be provided by testosterone. Estradiol levels in men are on average around 30 pg/mL, and estradiol levels of at least 20 to 30 pg/mL appear to be necessary for maintenance of bone density in men (Doran et al., 2001). A low-dose transdermal estradiol patch, for instance 14 to 25 μg/day, is likely to be adequate for achieving such levels. Alternatively, another option like transdermal estradiol gel (e.g., 0.75–1 mg/day) or low-dose oral estradiol (e.g., 0.5–1 mg/day) may be used instead.
Nandrolone likewise has progestogenic activity. However, the progestogenic activity of nandrolone is greatly enhanced relative to that of testosterone. The affinity of nandrolone for the PR is 5- to 20-fold higher than that of testosterone and its progestogenic potency is correspondingly improved (Wiki; Wiki; Bardin & Janne, 1986). Despite this however, the progestogenic potency of nandrolone is still relatively low. For instance, its affinity for the PR is only about 10 to 20% of that of progesterone and the nandrolone-derived progestin norethisterone (also known as 17α-ethynyl-19-nortestosterone). At the same time however, nandrolone is used at relatively large doses compared to norethisterone. This may help to compensate for its lower progestogenic potency and may allow for significant progestogenic effects at typical clinical doses (Camerino & Sciaky, 1975).
The following table shows human and rabbit PR RBAs and relative progestogenic activity (as measured by in-vivo induction of uteroglobin synthesis in rabbit uterus) of progesterone and several AAS including testosterone and nandrolone (Jänne et al., 1978; Bardin & Janne, 1986):
Steroid
hPR RBA
rbPR RBA
Progestogenic activity (rabbit)
Progesterone
100%
100%
100%
Testosterone
1.6%
1.6%
0.9%
Dihydrotestosterone
3.3%
3.3%
1.9%
Nandrolone
8.9%
12%
5.2%
Methyltestosterone
4.6%
3.4%
0.6%
Norethandrolone
130%
70%
115%
The development of nandrolone was an intermediate step in the eventual development of the 19-nortestosterone group of progestins, which are widely used in hormonal birth control. These include progestins like norethisterone and levonorgestrel, among many others.
Advantages of Nandrolone Over Testosterone
Because of its substantially lower androgenic strength in tissues that have high 5α-reductase expression relative to tissues that have minimal or no 5α-reductase expression, nandrolone is likely to have normal androgenic effects in muscle, bone, fat, and most other tissues but much weaker androgenic strength in skin and hair follicles than equivalent doses of testosterone. As a result of this, although nandrolone has high capacity for producing most aspects of masculinization, it has a lower potential for many of the undesirable androgenic skin and hair side effects of testosterone, including oily skin, acne, facial and body hair growth, and scalp hair loss. This may allow for unique advantages of nandrolone over testosterone in transfeminine and transmasculine hormone therapy.
The benefits of nandrolone are expected to partially differ in transfeminine people relative to transmasculine people however. This is due to the different doses of nandrolone used in these individuals, namely low, female replacement doses in transfeminine people and full, male replacement doses in transmasculine people. As an example, transmasculine people taking full male androgen replacement doses should probably expect no less oily skin or acne with nandrolone than with testosterone. This is because very low levels of testosterone are necessary for such effects, as evidenced by the fact that acne prevalence and severity is similar in females compared to males (Skroza et al., 2018) despite the fact that testosterone levels are 20-fold lower in women than in men (Styne & Grumbach, 2016). Conversely, transfeminine people taking nandrolone at doses equivalent to the effect of testosterone levels in the normal female range may experience less or possibly no oily skin or acne with nandrolone compared to use of testosterone instead. This is due to the equivalent testosterone levels being far closer to the biological threshold for manifestation of such effects.
Nandrolone can be anticipated to have far less potential for scalp hair loss relative to testosterone in transmasculine people (Wu & Kovac, 2016; Pan & Kovac, 2016). This is related to the lack of scalp hair loss in men with 5α-reductase type 2 deficiency and the high effectiveness of 5α-reductase inhibitors for scalp hair loss. However, nandrolone is theoretically even better than testosterone plus a 5α-reductase inhibitor when it comes to preservation of scalp hair. This is because again, nandrolone is not simply not potentiated, but is inactivated in tissues that express 5α-reductase. Nandrolone replacement of testosterone represents a highly promising treatment for scalp hair loss in men that offers potentially superior effectiveness to 5α-reductase inhibitors. Moreover, since nandrolone isn’t an inhibitor of 5α-reductase, it doesn’t interfere with 5α-reduced neurosteroid synthesis. Hence, nandrolone doesn’t have the possible psychiatric side effects that have been associated with 5α-reductase inhibitors, for instance depression (Irwig, 2015; Kuhl & Wiegratz, 2017; Wiki).
On the basis of 5α-reductase type 2 deficiency, nandrolone may be expected to produce reduced facial and particularly body hair growth relative to testosterone in transmasculine people. Essentially no body or facial hair growth is likely to occur with nandrolone at doses equivalent to female-range testosterone levels in transfeminine people, and even at supraphysiological levels, facial and body hair growth is likely to be less than with testosterone. However, facial and body hirsutism have nonetheless been reported with nandrolone at postmenopausal osteoporosis doses (Need et al., 1989; Passeri et al., 1993; Geusens, 1995; Flicker et al., 1997).
For transmasculine people who want the benefits of nandrolone except the lesser facial hair growth, topical testosterone to the beard area can potentially be used in conjunction with nandrolone injections to restore full facial hair growth. Another possibility for achieving effects of both testosterone and nandrolone in transmasculine people could be to start on testosterone and use it for a few years, allowing for facial/body hair growth and hairline masculinization, and then switch from testosterone to nandrolone for long-term therapy, allowing for preservation of scalp hair.
One of the reasons that nandrolone is attractive for androgen replacement therapy in cisgender men is that it has very weak relative effects in the prostate gland compared to testosterone. This is due to inactivation of nandrolone in the prostate gland by 5α-reductase similarly to other tissues that express this enzyme. It is anticipated that long-term androgen replacement therapy with nandrolone might allow for a reduced risk of enlarged prostate and prostate cancer compared to testosterone in men (Wu & Kovac, 2016; Pan & Kovac, 2016). As transfeminine people also have prostate glands, the weak effects of nandrolone in the prostate are potentially of relevance to us as well. However, due to estrogen therapy and androgen deprivation, the prostate is atrophied in transfeminine people and prostate cancer is very rare (Wiki). In relation to this, the favorable prostate profile of nandrolone may be of little significance for transfeminine people.
Although nandrolone is quite promising for transgender hormone therapy, it is important to be clear that there are currently no quality clinical studies comparing it to testosterone and showing that it is less androgenic in terms of skin and hair effects (even if there is strong theoretical basis for this notion, particularly in the case of scalp hair loss). Nor are there any studies demonstrating with certainty that it is as effective as testosterone in terms of inducing general masculinization. Moreover, the appropriate dosages of nandrolone for use in androgen replacement in women and men are uncertain. Finally, nandrolone has been little-studied for androgen replacement and its long-term tolerability and health safety for this use haven’t been properly characterized. For these reasons, androgen replacement with nandrolone in cisgender men and transmasculine people is an experimental therapy. Additional research is needed to properly characterize nandrolone for this indication.
Androgen Replacement in Transfeminine People
Some believe that testosterone is important in women for mood, well-being, energy, sexual desire and function, general health, and for other reasons. Androgen levels and activity may be low in many transfeminine people due to hormone therapy and/or gonadectomy, raising concerns about androgen deficiency. However, there is little or no change in androgen levels with natural menopause in cisgender women and only a small decrease in androgen levels with ovariectomy in women (Liu & Handelsman, 1998). Moreover, there is inadequate evidence to support claims of benefit with androgen replacement therapy in women at present, and there are no well-supported benefits of female-range doses of testosterone (Wiki). For these reasons, androgen replacement therapy in women is controversial (Liu & Handelsman, 1998).
Testosterone does stimulate sexual desire in women, but only at levels that are above the normal female range (>50 ng/dL) (Cappelletti & Wallen, 2016; Wiki). And even with high testosterone levels of 80 to 150 ng/dL, stimulation of sexual desire in women is modest (Cappelletti & Wallen, 2016; Wiki). It is likely that estradiol rather than testosterone (or progesterone) is the key sex hormone for sexual desire in women (Cappelletti & Wallen, 2016; Aly, 2020).
Androgens can have detrimental effects in transfeminine people. They can cause androgenic and masculinizing effects like oily skin, acne, seborrhea, facial/body hair growth, scalp hair loss, and voice deepening, among others. In addition, androgens oppose the effects of estrogens in the breasts, and may inhibit breast development even with low-level exposure or physiological levels in females (Dimitrakakis et al., 2003; Peters et al., 2011; Sas et al., 2014; Barbieri, 2017).
For these reasons, transfeminine people don’t necessarily require androgen replacement, and it shouldn’t be routinely used out of concern of androgen deficiency. In any case, some transfeminine people insist on androgen replacement, and others desire supraphysiological levels of androgens for purposes like stimulating libido or helping to build and maintain muscle mass. There is some evidence that even physiological levels of testosterone may help to support muscle mass in women (Huang & Basaria, 2017). Moreover, in transfeminine people who are fully hormonally transitioned, breast development is complete, and hence inhibition of the breasts by androgens is no longer a concern. Another potentially useful indication of androgens in transfeminine people is to counteract cellulite (Wiki; Gruber et al., 2002; Avram, 2004). Since nandrolone has full androgenic potential in fat tissue, it may be similarly effective as testosterone for this purpose. However, there are no good studies of androgens for treatment of cellulite at this time.
Although androgen replacement therapy isn’t recommended for cisgender women or transfeminine people because of a lack of evidence of benefit and potential adverse effects, nandrolone is a very favorable alternative to testosterone for such purposes in those who nonetheless opt for such therapy. This is due to its improved skin and hair profile and hence a probable lower risk of undesirable effects.
Additional Topics on Nandrolone
This section is for additional topics on nandrolone as an androgen in transfeminine and transmasculine people, including its availability, dosage, androgenic/masculinizing effects besides skin and hair (e.g., voice deepening, bottom growth/clitoral enlargement, sexual effects), and liver safety.
Availability of Nandrolone
Nandrolone esters remain widely available for medical use throughout the world (Drugs.com). However, the availability of AAS, including nandrolone esters, has become increasingly limited over time. The shorter-acting ester nandrolone phenylpropionate is no longer available in the United States or many other countries, and the more favorable longer-acting nandrolone decanoate was discontinued in the United States in 2019. However, nandrolone decanoate remains available from compounding pharmacies in the United States, for instance AnazaoHealth. It is only available from this particular pharmacy at a very high concentration of 200 mg/mL however, which although a potentially workable concentration for use in transmasculine people, is likely completely impractical for use in transfeminine people. Compounding pharmacies might be able to do custom concentrations upon request though.
Another potential means of delivering nandrolone is via an orally active nandrolone androgen prohormone like 19-nordehydroepiandrosterone (19-nor-DHEA). This compound is converted into nandrolone analogously to the use of DHEA as a prohormone of testosterone (Wiki). It is sold as an over-the-counter supplement from certain online vendors, similarly to DHEA. 19-Nor-DHEA may be a more suitable option for transfeminine people due to the lower doses needed and less suitable for transmasculine people due to the much higher doses required.
Dosage of Nandrolone
The dosage of nandrolone for use in androgen replacement therapy in women and men hasn’t been established. Hence, we don’t completely know what the appropriate dose is for use in transfeminine and transmasculine hormone therapy. In any case, it is possible for us to estimate.
One review recommended a clinical dose range in males of 50–400 mg/2–4 weeks for testosterone enanthate or cypionate but 50–100/3–4 weeks for nandrolone decanoate (Hickson et al., 1989). This is also in line with several-fold higher potency of nandrolone relative to testosterone.
Dosage for Transmasculine People
A typical dosage of testosterone enanthate for use in androgen replacement therapy in cisgender and transgender men is 50 to 100 mg once per week by intramuscular injection (Wiki; Wiki). Hence, an appropriate dosage of nandrolone decanoate, assuming 3-fold greater potency than testosterone, might be about 16.7 to 33.3 mg once per week by intramuscular injection (ignoring the small differences in molecular weight between testosterone enanthate and nandrolone decanoate). However, it must be emphasized that these doses are merely educated guesses. It’s notable that these doses are quite similar to those used in postmenopausal osteoporosis in women (about 12.5 to 25 mg per week total). Hence, although such doses have certainly been associated with masculinizing effects in women, they might be suboptimal in terms of masculinization for transmasculine people. Consequently, it’s possible that a higher dose, like 50 mg once per week, might be more appropriate. In addition to weekly use, nandrolone decanoate has a duration suitable for use once every 2 weeks (Graphs).
Nandrolone hexyloxyphenylpropionate (NHPP; brand name Anadur) was studied as a male hormonal contraceptive by the World Health Organization and others at a dose of 200 mg/3 weeks i.m. in combination with depot medroxyprogesterone acetate (Knuth et al., 1986; Nieschlag, 2010; Nieschlag & Behre, 2012). It was used as a replacement and alternative for testosterone and was given at a dosage of about 66.7 mg once per week. However, this was an intentionally supraphysiological dosage which was selected to achieve a male contraceptive effect, as suggested by suppression of gonadotropins to undetectable levels (Knuth et al., 1985). Hence, although safe and well-tolerated in limited studies, it might be a high dosage for transmasculine hormone therapy. Very high doses of nandrolone can reproduce the full spectrum of androgenic effects of testosterone, and hence doses of nandrolone that are too high may serve to nullify its advantages over testosterone (van der Vies, 1985).
Dosage for Transfeminine People
In postmenopausal women, nandrolone decanoate has been used for general androgen replacement at a dose of 25 to 50 mg once every 6 to 12 weeks (about 2–8 mg/week or 0.29–1.14 mg/day), and for prevention and treatment of osteoporosis at a dose of 50 mg once every 2 to 4 weeks (about 12.5–25 mg/week or 1.8–3.6 mg/day) (Wiki; Table). However, these doses of nandrolone decanoate are likely to be highly excessive for physiological androgen replacement in women and transfeminine people and are probably also spaced too widely in terms of dosing interval. This is based on the following: (1) normal production of testosterone in premenopausal women is about 150 μg/day; (2) nandrolone is more potent as an androgen receptor agonist than testosterone; and (3) pharmacokinetic concentration–time curves for nandrolone decanoate suggest that an appropriate dosing interval is once every 1 to 2 weeks (Graphs). Indeed, nandrolone decanoate at 50 mg/2–4 weeks has been found to produce significant masculinizing effects in women with long-term use (Geusens, 1995; Wiki). Since nandrolone has high theoretical masculinizing potential in most tissues in the body, like muscle, bone, fat, and vocal tissue, it’s very important that transfeminine people don’t take doses that are too large.
Androgenic and Masculinizing Effects Besides Skin and Hair
Nandrolone has sometimes been described as “non-masculinizing” or “minimally virilizing”, but this is misleading and inaccurate. Nandrolone has high theoretical potential to produce masculinizing skeletal, fat, and muscular effects, like growth of muscles, widening of shoulders, masculine enlargement, elongation, and shaping of bones, and masculine distribution of fat. It also has high capacity to produce voice deepening (the vocal tissue notably being part muscle). The only clear differences in masculinizing effect between nandrolone and testosterone are that nandrolone has a greatly reduced theoretical potential for androgenic effect in skin and hair follicles. Succinctly, nandrolone could be thought of as testosterone with minimization of the undesirable skin and hair effects.
Voice Deepening with Nandrolone
The vocal tissue, consisting of the vocal cords and the larynx, are part muscle, and 5α-reductase is expressed minimally or not at all in this tissue (Bhagavan, 2002; Kicman, 2008). Accordingly, voice deepening is normal in individuals with 5α-reductase type 2 deficiency (Imperato-McGinley & Zhu, 2002). As such, nandrolone would be expected to produce voice deepening similarly to testosterone. In accordance, voice deepening has been reported with nandrolone in women at doses used in postmenopausal osteoporosis (Gerritsma et al., 1994; Geusens, 1995; Frisoli et al., 2005). There are case reports of severe and complete masculinization of the voice in women treated with excessive doses of nandrolone (Damsté, 1964; Brodnitz, 1971; Baker, 1999). Voice changes have also been seen with nandrolone derivatives like normethandrone (Feldman et al., 1960).
Bottom Growth with Nandrolone
DHT is required for normal male sexual differentiation of the genitals during prenatal development. This is evidenced by 5α-reductase type 2 deficiency, in which the genitals are ambiguous but overall more female-like at birth and in childhood (Wiki). Although DHT is critical for prenatal genital masculinization, the same may not be true for pubertal development of the penis (Hiort, 2013). Individuals with 5α-reductase type 2 deficiency undergo masculinization of the genitals at puberty such that a small and near-functional penis develops (Peterson et al., 1977; Marks, 2004; Hiort, 2013; Photos). This is so striking that males with 5α-reductase type 2 deficiency in the Dominican Republic are referred to as “guevedoces”, which is said to literally mean “penis at 12”.
As 5α-reductase may not be critical for penile enlargement at puberty, nandrolone may allow for no less bottom growth (clitoral enlargement) in transmasculine people than does testosterone. Indeed, nandrolone has been reported to produce clitoral enlargement as a side effect in women and penile growth in prepubertal boys (Camerino & Sala, 1960; Camerino & Sciaky, 1975). Similar findings have been made for derivatives of nandrolone like normethandrone and norethandrolone (Feldman et al., 1960; Roche, Towns, & Wettenhall, 1963; Kirschvink et al., 1963; Prunty et al., 1958).
Since this article was published, a review suggesting nandrolone as a potential component of transgender hormone therapy for non-binary individuals has been published:
Cocchetti, C., Ristori, J., Romani, A., Maggi, M., & Fisher, A. D. (2020). Hormonal Treatment Strategies Tailored to Non-Binary Transgender Individuals. Journal of Clinical Medicine, 9(6), 1609. [DOI:10.3390/jcm9061609]
The review includes the following excerpts on nandrolone:
Other options may include nandrolone, an anabolic steroid administered via intramuscular injection, which is not as optimal a substrate for 5α-reductase as testosterone, but it has a stronger effect compared to the testosterone on target tissues devoid of 5α-reductase activity (e.g., muscular tissue) [15]. Indeed, nandrolone can be theoretically used in non-binary [assigned female at birth (AFAB)] individuals requesting masculinization of body shape (i.e., increased muscle mass) with a limited increase in facial and body hair. Regarding the safety profile of this compound, data are limited by the fact that most observations come from the setting of androgenic-anabolic steroid (AAS) abuse [16,17], thus their applicability to appropriate medical therapy is limited [18]. In this setting, concerns about cardiomyopathy and coronary artery disease risk emerged [19], although associated with the administration of nandrolone at extremely higher dosages [20]. Furthermore, nandrolone use does not seem associated to hepatotoxicity, since, as an injectable oil, it is not subject to first-pass hepatic metabolism.
Moreover, some AFAB transgender individuals can benefit from testosterone therapy combined with 5α-reductase inhibitors or from treatment with nandrolone (an androgenic compound less prone to 5α reduction) in case they wish only a partial virilization (i.e., voice deepening and lean mass increase without facial and body hair increase).
In addition to the above review, a second review suggesting nandrolone as a potential option for hormone therapy in non-binary individuals has been published (as a preprint):
Vetri, M., Cataldi, A., Naselli, A., & Vetri, A. (2021). Transsexualism Ethiology and Medical Management: Between Scientific Evidence and Personal Experiences. Preprints, 2021030172. [DOI:10.20944/preprints202103.0172.v1]:
With the following relevant excerpt:
In [female-to-males] (FtMs) requesting partial masculinization, it may be possible to reduce the dose of testosterone or substitute it with nandrolone, an anabolic steroid administered via intramuscular injection. So, we must accept alternative hormonal treatment regimens, other than those reported in current guidelines, for such nonbinary transgender individuals, to try to improve their psychological well-being and quality of life [40].
However, this preprint article appears to have never ended up being accepted for publication.
Update 3: Cocchetti et al. (2020) and Iuliano et al. (2021)
Further articles have mentioned nandrolone as a hypothetical option for transgender people, for instance Cocchetti et al. (2020):
Another hypothetic option [for management of hypoactive sexual desire disorder in transgender women] may include nandrolone, an androgenic compound administered via intramuscular injection, less prone to 5-alpha reduction anabolic steroid leading to limited virilizing dermatological undesired effects [72]. However, data on its efficacy on sexual desire are not yet available.
Actually, the classic view of gender binarism and [gender-affirming hormone therapy (GAHT)] should be reconsidered because of the increasing prevalence of non-binary individuals experiencing [gender dysphoria (GD)]. Therefore, new therapeutic strategies should be also considered [17]. Since there is a lack in standardized hormonal treatment protocols for non-binary [assigned female at birth (AFAB)], GAHT goals should be adjusted according to patients’ needs in order to improve the self-perception and the quality of life [18]. For instance, different testosterone doses and/or other androgen preparations (i.e., nandrolone) are suggested to modulate the requested body changes [18], even if serious ethical concerns on some drugs exist.
References
Anderson, R. A., Martin, C. W., Kung, A. W., Everington, D., Pun, T. C., Tan, K. C., Bancroft, J., Sundaram, K., Moo-Young, A. J., & Baird, D. T. (1999). 7α-Methyl-19-Nortestosterone Maintains Sexual Behavior and Mood in Hypogonadal Men. The Journal of Clinical Endocrinology & Metabolism, 84(10), 3556–3562. [DOI:10.1210/jcem.84.10.6028]
Anderson, R. A., Wallace, A. M., Sattar, N., Kumar, N., & Sundaram, K. (2003). Evidence for Tissue Selectivity of the Synthetic Androgen 7α-Methyl-19-Nortestosterone in Hypogonadal Men. The Journal of Clinical Endocrinology & Metabolism, 88(6), 2784–2793. [DOI:10.1210/jc.2002-021960]
Arif, T., Dorjay, K., Adil, M., & Sami, M. (2017). Dutasteride in Androgenetic Alopecia: An Update. Current Clinical Pharmacology, 12(1), 31–35. [DOI:10.2174/1574884712666170310111125]
Avram, M. M. (2004). Cellulite: a review of its physiology and treatment. Journal of Cosmetic and Laser Therapy, 6(4), 181–185. [DOI:10.1080/14764170410003057]
Azzouni, F., Godoy, A., Li, Y., & Mohler, J. (2012). The 5 Alpha-Reductase Isozyme Family: A Review of Basic Biology and Their Role in Human Diseases. Advances in Urology, 2012 (Personalized Cancer Therapy for Urological Cancers: From Bench to Bedside and Back), 530121. [DOI:10.1155/2012/530121]
Baker, J. (1999). A report on alterations to the speaking and singing voices of four women following hormonal therapy with virilizing agents. Journal of Voice, 13(4), 496–507. [DOI:10.1016/s0892-1997(99)80005-8]
Barbieri, R. L. (2019). Breast. In Strauss, J. F., & Barbieri, R. L. (Eds.). Yen and Jaffe’s Reproductive Endocrinology: Physiology, Pathophysiology, and Clinical Management, 8th Edition (pp. 248–255.e3). Philadelphia: Elsevier. [Google Books] [DOI:10.1016/B978-0-323-47912-7.00010-X]
Bardin, C. W., & Janne, O. A. (1986). Steroids of One Class Can Mimic, Inhibit and Potentiate the Biological Effects of Other Steroid Classes When Administered at High Doses. In Gregoire, A. T., & Blye, R. P. (Eds.). Contraceptive Steroids: Pharmacology and Safety (pp. 123–143). Boston, MA: Springer US. [DOI:10.1007/978-1-4613-2241-2_6]
Barrionuevo, P., Nabhan, M., Altayar, O., Wang, Z., Erwin, P. J., Asi, N., Martin, K. A., & Murad, M. H. (2018). Treatment Options for Hirsutism: A Systematic Review and Network Meta-Analysis. The Journal of Clinical Endocrinology & Metabolism, 103(4), 1258–1264. [DOI:10.1210/jc.2017-02052]
Bässler, R. (1970). The Morphology of Hormone Induced Structural Changes in the Female Breast. In Altmann, H.-W., et al. (Eds.). Current Topics in Pathology: Ergebnisse der Pathology, Volume 53 (pp. 1–89). Heidelberg: Springer Berlin. [DOI:10.1007/978-3-662-30514-0_1]
Behre, H. M., Nashan, D., Hubert, W., & Nieschlag, E. (1992). Depot gonadotropin-releasing hormone agonist blunts the androgen-induced suppression of spermatogenesis in a clinical trial of male contraception. The Journal of Clinical Endocrinology & Metabolism, 74(1), 84–90. [DOI:10.1210/jcem.74.1.1727833]
Behre, H., Kliesch, S., Lemcke, B., von Eckardstein, S., & Nieschlag, E. (2001). Suppression of spermatogenesis to azoospermia by combined administration of GnRH antagonist and 19-nortestosterone cannot be maintained by this non-aromatizable androgen alone. Human Reproduction, 16(12), 2570–2577. [DOI:10.1093/humrep/16.12.2570]
Bhagavan, N. V. (2002). Endocrine Metabolism V: Reproductive System. In Bhagavan, N. V. Medical Biochemistry, 4th Edition (pp. 781–801). San Diego: Harcourt/Academic Press. [Google Books] [WorldCat]
Bourg, R. (1950). Activité sécrétrice des glandes mammaires; consécutive a des doses massives de testostérone chez la femme après castration. [Secretory activity of the mammary glands; sequellae of massive testosterone doses in women following castration.] Annales d’Endocrinologie, 11(3), 254–260. [Google Scholar] [PubMed] [PDF]
Bricout, V., & Wright, F. (2004). Update on nandrolone and norsteroids: how endogenous or xenobiotic are these substances? European Journal of Applied Physiology, 92(1–2), 1–12. [DOI:10.1007/s00421-004-1051-3]
Brodnitz, F. S. (1971). Hormones and the human voice. Bulletin of the New York Academy of Medicine, 47(2), 183–191. [Google Scholar] [PubMed] [PubMed Central]
Buvat, J., Maggi, M., Guay, A., & Torres, L. O. (2013). Testosterone Deficiency in Men: Systematic Review and Standard Operating Procedures for Diagnosis and Treatment. The Journal of Sexual Medicine, 10(1), 245–284. [DOI:10.1111/j.1743-6109.2012.02783.x]
Camerino, B., & Sala, G. (1960). Anabolic Steroids. In Jucker, E. (Ed.). Fortschritte der Arzneimittelforschung / Progress in Drug Research / Progrès des Recherches Pharmaceutiques, Volume 2 (pp. 71–134). Basel: Birkhäuser Basel. [DOI:10.1007/978-3-0348-7038-2_2]
Camerino, B., & Sciaky, R. (1975). Structure and effects of anabolic steroids. Pharmacology & Therapeutics. Part B: General and Systematic Pharmacology, 1(2), 233–275. [DOI:10.1016/0306-039x(75)90007-0]
Cappelletti, M., & Wallen, K. (2016). Increasing women’s sexual desire: The comparative effectiveness of estrogens and androgens. Hormones and Behavior, 78, 178–193. [DOI:10.1016/j.yhbeh.2015.11.003]
Čeponis, J., Wang, C., Swerdloff, R. S., & Liu, P. Y. (2017). Anabolic and Metabolic Effects of Testosterone and Other Androgens: Direct Effects and Role of Testosterone Metabolic Products. In Simoni, M., & Huhtaniemi, I. T. (Eds.). Endocrinology of the Testis and Male Reproduction (pp. 373–394). Cham: Springer International Publishing. [DOI:10.1007/978-3-319-44441-3_11]
Cocchetti, C., Ristori, J., Romani, A., Maggi, M., & Fisher, A. D. (2020). Hormonal Treatment Strategies Tailored to Non-Binary Transgender Individuals. Journal of Clinical Medicine, 9(6), 1609. [DOI:10.3390/jcm9061609]
Cocchetti, C., Ristori, J., Mazzoli, F., Vignozzi, L., Maggi, M., & Fisher, A. D. (2020). Management of hypoactive sexual desire disorder in transgender women: a guide for clinicians. International journal of Impotence Research, 33(7), 703–709. [DOI:10.1038/s41443-021-00409-8]
Cooke, P. S., Nanjappa, M. K., Ko, C., Prins, G. S., & Hess, R. A. (2017). Estrogens in Male Physiology. Physiological Reviews, 97(3), 995–1043. [DOI:10.1152/physrev.00018.2016]
Crawford, B. A., Liu, P. Y., Kean, M. T., Bleasel, J. F., & Handelsman, D. J. (2003). Randomized Placebo-Controlled Trial of Androgen Effects on Muscle and Bone in Men Requiring Long-Term Systemic Glucocorticoid Treatment. The Journal of Clinical Endocrinology & Metabolism, 88(7), 3167–3176. [DOI:10.1210/jc.2002-021827]
Damsté, P. (1964). Virilization of the Voice due to Anabolic Stereoids. Folia Phoniatrica et Logopaedica, 16(1), 10–18. [DOI:10.1159/000262980]
Davis, S. (1999). The therapeutic use of androgens in women. The Journal of Steroid Biochemistry and Molecular Biology, 69(1–6), 177–184. [DOI:10.1016/s0960-0760(99)00054-0]
Dimitrakakis, C., Zhou, J., Wang, J., Belanger, A., LaBrie, F., Cheng, C., Powell, D., & Bondy, C. (2003). A physiologic role for testosterone in limiting estrogenic stimulation of the breast. Menopause, 10(4), 292–298. [DOI:10.1097/01.gme.0000055522.67459.89]
Doran, P. M., Riggs, B. L., Atkinson, E. J., & Khosla, S. (2001). Effects of Raloxifene, a Selective Estrogen Receptor Modulator, on Bone Turnover Markers and Serum Sex Steroid and Lipid Levels in Elderly Men. Journal of Bone and Mineral Research, 16(11), 2118–2125. [DOI:10.1359/jbmr.2001.16.11.2118]
Drugs.com. International > Nandrolone. Drugs.com. [URL]
Ebeling, P. R. (2010). Androgens and osteoporosis. Current Opinion in Endocrinology, Diabetes & Obesity, 17(3), 284–292. [DOI:10.1097/med.0b013e328339658c]
Feldman, E. B., Carter, A. C., Kossa, J. L., McCarrick, J. F., & Schwartz, H. L. (1960). Endocrinologic and Metabolic Effects of 17α-Methyl-19-nortestosterone in Women. The Journal of Clinical Endocrinology & Metabolism, 20(6), 842–857. [DOI:10.1210/jcem-20-6-842]
Flicker, L., Hopper, J. L., Larkins, R. G., Lichtenstein, M., Buirski, G., & Wark, J. D. (1997). Nandrolone decanoate and intranasal calcitonin as therapy in established osteoporosis. Osteoporosis International, 7(1), 29–35. [DOI:10.1007/bf01623456]
Friedl, K. E., Jones, R. E., Hannan, C. J., & Plymate, S. R. (1989). The Administration of Pharmacological Doses of Testosterone or 19-Nortestosterone to Normal Men is Not Associated with Increased Insulin Secretion or Impaired Glucose Tolerance. The Journal of Clinical Endocrinology & Metabolism, 68(5), 971–975. [DOI:10.1210/jcem-68-5-971]
Friedl, K. E., Dettori, J. R., Hannan, C. J., Patience, T. H., & Plymate, S. R. (1991). Comparison of the effects of high dose testosterone and 19-nortestosterone to a replacement dose of testosterone on strength and body composition in normal men. The Journal of Steroid Biochemistry and Molecular Biology, 40(4–6), 607–612, IN5–IN6. [DOI:10.1016/0960-0760(91)90283-b]
Frisoli, A., Chaves, P. H., Pinheiro, M. M., & Szejnfeld, V. L. (2005). The Effect of Nandrolone Decanoate on Bone Mineral Density, Muscle Mass, and Hemoglobin Levels in Elderly Women With Osteoporosis: A Double-Blind, Randomized, Placebo-Controlled Clinical Trial. The Journals of Gerontology Series A: Biological Sciences and Medical Sciences, 60(5), 648–653. [DOI:10.1093/gerona/60.5.648]
Gerritsma, E. J., Brocaar, M. P., Hakkesteegt, M. M., & Birkenhäger, J. C. (1994). Virilization of the voice in post-menopausal women due to the anabolic steroid nandrolone decanoate (Decadurabolin). The effects of medication for one year. Clinical Otolaryngology, 19(1), 79–84. [DOI:10.1111/j.1365-2273.1994.tb01153.x]
Geusens, P. (1995). Nandrolone decanoate: Pharmacological properties and therapeutic use in osteoporosis. Clinical Rheumatology, 14(S3), 32–39. [DOI:10.1007/bf02210686]
Gold, J., Batterham, M., Rekers, H., Harms, M., Geurts, T., Helmyr, P., Silva de Mendonca, J., Falleiros Carvalho, L., Panos, G., Pinchera, A., Aiuti, F., Lee, C., Horban, A., Gatell, J., Phanuphak, P., Prasithsirikul, W., Gazzard, B., Bloch, M., & Danner, S. (2006). Effects of nandrolone decanoate compared with placebo or testosterone on HIV-associated wasting. HIV Medicine, 7(3), 146–155. [DOI:10.1111/j.1468-1293.2006.00358.x]
Gruber, C. J., Wieser, F., Gruber, I. M., Ferlitsch, K., Gruber, D. M., & Huber, J. C. (2002). Current concepts in aesthetic endocrinology. Gynecological Endocrinology, 16(6), 431–441. [DOI:10.1080/gye.16.6.431.441]
Hamdy, R. C., Moore, S. W., Whalen, K. E., & Landy, C. (1998). Nandrolone Decanoate for Men With Osteoporosis. American Journal of Therapeutics, 5(2), 89–96. [DOI:10.1097/00045391-199803000-00006]
Handelsman, D. J. (2016). Androgen Physiology, Pharmacology, and Abuse. In Jameson, J. L., & De Groot, L. J. (Eds.). Endocrinology: Adult and Pediatric, 7th Edition, Volume 2 (pp. 2368–2393.e16). Philadelphia: Saunders/Elsevier. [Google Books] [DOI:10.1016/B978-0-323-18907-1.00138-4]
Hassager, C., Jensen, L., Johansen, J., Riis, B., Melkko, J., Pødenphant, J., Risteli, L., Christiansen, C., & Risteli, J. (1991). The carboxy-terminal propeptide of type I procollagen in serum as a marker of bone formation: The effect of nandrolone decanoate and female sex hormones. Metabolism, 40(2), 205–208. [DOI:10.1016/0026-0495(91)90176-w]
Hickson, R. C., Ball, K. L., & Falduto, M. T. (1989). Adverse Effects of Anabolic Steroids. Medical Toxicology and Adverse Drug Experience, 4(4), 254–271. [DOI:10.1007/bf03259912]
Hiort, O. (2013). The differential role of androgens in early human sex development. BMC Medicine, 11(1), 152. [DOI:10.1186/1741-7015-11-152]
Hirshburg, J. M., Kelsey, P. A., Therrien, C. A., Gavino, A. C., & Reichenberg, J. S. (2016). Adverse Effects and Safety of 5-alpha Reductase Inhibitors (Finasteride, Dutasteride): A Systematic Review. The Journal of Clinical and Aesthetic Dermatology, 9(7), 56–62. [Google Scholar] [PubMed] [PubMed Central]
Hobbs, C. J., Plymate, S. R., Rosen, C. J., & Adler, R. A. (1993). Testosterone administration increases insulin-like growth factor-I levels in normal men. The Journal of Clinical Endocrinology & Metabolism, 77(3), 776–779. [DOI:10.1210/jcem.77.3.7690364]
Hobbs, C. J., Jones, R. E., & Plymate, S. R. (1996). Nandrolone, a 19-nortestosterone, enhances insulin-independent glucose uptake in normal men. The Journal of Clinical Endocrinology & Metabolism, 81(4), 1582–1585. [DOI:10.1210/jcem.81.4.8636371]
Holterhus, P., Piefke, S., & Hiort, O. (2002). Anabolic steroids, testosterone-precursors and virilizing androgens induce distinct activation profiles of androgen responsive promoter constructs. The Journal of Steroid Biochemistry and Molecular Biology, 82(4–5), 269–275. [DOI:10.1016/s0960-0760(02)00220-0]
Huang, G., & Basaria, S. (2017). The Case for Androgens in Menopausal Women: When and How? In Pal, L., & Sayegh, R. A. (Eds.). Essentials of Menopause Management: A Case-Based Approach (pp. 173–196). Cham: Springer International Publishing. [DOI:10.1007/978-3-319-42451-4_10]
Imperato-McGinley, J., & Peterson, R. E. (1976). Male pseudohermaphroditism: The complexities of male phenotypic development. The American Journal of Medicine, 61(2), 251–272. [DOI:10.1016/0002-9343(76)90175-3]
Imperato-McGinley, J., & Zhu, Y. (2002). Androgens and male physiology the syndrome of 5α-reductase-2 deficiency. Molecular and Cellular Endocrinology, 198(1–2), 51–59. [DOI:10.1016/s0303-7207(02)00368-4]
Irwig, M. S. (2015). Safety concerns regarding 5α reductase inhibitors for the treatment of androgenetic alopecia. Current Opinion in Endocrinology, Diabetes & Obesity, 22(3), 248–253. [DOI:10.1097/med.0000000000000158]
Iuliano, S., Izzo, G., Zagari, M. C., Vergine, M., Brunetti, F. S., Brunetti, A., Di Luigi, L., & Aversa, A. (2021). Endocrine management of transgender adults: a clinical approach. Sexes, 2(1), 104–118. [DOI:10.3390/sexes2010009]
Jänne, O., Hemminki, S., Isomaa, V., Kokko, E., Torkkeli, H., Torkkeli, T., & Vierikko, P. (1978). Progestational Activity of Natural and Synthetic Androgens. International Journal of Andrology, 1(s2a) [Endocrine Approach to Male Contraception: Transactions of the Fifth Annual Workshop on the Testis, Held at Geilo, Norway on April 2-5, 1978], 162–174. [DOI:10.1111/j.1365-2605.1978.tb00015.x]
Kicman, A. T. (2008). Pharmacology of anabolic steroids. British Journal of Pharmacology, 154(3), 502–521. [DOI:10.1038/bjp.2008.165]
Kirschvink, J. F. (1963). Studies of Anabolic Steroids. American Journal of Diseases of Children, 106(4), 368–368. [DOI:10.1001/archpedi.1963.02080050370005]
Knuth, U. A., Behre, H., Belkien, L., Bents, H., & Nieschlag, E. (1985). Clinical trial of 19-nortestosterone-hexoxyphenylpropionate (Anadur) for male fertility regulation. Fertility and Sterility, 44(6), 814–821. [DOI:10.1016/s0015-0282(16)49043-6]
Knuth, U. A., Behre, H., Belkien, L., Bents, H., & Nieschlag, E. (1986). 19-Nortestosterone for male fertility regulation. In Zatuchni, G. I., Goldsmith, A., Spieler, J. M., & Sciarra, J. J. (Eds.). Male Contraception: Advances and Future Prospects: Proceedings of an International Workshop on Male Contraception, Advances and Future Prospects, May 28-31, 1985, Geneva, Switzerland (pp. 320–328). Philadelphia: Harper and Row. [Google Scholar] [Google Books] [WorldCat] [PDF]
Knuth, U. A., Yeung, C., & Nieschlag, E. (1989). Combination of 19-nortestosterone-hexyloxyphenylpropionate (Anadur) and depot-medroxyprogesterone-acetate (Clinovir) for male contraception. Fertility and Sterility, 51(6), 1011–1018. [DOI:10.1016/s0015-0282(16)60735-5]
Kuhl, H., & Wiegratz, I. (2017). Das Post-Finasterid-Syndrom. [Post Finasteride Syndrome.] Gynäkologische Endokrinologie, 15(2), 153–163. [DOI:10.1007/s10304-017-0126-2]
Kuiper, G. G., Carlsson, B., Grandien, K., Enmark, E., Häggblad, J., Nilsson, S., & Gustafsson, J. (1997). Comparison of the Ligand Binding Specificity and Transcript Tissue Distribution of Estrogen Receptors α and β. Endocrinology, 138(3), 863–870. [DOI:10.1210/endo.138.3.4979]
Kumar, N., Crozat, A., Li, F., Catterall, J., Bardin, C., & Sundaram, K. (1999). 7α-methyl-19-nortestosterone, a synthetic androgen with high potency: structure-activity comparisons with other androgens. The Journal of Steroid Biochemistry and Molecular Biology, 71(5–6), 213–222. [DOI:10.1016/s0960-0760(99)00143-0]
Lauritzen, C. (1984). Pre- and Postmenopause. In Platt, D. (Ed.). Geriatrics 3: Gynecology · Orthopaedics · Anesthesiology · Surgery · Otorhinolaryngology · Ophthalmology · Dermatology (pp. 2–45). Berlin/Heidelberg: Springer Berlin Heidelberg. [DOI:10.1007/978-3-642-68976-5_1]
Lemmey, A. B., Elamanchi, S. R., Marcora, S. M., Casanova, F., & Maddison, P. J. (2013). Efficacy of nandrolone decanoate in treating rheumatoid cachexia in male rheumatoid arthritis patients. In Matsuno, H. (Ed.). Innovative Rheumatology (pp. 271–285). Rijeka, Croatia: InTech. [DOI:10.5772/53236]
Liu, P. Y., & Handelsman, D. J. (1998). Androgen therapy in non-gonadal disease. In Nieschlag, E., & Behre, H. M. (Eds.). Testosterone: Action · Deficiency · Substitution, 2nd Edition (pp. 473–512). Berlin/Heidelberg: Springer. [DOI:10.1007/978-3-642-72185-4_17]
Marks, L. S. (2004). 5α-reductase: history and clinical importance. Reviews in Urology, 6(Suppl 9), S11–S21. [Google Scholar] [PubMed] [PubMed Central]
Mella, J. M., Perret, M. C., Manzotti, M., Catalano, H. N., & Guyatt, G. (2010). Efficacy and Safety of Finasteride Therapy for Androgenetic Alopecia. Archives of Dermatology, 146(10), 1141–1150. [DOI:10.1001/archdermatol.2010.256]
Need, A. (1989). Cross-over study of fat-corrected forearm mineral content during nandrolone decanoate therapy for osteoporosis. Bone, 10(1), 3–6. [DOI:10.1016/8756-3282(89)90139-7]
Neff, M. S., Goldberg, J., Slifkin, R. F., Eiser, A. R., Calamia, V., Kaplan, M., Baez, A., Gupta, S., & Mattoo, N. (1981). A Comparison of Androgens for Anemia in Patients on Hemodialysis. New England Journal of Medicine, 304(15), 871–875. [DOI:10.1056/nejm198104093041504]
Nieschlag, E. (2010). Clinical trials in male hormonal contraception. Contraception, 82(5), 457–470. [DOI:10.1016/j.contraception.2010.03.020]
Nieschlag, E., & Behre, H. M. (2012). The essential role of testosterone in hormonal male contraception. In Nieschlag, E., Behre, H. M., & Nieschlag, S. (Eds.). Testosterone: Action · Deficiency · Substitution, 4th Edition (pp. 470–493). Cambridge/New York: Cambridge University Press. [DOI:10.1017/cbo9781139003353.023]
Nieschlag, E., Kumar, N., & Sitruk-Ware, R. (2013). 7α-Methyl-19-nortestosterone (MENTR): the Population Council’s contribution to research on male contraception and treatment of hypogonadism. Contraception, 87(3), 288–295. [DOI:10.1016/j.contraception.2012.08.036]
Pan, M. M., & Kovac, J. R. (2016). Beyond testosterone cypionate: evidence behind the use of nandrolone in male health and wellness. Translational Andrology and Urology, 5(2), 213–219. [DOI:10.21037/tau.2016.03.03]
Passeri, M., Pedrazzoni, M., Pioli, G., Butturini, L., Ruys, A., & Cortenraad, M. (1993). Effects of nandrolone decanoate on bone mass in established osteoporosis. Maturitas, 17(3), 211–219. [DOI:10.1016/0378-5122(93)90049-n]
Peters, A. A., Ingman, W. V., Tilley, W. D., & Butler, L. M. (2011). Differential Effects of Exogenous Androgen and an Androgen Receptor Antagonist in the Peri- and Postpubertal Murine Mammary Gland. Endocrinology, 152(10), 3728–3737. [DOI:10.1210/en.2011-1133]
Peterson, R. E., Imperato-McGinley, J., Gautier, T., & Sturla, E. (1977). Male pseudohermaphroditism due to steroid 5α-reductase deficiency. The American Journal of Medicine, 62(2), 170–191. [DOI:10.1016/0002-9343(77)90313-8]
Propecia Finasteride Label. U.S. Food and Drug Administration. [URL] [PDF]
Prunty, F. T., Brooks, R. V., Clayton, B. E., & McSwiney, R. R. (1958). Some Effects of 17α-Ethyl-19-Nortestosterone in Man. Proceedings of the Royal Society of Medicine, 51(7), 557–558. [Google Scholar] [PubMed] [PubMed Central]
Roche, A., Towns, J. W., & Wettenhall, H. (1963). Influence of norethandrolone on the stature of short children. The Journal of Pediatrics, 63(5), 967–976. [DOI:10.1016/s0022-3476(63)80228-0]
Russell, N., & Grossmann, M. (2019). MECHANISMS IN ENDOCRINOLOGY: Estradiol as a male hormone. European Journal of Endocrinology, 181(1), R23–R43. [DOI:10.1530/eje-18-1000]
Sardar, P., Jha, A., Roy, D., Majumdar, U., Guha, P., Roy, S., Banerjee, R., Banerjee, A. K., & Bandyopadhyay, D. (2010). Therapeutic Effects of Nandrolone and Testosterone in Adult Male HIV Patients With AIDS Wasting Syndrome (AWS): A Randomized, Double-Blind, Placebo-Controlled Trial. HIV Clinical Trials, 11(4), 220–229. [DOI:10.1310/hct1104-220]
Sartorius, G. A., Ly, L. P., & Handelsman, D. J. (2014). Male Sexual Function Can Be Maintained Without Aromatization: Randomized Placebo‐Controlled Trial of Dihydrotestosterone (DHT) in Healthy, Older Men for 24 Months. The Journal of Sexual Medicine, 11(10), 2562–2570. [DOI:10.1111/jsm.12550]
Sas, T., Gault, E., Zeger Bardsley, M., Menke, L., Freriks, K., Perry, R., Otten, B., de Muinck Keizer-Schrama, S., Timmers, H., Wit, J., Ross, J., & Donaldson, M. (2014). Safety and Efficacy of Oxandrolone in Growth Hormone-Treated Girls with Turner Syndrome: Evidence from Recent Studies and Recommendations for Use. Hormone Research in Paediatrics, 81(5), 289–297. [DOI:10.1159/000358195]
Schürmeyer, T., Belkien, L., Knuth, U., & Nieschlag, E. (1984). Reversible azoospermia induced by the anabolic steroid 19-nortestosterone. The Lancet, 323(8374), 417–420. [DOI:10.1016/s0140-6736(84)91752-5]
Simpson, E. R., & Jones, M. E. (2007). Of Mice and Men: The Many Guises of Estrogens. In Korach, K. S., & Wintermantel, T. (Eds.). Tissue-Specific Estrogen Action: Novel Mechanisms, Novel Ligands, Novel Therapies (Ernst Schering Foundation Symposium Proceedings, Volume 2006/1) (pp. 45–68). Berlin/Heidelberg: Springer. [DOI:10.1007/2789_2006_016]
Skroza, N., Tolino, E., Mambrin, A., Zuber, S., Balduzzi, V., Marchesiello, A., Bernardini, N., Proietti, I., & Potenza, C. (2018). Adult Acne Versus Adolescent Acne: A Retrospective Study of 1,167 Patients. The Journal of Clinical and Aesthetic Dermatology, 11(1), 21–25. [Google Scholar] [PubMed] [PubMed Central] [URL]
Styne, D. M., & Grumbach, M. M. (2016). Physiology and Disorders of Puberty. In Melmed, S., Polonsky, K. S., Larsen, P. R., Kronenberg, & H. M. (Eds.). Williams Textbook of Endocrinology, 13th Edition (pp. 1074–1218). Philadelphia: Elsevier. [DOI:10.1016/b978-0-323-29738-7.00025-3]
Sundaram, K., & Kumar, N. (2000). 7alpha-Methyl-19-nortestosterone (MENT): the optimal androgen for male contraception and replacement therapy. International Journal of Andrology, 23(S2), 13–15. [DOI:10.1046/j.1365-2605.2000.00004.x]
Sundaram, K., Kumar, N., & Bardin, C. W. (1994). 7α-Methyl-19-nortestosterone: An Ideal Androgen for Replacement Therapy. In Bardin, W. C. (Ed.). Proceedings of the 1992 Laurentian Hormone Conference (Recent Progress in Hormone Research, Volume 49) (pp. 373–376). San Diego: Academic Press. [DOI:10.1016/b978-0-12-571149-4.50027-1]
Sundaram, K., Kumar, N., Monder, C., & Bardin, C. (1995). Different patterns of metabolism determine the relative anabolic activity of 19-norandrogens. The Journal of Steroid Biochemistry and Molecular Biology, 53(1–6), 253–257. [DOI:10.1016/0960-0760(95)00056-6]
Suvisaari, J. (2000). 7α-Methyl-19-Nortestosterone (MENT): Pharmacokinetics and Antigonadotropic Effects in Men. (Doctoral dissertation, University of Helsinki.) Helsinki: University of Helsinki. [Google Scholar] [URL] [PDF]
Thirumalai, A., Ceponis, J., Amory, J. K., Swerdloff, R., Surampudi, V., Liu, P. Y., Bremner, W. J., Harvey, E., Blithe, D. L., Lee, M. S., Hull, L., Wang, C., & Page, S. T. (2018). Effects of 28 Days of Oral Dimethandrolone Undecanoate in Healthy Men: A Prototype Male Pill. The Journal of Clinical Endocrinology & Metabolism, 104(2), 423–432. [DOI:10.1210/jc.2018-01452]
Tóth, M. (2009). Mioanabolikus Szteroidok és Szelektív Androgénreceptormodulátorok: Hatásmechanizmus és Terápiás Perspektívák. [Myoanabolic Steroids and Selective Androgen Receptor Modulators: Mechanism of Action and Perspectives. Orvosi Hetilap, 150(45), 2051–2059. [DOI:10.1556/oh.2009.28739] [Translation]
Tóth, M., & Zakár, T. (1986). Classification of Anabolic Steroids Using the Method of Competitive Metabolism. Experimental and Clinical Endocrinology & Diabetes, 87(2), 125–132. [DOI:10.1055/s-0029-1210533]
Trost, L., Saitz, T. R., & Hellstrom, W. J. (2013). Side Effects of 5‐Alpha Reductase Inhibitors: A Comprehensive Review. Sexual Medicine Reviews, 1(1), 24–41. [DOI:10.1002/smrj.3]
van der Vies, J. (1985). Implications of basic pharmacology in the therapy with esters of nandrolone. Acta Endocrinologica, 110(3 Suppl a), S38–S44. [DOI:10.1530/acta.0.109s0038]
van Zuuren, E. J., Fedorowicz, Z., Carter, B., & Pandis, N. (2015). Interventions for hirsutism (excluding laser and photoepilation therapy alone). Cochrane Database of Systematic Reviews, 2015, CD010334. [DOI:10.1002/14651858.cd010334.pub2]
Vetri, M., Cataldi, A., Naselli, A., & Vetri, A. (2021). Transsexualism Ethiology and Medical Management: Between Scientific Evidence and Personal Experiences. Preprints, 2021030172. [DOI:10.20944/preprints202103.0172.v1]
Wibowo, E., Schellhammer, P., & Wassersug, R. J. (2011). Role of Estrogen in Normal Male Function: Clinical Implications for Patients With Prostate Cancer on Androgen Deprivation Therapy. Journal of Urology, 185(1), 17–23. [DOI:10.1016/j.juro.2010.08.094]
Wibowo, E., & Wassersug, R. J. (2013). The effect of estrogen on the sexual interest of castrated males: Implications to prostate cancer patients on androgen-deprivation therapy. Critical Reviews in Oncology/Hematology, 87(3), 224–238. [DOI:10.1016/j.critrevonc.2013.01.006]
Winters, S. J. (1990). Androgens: Endocrine Physiology and Pharmacology. In Lin, G. C., & Erinoff, L. (Eds.). Anabolic Steroid Abuse (National Institute on Drug Abuse Research Monograph Series, Volume 102) (pp. 113–130). Rockville, Maryland: National Institute on Drug Abuse/U.S. Department of Health and Human Services. [Google Scholar] [PubMed] [Google Books] [PDF]
World Health Organization & Task Force on Methods for the Regulation of Male Fertility. (1993). Comparison of two androgens plus depot-medroxyprogesterone acetate for suppression to azoospermia in Indonesian men. Fertility and Sterility, 60(6), 1062–1068. [DOI:10.1016/s0015-0282(16)56411-5]
Wu, C., & Kovac, J. R. (2016). Novel Uses for the Anabolic Androgenic Steroids Nandrolone and Oxandrolone in the Management of Male Health. Current Urology Reports, 17(10), 72. [DOI:10.1007/s11934-016-0629-8]
Wu, S., Yuen, F., Swerdloff, R. S., Pak, Y., Thirumalai, A., Liu, P. Y., Amory, J. K., Bai, F., Hull, L., Blithe, D. L., Anawalt, B. D., Parman, T., Kim, K., Lee, M. S., Bremner, W. J., Page, S. T., & Wang, C. (2018). Safety and Pharmacokinetics of Single-Dose Novel Oral Androgen 11β-Methyl-19-Nortestosterone-17β-Dodecylcarbonate in Men. The Journal of Clinical Endocrinology & Metabolism, 104(3), 629–638. [DOI:10.1210/jc.2018-01528]
Yuen, F., Thirumalai, A., Pham, C., Swerdloff, R. S., Anawalt, B. D., Liu, P. Y., Amory, J. K., Bremner, W. J., Dart, C., Wu, H., Hull, L., Blithe, D. L., Long, J., Wang, C., & Page, S. T. (2020). Daily Oral Administration of the Novel Androgen 11β-MNTDC Markedly Suppresses Serum Gonadotropins in Healthy Men. The Journal of Clinical Endocrinology & Metabolism, 105(3), e835–e847. [DOI:10.1210/clinem/dgaa032]
\ No newline at end of file
diff --git a/transfemscience.org/articles/oral-p4-low-levels/index.html b/transfemscience.org/articles/oral-p4-low-levels/index.html
index d737636a..767f4807 100644
--- a/transfemscience.org/articles/oral-p4-low-levels/index.html
+++ b/transfemscience.org/articles/oral-p4-low-levels/index.html
@@ -1 +1 @@
-Oral Progesterone Achieves Very Low Levels of Progesterone and Has Only Weak Progestogenic Effects - Transfeminine Science
Oral Progesterone Achieves Very Low Levels of Progesterone and Has Only Weak Progestogenic Effects
By Aly | First published August 4, 2018 | Last modified March 30, 2023
Abstract / TL;DR
Oral progesterone is the most widely used form of progesterone in transfeminine hormone therapy. Because of previous studies using inaccurate blood tests (immunoassays without adequate chromatographic purification), it was thought that typical therapeutic dosages of oral progesterone produced progesterone levels that reached typical luteal-phase levels in cisgender women (which range from about 7 to 22 ng/mL). However, newer studies using more accurate blood tests (immunoassays with adequate purification and mass spectrometry-based assays) have shown that 100 mg/day progesterone—with or without food—achieves very low peak progesterone levels of only about 2 to 3 ng/mL and average progesterone levels over 24 hours of only about 0.1 to 0.6 ng/mL. In accordance, oral progesterone has often shown only weak progestogenic effects in clinical studies. Higher doses of oral progesterone that might achieve better levels are limited by persistingly low progesterone levels, pronounced neurosteroid side effects caused by the first pass of progesterone through the liver, and substantial variability between individuals. While the progesterone levels with oral progesterone are apparently sufficient for endometrial protection in cisgender women, they are unlikely to be adequate for desired effects in transfeminine people. For these reasons, transfeminine people and their clinicians may wish to avoid oral progesterone if the aim is therapeutic progestogenic effects. Instead, non-oral forms of progesterone with greater bioavailability like rectal or injectable progesterone can be used. Alternatively, progestins, which are likewise fully effective progestogens, can be employed.
Introduction
The major female sex hormones are estrogens and progestogens, and both may be used in transfeminine hormone therapy. Progestogens are useful in transfeminine people for helping to suppress testosterone levels and possibly though not certainly influencing breast development. Progestogens include progesterone as well as synthetic progestogens known as progestins. Progesterone has relatively unfavorable pharmacokinetics, which has been overcome with progestins. However, progestins have differing pharmacodynamic properties compared to progesterone, which can potentially be unfavorable. As such, there is interest in using progesterone instead of progestins in transfeminine people and other populations like cisgender women despite its poor pharmacokinetic properties.
Progesterone is available in formulations for use via a variety of different routes, including oral, sublingual, topical, vaginal, rectal, and injectable administration (Wiki; Table). Among these routes, oral administration is the easiest and most convenient, and in relation to this, oral progesterone is the most widely used form of progesterone in transfeminine people. However, the pharmacokinetic problems of progesterone limit the favorability of oral progesterone. Moreover, these limitations of oral progesterone actually appear to be much more substantial than is generally realized, a fact that has been obscured by methodological limitations of many—but not all—of the pharmacokinetic studies that have characterized oral progesterone. The purpose of this article is to explain and review these findings, as well as to explore solutions and alternatives to oral progesterone for progestogen therapy in transfeminine people.
Progesterone Levels with Oral Progesterone
Oral micronized progesterone, or simply oral progesterone, is the form of progesterone that is used by the oral route as a pharmaceutical medication. It is an oil suspension of micronized progesterone crystals contained in gelatin capsules. The formulation is marketed under brand names including Prometrium, Utrogestan, and Microgest, among many others. Oral progesterone has very low bioavailability (≤10%) due to the first pass through the intestines and liver with oral administration. As a result of the first pass, most of the delivered progesterone with oral progesterone is metabolized into neurosteroid metabolites such as allopregnanolone and pregnanolone before reaching the bloodstream (de Lignieres, Dennerstein, & Backstrom, 1995). This is why oral progesterone has alcohol-like side effects like sedation that are not shared by typical doses of non-oral progesterone such as vaginal progesterone or progesterone by injection. In spite of the low bioavailability of oral progesterone, typical clinical doses of oral progesterone, such as 100 to 300 mg/day, have been reported to produce progesterone levels measured with immunoassays that are similar to those in the normal luteal phase of the menstrual cycle in cisgender women (Simon et al., 1993). For this reason, it has been believed that oral progesterone can achieve high and physiologically adequate levels of progesterone.
Figure 1: Progesterone levels during the menstrual cycle in normal premenopausal women (Stricker et al., 2006). The dashed horizontal lines are the mean levels for each curve and the dashed vertical line demarcates mid-cycle (when ovulation occurs). Progesterone levels are normally elevated only during the luteal phase.
Figure 2: Progesterone levels measured by immunoassay after single 100 to 300 mg doses of oral micronized progesterone in postmenopausal women (Simon et al., 1993). The horizontal dashed lines are mean levels over 24 hours. Progesterone levels appeared to reach concentrations comparable to normal luteal-phase levels. However, these levels were in fact not accurate due to the use of immunoassays (Nahoul & de Ziegler, 1994).
A notable study using LC–MS found maximal progesterone levels of only about 2 ng/mL and average progesterone levels over a period of 24 hours of only about 0.14 ng/mL after a single 100 mg dose of oral progesterone (Levine & Watson, 2000; Kuhl & Schneider, 2013). Another more recent study with LC–MS found progesterone levels of around 2.5 to 3 ng/mL at peak and average progesterone levels over 24 hours of around 0.6 ng/mL after a single 100 mg dose of oral progesterone with food (Lobo et al., 2019). (It should be noted that intake with food is known to increase the bioavailability of oral progesterone by a few-fold (Wiki; Bijuva FDA Label; Simon et al., 1993; Prometrium FDA Review, 1996; Pickar et al., 2015).) These progesterone levels are well below normal luteal-phase levels of progesterone, which range from 7 to 22 ng/mL with LC–MS (Nakamoto, 2016). Studies that have directly compared quantification of progesterone with immunoassays against more reliable methods have found that immunoassays overestimate progesterone levels by 5- to 8-fold (Nahoul, Dehennin, & Scholler, 1987; Nahoul & de Ziegler, 1994; Levine & Watson, 2000; Kuhl, 2011; Kuhl & Schneider, 2013; Davey, 2018). In one small study of a few individuals, the degree of overestimation varied from 2-fold to 40-fold with several different commercial immunoassays (Sapin et al., 2000). These findings are obscure and still relatively little-known in the scientific and medical communities. In any case, it is clear that oral progesterone achieves progesterone levels that are far lower than once thought and are well below the luteal-phase levels that would be therapeutically desirable for transfeminine people.
Figure 3: Progesterone levels measured by immunoassay or LC–MS after a single dose of oral or vaginal micronized progesterone in postmenopausal women (Levine & Watson, 2000; Kuhl & Schneider, 2013). Levels of progesterone with oral progesterone measured by immunoassay were falsely high due to cross-reactivity. Conversely, progesterone levels measured by LC–MS or with vaginal progesterone can be considered accurate.
Figure 4: Progesterone levels measured by LC–MS with 100 mg/day oral micronized progesterone taken with food in postmenopausal women (Lobo et al., 2019). The horizontal dashed line is the mean level over 24 hours. Food increases progesterone levels with oral progesterone by about 2- to 3-fold (Bijuva FDA Label; Simon et al., 1993). The progesterone levels measured in this study can be considered accurate to due to the use of LC–MS.
Therapeutic Implications
Progestogenic Potency and Effects
A variety of perplexing findings on the clinical progestogenic effects of oral progesterone have been made over the decades and can now be readily explained by the newer data on oral progesterone with better analytic methods. Oral progesterone is used in clinical medicine mainly to protect the endometrium from unopposed stimulation by estrogens in menopausal cisgender women and is able to reliably prevent endometrial hyperplasia induced by estrogens even with the low progesterone levels that typical clinical doses achieve (Wiki). However, oral progesterone failed to provide adequate protection against estrogen-mediated endometrial cancer risk in a large observational study (Davey, 2018). Oral progesterone even at very high doses also is unable to produce full endometrial transformation—a normal effect of luteal-phase levels of progesterone—whereas vaginal and injectable progesterone are effective (de Ziegler et al., 2013). For this reason, oral progesterone, in contrast to parenteral progesterone, is considered to be inappropriate for use in assisted reproduction (de Ziegler et al., 2013). Oral progesterone additionally failed to suppress testosterone levels even at high doses (400 mg/day) in cisgender males (Trollan et al., 1993; Wiki). Conversely, progestins, rectal progesterone, and injectable progesterone can all produce robust testosterone suppression in cisgender males (Wiki; Aly, 2019). Similarly, oral progesterone has little or no apparent antigonadotropic effect in menopausal cisgender women, which is again in notable contrast to progestins (Holst, 1983; Holst et al., 1983; Ottosson, 1984; Maxson & Hargrove, 1985; Saarikoski, Yliskosk, & Penttilä, 1990).
Unlike other clinically used progestogens, the addition of oral progesterone to estrogen therapy in menopausal women has not been associated with increased risk of venous thromboembolism (VTE; blood clots) (Wiki). Nor has it been associated with increased breast cancer risk in the short-term (<5 years of therapy) (Wiki). However, with long-term use (≥5 years), the combination of estrogen plus oral progesterone is associated with significantly greater risk of breast cancer relative to estrogen alone similarly to other progestogens (Aly, 2020; Sam, 2020; Wiki; Table). This has been said to be consistent with a weak proliferative effect of oral progesterone on the breasts such that a longer duration of exposure is necessary for a quantifiable increase in breast cancer risk to manifest (Kuhl & Schneider, 2013; Davey, 2018). It is also consistent with preclinical research, which clearly suggests a carcinogenic role for progesterone and progesterone receptor activation in the breast (Kuhl & Schneider, 2013; Trabert et al., 2020). The preceding clinical findings on endometrial efficacy, testosterone and gonadotropin suppression, VTE risk, and breast cancer risk with oral progesterone are in contrast to those with almost all clinically used progestins (with the exception of the oral progesterone-like dydrogesterone). These previously perplexing discrepancies can be readily explained by the very low levels of progesterone that are now known to be achieved with oral progesterone.
Bioavailability, Half-Life, and Duration
Considering the much lower levels of progesterone observed with oral progesterone in studies using reliable analytic methods, the bioavailability of oral progesterone needs to be reassessed. In studies with immunoassays, the bioavailability of oral progesterone has been reported to be around 10% (Wiki). The true oral bioavailability of progesterone is unknown at this time as studies with reliable analytic methods have not been conducted. In any case, it can be assumed that it may be closer to around 1 or 2% based on the findings that immunoassays overestimate progesterone levels by 5- to 8-fold.
The elimination half-life of progesterone with oral progesterone has been determined in studies employing immunoassays to be 16 to 18 hours (Wiki). Based on the fact that the blood half-life of progesterone administered by intravenous injection is very short at a range of only 3 minutes to 1.5 hours (Wiki), the reported half-life of progesterone with oral progesterone is much longer than one would expect. Oral estradiol has a relatively long half-life of 13 to 20 hours due to formation with the first pass of a circulating reservoir of estrogen conjugates that are slowly converted back into estradiol (Kuhl, 2005; Wiki). In contrast to estradiol however, progesterone itself has no available hydroxyl groups for conjugation and an analogous circulating reservoir of progesterone conjugates that can be converted back into progesterone is not known to be the case (Kuhl, 2005).
Studies with more reliable analytic methods like LC–MS have found a half-life of progesterone with oral progesterone of 5 to 10 hours and a duration of highly elevated progesterone levels of only about 4 to 8 hours (Wiki; Graphs). These findings indicate that oral progesterone has a much shorter duration than previously thought as well. As such, if oral progesterone is used, it may be advisable to take it in divided doses multiple times per day to allow for more sustained progestogenic exposure.
Higher Oral Progesterone Doses and Neurosteroid Side Effects
Use of higher doses of oral progesterone than typical doses is likely to achieve dose-dependently higher progesterone levels (Table). However, based on how low progesterone levels are with oral progesterone using reliable analytic techniques, even very high doses would still be expected to achieve only low progesterone levels in most cases. Moreover, high doses of oral progesterone result in very high levels of its neurosteroid metabolites and have been found to produce substantial alcohol-like side effects (i.e., central depression and effects within that umbrella) (Wiki; Wiki). These limitations are likely to preclude higher doses of oral progesterone from being practical.
Figure 5: Levels of progesterone, allopregnanolone, and pregnanolone in premenopausal women following a single dose of oral progesterone or vaginal progesterone (as a suppository) (de Lignieres, Dennerstein, & Backstrom, 1995). Allopregnanolone and pregnanolone levels were determined by MS-based assays while progesterone levels were measured by immunoassay with chromatographic separation. Hence, the levels should be reliable.
A Note on Oral Progesterone’s Metabolites
Although progesterone levels with oral progesterone are very low, the metabolites of progesterone are formed in disproportionate amounts with the first pass (Sitruk-Ware et al., 1987; de Lignieres, Dennerstein, & Backstrom, 1995; de Lignieres, 1999; de Ziegler & Fanchin, 2000; Lobo, 2000; Kuhl, 2005). Moreover, while much less potent than progesterone, some of these metabolites have been found to have progestogenic activity similarly to progesterone (e.g., Besch et al., 1965; Junkermann, Runnebaum, & Lisboa, 1977; Lobo, 2000). This activity derives either from them having intrinsic progestogenic activity of their own or from being converted back into progesterone or other progestogenic metabolites (including in an intracrine fashion within tissues, for instance in the uterus). Examples of such metabolites include 20α-dihydroprogesterone, 20β-dihydroprogesterone, 5α-dihydroprogesterone, 3β-dihydroprogesterone, allopregnanolone, and 11-deoxycorticosterone. If the metabolites of oral progesterone contribute significantly to its progestogenic activity, then the progestogenic strength of oral progesterone would be greater than that implied by the progesterone levels that occur with it alone. However, this possibility is only theoretical and there is little literature discussing it. More research would be needed to determine if the metabolites of oral progesterone do indeed play a meaningful role in its progestogenic potency. In any case, oral progesterone is still a relatively weak progestogen based on clinical studies of its progestogenic effects.
Alternative Options to Oral Progesterone
Non-Oral Forms of Progesterone
Non-oral forms of progesterone, such as vaginal progesterone, rectal progesterone, sublingual progesterone, and progesterone by injection, have been found to achieve much higher progesterone levels than oral progesterone (Wiki). They can be used instead of oral progesterone to achieve higher and more adequate progesterone levels. Unfortunately however, while more effective than oral progesterone, non-oral progesterone routes have various limitations of their own.
Vaginal progesterone is of course not possible in transfeminine people who have not undergone vaginoplasty. And in those who have undergone vaginoplasty, the lining of the neovagina is either skin (penile inversion vaginoplasty) or intestine (sigmoid colon vaginoplasty) rather than the normal vaginal mucosa. As such, the absorptive characteristics of neovaginal administration are likely not the same as vaginal administration (Aly, 2018). It is notable that transdermal progesterone achieves very low progesterone levels similarly to oral progesterone and is not a good option for progesterone therapy (Wiki; Hermann et al., 2005; Graph). Progesterone levels with neovaginal administration of progesterone in those who have undergone penile inversion vaginoplasty are likely to be low similarly.
Rectal progesterone is an excellent route that achieves high progesterone levels comparable to the levels of progesterone that occur during the normal luteal phase (Wiki; Graphs). It has a somewhat short duration and twice daily use may be warranted for more sustained levels however. A more important problem is that the availability of pharmaceutical rectal progesterone suppositories throughout the world is limited and they are not marketed in most countries (Wiki). In any case, rectal progesterone suppositories may be available from compounding pharmacies in some countries. In addition, oral micronized progesterone capsules are available ubiquitously and have been administered vaginally instead of orally with success (Miles et al., 1994; Wang et al., 2019). Administration of oral micronized progesterone capsules rectally instead of orally likewise may be effective and may achieve much higher progesterone levels than oral administration (Aly, 2018). However, rectal administration of oral progesterone capsules has not been formally studied. Although rectal progesterone is effective, it is fairly inconvenient. This may be especially true with long-term therapy. In any case, of the available non-oral forms of progesterone, rectal progesterone is probably the best overall.
Figure 6: Progesterone levels with a single suppository containing 100 mg progesterone administered rectally or vaginally in premenopausal women (Chakmakjian & Zachariah, 1987).
Sublingual progesterone appears to achieve high and more physiological progesterone levels than oral progesterone but has a short duration of highly elevated progesterone levels similarly and necessitates administration several times per day (Wiki; Graph). Moreover, although sublingual progesterone may have been more widely available in the past (Wiki), it is available today only in a couple of Eastern European countries (Wiki). It might be available from compounding pharmacies in some countries however. While never formally studied, it may be possible to use oral micronized progesterone capsules sublingually instead of orally. However, this route is complicated by the fact that this form of progesterone is suspended in oil within gelatin capsules. Hence, sublingual administration of oral micronized progesterone is likely to be difficult and potentially unpleasant.
Progesterone by intramuscular or subcutaneous injection can easily achieve very high progesterone levels (Wiki; Graphs; Wiki; Graph). However, progesterone administered by this route has a relatively short duration when compared to other injectable sex-hormone formulations and requires injection once every 1 to 3 days. This is simply too frequent for most people, especially with long-term therapy. In addition, progesterone by subcutaneous injection, which is more convenient than progesterone by intramuscular injection, has limited availability and is marketed mostly only in Europe (Wiki). In contrast to other sex hormones like estradiol and testosterone, progesterone esters that are more fat-soluble than progesterone and extend its duration when used in injectable form are not possible since progesterone has no free hydroxyl groups available for esterification. Injectable aqueous suspensions of progesterone that had much longer durations than the oil solutions and aqueous solutions that are used by injection today were previously available (Wiki; Wiki; Aly, 2019). However, they were associated with painful injection site reactions and this led to their discontinuation. In any case, injectable aqueous suspensions of progesterone do actually seem to remain available for people in a couple of Eastern European countries today (Aly, 2019).
In conclusion, oral progesterone achieves very low progesterone levels at typical clinical doses and produces only weak progestogenic effects that seem to be far from physiologically adequate. Although use of higher doses of oral progesterone is likely to achieve higher progesterone levels, such doses are likely to be impractical because progesterone levels will still be low even at higher doses and the neurosteroid side effects of oral progesterone will be much more substantial and difficult to tolerate.
Due to its limitations, transfeminine people and clinicians treating them may wish to avoid oral progesterone if the intended goal is to produce therapeutic progestogenic effects. Instead, non-oral progesterone routes, such as rectal and injected progesterone, although with various limitations such as limited availability and inconvenience, can be used. Alternatively, progestins, particularly those with more favorable profiles, can be used instead of progesterone altogether.
Oral progesterone may perhaps be most appropriately conceptualized as a potent neurosteroid prodrug with weak progestogenic effects. Conversely, non-oral progesterone, as well as progestins, can be regarded as potent progestogens with either physiological or no neurosteroid effects, respectively.
Additional Content
Literature
The sources and excerpts collected here go in-depth on much of what has been described in this article on the topic of the measurement problems and low progesterone levels with oral progesterone.
Besch, P. K., Barry, R. D., Vorys, N., Stevens, V., & Ullery, J. C. (1965). A review of some aspects of the metabolism of progestational agents. Metabolism, 14(3), 432–443. [DOI:10.1016/0026-0495(65)90031-4]
Bijuva Estradiol/Progesterone Label. U.S. Food and Drug Administration. [URL] [PDF]
Chakmakjian, Z. H., & Zachariah, N. Y. (1987). Bioavailability of progesterone with different modes of administration. The Journal of Reproductive Medicine, 32(6), 443–448. [Google Scholar] [PubMed] [PDF]
Conklin, S. E., & Knezevic, C. E. (2020). Advancements in the gold standard: Measuring steroid sex hormones by mass spectrometry. Clinical Biochemistry, 82, 21–32. [DOI:10.1016/j.clinbiochem.2020.03.008]
Davey, D. A. (2018). Menopausal hormone therapy: a better and safer future. Climacteric, 21(5), 454–461. [DOI:10.1080/13697137.2018.1439915]
de Lignières, B., Dennerstein, L., & Backstrom, T. (1995). Influence of route of administration on progesterone metabolism. Maturitas, 21(3), 251–257. [DOI:10.1016/0378-5122(94)00882-8]
de Lignières, B. (1999). Oral micronized progesterone. Clinical Therapeutics, 21(1), 41–60. [DOI:10.1016/S0149-2918(00)88267-3]
de Ziegler, D., & Fanchin, R. (2000). Progesterone and progestins: applications in gynecology. Steroids, 65(10–11), 671–679. [DOI:10.1016/S0039-128X(00)00123-9]
de Ziegler, D., Streuli, I., Marszalek, A., Gayet, V., & Chapron, C. (2013). Preparing the Endometrium to Maximize Success: The Dynamics of Artificial Cycles. In Sauer, M. V. (Ed.). Principles of Oocyte and Embryo Donation, 2nd Edition (pp. 109–127). London: Springer. [DOI:10.1007/978-1-4471-2392-7_9]
Hermann, A. C., Nafziger, A. N., Victory, J., Kulawy, R., Rocci Jr, M. L., & Bertino Jr, J. S. (2005). Over‐the‐Counter Progesterone Cream Produces Significant Drug Exposure Compared to a Food and Drug Administration‐Approved Oral Progesterone Product. The Journal of Clinical Pharmacology, 45(6), 614–619. [DOI:10.1177/0091270005276621]
Holst, J. (1983). Percutaneous estrogen therapy: Endometrial response and metabolic effects. Acta Obstetricia et Gynecologica Scandinavica, 62(Suppl 115), 4–30. [DOI:10.3109/00016348309155363]
Holst, J., Cajander, S., Carlström, K., Damber, M. G., & von Schoultz, B. (1983). Percutaneous oestrogen therapy opposed by lynestrenol or natural progesterone-effects on circulating oestrogens, FSH, sex hormone binding globulin and pregnancy zone protein. Maturitas, 5(1), 1–8. [DOI:10.1016/0378-5122(83)90015-4]
Junkermann, H., Runnebaum, B., & Lisboa, B. P. (1977). New progesterone metabolites in human myometrium. Steroids, 30(1), 1–14. [DOI:10.1016/0039-128X(77)90131-3]
Kuhl, H. (2005). Pharmacology of Estrogens and Progestogens: Influence of Different Routes of Administration. Climacteric, 8(Suppl 1), 3–63. [DOI:10.1080/13697130500148875] [PDF]
Kuhl, H. (2011). Pharmacology of progestogens. Journal für Reproduktionsmedizin und Endokrinologie [Journal of Reproductive Medicine and Endocrinology], 8(1), 157–177. [URL]
Kuhl, H., & Schneider, H. P. G. (2013). Progesterone–promoter or inhibitor of breast cancer. Climacteric, 16(Suppl 1), 54–68. [DOI:10.3109/13697137.2013.768806]
Lobo, R. A. (2000). Progestogens. In Lobo, R. A., Kelsey, J., & Marcus, R. (Eds.). Menopause: Biology and Pathobiology (pp. 429–444). Burlington: Academic Press. [Google Books]
Lobo, R. A., Liu, J., Stanczyk, F. Z., Constantine, G. D., Pickar, J. H., Shadiack, A. M., Bernick, B., & Mirkin, S. (2019). Estradiol and progesterone bioavailability for moderate to severe vasomotor symptom treatment and endometrial protection with the continuous-combined regimen of TX-001HR (oral estradiol and progesterone capsules). Menopause (New York, NY), 26(7), 720–727.[DOI:10.1097/GME.0000000000001306]
Levine, H., & Watson, N. (2000). Comparison of the pharmacokinetics of Crinone 8% administered vaginally versus Prometrium administered orally in postmenopausal women. Fertility and Sterility, 73(3), 516–521. [DOI:10.1016/S0015-0282(99)00553-1]
Maxson, W. S., & Hargrove, J. T. (1985). Bioavailability of oral micronized progesterone. Fertility and Sterility, 44(5), 622–626. [DOI:10.1016/S0015-0282(16)48977-6]
Miles, R. A., Paulson, R. J., Lobo, R. A., Press, M. F., Dahmoush, L., & Sauer, M. V. (1994). Pharmacokinetics and endometrial tissue levels of progesterone after administration by intramuscular and vaginal routes: a comparative study. Fertility and Sterility, 62(3), 485–490. [DOI:10.1016/S0015-0282(16)56935-0]
Nahoul, K., Dehennin, L., & Scholler, R. (1987). Radioimmunoassay of plasma progesterone after oral administration of micronized progesterone. Journal of Steroid Biochemistry, 26(2), 241–249. [DOI:10.1016/0022-4731(87)90078-1]
Nahoul, K., Dehennin, L., Jondet, M., & Roger, M. (1993). Profiles of plasma estrogens, progesterone and their metabolites after oral or vaginal administration of estradiol or progesterone. Maturitas, 16(3), 185–202. [DOI:10.1016/0378-5122(93)90064-O]
Nahoul, K., & de Ziegler, D. (1994). “ Validity” of serum progesterone levels after oral progesterone. Fertility and Sterility, 61(4), 790–792. [DOI:10.1016/S0015-0282(16)56666-7]
Nakamoto, J. (2016). Endocrine Testing. In Jameson, J. L., & De Groot, L. J. (Eds.). Endocrinology: Adult and Pediatric, 7th Edition (pp. 2655–2688.e1). Philadelphia: Saunders/Elsevier. [DOI:10.1016/B978-0-323-18907-1.00154-2]
Ottosson, U. B. (1984). Oral progesterone and estrogen/progestogen therapy: effects of natural and synthetic hormones on subfractions of HDL cholesterol and liver proteins. Acta Obstetricia et Gynecologica Scandinavica, 63(Suppl 127), 1–37. [DOI:10.3109/00016348409157016]
Pickar, J. H., Bon, C., Amadio, J. M., Mirkin, S., & Bernick, B. (2015). Pharmacokinetics of the first combination 17β-estradiol/progesterone capsule in clinical development for menopausal hormone therapy. Menopause (New York, NY), 22(12), 1308–1316. [DOI:10.1097/GME.0000000000000467]
Prometrium FDA Review 1996. Application Number: NDA 19-781. Clinical Pharmacology and Biopharmaceutics Review(s) [Prometrium]. Center for Drug Evaluation and Research, U.S. Food and Drug Administration. [PDF]
Saarikoski, S., Yliskosk, M., & Penttilä, I. (1990). Sequential use of norethisterone and natural progesterone in pre-menopausal bleeding disorders. Maturitas, 12(2), 89–97. [DOI:10.1016/0378-5122(90)90086-L]
Sapin, R., Neamtu, D., Gasser, F., Ohl, J., Grunenberger, F., & Grucker, D. (2000). De la prudence lors de l’utilisation des dosages directs de progestérone. [Caution when using direct progesterone assays.] Immuno-analyse et Biologie Spécialisée, 3(15), 203–204. [DOI:10.1016/S0923-2532(00)80010-1] [Translation]
Simon, J. A., Robinson, D. E., Andrews, M. C., Hildebrand III, J. R., Rocci Jr, M. L., Blake, R. E., & Hodgen, G. D. (1993). The absorption of oral micronized progesterone: the effect of food, dose proportionality, and comparison with intramuscular progesterone. Fertility and Sterility, 60(1), 26–33. [DOI:10.1016/S0015-0282(16)56031-2]
Sitruk-Ware, R., Bricaire, C., De Lignieres, B., Yaneva, H., & Mauvais-Jarvis, P. (1987). Oral micronized progesterone: Bioavailability pharmacokinetics, pharmacological and therapeutic implications—A review. Contraception, 36(4), 373–402. [DOI:10.1016/0010-7824(87)90088-6]
Stricker, R., Eberhart, R., Chevailler, M. C., Quinn, F. A., Bischof, P., & Stricker, R. (2006). Establishment of detailed reference values for luteinizing hormone, follicle stimulating hormone, estradiol, and progesterone during different phases of the menstrual cycle on the Abbott ARCHITECT® analyzer. Clinical Chemistry and Laboratory Medicine (CCLM), 44(7), 883–887. [DOI:10.1515/CCLM.2006.160]
Tollan, A., Øian, P., Kjeldsen, S. E., Eide, I., & Maltau, J. M. (1993). Progesterone reduces sympathetic tone without changing blood pressure or fluid balance in men. Gynecologic and Obstetric Investigation, 36(4), 234–238. [DOI:10.1159/000292636]
Trabert, B., Sherman, M. E., Kannan, N., & Stanczyk, F. Z. (2020). Progesterone and breast cancer. Endocrine Reviews, 41(2), 320–344. [DOI:10.1210/endrev/bnz001]
Wang, H., Liu, M., Fu, Q., & Deng, C. (2019). Pharmacokinetics of hard micronized progesterone capsules via vaginal or oral route compared with soft micronized capsules in healthy postmenopausal women: a randomized open-label clinical study. Drug Design, Development and Therapy, 13, 2475–2482. [DOI:10.2147/dddt.s204624]
Woodward, G. M., & Rumsby, G. (2019). Steroid Profiling: Analytical Perspectives. In Rumsby, G., Woodward, G. M. (Eds.). Disorders of Steroidogenesis: Guide to Steroid Profiling and Biochemical Diagnosis (pp. 27–40). Cham: Springer. [DOI:10.1007/978-3-319-96364-8_3]
\ No newline at end of file
+Oral Progesterone Achieves Very Low Levels of Progesterone and Has Only Weak Progestogenic Effects - Transfeminine Science
Oral Progesterone Achieves Very Low Levels of Progesterone and Has Only Weak Progestogenic Effects
By Aly | First published August 4, 2018 | Last modified May 8, 2025
Abstract / TL;DR
Oral progesterone is the most widely used form of progesterone in transfeminine hormone therapy. Because of previous studies using inaccurate blood tests (immunoassays without adequate chromatographic purification), it was thought that typical therapeutic dosages of oral progesterone produced progesterone levels that reached typical luteal-phase levels in cisgender women (which range from about 7 to 22 ng/mL). However, newer studies using more accurate blood tests (immunoassays with adequate purification and mass spectrometry-based assays) have shown that 100 mg/day progesterone—with or without food—achieves very low peak progesterone levels of only about 2 to 3 ng/mL and average progesterone levels over 24 hours of only about 0.1 to 0.6 ng/mL. In accordance, oral progesterone has often shown only weak progestogenic effects in clinical studies. Higher doses of oral progesterone that might achieve better levels are limited by persistingly low progesterone levels, pronounced neurosteroid side effects caused by the first pass of progesterone through the liver, and substantial variability between individuals. While the progesterone levels with oral progesterone are apparently sufficient for endometrial protection in cisgender women, they are unlikely to be adequate for desired effects in transfeminine people. For these reasons, transfeminine people and their clinicians may wish to avoid oral progesterone if the aim is therapeutic progestogenic effects. Instead, non-oral forms of progesterone with greater bioavailability like rectal or injectable progesterone can be used. Alternatively, progestins, which are likewise fully effective progestogens, can be employed.
Introduction
The major female sex hormones are estrogens and progestogens, and both may be used in transfeminine hormone therapy. Progestogens are useful in transfeminine people for helping to suppress testosterone levels and possibly though not certainly influencing breast development. Progestogens include progesterone as well as synthetic progestogens known as progestins. Progesterone has relatively unfavorable pharmacokinetics, which has been overcome with progestins. However, progestins have differing pharmacodynamic properties compared to progesterone, which can potentially be unfavorable. As such, there is interest in using progesterone instead of progestins in transfeminine people and other populations like cisgender women despite its poor pharmacokinetic properties.
Progesterone is available in formulations for use via a variety of different routes, including oral, sublingual, topical, vaginal, rectal, and injectable administration (Wiki; Table). Among these routes, oral administration is the easiest and most convenient, and in relation to this, oral progesterone is the most widely used form of progesterone in transfeminine people. However, the pharmacokinetic problems of progesterone limit the favorability of oral progesterone. Moreover, these limitations of oral progesterone actually appear to be much more substantial than is generally realized, a fact that has been obscured by methodological limitations of many—but not all—of the pharmacokinetic studies that have characterized oral progesterone. The purpose of this article is to explain and review these findings, as well as to explore solutions and alternatives to oral progesterone for progestogen therapy in transfeminine people.
Progesterone Levels with Oral Progesterone
Oral micronized progesterone, or simply oral progesterone, is the form of progesterone that is used by the oral route as a pharmaceutical medication. It is an oil suspension of micronized progesterone crystals contained in gelatin capsules. The formulation is marketed under brand names including Prometrium, Utrogestan, and Microgest, among many others. Oral progesterone has very low bioavailability (≤10%) due to the first pass through the intestines and liver with oral administration. As a result of the first pass, most of the delivered progesterone with oral progesterone is metabolized into neurosteroid metabolites such as allopregnanolone and pregnanolone before reaching the bloodstream (de Lignieres, Dennerstein, & Backstrom, 1995). This is why oral progesterone has alcohol-like side effects like sedation that are not shared by typical doses of non-oral progesterone such as vaginal progesterone or progesterone by injection. In spite of the low bioavailability of oral progesterone, typical clinical doses of oral progesterone, such as 100 to 300 mg/day, have been reported to produce progesterone levels measured with immunoassays that are similar to those in the normal luteal phase of the menstrual cycle in cisgender women (Simon et al., 1993). For this reason, it has been believed that oral progesterone can achieve high and physiologically adequate levels of progesterone.
Figure 1: Progesterone levels during the menstrual cycle in normal premenopausal women (Stricker et al., 2006). The dashed horizontal lines are the mean levels for each curve and the dashed vertical line demarcates mid-cycle (when ovulation occurs). Progesterone levels are normally elevated only during the luteal phase.
Figure 2: Progesterone levels measured by immunoassay after single 100 to 300 mg doses of oral micronized progesterone in postmenopausal women (Simon et al., 1993). The horizontal dashed lines are mean levels over 24 hours. Progesterone levels appeared to reach concentrations comparable to normal luteal-phase levels. However, these levels were in fact not accurate due to the use of immunoassays (Nahoul & de Ziegler, 1994).
A notable study using LC–MS found maximal progesterone levels of only about 2 ng/mL and average progesterone levels over a period of 24 hours of only about 0.14 ng/mL after a single 100 mg dose of oral progesterone (Levine & Watson, 2000; Kuhl & Schneider, 2013). Another more recent study with LC–MS found progesterone levels of around 2.5 to 3 ng/mL at peak and average progesterone levels over 24 hours of around 0.6 ng/mL after a single 100 mg dose of oral progesterone with food (Lobo et al., 2019). (It should be noted that intake with food is known to increase the bioavailability of oral progesterone by a few-fold (Wiki; Bijuva FDA Label; Simon et al., 1993; Prometrium FDA Review, 1996; Pickar et al., 2015).) These progesterone levels are well below normal luteal-phase levels of progesterone, which range from 7 to 22 ng/mL with LC–MS (Nakamoto, 2016). Studies that have directly compared quantification of progesterone with immunoassays against more reliable methods have found that immunoassays overestimate progesterone levels by 5- to 8-fold (Nahoul, Dehennin, & Scholler, 1987; Nahoul & de Ziegler, 1994; Levine & Watson, 2000; Kuhl, 2011; Kuhl & Schneider, 2013; Davey, 2018). In one small study of a few individuals, the degree of overestimation varied from 2-fold to 40-fold with several different commercial immunoassays (Sapin et al., 2000). These findings are obscure and still relatively little-known in the scientific and medical communities. In any case, it is clear that oral progesterone achieves progesterone levels that are far lower than once thought and are well below the luteal-phase levels that would be therapeutically desirable for transfeminine people.
Figure 3: Progesterone levels measured by immunoassay or LC–MS after a single dose of oral or vaginal micronized progesterone in postmenopausal women (Levine & Watson, 2000; Kuhl & Schneider, 2013). Levels of progesterone with oral progesterone measured by immunoassay were falsely high due to cross-reactivity. Conversely, progesterone levels measured by LC–MS or with vaginal progesterone can be considered accurate.
Figure 4: Progesterone levels measured by LC–MS with 100 mg/day oral micronized progesterone taken with food in postmenopausal women (Lobo et al., 2019). The horizontal dashed line is the mean level over 24 hours. Food increases progesterone levels with oral progesterone by about 2- to 3-fold (Bijuva FDA Label; Simon et al., 1993). The progesterone levels measured in this study can be considered accurate to due to the use of LC–MS.
Therapeutic Implications
Progestogenic Potency and Effects
A variety of perplexing findings on the clinical progestogenic effects of oral progesterone have been made over the decades and can now be readily explained by the newer data on oral progesterone with better analytic methods. Oral progesterone is used in clinical medicine mainly to protect the endometrium from unopposed stimulation by estrogens in menopausal cisgender women and is able to reliably prevent endometrial hyperplasia induced by estrogens even with the low progesterone levels that typical clinical doses achieve (Wiki). However, oral progesterone failed to provide adequate protection against estrogen-mediated endometrial cancer risk in a large observational study (Davey, 2018). Oral progesterone even at very high doses also is unable to produce full endometrial transformation—a normal effect of luteal-phase levels of progesterone—whereas vaginal and injectable progesterone are effective (de Ziegler et al., 2013). For this reason, oral progesterone, in contrast to parenteral progesterone, is considered to be inappropriate for use in assisted reproduction (de Ziegler et al., 2013). Oral progesterone additionally failed to suppress testosterone levels even at high doses (400 mg/day) in cisgender males (Trollan et al., 1993; Wiki). Conversely, progestins, rectal progesterone, and injectable progesterone can all produce robust testosterone suppression in cisgender males (Wiki; Aly, 2019). Similarly, oral progesterone has little or no apparent antigonadotropic effect in menopausal cisgender women, which is again in notable contrast to progestins (Holst, 1983; Holst et al., 1983; Ottosson, 1984; Maxson & Hargrove, 1985; Saarikoski, Yliskosk, & Penttilä, 1990).
Unlike other clinically used progestogens, the addition of oral progesterone to estrogen therapy in menopausal women has not been associated with increased risk of venous thromboembolism (VTE; blood clots) (Wiki). Nor has it been associated with increased breast cancer risk in the short-term (<5 years of therapy) (Wiki). However, with long-term use (≥5 years), the combination of estrogen plus oral progesterone is associated with significantly greater risk of breast cancer relative to estrogen alone similarly to other progestogens (Aly, 2020; Sam, 2020; Wiki; Table). This has been said to be consistent with a weak proliferative effect of oral progesterone on the breasts such that a longer duration of exposure is necessary for a quantifiable increase in breast cancer risk to manifest (Kuhl & Schneider, 2013; Davey, 2018). It is also consistent with preclinical research, which clearly suggests a carcinogenic role for progesterone and progesterone receptor activation in the breast (Kuhl & Schneider, 2013; Trabert et al., 2020). The preceding clinical findings on endometrial efficacy, testosterone and gonadotropin suppression, VTE risk, and breast cancer risk with oral progesterone are in contrast to those with almost all clinically used progestins (with the exception of the oral progesterone-like dydrogesterone). These previously perplexing discrepancies can be readily explained by the very low levels of progesterone that are now known to be achieved with oral progesterone.
Bioavailability, Half-Life, and Duration
Considering the much lower levels of progesterone observed with oral progesterone in studies using reliable analytic methods, the bioavailability of oral progesterone needs to be reassessed. In studies with immunoassays, the bioavailability of oral progesterone has been reported to be around 10% (Wiki). The true oral bioavailability of progesterone is unknown at this time as studies with reliable analytic methods have not been conducted. In any case, it can be assumed that it may be closer to around 1 or 2% based on the findings that immunoassays overestimate progesterone levels by 5- to 8-fold.
The elimination half-life of progesterone with oral progesterone has been determined in studies employing immunoassays to be 16 to 18 hours (Wiki). Based on the fact that the blood half-life of progesterone administered by intravenous injection is very short at a range of only 3 minutes to 1.5 hours (Wiki), the reported half-life of progesterone with oral progesterone is much longer than one would expect. Oral estradiol has a relatively long half-life of 13 to 20 hours due to formation with the first pass of a circulating reservoir of estrogen conjugates that are slowly converted back into estradiol (Kuhl, 2005; Wiki). In contrast to estradiol however, progesterone itself has no available hydroxyl groups for conjugation and an analogous circulating reservoir of progesterone conjugates that can be converted back into progesterone is not known to be the case (Kuhl, 2005).
Studies with more reliable analytic methods like LC–MS have found a half-life of progesterone with oral progesterone of 5 to 10 hours and a duration of highly elevated progesterone levels of only about 4 to 8 hours (Wiki; Graphs). These findings indicate that oral progesterone has a much shorter duration than previously thought as well. As such, if oral progesterone is used, it may be advisable to take it in divided doses multiple times per day to allow for more sustained progestogenic exposure.
Higher Oral Progesterone Doses and Neurosteroid Side Effects
Use of higher doses of oral progesterone than typical doses is likely to achieve dose-dependently higher progesterone levels (Table). However, based on how low progesterone levels are with oral progesterone using reliable analytic techniques, even very high doses would still be expected to achieve only low progesterone levels in most cases. Moreover, high doses of oral progesterone result in very high levels of its neurosteroid metabolites and have been found to produce substantial alcohol-like side effects (i.e., central depression and effects within that umbrella) (Wiki; Wiki). These limitations are likely to preclude higher doses of oral progesterone from being practical.
Figure 5: Levels of progesterone, allopregnanolone, and pregnanolone in premenopausal women following a single dose of oral progesterone or vaginal progesterone (as a suppository) (de Lignieres, Dennerstein, & Backstrom, 1995). Allopregnanolone and pregnanolone levels were determined by MS-based assays while progesterone levels were measured by immunoassay with chromatographic separation. Hence, the levels should be reliable.
A Note on Oral Progesterone’s Metabolites
Although progesterone levels with oral progesterone are very low, the metabolites of progesterone are formed in disproportionate amounts with the first pass (Sitruk-Ware et al., 1987; de Lignieres, Dennerstein, & Backstrom, 1995; de Lignieres, 1999; de Ziegler & Fanchin, 2000; Lobo, 2000; Kuhl, 2005). Moreover, while much less potent than progesterone, some of these metabolites have been found to have progestogenic activity similarly to progesterone (e.g., Besch et al., 1965; Junkermann, Runnebaum, & Lisboa, 1977; Lobo, 2000). This activity derives either from them having intrinsic progestogenic activity of their own or from being converted back into progesterone or other progestogenic metabolites (including in an intracrine fashion within tissues, for instance in the uterus). Examples of such metabolites include 20α-dihydroprogesterone, 20β-dihydroprogesterone, 5α-dihydroprogesterone, 3β-dihydroprogesterone, allopregnanolone, and 11-deoxycorticosterone. If the metabolites of oral progesterone contribute significantly to its progestogenic activity, then the progestogenic strength of oral progesterone would be greater than that implied by the progesterone levels that occur with it alone. However, this possibility is only theoretical and there is little literature discussing it. More research would be needed to determine if the metabolites of oral progesterone do indeed play a meaningful role in its progestogenic potency. In any case, oral progesterone is still a relatively weak progestogen based on clinical studies of its progestogenic effects.
Alternative Options to Oral Progesterone
Non-Oral Forms of Progesterone
Non-oral forms of progesterone, such as vaginal progesterone, rectal progesterone, sublingual progesterone, and progesterone by injection, have been found to achieve much higher progesterone levels than oral progesterone (Wiki). They can be used instead of oral progesterone to achieve higher and more adequate progesterone levels. Unfortunately however, while more effective than oral progesterone, non-oral progesterone routes have various limitations of their own.
Vaginal progesterone is of course not possible in transfeminine people who have not undergone vaginoplasty. And in those who have undergone vaginoplasty, the lining of the neovagina is either skin (penile inversion vaginoplasty) or intestine (sigmoid colon vaginoplasty) rather than the normal vaginal mucosa. As such, the absorptive characteristics of neovaginal administration are likely not the same as vaginal administration (Aly, 2018). It is notable that transdermal progesterone achieves very low progesterone levels similarly to oral progesterone and is not a good option for progesterone therapy (Wiki; Hermann et al., 2005; Graph). Progesterone levels with neovaginal administration of progesterone in those who have undergone penile inversion vaginoplasty are likely to be low similarly.
Rectal progesterone is an excellent route that achieves high progesterone levels comparable to the levels of progesterone that occur during the normal luteal phase (Wiki; Graphs). It has a somewhat short duration and twice daily use may be warranted for more sustained levels however. A more important problem is that the availability of pharmaceutical rectal progesterone suppositories throughout the world is limited and they are not marketed in most countries (Wiki). In any case, rectal progesterone suppositories may be available from compounding pharmacies in some countries. In addition, oral micronized progesterone capsules are available ubiquitously and have been administered vaginally instead of orally with success (Miles et al., 1994; Wang et al., 2019). Administration of oral micronized progesterone capsules rectally instead of orally likewise may be effective and may achieve much higher progesterone levels than oral administration (Aly, 2018). However, rectal administration of oral progesterone capsules has not been formally studied. Although rectal progesterone is effective, it is fairly inconvenient. This may be especially true with long-term therapy. In any case, of the available non-oral forms of progesterone, rectal progesterone is probably the best overall. A significant subset of transfeminine people on progestogens take progesterone rectally (Chang et al., 2024).
Figure 6: Progesterone levels with a single suppository containing 100 mg progesterone administered rectally or vaginally in premenopausal women (Chakmakjian & Zachariah, 1987).
Sublingual progesterone appears to achieve high and more physiological progesterone levels than oral progesterone but has a short duration of highly elevated progesterone levels similarly and necessitates administration several times per day (Wiki; Graph). Moreover, although sublingual progesterone may have been more widely available in the past (Wiki), it is available today only in a couple of Eastern European countries (Wiki). It might be available from compounding pharmacies in some countries however. While never formally studied, it may be possible to use oral micronized progesterone capsules sublingually instead of orally. However, this route is complicated by the fact that this form of progesterone is suspended in oil within gelatin capsules. Hence, sublingual administration of oral micronized progesterone is likely to be difficult and potentially unpleasant.
Progesterone by intramuscular or subcutaneous injection can easily achieve very high progesterone levels (Wiki; Graphs; Wiki; Graph). However, progesterone administered by this route has a relatively short duration when compared to other injectable sex-hormone formulations and requires injection once every 1 to 3 days. This is simply too frequent for most people, especially with long-term therapy. In addition, progesterone by subcutaneous injection, which is more convenient than progesterone by intramuscular injection, has limited availability and is marketed mostly only in Europe (Wiki). In contrast to other sex hormones like estradiol and testosterone, progesterone esters that are more fat-soluble than progesterone and extend its duration when used in injectable form are not possible since progesterone has no free hydroxyl groups available for esterification. Injectable aqueous suspensions of progesterone that had much longer durations than the oil solutions and aqueous solutions that are used by injection today were previously available (Wiki; Wiki; Aly, 2019). However, they were associated with painful injection site reactions and this led to their discontinuation. In any case, injectable aqueous suspensions of progesterone do actually seem to remain available for people in a couple of Eastern European countries today (Aly, 2019).
In conclusion, oral progesterone achieves very low progesterone levels at typical clinical doses and produces only weak progestogenic effects that seem to be far from physiologically adequate. Although use of higher doses of oral progesterone is likely to achieve higher progesterone levels, such doses are likely to be impractical because progesterone levels will still be low even at higher doses and the neurosteroid side effects of oral progesterone will be much more substantial and difficult to tolerate.
Due to its limitations, transfeminine people and clinicians treating them may wish to avoid oral progesterone if the intended goal is to produce therapeutic progestogenic effects. Instead, non-oral progesterone routes, such as rectal and injected progesterone, although with various limitations such as limited availability and inconvenience, can be used. Alternatively, progestins, particularly those with more favorable profiles, can be used instead of progesterone altogether.
Oral progesterone may perhaps be most appropriately conceptualized as a potent neurosteroid prodrug with weak progestogenic effects. Conversely, non-oral progesterone, as well as progestins, can be regarded as potent progestogens with either physiological or no neurosteroid effects, respectively.
Additional Content
Literature
The sources and excerpts collected here go in-depth on much of what has been described in this article on the topic of the measurement problems and low progesterone levels with oral progesterone.
Besch, P. K., Barry, R. D., Vorys, N., Stevens, V., & Ullery, J. C. (1965). A review of some aspects of the metabolism of progestational agents. Metabolism, 14(3), 432–443. [DOI:10.1016/0026-0495(65)90031-4]
Bijuva Estradiol/Progesterone Label. U.S. Food and Drug Administration. [URL] [PDF]
Chakmakjian, Z. H., & Zachariah, N. Y. (1987). Bioavailability of progesterone with different modes of administration. The Journal of Reproductive Medicine, 32(6), 443–448. [Google Scholar] [PubMed] [PDF]
Chang, J. J., Tran, N. K., Flentje, A., Lubensky, M. E., Obedin-Maliver, J., Lunn, M. R., & Ariel, D. (2024). 12330 Progestogen Experience And Perception Among Transfeminine Adults - A National Survey. Journal of the Endocrine Society, 8(Suppl 1), bvae163.1657. [DOI:10.1210/jendso/bvae163.1657]
Conklin, S. E., & Knezevic, C. E. (2020). Advancements in the gold standard: Measuring steroid sex hormones by mass spectrometry. Clinical Biochemistry, 82, 21–32. [DOI:10.1016/j.clinbiochem.2020.03.008]
Davey, D. A. (2018). Menopausal hormone therapy: a better and safer future. Climacteric, 21(5), 454–461. [DOI:10.1080/13697137.2018.1439915]
de Lignières, B., Dennerstein, L., & Backstrom, T. (1995). Influence of route of administration on progesterone metabolism. Maturitas, 21(3), 251–257. [DOI:10.1016/0378-5122(94)00882-8]
de Lignières, B. (1999). Oral micronized progesterone. Clinical Therapeutics, 21(1), 41–60. [DOI:10.1016/S0149-2918(00)88267-3]
de Ziegler, D., & Fanchin, R. (2000). Progesterone and progestins: applications in gynecology. Steroids, 65(10–11), 671–679. [DOI:10.1016/S0039-128X(00)00123-9]
de Ziegler, D., Streuli, I., Marszalek, A., Gayet, V., & Chapron, C. (2013). Preparing the Endometrium to Maximize Success: The Dynamics of Artificial Cycles. In Sauer, M. V. (Ed.). Principles of Oocyte and Embryo Donation, 2nd Edition (pp. 109–127). London: Springer. [DOI:10.1007/978-1-4471-2392-7_9]
Hermann, A. C., Nafziger, A. N., Victory, J., Kulawy, R., Rocci Jr, M. L., & Bertino Jr, J. S. (2005). Over‐the‐Counter Progesterone Cream Produces Significant Drug Exposure Compared to a Food and Drug Administration‐Approved Oral Progesterone Product. The Journal of Clinical Pharmacology, 45(6), 614–619. [DOI:10.1177/0091270005276621]
Holst, J. (1983). Percutaneous estrogen therapy: Endometrial response and metabolic effects. Acta Obstetricia et Gynecologica Scandinavica, 62(Suppl 115), 4–30. [DOI:10.3109/00016348309155363]
Holst, J., Cajander, S., Carlström, K., Damber, M. G., & von Schoultz, B. (1983). Percutaneous oestrogen therapy opposed by lynestrenol or natural progesterone-effects on circulating oestrogens, FSH, sex hormone binding globulin and pregnancy zone protein. Maturitas, 5(1), 1–8. [DOI:10.1016/0378-5122(83)90015-4]
Junkermann, H., Runnebaum, B., & Lisboa, B. P. (1977). New progesterone metabolites in human myometrium. Steroids, 30(1), 1–14. [DOI:10.1016/0039-128X(77)90131-3]
Kuhl, H. (2005). Pharmacology of Estrogens and Progestogens: Influence of Different Routes of Administration. Climacteric, 8(Suppl 1), 3–63. [DOI:10.1080/13697130500148875] [PDF]
Kuhl, H. (2011). Pharmacology of progestogens. Journal für Reproduktionsmedizin und Endokrinologie [Journal of Reproductive Medicine and Endocrinology], 8(1), 157–177. [URL]
Kuhl, H., & Schneider, H. P. G. (2013). Progesterone–promoter or inhibitor of breast cancer. Climacteric, 16(Suppl 1), 54–68. [DOI:10.3109/13697137.2013.768806]
Lobo, R. A. (2000). Progestogens. In Lobo, R. A., Kelsey, J., & Marcus, R. (Eds.). Menopause: Biology and Pathobiology (pp. 429–444). Burlington: Academic Press. [Google Books]
Lobo, R. A., Liu, J., Stanczyk, F. Z., Constantine, G. D., Pickar, J. H., Shadiack, A. M., Bernick, B., & Mirkin, S. (2019). Estradiol and progesterone bioavailability for moderate to severe vasomotor symptom treatment and endometrial protection with the continuous-combined regimen of TX-001HR (oral estradiol and progesterone capsules). Menopause (New York, NY), 26(7), 720–727.[DOI:10.1097/GME.0000000000001306]
Levine, H., & Watson, N. (2000). Comparison of the pharmacokinetics of Crinone 8% administered vaginally versus Prometrium administered orally in postmenopausal women. Fertility and Sterility, 73(3), 516–521. [DOI:10.1016/S0015-0282(99)00553-1]
Maxson, W. S., & Hargrove, J. T. (1985). Bioavailability of oral micronized progesterone. Fertility and Sterility, 44(5), 622–626. [DOI:10.1016/S0015-0282(16)48977-6]
Miles, R. A., Paulson, R. J., Lobo, R. A., Press, M. F., Dahmoush, L., & Sauer, M. V. (1994). Pharmacokinetics and endometrial tissue levels of progesterone after administration by intramuscular and vaginal routes: a comparative study. Fertility and Sterility, 62(3), 485–490. [DOI:10.1016/S0015-0282(16)56935-0]
Nahoul, K., Dehennin, L., & Scholler, R. (1987). Radioimmunoassay of plasma progesterone after oral administration of micronized progesterone. Journal of Steroid Biochemistry, 26(2), 241–249. [DOI:10.1016/0022-4731(87)90078-1]
Nahoul, K., Dehennin, L., Jondet, M., & Roger, M. (1993). Profiles of plasma estrogens, progesterone and their metabolites after oral or vaginal administration of estradiol or progesterone. Maturitas, 16(3), 185–202. [DOI:10.1016/0378-5122(93)90064-O]
Nahoul, K., & de Ziegler, D. (1994). “ Validity” of serum progesterone levels after oral progesterone. Fertility and Sterility, 61(4), 790–792. [DOI:10.1016/S0015-0282(16)56666-7]
Nakamoto, J. (2016). Endocrine Testing. In Jameson, J. L., & De Groot, L. J. (Eds.). Endocrinology: Adult and Pediatric, 7th Edition (pp. 2655–2688.e1). Philadelphia: Saunders/Elsevier. [DOI:10.1016/B978-0-323-18907-1.00154-2]
Ottosson, U. B. (1984). Oral progesterone and estrogen/progestogen therapy: effects of natural and synthetic hormones on subfractions of HDL cholesterol and liver proteins. Acta Obstetricia et Gynecologica Scandinavica, 63(Suppl 127), 1–37. [DOI:10.3109/00016348409157016]
Pickar, J. H., Bon, C., Amadio, J. M., Mirkin, S., & Bernick, B. (2015). Pharmacokinetics of the first combination 17β-estradiol/progesterone capsule in clinical development for menopausal hormone therapy. Menopause (New York, NY), 22(12), 1308–1316. [DOI:10.1097/GME.0000000000000467]
Prometrium FDA Review 1996. Application Number: NDA 19-781. Clinical Pharmacology and Biopharmaceutics Review(s) [Prometrium]. Center for Drug Evaluation and Research, U.S. Food and Drug Administration. [PDF]
Saarikoski, S., Yliskosk, M., & Penttilä, I. (1990). Sequential use of norethisterone and natural progesterone in pre-menopausal bleeding disorders. Maturitas, 12(2), 89–97. [DOI:10.1016/0378-5122(90)90086-L]
Sapin, R., Neamtu, D., Gasser, F., Ohl, J., Grunenberger, F., & Grucker, D. (2000). De la prudence lors de l’utilisation des dosages directs de progestérone. [Caution when using direct progesterone assays.] Immuno-analyse et Biologie Spécialisée, 3(15), 203–204. [DOI:10.1016/S0923-2532(00)80010-1] [Translation]
Simon, J. A., Robinson, D. E., Andrews, M. C., Hildebrand III, J. R., Rocci Jr, M. L., Blake, R. E., & Hodgen, G. D. (1993). The absorption of oral micronized progesterone: the effect of food, dose proportionality, and comparison with intramuscular progesterone. Fertility and Sterility, 60(1), 26–33. [DOI:10.1016/S0015-0282(16)56031-2]
Sitruk-Ware, R., Bricaire, C., De Lignieres, B., Yaneva, H., & Mauvais-Jarvis, P. (1987). Oral micronized progesterone: Bioavailability pharmacokinetics, pharmacological and therapeutic implications—A review. Contraception, 36(4), 373–402. [DOI:10.1016/0010-7824(87)90088-6]
Stricker, R., Eberhart, R., Chevailler, M. C., Quinn, F. A., Bischof, P., & Stricker, R. (2006). Establishment of detailed reference values for luteinizing hormone, follicle stimulating hormone, estradiol, and progesterone during different phases of the menstrual cycle on the Abbott ARCHITECT® analyzer. Clinical Chemistry and Laboratory Medicine (CCLM), 44(7), 883–887. [DOI:10.1515/CCLM.2006.160]
Tollan, A., Øian, P., Kjeldsen, S. E., Eide, I., & Maltau, J. M. (1993). Progesterone reduces sympathetic tone without changing blood pressure or fluid balance in men. Gynecologic and Obstetric Investigation, 36(4), 234–238. [DOI:10.1159/000292636]
Trabert, B., Sherman, M. E., Kannan, N., & Stanczyk, F. Z. (2020). Progesterone and breast cancer. Endocrine Reviews, 41(2), 320–344. [DOI:10.1210/endrev/bnz001]
Wang, H., Liu, M., Fu, Q., & Deng, C. (2019). Pharmacokinetics of hard micronized progesterone capsules via vaginal or oral route compared with soft micronized capsules in healthy postmenopausal women: a randomized open-label clinical study. Drug Design, Development and Therapy, 13, 2475–2482. [DOI:10.2147/dddt.s204624]
Woodward, G. M., & Rumsby, G. (2019). Steroid Profiling: Analytical Perspectives. In Rumsby, G., Woodward, G. M. (Eds.). Disorders of Steroidogenesis: Guide to Steroid Profiling and Biochemical Diagnosis (pp. 27–40). Cham: Springer. [DOI:10.1007/978-3-319-96364-8_3]
\ No newline at end of file
diff --git a/transfemscience.org/articles/progestogens-breast-dev/index.html b/transfemscience.org/articles/progestogens-breast-dev/index.html
index 53354097..6524fe45 100644
--- a/transfemscience.org/articles/progestogens-breast-dev/index.html
+++ b/transfemscience.org/articles/progestogens-breast-dev/index.html
@@ -1 +1 @@
-A Comprehensive Review of the Potential of Progestogens for Enhancing Breast Development in Transfeminine People - Transfeminine Science
A Comprehensive Review of the Potential of Progestogens for Enhancing Breast Development in Transfeminine People
By Aly | First published February 14, 2020 | Last modified June 28, 2024
Abstract / TL;DR
The major female sex hormones are estrogen and progesterone. Both of these hormones are known to be importantly involved in the development of the breasts at different stages of life. Speculation, use, and anecdotes of progestogens for enhancing breast development in transfeminine people date back to at least the 1960s. A limited number of clinical studies have assessed breast development with progestogens in transfeminine people, but current evidence on progestogens for improving breast development is of very low quality and is inconclusive. Studies of progestogens and breast development in cisgender girls and women are similarly limited. In any case, more studies evaluating progestogens and breast development are currently underway. The possible role of progestogens in enhancing breast development can also be informed by indirect and circumstantial evidence, including notably findings on progesterone and breast changes during normal puberty, the menstrual cycle, and pregnancy in humans and animals. Available evidence overall is not suggestive of an essential role for progesterone in breast growth during puberty, but progesterone does have a clear and key role in lobuloalveolar development of the breasts during pregnancy. However, breast changes in pregnancy revert following cessation of lactation and breastfeeding. Progesterone may additionally contribute to reversible breast enlargement during the luteal phase of the menstrual cycle. There are some findings to suggest that progestogens may have antiestrogenic effects in the breasts and may have a stunting influence on breast development if introduced too early following initiation of hormone therapy. However, more research is needed to assess this possibility. In any case, if progestogens are used, it may be advisable to delay their introduction until most or all estrogen-mediated breast development is complete. Options for progestogen therapy in transfeminine people include bioidentical progesterone and progestins. However, oral progesterone has major bioavailability problems and does not achieve satisfactory progesterone levels. Progestogens, including progesterone, have been variously linked to significant health risks, which is an important consideration in terms of their use in transfeminine people. Overall, based on current knowledge, progestogens do not seem to be promising for lastingly improving breast development in transfeminine people, but more research and data are still needed for clear conclusions.
Introduction
Breast development in terms of size and shape is often less than desired in transfeminine people, and there is a need for therapeutic approaches that improve breast growth in this population. There are two major types of female hormones, estrogens and progestogens. Estrogens are almost universally employed in transfeminine hormone therapy, while progestogens are used in a subset of transfeminine people. Progestogens that have been commonly employed in transfeminine people include bioidenticalprogesterone, the progestin (synthetic progestogen) medroxyprogesterone acetate (MPA), and the strongly progestogenic antiandrogen cyproterone acetate (CPA). Estrogens are the major mediators of feminization and breast development in females. However, progestogens also have physiological effects on the breasts, and in relation to this, may or may not provide benefits to breast development as well.
The topic of progestogens and breast development has been discussed for many years in the transgender community and is a controversial subject (Coleman et al., 2012). Use of progestogens to improve breast development in transfeminine people goes back at least as far as Harry Benjamin and Christian Hamburger in the 1960s (Benjamin, 1966; Benjamin, 1967; Hamburger & Benjamin, 1969; Wiki). Arguments have been made both for (e.g., Bevan, 2012; Bellwether, 2019; Bevan, 2019) and against (e.g., Curtis, 2009) a possible role of progestogens in terms of breast development. It is often claimed that progestogens can enhance breast development or are even required for full breast development in cisgender females and transfeminine people. With respect to the latter, it is sometimes said that progestogens are necessary for people to move from Tanner stage 4 to Tanner stage 5 pubertal breast development and that progestogens help to fill and round out the breasts (e.g., Vorherr, 1974a; Basson & Prior, 1998; Kaiser & Ho, 2015; Prior, 2011; Prior, 2019a; Prior, 2020). It has even been claimed by some that without progestogens, the breasts will remain conical and “pointy” like they are in the earlier Tanner stages. On the other extreme, certain critics have claimed that there are “no biologically significant progesterone receptor sites for biological males” and that progesterone is not produced during normal female puberty until after breast development has been fully completed (Barrett, 2009; Seal, 2017; Coxon & Seal, 2018; Price, McManus, & Barrett, 2019; Richards & Barrett, 2020). In turn, these particular authors have argued against the use of progestogens in transfeminine people in various of their publications (Google Scholar). In general, the use of progestogens in transfeminine people has longstandingly been controversial, with positions both for and against (Sam, 2020).
The purpose of this article is to review the available direct and circumstantial evidence on the topic of progestogens and breast development in order to help inform whether progestogen therapy may be able to enhance breast development in transfeminine people. Aside from an involvement in breast development, progestogens are not otherwise currently thought to be or known to be involved in physical feminization (e.g., Coleman et al., 2012; Gooren, 2016). In relation to this, the present article will limit its discussion to breast development with progestogens, and will not explore feminization in general.
Progestogen Therapy and Breast Development in Humans
Progestogens and Breast Development in Transfeminine People
Orentreich & Durr (1974) was one of the earliest studies on breast development in transfeminine people. They employed combinations of estrogens and progestogens as well as gonadectomy to produce feminization and breast development in a case series of 5 transfeminine people. The employed estrogens were estradiol valerate 30 mg/2 weeks by intramuscular injection and oral conjugated estrogens 1.25–5.0 mg/day and the used progestogens were “60 mg medroxyprogesterone caproate” every 2 weeks by intramuscular injection and oral medroxyprogesterone acetate 0–10 mg/day. Medroxyprogesterone caproate (MPC) has never been used pharmaceutically, so this was likely a typo and the actual progestogen employed was likely either MPA or hydroxyprogesterone caproate (OHPC). The authors reported that estrogen and progestogen therapy produced modest to significant breast development in the transfeminine people that was not strictly dose-related and included clinical photographs of the breasts. They concluded that the breast development was comparable to that of adult cisgender women. Orentreich and colleagues also discussed the topic of lobuloalveolar maturation of the breasts, which was known to be progestogen-dependent, but noted that they had not done histological assessment and that the degree of lobuloalveolar development of the breasts does not necessarily correlate with clinical breast size per findings in cisgender women. The findings of Orentreich and colleagues are limited by methodological problems like lack of objective measurements, lack of estrogen-only controls, and the small sample size of only 5 transfeminine people, and hence the study is of limited value in terms of assessing the involvement of progestogens in breast development.
Meyer et al. (1986) assessed the effects of progestogens added to estrogen therapy on breast development and other clinical parameters in transfeminine people. Of the 60 transfeminine people in the study, 15 (25%) received an oral progestogen, usually MPA at a dosage of 10 mg/day, for “at least for a short time”, and with only 8 (13.3%) receiving progestogen therapy for the full treatment period. In an earlier report of the study, it was noted that in 90% of observation periods the dose was 10 mg/day and for the remainder it was 20 mg/day (Meyer et al., 1981). A dosage of 10 mg/day MPA is roughly comparable to luteal-phase progesterone exposure in terms of progestogenic potency (Wiki). Breast development was measured in the study via breast hemicircumference (Diagram). Progestogen therapy was reported to not modify estrogen-induced changes, including laboratory measurements, hormone levels, and physical parameters like weight and breast growth. The lack of apparent changes in hormone levels is unexpected, as MPA in higher-quality studies has shown clear testosterone suppression (e.g., Jain, Kwan, & Forcier, 2019; Wiki). Meyer and colleagues concluded that adding progestogens to estrogen does not seem to enhance breast development in transfeminine people. However, they noted that the number of individuals who received progestogens was small and further studies were needed.
Prior et al. (1986) and Prior, Vigna, & Watson (1989) studied estrogen, high-dose spironolactone (100–600 mg/day), and MPA (10–20 mg/day cylically or continuously) in transfeminine people who were either pre-hormone therapy or had previously been on higher doses of estrogens (and/or progestogens) without spironolactone prior to the study. The researchers reported that following 12 months of treatment with the study’s hormone therapy regimen, there was increased breast size and increased nipple development. Most individuals reached an A cup size, or approximately 8 to 14 cm in diameter of breast tissue, by the end of the study. Breast development was measured in part with photographic documentation. Although breast development reportedly improved, the researchers themselves noted that it was difficult to determine whether the enhanced breast development could be attributed to spironolactone or to MPA. Moreover, testosterone suppression was inadequate before the study and improved with the study’s hormone therapy regimen, which may have helped to improve breast development regardless of any potential direct progestogenic action of MPA on the breasts. Finally, it is possible that breast development with estrogen may not yet have been complete, and that the improved breast development may have simply been continued progression due to estrogen alone. In other publications, Jerilynn Prior, the lead study author, has claimed that progesterone enhances breast development, and has cited the preceding studies by her in support of this claim (Prior, 2011; Prior, 2019a; Prior, 2019b; Prior, 2020). However, her claim is not well-supported due to the study limitations discussed.
Dittrich et al. (2005) reported that the combination of oral estradiol valerate and a gonadotropin-releasing hormone (GnRH) agonist for 2 years in transfeminine people resulted in self-reported breast cup sizes of C cup or greater in 5%, B cup in 30%, A cup in 35%, and less than A cup in 30%. They noted however that 70% of the individuals were unsatisfied with their breast development and wished to undergo breast augmentation surgery. The researchers claimed that the regimen had similar effectiveness in terms of feminization, including increases in breast size, compared to prior reported treatment regimens of ethinylestradiol and CPA. No other details or specifics were given. The claim about similar breast development to regimens containing CPA is relevant as CPA is a very strong progestogen at the doses used historically in transfeminine people (Aly, 2019). It should be cautioned however that this study did not actually employ or study progestogen therapy itself. In addition, self-reported breast cup size is a subjective and low-quality means of measuring breast development and size. As such, the findings of this study are of questionable value in terms of understanding progestogens and breast development.
Estrogen is primarily involved in ductal development of the breasts, whereas progesterone is mainly involved in lobuloalveolar development. Kanhai et al. (2000) compared internal histological breast tissue changes with estrogen and CPA 100 mg/day (i.e. very-high-dose progestogen) therapy in 14 transfeminine people versus nonsteroidal antiandrogen monotherapy with flutamide or bicalutamide in 2 cisgender men with prostate cancer. Both types of treatments block androgens, increase estrogen levels, and are known to induce breast development or gynecomastia at similarly high rates. However, nonsteroidal antiandrogen monotherapy differs from combined estrogen and progestogen therapy in that it lacks any progestogenic effects. In the transfeminine people, full lobuloalveolar formation was apparent in the biopsied breast tissue, whereas in the men with prostate cancer, only “moderate” and incomplete lobuloalveolar maturation was found. It was also noted that lobuloalveolar formation tended to regress upon discontinuation of CPA following gonadectomy in transfeminine people. The researchers concluded that progestogenic exposure is needed for the breasts to fully develop on a histological level and for the breast tissue of transfeminine people to completely mimic the histology of the mature female breast. While the findings of this study are interesting, they only concern tissue characteristics and do not actually provide any information about breast development in terms of physical form or appearance. With regard to this, tissue-level differences may or may not translate to relevant differences in for instance breast size or shape. As such, the study is of limited value in understanding whether progestogens improve breast development in transfeminine people in the ways that are actually valued.
Seal and colleagues conducted a retrospective chart review assessing clinical predictors for surgical breast augmentation in transfeminine people (Seal et al., 2012). In the transfeminine people who underwent breast augmentation, significantly more of them were taking spironolactone than were those who did not undergo breast augmentation. Conversely, the differential rates of use of specific antiandrogens were not significantly discordant between those who did and did not undergo breast augmentation in the case of the other prescribed antiandrogens, including cyproterone acetate, the 5α-reductase inhibitors, and GnRH analogues. However, this study had many methodological limitations, including the use of almost three dozen t-tests with no adjustment for multiple comparisons (and hence risk of false positives and concerns about p-hacking), small sample sizes for individual antiandrogens, use of undergoing breast augmentation as a surrogate for breast development with no actual physical measurement of the breasts or breast sizes, and a correlational design with lack of control for potential confounding variables. As such, the study does not show that different antiandrogens result in differences in breast development, and its findings must be considered with due caution.
Jain, Kwan, & Forcier (2019) studied sublingual estradiol and spironolactone with and without MPA in 92 transfeminine people. MPA was given at a dose of 5 to 10 mg/day sublingually or at a dose of 150 mg once every 3 months by intramuscular injection. Of 39 transfeminine people who received MPA, 26 (67%) self-reported improved breast development. No further details were provided, but measurement of breast development was presumably subjective and anecdotal. Igo & Visram (2021) studied addition of progesterone to hormone therapy in transfeminine people. Progesterone was provided as 100 mg micronized progesterone (probably oral) and was prescribed when progesterone was specifically requested by the patient or when the patient expressed dissatisfaction with feminization and/or breast development. Of 190 individuals, 51 (26.8%) received progesterone therapy. Treatment with progesterone on average began after 12.7 months of estradiol therapy, and the mean total follow-up time was 14.3 months of hormone therapy. Of those who received progesterone, only 6 (11.8%) reported benefit to breast development. No further details were provided, but as with other studies, breast development was likely quantified anecdotally via self-report. As breast development does not appear to have been objectively measured or compared to a control group in either Jain, Kwan, & Forcier (2019) or Igo & Visram (2021), the findings of these studies are limitedly informative.
Nolan and colleagues assessed the short-term effects of low-dose oral micronized progesterone on breast development in transfeminine people on stable hormone therapy in a prospective controlled study (Nolan et al., 2022a; Nolan et al., 2022b). Progesterone was given at a dose of 100 mg/day for 3 months to 23 transfeminine people and findings were compared to those of a control group of 19 transfeminine people. Breast development was measured using self-reported Tanner stage, with participants provided photographs of different Tanner stages to self-select from. At the end of the 3 months, Tanner stage was not significantly different between groups (mean 3.5, 95% CI 3.2–3.7 for progesterone vs. mean 3.6, 95% CI 3.3–3.9 for controls; p = 0.42). A limitation of this study is that oral progesterone has very low bioavailability and 100 mg/day oral progesterone achieves very low progesterone levels that are well below normal luteal-phase progesterone levels (Aly, 2018a; Wiki). As such, progestogenic exposure in this study, and notably also in Igo & Visram (2021) and other studies, is likely to have been inadequate. Besides the issue of progestogenic strength, the very short duration of the study (3 months) and the reliance on self-reported subjective Tanner stages (as opposed to more objective physical breast measurements) are also major limitations. In any case, this study is of higher quality than previous studies, and is notably likely to continue and report further follow-up at later points in the future.
Bahr et al. (2024) conducted a retrospective chart review at their clinic and compared 29 transfeminine people who had received progestogens versus 59 transfeminine people who had not. The form of progestogen used was oral or rectal progesterone in 93% of cases and MPA by intramuscular injection in the remaining 7% of cases. Of those who took progesterone, 25 (93%) used it orally and 2 (7%) used oral progesterone capsules rectally. Progestogen doses were not reported, except that 100 mg progesterone capsules were employed. Most of those in the progestogen-treated group (59%) had started it 1 to 6 months following initiation of standard hormone therapy. The researchers found that progestogen-treated group had significantly better self-reported breast development satisfaction (rated as satisfied, neutral, or unsatisfied) compared to the group that did not receive progestogens at 6 months (satisfied: 53.8% vs. 19.6%; p = 0.004) and 9 months (satisfied: 71.4% vs. 20.8%; p = 0.003) of hormone therapy. Limitations of this study include the lack of objective measurement of breast development, the restrospective nature of the study, and the lack of randomization of treatment, among others.
Aside from the above studies, a variety of other studies have also reported breast development with estrogen and CPA in transfeminine people. These studies have often employed objective physical measurements of breast development (e.g., breast volume, breast–chest difference, breast cup size, breast hemicircumference). However, they have lacked comparison groups, thereby precluding comparison of progestogenic versus non-progestogenic hormone therapy. In addition, CPA is unusual among progestogens in that it is employed at very high doses in transfeminine people (Aly, 2019), which may result in different and potentially stunted outcomes in terms of breast development than more physiological progestogenic exposure. As such, most studies of breast development with estrogen and CPA in transfeminine people have not been discussed in the present section and are instead discussed elsewhere in this article (see the section below). In any case, to briefly summarize the findings, breast development in transfeminine people with estrogen and CPA has generally been poor in these studies. The outcomes have included incomplete maturation in terms of Tanner staging (stage 2–4), small cup sizes, small breast volumes, and breasts much smaller in size than those in cisgender women.
The findings from the preceding studies in transfeminine people are of very low-quality due to methodological limitations, including lack of control groups, lack of randomization, reliance on poor measures of breast development (e.g., subjective and self-report) rather than objective physical measurements (Wiki), short treatment durations, and small sample sizes, among others. This may explain the conflicting results of the studies. More research is still needed to assess the influence of progestogens on breast development in transfeminine people. There is specifically a need for randomized controlled trials (RCTs) of feminizing hormone therapy with versus without progestogen therapy that employ objective measures of breast development, have adequate sample sizes, and have sufficient follow-up durations. Additional variables like progestogen type, route, dose, and timing of introduction would also be of value to explore. A 2014 review on hormone therapy in transfeminine people summarizes the state of research on progestogens and breast development in transfeminine people, with their conclusions still holding true today (Wierckx, Gooren, & T’Sjoen, 2014):
Our knowledge concerning the natural history and effects of different cross-sex hormone therapies on breast development in trans women is extremely sparse and based on low quality of evidence. Current evidence does not provide evidence that progestogens enhance breast development in trans women. Neither do they prove the absence of such an effect. This prevents us from drawing any firm conclusion at this moment and demonstrates the need for further research to clarify these important clinical questions.
Several studies of progesterone and other progestogens in transfeminine people are currently underway. These studies include (1) an RCT of oral progesterone added to hormone therapy by Sandeep Dhindsa and colleagues in St. Louis, Missouri in the United States (ClinicalTrials.gov; MediFind; ICH GCP); (2) a prospectiveobservational study and/or RCT of addition of oral progesterone to hormone therapy by Ada Cheung and colleagues in Melbourne, Australia (University of Melbourne; University of Melbourne); (3) an RCT of estradiol plus spironolactone versus estradiol plus CPA also by Ada Cheung and colleagues (ANZCTR; WHO ICTRP; Trans Health Research [Flyer] [Poster]; University of Melbourne) (update: see below); and (4) a large RCT of oral progesterone at different doses added to hormone therapy by Martin den Heijer and colleagues at the Vrije Universiteit University Medical Center (VUMC) in Amsterdam, the Netherlands (Dijkman et al., 2023a; General Info/Links; Info Sheet Dutch; Info Sheet English Translated). Unfortunately however, all of the studies using progesterone employ oral progesterone, which has major bioavailability and potency problems (Aly, 2018a; Wiki). In any case, it was said that the VUMC researchers may follow their trial up with studies of other progesterone routes (General Info/Links). The preceding studies may provide more insight on the question of whether progestogen therapy is of therapeutic benefit to breast development in transfeminine people.
Progestogens and Breast Development in Cisgender Females
To date, there appear to be no useful studies on breast development with progesterone or other progestogens in cisgender females. There seem to mostly only be a few brief and conflicting anecdotal clinical statements in this area that are scattered throughout the literature. These include the following literature excerpts, which are specifically in the context of progestogens as part of puberty induction in cisgender girls and women with delayed or absent puberty due to hypogonadism:
I […] performed studies on three women lacking mammary development and exhibiting signs of marked hypogonadism. […] Corpus luteum extract, 5 international units daily for a period of thirty days, when given alone produced no detectable change in the breasts. This is in accord with the experimental observations on animals of Turner,2 Corner 3 and others. When, however, patients were given alternate daily injections of 1 international unit of progesterone and from 20,000 to 50,000 international units of estrone or of estradiol benzoate, breast growth was more rapid than that produced by the estrogenic hormones alone. The simultaneous use of the corpus luteum and estrogenic therapy definitely produced a much firmer breast growth, which was distinctly lobular to palpation, whereas the growth produced by the estrogenic hormones alone was smooth and the borders of the glandular tissue were difficult to define. Rapid regression in the size of the breasts followed the omission of the hormone injections, but the regression was less rapid when the combined therapy had been used. [MacBryde (1939)]
There are authorities who consider that breast growth is better if a progestogen is combined with oestrogen for the latter part of the cycle of treatment (Capraro, 1971). Shearman (1971) employs sequential therapy in his cases. Huffman (1971) however, does not believe that there is any improvement with the addition of progestogens. [Dewhurst (1971a)]
The effects of progesterone on the human breast remain obscure. Although widely stated to cause glandular development, the evidence for this is slender (Benson et al 1959). [Shearman (1972a)]
Many people use oestrogens alone, but the addition of a progestin for 6 or 10 days each month gives much better cycle control and appears to cause better breast development. [Shearman (1972b)]
Some authorities consider that breast growth is better if a progestogen is given for the latter part of each course of treatment. [Capraro & Dewhurst (1975)]
It has been suggested that progestins be added during the last week of each cycle of estrogen therapy in order to develop more rounded breasts rather than the conical breasts many of these patients develop, but we have been unable to detect any difference in breast contour with or without progestins. [Davajan & Kletzky (1979)]
I have been satisfied that the addition of a progestogen was necessary to get a good breast response to hormone treatment although the progestogen, as I have said, is required after the first year if the uterus is present. [Dewhurst (1982)]
In addition to the preceding instances, Werner (1935) and Geschickter (1945) assessed the effects of progesterone on the breasts in cisgender women. Werner (1935) attempted to induce lactation in 8 surgically gonadectomized cisgender women with combinations of estrogen, progesterone, and prolactin, all in the form of crude extracts by injection. In two women who were given progesterone, he claimed that a marked increase in the size of the breasts beyond that with estrogen alone was observed. Additionally, he claimed that the breasts were more firm, the glandular tissue “more tortuous and nodular”, and the nipples more prominent. He was not successful in inducing lactation in the women in this study. The doses of hormones used were unclear as they were in the form of extracts, and were likely supraphysiological, potentially pregnancy-like due to the nature of the experiment. Werner’s study was also briefly discussed by Nelson (1936), among other citations. Geschickter (1945) observed lobuloalveolar growth on histological examination with administration of progesterone for 6 weeks to 2 months in one woman but not in another woman. However, the exterior physical changes of the breasts were not assessed or reported by this author and hence his findings are limitedly informative.
Surprisingly, there have been few analogous studies of the effects of progestogens on the breasts in cisgender girls and women following the preceding reports and anecdotes. Although there are very little data on progestogens and breast growth in cisgender females, clinical studies are finally starting to look more closely at the specifics of hormonal medications, including progestogens, in terms of breast development in girls undergoing puberty induction (e.g., Rodari et al., 2023). As such, future studies may provide more insight on the subject of progestogens and breast development in cisgender females.
Progesterone and its Physiological Role in Breast Development in Humans
Progesterone and Breast Development in Puberty
The role of progesterone in breast development and its possible usefulness for helping with breast development in transfeminine hormone therapy can be informed by the normal biological circumstances of puberty in cisgender females. Puberty in cisgender girls usually starts around age 11 (range 8–13 years) and completes around age 15 years (range 12–19 years), taking on average 3 to 4 years (but with a range of about 1.5–6 years in most cases) (Schauffler, 1942; Marshall & Tanner, 1969; Marshall, 1978; Begley, Firth, & Hoult, 1980; Drife, 1986). Progesterone essentially does not appear during puberty until ovulatorymenstrual cycles begin. Menarche, the onset of menstruation and hence of menstrual cycling, occurs on average at Tanner breast stage 4 or about 13 years of age, although it occurs at Tanner breast stage 3 or Tanner breast stage 5 in significant subsets of girls (26% for Tanner stage 3, 62% for Tanner stage 4, and 10% for Tanner stage 5) (Marshall & Tanner, 1969; Marshall, 1978; Drife, 1986; Hillard, 2007). Hence, the appearance of progesterone in normal female puberty is a relatively late event (Scott et al., 1950; Marshall, 1978; Begley, Firth, & Hoult, 1980; Drife, 1986), and most breast development appears to be complete by menarche and thus by the time that progesterone is first produced (Huffman, Dewhurst, & Capraro, 1981; Drife, 1982). Moreover, a small but significant subset of girls reaches Tanner breast stage 5 and hence fully developed breasts before menarche (Edmonds, 1989), which suggests that progesterone may not be essential for complete pubertal breast development.
Only a handful of studies and sources have reported progesterone levels during puberty across Tanner stages or by age in cisgender girls (e.g., Sizonenko, 1978 [Graph]; Kühnel, 2000; Lee, 2001 [Table]; Aly, 2020a). They corroborate the above findings with regard to limited progesterone exposure during puberty. The “A Girl’s First Period Study” is an ambitious research project announced in 2022 that aims to better characterize reproductive hormone levels in pubertal and adolescent girls and may shed more light on the physiological role of progesterone during puberty (Lucien et al., 2022). The researchers have specifically highlighted the possible role of progesterone in breast development as part of their interests:
Does exposure to low levels of [progesterone (P4)], as occurs before menarche, during anovulatory cycles with some degree of follicle luteinization, and during early, immature ovulatory cycles play an important role in normal breast development during puberty? This question has important clinical implications as hormone replacement during puberty does not typically include low-dose P4; rather, it is conducted using a staggered approach of estrogen-only therapy followed by the addition of full adult doses of exogenous P4 only after 2 years or when breakthrough bleeding occurs.27 This is done to avoid development of tubular breasts, although there are limited data linking early P4 exposure to suboptimal breast development.28
Taken together, production of progesterone is a late event in normal female puberty, and even once it does begin, exposure to progesterone is low and sporadic until well after puberty has completed. Moreover, a subset of girls complete breast development before progesterone production starts. These facts call into some question the role of progesterone in breast development in female puberty, as most breast development appears to be complete prior to the appearance of progesterone. However, more research is still needed on the role of progesterone in breast development during normal puberty.
On the basis of normal female puberty, it seems it may be advisable that if progestogens are introduced in an attempt to enhance breast development in transfeminine people, their introduction be delayed until after 2 or 3 years of hormone therapy, so as to mimic the normal progestogenic exposure of puberty.
Progesterone and Breast Development in Pregnancy
During pregnancy, under the influence of ovarian hyperstimulation and placental formation, there are profound changes in hormonal profiles, including of hormones like estrogen, progesterone, and prolactin, among many others (Table 1). Comparing hormone levels during the menstrual cycle to those during the third trimester of pregnancy, estradiol levels increase on the order of 100-fold, progesterone levels increase on the order of 10- to 20-fold, and prolactin levels increase by around 10-fold (Table 1). Levels of numerous other hormones also change considerably during pregnancy, for instance other estrogens besides estradiol, androgens, gonadotropins (e.g., human choronic gonadotropin or hCG), human placental lactogen (hPL), relaxin, adrenocorticotropic hormone (ACTH), cortisol, aldosterone, growth hormone (GH), and insulin-like growth factor 1 (IGF-1), among others (Goodman, 2009 [Figure]; Mesiano, 2019). These hormones are variously produced by the ovaries, the placenta, and the pituitary gland, among other glands. In response to the myriad hormonal changes during pregnancy, there are dramatic changes to the breasts, which prepare the mother for postpartumlactation and breastfeeding.
Table 1: Changes in hormone levels (estradiol, progesterone, and prolactin) during normal pregnancy:
There are large and dramatic changes in levels of numerous hormones during pregnancy, and the exact hormones responsible for the breast changes during pregnancy are not known (Hytten & Leitch, 1971a; Hytten, 1976). However, it is considered likely, on the basis of animal studies, that a variety of hormones, including estrogen, progesterone, prolactin, placental lactogen, glucocorticoids, and growth hormone, are all importantly involved in different aspects of the maturation (Hytten & Leitch, 1971a; Hytten, 1976; Cox et al., 1999). Moreover, in a quantitative clinical study of breast changes during pregnancy, increases in breast volume and areola size were positively correlated with levels of hPL, while increases in nipple size were positively correlated with levels of prolactin (Cox et al., 1999). Progesterone and prolactin have specifically been implicated in the lobuloalveolar development of the breasts during pregnancy (Bässler, 1970; Lee & Ormandy, 2012; Obr & Edwards, 2012). Both hormones appear to be independently essential in normal lobuloalveolar growth per animal studies (Obr & Edwards, 2012; McNally & Stein, 2017; Hannan et al., 2023). Prolactin likewise appears to be essential in humans, based on case reports of lactation failure in women with isolated prolactin deficiency (Buhimschi, 2004). Conversely, hPL may not be essential for lactation based on case reports of normal lactation in women with very low levels of hPL during pregnancy (Gaede, Trolle, & Pedersen, 1978; Hannan et al., 2023).
On the basis of the preceding, in spite of rather extreme hormonal stimulation, the breast changes of pregnancy, although quite dramatic, are essentially temporary and fully reversible, remaining only as long as continuous hormonal exposure is maintained. This hormonal stimulation includes exposure to extremely high levels of progesterone. It would seem, based on pregnancy, that once pubertal breast development is completed, the breasts are rather unamenable to permanent further growth, whether that involves exposure to progestogens or to a variety of other hormones known to act on the breasts.
Breast Composition and Lobuloalveolar Tissue Proportion
The breasts are made up of two main types of tissue: (1) epithelial tissue, the actual functional internal mammary glandular tissue, including ducts and alveoli or lobules; and (2) stromal tissue, a mixture of connective tissue and adipose (fat) tissue. Lobuloalveolar development refers to growth and maturation of the alveoli and lobules, and hence is a form of epithelial or glandular development. Progestogens are involved primarily in lobuloalveolar development of the breasts, which is the type of breast development that is necessary for lactation and breastfeeding and that occurs mainly during pregnancy.
During pregnancy and lactation in humans, the breasts undergo dramatic changes, and epithelial tissue comes to make up a much greater proportion of the breasts (Ramsay et al., 2005; Bland, Copeland, & Klimberg, 2018). In fact, sources state that glandular tissue comprises a majority of the breast during pregnancy and lactation, with one study of lactating women finding that the breasts were composed 63% (range 46–83%) of glandular tissue (Ramsay et al., 2005). This is not merely due to lobuloalveolar development and glandular growth, but is also due to a marked reversible reduction in mammary adipose tissue (Wang & Scherer, 2019; Alex, Bhandary, & McGuire, 2020). In any case, under more normal physiological circumstances and progesterone exposure, the contribution of lobuloalveolar tissue to the size of the breasts would appear to be quite small. In relation to this, outside of pregnancy levels of progesterone, the significance of progestogen-mediated breast lobuloalveolar growth in terms of breast size is unclear but seemingly questionable (Orentreich & Durr, 1974; Wierkcx, Gooren, & T’Sjoen, 2014).
Breast Development in Cisgender Women with Complete Androgen Insensitivity Syndrome and Consequent Absence of Progesterone
It has been claimed that progesterone helps to move transfeminine people and cisgender females from Tanner stage 4 to 5 breast development and that it helps to round out the breasts (e.g., Vorherr, 1974a; Prior, 2011; Prior, 2019a; Prior, 2020). It has also sometimes been claimed in the online transgender community that cisgender women with complete androgen insensitivity syndrome (CAIS), an experiment of nature of women who lack progesterone, are stuck at Tanner stage 4 breast growth and have “cone-shaped” breasts due to their absence of progesterone. In actuality however, there is no good evidence at this time that progesterone is required for normal pubertal breast development, that progesterone is needed to reach Tanner stage 5, or that it helps to round out the breasts. Such claims are contradicted by extensive available literature and evidence, including notably the literature on CAIS women themselves.
Women with CAIS are individuals who have a 46,XY karyotype (i.e., are genetically “male”), testes, and who would otherwise have physically developed as males, but did not because they have a mutation in the gene encoding the androgen receptor that makes them completely insensitive to the effects of androgens. There are also incomplete forms of the syndrome, like partial androgen insensitivity syndrome (PAIS) and mild androgen insensitivity syndrome (MAIS). CAIS women have a male-typical hormonal profile, generated by their testes, including high male-range levels of testosterone, low female-range estradiol levels, and negligible progesterone levels (Wiki; Table). Instead of developing physically as males however, CAIS women are perfectly phenotypically female, with a normal female body, vagina, and breasts (Wiki; Photo). Their testosterone has been unable to masculinize them, while their estradiol, unopposed by androgens, is able to fully feminize them. The internal reproductive system in CAIS women is essentially that of a highly underdeveloped male, with testes instead of ovaries, no uterus, fallopian tubes, or cervix, and no prostate gland or seminal vesicles. The testes are internally located, either intra-abdominally, inguinally, or labially. They are usually surgically removed by early adulthood, as they otherwise have a high risk of developing testicular cancer because of their location. The vagina in CAIS women is often short and is blind-ending, which is related to their lack of a uterus. In terms of behavior, gender, and sexuality, CAIS women are described as feminine.
Despite claims that CAIS women have generous breast sizes however, in actuality, some CAIS women have large breasts, while some have small breasts. One study found a wide range of breast size measurements of 16×14 cm to 41×31 cm, which equates to an almost 6-fold variation in breast size as quantified by area (Wisniewski et al., 2000). Moreover, the breasts of CAIS women have never been directly compared to those of normal women. Hence, there are no clear data at this time that the breasts of CAIS women are actually larger than average for women. The variation in breast growth in CAIS women parallels the same large variation in breast size between individuals that is seen in cisgender women in general. Here is a collection of photos of CAIS women and their breast development from published case reports and reviews throughout the literature. As can be seen from these photos, breast development in CAIS women is normal and often excellent, although subject to considerable variation between individuals in terms of breast size and shape as in women generally.
If CAIS women truly do have enhanced breast development and breast sizes compared to normal women, it may be that their androgen insensitivity, and hence lack of inhibition of estrogen-mediated breast development by androgens, is responsible for this (Wilson, 1968; Sobrinho, Kase, & Grunt, 1971; Andler & Zachmann, 1979; Zachmann et al., 1986; Patterson, McPhaul, & Hughes, 1994; Barbieri, 2019). Another theoretical possibility is that the high testosterone levels may be aromatized into greater amounts of estradiol locally within the breasts and other tissues in CAIS women and that this may somehow allow for enhanced breast development (Ladjouze & Donaldson, 2019). Interestingly, it has been claimed anecdotally by some researchers that breast development is much better in CAIS women who are allowed to naturally undergo puberty with their own endogenous hormones compared to CAIS women who undergo gonadectomy before puberty and have pubertal maturation induced with exogenous estrogen therapy (Dewhurst, 1972; Glenn, 1976; Dewhurst, 1981; Reindollar & McDonough, 1985; Shearman, 1985; Laufer, Goldstein, & Hendren, 2005). This is to the extent that some CAIS women who have had induced puberty have needed to undergo surgical breast augmentation due to poorly developed breasts (Dewhurst, 1981; Shearman, 1985). In relation to the preceding, it is usually standard clinical practice to delay gonadectomy in CAIS women until puberty has fully completed (Laufer, Goldstein, & Hendren, 2005). However, one clinical study reported good breast development rated as Tanner stage 5 in all cases in CAIS women who experienced either spontaneous or therapeutic puberty (Cheikhelard et al., 2008). It may be important to mimic normal pubertal estrogen exposure with puberty induction in CAIS females by employing low physiological estradiol levels that are slowly and gradually increased over a few years (Dewhurst, 1981; Cheikhelard et al., 2008; Bertelloni et al., 2011).
Baron evaluated a total of 41 people with androgen insensitivity syndrome (AIS) and found that 97% of CAIS women had normal breast development while 63% of individuals with “incomplete AIS” (likely PAIS) had normal breast development (Baron, 1993; Baron, 1994a; Baron, 1994b). In another earlier published study of 50 CAIS females, by Sir Christopher John Dewhurst, 76% were rated as having full breast development, 14% as having moderate breast development, 10% as having “mild” breast development, and 0% as having absent breast development (Dewhurst, 1971b). Hence, based on findings in large samples of CAIS females, most to almost all have normal or full breast development. That a minority of CAIS females have had less breast growth may be due to factors like low and inadequate estradiol levels in some individuals, young age at time of assessment by which point breast development has not fully completed, and/or a small subset of women in general having underdeveloped or small breasts.
CAIS women have never been described in the literature as having “cone-shaped”, “pointy”, or otherwise abnormal breasts. The only exception is that they are often said to have nipples and areolas that are described as “juvenile”, “infantile”, “small”, “pale”, and “non-pigmented” (e.g., Photo) (e.g., Morris, 1953; Morris & Mahesh, 1963; Simmer, Pion, & Dignam, 1965; Dewhurst, 1967; Khoo & Mackay, 1972; Perez-Palacios & Jaffe, 1972; Dewhurst & Spence, 1977). This has been said to be the case regardless of breast size or maturation (Khoo & Mackay, 1972). A possible reason for this phenomenon is that estradiol levels in CAIS women are relatively low, only about 35 pg/mL (130 pmol/L) on average (Wiki; Table). This is relevant as estrogens are known to concentration-dependently produce nipple and areolar pigmentation and enlargement (e.g., Davis et al., 1945 [Figure]; Kennedy & Nathanson, 1953). In contrast to estrogens, progestogens have not been implicated in nipple or areolar pigmentation. Hence, it seems that higher estrogen levels may be necessary for full adult-like nipple and areolar maturation.
Despite their often large breasts, CAIS women are said to have relatively little breast glandular tissue, as opposed to fat and connective tissue, and to have minimal breast lobuloalveolar development (Morris, 1953; Morris & Mahesh, 1963; Simmer, Pion, & Dignam, 1965; McMillan, 1966; Perez-Palacios & Jaffe, 1972; Dewhurst & Spence, 1977; Shapiro, 1982). This is in accordance with the lack of progesterone in CAIS women, since progesterone is important in mediating lobuloalveolar growth. The retained breast sizes of CAIS women despite reduced glandular and lobuloalveolar structures is consistent with the fact that the breasts are composed mostly of stromal adipose and connective tissue. Hence, as touched on previously in this article, greater glandular or lobuloalveolar formation in the breasts may not necessarily translate to greater breast size, which seems readily apparent in CAIS women.
The normal and excellent breast development of CAIS women is notable because these individuals, owing to their testes and hence absence of significant gonadal progesterone production, have very low and negligible levels of progesterone (Wiki; Table; Barbieri, 2019). CAIS womens’ normal breast development, often large breasts, and ability to reach complete breast maturation, as measured by the Tanner scale, are collectively suggestive that progesterone is not required for normal or complete pubertal breast development (Barbieri, 2019). In any case, it must be noted and cautioned again that the breasts of CAIS women have never been directly compared to those in normal women. In addition, quantitative studies of the breasts of CAIS women are very scarce, and much of our knowledge in this area is based on anecdotal clinical experience and subjective breast evaluation. This is in large part due to the rarity of CAIS women and the difficulty in obtaining decent samples of them for study. Furthermore, CAIS women also have other differences from regular women besides their lack of progesterone, for instance their relatively low circulating estradiol levels, high testosterone levels (which can be aromatized into estradiol within tissues like the breasts), androgen insensitivity, and XY karyotype, among others. Hence, the insights into breast development provided by CAIS women come with a variety of caveats.
Interestingly, in spite of their well-developed breasts, breast cancer has never been reported in CAIS women, and would appear to be very rare in these individuals (Aly, 2020b; Aly, 2020c). This may be related to factors like the lack of progesterone and lobuloalveolar maturation in CAIS women and/or their absence of a second X chromosome (Aly, 2020b; Aly, 2020c). CAIS women suggest that breast cancer is not an inherent eventual consequence of excellent breast development.
Menstrual Cycles and Temporary Cyclic Breast Enlargement
The enlargement of the breasts during the luteal phase of the menstrual cycle is believed to be due to temporary glandular and stromal tissue growth, luminal dilation of the ducts and alveoli, fluid retention in the glandular and stromal structures, and increased vascularization and blood flow (Scott et al., 1950; Drife, 1989; Fowler et al., 1990; Hussain et al., 1999; Alekseev, 2021; Biswas et al., 2022). However, studies suggest that most of the changes are merely due to water fluctuations and that change in breast glandular volume is relatively small (Rix et al., 2023). The breast changes during the menstrual cycle have been positively correlated with increased levels of estradiol and progesterone during the luteal phase (Jemström & Olsson, 1997; Clendenen et al., 2013; Rix et al., 2023). In addition, estrogen therapy has been found to reversibly increase breast size (e.g., Hartmann et al., 1998) and estradiol levels are positively associated with breast tenderness (e.g., de Lignières & Mauvais-Jarvis, 1981 [Figures]; Sitruk-Ware et al., 1984). Both estradiol and progesterone can promote water retention via distinct hormonal mechanisms as well as mediate breast glandular growth and changes (Rix et al., 2023). As such, the breast changes during the menstrual cycle are assumed to be due to changing levels of estradiol and progesterone, though it is noteworthy that progesterone has been particularly implicated owing to the breast volume increase occurring during the luteal phase (Lawrence & Lawrence, 2015; Rix et al., 2023). There is a delay in breast volume increases following the peaks of estradiol and progesterone levels during the menstrual cycle and hence the changes are not instantaneous (Rix et al., 2023).
Combined oral contraceptives, which are estrogen–progestogen preparations, as well as menopausal estrogen–progestogen hormone therapy, may produce temporary breast enlargement and feelings of breast fullness analogous to those that occur during the luteal phase of the menstrual cycle (Milligan, Drife, & Short, 1975; Dennerstein et al., 1980 [Figure]; Malini, Smith, & Goldzieher, 1985; Jemström & Olsson, 1997; Jernström et al., 2005). In one study, breast volume was around 100 mL greater (~30% higher) in women who were currently taking oral contraceptives relative to those who had not taken or had previously taken oral contraceptives (Jemström & Olsson, 1997). In some women, the increase in breast size with oral contraceptives was subjectively reported to be up to a single bra cup size in volume (Jemström & Olsson, 1997). However, in another study by the same group of researchers that had a much larger sample size (n=258 vs. n=65), breast volumes were not significantly different between current hormonal contraceptive users and non-users (Jernström et al., 2005). Additionally, another study found no significant differences in breast volume in women between different estrogen–progestogen oral contraceptives that had about 6-fold variation in dose of the same progestin (0.4 to 2.5 mg/day norethisterone) as well as non-users (Malini, Smith, & Goldzieher, 1985). However, this study was underpowered due to small sample sizes (n=5 to n=15 per group) (Malini, Smith, & Goldzieher, 1985).
Engman et al. (2008) conducted an RCT of treatment with mifepristone, a selective progesterone receptor modulator (SPRM) with predominantly antiprogestogenic effects, versus placebo for 3 months in normally cycling premenopausal cisgender women, and evaluated the effects of this progesterone receptor blockade on the breasts. They found that mifepristone significantly reduced Ki-67 index, a measure of cellular proliferation in the breasts, and reduced subjectively rated symptom scores on the Breast Symptom Index (BSI). More specifically, breast soreness, breast swelling, sense of increased breast volume, and the total breast symptoms score were all significantly reduced on the BSI. However, breast volume was not objectively measured in this study. A major limitation of this study is that mifepristone inhibits ovulation and modifies levels of estradiol and other hormones (Spitz et al., 1989; Spitz et al., 1994; Engman et al., 2008, Spitz, 2010). As such, it is unclear whether the effects observed by Engman and colleagues were specifically due to progesterone receptor antagonism in the breasts or due to disruption of the hypothalamic–pituitary–gonadal (HPG) axis, for instance lowered estradiol levels.
An interesting case report of an adult woman with CAIS documented a significant increase in breast volume with combined estrogen–progestogen therapy relative to estrogen monotherapy (Dijkman et al., 2023b). The woman was started on cyclic oral estradiol 2 mg/day and dydrogesterone 10 mg/day and subjectively experienced breast pain and fluctuations in breast volume of about one cup size while on this regimen. Subsequently, she was switched to oral estradiol valerate 3 mg/day monotherapy and the fluctuations in breast volume ceased. However, her overall breast volume was reduced as well, and the woman decided to resume combined estradiol and dydrogesterone therapy. Her clinicians proceeded to measure her breast volume using 3D body scanning. Her left breast was 758 mL and right breast was 673 mL with estrogen monotherapy, and her breasts increased to respective volumes of 875 mL and 784 mL during combined estrogen–progestogen therapy, giving net volume increases of 117 mL (+16%) and 111 mL (+17%). These differences in volume corresponded to an almost one bra cup difference in size. The researchers noted that estradiol and progesterone are associated with cyclical breast changes, and hypothesized that the changes in their patient were due to increased fluid retention in the breasts. Taken together, the case report demonstrates that progestogens can cause rapid and considerable reversible breast enlargement in some women analogous to that during the normal menstrual cycle.
Progesterone and Mammary Development in Animals
Progesterone and Pubertal Mammary Development in Animals
Although progesterone does not seem to be essential in normal pubertal mammary development in mice, studies have interestingly found that it is able to substitute for estrogen in mediating pubertal ductal mammary development in this species. Ruan, Monaco, & Kleinberg (2005) studied the effects of various combinations of exogenous estradiol, progesterone, and IGF-1 on mammary development in oophorectomized female IGF-1-knockout mice. In terms of stimulation of ductal development to occupy the mammary gland fat pad, the combination of progesterone and IGF-1 produced 92% occupation, estradiol and IGF-1 resulted in 92% occupation, estradiol, progesterone, and IGF-1 achieved 96% occupation, and IGF-1 alone resulted in only 28% occupation (Ruan, Monaco, & Kleinberg, 2005; Kleinberg & Ruan, 2008). In terms of gross anatomical appearance, the ductal tree with progesterone and IGF-1 was said to resemble that of a normal fully developed pubertal mammary gland (Ruan, Monaco, & Kleinberg, 2005). However, differences in mammary development between the combination of estradiol and IGF-1 and the combination of progesterone and IGF-1 were apparent, with estradiol and IGF-1 having greater effect on terminal end bud formation, ductal decorations, and slight alveolar maturation, and progesterone and IGF-1 having more effect on ductal formation, extension, and branching (Ruan, Monaco, & Kleinberg, 2005; Kleinberg & Ruan, 2008). The effects of progesterone on mammary development were reversed by the progesterone receptor antagonist mifepristone (Ruan, Monaco, & Kleinberg, 2005). Only the combination of estradiol, progesterone, and IGF-1 produced mammary development that resembled that during mid-pregnancy, with full maturation of secretory alveolar structures (Ruan, Monaco, & Kleinberg, 2005; Kleinberg & Ruan, 2008).
A limitation of studies that have used exogenous progesterone to stimulate pubertal ductal mammary development in mice is that the doses of progesterone employed, in conjunction with other hormones like estradiol, have been sufficient to mediate mammary growth to a level typical of pregnancy, with robust maturation of mammary lobuloalveolar structures (e.g., Škarda, Fremrová, & Bezecný, 1989; Ruan, Monaco, & Kleinberg, 2005). Pregnancy is a time when hormone levels are much higher than usual. Hence, the progesterone exposure in these studies may have been supraphysiological relative to normal puberty, and may have produced effects on mammary growth that would not otherwise occur during this time. Accordingly, Škarda, Fremrová, & Bezecný (1989) found that whereas untreated normal female mice naturally grew to a mammary gland area of 26.4 mm2 and normal female mice treated with exogenous estradiol grew to a mammary gland area of 25.3 mm2, normal female mice treated with exogenous estradiol and progesterone grew to a mammary gland area of 43.5 mm2 and with exogenous progesterone alone to a mammary gland area of 64.6 mm2. The untreated control mice did not show alveolar buds, whereas the progesterone-treated groups did have alveolar maturation, indicating supraphysiological and pregnancy-like development compared to non-pregnant mice (Škarda, Fremrová, & Bezecný, 1989). In any case, one study employed low doses of progesterone (0.1 mg/day), one-tenth of that used in most other studies (1 mg/day), and found that progesterone still stimulated significant ductal development in mice at these doses (Aupperlee et al., 2013; Berryhill, Trott, & Hovey, 2016). Hence, progesterone is still able to stimulate some level of ductal growth in mice even at lower levels.
Although progestogens by themselves can apparently stimulate normal pubertal mammary development in lieu of estrogen exposure in mice, it is not clear that they do so similarly in humans. It is well-known that progestogens alone, without concomitant estrogenic activity, do not generally produce breast development in humans. As an example, progestogens, for instance MPA and CPA, have been used as puberty blockers in boys and girls at very high doses, and do not produce breast development in this context, instead causing arrest and regression of breast development via gonadal suppression (Lyon, De Bruyn, & Grant, 1985; Fuqua & Eugster, 2022). Cases of gynecomastia in boys have occurred with CPA, but only in a minority and with this easily attributable to other causes than progestogenic activity, for instance the antiandrogenic activity of CPA and disruption of the HPG axis (Kauli et al., 1984; Laron & Kauli, 2000). Similarly, progestogens like MPA and CPA have been used at very high doses in men to treat prostate conditions and sexual disorders, and likewise do not usually produce gynecomastia under these circumstances. Rates of gynecomastia with CPA used in the treatment of prostate cancer are low and are not noticeably different from the rates with surgical or medical castration (~10%) (Fourcade & McLeod, 2004; Di Lorenzo et al., 2005). This is in major contrast to the high rates of gynecomastia with estrogens and nonsteroidal antiandrogens (up to 70–80%) (Fourcade & McLeod, 2004; Di Lorenzo et al., 2005; Deepinder & Braunstein, 2012). Species differences may be present such that progestogens can produce robust pubertal mammary development in mice but do not do so in humans.
Progesterone and Gestational Mammary Development in Animals
Therapeutic or pharmacological pseudopregnancy is a type of hormone therapy that attempts to replicate the hormonal mileu of pregnancy for certain medical indications in cisgender females by administering exogenous hormones. In practice, this has involved the administration of very high doses of estrogens and progestogens, with most other pregnancy hormones not included. Therapeutic pseudopregnancy was first developed in the 1950s and is largely no longer used in medicine today (Kaiser, 1993).
The effects of therapeutic pseudopregnancy on the breasts are of interest due to the breast changes that occur during pregnancy, for instance lobuloalveolar development and substantial reversible breast enlargement. In the 1980s, Lauritzen and colleagues conducted a study of therapeutic pseudopregnancy for treatment of breast hypoplasia (small/underdeveloped breasts) in cisgender women (Lauritzen, 1980; Lauritzen, 1982; Lauritzen, 1989; Göretzlehner & Lauritzen, 1992). They employed the estrogen estradiol valerate 40 mg/week and the progestogen hydroxyprogesterone caproate (OHPC) 250 to 500 mg/week both by intramuscular injection for 4 to 5 months. The estradiol valerate dosage employed was very high, with other studies by the same authors reporting that this dosage of estradiol valerate resulted in first-trimester pregnancy levels of estradiol in women (~3,000 pg/mL [~11,000 pmol/L]) (Ulrich, Pfeifer, & Lauritzen, 1994; Ulrich et al., 1995). These estradiol levels are roughly 30 times the normal concentrations outside of pregnancy (Aly, 2018b). Similarly, the OHPC doses were very high, with 250 to 500 mg per month being similar in strength to luteal-phase progestogenic exposure (Wiki). Hence, as the same OHPC doses were used weekly in the study, the doses were roughly around 4.5 times luteal-phase exposure and thus were analogously similar to first- or second-trimester progesterone levels in terms of strength (Aly, 2020d). The authors noted that they had initially tried lower hormone doses, similar to those originally used in the 1950s, but did not achieve significant breast growth with these doses, and so increased the dosage. Breast changes were measured in the study with a tape measure (applied horizontally and vertically to the breast area), photographs, breast imaging using mammography and sonography, and, later in the study, plasticine impressions/molds with determination of the filling volume.
Lauritzen and colleagues reported the study findings in four different publications with different follow-up times and growing sample sizes. In the final follow-up, a total of 221 women had been treated. In the second follow-up, when 78 women had been treated, it was noted that 29 of the cases (37%) were less than 18 years old. However, in the final follow-up of 221 women, the age range was listed as 18 to 42 years. The researchers found that breast volume increased by 10 to 30% above baseline in 65% of the women. This was also accompanied by breast tenderness in almost all of the women, though the breast tenderness progressively declined during the treatment period. Other breast-related side effects like pigmentation and stretch marks were rarely observed. Prolactin levels slightly increased to 14 to 28 pg/mL by the end of treatment. Breast imaging showed an increase in the density of breast glandular tissue. The researchers claimed that the increase in breast size in their study was due to increased adipose tissue, water retention, and moderate hypertrophy of the glandular tissue.
Following treatment discontinuation, the increases in breast volume gradually and partially regressed in 40% of the women, to an increase of 10 to 20% above baseline. However, the authors claimed that the regression in breast volume could be reduced with adequate-dose combined estrogen–progestogen birth control pills or with topical estrogen and progestogen therapy applied to the breasts. In addition, they noted that therapeutic pseudopregnancy could be repeated to increase breast volume again. This was performed in a subset of the women, with treatment repeated 1 to 2 times after 6 months. In the second follow-up, which had 78 women, it was noted that 12 women (15%) had undergone multiple treatments. Aside from Lauritzen and colleagues, many other researchers have also reported substantial or full regression in breast size following estrogen and/or progestogen therapy to increase breast size in cisgender women (e.g., Cernea, 1944; Müller, 1953; Anderson, 1962; Bruck & Müller, 1967; Keller, 1984; Kaiser & Leidenberger, 1991; Keller, 1995; Hartmann et al., 1998).
The findings of Lauritzen and colleagues were reported very informally, in the form of non-peer-reviewed book chapters, conference papers, and medical magazines, and were never published in a peer-reviewed journal article. In relation to this, the methodology and results of the study were only briefly and imprecisely described. There are also additional concerns related to study design, such as lack of controls, randomization, and the quality of the breast measurement methods. As a result of the preceding issues, it is difficult to fully interpret the results of the study and to have complete confidence in its findings. In any case, Lauritzen and colleages’ results suggest that treatment with high-dose combined estrogen–progestogen therapy, achieving earlier-pregnancy estrogenic and progestogenic exposure, may be able to produce a significant temporary increase in breast size and a smaller long-term increase. The findings of a permanent increase in breast size conflict with those of other researchers who have reported complete regression in breast changes following treatment discontinuation. Moreover, the results are contradicted by findings in pregnant women, who, as described previously, show complete reversion to pre-pregnancy breast size or to even slightly smaller breasts following cessation of lactation.
It is difficult to evaluate the relative roles of the estrogen and the progestogen in the findings of Lauritzen and colleagues, as there were no comparison groups employing estrogen or progestogen therapy alone in the study. Both estrogens and progestogens have been implicated in causing breast enlargement and plausibly could have contributed to the breast changes. As such, it is unclear to what extent the breast changes were specifically due to progestogenic exposure rather than to estrogenic exposure.
The breast size increases observed by Lauritzen and colleagues were seemingly more modest relative to those that occur normally during pregnancy. They also lacked certain characteristics of pregnancy-related breast changes, like nipple and areolar pigmentation. The reasons for this are not fully clear. The subject populations between these studies were different, for instance in terms of factors like initial breast size and age, which may be contributing reasons. Another possible contributing factor is that only estrogen and progestogen levels increased in the study, whereas levels of other pregnancy hormones, besides the slight increase in prolactin levels, did not increase. These other pregnancy hormones, for instance hPL and IGF-1, may also be involved in breast development during pregnancy. Finally, the treatment duration was only 4 to 5 months, and the estrogen and progestogen exposure was only similar to that during early-to-mid pregnancy, whereas normal pregnancy lasts 9 months and involves continued dramatic increases in estrogen and progesterone levels through to childbirth.
It should be noted that, owing to the highly supraphysiological estrogen and progestogen levels required, which can cause serious health complications like blood clots and cardiovascular problems (Aly, 2020e), as well as the small to negligible lasting increase in breast volume, therapeutic pseudopregnancy is inadvisable for transfeminine people and should not be pursued or employed. Nonetheless, the historical findings of therapeutic pseudopregnancy for increasing breast size in cisgender females are of significant theoretical interest in exploring the roles of estrogens and progestogens in breast growth.
Early Progestogen Exposure and the Possibility of Suboptimal Breast Development
While progestogens are typically sought after by transfeminine people for their potential in improving breast development, there have also been various suggestions in the literature that early or premature exposure to progestogens may result in suboptimal breast development and that progestogens may suppress or reduce estrogen-mediated breast development. These suggestions include progestogens having known antiestrogenic effects in the breasts, animal studies finding stunted mammary development with high doses of progestogens, clinical publications cautioning against premature introduction of progestogens in female puberty induction due to concerns about possibly stunted breast growth, clinical use of progestogens to treat macromastia in cisgender females, poor breast development with estrogen therapy in cisgender girls with a disorder of sexual development that results in high progesterone exposure, and breast development with estrogen and CPA (a very strong progestogen) typically being poor in transfeminine people. As with the question of whether progestogens can enhance breast development, it is currently unknown whether progestogens could worsen breast development. It is also unknown what dosage level and timing of introduction would be required for such an effect. In any case, for informational purposes, the preceding topics will each be discussed in the subsequent sections.
Antiestrogenic Effects of Progestogens in the Breasts
Stunted Mammary Growth with Progestogens in Animal Studies
Animal studies using progestogens including bioidentical progesterone and chlormadinone acetate (CMA), a progestin closely related to CPA, have found that high doses of these progestogens substantially stunt mammary gland development in rabbits, whereas lower doses do not do so (Lyons & McGinty, 1941; Beyer, Cruz, & Martinez-Manautou, 1970). See here for relevant literature excerpts as well as figures from these studies. Lyons & McGinty (1941) [Figure] found that estrogen alone induced ductal mammary development and estrogen plus progesterone 0.25 to 1 mg/day produced ductal development and slight to “fair” lobuloalveolar development. Conversely, estrogen plus progesterone 4 to 8 mg/day, which were 4- to 8-fold higher doses of progesterone than the most optimal dose, produced stunted mammary development with inhibited ductal development, only slight lobuloalveolar development, and, at the highest dosage, resulted in a much smaller mammary gland in terms of size than in the ≤1 mg/day groups. They concluded that high doses of progesterone are inhibitory and result in relatively poor mammary development. In the paper, doses of progesterone in international units (IU) were reported, but a citing review, Pfeiffer (1943), indicated that 1 IU progesterone is equal to 1 mg progesterone. As such, the milligram doses are listed above instead. Beyer, Cruz, & Martinez-Manautou (1970) [Figure] found that estrogen alone produced good ductal development without lobuloalveolar growth (mean mammary area = 376 mm2) and both estrogen plus CMA 0.5 mg/day and estrogen plus progesterone 2.5 mg/day produced optimal ductal and lobuloalveolar development (mean mammary area = 765 mm2 and mean mammary area = 688 mm2, respectively). Conversely, estrogen plus CMA 2.5 mg/day, a 5-fold higher dose of CMA than the optimal dose, resulted in dramatically reduced ductal development and mammary gland size albeit with significant lobuloalveolar growth (mean mammary area = 284 mm2). The authors concluded that moderate doses of progestogens stimulate mammary gland growth whereas large doses inhibit mammary gland development.
While these animal studies are suggestive that high doses of progestogens may be able to stunt breast development in humans, this is far from a certainty. There are species differences in hormone-mediated mammary development such that findings in one species, such as rabbits, may not translate to another species, like humans, or sometimes even to closely related species, like rats or guinea pigs (Bässler, 1970). As far as the present author is aware, stunted mammary development with high doses of progestogens has not been studied or reported in other animal species, for instance other rodent species or monkeys. It is also unclear that the doses employed in these animal studies are necessarily relevant to progestogen therapy in humans. This is because pregnancy levels of progesterone, which are much higher than luteal-phase progesterone levels, are necessary for substantial mammary lobuloalveolar development, and the doses of progestogens used in these studies were above that magnitude of progestogenic exposure. Hence, the doses may have corresponded to what in humans would be extremely high doses. However, such doses could still be relevant in the case of CPA used as an antiandrogen in humans, as CPA is used in this context at very high doses (see section below). The present author is unaware of any animal studies finding that physiological non-pregnancy levels of progesterone have any stunting or other adverse influence on mammary development, suggesting that only high doses of progestogens may have such effects. Finally, it seems notable that the estrogen and progestogen were initiated simultaneously in these animal studies and yet produced optimal pregnancy-like mammary development at the right doses. This suggests that early or immediate progestogen exposure might not be unfavorable in terms of breast development in humans. However, once again species differences may be present and confirmatory clinical studies are needed in humans.
Clinical Publications Cautioning Against Premature Introduction of Progestogens Due to Possibly Stunted Breast Development
A large number of clinical publications largely in the pediatric endocrinology literature have warned that premature exposure to progestogens during for instance puberty induction may result in suboptimal breast development in cisgender girls and/or transfeminine people (Zacharin, 2000; Bondy et al., 2007; Colvin, Devineni, & Ashraf, 2014; Wierckx, Gooren, & T’Sjoen, 2014; Kaiser & Ho, 2015; Bauman, Novello, & Kreitzer, 2016; Gawlik et al., 2016; Randolph, 2018; Donaldson et al., 2019; Heath & Wynne, 2019a; Heath & Wynne, 2019b; Iwamoto et al., 2019; Crowley & Pitteloud, 2020; Naseem, Lokman, & Fitzgerald, 2021; Federici et al., 2022; Lucien et al., 2022; Rothman & Iwamoto, 2022). The full relevant excerpts from these sources can be found here. In relation to these claims, and in order to mimic normal female puberty, a progestogen is not typically added to estrogen therapy during puberty induction in cisgender girls with delayed puberty until after about 2 to 3 years of treatment, by which point breast growth is generally considered complete. Additionally, progestogens are generally never added as part of puberty induction in transfeminine adolescents. Despite the preceding widespread literature statements and accepted clinical practices in the field of puberty induction however, it is important to note that the claims that premature introduction of progestogens might stunt breast development in this context are currently not based on any actual reliable clinical evidence and hence remain unsubstantiated. It is not even clear that these statements are based on anecdotal clinical experience as opposed to simple conjecture. The absence of data in this area may finally change in the future as more clinical studies of progestogens in puberty induction in cisgender girls are conducted (e.g., Rodari et al., 2023).
Rodari and colleagues studied optimization of puberty induction with estrogen therapy followed by eventual introduction of progestogen therapy in 49 cisgender girls with hypogonadism (e.g., Rodari et al., 2022; Rodari, 2022; Rodari et al., 2023). The researchers employed incrementally titrated low-dose transdermal estradiol to mimic the low and gradually increasing estradiol levels during normal puberty and added a progestogen only once menstrual bleeding began. The total duration of treatment was mean 2.65 ± 1 years, the time of first menstrual bleeding occurrence was 2.3 ± 1 years, and the time of progestogen introduction was median 2.22 years (IQR 1.56–2.87 years). Of the girls, 90% reached Tanner breast stage 4, but only 41% reached Tanner breast stage 5. Reaching the final Tanner breast stage was significantly associated with the number of estradiol dose increases (i.e., gradual estradiol dose titration) and the estradiol dose at progestogen introduction. The researchers interpreted the latter finding as progestogen exposure potentially hampering breast development. They questioned introducing progestogen therapy in the presence of incompletely developed breasts and suggested that instead of adding a progestogen upon onset of menstrual bleeding, clinicians should consider slightly reducing the estradiol dosage to delay progestogen introduction until the breasts complete maturation. While interesting, it must be noted that the findings of Rodari and colleagues are merely correlational, are open to multiple interpretations, and do not causally show that progestogens impair breast maturation.
Progestogens in the Treatment of Breast Hypertrophy
More recently, a couple of studies, both by the same group of researchers, assessed the impact of different types of hormonal contraception on macromastia in adolescent cisgender females with macromastia (Nuzzi et al., 2021; Nuzzi et al., 2022). They found that use of progestin-only contraceptives was associated with significantly more breast tissue removed upon surgical breast reduction (959.9 g/m2 vs. 735.9 g/m2 [+30%]; p = 0.04) and worse clinical symptoms (e.g., breast pain—odds ratio, 4.94, p = 0.005) relative to non-users of hormonal contraception (Nuzzi et al., 2021). Conversely, use of combined oral contraceptives, which are estrogen–progestogen preparations, was associated with significantly less breast tissue removed with breast reduction (639.5 g/m2 vs. 735.9 g/m2 [−13%]; p = 0.003), though not with any differences in clinical symptoms, relative to those naive to hormonal contraception (Nuzzi et al., 2022). It should be noted that progestin-only contraceptives suppress the HPG axis and result in low estradiol levels, whereas combined oral contraceptives suppress the HPG axis and lower estradiol production but simultaneously supplement estrogen signaling by delivering exogenous estrogen. This difference may somehow be responsible for the opposite influence of estrogen–progestogen therapy versus progestogen-alone therapy on macromastia severity. While the findings of Nuzzi and colleagues are interesting, it is noteworthy that the methodology and findings of their research were criticized on various grounds in a letter to the editor concerning one of the articles (Karp, 2022).
Santen et al. (2024), in a case series of cisgender girls with juvenile gigantomastia, noted that breast growth continues for only a number of years following onset and hence there must be some form of stop signal that is activated and that prevents further breast growth. They speculated that this signal may be related to apoptosis (programmed cell death). Santen and colleagues noted that in adult cisgender women, proliferation of breast cells is increased during the follicular phase of the menstrual cycle, whereas apoptosis in breast cells is increased during the luteal phase of the cycle. They hypothesized that the apoptosis during the luteal phase may block further breast development. Since progesterone is produced during the luteal phase and may mediate said apoptosis, this would substantiate the use of progestogens in the treatment of breast hypertrophy. However, the researchers noted that no data exist on apoptosis in the breasts of girls with juvenile gigantomastia. Moreover, an important point against the authors’ hypothesis is that estrogen-induced breast growth gradually slows and ceases in people who do not have menstrual cycles and luteal phases or progestogenic exposure just as it does in normal cisgender girls. Prominent examples of such individuals include CAIS women, transfeminine people, and cisgender men with prostate cancer treated with estrogen therapy.
Poor Breast Development in 17α-Hydroxylase/17,20-Lyase Deficiency
Non-Comparative Clinical Studies of Breast Development with Estrogen and Cyproterone Acetate in Transfeminine People
The possibility of suboptimal breast development with premature exposure to progestogens is of particular relevance in the case of CPA used as an antiandrogen in transfeminine people. This is because CPA is a potent progestogen in addition to antiandrogen, starts to be taken at the initiation of hormone therapy, and happens to be used in transfeminine people at doses that result in very strong to profound progestogenic exposure (Aly, 2019). In terms of progestogenic strength, CPA at a dosage of 2 mg/day is comparable to the progesterone exposure during the luteal phase of the menstrual cycle (Aly, 2019; Wiki). For comparison, CPA has been used in transfeminine people at doses ranging from 10 to 100 mg/day (Aly, 2019). This would mean that CPA provides roughly 6.25 times the progestogenic impact of luteal-phase progesterone exposure at a dosage of 12.5 mg/day, 12.5 times the impact at 25 mg/day, 25 times the impact at 50 mg/day, and 50 times the impact at 100 mg/day. Moreover, this does not consider the fact that progesterone is only produced during the luteal phase, or half of the menstrual cycle, whereas CPA is taken continuously every day of the month. The preceding magnitudes of progestogenic exposure with CPA are on par with and even beyond those during pregnancy. Only recently have lower doses of CPA (e.g., ≤12.5 mg/day) started to be used in transfeminine hormone therapy.
Studies in pubertal and adolescent transfeminine people given GnRH agonists to block puberty plus estrogen therapy have reported good breast development in these individuals as assessed by subjective clinical impression or Tanner staging (de Vries et al., 2010; Hannema et al., 2017). However, quality objective measures of breast development were not employed in these studies. Conversely, non-comparative studies using estrogen plus CPA in adult transfeminine people have commonly reported modest breast development, including incomplete breast development only to Tanner stage 2 to 4, small breast cup sizes, and small breast volumes (Kanhai et al., 1999; Sosa et al., 2003; Sosa et al., 2004; Wierckx et al., 2014; Fisher et al., 2016; Tack et al., 2017; de Blok et al., 2018; Reisman, Goldstein, & Safer, 2019; Meyer et al., 2020; de Blok et al., 2021). Additionally, breast sizes smaller than those in cisgender women have been reported (Asscheman & Gooren, 1992; Kanhai et al., 1999). In one study, breast development with estrogen plus CPA was also poor in late-adolescent transfeminine people (Tack et al., 2017). However, in this particular study, the estrogen dose used was likely too low and resulted in inadequate estradiol levels, as noted by the authors themselves, and this is a potential confounding factor in their findings (Tack et al., 2017). In any case, breast growth with estrogen plus CPA in transfeminine people would seem to consistently be poor. In contrast to the regimen of estrogen and CPA, breast development with other hormone therapy regimens, for instance estrogen with non-progestogenic antiandrogens like spironolactone, bicalutamide, and GnRH modulators, has not been nearly as well-studied in comparison, and hence comparisons of outcomes between regimens is difficult.
In one of the highest quality studies of estrogen and CPA and breast development in adult transfeminine people, breast volume measured with 3D body scanning (Vectra XT) was approximately mean 100 mL (95% CI ~75–125 mL; range up to ~750 mL), equating to less than an A cup size on average, after 3 years of hormone therapy with estrogen and CPA in 69 transfeminine people (de Blok et al., 2021 [Figure]). In this study, breast changes over time had clearly plateaued, suggesting that breast development was either complete or was nearly so (de Blok et al., 2021 [Figure]). Although most of the transfeminine people in this study had less than an A cup breast size (71%), a minority had cup sizes ranging from an A cup (9%), B cup (16%), C cup (3%), to E cup (1%) (de Blok et al., 2021 [Figure]). For comparison, a study of normative data on breast volumes in cisgender women, using a different 3D body scanning device (Artec Eva 3D), found breast volumes of median ~515 mL and mean ~650 mL (IQR ~310–850 mL; range ~50–3,100 mL) in 378 cisgender women (Coltman, Steele, & McGhee, 2017). As such, adult transfeminine people treated with estrogen and CPA would appear to have substantially smaller breasts than cisgender women. However, it must be emphasized that the preceding data come from separate clinical studies and hence are not directly comparative. It is noteworthy in this regard that breast volumes can vary considerably between different studies even using similar measurement methods (e.g., magnetic resonance imaging) (Sindi et al., 2019 [Table]). Hence, there is a need for studies directly comparing breast volumes in transfeminine people to those in cisgender women using the same measurement method in order to comparatively evaluate breast development.
Regardless of the preceding, transfeminine people could simply have poor breast development in general without this necessarily being related to CPA or progestogenic exposure. Indeed, a more recent study in transfeminine people who underwent pubertal suppression in adolescence, presumably with GnRH agonists and then estrogen therapy, found similarly poor breast development as has been reported in adults (Boogers et al., 2022; c.f. de Blok et al., 2021). This study used breast volume via 3D body scanning to measure breast development and found a mean breast volume of 114 mL (IQR 58–203 mL), equating to less than an A cup size, after 4.2 years of hormone therapy (Boogers et al., 2022). It was notably conducted by the same group of researchers who did the earlier higher-quality study in adult transfeminine people, and hence likely used the same 3D scanning method (de Blok et al., 2021).
No directly comparative studies of breast development with CPA versus other antiandrogens in transfeminine people are currently available. Hence, it’s not fully known whether the findings are specific to CPA or also generalize to other antiandrogens that are not also strongly progestogenic. The RCT of estradiol and spironolactone versus estradiol and CPA in transfeminine people by Ada Cheung and colleagues underway in Australia may provide more insight on this issue, as spironolactone is only a weakly or clinically non-progestogenic antiandrogen (Aly, 2018b; Wiki; update: see below).
Additional Considerations for Progestogen Therapy and Breast Development in Transfeminine People
Anecdotes About Progestogens and Breast Development
Many transfeminine people who have taken progestogens as part of hormone therapy have anedotally reported that the progestogens improved their breast development. At the same time, many other transfeminine people have anecdotally reported no benefit of progestogens to breast development. It must be cautioned in general that anecdotal reports are unreliable and represent a very low form of medical evidence. This is because subjective observations and attributions are often erroneous. Perceptions can be faulty and inaccurate, especially with slowly developing physical changes, and true physical changes can be due to coincidence and unrelated confounding factors rather than due to a person’s causal attributions. A couple notable examples of potential confounding factors with regard to progestogens and breast development include: (1) continued breast development from estrogen acting on its own; and (2) temporary breast enlargement due to local fluid retention, increased blood flow, and reversible lobuloalveolar growth caused by progestogens. Such factors have the potential to mislead, and may contribute significantly to anecdotal reports of enhanced breast development with progestogens in transfeminine people. Clinical studies that are well-designed, controlled, and employ reliable objective measures, with long-term follow-up and eventual discontinuation of the progestogen to control for reversible effects, are needed to properly evaluate the effects of progestogens on breast development.
Therapeutic Limitations of Oral Progesterone
Oral progesterone produces very low progesterone levels and has only weak progestogenic effects even at high doses (Aly, 2018a; Wiki). These low progesterone levels are likely to be inadequate in terms of desired physiological progestogenic effects, for instance in the breasts. Oral progesterone also uniquely has potent neurosteroid actions via active metabolites like allopregnanolone, which can result in prominent side effects such as alcohol-like central nervous system inhibition as well as mood swings (Aly, 2018b; Wiki; Wiki). These neurosteroid effects are dose-dependent and are more severe at high doses. Non-oral progesterone forms like rectal or injectable progesterone or progestins, which do not have the preceding problems, can be used instead to avoid such concerns (Aly, 2018a; Aly, 2018b).
Tolerability and Safety Considerations for Progestogens
Progestogens have a variety of tolerability issues and safety risks (Aly, 2018b). Examples of such risks variously include adverse mood changes, breast cancer, blood clots, cardiovascular complications, benignbrain tumors including prolactinomas and meningiomas, and off-target actions with undesirable effects (e.g., androgenic or glucocorticoid activity), among others (Aly, 2018b). CPA at high doses also uniquely has a significant risk of serious liver toxicity (Aly, 2018b). The risks of progestogens vary depending on the specific progestogen and dosage, but all progestogens, including even bioidentical progesterone, have significant known risks. The risks of progestogens, along with lack of evidence of beneficial effects in terms of feminization, well-being, and health, are why there are concerns about and hesitations on their use in transfeminine people (Aly, 2018b). However, cisgender women naturally have progesterone in their bodies, and the absolute risks of progestogens are low (Aly, 2018b). The risks of progestogens can be minimized by use for a limited duration of time (e.g., a few years), by using the lowest dosages expected to be effective in terms of desired effects, and by selection of progestogens with more favorable pharmacological profiles (Aly, 2018a; Aly, 2018b).
Updates
Update 1: Angus et al. (2023–2024)
It was previously reported in this article that an RCT assessing breast development with estradiol plus spironolactone versus estradiol plus CPA in transfeminine people was being conducted by Ada Cheung and colleagues. This study could provide more insight into breast development with progestogens, as CPA is a very potent progestogen whereas spironolactone is not meaningfully progestogenic. Cheung and colleagues’ study, led by Lachlan Angus, has now been published in the form of the following two conference abstracts, with a journal article also currently in the process of being published:
Angus, L. M., Leemaqz, S., Zajac, J. D., & Cheung, A. S. (November 2023). A randomised controlled trial of spironolactone versus cyproterone in trans people commencing estradiol. AusPATH 2023 Symposium. [URL] [PDF] [Trans Health Research Blog Post]
Angus, L. M., Leemaqz, S. Y., Zajac, J. D., & Cheung, A. S. (November 2023). The effect of cyproterone and spironolactone on breast development in transgender women: a randomised controlled trial. ESA/SRB/ENSA 2023 ASM 26-29 November, Brisbane, 54–55 (abstract no. 132). [URL] [PDF] [Full Abstract Book] [Trans Health Research Blog Post]
The study assessed estradiol plus spironolactone 100 mg/day versus estradiol plus CPA 12.5 mg/day in 55 transfeminine people, with 27 in the spironolactone group and 28 in the CPA group. Hormone therapy duration, at least at this follow-up point in the study, was 6 months. The measures of breast development included breast–chest difference (primary) and estimated breast volume (secondary).
Breast development, measured by breast–chest difference (mean ± SD), was 8.3 ± 2.7 cm with spironolactone and 9.2 ± 3.0 cm with CPA, with the differences between groups not statistically significant (p = 0.27). In addition, breast development, measured by estimated breast volume (mean ± SD), was 158 ± 112 mL with spironolactone and 190 ± 159 mL with CPA, with the differences between groups not statistically significant (p = 0.39). There was variability between individuals in estimated breast volume, with breast volume measurements ranging from 20 to 788 mL. Besides breast growth, the researchers found that CPA also resulted in a greater increase in body fat percentage and gynoid fat compared to spironolactone. Estradiol levels were comparable between antiandrogen groups, whereas total testosterone levels were (mean ± SD) 4.29 ± 5.44 nmol/L (124 ± 157 ng/dL) with spironolactone and 1.48 ± 3.45 nmol/L (43 ± 99 ng/dL) with CPA, a difference that was statistically significant (p = 0.04).
The researchers concluded that there was no difference in breast development with spironolactone versus CPA in their study and that antiandrogen choice should be individualized based on patient and clinician preference as well as consideration of associated side effects. Moreover, they concluded that further research is needed to optimize breast development in transfeminine people.
Angus, L., Mikolajczyk, M., Cheung, A., Zajac, J., Antoszewski, B., & Kasielska-Trojan, A. (2022). Estimation of breast volume in transgender women using 2D photography: validation of the BreastIdea Volume Estimator in men and transgender women. ESA/SRB/APEG/NZSE ASM 2022, November 13-16, Christchurch, Abstracts and Programme, 127–127 (abstract no. 279). [URL] [PDF] [Full Abstract Book]
In studies by the developers of the BreastIdea Volume Estimator, they reported breast volumes measured with the tool in cisgender women. These estimated breast volumes can provide comparison to the breast-volume findings in transfeminine people by Cheung and Angus and colleagues. The developers of the BreastIdea Volume Estimator reported that breast volume (mean ± SD) in cisgender women with normal breasts (n=30) was 283 ± 144 mL and in cisgender women with macromastia or gigantomastia (n=35) was 888 ± 277 mL (Kasielska-Trojan, Zawadzki, & Antoszewski, 2022). In another study, they reported that breast volume (mean ± SD) in cisgender women was 272 ± 150 mL, with a range of 99 to 694 mL (Kasielska-Trojan, Mikołajczyk, & Antoszewski, 2020).
Although the BreastIdea Volume Estimator is an interesting and promising tool for quantifying breast development, it has notable limitations, such as its resolution and accuracy being much less than that with 3D scanners like the Artec Eva and Vectra XT (Mikołajczyk, Kasielska-Trojan, & Antoszewski, 2019). Vectra and Artec 3D scanners have been and are being employed to measure breast development with hormone therapy in other studies in transfeminine people (de Blok et al., 2021; Boogers et al., 2022; Dijkman et al., 2023a; Dijkman et al., 2023b; Lopez et al., 2023). The accuracy limitations of the BreastIdea Volume Estimator may explain why the breast volume findings with it in transfeminine people and cisgender women were different from those seen in other studies that employed more advanced 3D scanning methods. Aside from the breast volume measurement, breast–chest difference also has limitations as a measure of breast development in transfeminine people, for instance failing to identify continued breast growth that can be detected with breast volume measurement (de Blok et al., 2021).
Besides the employed measurement methods for breast development, limitations of Lachlan Angus and colleagues’ RCT of breast development with spironolactone and CPA in transfeminine people include its limited duration of follow-up of only 6 months, the fact that testosterone levels were non-equivalent between the spironolactone and CPA groups, and its limited sample size. The incompletely suppressed testosterone levels with spironolactone are notable as androgens oppose estrogen-mediated breast development and could have reduced breast development in the spironolactone group. The limited sample size of the study was responsible for the numeric difference in breast measurements between antiandrogen groups not being statistically significant. In any case, Angus and colleagues’ findings are suggestive that CPA, which is highly progestogenic, neither enhances nor stunts breast development, at least relative to non-progestogenic spironolactone for up to 6 months of hormone therapy. It seems likely that the RCT will continue to longer follow-up times and durations of hormone therapy in the future.
Update 2: Flamant, Vervalcke, & T’Sjoen (2023) and Yang et al. (2024)
The following two recent studies provide additional information on the topic of breast development with progestogen exposure—specifically with CPA—in transfeminine people:
Flamant, T., Vervalcke, J., & T’Sjoen, G. (November 2023). Dose Reduction of Cyproterone Acetate in Trans Women and the Effect on Patient-reported Outcomes: Results from the ENIGI Study. Endocrine Abstracts, 97 [Belgian Endocrine Society 2023], 5–5 (abstract no. 007). [URL] [PDF]
Yang, W., Hong, T., Chang, X., Han, M., Gao, H., Pan, B., Zhao, Z., & Liu, Y. (2024). The efficacy of and user satisfaction with different antiandrogens in Chinese transgender women. International Journal of Transgender Health, advance online publication. [DOI:10.1080/26895269.2024.2323514]
In the first study, Flamant, Vervalcke, & T’Sjoen (2023), clinical outcomes in transfeminine people at the University of Ghent, Belgium clinic were compared in 72 people taking CPA at low doses (10–12.5 mg/day) or high doses (25–50 mg/day). Testosterone suppression was equivalent between the two dose groups. Breast development satisfaction, measured with the Body Image Scale, was not significantly different with low-dose CPA versus high-dose CPA following 1 year of hormone therapy (p = 0.078). However, the p-value indicates that there was almost a statistically significant difference between groups, though it was not stated which group was numerically higher in terms of satisfaction. In any case, the researchers stated that breast development satisfaction was “non-inferior” with low-dose CPA compared to high-dose CPA, which seems suggestive that satisfaction may have been higher in the high-dose CPA group. These findings suggest that higher doses of CPA may not stunt breast development relative to doses of CPA that are lower, although still quite high in terms of progestogenic activity.
In the second study, Yang et al. (2024), clinical outcomes in transfeminine people at the Peking University Third Hospital in China with estradiol plus spironolactone (n=43) versus estradiol plus CPA (n=53) were retrospectively compared. Testosterone levels were much higher in the spironolactone group relative to the CPA group (374 ng/dL [13.0 nmol/L] vs. 20 ng/dL [0.7 nmol/L]; p < 0.001) and duration of hormone therapy was shorter in the spironolactone group than in the CPA group (median 12 months vs. 18 months). Breast development satisfaction, measured with a visual analogue scale (VAS), was median 6.0 (IQR 4.0–7.0) with spironolactone and 6.0 (IQR 4.0–7.0) with CPA, and was not statistically different. On the other hand, the CPA group outperformed the spironolactone group in terms of several other VAS-based clinical-outcome measures, including figure feminization, testicular atrophy, decreased penile erections, and in terms of a composite overall satifaction score. These findings suggest, as with the RCT by Lachlan Angus and colleagues, that spironolactone and CPA result in similar breast development in transfeminine people despite differences in testosterone levels and other clinical outcomes.
Abduljalil, K., Furness, P., Johnson, T. N., Rostami-Hodjegan, A., & Soltani, H. (2012). Anatomical, Physiological and Metabolic Changes with Gestational Age during Normal Pregnancy. Clinical Pharmacokinetics, 51(6), 365–396. [DOI:10.2165/11597440-000000000-00000]
Adams, R. D., Kliman, B., Federman, D. D., Ulfelder, H. S., & Holmes, L. B. (1970). Syndromes of Testicular Feminization. Clinical Pediatrics, 9(3), 165–178. [DOI:10.1177/000992287000900312]
Alekseev, N. P. (2021). Origin and Development of the Mammary Glands. In Alekseev, N. P. Physiology of Human Female Lactation (pp. 11–66). Cham: Springer. [DOI:10.1007/978-3-030-66364-3_2]
Alex, A., Bhandary, E., & McGuire, K. P. (2020). Anatomy and Physiology of the Breast during Pregnancy and Lactation. In Alipour, S., & Omranipour, R. (Eds.). Diseases of the Breast during Pregnancy and Lactation (Advances in Experimental Medicine and Biology, Volume 1252) (pp. 3–7). Cham: Springer. [DOI:10.1007/978-3-030-41596-9]
Anderson, W. A. (1962). Experimental stimulation of breast development in the teen-age female. The Journal of the Medical Society of New Jersey, 59(10), 541–543. [Google Scholar] [PubMed] [PDF]
Andler, W., & Zachmann, M. (1979). Spontaneous breast development in an adolescent girl with testicular feminization after castration in early childhood. The Journal of Pediatrics, 94(2), 304–305. [DOI:10.1016/s0022-3476(79)80852-5]
Angus, L. M., Leemaqz, S., Zajac, J. D., & Cheung, A. S. (2023). A randomised controlled trial of spironolactone versus cyproterone in trans people commencing estradiol. AusPATH 2023 Symposium. [URL] [PDF] [Trans Health Research Blog Post]
Angus, L. M., Leemaqz, S. Y., Zajac, J. D., & Cheung, A. S. (2023). The effect of cyproterone and spironolactone on breast development in transgender women: a randomised controlled trial. ESA/SRB/ENSA 2023 ASM 26-29 November, Brisbane, 54–55 (abstract no. 132). [URL] [PDF] [Full Abstract Book] [Trans Health Research Blog Post]
Angus, L., Mikolajczyk, M., Cheung, A., Zajac, J., Antoszewski, B., & Kasielska-Trojan, A. (2022). Estimation of breast volume in transgender women using 2D photography: validation of the BreastIdea Volume Estimator in men and transgender women. ESA/SRB/APEG/NZSE ASM 2022, November 13-16, Christchurch, Abstracts and Programme, 127–127 (abstract no. 279). [URL] [PDF] [Full Abstract Book]
Apter, D. (1980). Serum steroids and pituitary hormones in female puberty: a partly longitudinal study. Clinical Endocrinology, 12(2), 107–120. [DOI:10.1111/j.1365-2265.1980.tb02125.x]
Apter, D., Räisänen, I., Ylöstalo, P., & Vihko, R. (1987). Follicular growth in relation to serum hormonal patterns in adolescent compared with adult menstrual cycles. Fertility and Sterility, 47(1), 82–88. [DOI:10.1016/s0015-0282(16)49940-1]
Aritaki, S., Miyazawa, H., Ogihara, M., Ushio, M., & Izumizawa, A. (1992). An Endocrinological Study of Persistent Pubertal Macromastia. The Tohoku Journal of Experimental Medicine, 167(3), 189–196. [DOI:10.1620/tjem.167.189]
Arya, S., Barnabas, R., Lila, A. R., Sarathi, V., Memon, S. S., Bhandare, V. V., Thakkar, K., Patil, V., Shah, N. S., Kunwar, A., & Bandgar, T. (2021). Clinical, Hormonal, Genetic, and Molecular Characteristics in Androgen Insensitivity Syndrome in an Asian Indian Cohort from a Single Centre in Western India. Sexual Development, 15(4), 253–261. [DOI:10.1159/000517763]
Asscheman, H., & Gooren, L. J. (1992). Hormone Treatment in Transsexuals. In Bocking, W. O., Coleman, E. (Eds). Gender Dysphoria: Interdisciplinary Approaches in Clinical Management (pp. 39–54). Binghamton: Haworth Press. / Journal of Psychology & Human Sexuality, 5(4), 39–54. [Google Scholar] [Google Books] [DOI:10.1300/J056v05n04_03]
Athanasoulia, A., Auer, M., Riepe, F., & Stalla, G. (2013). Rare Missense P450c17 (CYP17A1) Mutation in Exon 1 as a Cause of 46,XY Disorder of Sexual Development: Implications of Breast Tissue ‘Unresponsiveness’ despite Adequate Estradiol Substitution. Sexual Development, 7(4), 212–215. [DOI:10.1159/000348301]
Atwood, C., Hovey, R., Glover, J., Chepko, G., Ginsburg, E., Robison, W., & Vonderhaar, B. (2000). Progesterone induces side-branching of the ductal epithelium in the mammary glands of peripubertal mice. Journal of Endocrinology, 167(1), 39–52. [DOI:10.1677/joe.0.1670039]
Aupperlee, M. D., Leipprandt, J. R., Bennett, J. M., Schwartz, R. C., & Haslam, S. Z. (2013). Amphiregulin mediates progesterone-induced mammary ductal development during puberty. Breast Cancer Research, 15(3), R44. [DOI:10.1186/bcr3431]
Bahr, C., Ewald, J., Dragovich, R., & Gothard, M. D. (2024). Effects of progesterone on gender affirmation outcomes as part of feminizing hormone therapy. Journal of the American Pharmacists Association, 64(1), 268–272. [DOI:10.1016/j.japh.2023.08.001]
Baird, D., Hytten, F. E., & Thomson, A. M. (1958). Age and Human Reproduction. BJOG, 65(6), 865–876. [DOI:10.1111/j.1471-0528.1958.tb08582.x]
Baker, S. B., Burkey, B. A., Thornton, P., & LaRossa, D. (2001). Juvenile Gigantomastia: Presentation of Four Cases and Review of the Literature. Annals of Plastic Surgery, 46(5), 517–526. [DOI:10.1097/00000637-200105000-00011]
Bames, H. O. (1948). Reduction of massive breast hypertrophy. Plastic and Reconstructive Surgery, 3(5), 560–569. [DOI:10.1097/00006534-194809000-00006]
Barbieri, R. L. (2019). Breast. In Strauss, J. F., & Barbieri, R. L. (Eds.). Yen and Jaffe’s Reproductive Endocrinology: Physiology, Pathophysiology, and Clinical Management, 8th Edition (pp. 248–255.e3). Philadelphia: Elsevier. [Google Books] [DOI:10.1016/B978-0-323-47912-7.00010-X]
Baron, J. (1993). Zespół braku wrazliwości na androgeny. Studium kliniczne i endokrynologiczne 40 osobników [Androgen insensitivity syndrome. Clinical and endocrinologic study of 40 cases]. Endokrynologia Polska, 44(2), 175–186. [Google Scholar] [PubMed]
Baron, J. (1994). Klasyczne i niepełne zespoły braku wrazliwości na androgeny [Classical and incomplete androgen insensitivity syndromes]. Ginekologia Polska, 65(7), 377–386. [Google Scholar] [PubMed]
Baron, J. (1994). Niepełny lub cześciowy zespół braku wrazliwości na androgeny [Partial androgen insensitivity syndrome]. Ginekologia Polska, 65(6), 319–325. [Google Scholar] [PubMed]
Barrat, J., de Lignières, B., Marpeau, L., Larue, L., Fournier, S., Nahoul, K., Linares, G., Giorgi, H., & Contesso, G. (1990). Effet in vivo de l’administration locale de progestérone sur l’activité mitotique des galactophores humains. Résultat d’une étude pilote. [The in vivo effect of the local administration of progesterone on the mitotic activity of human ductal breast tissue. Results of a pilot study.] Journal de Gynecologie, Obstetrique et Biologie de la Reproduction, 19(3), 269–274. [Google Scholar 1] [Google Scholar 2] [PubMed]
Barrett, J. (2009). The clinical risks associated with the diagnosis and management of disorders of gender identity. Clinical Risk, 15(4), 131–134. [DOI:10.1258/cr.2008.080069]
Bässler, R. (1970). The Morphology of Hormone Induced Structural Changes in the Female Breast. In Altmann, H.-W., et al. (Eds.). Current Topics in Pathology: Ergebnisse der Pathology, Volume 53 (pp. 1–89). Heidelberg: Springer Berlin. [DOI:10.1007/978-3-662-30514-0_1] [PDF]
Basson, R., & Prior, J. C. (1998). Hormonal Therapy of Gender Dysphoria: The Male-to-Female Transsexual. In Denny, D. (Ed.). Concepts in Transgender Identity (Garland Gay and Lesbian Studies, Volume 11) (pp. 277–296). New York: Garland Publishing Inc. [Google Scholar] [Google Books] [DOI:10.4324/9780203775134-19] [PDF]
Bauman, A., Novello, L., & Kreitzer, P. (2016). Endocrine Disorders and Delayed Puberty. In Appelbaum, H. (Ed.). Abnormal Female Puberty: A Clinical Casebook (pp. 87–107). Cham: Springer. [DOI:10.1007/978-3-319-27225-2_5]
Bayer, C. M., Bani, M. R., Schneider, M., Dammer, U., Raabe, E., Haeberle, L., Faschingbauer, F., Schneeberger, S., Renner, S. P., Fischer, D., Schulz-Wendtland, R., Fasching, P. A., Beckmann, M. W., & Jud, S. M. (2014). Assessment of breast volume changes during human pregnancy using a three-dimensional surface assessment technique in the prospective CGATE study. European Journal of Cancer Prevention, 23(3), 151–157. [DOI:10.1097/cej.0b013e3283651ccb]
Beck, P. (1972). Lactogenic Activity of Human Chorionic Somatomammotropin in Rhesus Monkeys. Experimental Biology and Medicine, 140(1), 183–187. [DOI:10.3181/00379727-140-36422]
Begley, D. J., Firth, J. A., & Hoult, J. R. (1980). The Breast and Lactation. In Begley, D. J., Firth, J. A., & Hoult, J. R. Human Reproduction and Developmental Biology (pp. 204–219). London: Macmillan Education UK. [DOI:10.1007/978-1-349-16260-4_14]
Bellwether, C. J. (2020). Why Should a Transfeminine Person Consider Progesterone? Google Docs. [URL]
Benjamin, H. (1966). Nonsurgical Management of Transsexualism. In Benjamin, H. The Transsexual Phenomenon (pp. 86–99). New York: Julian Press. [Google Scholar] [Google Books] [OpenLibrary] [WorldCat] [PDF]
Benjamin, H. (1967). Transvestism and Transsexualism in the male and female. Journal of Sex Research, 3(2), 107–127. [DOI:10.1080/00224496709550519]
Berliere, M., Coche, M., Lacroix, C., Riggi, J., Coyette, M., Coulie, J., Galant, C., Fellah, L., Leconte, I., Maiter, D., Duhoux, F. P., & François, A. (2022). Effects of Hormones on Breast Development and Breast Cancer Risk in Transgender Women. Cancers, 15(1), 245. [DOI:10.3390/cancers15010245]
Berryhill, G. E., Trott, J. F., & Hovey, R. C. (2016). Mammary gland development—It’s not just about estrogen. Journal of Dairy Science, 99(1), 875–883. [DOI:10.3168/jds.2015-10105]
Bertelloni, S., Dati, E., Baroncelli, G. I., & Hiort, O. (2011). Hormonal Management of Complete Androgen Insensitivity Syndrome from Adolescence Onward. Hormone Research in Paediatrics, 76(6), 428–433. [DOI:10.1159/000334162]
Bethea, C. L., Kohama, S. G., & Pecins-Thompson, M. (1997). Pituitary and Brain Actions of Estrogen and Progesterone in the Regulation of Primate Prolactin Secretion. In Pavlik, E. J. (Ed.). Estrogens, Progestins, and Their Antagonists: Functions and Mechanisms of Action (pp. 3–46). Boston: Birkhäuser. [DOI:10.1007/978-1-4612-2004-6_1]
Bevan, D. J. (2012). Progesterone for Breast Development? / Should Male-to-Female Transsexuals Take Progesterone as part of Hormone Therapy (HT) for Better Breast Development? Biopsychology of TSTG / Transgender Forum. [URL 1] [URL 2]
Bevan, D. J. (2019). Grow Your Own : Breast Development Update. Transgender Forum. [URL]
Beyer, C., Cruz, M. L., & Martinez-Manautou, J. (1970). Effect of Chlormadinone Acetate on Mammary Development and Lactation in the Rabbit. Endocrinology, 86(5), 1172–1174. [DOI:10.1210/endo-86-5-1172]
Biswas, S. K., Banerjee, S., Baker, G. W., Kuo, C., & Chowdhury, I. (2022). The Mammary Gland: Basic Structure and Molecular Signaling during Development. International Journal of Molecular Sciences, 23(7), 3883. [DOI:10.3390/ijms23073883]
Bland, K. I., Copeland, E. M., & Klimberg, V. S. (2018). Anatomy of the Breast, Axilla, Chest Wall, and Related Metastatic Sites. In Bland, K. I., Copeland, E. M., Klimberg, V. S., Gradishar, W. J., White, J., & Korourian, S. (Eds.). The Breast: Comprehensive Management of Benign and Malignant Diseases, 5th Edition (pp. 20–36.e2). Philadelphia: Elsevier. [DOI:10.1016/b978-0-323-35955-9.00002-7]
Bland, K. I., Harrison Howard, J., & Romrell, L. J. (2009). Congenital and Acquired Disturbances of Breast Development and Growth. In Bland, K. I., & Copeland, E. M. (Eds.). The Breast: Comprehensive Management of Benign and Malignant Diseases, 4th Edition (pp. 189–207). Philadelphia: Saunders/Elsevier. [Google Scholar] [Google Books] [OpenLibrary] [WorldCat]
Bondy, C. A., & Turner Syndrome Consensus Study Group. (2007). Care of girls and women with Turner syndrome: a guideline of the Turner Syndrome Study Group. The Journal of Clinical Endocrinology & Metabolism, 92(1), 10–25. [DOI:10.1210/jc.2006-1374]
Boogers, L., Infirri, S. S., Bouchareb, A., de Blok, C., Liberton, N., van Trotsenburg, P., Dreijerink, K., den Heijer, M., Wiepjes, C., & Hannema, S. (2022). The effect of timing of puberty suppression on breast development in trans girls; a cross-sectional study. Hormone Research in Paediatrics, 95(Suppl 2) [60th Annual Meeting of the European Society for Paediatric Endocrinology (ESPE), Rome, Italy, September 15–17, 2022], 390–391 (abstract no. P1-379). [Google Scholar] [DOI:10.1159/000525606] [URL] [PDF 1] [PDF 2]
Boyce, S. W., Hoffman, P. G., & Mathes, S. J. (1984). Recurrent Macromastia after Subcutaneous Mastectomy. Annals of Plastic Surgery, 13(6), 511–518. [DOI:10.1097/00000637-198412000-00008]
Bruck, H. G., & Müller, G. (1967). Zur Hormontherapie der Hypoplastischen Weiblichen Brust. [On Hormonal Therapy of the Hypoplastic Female Breast.] Ästhetische Medizin [Ästhetische Medizin : Kongreß-Organ der Deutschen Gesellschaft für die Ästhetische Medizin und ihre Grenzgebiete], 16(12), 365–366. [ISSN:0400-6755] [Google Scholar] [PubMed] [WorldCat] [PDF] [Translation]
Bryant, R., Underwood, A., Robinson, A., Stephenson, T., & Underwood, J. (1998). Determination of breast tissue composition for improved accuracy in estimating radiation doses and risks in mammographic screening. The Breast, 7(2), 95–98. [DOI:10.1016/s0960-9776(98)90064-9]
Buhimschi, C. S. (2004). Endocrinology of lactation. Obstetrics and Gynecology Clinics of North America, 31(4), 963–979. [DOI:10.1016/j.ogc.2004.08.002]
Camilletti, M. A., Abeledo-Machado, A., Faraoni, E. Y., Thomas, P., & Díaz-Torga, G. (2019). New insights into progesterone actions on prolactin secretion and prolactinoma development. Steroids, 152, 108496. [DOI:10.1016/j.steroids.2019.108496]
Çamtosun, E., Şıklar, Z., Ceylaner, S., Kocaay, P., & Berberoğlu, M. (2017). Delayed Diagnosis of a 17-Hydroxylase/17,20-Lyase Deficient Patient Presenting as a 46,XY Female: A Low Normal Potassium Level Can Be an Alerting Diagnostic Sign. Journal of Clinical Research in Pediatric Endocrinology, 9(2), 163–167. [DOI:10.4274/jcrpe.3839]
Capraro, V. J., & Dewhurst, C. J. (1975). Breast Disorders in Childhood and Adolescence. Clinical Obstetrics and Gynecology, 18(2), 25–50. [DOI:10.1097/00003081-197506000-00003]
Carlson, L. J., & Shaw, N. D. (2019). Development of Ovulatory Menstrual Cycles in Adolescent Girls. Journal of Pediatric and Adolescent Gynecology, 32(3), 249–253. [DOI:10.1016/j.jpag.2019.02.119]
Caro, T. M. (1987). Human breasts: Unsupported hypotheses reviewed. Human Evolution, 2(3), 271–282. [DOI:10.1007/bf03016112]
Ceriani, R. L. (1974). Hormones and Other Factors Controlling Growth in the Mammary Gland: A Review. Journal of Investigative Dermatology, 63(1), 93–108. [DOI:10.1111/1523-1747.ep12678104]
Cernea, R. (1944). Lokale Hormonbehandlung bei Mammaatrophie und Unterentwicklung. [Local Hormone Treatment in Mammary Atrophy and Underdevelopment.] Medizinische Klinik, 40(11/12), 169–170. [Google Scholar] [PDF] [Translation]
Chang, K., Lee, T. T., Linares-Cruz, G., Fournier, S., & de Ligniéres, B. (1995). Influences of percutaneous administration of estradiol and progesterone on human breast epithelial cell cycle in vivo. Fertility and Sterility, 63(4), 785–791. [DOI:10.1016/s0015-0282(16)57482-2]
Cheikhelard, A., Morel, Y., Thibaud, E., Lortat-Jacob, S., Jaubert, F., Polak, M., & Nihoul-Fekete, C. (2008). Long-Term Followup and Comparison Between Genotype and Phenotype in 29 Cases of Complete Androgen Insensitivity Syndrome. Journal of Urology, 180(4), 1496–1501. [DOI:10.1016/j.juro.2008.06.045]
Ciarloni, L., Mallepell, S., & Brisken, C. (2007). Amphiregulin is an essential mediator of estrogen receptor α function in mammary gland development. Proceedings of the National Academy of Sciences, 104(13), 5455–5460. [DOI:10.1073/pnas.0611647104]
Clendenen, T. V., Kim, S., Moy, L., Wan, L., Rusinek, H., Stanczyk, F. Z., Pike, M. C., & Zeleniuch-Jacquotte, A. (2013). Magnetic Resonance Imaging (MRI) of hormone-induced breast changes in young premenopausal women. Magnetic Resonance Imaging, 31(1), 1–9. [DOI:10.1016/j.mri.2012.06.022]
Cline, J. M., & Wood, C. E. (2006). Hormonal Effects on the Mammary Gland of Postmenopausal Nonhuman Primates. Breast Disease, 24(1), 59–70. [DOI:10.3233/bd-2006-24105]
Cline, J. M., & Wood, C. E. (2008). The Mammary Glands of Macaques. Toxicologic Pathology, 36(7 Suppl), 130S–141S. [DOI:10.1177/0192623308327411]
Cole, R. D., & Hopkins, T. R. (1962). A Biochemical Test of Artificial Mammogenesis and Lactogenesis As Models of the Natural Processes. Endocrinology, 70(3), 375–380. [DOI:10.1210/endo-70-3-375]
Coleman, E., Bockting, W., Botzer, M., Cohen-Kettenis, P., DeCuypere, G., Feldman, J., Fraser, L., Green, J., Knudson, G., Meyer, W. J., Monstrey, S., Adler, R. K., Brown, G. R., Devor, A. H., Ehrbar, R., Ettner, R., Eyler, E., Garofalo, R., Karasic, D. H., Lev, A. I., Mayer, G., Meyer-Bahlburg, H., Hall, B. P., Pfaefflin, F., Rachlin, K., Robinson, B., Schechter, L. S., Tangpricha, V., van Trotsenburg, M., Vitale, A., Winter, S., Whittle, S., Wylie, K. R., & Zucker, K. (2012). [World Professional Association for Transgender Health (WPATH)] Standards of Care for the Health of Transsexual, Transgender, and Gender-Nonconforming People, Version 7. International Journal of Transgenderism, 13(4), 165–232. [DOI:10.1080/15532739.2011.700873] [URL] [PDF]
Coleman, E., Radix, A. E., Bouman, W. P., Brown, G. R., de Vries, A. L., Deutsch, M. B., Ettner, R., Fraser, L., Goodman, M., Green, J., Hancock, A. B., Johnson, T. W., Karasic, D. H., Knudson, G. A., Leibowitz, S. F., Meyer-Bahlburg, H. F., Monstrey, S. J., Motmans, J., Nahata, L., … & Arcelus, J. (2022). [World Professional Association for Transgender Health (WPATH)] Standards of Care for the Health of Transgender and Gender Diverse People, Version 8. International Journal of Transgender Health, 23(Suppl 1), S1–S259. [DOI:10.1080/26895269.2022.2100644] [URL] [PDF]
Coltman, C. E., Steele, J. R., & McGhee, D. E. (2017). Breast volume is affected by body mass index but not age. Ergonomics, 60(11), 1576–1585. [DOI:10.1080/00140139.2017.1330968]
Colvin, C., Devineni, G., & Ashraf, A. P. (2014). Delayed Puberty. In Bandeira, F., Gharib, H., Golbert, A., Griz, L., & Faria, M. (Eds.). Endocrinology and Diabetes (pp. 203–217). New York: Springer. [DOI:10.1007/978-1-4614-8684-8_17]
Cowie, A. T., & Folley, S. J. (1961). The Mammary Gland and Lactation. In Young, W. C. (Ed.). Sex and Internal Secretions, 3rd Edition, Volume I (pp. 590–642). Baltimore: Williams & Wilkins. [Google Scholar] [Google Books] [OpenLibrary] [WorldCat] [Archive.org]
Cowie, A. T., Forsyth, I. A., & Hart, I. C. (1980). Growth and Development of the Mammary Gland. In Cowie, A. T., Forsyth, I. A., & Hart, I. C. Hormonal Control of Lactation (Monographs on Endocrinology, Volume 15) (pp. 58–145). Berlin/Heidelberg: Springer Berlin Heidelberg. [DOI:10.1007/978-3-642-81389-4_3]
Cox, D. B., Kent, J. C., Casey, T. M., Owens, R. A., & Hartmann, P. E. (1999). Breast Growth and the Urinary Excretion of Lactose During Human Pregnancy and Early Lactation: Endocrine Relationships. Experimental Physiology, 84(2), 421–434. [DOI:10.1111/j.1469-445x.1999.01807.x]
Cox, C. B., Kent, J. C., Owens, R., & Hartmann, P. E. (1994). Mammary morphological and functional changes during pregnancy in women. In Thompson, J. (Ed.). Proceedings of the Twenty-Sixth Annual Conference, Hilton Hotel, Brisbane, 26–28 September, 1994 [The Australian Society for Reproductive Biology Inc., Twenty Sixth Annual Conference, The Hilton Hotel, Brisbane, September 26 - 28 1994, Programme and Miniposters of Papers] (pp. 47–47). Australia: Australian Society for Reproductive Biology. [Google Scholar] [WorldCat] [URL] [PDF]
Coxon, J., & Seal, L. (2018). Hormone management of trans women. Trends in Urology & Men’s Health, 9(6), 10–14. [DOI:10.1002/tre.663]
Cregan, M. D., & Hartmann, P. E. (1999). Computerized Breast Measurement from Conception to Weaning: Clinical Implications. Journal of Human Lactation, 15(2), 89–96. [DOI:10.1177/089033449901500202]
Crowley, W. F., & Pitteloud, N. (2020). Approach to the patient with delayed puberty. UpToDate. [Google Scholar] [URL]
Cruz-Korchin, N., Korchin, L., González-Keelan, C., Climent, C., & Morales, I. (2002). Macromastia. Plastic and Reconstructive Surgery, 109(1), 64–68. [DOI:10.1097/00006534-200201000-00011]
Curtis, R. J. (2009 July 10). The Lowdown on Progesterone. London: The London Gender Clinic. [Google Scholar] [URL] [PDF]
Dallmann, A., Ince, I., Meyer, M., Willmann, S., Eissing, T., & Hempel, G. (2017). Gestation-Specific Changes in the Anatomy and Physiology of Healthy Pregnant Women: An Extended Repository of Model Parameters for Physiologically Based Pharmacokinetic Modeling in Pregnancy. Clinical Pharmacokinetics, 56(11), 1303–1330. [DOI:10.1007/s40262-017-0539-z]
Dancey, A., Khan, M., Dawson, J., & Peart, F. (2008). Gigantomastia – a classification and review of the literature. Journal of Plastic, Reconstructive & Aesthetic Surgery, 61(5), 493–502. [DOI:10.1016/j.bjps.2007.10.041]
Davajan, V., & Kletzky, O. A. (1979). Amenorrhea without Galactorrhea or Hirsutism. In Mishell, D. R., & Davajan, V. (Eds.). Reproductive Endocrinology, Infertility, and Contraception (pp. 219–248). Philadelphia: F. A. Davis Co. [Google Scholar] [Google Books] [OpenLibrary] [WorldCat] [Archive.org]
Davis, M. E., Boynton, M. W., Ferguson, J. H., & Rothman, S. (1945). Studies on Pigmentation of Endocrine Origin. The Journal of Clinical Endocrinology & Metabolism, 5(3), 138–146. [DOI:10.1210/jcem-5-3-138]
de Blok, C. J., Dijkman, B. A., Wiepjes, C. M., Staphorsius, A. S., Timmermans, F. W., Smit, J. M., Dreijerink, K. M., & den Heijer, M. (2021). Sustained Breast Development and Breast Anthropometric Changes in 3 Years of Gender-Affirming Hormone Treatment. The Journal of Clinical Endocrinology & Metabolism, 106(2), e782–e790. [DOI:10.1210/clinem/dgaa841]
de Blok, C. J., Klaver, M., Wiepjes, C. M., Nota, N. M., Heijboer, A. C., Fisher, A. D., Schreiner, T., T’Sjoen, G., & den Heijer, M. (2017). Breast Development in Transwomen After 1 Year of Cross-Sex Hormone Therapy: Results of a Prospective Multicenter Study. The Journal of Clinical Endocrinology & Metabolism, 103(2), 532–538. [DOI:10.1210/jc.2017-01927]
de Lignières, B. (2002). Effects of progestogens on the postmenopausal breast. Climacteric, 5(3), 229–235. [DOI:10.1080/cmt.5.3.229.235]
de Lignières, B., & Mauvais-Jarvis, P. (1981). Hormonal Dependence of Benign Breast Disease, Gynecomastia and Breast Cancer. In Hollman, K. H., Brux, J., & Verley, J. M. (Eds.). New Frontiers in Mammary Pathology (pp. 287–308). Boston: Springer US. [DOI:10.1007/978-1-4757-0019-0_17]
de Vries, A. L., Steensma, T. D., Wagemaar, E. C. F., Doreleijers, T. A., & Cohen-Kettenis, P. T. (2010). Puberty suppression followed by cross-sex hormones and gender reassignment surgery: A prospective follow-up of gender dysphoric adolescents into adulthood. In de Vries, A. L. (Ed.). Gender Dysphoria in Adolescents: Mental Health and Treatment Evaluation (pp. 91–106). (Doctoral thesis, Vrije Universiteit Amsterdam.) [Google Scholar] [URL] [PDF]
Deeb, A., Al Suwaidi, H., Attia, S., & Al Ameri, A. (2015). 17-hydroxylase/17,20-lyase deficiency due to a R96Q mutation causing hypertension and poor breast development. Endocrinology, Diabetes & Metabolism Case Reports, 2015(1), 15-0069. [DOI:10.1530/EDM-15-0069]
Deepinder, F., & Braunstein, G. D. (2012). Drug-induced gynecomastia: an evidence-based review. Expert Opinion on Drug Safety, 11(5), 779–795. [DOI:10.1517/14740338.2012.712109]
Dennerstein, L., Burrows, G. D., Hyman, G. J., & Sharpe, K. (1980). Some clinical effects of oestrogen-progestogen therapy in surgically castrated women. Maturitas, 2(1), 19–28. [DOI:10.1016/0378-5122(80)90056-0]
Dewhurst, C. J. (1971). Sex Chromosome Abnormalities and the Gynaecologist. BJOG, 78(12), 1058–1076. [DOI:10.1111/j.1471-0528.1971.tb00227.x]
Dewhurst, C. J. (1971). The XY female. American Journal of Obstetrics and Gynecology, 109(5) [Transactions of the Eighty-First Annual Meeting of the American Association of Obstetricians and Gynecologists], 675–688. [DOI:10.1016/0002-9378(71)90753-8]
Dewhurst, C. (1972). Amenorrhoea and the Paediatrician. Pediatric Clinics of North America, 19(3), 605–618. [DOI:10.1016/s0031-3955(16)32741-9]
Dewhurst, C. J., & Spence, J. E. (1977). The XY female. British Journal of Hospital Medicine, 17(5), 498, 501–506. [Google Scholar] [PubMed] [PDF]
Dewhurst, J. (1981). Breast Disorders in Children and Adolescents. Pediatric Clinics of North America, 28(2), 287–308. [DOI:10.1016/s0031-3955(16)33997-9]
Dewhurst, J. (1982). Breast Hypoplasia. In Bruni, V., Gasparri, F., Dewhurst, J., & Rey-Stocker, I. (Eds.). Pediatric and Adolescent Gynaecology [Proceedings of the IVth International Symposium, Florence, October 5-7, 1978] (pp. 205–212). Rome, Italy: Serono Symposia. [Google Scholar] [Google Books] [WorldCat] [PDF]
Di Lorenzo, G., Autorino, R., Perdonà, S., & De Placido, S. (2005). Management of gynaecomastia in patients with prostate cancer: a systematic review. The Lancet Oncology, 6(12), 972–979. [DOI:10.1016/s1470-2045(05)70464-2]
Dickson, L. M., & Hewer, E. E. (1950). The structure of the breast. In Saner, F. D. (Ed.). The Breast: Structure, Function, Disease (pp. 1–52). Baltimore: William & Wilins. [Google Scholar] [Google Books] [OpenLibrary] [WorldCat] [URL] [PDF]
Dijkman, B. A., Blok, C. J., Dreijerink, K. M., & den Heijer, M. (2023). Progestin-related breast volume changes in a woman with complete androgen insensitivity syndrome (CAIS). Endocrinology, Diabetes & Metabolism Case Reports, 2023(2), 22-0346. [DOI:10.1530/edm-22-0346]
Dijkman, B. A., Helder, D., Boogers, L. S., Gieles, N. C., van Heesewijk, J. O., Slaa, S. t., Liberton, N. P., Wiepjes, C. M., de Blok, C. J., den Heijer, M., & Dreijerink, K. M. (2023). Addition of progesterone to feminizing gender-affirming hormone therapy in transgender individuals for breast development: a randomized controlled trial. BMC Pharmacology and Toxicology, 24(1), 80. [DOI:10.1186/s40360-023-00724-4]
Dittrich, R., Binder, H., Cupisti, S., Hoffmann, I., Beckmann, M., & Mueller, A. (2005). Endocrine Treatment of Male-to-Female Transsexuals Using Gonadotropin-Releasing Hormone Agonist. Experimental and Clinical Endocrinology & Diabetes, 113(10), 586–592. [DOI:10.1055/s-2005-865900]
Donaldson, M., Kriström, B., Ankarberg-Lindgren, C., Verlinde, S., van Alfen-van der Velden, J., Gawlik, A., van Gelder, M., Sas, T., & (2019). Optimal Pubertal Induction in Girls with Turner Syndrome Using Either Oral or Transdermal Estradiol: A Proposed Modern Strategy. Hormone Research in Paediatrics, 91(3), 153–163. [DOI:10.1159/000500050]
Dorgan, J. F., Klifa, C., Deshmukh, S., Egleston, B. L., Shepherd, J. A., Kwiterovich, P. O., Van Horn, L., Snetselaar, L. G., Stevens, V. J., Robson, A. M., Lasser, N. L., & Hylton, N. M. (2013). Menstrual and reproductive characteristics and breast density in young women. Cancer Causes & Control, 24(11), 1973–1983. [DOI:10.1007/s10552-013-0273-2]
Döring, G. K. (1963). Über die relative Häufigkeit des anovulatorischen Cyclus im Leben der Frau. [On the relative frequency of the anovulatory cycle in women’s lives.] Archiv für Gynäkologie, 199(2), 115–123. [DOI:10.1007/bf00668062]
Drąsutis, J. (2017). Changes in breast morphological parameters, body size and shape, blood serum prolactin and lipids during pregnancy, multiple relationships of these indicators and morphological markers for health risk. (Doctoral dissertation, Vilniaus Universitetas.) [Google Scholar] [URL]
Drife, J. O. (1982). The effects of parity and the menstrual cycle on the normal mammary gland and their possible relationship to malignant change. (Doctoral dissertation, University of Edinburgh). [Google Scholar] [Google Books] [WorldCat] [URL] [PDF]
Drife, J. O. (1984). The pill and the breast. IPPF Medical Bulletin, 18(6), 1–2. [Google Scholar] [PubMed]
Drife, J. O. (1986). Breast Development in Puberty. Annals of the New York Academy of Sciences, 464(1) [Endocrinology of the Breast: Basic and Clinical Aspects], 58–65. [DOI:10.1111/j.1749-6632.1986.tb15993.x]
Drife, J. O. (1989). Breast modifications during the menstrual cycle. Supplement to International Journal of Gynecology and Obstetrics, 1, 19–24. / International Journal of Gynecology and Obstetrics, 1989(Suppl 1), 19–24. [Google Scholar] [PubMed] [Archive.org]
Drife, J. O. (1990). Premenopausal Hormone Therapy. In Drife, J. O., & Studd, J. W. W. (Eds.). HRT and Osteoporosis (pp. 351–362). London: Springer London. [DOI:10.1007/978-1-4471-1799-5_25]
Duncan, M. (2010). Sexual Selection and Human Breast Morphology. (Doctoral dissertation, Te Herenga Waka-Victoria University of Wellington.) [Google Scholar] [URL]
Edmonds, D. K. (1989). Normal Puberty. In Edmonds, D. K. Dewhurst’s Practical Paediatric and Adolescent Gynaecology, 2nd Edition (pp. 56–62). London: Butterworths. [Google Scholar] [Google Books] [OpenLibrary] [WorldCat] [URL] [Archive.org]
Elling, S. V., & Powell, F. C. (1997). Physiological changes in the skin during pregnancy. Clinics in Dermatology, 15(1), 35–43. [DOI:10.1016/s0738-081x(96)00108-3]
Engman, M., Skoog, L., Soderqvist, G., & Gemzell-Danielsson, K. (2008). The effect of mifepristone on breast cell proliferation in premenopausal women evaluated through fine needle aspiration cytology. Human Reproduction, 23(9), 2072–2079. [DOI:10.1093/humrep/den228]
Federici, S., Goggi, G., Quinton, R., Giovanelli, L., Persani, L., Cangiano, B., & Bonomi, M. (2021). New and Consolidated Therapeutic Options for Pubertal Induction in Hypogonadism: In-depth Review of the Literature. Endocrine Reviews, 43(5), 824–851. [DOI:10.1210/endrev/bnab043]
Fernández-Cancio, M., García-García, E., González-Cejudo, C., Martínez-Maestre, M., Mangas-Cruz, M., Guerra-Junior, G., Pandi de Mello, M., Arnhold, I. J., Nishi, M. Y., Bilharinho Mendonça, B., García-Arumí, E., Audí, L., Tizzano, E., & Carrascosa, A. (2017). Discordant Genotypic Sex and Phenotype Variations in Two Spanish Siblings with 17α-Hydroxylase/17,20-Lyase Deficiency Carrying the Most Prevalent Mutated CYP17A1 Alleles of Brazilian Patients. Sexual Development, 11(2), 70–77. [DOI:10.1159/000468160]
Fernandez-Valdivia, R., Mukherjee, A., Mulac-Jericevic, B., Conneely, O. M., DeMayo, F. J., Amato, P., & Lydon, J. P. (2005). Revealing Progesterone’s Role in Uterine and Mammary Gland Biology: Insights from the Mouse. Seminars in Reproductive Medicine, 23(1), 22–37. [DOI:10.1055/s-2005-864031]
Finkenzeller, D. A., & Loveless, M. B. (2007). Pediatric Gynecology. In Fortner, K. B., Szymanski, L. M., Fox, H. E., & Wallach, E. E. (Eds.). The Johns Hopkins Manual of Gynecology and Obstetrics, 3rd Edition (Spiral Manual Series) (pp. 363–379). Philadelphia: Lippincott Williams & Wilkins. [Google Scholar] [Google Books] [OpenLibrary] [WorldCat]
Fisher, A. D., Castellini, G., Ristori, J., Casale, H., Cassioli, E., Sensi, C., Fanni, E., Amato, A. M., Bettini, E., Mosconi, M., Dèttore, D., Ricca, V., & Maggi, M. (2016). Cross-Sex Hormone Treatment and Psychobiological Changes in Transsexual Persons: Two-Year Follow-Up Data. The Journal of Clinical Endocrinology & Metabolism, 101(11), 4260–4269. [DOI:10.1210/jc.2016-1276]
Foidart, J. M., Colin, C., Denoo, X., Desreux, J., Fournier, S., & de Linières, B. (1996). Influence of percutaneous administration of estradiol and progesterone on the proliferation of human breast epithelial cells. In Calvo, F., Crépin, M., & Magdelenat, H. (Eds.). Breast Cancer: Advances in Biology and Therapeutics [21st Meeting of the International Association for Breast Cancer Research, July 3-4-5, 1996, Paris] (pp. 329–334). Montrouge/Paris: John Libbey Eurotext. [Google Scholar] [Google Books] [OpenLibrary] [WorldCat]
Foidart, J., Colin, C., Denoo, X., Desreux, J., Béliard, A., Fournier, S., & de Lignières, B. (1998). Estradiol and Progesterone Regulate the Proliferation of Human Breast Epithelial Cells. Fertility and Sterility, 69(5), 963–969. [DOI:10.1016/s0015-0282(98)00042-9]
Folley, S. J. (1947). Endocrine Control of the Mammary Gland. British Medical Bulletin, 5(2–3), 130–134. [DOI:10.1093/oxfordjournals.bmb.a073121]
Folley, S. J. (1950). Lactational Physiology. In Bowes, K. (Ed.). Modern Trends in Obstetrics and Gynaecology (pp. 441–453). London: Butterworth. [Google Scholar] [Google Books] [OpenLibrary] [WorldCat] [PDF]
Folley, S. J. (1952). Lactation. In Parkes, A. S. (Ed.). Marshall’s Physiology of Reproduction, 3rd Edition, Volume II (pp. 525–647). Longmans, Green & Co.: London. [Google Scholar] [Google Books] [OpenLibrary] [WorldCat] [PDF]
Folley, S. J. (1956). Recent Studies on the Development of the Mammary Gland. In Folley, S. J. The Physiology and Biochemistry of Lactation, 1st Edition (pp. 1–22). Edinburgh: Oliver & Boyd. [Google Scholar] [Google Books] [OpenLibrary] [WorldCat]
Folley, S. J., & Malpress, F. H. (1948). Hormonal Control of Mammary Growth. In Pincus, G., & Thimann, K. V. (Eds.). The Hormones: Physiology, Chemistry and Applications, Volume I (pp. 695–743). New York: Academic Press. [Google Scholar] [Google Books] [OpenLibrary] [WorldCat] [PDF]
Fourcade, R., & McLeod, D. (2004). Tolerability of Antiandrogens in the Treatment of Prostate Cancer. UroOncology, 4(1), 5–13. [DOI:10.1080/1561095042000191655]
Fowler, P. A., Casey, C. E., Cameron, G. G., Foster, M. A., & Knight, C. H. (1990). Cyclic changes in composition and volume of the breast during the menstrual cycle, measured by magnetic resonance imaging. BJOG, 97(7), 595–602. [DOI:10.1111/j.1471-0528.1990.tb02546.x]
Fridriksdottir, A. J., Petersen, O. W., & Rnnov-Jessen, L. (2011). Mammary gland stem cells: current status and future challenges. The International Journal of Developmental Biology, 55(7–8–9), 719–729. [DOI:10.1387/ijdb.113373af]
Fuqua, J. S., & Eugster, E. A. (2022). History of Puberty: Normal and Precocious. Hormone Research in Paediatrics, 95(6), 568–578. [DOI:10.1159/000526464]
Gaede, P., Trolle, D., & Pedersen, H. (1978). Extremely low placental lactogen hormone (hpl) values in an otherwise uneventful pregnancy preceding delivery of a normal baby. Acta Obstetricia et Gynecologica Scandinavica, 57(3), 203–209. [DOI:10.3109/00016347809154883]
Galani, A., Kitsiou-Tzeli, S., Sofokleous, C., Kanavakis, E., & Kalpini-Mavrou, A. (2008). Androgen insensitivity syndrome: clinical features and molecular defects. Hormones, 7(3), 217–229. [DOI:10.14310/horm.2002.1201]
Galbarczyk, A. (2011). Unexpected changes in maternal breast size during pregnancy in relation to infant sex: An evolutionary interpretation. American Journal of Human Biology, 23(4), 560–562. [DOI:10.1002/ajhb.21177]
Gawlik, A., Hankus, M., Such, K., Drosdzol-Cop, A., Madej, P., Borkowska, M., Zachurzok, A., & Malecka-Tendera, E. (2016). Hypogonadism and Sex Steroid Replacement Therapy in Girls with Turner Syndrome. Journal of Pediatric and Adolescent Gynecology, 29(6), 542–550. [DOI:10.1016/j.jpag.2016.03.005]
Gershon-Cohen, J. (1970). The Normal Breast. In Gershon-Cohen, J. Atlas of Mammography (pp. 23–38). Berlin/Heidelberg: Springer. [DOI:10.1007/978-3-642-85678-5_4] [Google Books]
Gertig, D. M., Stillman, I. E., Byrne, C., Spiegelman, D., Schnitt, S. J., Connolly, J. L., Colditz, G. A., & Hunter, D. J. (1999). Association of age and reproductive factors with benign breast tissue composition. Cancer Epidemiology, Biomarkers & Prevention, 8(10), 873–879. [Google Scholar] [PubMed] [URL]
Geschickter, C. F. (1945). Endocrine Physiology of the Breast. In Geschickter, C. F. Diseases of the Breast: Diagnosis, Pathology, Treatment, 2nd Edition (pp. 42–81). Philadelphia: J.B. Lippincott. [Google Scholar] [Google Books] [OpenLibrary] [WorldCat] [PDF]
Glenn, J. F. (1976). Testicular feminization syndrome current clinical considerations. Urology, 7(6), 569–577. [DOI:10.1016/0090-4295(76)90079-0]
Gliosci, A., & Presutti, F. (1993). Virginal gigantomastia: Validity of combined surgical and hormonal treatments. Aesthetic Plastic Surgery, 17(1), 61–65. [DOI:10.1007/bf00455051]
Gompel, A., & Plu-Bureau, G. (2018). Progesterone, progestins and the breast in menopause treatment. Climacteric, 21(4), 326–332. [DOI:10.1080/13697137.2018.1476483]
Goodman, H. M. (2009). Hormonal Control of Pregnancy and Lactation. In Goodman, H. M. Basic Medical Endocrinology, 4th Edition (pp. 277–301). Amsterdam: Academic Press/Elsevier. [DOI:10.1016/b978-0-12-373975-9.00014-8]
Gooren, L. J. (2016). Hormone Treatment of Adult Transgender People. In Ettner, R., Monstrey, S., & Coleman, E. (Eds.). Principles of Transgender Medicine and Surgery, 2nd Edition (pp. 167–179). New York: Routledge. [Google Scholar] [Google Books] [DOI:10.4324/9781315718972-11]
Gordon, C. M., & Laufer, M. R. (2005) The Physiology of Puberty. In Emans, S. J., Laufer, M. R., & Goldstein, D. P. (Eds.). Pediatric and Adolescent Gynecology, 5th Edition (pp. 120–155). Philadelphia: Lippincott Williams & Wilkins. [Google Scholar] [Google Books] [OpenLibrary] [WorldCat] [Archive.org]
Göretzlehner, G. & Lauritzen, C. (1992). Hormontherapie bei Gynäkologischen Erkrankungen [Hormone Therapy for Gynecological Diseases]. In Göretzlehner, G. & Lauritzen, C. Praktische Hormontherapie in der Gynäkologie, 1. Auflage [Practical Hormone Therapy in Gynecology, 1st Edition] (pp. 245–299). Berlin/New York: de Gruyter. [DOI:10.1515/9783112417706-007] [Google Books] [PDF] [Translation]
Graham, J. D., & Clarke, C. L. (1997). Physiological Action of Progesterone in Target Tissues. Endocrine Reviews, 18(4), 502–519. [DOI:10.1210/edrv.18.4.0308]
Graham, S. J., Stanchev, P. L., Lloyd‐Smith, J. O., Bronskill, M. J., & Plewes, D. B. (1995). Changes in Fibroglandular Volume and Water Content of Breast Tissue During the Menstrual Cycle Observed by MR Imaging at 1.5 T. Journal of Magnetic Resonance Imaging, 5(6), 695–701. [DOI:10.1002/jmri.1880050613]
Greydanus, D. E., Omar, H. A., Matytsina, L. A., & Tsitsika, A. (2010). Breast Disorders in Children and Adolescents. In Omar, H. A., Greydanus, D. E., Tsitsika, A. K., Patel, D. R., & Merrick, J. (Eds.). Pediatric and Adolescent Sexuality and Gynecology: Principles for the Primary Care Clinician (pp. 245–316). Hauppauge: Nova Science Publishers. [Google Scholar] [Google Books] [URL] [OpenLibrary] [WorldCat] [PDF]
Guaragna-Filho, G., Guerra-Junior, G., Tadokoro-Cuccaro, R., Hughes, I. A., Barros, B. A., Hiort, O., Balsamo, A., Guran, T., Holterhus, P. M., Hannema, S., Poyrazoglu, S., Darendeliler, F., Bryce, J., Ahmed, S. F., & Quigley, C. A. (2023). Pubertal and Gonadal Outcomes in 46,XY Individuals with Partial Androgen Insensitivity Syndrome Raised as Girls. Sexual Development, 17(1), 16–25. [DOI:10.1159/000526997]
Gunn, H. M., Tsai, M., McRae, A., & Steinbeck, K. S. (2018). Menstrual Patterns in the First Gynecological Year: A Systematic Review. Journal of Pediatric and Adolescent Gynecology, 31(6), 557–565.e6. [DOI:10.1016/j.jpag.2018.07.009]
Günzel, P., Hasan, S. H., Düsterberg, B., Hümpel, M., Putz, B., & Lehmann, M. (1987). Zur toxikologischen Prüfung von Steroidhormonen. [For the Toxicological Testing of Steroid Hormones.] In Burger, O. K., Grosdanoff, P., Henschler, D., Kraupp, O., & Schnieders, B. (Eds.). Aktuelle Probleme der Biomedizin (pp. 93–112). Berlin/New York: De Gruyter. [Google Scholar] [Google Books] [DOI:10.1515/9783110898231-014]
Hagisawa, S., Shimura, N., & Arisaka, O. (2012). Effect of Excess Estrogen on Breast and External Genitalia Development in Growth Hormone Deficiency. Journal of Pediatric and Adolescent Gynecology, 25(3), e61–e63. [DOI:10.1016/j.jpag.2011.11.005]
Hamburger, C., & Benjamin, H. (1969). Endocrine Treatment of Male and Female Transsexualism / Appendix for the Practicing Physician: Suggestions and Guidelines for the Management of Transsexuals. In Green, R., & Money, J. (Eds.). Transsexualism and Sex Reassignment (pp. 291–307). Baltimore: John Hopkins University Press. [Google Scholar] [Google Books] [PDF]
Hannan, F. M., Elajnaf, T., Vandenberg, L. N., Kennedy, S. H., & Thakker, R. V. (2022). Hormonal regulation of mammary gland development and lactation. Nature Reviews Endocrinology, 19(1), 46–61. [DOI:10.1038/s41574-022-00742-y]
Hannema, S. E., Schagen, S. E., Cohen-Kettenis, P. T., & Delemarre-van de Waal, H. A. (2017). Efficacy and Safety of Pubertal Induction Using 17β-Estradiol in Transgirls. The Journal of Clinical Endocrinology & Metabolism, 102(7), 2356–2363. [DOI:10.1210/jc.2017-00373]
Hartmann, B. W., Laml, T., Albrecht, A. E., Huber, J. C., & Kirchengast, S. (1998). Hormonal Breast Augmentation: Prognostic Relevance of Insulin-Like Growth Factor-I. Gynecological Endocrinology, 12(2), 123–127. [DOI:10.3109/09513599809024960]
Hartmann, P. E., Owens, R. A., Cox, D. B., & Kent, J. C. (1996). Breast Development and Control of Milk Synthesis. Food and Nutrition Bulletin, 17(4), 1–12. [DOI:10.1177/156482659601700404]
Hasan, S. (1974). Steroid Hormone Levels During Pregnancy in Various Species. In Bernhard, S., & Raspé, G. (Ed.). Hormones and Embryonic Development (Advances in the Biosciences, Volume 13) (pp. 181–197). Oxford/New York: Pergamon Press. [Google Scholar] [Google Books] [DOI:10.1016/b978-0-08-018239-1.50014-3] [OpenLibrary] [Archive.org]
Hassiotou, F., & Geddes, D. (2012). Anatomy of the human mammary gland: Current status of knowledge. Clinical Anatomy, 26(1), 29–48. [DOI:10.1002/ca.22165]
Heath, R. A., & Wynne, K. (2019). Children and Adolescents. In Heath, R. A., & Wynne, K. A Guide to Transgender Health: State-of-the-art Information for Gender-Affirming People and Their Supporters (pp. 87–106). Santa Barbara: Praeger/ABC-CLIO. [Google Books]
Heath, R. A., & Wynne, K. (2019). Hormone and Surgical Therapies for Adults. In Heath, R. A., & Wynne, K. A Guide to Transgender Health: State-of-the-art Information for Gender-Affirming People and Their Supporters (pp. 107–146). Santa Barbara: Praeger/ABC-CLIO. [Google Books]
Hertz, R., Odell, W. D., & Ross, G. T. (1966). Diagnostic Implications of Primary Amenorrhea: Combined Clinical Staff Conference at the National Institutes of Health. Annals of Internal Medicine, 65(4), 800–820. [DOI:10.7326/0003-4819-65-4-800]
Hillard, P. J. A. (2007). Benign Diseases of the Female Reproductive Tract. In Berek, J. S., & Novak, E. (Eds.). Berek & Novak’s Gynecology, 14th Edition (pp. 431–496). Philadelphia: Lippincott Williams and Wilkins. [Google Scholar] [OpenLibrary] [WorldCat] [Archive.org]
Hoppe, I. C., Patel, P. P., Singer-Granick, C. J., & Granick, M. S. (2011). Virginal Mammary Hypertrophy: A Meta-Analysis and Treatment Algorithm. Plastic and Reconstructive Surgery, 127(6), 2224–2231. [DOI:10.1097/prs.0b013e3182131bd1]
Hovey, R. C., Trott, J. F., Ginsburg, E., Goldhar, A., Sasaki, M. M., Fountain, S. J., Sundararajan, K., & Vonderhaar, B. K. (2001). Transcriptional and spatiotemporal regulation of prolactin receptor mRNA and cooperativity with progesterone receptor function during ductal branch growth in the mammary gland. Developmental Dynamics, 222(2), 192–205. [DOI:10.1002/dvdy.1179]
Howard, B. A., & Gusterson, B. A. (2000). Human Breast Development. Journal of Mammary Gland Biology and Neoplasia, 5(2), 119–137. [DOI:10.1023/a:1026487120779]
Huffman, J., Dewhurst, C. J., & Capraro, V. J. (1981). The Breast and its Disorders in Childhood and Adolescence. In Huffman, J., Dewhurst, J., & Capraro, V. The Gynecology of Childhood and Adolescence, 2nd Edition (pp. 542–559). Philadelphia: Saunders. [Google Scholar] [Google Books] [OpenLibrary] [WorldCat] [Archive.org] [PDF]
Hussain, Z., Brooks, J., & Percy, D. (2008). Menstrual variation of breast volume and T2 relaxation times in cyclical mastalgia. Radiography, 14(1), 8–16. [DOI:10.1016/j.radi.2006.07.003]
Hussain, Z., Roberts, N., Whitehouse, G. H., García-Fiñana, M., & Percy, D. (1999). Estimation of breast volume and its variation during the menstrual cycle using MRI and stereology. The British Journal of Radiology, 72(855), 236–245. [DOI:10.1259/bjr.72.855.10396212]
Hutson, S. W., Cowen, P. N., & Bird, C. C. (1985). Morphometric studies of age related changes in normal human breast and their significance for evolution of mammary cancer. Journal of Clinical Pathology, 38(3), 281–287. [DOI:10.1136/jcp.38.3.281]
Hytten, F. E. (1954). Clinical and Chemical Studies in Human Lactation–VI. BMJ, 1(4867), 912–915. [DOI:10.1136/bmj.1.4867.912]
Hytten, F. E. (1976). The physiology of lactation. International Journal of Food Sciences and Nutrition, 30(4), 225–232. [DOI:10.3109/09637487609142745]
Hytten, F. E., & Baird, D. (1958). The Development of the Nipple in Pregnancy. The Lancet, 271(7032), 1201–1204. [DOI:10.1016/s0140-6736(58)91908-1]
Hytten, F. E., & Leitch, I. (1971). Preparations for Breast Feeding. In Hytten, F. E., & Leitch, I. The Physiology of Human Pregnancy, 2nd Edition (pp. 234–241). Oxford: Blackwell Scientific Publications. [Google Scholar] [Google Books] [OpenLibrary] [WorldCat] [Archive.org]
Hytten, F. E., & Leitch, I. (1971). Preparations for Breast Feeding. In Hytten, F. E., & Leitch, I. The Physiology of Human Pregnancy, 2nd Edition (pp. 234–241). Oxford: Blackwell Scientific Publications. [Google Scholar] [Google Books] [OpenLibrary] [WorldCat] [Archive.org]
Hytten, F. E., & Thomson, A. M. (1965). Pregnancy, childbirth and lactation. In Edholm, O. G., & Bacharach, A. L. (Eds.). The Physiology of Human Survival (pp. 327–350). London/New York: Academic Press. [Google Scholar] [Google Books] [OpenLibrary] [WorldCat] [Archive.org]
Hytten, F. E., & Thomson, A. M. (1968). Maternal physiological adjustments. In Assali, N. S. (Ed.). The Maternal Organism, Volume I (Biology of Gestation) (pp. 449–479). New York: Academic Press. [Google Scholar] [Google Books] [WorldCat]
Igo, J., & Visram, H. (2021). Progesterone Therapy Use and Safety in Male to Female Transgender Patients. Canadian Journal of Diabetes, 45(7 Suppl), S39–S39 (abstract no. 109). [DOI:10.1016/j.jcjd.2021.09.119] [URL] [PDF]
Ingleby, H. (1949). Changes in breast volume in a group of normal young women. Bulletin of the International Association of Medical Museums, 29, 87–92. [Google Scholar] [Google Books] [HathiTrust]
Ingleby, H., Moore, L., & Gershon-Cohen, J. (1957). Gestational breast changes: x-ray studies of the human breast. Obstetrics & Gynecology, 10(2), 149–157. [Google Scholar] [PubMed] [URL]
Ismail, P. M., Amato, P., Soyal, S. M., DeMayo, F. J., Conneely, O. M., O’Malley, B. W., & Lydon, J. P. (2003). Progesterone involvement in breast development and tumorigenesis—as revealed by progesterone receptor “knockout” and “knockin” mouse models. Steroids, 68(10–13), 779–787. [DOI:10.1016/s0039-128x(03)00133-8]
Iwamoto, S. J., Defreyne, J., Rothman, M. S., Van Schuylenbergh, J., Van de Bruaene, L., Motmans, J., & T’Sjoen, G. (2019). Health considerations for transgender women and remaining unknowns: a narrative review. Therapeutic Advances in Endocrinology and Metabolism, 10, 204201881987116. [DOI:10.1177/2042018819871166]
Jacobsohn, D. (1961). Hormonal Regulation of Mammary Gland Growth. In Kon, S. K., & Cowie, A. T. (Eds.). Milk: The Mammary Gland and Its Secretion, Volume 1 (pp. 127–160). New York: Academic Press. [Google Scholar] [Google Books] [OpenLibrary] [WorldCat] [PDF]
Jain, J., Kwan, D., & Forcier, M. (2019). Medroxyprogesterone Acetate in Gender-Affirming Therapy for Transwomen: Results From a Retrospective Study. The Journal of Clinical Endocrinology & Metabolism, 104(11), 5148–5156. [DOI:10.1210/jc.2018-02253]
Jamal, N., Ng, K., McLean, D., Looi, L., & Moosa, F. (2004). Mammographic Breast Glandularity in Malaysian Women: Data Derived from Radiography. American Journal of Roentgenology, 182(3), 713–717. [DOI:10.2214/ajr.182.3.1820713]
Jemstrom, H., & Olsson, H. (1997). Breast Size in Relation to Endogenous Hormone Levels, Body Constitution, and Oral Contraceptive Use in Healthy Nulligravid Women Aged 19-25 Years. American Journal of Epidemiology, 145(7), 571–580. [DOI:10.1093/oxfordjournals.aje.a009153]
Jernström, H., Sandberg, T., Bågeman, E., Borg, Å., & Olsson, H. (2005). Insulin-like growth factor-1 (IGF1) genotype predicts breast volume after pregnancy and hormonal contraception and is associated with circulating IGF-1 levels: implications for risk of early-onset breast cancer in young women from hereditary breast cancer families. British Journal of Cancer, 92(5), 857–866. [DOI:10.1038/sj.bjc.6602389]
Jeruss, J. S. (2006). Molecular Basis of Breast Cancer. In Winchester, D. J., Winchester, D. P., Hudis, C. A., & Norton, L. (Eds.). Breast Cancer, 2nd Edition (pp. 83–95). Hamilton: B.C. Decker. [Google Scholar] [Google Books] [WorldCat]
Johnson, M. C., & Cutler, M. L. (2016). Anatomy and Physiology of the Breast. In Jatoi, I., & Rody, A. (Eds.). Management of Breast Diseases (pp. 1–39). Cham: Springer. [DOI:10.1007/978-3-319-46356-8_1]
Kaiser, R. (1993). Gestagen-Östrogen-Kombinationen in der Gynäkologie. Zur Geschichte, Dosierung und Anwendung eines Hormonprinzips. [Gestagen-Oestrogen Combinations in Gynaecology. History, Dosage and Use of a Hormonal Principle.] Geburtshilfe und Frauenheilkunde, 53(7), 503–513. [Google Scholar] [PubMed] [DOI:10.1055/s-2007-1022924]
Kaiser, R., & Leidenberger, F. (1991). Hormonbehandlung bei Benign Mammaerkrankungen: Mammahypoplasie. [Hormonal Treatment in Benign Breast Diseases: Breast Hypoplasia.] In Kaiser, R., & Leidenberger, F. Hormonbehandlung in der Gynäkologischen Praxis, 7. Auflage [Hormone Treatment in Gynecological Practice, 7th Edition] (pp. 138–138). Stuttgart: Georg Thieme Verlag. [Google Books] [OpenLibrary] [WorldCat] [PDF] [Translation]
Kaiser, U., & Ho, K. K. (2015). Pituitary Physiology and Diagnostic Evaluation. In Melmed, S., Polonsky, K. S., Larsen, P. R., Kronenberg, & H. M. (Eds.). Williams Textbook of Endocrinology, 13th Edition (pp. 176–231). Philadelphia: Elsevier. [DOI:10.1016/B978-0-323-29738-7.00008-3] [Google Books]
Kanhai, R. C., Hage, J. J., Asscheman, H., Mulder, W. J., & Hage, J. J. (1999). Augmentation Mammaplasty in Male-to-Female Transsexuals. Plastic and Reconstructive Surgery, 104(2), 542–549. [DOI:10.1097/00006534-199908000-00040]
Kanhai, R. C., Hage, J. J., van Diest, P. J., Bloemena, E., & Mulder, J. W. (2000). Short-Term and Long-Term Histologic Effects of Castration and Estrogen Treatment on Breast Tissue of 14 Male-to-Female Transsexuals in Comparison With Two Chemically Castrated Men. The American Journal of Surgical Pathology, 24(1), 74–80. [DOI:10.1097/00000478-200001000-00009]
Kardelen, A. D., Toksoy, G., Baş, F., Yavaş Abalı, Z., Gençay, G., Poyrazoğlu, Ş., Bundak, R., Altunoğlu, U., Avcı, Ş., Najaflı, A., Uyguner, O., Karaman, B., Başaran, S., & Darendeliler, F. (2018). A Rare Cause of Congenital Adrenal Hyperplasia: Clinical and Genetic Findings and Follow-up Characteristics of Six Patients with 17-Hydroxylase Deficiency Including Two Novel Mutations. Journal of Clinical Research in Pediatric Endocrinology, 10(3), 206–215. [DOI:10.4274/jcrpe.0032]
Kariagina, A., Xie, J., Leipprandt, J. R., & Haslam, S. Z. (2010). Amphiregulin Mediates Estrogen, Progesterone, and EGFR Signaling in the Normal Rat Mammary Gland and in Hormone-Dependent Rat Mammary Cancers. Hormones and Cancer, 1(5), 229–244. [DOI:10.1007/s12672-010-0048-0]
Karp, N. S. (2022). Discussion: The Impact of Combined Oral Contraceptives on Adolescents with Macromastia. Plastic & Reconstructive Surgery, 150(4), 739–740. [DOI:10.1097/prs.0000000000009514]
Kasielska-Trojan, A., Mikołajczyk, M., & Antoszewski, B. (2020). BreastIdea Volume Estimator: A New Tool for Breast Volume Estimation—Presentation and Validation for Women. Plastic & Reconstructive Surgery, 146(6), 744e–748e. [DOI:10.1097/prs.0000000000007373]
Kasielska-Trojan, A., Zawadzki, T., & Antoszewski, B. (2022). Breast Fluctuating Asymmetry in Women with Macromastia/Gigantomastia. International Journal of Environmental Research and Public Health, 19(24), 16895. [DOI:10.3390/ijerph192416895]
Kauli, R., Pertzelan, A., Ben‐Zeev, Z., Lewin, R. P., Kaufman, H., Schally, A. C., Schally, A. V., & Laron, Z. (1984). Treatment of precocious puberty with LHRH analogue in combination with cyproterone acetate—further experience. Clinical Endocrinology, 20(4), 377–387. [DOI:10.1111/j.1365-2265.1984.tb03433.x]
Keller, P. J. (1984). Diagnostik und Therapie wichtiger hormonaler Störungen: Mammahypoplasie. [Diagnosis and Treatment of Important Hormonal Disorders: Mammary Hypoplasia.] In Keller, P. J. Hormonale Störungen in der Gynäkologie: Diagnostik und Behandlung, 3. Auflage [Hormonal Disorders in Gynecology: Diagnosis and Treatment, 3rd Edition] (Kliniktaschenbücher) (pp. 133–134). Berlin/Heidelberg: Springer. [Google Books] [DOI:10.1007/978-3-662-00442-5_3]
Keller, P. J. (1995). Diagnostik und Therapie wichtiger Störungen: Mammahypoplasie. [Diagnosis and Treatment of Important Disorders: Mammary Hypoplasia.] In Keller, P. J. Hormon- und Fertilitätsstörungen in der Gynäkologie, 4. Auflage [Hormonal and Fertility Disorders in Gynecology, 4th Edition] (pp. 145–146). Berlin/Heidelberg: Springer. [Google Books] [DOI:10.1007/978-3-662-12026-2_3]
Kennedy, B. J. (1953). Effects of intensive sex steroid hormone therapy in advanced breast cancer. JAMA, 152(12), 1135–1141. [DOI:10.1001/jama.1953.63690120004013]
Kent, J. C., Mitoulas, L., Cox, D. B., Owens, R. A., & Hartmann, P. E. (1999). Breast Volume and Milk Production During Extended Lactation in Women. Experimental Physiology, 84(2), 435–447. [DOI:10.1111/j.1469-445x.1999.01808.x]
Khoo, S. K., & Mackay, E. V. (1972). Testicular Feminization: The Clinical Features, Endocrine Function and Gonadal Pathology in Six Patients. Australian and New Zealand Journal of Obstetrics and Gynaecology, 12(1), 1–13. [DOI:10.1111/j.1479-828x.1972.tb00721.x]
Klein, R., Aichinger, H., Dierker, J., Jansen, J. T., Joite-Barfuß, S., Säbel, M., Schulz-Wendtland, R., & Zoetelief, J. (1997). Determination of average glandular dose with modern mammography units for two large groups of patients. Physics in Medicine and Biology, 42(4), 651–671. [DOI:10.1088/0031-9155/42/4/004]
Kleinberg, D. L. (2006). Endocrinology of lactation. In DeGroot, L. J., & Jameson, J. L. (Eds). Endocrinology, 5th Edition (pp. 3461–3473). Philadelphia: Elsevier Saunders. [Google Scholar] [Google Books] [OpenLibrary] [WorldCat] [Archive.org]
Kleinberg, D. L., & Barcellos-Hoff, M. H. (2011). The Pivotal Role of Insulin-Like Growth Factor I in Normal Mammary Development. Endocrinology and Metabolism Clinics of North America, 40(3), 461–471. [DOI:10.1016/j.ecl.2011.06.001]
Kleinberg, D. L., & Ruan, W. (2008). IGF-I, GH, and Sex Steroid Effects in Normal Mammary Gland Development. Journal of Mammary Gland Biology and Neoplasia, 13(4), 353–360. [DOI:10.1007/s10911-008-9103-7]
Kleinberg, D. L., Wood, T. L., Furth, P. A., & Lee, A. V. (2008). Growth Hormone and Insulin-Like Growth Factor-I in the Transition from Normal Mammary Development to Preneoplastic Mammary Lesions. Endocrine Reviews, 30(1), 51–74. [DOI:10.1210/er.2008-0022]
Kühnel, W. (2000). IMMULITE® and IMMULITE® 2000 Reference Range Compendium, First English Edition. Los Angeles, California: Diagnostic Products Corporation. [Google Scholar] [URL] [PDF 1] [PDF 2]
Kustin, J., & Rebar, R. W. (1987). Menstrual Disorders in the Adolescent Age Group. Primary Care: Clinics in Office Practice, 14(1), 139–166. [DOI:10.1016/s0095-4543(21)01004-6]
Kutten, F., Malet, C., & Leygue, E. (1994). Antiestrogen action of progestogens in human breast cells. In Berg, G., & Hammar, M. (Eds.). The Modern Management of the Menopause: A Perspective for the 21st Century [The Proceedings of the VII International Congress on the Menopause, Stockholm, Sweden 1993] (pp. 419–433). Canforth: Parthenon. [Google Scholar] [Google Books] [OpenLibrary] [WorldCat] [Archive.org] [PDF]
Ladjouze, A., & Donaldson, M. (2019). Primary gonadal failure. Best Practice & Research Clinical Endocrinology & Metabolism, 33(3), 101295. [DOI:10.1016/j.beem.2019.101295]
Laessle, R. G., Tuschi, R. J., Schweiger, U., & Pirke, K. M. (1990). Mood changes and physical complaints during the normal menstrual cycle in healthy young women. Psychoneuroendocrinology, 15(2), 131–138. [DOI:10.1016/0306-4530(90)90021-z]
LaMarca, H. L., & Rosen, J. M. (2007). Estrogen regulation of mammary gland development and breast cancer: amphiregulin takes center stage. Breast Cancer Research, 9(4), 304. [DOI:10.1186/bcr1740]
Laron, Z., & Kauli, R. (2000). Experience with Cyproterone Acetate in the Treatment of Precocious Puberty. Journal of Pediatric Endocrinology and Metabolism, 13(Suppl 1), 805–810. [DOI:10.1515/jpem.2000.13.s1.805]
Laufer, M. R., Goldstein, D. P., & Hendren, W. H. (2005). Structural Abnormalities of the Female Reproductive Tract. In Emans, J. E., Laufer, M. R., & Goldstein, D. P. (Eds.). Pediatric and Adolescent Gynecology, 5th Edition (pp. 334–416). Philadelphia: Lippincott Williams and Wilkins. [Google Scholar] [Google Books] [OpenLibrary] [WorldCat] [Archive.org]
Lauritzen, C. (1980 October 27). Hormonkur Kann Hypoplastischer Mamma Aufhelfen. [Hormone Therapy Can Help Hypoplastic Breasts.] Selecta: Medizin aktuell; das Magazin für ärztliche Fortbildung [Selecta: Medicine Currently; the Magazine for Medical Training], 22(43), 3798–3801. Planegg: Selecta-Verlag. [ISSN:0582-4877] [WorldCat] [PDF] [Translation]
Lauritzen, C. (1982). Treatment of mammary- and uterus hypoplasia by estrogen-progestagen pseudopregnancy. In Richter, K., Huber, A., Terruhn, V. (Eds.) 1. Europäisches Symposium für Kinder- und Jugendgynäkologie. München 19.-21.3.1981, Band 2 [First European Symposium on Pediatric and Adolescent Gynaecology. München, March 19–21, 1981, Volume 2] (pp. 487–489). Friedrichsdorf/Taunus: Milupa-Aktiengesellschaft, Wissenschaftliche Abteilung. [Google Scholar] [PDF]
Lauritzen, C. (1989). Hormonelle Substitutionstherapie zur Brustvergrößerung. [Hormonal Substitution Therapy for Breast Enlargement.] In Beller, F. K. & Seitzer, D. (Eds.). 7. Siebte Wissenschaftliche Tagung der Deutschen Gesellschaft für Senologie, Münster, 25. - 27. September 1987: Ausgewählte Referate [7th Scientific Conference of the German Society for Senology, Münster, [Germany,] September 25–27, 1987: Selected Papers] (pp. 39–41). Mülheim, Germany: H.U.F. Verlag. [Google Scholar] [WorldCat 1] [WorldCat 2] [WorldCat 3] [Cited By 1] [Cited By 2] [Cited By 3] [PDF] [Translation]
Lawrence, R. A., & Lawrence, R. M. (2015). Physiology of Lactation. In Lawrence, R. A., & Lawrence, R. M. Breastfeeding: A Guide for the Medical Profession, 8th Edition (pp. 56–90). Philadelphia: Elsevier. [Google Scholar] [Google Books] [OpenLibrary] [WorldCat] [Archive.org]
Lee, H. J., & Ormandy, C. J. (2012). Interplay between progesterone and prolactin in mammary development and implications for breast cancer. Molecular and Cellular Endocrinology, 357(1–2), 101–107. [DOI:10.1016/j.mce.2011.09.020]
Lee, P. A. (2001). Physiology of Puberty. In Becker, K. L., Bilezikian, J. P., Bremner, W. J., Hung, W., Kahn, C. R., Loriaux, D. L., Nylén, E. S., Rebar, R. W., Robertson, G. L., Snider, R. H., Wartofsky, L. (Eds.). Principles and Practice of Endocrinology and Metabolism, 3rd Edition (pp. 885–893). Philadelphia: Lippincott Williams & Wilkins. [Google Scholar] [Google Books] [OpenLibrary] [WorldCat] [Archive.org]
Lee, S. W., Kwak, D. S., Jung, I. S., Kwak, J. H., Park, J. H., Hong, S. M., Lee, C. B., Park, Y. S., Kim, D. S., Choi, W. H., & Ahn, Y. H. (2015). Partial Androgen Insensitivity Syndrome Presenting with Gynecomastia. Endocrinology and Metabolism, 30(2), 226–230. [DOI:10.3803/enm.2015.30.2.226]
Lejour, M. (1994). Vertical Mammaplasty and Liposuction of the Breast. Plastic and Reconstructive Surgery, 94(1), 100–114. [DOI:10.1097/00006534-199407000-00010]
Lejour, M. (1997). Evaluation of Fat in Breast Tissue Removed by Vertical Mammaplasty. Plastic and Reconstructive Surgery, 99(2), 386–393. [DOI:10.1097/00006534-199702000-00012]
Lemarchand-Béraud, T., Zufferey, M., Reymond, M., & Rey, I. (1982). Maturation of the Hypothalamo-Pituitary-Ovarian Axis in Adolescent Girls. The Journal of Clinical Endocrinology & Metabolism, 54(2), 241–246. [DOI:10.1210/jcem-54-2-241]
Lewin, R. (2016). Breast Hypertrophy and Outcome of Breast Reduction Surgery. (Doctoral thesis, University of Gothenburg. Sahlgrenska Academy.) [Google Scholar] [URL]
Lim, L. Y., Ho, P. J., Liu, J., Chay, W. Y., Tan, M., Hartman, M., & Li, J. (2018). Determinants of breast size in Asian women. Scientific Reports, 8(1), 1201. [DOI:10.1038/s41598-018-19437-4]
Lloyd, C. W., & Leathem, J. H. (1964). Growth and development of the breast and lactation. In Lloyd, C. W. (Ed.). Human Reproduction and Sexual Behavior (pp. 117–134). Philadelphia: Lea & Febiger. [Google Scholar] [Google Books] [OpenLibrary] [WorldCat]
Lopez, X., Panton, J., Nagarkar, P., Preston, S., Abramowitz, J., & Amirlak, B. (2023). Initial Assessment of VECTRA Three-Dimensional Imaging to Accurately Simulate Breast Volume Changes in Transfeminine Patients: A Mannequin Study. Aesthetic Surgery Journal Open Forum, 5, online ahead of print. [DOI:10.1093/asjof/ojad015]
Lorincz, A. M., & Sukumar, S. (2006). Molecular links between obesity and breast cancer. Endocrine-Related Cancer, 13(2), 279–292. [DOI:10.1677/erc.1.00729]
Lucien, J. N., Ortega, M. T., Calvert, M. E., Smith, C., White, X., Rogers, H., Mosley, B., Agrawal, R., Drude, A., McGee, C., George, M., Brown, A., Downey, K., Wild, C., Njunge, A., Kuzmiak, C. M., Zava, D., Zava, T., Pollard, J., Francis, J., Beery, B. L., Harlin, M., Gonzalez, G. R., & Shaw, N. D. (2022). The Launch of A Girl’s First Period Study: Demystifying Reproductive Hormone Profiles in Adolescent Girls. Journal of Pediatric and Adolescent Gynecology, 35(4), 420–425. [DOI:10.1016/j.jpag.2021.12.018]
Lydon, J. P., DeMayo, F. J., Funk, C. R., Mani, S. K., Hughes, A. R., Montgomery, C. A., Shyamala, G., Conneely, O. M., & O’Malley, B. W. (1995). Mice lacking progesterone receptor exhibit pleiotropic reproductive abnormalities. Genes & Development, 9(18), 2266–2278. [DOI:10.1101/gad.9.18.2266]
Lyon, A. J., De Bruyn, R., & Grant, D. B. (1985). Isosexual Precocious Puberty in Girls. Acta Paediatrica, 74(6), 950–955. [DOI:10.1111/j.1651-2227.1985.tb10063.x]
Lyons, W. R. (1958). Hormonal synergism in mammary growth. Proceedings of the Royal Society of London. Series B - Biological Sciences, 149(936), 303–325. [DOI:10.1098/rspb.1958.0071]
Lyons, W. R., & McGinty, D. A. (1941). Effects of estrone and progesterone on male rabbit mammary glands. I. Varying doses of progesterone. Proceedings of the Society for Experimental Biology and Medicine, 48(1), 83–86. [DOI:10.3181/00379727-48-13227]
Lyons, W. R., Li, C. H., & Johnson, R. E. (1958). The Hormonal Control of Mammary Growth and Lactation. In Pincus, G. (Ed.). Recent Progress in Hormone Research, Volume 14 [Proceedings of the Laurentian Hormone Conference 1957, Held at Mont Tremblant, Quebec] (pp. 219–254). New York/London: Academic Press. [Google Scholar] [Google Books] [PubMed] [OpenLibrary] [WorldCat] [PDF]
MacBryde, C. M. (1939). The Production of Breast Growth in the Human Female. Journal of the American Medical Association, 112(11), 1045–1049. [DOI:10.1001/jama.1939.02800110025006]
Malet, C., Gompel, A., Yaneva, H., Cren, H., Fidji, N., Mowszowicz, I., Kuttenn, F., & Mauvais-Jarvis, P. (1991). Estradiol and Progesterone Receptors in Cultured Normal Human Breast Epithelial Cells and Fibroblasts: Immunocytochemical Studies. The Journal of Clinical Endocrinology & Metabolism, 73(1), 8–17. [DOI:10.1210/jcem-73-1-8]
Malini, S., Smith, E. O., & Goldzieher, J. W. (1985). Measurement of breast volume by ultrasound during normal menstrual cycles and with oral contraceptive use. Obstetrics and Gynecology, 66(4), 538–541. [Google Scholar] [PubMed] [URL] [PDF]
Marshall, W. A. (1978). Puberty. In Falkner, F., & Tanner, J. M. (Eds.). Human Growth: Postnatal Growth (pp. 141–181). Boston: Springer US. [DOI:10.1007/978-1-4684-2622-9_6]
Marshall, W. A., & Tanner, J. M. (1969). Variations in pattern of pubertal changes in girls. Archives of Disease in Childhood, 44(235), 291–303. [DOI:10.1136/adc.44.235.291]
Mauvais-Jarvis, P., Kuttenn, F., & Gompel, A. (1986). Antiestrogen action of progesterone in breast tissue. Breast Cancer Research and Treatment, 8(3), 179–188. [DOI:10.1007/bf01807330]
Mauvais-Jarvis, P., Kuttenn, F., & Gompel, A. (1986). Estradiol/Progesterone Interaction in Normal and Pathologic Breast Cells. Annals of the New York Academy of Sciences, 464(1), 152–167. [DOI:10.1111/j.1749-6632.1986.tb16002.x]
Mauvais-Jarvis, P., Kuttenn, F., & Gompel, A. (1987). Antiestrogen Action of Progesterone in Breast Tissue. Hormone Research, 28(2–4), 212–218. [DOI:10.1159/000180946]
Mauvais-Jarvis, P., Kuttenn, F., Gompel, A., & Benotmane, A. (1987). Action anti-estrogène de la progestérone dans le sein. [Antiestrogen action of progesterone in the breast]. Pathologie-Biologie, 35(7), 1081–1086. [Google Scholar 1] [Google Scholar 2] [PubMed]
Mauvais-Jarvis, P., Sitruk-Ware, R., & Kuttenn, F. (1981). Benign Breast Disease. In McGuire, W. L. (Ed.). Breast Cancer 4: Advances in Research and Treatment (pp. 51–94). Boston: Springer US. [DOI:10.1007/978-1-4615-6571-0_3]
McArthur, J. W. (1966). The Reproductive Endocrinology of Adolescence. In Heald, F. P. (Ed.). Adolescent Gynecology (pp. 9–20). Baltimore: Williams & Wilkins. [Google Scholar] [Google Books] [OpenLibrary] [WorldCat]
McBryan, J., Howlin, J., Napoletano, S., & Martin, F. (2008). Amphiregulin: Role in Mammary Gland Development and Breast Cancer. Journal of Mammary Gland Biology and Neoplasia, 13(2), 159–169. [DOI:10.1007/s10911-008-9075-7]
McDonough, P. G., Spicer, D. V., Ursin, G., & Pike, M. C. (1996). Progesterone Concentrations—Physiologic or Pharmacologic? Fertility and Sterility, 65(5), 1077–1078. [DOI:10.1016/s0015-0282(16)58295-8]
McMillan, M. (1966). Five cases of testicular feminisation including one with a teratoma of the testis. The Journal of Pathology and Bacteriology, 91(2), 417–427. [DOI:10.1002/path.1700910216]
McNally, S., & Stein, T. (2016). Overview of Mammary Gland Development: A Comparison of Mouse and Human. In Martin, F., Stein, T., & Howlin, J. (Eds.). Mammary Gland Development (Methods in Molecular Biology, Volume 1501) (pp. 1–17). New York: Springer New York. [DOI:10.1007/978-1-4939-6475-8_1]
McPhaul, M. J. (2002). Androgen receptor mutations and androgen insensitivity. Molecular and Cellular Endocrinology, 198(1–2), 61–67. [DOI:10.1016/s0303-7207(02)00369-6]
Mesiano, S. (2019). Endocrinology of Human Pregnancy and Fetal-Placental Neuroendocrine Development. In Strauss, J. F., & Barbieri, R. L. (Eds.). Yen and Jaffe’s Reproductive Endocrinology: Physiology, Pathophysiology, and Clinical Management, 8th Edition (pp. 256–284.e9). Philadelphia: Elsevier. [Google Books] [DOI:10.1016/b978-0-323-47912-7.00011-1]
Meyer, G., Mayer, M., Mondorf, A., Flügel, A. K., Herrmann, E., & Bojunga, J. (2020). Safety and rapid efficacy of guideline-based gender-affirming hormone therapy: an analysis of 388 individuals diagnosed with gender dysphoria. European Journal of Endocrinology, 182(2), 149–156. [DOI:10.1530/eje-19-0463]
Meyer, W. J., Finkelstein, J. W., Stuart, C. A., Webb, A., Smith, E. R., Payer, A. F., & Walker, P. A. (1981). Physical and hormonal evaluation of transsexual patients during hormonal therapy. Archives of Sexual Behavior, 10(4), 347–356. [DOI:10.1007/bf01565538]
Meyer, W. J., Webb, A., Stuart, C. A., Finkelstein, J. W., Lawrence, B., & Walker, P. A. (1986). Physical and hormonal evaluation of transsexual patients: A longitudinal study. Archives of Sexual Behavior, 15(2), 121–138. [DOI:10.1007/bf01542220]
Mikołajczyk, M., Kasielska-Trojan, A., & Antoszewski, B. (2019). A New Tool for Breast Anthropometric Measurements: Presentation and Validation for Women and Men. Aesthetic Plastic Surgery, 43(5), 1160–1170. [DOI:10.1007/s00266-019-01467-6]
Milionis, C., Ilias, I., & Koukkou, E. (2022). Progesterone in gender-affirming therapy of trans women. World Journal of Biological Chemistry, 13(3), 66–71. [DOI:10.4331/wjbc.v13.i3.66]
Milligan, D., Drife, J. O., & Short, R. V. (1975). Changes in breast volume during normal menstrual cycle and after oral contraceptives. BMJ, 4(5995), 494–496. [DOI:10.1136/bmj.4.5995.494]
Morris, J. M. (1953). The syndrome of testicular feminization in male pseudohermaphrodites. American Journal of Obstetrics and Gynecology, 65(6), 1192–1211. [DOI:10.1016/0002-9378(53)90359-7]
Morris, J. M., & Mahesh, V. B. (1963). Further observations on the syndrome, “testicular feminization”. American Journal of Obstetrics and Gynecology, 87(6), 731–748. [Google Scholar 1] [Google Scholar 2] [PubMed] [PDF]
Muallem, M. M., & Rubeiz, N. G. (2006). Physiological and biological skin changes in pregnancy. Clinics in Dermatology, 24(2), 80–83. [DOI:10.1016/j.clindermatol.2005.10.002]
Müller, C. (1953). Zur Hormonalen Kosmetik der Weiblichen Brust: Wirkung und Nebenwirkung Östrogenhaltiger Kosmetischer Präparate. [Hormonal Cosmetics of the Female Breast: Effects and Side Effects of Estrogen-Containing Cosmetic Preparations.] Schweizerische Medizinische Wochenschrift [Swiss Medical Weekly], 83(4), 81–84. [Google Scholar 1] [Google Scholar 2] [PubMed] [PDF] [Translation]
Muzaffar, F., Hussain, I., & Haroon, T. S. (1998). Physiologic skin changes during pregnancy: a study of 140 cases. International Journal of Dermatology, 37(6), 429–431. [DOI:10.1046/j.1365-4362.1998.00281.x]
Naik, M., Diwakar, R. K., Patre, S., & Singh, S. (2015). Gigantomastia: A Rare Complication In Pregnancy. Journal of Medical Science and Clinical Research, 3(7), 6873–6876. [Google Scholar] [URL] [PDF]
Naseem, H., Lokman, M., & Fitzgerald, C. (2021). Management of congenital hypogonadotropic hypogonadism in females. Human Fertility, 26(3), 622–631. [DOI:10.1080/14647273.2021.1998929]
Nelson, W. O. (1936). Endocrine Control of the Mammary Gland. Physiological Reviews, 16(3), 488–526. [DOI:10.1152/physrev.1936.16.3.488]
Nolan, B. J., Frydman, A. S., Leemaqz, S. Y., Carroll, M., Grossmann, M., Zajac, J. D., & Cheung, A. S. (2022). Effects of low-dose oral micronised progesterone on sleep, psychological distress, and breast development in transgender individuals undergoing feminising hormone therapy: a prospective controlled study. Endocrine Connections, 11(5), e220170. [DOI:10.1530/EC-22-0170]
Nolan, B. J., Frydman, A. S., Leemaqz, S. Y., Carroll, M., Grossmann, M., Zajac, J. D., & Cheung, A. S. (2022). Effects Of Low-dose Oral Micronised Progesterone On Sleep, Psychological Distress And Breast Development In Transgender Individuals Undergoing Feminising Hormone Therapy: A Prospective Controlled Study. Journal of the Endocrine Society, 6(Suppl 1), A653–A654 (abstract no. LBODP089). [DOI:10.1210/jendso/bvac150.1351]
Nussbaum, R., & Benedetto, A. V. (2006). Cosmetic aspects of pregnancy. Clinics in Dermatology, 24(2), 133–141. [DOI:10.1016/j.clindermatol.2005.10.007]
Nuzzi, L. C., Pramanick, T., Massey, G. G., Walsh, L. R., McNamara, C. T., Firriolo, J. M., DiVasta, A. D., & Labow, B. I. (2021). The Impact of Progestin-only Contraception on Adolescents with Macromastia. Plastic and Reconstructive Surgery - Global Open, 9(2), e3421. [DOI:10.1097/gox.0000000000003421]
Nuzzi, L. C., Pramanick, T., Massey, G. G., Walsh, L. R., McNamara, C. T., Firriolo, J. M., DiVasta, A. D., & Labow, B. I. (2022). The Impact of Combined Oral Contraceptives on Adolescents with Macromastia. Plastic and Reconstructive Surgery, 150(4), 731–738. [DOI:10.1097/prs.0000000000009513]
Oakes, M. B., Eyvazzadeh, A. D., Quint, E., & Smith, Y. R. (2008). Complete Androgen Insensitivity Syndrome—A Review. Journal of Pediatric and Adolescent Gynecology, 21(6), 305–310. [DOI:10.1016/j.jpag.2007.09.006]
Obr, A. E., & Edwards, D. P. (2012). The biology of progesterone receptor in the normal mammary gland and in breast cancer. Molecular and Cellular Endocrinology, 357(1–2), 4–17. [DOI:10.1016/j.mce.2011.10.030]
Olanrewaju, F., Onayemi, O., Olasode, O., Adeyemi, A., Oninla, A., Oripelaye, M., Ezejiofor, O., & Oke, O. (2017). Prevalence and Pattern of Pigmentary Changes among Primigravidae Attending a Tertiary Health Facility in South-Western Nigeria. British Journal of Medicine and Medical Research, 21(5), 1–9. [DOI:10.9734/bjmmr/2017/33382]
Orentreich, N., & Durr, N. P. (1974). Mammogenesis in Transsexuals. Journal of Investigative Dermatology, 63(1), 142–146. [DOI:10.1111/1523-1747.ep12678272]
Pandya, S., & Moore, R. G. (2011). Breast Development and Anatomy. Clinical Obstetrics & Gynecology, 54(1), 91–95. [DOI:10.1097/grf.0b013e318207ffe9]
Park, I. Y., Kim, M. R., Jo, H. H., Lee, M. K., & Kim, M. J. (2014). Association of the Nipple-Areola Complexes with Age, Parity, and Breastfeeding in Korean Premenopausal Women. Journal of Human Lactation, 30(4), 474–479. [DOI:10.1177/0890334414549049]
Pasqualini, J. R. (2007). Progestins and breast cancer. Gynecological Endocrinology, 23(Suppl 1), 32–41. [DOI:10.1080/09513590701585003]
Pasqualini, J. R. (2009). Breast cancer and steroid metabolizing enzymes: The role of progestogens. Maturitas, 65(Suppl 1), S17–S21. [DOI:10.1016/j.maturitas.2009.11.006]
Pasqualini, J. R., & Kincl, F. A. (1985). Hormone Production and Concentrations During Pregnancy in Humans and in Other Mammalian Species. In Pasqualini, J. R., & Kincl, F. A. Hormones and the Fetus, Volume I: Production, Concentration and Metabolism During Pregnancy (pp. 173–334). Oxford: Pergamon Press. [DOI:10.1016/b978-0-08-019708-1.50007-6]
Patel, H., Arruarana, V., Yao, L., Cui, X., & Ray, E. (2020). Effects of hormones and hormone therapy on breast tissue in transgender patients: a concise review. Endocrine, 68(1), 6–15. [DOI:10.1007/s12020-020-02197-5]
Patel, K. T., Adeel, S., Rodrigues Miragaya, J., & Tangpricha, V. (2022). Progestogen Use in Gender-Affirming Hormone Therapy: A Systematic Review. Endocrine Practice, 28(12), 1244–1252. [DOI:10.1016/j.eprac.2022.08.012]
Patterson, M. N., McPhaul, M. J., & Hughes, I. A. (1994). Androgen insensitivity syndrome. Baillière’s Clinical Endocrinology and Metabolism, 8(2), 379–404. [DOI:10.1016/s0950-351x(05)80258-7]
Pawłowski, B., & Żelaźniewicz, A. (2021). The evolution of perennially enlarged breasts in women: a critical review and a novel hypothesis. Biological Reviews, 96(6), 2794–2809. [DOI:10.1111/brv.12778]
Perez-Palacios, G., & Jaffe, R. B. (1972). The Syndrome of Testicular Feminization. Pediatric Clinics of North America, 19(3), 653–667. [DOI:10.1016/s0031-3955(16)32744-4]
Petrakis, N. (1978). Recurrent extreme breast involution following pregnancy and susceptibility to breast cancer: A hypothesis. Medical Hypotheses, 4(3), 268–272. [DOI:10.1016/0306-9877(78)90006-3]
Pfeiffer, C. A. (1943). Endocrinology of Reproduction. Annual Review of Physiology, 5(1), 413–452. [DOI:10.1146/annurev.ph.05.030143.002213]
Pipkin, F. B. (2019). Physiological Changes in Pregnancy. In Symonds, I. M., & Arulkumaran, S. (Eds.). Essential Obstetrics and Gynaecology, 6th Edition (pp. 22–40). Edinburgh: Elsevier. [Google Books] [OpenLibrary] [WorldCat]
Plu-Bureau, G., Touraine, P., & Mauvais-Jarvis, P. (1999). Interactions Between Estradiol and Progesterone in Normal Breast: Implications for Mammary Carcinogenesis. In Manni, A. (Ed.). Endocrinology of Breast Cancer (Contemporary Endocrinology, Volume 11) (pp. 21–37). Totowa, New Jersey: Humana Press. [DOI:10.1007/978-1-59259-699-7_2] [OpenLibrary] [Archive.org]
Pocock, G., Richards, C. D., & Richards, D. A. (2013). Fertilization, Pregnancy, and Lactation. In Pocock, G., Richards, C. D., & Richards, D. A. Human Physiology, 4th Edition (pp. 655–752). Oxford: Oxford University Press. [Google Scholar] [Google Books]
Polani, P. E. (1970). Hormonal and clinical aspects of hermaphroditism and the testicular feminizing syndrome in man. Philosophical Transactions of the Royal Society of London. B, Biological Sciences, 259(828), 187–206. [DOI:10.1098/rstb.1970.0058]
Price, S., McManus, J., & Barrett, J. (2019). The transgender population: improving awareness for gynaecologists and their role in the provision of care. The Obstetrician & Gynaecologist, 21(1), 11–20. [DOI:10.1111/tog.12521]
Prior, J. C. (2011). Progesterone for Symptomatic Perimenopause Treatment - Progesterone politics, physiology and potential for perimenopause. Facts, Views & Vision in ObGyn, 3(2), 109–120. [PubMed] [PubMed Central] [PDF]
Prior, J. C. (2019). Progesterone Is Important for Transgender Women’s Therapy—Applying Evidence for the Benefits of Progesterone in Ciswomen. The Journal of Clinical Endocrinology & Metabolism, 104(4), 1181–1186. [DOI:10.1210/jc.2018-01777]
Prior, J. C. (2019). Response to Letter to the Editor: “Progesterone Is Important for Transgender Women’s Therapy—Applying Evidence for the Benefits of Progesterone in Ciswomen”. The Journal of Clinical Endocrinology & Metabolism, 104(8), 3129–3130. [DOI:10.1210/jc.2019-00524]
Prior, J. C. (2020). Women’s Reproductive System as Balanced Estradiol and Progesterone Actions—A revolutionary, paradigm-shifting concept in women’s health. Drug Discovery Today: Disease Models, 32(Part B), 31–40. [DOI:10.1016/j.ddmod.2020.11.005]
Prior, J. C., Vigna, Y. M., & Watson, D. (1989). Spironolactone with physiological female steroids for presurgical therapy of male-to-female transsexualism. Archives of Sexual Behavior, 18(1), 49–57. [DOI:10.1007/bf01579291]
Prior, J. C., Vigna, Y. M., Watson, D., Diewold, P., & Robinow, O. (1986). Spironolactone in the presurgical therapy of male to female transsexuals: Philosophy and experience of the Vancouver Gender Dysphoria Clinic. Journal of Sex Information & Education Council of Canada, 1(1), 1–7. [Google Scholar] [PDF]
Quigley, C. A. (1998). The androgen receptor: Physiology and pathophysiology. In Nieschlag, E., & Behre, H. M. (Eds.). Testosterone: Action · Deficiency · Substitution, 2nd Edition (pp. 33–106). Berlin/Heidelberg: Springer. [DOI:10.1007/978-3-642-72185-4_2]
Quigley, C. A., Bellis, A. D., Marschke, K. B., El-Awady, M. K., Wilson, E. M., & French, F. S. (1995). Androgen Receptor Defects: Historical, Clinical, and Molecular Perspectives. Endocrine Reviews, 16(3), 271–321. [DOI:10.1210/edrv-16-3-271]
Radisky, D. C., & Hartmann, L. C. (2009). Mammary Involution and Breast Cancer Risk: Transgenic Models and Clinical Studies. Journal of Mammary Gland Biology and Neoplasia, 14(2), 181–191. [DOI:10.1007/s10911-009-9123-y]
Ramos, L., Chávez, B., Mares, L., Valdés, E., & Vilchis, F. (2018). Mutational analysis of the androgen receptor (NR3C4) gene in patients with 46,XY DSD. Gene, 641, 86–93. [DOI:10.1016/j.gene.2017.10.038]
Ramsay, D. T., Kent, J. C., Hartmann, R. A., & Hartmann, P. E. (2005). Anatomy of the lactating human breast redefined with ultrasound imaging. Journal of Anatomy, 206(6), 525–534. [DOI:10.1111/j.1469-7580.2005.00417.x]
Randolph, J. F. (2018). Gender-Affirming Hormone Therapy for Transgender Females. Clinical Obstetrics & Gynecology, 61(4), 705–721. [DOI:10.1097/grf.0000000000000396]
Rauh, C., Faschingbauer, F., Haeberle, L., Jud, S. M., Heusinger, K., Fasching, P. A., Goecke, T. W., Rajakaruna, N., Voigt, F., Bani, M. R., Lux, M. P., Renner, S. P., Loehberg, C. R., Hartmann, A., Schulz-Wendtland, R., Beckmann, M. W., & Bayer, C. M. (2013). Factors influencing breast changes after pregnancy. European Journal of Cancer Prevention, 22(3), 259–261. [DOI:10.1097/cej.0b013e328359cb81]
Rebar, R. W. (1988). The Ovaries. In Wyngaarden, J. B., & Smith, L. H. (Eds.). Cecil Textbook of Medicine, 18th Edition (pp. 1425–1446). Philadelphia: W. B. Saunders. [Google Books] [OpenLibrary] [WorldCat] [Archive.org]
Rebar, R. W. (1990). Disorders of Menstruation, Ovulation, and Sexual Response. In Becker, K. L., Bilezikian, J. P., Bremner, W. J., Hung, W., Kahn, C. R., Loriaux, D. L., Rebar, R. W., Robertson, G. L., & Wartofsky, L. (Eds.). Principles and Practice of Endocrinology and Metabolism, 1st Edition (pp. 798–814). Philadelphia: Lippincott. [Google Scholar—3rd/2001 Edition] [Google Books—3rd/2001 Edition] [OpenLibrary] [WorldCat] [Archive.org]
Rebar, R. W. (1993). Normal and Abnormal Sexual Differentiation and Pubertal Development. In Moore, T. R., Reiter, R. C., Rebar, R. W., & Baker, W. (Eds.). Gynecology & Obstetrics: A Longitudinal Approach (pp. 97–133). New York: Churchill Livingstone. [Google Books] [OpenLibrary] [WorldCat] [Archive.org]
Rebar, R. W. (1996). Puberty. In Berek, J. S., Adashi, E. Y., & Hillard, P. A. (Eds.). Novak’s Gynecology, 12th Edition (pp. 771–807). Baltimore: Williams & Wilkins. [Google Scholar] [Google Books] [OpenLibrary] [WorldCat] [Archive.org]
Reindollar, R. H., & McDonough, P. G. (1985). The Child with Ambiguous Genitalia. In Lavery, J. P., & Sanfilippo, J. S. (Eds.). Pediatric and Adolescent Obstetrics and Gynecology, 1st Edition (Clinical Perspective in Obstetrics and Gynecology) (pp. 38–60). New York: Springer. [DOI:10.1007/978-1-4612-5064-7_5]
Reisman, T., Goldstein, Z., & Safer, J. D. (2019). A Review of Breast Development in Cisgender Women and Implications for Transgender Women. Endocrine Practice, 25(12), 1338–1345. [DOI:10.4158/ep-2019-0183]
Richards, C., & Barrett, J. (2020). Physical Treatments for Trans People and Their Interactions with Psychiatric Treatments. In Richards, C., & Barrett, J. Trans and Non-binary Gender Healthcare for Psychiatrists, Psychologists, and Other Health Professionals (pp. 31–44). Cambridge: Cambridge University Press. [DOI:10.1017/9781108628419.003]
Richert, M. M., Schwertfeger, K. L., Ryder, J. W., & Anderson, S. M. (2000). An Atlas of Mouse Mammary Gland Development. Journal of Mammary Gland Biology and Neoplasia, 5(2), 227–241. [DOI:10.1023/a:1026499523505]
Rix, J., Mills, C., Ross, E., Allen, S., Lai, A., & Wakefield-Scurr, J. (2023). Breast volume fluctuations are associated with oestradiol and progesterone changes across the menstrual cycle. Research Square, preprint. [Google Scholar] [DOI:10.21203/rs.3.rs-3753080/v1] [PDF]
Rodari, G. (2022). Pubertal induction in girls with hypogonadism: estrogen replacement therapy outcomes and optimization of progesterone introduction. (Doctoral thesis, Università degli Studi di Milano.) [URL]
Rodari, G., Federici, S., Cattoni, A., Todisco, T., Ubertini, G., Giacchetti, F., Profka, E., Dall’Antonia, A., Cangiano, B., Arosio, M., Bonomi, M., Cappa, M., & Giavoli, C. (2022). Pubertal induction in girls with hypogonadism: insight into estrogen replacement therapy outcomes and optimization of progesterone introduction. Endocrine Abstracts, 81 [24th European Congress of Endocrinology 2022 21–24 May 2022, Milan, Italy], 107–107 (abstract no. RC12.7). [DOI:10.1530/endoabs.81.rc12.7] [PDF]
Rodari, G., Federici, S., Todisco, T., Ubertini, G., Cattoni, A., Pagano, M., Giacchetti, F., Profka, E., Citterio, V., Messetti, D., Collini, V., Soranna, D., Carbone, E., Arosio, M., Mantovani, G., Persani, L., Cappa, M., Bonomi, M., & Giavoli, C. (2023). Towards an individualized management of pubertal induction in girls with hypogonadism: insight into the best replacement outcomes from a large multicentre registry. European Journal of Endocrinology, 188(6), 467–476. [DOI:10.1093/ejendo/lvad056]
Rohn, R. D. (1989). Nipple (papilla) development in girls: III. Journal of Adolescent Health Care, 10(1), 39–40. [DOI:10.1016/0197-0070(89)90045-4]
Rosenfield, R. L. (2013). Adolescent Anovulation: Maturational Mechanisms and Implications. The Journal of Clinical Endocrinology & Metabolism, 98(9), 3572–3583. [DOI:10.1210/jc.2013-1770]
Rosenfield, R. L., Cooke, D. W., & Radovick, S. (2021). Puberty in the Female and Its Disorders. In Sperling, M. A., Majzoub, J. A., Menon, R. K., & Stratakis, C. A. (Eds.). Sperling Pediatric Endocrinology, 5th Edition (pp. 528–626). Philadelphia: Elsevier. [DOI:10.1016/B978-0-323-62520-3.00016-6]
Rothman, M. S., & Iwamoto, S. J. (2022). Feminizing Gender-Affirming Hormone Therapy: Special Considerations for Older Adults. In Davis, T. F. (Ed.). A Case-Based Guide to Clinical Endocrinology (pp. 513–523). Cham: Springer. [DOI:10.1007/978-3-030-84367-0_58]
Ruan, W., Monaco, M. E., & Kleinberg, D. L. (2005). Progesterone Stimulates Mammary Gland Ductal Morphogenesis by Synergizing with and Enhancing Insulin-Like Growth Factor-I Action. Endocrinology, 146(3), 1170–1178. [DOI:10.1210/en.2004-1360]
Rutgers, J. L., & Scully, R. E. (1991). The Androgen Insensitivity Syndrome (Testicular Feminization). International Journal of Gynecological Pathology, 10(2), 126–144. [DOI:10.1097/00004347-199104000-00002]
Ryan, R. F., & Pernoll, M. L. (1985). Virginal Hypertrophy. Plastic and Reconstructive Surgery, 75(5), 737–742. [DOI:10.1097/00006534-198505000-00024]
Saito, R., Yamamoto, Y., Goto, M., Araki, S., Kubo, K., Kawagoe, R., Kawada, Y., Kusuhara, K., Igarashi, M., & Fukami, M. (2014). Tamoxifen Treatment for Pubertal Gynecomastia in Two Siblings with Partial Androgen Insensitivity Syndrome. Hormone Research in Paediatrics, 81(3), 211–216. [DOI:10.1159/000356923]
Sandhu, R., Chollet-Hinton, L., Kirk, E. L., Midkiff, B., & Troester, M. A. (2016). Digital histologic analysis reveals morphometric patterns of age-related involution in breast epithelium and stroma. Human Pathology, 48, 60–68. [DOI:10.1016/j.humpath.2015.09.031]
Santen, R. J., Karaguzel, G., Livaoglu, M., Yue, W., Cline, J. M., Ratan, A., & Sasano, H. (2024). Role of ERα and aromatase in juvenile gigantomastia. The Journal of Clinical Endocrinology and Metabolism, online ahead of print. [DOI:10.1210/clinem/dgae019]
Sanuki, J., Fukuma, E., & Uchida, Y. (2008). Morphologic Study of Nipple-Areola Complex in 600 Breasts. Aesthetic Plastic Surgery, 33(3), 295–297. [DOI:10.1007/s00266-008-9194-y]
Satoh, K., Hovey, R. C., Malewski, T., Warri, A., Goldhar, A. S., Ginsburg, E., Saito, K., Lydon, J. P., & Vonderhaar, B. K. (2007). Progesterone enhances branching morphogenesis in the mouse mammary gland by increased expression of Msx2. Oncogene, 26(54), 7526–7534. [DOI:10.1038/sj.onc.1210555]
Schauffler, G. C. (1942). Disorders During Adolescence—The Onset of Menstruation. In Schauffler, G. C. Pediatric Gynecology; with Sections on Urology and Proctology, 1st Edition (pp. 169–211). Chicago: Year Book. [Google Scholar] [Google Books] [OpenLibrary] [WorldCat] [URL]
Schindler, A. E. (2010). Dydrogesterone and other progestins in benign breast disease: an overview. Archives of Gynecology and Obstetrics, 283(2), 369–371. [DOI:10.1007/s00404-010-1456-7]
Scott, P. P., Greene, R., Lane-Roberts, C. S., & Swain, V. (1950). The Function of the Breast. In Saner, F. D. (Ed.). The Breast: Structure, Function, Disease (pp. 53–86). Baltimore: Williams and Wilkins. [Google Scholar] [Google Books] [OpenLibrary] [WorldCat] [URL] [PDF]
Seal, L. (2017). Adult Endocrinology. In Richards, C., Bouman, W. P., & Barker, M.-J. (Eds.). Genderqueer and Non-Binary Genders (Critical and Applied Approaches in Sexuality, Gender and Identity) (pp. 183–223). London: Palgrave Macmillan UK. [DOI:10.1057/978-1-137-51053-2_10]
Seal, L. J., Franklin, S., Richards, C., Shishkareva, A., Sinclaire, C., & Barrett, J. (2012). Predictive Markers for Mammoplasty and a Comparison of Side Effect Profiles in Transwomen Taking Various Hormonal Regimens. The Journal of Clinical Endocrinology & Metabolism, 97(12), 4422–4428. [DOI:10.1210/jc.2012-2030]
Seibert, B., & Günzel, P. (1994). Animal toxicity studies performed for risk assessment of the once-a-month injectable contraceptive Mesigyna®. Contraception, 49(4), 303–333. [DOI:10.1016/0010-7824(94)90030-2]
Shapiro, L. R. (1982). Disorders of Female Sex Differentiation. In Blaustein, A. (Ed.). Pathology of the Female Genital Tract, 2nd Edition (pp. 479–510). New York: Springer New York. [DOI:10.1007/978-1-4757-1767-9_20]
Shearman, R. P. (1972). Ovarian Function and its Control. In Shearman, R. P. (Ed.). Human Reproductive Physiology, 1st Edition (pp. 45–90). Oxford: Blackwell Scientific Publications. [Google Scholar] [Google Books] [OpenLibrary] [WorldCat] [Archive.org]
Shearman, R. P. (1972). Primary Ammenorhoea. In Dewhurst, C. J. (Ed.). Integrated Obstetrics and Gynaecology for Postgraduates, 1st Edition (pp. 55–62). Oxford: Blackwell Scientific Publications. [Google Scholar] [Google Books] [OpenLibrary] [WorldCat] [Archive.org]
Shi, H. Y., Lydon, J. P., & Zhang, M. (2004). Hormonal Defect in Maspin Heterozygous Mice Reveals a Role of Progesterone in Pubertal Ductal Development. Molecular Endocrinology, 18(9), 2196–2207. [DOI:10.1210/me.2004-0052]
Shuttleworth, F. K. (1938). The Adolescent Period: A Graphic and Pictorial Atlas (Monographs of the Society for Research in Child Development, Volume 3, Number 3 / Serial No. 16). Washington, D. C.: Society for Research in Child Development. [Google Scholar] [Google Books] [DOI:10.2307/1165482]
Simmer, H. H., Pion, R. J., & Dignam, W. J. (1965). Testicular Feminization: Endocrine Function of Feminizing Testes, Comparison with Normal Testes. Springfield, Illinois: Thomas. [Google Scholar] [Google Books] [OpenLibrary] [WorldCat]
Simpson, J. L., & Rebar, R. W. (1990). Normal and Abnormal Sexual Differentiation and Development. In Becker, K. L., Bilezikian, J. P., Bremner, W. J., Hung, W., Kahn, C. R., Loriaux, D. L., Rebar, R. W., Robertson, G. L., & Wartofsky, L. (Eds.). Principles and Practice of Endocrinology and Metabolism, 1st Edition (pp. 710–739). Philadelphia: Lippincott. [Google Scholar] [Google Books—3rd/2001 Edition] [OpenLibrary] [WorldCat] [Archive.org]
Sindi, R., Sá Dos Reis, C., Bennett, C., Stevenson, G., & Sun, Z. (2019). Quantitative Measurements of Breast Density Using Magnetic Resonance Imaging: A Systematic Review and Meta-Analysis. Journal of Clinical Medicine, 8(5), 745. [DOI:10.3390/jcm8050745]
Sitruk-Ware, R., Basdevant, A., de Lignières, B., & Mauvais-Jarvis, P. (1984). Percutaneous oestrogen therapy. In van Herendael, H., van Herendael, B., Riphagen, F. E., Goessens, L., & van der Plas, H. (Eds.). The Climacteric: An Update: Proceedings of the fourth Jan Palfijn Symposium, European Conference on the Menopause, held in Antwerp, Belgium, on September 1–2, 1983, under the auspices of ‘De Vereniging voor Nederlandstalige gynecologen van België’ and ‘The International Menopause Society’ (pp. 127–139). Lancaster: MTP Press. [Google Scholar] [Google Books] [OpenLibrary] [WorldCat] [DOI:10.1007/978-94-009-5608-7_14]
Sizonenko, P. C. (1978). Endocrinology in Preadolescents and Adolescents. American Journal of Diseases of Children, 132(7), 704–712. [DOI:10.1001/archpedi.1978.02120320064015]
Škarda, J., Fremrová, V., & Bezecný, I. (1989). Progesterone alone is responsible for stimulation of the growth of ducts and of mammary alveolar structures in mice. Endocrinologia Experimentalis, 23(1), 17–28. [Google Scholar] [PubMed] [PDF]
Sobrinho, L. G., Kase, N., & Grunt, J. A. (1971). Spontaneous pubertal breast growth in a castrated patient with the syndrome of testicular feminization. The Yale Journal of Biology and Medicine, 44(2), 225–9. [Google Scholar] [PubMed] [PubMed Central] [PDF]
Sosa, M., Jódar, E., Arbelo, E., Domínguez, C., Saavedra, P., Torres, A., Salido, E., de Tejada, M. J., & Hernández, D. (2003). Bone Mass, Bone Turnover, Vitamin D, and Estrogen Receptor Gene Polymorphisms in Male to Female Transsexuals. Journal of Clinical Densitometry, 6(3), 297–304. [DOI:10.1385/jcd:6:3:297]
Sosa, M., Jódar, E., Arbelo, E., Domı́nguez, C., Saavedra, P., Torres, A., Salido, E., Limiñana, J., Gómez de Tejada, M. J., & Hernández, D. (2004). Serum lipids and estrogen receptor gene polymorphisms in male-to-female transsexuals: effects of estrogen treatment. European Journal of Internal Medicine, 15(4), 231–237. [DOI:10.1016/j.ejim.2004.04.009]
Soyal, S., Ismail, P. M., Li, J., Mulac-Jericevic, B., Conneely, O. M., & Lydon, J. P. (2002). Progesterone receptors - animal models and cell signaling in breast cancer: Progesterone’s role in mammary gland development and tumorigenesis as disclosed by experimental mouse genetics. Breast Cancer Research, 4(5), 191. [DOI:10.1186/bcr451]
Sperling, R. L., & Gold, J. J. (1973). Use of an anti-estrogen after a reduction mammaplasty to prevent recurrence of virginal hypertrophy of breasts. Plastic and Reconstructive Surgery, 52(4), 439–442. [DOI:10.1097/00006534-197352040-00030]
Spitz, I. M., Shoupe, D., Sitruk-Ware, R., & Mishell, D. R. (1989). Response to the antiprogestagen RU 486 (mifepristone) during early pregnancy and the menstrual cycle in women. Journal of Reproduction and Fertility Supplement, 37, 253–260. [Google Scholar] [PubMed]
Spitz, I., Croxatto, H., Lahteenmaki, P., Heikinheimo, O., & Bardin, C. (1994). Effect of mifepristone on inhibition of ovulation and induction of luteolysis. Human Reproduction, 9(Suppl 1), 69–76. [DOI:10.1093/humrep/9.suppl_1.69]
Spitz, I. M. (2010). Mifepristone: where do we come from and where are we going? Contraception, 82(5), 442–452. [DOI:10.1016/j.contraception.2009.12.012]
Sridhar, G. R., & Sinha, M. J. (1995). Macromastia in adolescent girls. Indian Pediatrics, 32(4), 496–499. [Google Scholar] [PubMed] [PDF]
Sun, B. Z., Kangarloo, T., Adams, J. M., Sluss, P. M., Welt, C. K., Chandler, D. W., Zava, D. T., McGrath, J. A., Umbach, D. M., Hall, J. E., & Shaw, N. D. (2018). Healthy Post-Menarchal Adolescent Girls Demonstrate Multi-Level Reproductive Axis Immaturity. The Journal of Clinical Endocrinology & Metabolism, 104(2), 613–623. [DOI:10.1210/jc.2018-00595]
Sun, S. X., Bostanci, Z., Kass, R. B., Mancino, A. T., Rosenbloom, A. L., Klimberg, V. S., & Bland, K. I. (2018). Breast Physiology: Normal and Abnormal Development and Function. In Bland, K. I., Copeland, E. M., Klimberg, V. S., Gradishar, W. J., White, J., & Korourian, S. (Eds.). The Breast: Comprehensive Management of Benign and Malignant Diseases, 5th Edition (pp. 37–56.e6). Philadelphia: Elsevier. [DOI:10.1016/b978-0-323-35955-9.00003-9]
Swelstad, M. R., Swelstad, B. B., Rao, V. K., & Gutowski, K. A. (2006). Management of Gestational Gigantomastia. Plastic and Reconstructive Surgery, 118(4), 840–848. [DOI:10.1097/01.prs.0000232364.40958.47]
Tack, L. J., Heyse, R., Craen, M., Dhondt, K., Bossche, H. V., Laridaen, J., & Cools, M. (2017). Consecutive Cyproterone Acetate and Estradiol Treatment in Late-Pubertal Transgender Female Adolescents. The Journal of Sexual Medicine, 14(5), 747–757. [DOI:10.1016/j.jsxm.2017.03.251]
Talbert, L. M., Hammond, M. G., Groff, T., & Udry, J. R. (1985). Relationship of age and pubertal development to ovulation in adolescent girls. Obstetrics & Gynecology, 66(4), 542–544. [Google Scholar] [PubMed] [URL]
Tanos, T., & Brisken, C. (2008). What Signals Operate in the Mammary Niche? Breast Disease, 29(1), 69–82. [DOI:10.3233/bd-2008-29108]
Thanaboonyawat, I., Chanprapaph, P., Lattalapkul, J., & Rongluen, S. (2013). Pilot Study of Normal Development of Nipples during Pregnancy. Journal of Human Lactation, 29(4), 480–483. [DOI:10.1177/0890334413493350]
Thody, A. J., & Smith, A. G. (1977). Hormones and Skin Pigmentation in the Mammal. International Journal of Dermatology, 16(8), 657–664. [DOI:10.1111/j.1365-4362.1977.tb01876.x]
Thoresen, M., & Wesche, J. (1988). Doppler measurements of changes in human mammary and uterine blood flow during pregnancy and lactation. Acta Obstetricia et Gynecologica Scandinavica, 67(8), 741–745. [DOI:10.3109/00016349809004301]
Tiefenbacher, K., & Daxenbichler, G. (2008). The Role of Androgens in Normal and Malignant Breast Tissue. Breast Care, 3(5), 325–331. [DOI:10.1159/000158055]
Tim, F., Jeroen, V., & T’Sjoen, G. (2023). Dose Reduction of Cyproterone Acetate in Trans Women and the Effect on Patient-reported Outcomes: Results from the ENIGI Study. Endocrine Abstracts, 97 [Belgian Endocrine Society 2023], 5–5 (abstract no. 007). [URL] [PDF]
Trabert, B., Sherman, M. E., Kannan, N., & Stanczyk, F. Z. (2019). Progesterone and Breast Cancer. Endocrine Reviews, 41(2), 320–344. [DOI:10.1210/endrev/bnz001]
Tucker, H. (2000). Hormones, Mammary Growth, and Lactation: a 41-Year Perspective. Journal of Dairy Science, 83(4), 874–884. [DOI:10.3168/jds.s0022-0302(00)74951-4]
Turan, S., Bereket, A., Guran, T., Akcay, T., Papari-Zareei, M., & Auchus, R. J. (2009). Puberty in a case with novel 17-hydroxylase mutation and the putative role of estrogen in development of pubic hair. European Journal of Endocrinology, 160(2), 325–330. [DOI:10.1530/eje-08-0632]
Turner, C. W. (1939). The Mammary Glands. In Allen, E., Danforth, C. H., & Doisy, E. A. (Eds.). Sex and Internal Secretions: A Survey of Recent Research, 2nd Edition (pp. 740–803). Baltimore: Williams & Wilkins. [Google Scholar] [Google Books] [OpenLibrary] [WorldCat]
Ulrich, U., Pfeifer, T., & Lauritzen, C. (1994). Rapid Increase in Lumbar Spine Bone Density in Osteopenic Women by High-Dose Intramuscular Estrogen-Progestogen Injections. Hormone and Metabolic Research, 26(9), 428–431. [DOI:10.1055/s-2007-1001723]
Ulrich, U., Pfeifer, T., Buck, G., Keckstein, J., & Lauritzen, C. (1995). High-dose estrogen-progestogen injections in gonadal dysgenesis, ovarian hypoplasia, and androgen insensitivity syndrome: Impact on bone density. Adolescent and Pediatric Gynecology, 8(1), 20–23. [DOI:10.1016/s0932-8610(12)80156-3]
Valentine, G. H. (1969). Chromosome Anomalies in the Female. In Valentine, G. H. The Chromosome Disorders: An Introduction for Clinicians, 2nd Edition (pp. 126–143). London: W. Heinemann Medical Books. [Google Scholar] [Google Books] [OpenLibrary] [WorldCat] [Archive.org]
van der Meulen, A. J. (1974). An unusual case of massive hypertrophy of the breasts. South African Medical Journal=Suid-Afrikaanse Tydskrif vir Geneeskunde, 48(34), 1465–1466. [Google Scholar] [PubMed] [URL 1] [URL 2]
Vandeweyer, E., & Hertens, D. (2002). Quantification of glands and fat in breast tissue: An experimental determination. Annals of Anatomy - Anatomischer Anzeiger, 184(2), 181–184. [DOI:10.1016/s0940-9602(02)80016-4]
Venturoli, S., Fabbri, R., Porcu, E., Paradisi, R., Orsini, L. F., Brondelli, L., Ruggeri, S., & Flamigni, C. (1989). Endocrine and ovarian parameters at various frequencies of ovulation in adolescents. Archives of Gynecology and Obstetrics, 246(2), 107–114. [DOI:10.1007/bf00934127]
Venturoli, S., Porcu, E., Fabbri, R., Magrini, O., Paradisi, R., Pallotti, G., Gammi, L., & Flamigni, C. (1987). Postmenarchal evolution of endocrine pattern and ovarian aspects in adolescents with menstrual irregularities. Fertility and Sterility, 48(1), 78–85. [DOI:10.1016/s0015-0282(16)59294-2]
Vorherr, H. (1974). Development of the Female Breast. In Vorherr, H. The Breast: Morphology, Physiology, and Lactation (pp. 1–19). New York: Academic Press. [Google Scholar] [Google Books] [OpenLibrary] [WorldCat]
Vorherr, H. (1974). Morphology of the Mature Female Breast. In Vorherr, H. The Breast: Morphology, Physiology, and Lactation (pp. 20–70). New York: Academic Press. [Google Scholar] [Google Books] [OpenLibrary] [WorldCat]
Wade, T. R., Wade, S. L., & Jones, H. E. (1978). Skin changes and diseases associated with pregnancy. Obstetrics and Gynecology, 52(2), 233–242. [Google Scholar] [PubMed] [URL]
Walker, M., Baker, G., & Lamb, M. (2013). Physiology of the Breast During Pregnancy and Lactation. In Mannel, R., Martens, P. J., & Walker, M. (Eds.). Core Curriculum for Lactation Consultant Practice, 3rd Edition (pp. 287–300). Burlington: Jones & Bartlett Learning. [Google Scholar] [Google Books—2013/3rd Edition] [Google Books—2008/2nd Edition] [OpenLibrary] [WorldCat]
Wang, C., Luan, J., Cheng, H., Chen, L., Li, Z., Panayi, A. C., & Liu, C. (2018). Menstrual Cycle-Related Fluctuations in Breast Volume Measured Using Three-Dimensional Imaging: Implications for Volumetric Evaluation in Breast Augmentation. Aesthetic Plastic Surgery, 43(1), 1–6. [DOI:10.1007/s00266-018-1243-6]
Wang, Q. A., & Scherer, P. E. (2019). Remodeling of Murine Mammary Adipose Tissue during Pregnancy, Lactation, and Involution. Journal of Mammary Gland Biology and Neoplasia, 24(3), 207–212. [DOI:10.1007/s10911-019-09434-2]
Weisberg, M. G., Malkasian, G. D., & Pratt, J. H. (1970). Testicular feminization syndrome. American Journal of Obstetrics and Gynecology, 107(8), 1181–1187. [DOI:10.1016/s0002-9378(15)30367-7]
Wellons, M. F., & Rebar, R. W. (2013). Amenorrhea. In Falcone, T., & Hurd, W. W. (Eds.). Clinical Reproductive Medicine and Surgery: A Practical Guide, 2nd Edition (pp. 105–112). New York: Springer New York. [DOI:10.1007/978-1-4614-6837-0_7]
Wellons, M. F., Weeber, K. M., & Rebar, R. W. (2017). Amenorrhea. In Falcone, T., & Hurd, W. W. (Eds.). Clinical Reproductive Medicine and Surgery, 3rd Edition (pp. 109–122). Cham: Springer International Publishing. [DOI:10.1007/978-3-319-52210-4_6]
Werner, A. A. (1935). Experiment to produce lactation in castrate women. Endocrinology, 19(2), 144–150. [DOI:10.1210/endo-19-2-144]
Whiteley, S. (1994). Predictors of Milk Production in Lactating Women. (Master’s thesis, The Open University.) [Google Scholar] [DOI:10.21954/ou.ro.0000fe02] [URL]
Wierckx, K., Gooren, L., & T’Sjoen, G. (2014). Clinical Review: Breast Development in Trans Women Receiving Cross-Sex Hormones. The Journal of Sexual Medicine, 11(5), 1240–1247. [DOI:10.1111/jsm.12487]
Wierckx, K., Van Caenegem, E., Schreiner, T., Haraldsen, I., Fisher, A., Toye, K., Kaufman, J. M., & T’Sjoen, G. (2014). Cross‐Sex Hormone Therapy in Trans Persons Is Safe and Effective at Short‐Time Follow‐Up: Results from the European Network for the Investigation of Gender Incongruence. The Journal of Sexual Medicine, 11(8), 1999–2011. [DOI:10.1111/jsm.12571]
Wilson, J. D. (1968 March 28). Medical Grand Rounds: Testicular Feminization. Parkland Memorial Hospital, UT Southwestern Medical Center. [Google Scholar] [URL] [PDF]
Wilson, C. L., Sims, A. H., Howell, A., Miller, C. J., & Clarke, R. B. (2006). Effects of oestrogen on gene expression in epithelium and stroma of normal human breast tissue. Endocrine-Related Cancer, 13(2), 617–628. [DOI:10.1677/erc.1.01165]
Winkler, U. H., Schindler, A. E., Brinkmann, U. S., Ebert, C., & Oberhoff, C. (2001). Cyclic progestin therapy for the management of mastopathy and mastodynia. Gynecological Endocrinology, 15(Suppl 6), 37–43. [DOI:10.1080/gye.15.s6.37.43]
Wisniewski, A. B., Migeon, C. J., Meyer-Bahlburg, H. F., Gearhart, J. P., Berkovitz, G. D., Brown, T. R., & Money, J. (2000). Complete Androgen Insensitivity Syndrome: Long-Term Medical, Surgical, and Psychosexual Outcome. The Journal of Clinical Endocrinology & Metabolism, 85(8), 2664–2669. [DOI:10.1210/jcem.85.8.6742]
Wong, R. C., & Ellis, C. N. (1984). Physiologic skin changes in pregnancy. Journal of the American Academy of Dermatology, 10(6), 929–940. [DOI:10.1016/s0190-9622(84)80305-9]
Wren, B. G., & Eden, J. A. (1996). Do Progestogens Reduce The Risk of Breast Cancer? A Review of the Evidence. Menopause, 3(1), 4–12. [DOI:10.1097/00042192-199603010-00003]
Wright, E. M. (2015). Breastfeeding and the Mother–Newborn Dyad (pp. 1157–1182). In King, T. L., Brucker, M. C., Kriebs, J. M., Fahey, J. O., Gegor, C. L., & Varney, H. (Eds.). Varney’s Midwifery, 5th Edition. Burlington: Jones & Bartlett Learning. [Google Scholar] [Google Books] [OpenLibrary] [WorldCat]
Xu, P., Ye, W., Zhong, S., Li, H., Feng, E., Lin, S. H., Kuo, C. T., Liu, J. Y., & Lin, Y. C. (2010). Leptin and zeranol up-regulate cyclin D1 expression in primary cultured normal human breast pre-adipocytes. Molecular Medicine Reports, 3(6), 983–990. [DOI:10.3892/mmr.2010.370]
Yang, W., Hong, T., Chang, X., Han, M., Gao, H., Pan, B., Zhao, Z., & Liu, Y. (2024). The efficacy of and user satisfaction with different antiandrogens in Chinese transgender women. International Journal of Transgender Health, advance online publication. [DOI:10.1080/26895269.2024.2323514]
Zacharin, M. (2000). Use of androgens and oestrogens in adolescents - A review of hormone replacement treatment. Journal of Pediatric Endocrinology and Metabolism, 13(1), 3–12. [DOI:10.1515/JPEM.2000.13.1.3]
Zachmann, M., Prader, A., Sobel, E. H., Crigler, J. F., Ritzén, E. M., Atarés, M., & Ferrandez, A. (1986). Pubertal growth in patients with androgen insensitivity: Indirect evidence for the importance of estrogens in pubertal growth of girls. The Journal of Pediatrics, 108(5), 694–697. [DOI:10.1016/s0022-3476(86)81043-5]
Żelaźniewicz, A., & Pawłowski, B. (2015). Breast size and asymmetry during pregnancy in dependence of a fetus’s sex. American Journal of Human Biology, 27(5), 690–696. [DOI:10.1002/ajhb.22716]
Żelaźniewicz, A., & Pawłowski, B. (2018). Maternal breast volume in pregnancy and lactation capacity. American Journal of Physical Anthropology, 168(1), 180–189. [DOI:10.1002/ajpa.23734]
Zhang, D., Yao, F., Tian, T., Deng, S., Luo, M., & Tian, Q. (2021). Clinical characteristics and molecular genetics of complete androgen insensitivity syndrome patients: a series study of 30 cases from a Chinese tertiary medical center. Fertility and Sterility, 115(5), 1270–1279. [DOI:10.1016/j.fertnstert.2020.12.008]
\ No newline at end of file
+A Comprehensive Review of the Potential of Progestogens for Enhancing Breast Development in Transfeminine People - Transfeminine Science
A Comprehensive Review of the Potential of Progestogens for Enhancing Breast Development in Transfeminine People
By Aly | First published February 14, 2020 | Last modified June 28, 2024
Abstract / TL;DR
The major female sex hormones are estrogen and progesterone. Both of these hormones are known to be importantly involved in the development of the breasts at different stages of life. Speculation, use, and anecdotes of progestogens for enhancing breast development in transfeminine people date back to at least the 1960s. A limited number of clinical studies have assessed breast development with progestogens in transfeminine people, but current evidence on progestogens for improving breast development is of very low quality and is inconclusive. Studies of progestogens and breast development in cisgender girls and women are similarly limited. In any case, more studies evaluating progestogens and breast development are currently underway. The possible role of progestogens in enhancing breast development can also be informed by indirect and circumstantial evidence, including notably findings on progesterone and breast changes during normal puberty, the menstrual cycle, and pregnancy in humans and animals. Available evidence overall is not suggestive of an essential role for progesterone in breast growth during puberty, but progesterone does have a clear and key role in lobuloalveolar development of the breasts during pregnancy. However, breast changes in pregnancy revert following cessation of lactation and breastfeeding. Progesterone may additionally contribute to reversible breast enlargement during the luteal phase of the menstrual cycle. There are some findings to suggest that progestogens may have antiestrogenic effects in the breasts and may have a stunting influence on breast development if introduced too early following initiation of hormone therapy. However, more research is needed to assess this possibility. In any case, if progestogens are used, it may be advisable to delay their introduction until most or all estrogen-mediated breast development is complete. Options for progestogen therapy in transfeminine people include bioidentical progesterone and progestins. However, oral progesterone has major bioavailability problems and does not achieve satisfactory progesterone levels. Progestogens, including progesterone, have been variously linked to significant health risks, which is an important consideration in terms of their use in transfeminine people. Overall, based on current knowledge, progestogens do not seem to be promising for lastingly improving breast development in transfeminine people, but more research and data are still needed for clear conclusions.
Introduction
Breast development in terms of size and shape is often less than desired in transfeminine people, and there is a need for therapeutic approaches that improve breast growth in this population. There are two major types of female hormones, estrogens and progestogens. Estrogens are almost universally employed in transfeminine hormone therapy, while progestogens are used in a subset of transfeminine people. Progestogens that have been commonly employed in transfeminine people include bioidenticalprogesterone, the progestin (synthetic progestogen) medroxyprogesterone acetate (MPA), and the strongly progestogenic antiandrogen cyproterone acetate (CPA). Estrogens are the major mediators of feminization and breast development in females. However, progestogens also have physiological effects on the breasts, and in relation to this, may or may not provide benefits to breast development as well.
The topic of progestogens and breast development has been discussed for many years in the transgender community and is a controversial subject (Coleman et al., 2012). Use of progestogens to improve breast development in transfeminine people goes back at least as far as Harry Benjamin and Christian Hamburger in the 1960s (Benjamin, 1966; Benjamin, 1967; Hamburger & Benjamin, 1969; Wiki). Arguments have been made both for (e.g., Bevan, 2012; Bellwether, 2019; Bevan, 2019) and against (e.g., Curtis, 2009) a possible role of progestogens in terms of breast development. It is often claimed that progestogens can enhance breast development or are even required for full breast development in cisgender females and transfeminine people. With respect to the latter, it is sometimes said that progestogens are necessary for people to move from Tanner stage 4 to Tanner stage 5 pubertal breast development and that progestogens help to fill and round out the breasts (e.g., Vorherr, 1974a; Basson & Prior, 1998; Kaiser & Ho, 2015; Prior, 2011; Prior, 2019a; Prior, 2020). It has even been claimed by some that without progestogens, the breasts will remain conical and “pointy” like they are in the earlier Tanner stages. On the other extreme, certain critics have claimed that there are “no biologically significant progesterone receptor sites for biological males” and that progesterone is not produced during normal female puberty until after breast development has been fully completed (Barrett, 2009; Seal, 2017; Coxon & Seal, 2018; Price, McManus, & Barrett, 2019; Richards & Barrett, 2020). In turn, these particular authors have argued against the use of progestogens in transfeminine people in various of their publications (Google Scholar). In general, the use of progestogens in transfeminine people has longstandingly been controversial, with positions both for and against (Sam, 2020).
The purpose of this article is to review the available direct and circumstantial evidence on the topic of progestogens and breast development in order to help inform whether progestogen therapy may be able to enhance breast development in transfeminine people. Aside from an involvement in breast development, progestogens are not otherwise currently thought to be or known to be involved in physical feminization (e.g., Coleman et al., 2012; Gooren, 2016). In relation to this, the present article will limit its discussion to breast development with progestogens, and will not explore feminization in general.
Progestogen Therapy and Breast Development in Humans
Progestogens and Breast Development in Transfeminine People
Orentreich & Durr (1974) was one of the earliest studies on breast development in transfeminine people. They employed combinations of estrogens and progestogens as well as gonadectomy to produce feminization and breast development in a case series of 5 transfeminine people. The employed estrogens were estradiol valerate 30 mg/2 weeks by intramuscular injection and oral conjugated estrogens 1.25–5.0 mg/day and the used progestogens were “60 mg medroxyprogesterone caproate” every 2 weeks by intramuscular injection and oral medroxyprogesterone acetate 0–10 mg/day. Medroxyprogesterone caproate (MPC) has never been used pharmaceutically, so this was likely a typo and the actual progestogen employed was likely either MPA or hydroxyprogesterone caproate (OHPC). The authors reported that estrogen and progestogen therapy produced modest to significant breast development in the transfeminine people that was not strictly dose-related and included clinical photographs of the breasts. They concluded that the breast development was comparable to that of adult cisgender women. Orentreich and colleagues also discussed the topic of lobuloalveolar maturation of the breasts, which was known to be progestogen-dependent, but noted that they had not done histological assessment and that the degree of lobuloalveolar development of the breasts does not necessarily correlate with clinical breast size per findings in cisgender women. The findings of Orentreich and colleagues are limited by methodological problems like lack of objective measurements, lack of estrogen-only controls, and the small sample size of only 5 transfeminine people, and hence the study is of limited value in terms of assessing the involvement of progestogens in breast development.
Meyer et al. (1986) assessed the effects of progestogens added to estrogen therapy on breast development and other clinical parameters in transfeminine people. Of the 60 transfeminine people in the study, 15 (25%) received an oral progestogen, usually MPA at a dosage of 10 mg/day, for “at least for a short time”, and with only 8 (13.3%) receiving progestogen therapy for the full treatment period. In an earlier report of the study, it was noted that in 90% of observation periods the dose was 10 mg/day and for the remainder it was 20 mg/day (Meyer et al., 1981). A dosage of 10 mg/day MPA is roughly comparable to luteal-phase progesterone exposure in terms of progestogenic potency (Wiki). Breast development was measured in the study via breast hemicircumference (Diagram). Progestogen therapy was reported to not modify estrogen-induced changes, including laboratory measurements, hormone levels, and physical parameters like weight and breast growth. The lack of apparent changes in hormone levels is unexpected, as MPA in higher-quality studies has shown clear testosterone suppression (e.g., Jain, Kwan, & Forcier, 2019; Wiki). Meyer and colleagues concluded that adding progestogens to estrogen does not seem to enhance breast development in transfeminine people. However, they noted that the number of individuals who received progestogens was small and further studies were needed.
Prior et al. (1986) and Prior, Vigna, & Watson (1989) studied estrogen, high-dose spironolactone (100–600 mg/day), and MPA (10–20 mg/day cylically or continuously) in transfeminine people who were either pre-hormone therapy or had previously been on higher doses of estrogens (and/or progestogens) without spironolactone prior to the study. The researchers reported that following 12 months of treatment with the study’s hormone therapy regimen, there was increased breast size and increased nipple development. Most individuals reached an A cup size, or approximately 8 to 14 cm in diameter of breast tissue, by the end of the study. Breast development was measured in part with photographic documentation. Although breast development reportedly improved, the researchers themselves noted that it was difficult to determine whether the enhanced breast development could be attributed to spironolactone or to MPA. Moreover, testosterone suppression was inadequate before the study and improved with the study’s hormone therapy regimen, which may have helped to improve breast development regardless of any potential direct progestogenic action of MPA on the breasts. Finally, it is possible that breast development with estrogen may not yet have been complete, and that the improved breast development may have simply been continued progression due to estrogen alone. In other publications, Jerilynn Prior, the lead study author, has claimed that progesterone enhances breast development, and has cited the preceding studies by her in support of this claim (Prior, 2011; Prior, 2019a; Prior, 2019b; Prior, 2020). However, her claim is not well-supported due to the study limitations discussed.
Dittrich et al. (2005) reported that the combination of oral estradiol valerate and a gonadotropin-releasing hormone (GnRH) agonist for 2 years in transfeminine people resulted in self-reported breast cup sizes of C cup or greater in 5%, B cup in 30%, A cup in 35%, and less than A cup in 30%. They noted however that 70% of the individuals were unsatisfied with their breast development and wished to undergo breast augmentation surgery. The researchers claimed that the regimen had similar effectiveness in terms of feminization, including increases in breast size, compared to prior reported treatment regimens of ethinylestradiol and CPA. No other details or specifics were given. The claim about similar breast development to regimens containing CPA is relevant as CPA is a very strong progestogen at the doses used historically in transfeminine people (Aly, 2019). It should be cautioned however that this study did not actually employ or study progestogen therapy itself. In addition, self-reported breast cup size is a subjective and low-quality means of measuring breast development and size. As such, the findings of this study are of questionable value in terms of understanding progestogens and breast development.
Estrogen is primarily involved in ductal development of the breasts, whereas progesterone is mainly involved in lobuloalveolar development. Kanhai et al. (2000) compared internal histological breast tissue changes with estrogen and CPA 100 mg/day (i.e. very-high-dose progestogen) therapy in 14 transfeminine people versus nonsteroidal antiandrogen monotherapy with flutamide or bicalutamide in 2 cisgender men with prostate cancer. Both types of treatments block androgens, increase estrogen levels, and are known to induce breast development or gynecomastia at similarly high rates. However, nonsteroidal antiandrogen monotherapy differs from combined estrogen and progestogen therapy in that it lacks any progestogenic effects. In the transfeminine people, full lobuloalveolar formation was apparent in the biopsied breast tissue, whereas in the men with prostate cancer, only “moderate” and incomplete lobuloalveolar maturation was found. It was also noted that lobuloalveolar formation tended to regress upon discontinuation of CPA following gonadectomy in transfeminine people. The researchers concluded that progestogenic exposure is needed for the breasts to fully develop on a histological level and for the breast tissue of transfeminine people to completely mimic the histology of the mature female breast. While the findings of this study are interesting, they only concern tissue characteristics and do not actually provide any information about breast development in terms of physical form or appearance. With regard to this, tissue-level differences may or may not translate to relevant differences in for instance breast size or shape. As such, the study is of limited value in understanding whether progestogens improve breast development in transfeminine people in the ways that are actually valued.
Seal and colleagues conducted a retrospective chart review assessing clinical predictors for surgical breast augmentation in transfeminine people (Seal et al., 2012). In the transfeminine people who underwent breast augmentation, significantly more of them were taking spironolactone than were those who did not undergo breast augmentation. Conversely, the differential rates of use of specific antiandrogens were not significantly discordant between those who did and did not undergo breast augmentation in the case of the other prescribed antiandrogens, including cyproterone acetate, the 5α-reductase inhibitors, and GnRH analogues. However, this study had many methodological limitations, including the use of almost three dozen t-tests with no adjustment for multiple comparisons (and hence risk of false positives and concerns about p-hacking), small sample sizes for individual antiandrogens, use of undergoing breast augmentation as a surrogate for breast development with no actual physical measurement of the breasts or breast sizes, and a correlational design with lack of control for potential confounding variables. As such, the study does not show that different antiandrogens result in differences in breast development, and its findings must be considered with due caution.
Jain, Kwan, & Forcier (2019) studied sublingual estradiol and spironolactone with and without MPA in 92 transfeminine people. MPA was given at a dose of 5 to 10 mg/day sublingually or at a dose of 150 mg once every 3 months by intramuscular injection. Of 39 transfeminine people who received MPA, 26 (67%) self-reported improved breast development. No further details were provided, but measurement of breast development was presumably subjective and anecdotal. Igo & Visram (2021) studied addition of progesterone to hormone therapy in transfeminine people. Progesterone was provided as 100 mg micronized progesterone (probably oral) and was prescribed when progesterone was specifically requested by the patient or when the patient expressed dissatisfaction with feminization and/or breast development. Of 190 individuals, 51 (26.8%) received progesterone therapy. Treatment with progesterone on average began after 12.7 months of estradiol therapy, and the mean total follow-up time was 14.3 months of hormone therapy. Of those who received progesterone, only 6 (11.8%) reported benefit to breast development. No further details were provided, but as with other studies, breast development was likely quantified anecdotally via self-report. As breast development does not appear to have been objectively measured or compared to a control group in either Jain, Kwan, & Forcier (2019) or Igo & Visram (2021), the findings of these studies are limitedly informative.
Nolan and colleagues assessed the short-term effects of low-dose oral micronized progesterone on breast development in transfeminine people on stable hormone therapy in a prospective controlled study (Nolan et al., 2022a; Nolan et al., 2022b). Progesterone was given at a dose of 100 mg/day for 3 months to 23 transfeminine people and findings were compared to those of a control group of 19 transfeminine people. Breast development was measured using self-reported Tanner stage, with participants provided photographs of different Tanner stages to self-select from. At the end of the 3 months, Tanner stage was not significantly different between groups (mean 3.5, 95% CI 3.2–3.7 for progesterone vs. mean 3.6, 95% CI 3.3–3.9 for controls; p = 0.42). A limitation of this study is that oral progesterone has very low bioavailability and 100 mg/day oral progesterone achieves very low progesterone levels that are well below normal luteal-phase progesterone levels (Aly, 2018a; Wiki). As such, progestogenic exposure in this study, and notably also in Igo & Visram (2021) and other studies, is likely to have been inadequate. Besides the issue of progestogenic strength, the very short duration of the study (3 months) and the reliance on self-reported subjective Tanner stages (as opposed to more objective physical breast measurements) are also major limitations. In any case, this study is of higher quality than previous studies, and is notably likely to continue and report further follow-up at later points in the future.
Bahr et al. (2024) conducted a retrospective chart review at their clinic and compared 29 transfeminine people who had received progestogens versus 59 transfeminine people who had not. The form of progestogen used was oral or rectal progesterone in 93% of cases and MPA by intramuscular injection in the remaining 7% of cases. Of those who took progesterone, 25 (93%) used it orally and 2 (7%) used oral progesterone capsules rectally. Progestogen doses were not reported, except that 100 mg progesterone capsules were employed. Most of those in the progestogen-treated group (59%) had started it 1 to 6 months following initiation of standard hormone therapy. The researchers found that progestogen-treated group had significantly better self-reported breast development satisfaction (rated as satisfied, neutral, or unsatisfied) compared to the group that did not receive progestogens at 6 months (satisfied: 53.8% vs. 19.6%; p = 0.004) and 9 months (satisfied: 71.4% vs. 20.8%; p = 0.003) of hormone therapy. Limitations of this study include the lack of objective measurement of breast development, the restrospective nature of the study, and the lack of randomization of treatment, among others.
Aside from the above studies, a variety of other studies have also reported breast development with estrogen and CPA in transfeminine people. These studies have often employed objective physical measurements of breast development (e.g., breast volume, breast–chest difference, breast cup size, breast hemicircumference). However, they have lacked comparison groups, thereby precluding comparison of progestogenic versus non-progestogenic hormone therapy. In addition, CPA is unusual among progestogens in that it is employed at very high doses in transfeminine people (Aly, 2019), which may result in different and potentially stunted outcomes in terms of breast development than more physiological progestogenic exposure. As such, most studies of breast development with estrogen and CPA in transfeminine people have not been discussed in the present section and are instead discussed elsewhere in this article (see the section below). In any case, to briefly summarize the findings, breast development in transfeminine people with estrogen and CPA has generally been poor in these studies. The outcomes have included incomplete maturation in terms of Tanner staging (stage 2–4), small cup sizes, small breast volumes, and breasts much smaller in size than those in cisgender women.
The findings from the preceding studies in transfeminine people are of very low-quality due to methodological limitations, including lack of control groups, lack of randomization, reliance on poor measures of breast development (e.g., subjective and self-report) rather than objective physical measurements (Wiki), short treatment durations, and small sample sizes, among others. This may explain the conflicting results of the studies. More research is still needed to assess the influence of progestogens on breast development in transfeminine people. There is specifically a need for randomized controlled trials (RCTs) of feminizing hormone therapy with versus without progestogen therapy that employ objective measures of breast development, have adequate sample sizes, and have sufficient follow-up durations. Additional variables like progestogen type, route, dose, and timing of introduction would also be of value to explore. A 2014 review on hormone therapy in transfeminine people summarizes the state of research on progestogens and breast development in transfeminine people, with their conclusions still holding true today (Wierckx, Gooren, & T’Sjoen, 2014):
Our knowledge concerning the natural history and effects of different cross-sex hormone therapies on breast development in trans women is extremely sparse and based on low quality of evidence. Current evidence does not provide evidence that progestogens enhance breast development in trans women. Neither do they prove the absence of such an effect. This prevents us from drawing any firm conclusion at this moment and demonstrates the need for further research to clarify these important clinical questions.
Several studies of progesterone and other progestogens in transfeminine people are currently underway. These studies include (1) an RCT of oral progesterone added to hormone therapy by Sandeep Dhindsa and colleagues in St. Louis, Missouri in the United States (ClinicalTrials.gov; MediFind; ICH GCP); (2) a prospectiveobservational study and/or RCT of addition of oral progesterone to hormone therapy by Ada Cheung and colleagues in Melbourne, Australia (University of Melbourne; University of Melbourne); (3) an RCT of estradiol plus spironolactone versus estradiol plus CPA also by Ada Cheung and colleagues (ANZCTR; WHO ICTRP; Trans Health Research [Flyer] [Poster]; University of Melbourne) (update: see below); and (4) a large RCT of oral progesterone at different doses added to hormone therapy by Martin den Heijer and colleagues at the Vrije Universiteit University Medical Center (VUMC) in Amsterdam, the Netherlands (Dijkman et al., 2023a; General Info/Links; Info Sheet Dutch; Info Sheet English Translated). Unfortunately however, all of the studies using progesterone employ oral progesterone, which has major bioavailability and potency problems (Aly, 2018a; Wiki). In any case, it was said that the VUMC researchers may follow their trial up with studies of other progesterone routes (General Info/Links). The preceding studies may provide more insight on the question of whether progestogen therapy is of therapeutic benefit to breast development in transfeminine people.
Progestogens and Breast Development in Cisgender Females
To date, there appear to be no useful studies on breast development with progesterone or other progestogens in cisgender females. There seem to mostly only be a few brief and conflicting anecdotal clinical statements in this area that are scattered throughout the literature. These include the following literature excerpts, which are specifically in the context of progestogens as part of puberty induction in cisgender girls and women with delayed or absent puberty due to hypogonadism:
I […] performed studies on three women lacking mammary development and exhibiting signs of marked hypogonadism. […] Corpus luteum extract, 5 international units daily for a period of thirty days, when given alone produced no detectable change in the breasts. This is in accord with the experimental observations on animals of Turner,2 Corner 3 and others. When, however, patients were given alternate daily injections of 1 international unit of progesterone and from 20,000 to 50,000 international units of estrone or of estradiol benzoate, breast growth was more rapid than that produced by the estrogenic hormones alone. The simultaneous use of the corpus luteum and estrogenic therapy definitely produced a much firmer breast growth, which was distinctly lobular to palpation, whereas the growth produced by the estrogenic hormones alone was smooth and the borders of the glandular tissue were difficult to define. Rapid regression in the size of the breasts followed the omission of the hormone injections, but the regression was less rapid when the combined therapy had been used. [MacBryde (1939)]
There are authorities who consider that breast growth is better if a progestogen is combined with oestrogen for the latter part of the cycle of treatment (Capraro, 1971). Shearman (1971) employs sequential therapy in his cases. Huffman (1971) however, does not believe that there is any improvement with the addition of progestogens. [Dewhurst (1971a)]
The effects of progesterone on the human breast remain obscure. Although widely stated to cause glandular development, the evidence for this is slender (Benson et al 1959). [Shearman (1972a)]
Many people use oestrogens alone, but the addition of a progestin for 6 or 10 days each month gives much better cycle control and appears to cause better breast development. [Shearman (1972b)]
Some authorities consider that breast growth is better if a progestogen is given for the latter part of each course of treatment. [Capraro & Dewhurst (1975)]
It has been suggested that progestins be added during the last week of each cycle of estrogen therapy in order to develop more rounded breasts rather than the conical breasts many of these patients develop, but we have been unable to detect any difference in breast contour with or without progestins. [Davajan & Kletzky (1979)]
I have been satisfied that the addition of a progestogen was necessary to get a good breast response to hormone treatment although the progestogen, as I have said, is required after the first year if the uterus is present. [Dewhurst (1982)]
In addition to the preceding instances, Werner (1935) and Geschickter (1945) assessed the effects of progesterone on the breasts in cisgender women. Werner (1935) attempted to induce lactation in 8 surgically gonadectomized cisgender women with combinations of estrogen, progesterone, and prolactin, all in the form of crude extracts by injection. In two women who were given progesterone, he claimed that a marked increase in the size of the breasts beyond that with estrogen alone was observed. Additionally, he claimed that the breasts were more firm, the glandular tissue “more tortuous and nodular”, and the nipples more prominent. He was not successful in inducing lactation in the women in this study. The doses of hormones used were unclear as they were in the form of extracts, and were likely supraphysiological, potentially pregnancy-like due to the nature of the experiment. Werner’s study was also briefly discussed by Nelson (1936), among other citations. Geschickter (1945) observed lobuloalveolar growth on histological examination with administration of progesterone for 6 weeks to 2 months in one woman but not in another woman. However, the exterior physical changes of the breasts were not assessed or reported by this author and hence his findings are limitedly informative.
Surprisingly, there have been few analogous studies of the effects of progestogens on the breasts in cisgender girls and women following the preceding reports and anecdotes. Although there are very little data on progestogens and breast growth in cisgender females, clinical studies are finally starting to look more closely at the specifics of hormonal medications, including progestogens, in terms of breast development in girls undergoing puberty induction (e.g., Rodari et al., 2023). As such, future studies may provide more insight on the subject of progestogens and breast development in cisgender females.
Progesterone and its Physiological Role in Breast Development in Humans
Progesterone and Breast Development in Puberty
The role of progesterone in breast development and its possible usefulness for helping with breast development in transfeminine hormone therapy can be informed by the normal biological circumstances of puberty in cisgender females. Puberty in cisgender girls usually starts around age 11 (range 8–13 years) and completes around age 15 years (range 12–19 years), taking on average 3 to 4 years (but with a range of about 1.5–6 years in most cases) (Schauffler, 1942; Marshall & Tanner, 1969; Marshall, 1978; Begley, Firth, & Hoult, 1980; Drife, 1986). Progesterone essentially does not appear during puberty until ovulatorymenstrual cycles begin. Menarche, the onset of menstruation and hence of menstrual cycling, occurs on average at Tanner breast stage 4 or about 13 years of age, although it occurs at Tanner breast stage 3 or Tanner breast stage 5 in significant subsets of girls (26% for Tanner stage 3, 62% for Tanner stage 4, and 10% for Tanner stage 5) (Marshall & Tanner, 1969; Marshall, 1978; Drife, 1986; Hillard, 2007). Hence, the appearance of progesterone in normal female puberty is a relatively late event (Scott et al., 1950; Marshall, 1978; Begley, Firth, & Hoult, 1980; Drife, 1986), and most breast development appears to be complete by menarche and thus by the time that progesterone is first produced (Huffman, Dewhurst, & Capraro, 1981; Drife, 1982). Moreover, a small but significant subset of girls reaches Tanner breast stage 5 and hence fully developed breasts before menarche (Edmonds, 1989), which suggests that progesterone may not be essential for complete pubertal breast development.
Only a handful of studies and sources have reported progesterone levels during puberty across Tanner stages or by age in cisgender girls (e.g., Sizonenko, 1978 [Graph]; Kühnel, 2000; Lee, 2001 [Table]; Aly, 2020a). They corroborate the above findings with regard to limited progesterone exposure during puberty. The “A Girl’s First Period Study” is an ambitious research project announced in 2022 that aims to better characterize reproductive hormone levels in pubertal and adolescent girls and may shed more light on the physiological role of progesterone during puberty (Lucien et al., 2022). The researchers have specifically highlighted the possible role of progesterone in breast development as part of their interests:
Does exposure to low levels of [progesterone (P4)], as occurs before menarche, during anovulatory cycles with some degree of follicle luteinization, and during early, immature ovulatory cycles play an important role in normal breast development during puberty? This question has important clinical implications as hormone replacement during puberty does not typically include low-dose P4; rather, it is conducted using a staggered approach of estrogen-only therapy followed by the addition of full adult doses of exogenous P4 only after 2 years or when breakthrough bleeding occurs.27 This is done to avoid development of tubular breasts, although there are limited data linking early P4 exposure to suboptimal breast development.28
Taken together, production of progesterone is a late event in normal female puberty, and even once it does begin, exposure to progesterone is low and sporadic until well after puberty has completed. Moreover, a subset of girls complete breast development before progesterone production starts. These facts call into some question the role of progesterone in breast development in female puberty, as most breast development appears to be complete prior to the appearance of progesterone. However, more research is still needed on the role of progesterone in breast development during normal puberty.
On the basis of normal female puberty, it seems it may be advisable that if progestogens are introduced in an attempt to enhance breast development in transfeminine people, their introduction be delayed until after 2 or 3 years of hormone therapy, so as to mimic the normal progestogenic exposure of puberty.
Progesterone and Breast Development in Pregnancy
During pregnancy, under the influence of ovarian hyperstimulation and placental formation, there are profound changes in hormonal profiles, including of hormones like estrogen, progesterone, and prolactin, among many others (Table 1). Comparing hormone levels during the menstrual cycle to those during the third trimester of pregnancy, estradiol levels increase on the order of 100-fold, progesterone levels increase on the order of 10- to 20-fold, and prolactin levels increase by around 10-fold (Table 1). Levels of numerous other hormones also change considerably during pregnancy, for instance other estrogens besides estradiol, androgens, gonadotropins (e.g., human choronic gonadotropin or hCG), human placental lactogen (hPL), relaxin, adrenocorticotropic hormone (ACTH), cortisol, aldosterone, growth hormone (GH), and insulin-like growth factor 1 (IGF-1), among others (Goodman, 2009 [Figure]; Mesiano, 2019). These hormones are variously produced by the ovaries, the placenta, and the pituitary gland, among other glands. In response to the myriad hormonal changes during pregnancy, there are dramatic changes to the breasts, which prepare the mother for postpartumlactation and breastfeeding.
Table 1: Changes in hormone levels (estradiol, progesterone, and prolactin) during normal pregnancy:
There are large and dramatic changes in levels of numerous hormones during pregnancy, and the exact hormones responsible for the breast changes during pregnancy are not known (Hytten & Leitch, 1971a; Hytten, 1976). However, it is considered likely, on the basis of animal studies, that a variety of hormones, including estrogen, progesterone, prolactin, placental lactogen, glucocorticoids, and growth hormone, are all importantly involved in different aspects of the maturation (Hytten & Leitch, 1971a; Hytten, 1976; Cox et al., 1999). Moreover, in a quantitative clinical study of breast changes during pregnancy, increases in breast volume and areola size were positively correlated with levels of hPL, while increases in nipple size were positively correlated with levels of prolactin (Cox et al., 1999). Progesterone and prolactin have specifically been implicated in the lobuloalveolar development of the breasts during pregnancy (Bässler, 1970; Lee & Ormandy, 2012; Obr & Edwards, 2012). Both hormones appear to be independently essential in normal lobuloalveolar growth per animal studies (Obr & Edwards, 2012; McNally & Stein, 2017; Hannan et al., 2023). Prolactin likewise appears to be essential in humans, based on case reports of lactation failure in women with isolated prolactin deficiency (Buhimschi, 2004). Conversely, hPL may not be essential for lactation based on case reports of normal lactation in women with very low levels of hPL during pregnancy (Gaede, Trolle, & Pedersen, 1978; Hannan et al., 2023).
On the basis of the preceding, in spite of rather extreme hormonal stimulation, the breast changes of pregnancy, although quite dramatic, are essentially temporary and fully reversible, remaining only as long as continuous hormonal exposure is maintained. This hormonal stimulation includes exposure to extremely high levels of progesterone. It would seem, based on pregnancy, that once pubertal breast development is completed, the breasts are rather unamenable to permanent further growth, whether that involves exposure to progestogens or to a variety of other hormones known to act on the breasts.
Breast Composition and Lobuloalveolar Tissue Proportion
The breasts are made up of two main types of tissue: (1) epithelial tissue, the actual functional internal mammary glandular tissue, including ducts and alveoli or lobules; and (2) stromal tissue, a mixture of connective tissue and adipose (fat) tissue. Lobuloalveolar development refers to growth and maturation of the alveoli and lobules, and hence is a form of epithelial or glandular development. Progestogens are involved primarily in lobuloalveolar development of the breasts, which is the type of breast development that is necessary for lactation and breastfeeding and that occurs mainly during pregnancy.
During pregnancy and lactation in humans, the breasts undergo dramatic changes, and epithelial tissue comes to make up a much greater proportion of the breasts (Ramsay et al., 2005; Bland, Copeland, & Klimberg, 2018). In fact, sources state that glandular tissue comprises a majority of the breast during pregnancy and lactation, with one study of lactating women finding that the breasts were composed 63% (range 46–83%) of glandular tissue (Ramsay et al., 2005). This is not merely due to lobuloalveolar development and glandular growth, but is also due to a marked reversible reduction in mammary adipose tissue (Wang & Scherer, 2019; Alex, Bhandary, & McGuire, 2020). In any case, under more normal physiological circumstances and progesterone exposure, the contribution of lobuloalveolar tissue to the size of the breasts would appear to be quite small. In relation to this, outside of pregnancy levels of progesterone, the significance of progestogen-mediated breast lobuloalveolar growth in terms of breast size is unclear but seemingly questionable (Orentreich & Durr, 1974; Wierkcx, Gooren, & T’Sjoen, 2014).
Breast Development in Cisgender Women with Complete Androgen Insensitivity Syndrome and Consequent Absence of Progesterone
It has been claimed that progesterone helps to move transfeminine people and cisgender females from Tanner stage 4 to 5 breast development and that it helps to round out the breasts (e.g., Vorherr, 1974a; Prior, 2011; Prior, 2019a; Prior, 2020). It has also sometimes been claimed in the online transgender community that cisgender women with complete androgen insensitivity syndrome (CAIS), an experiment of nature of women who lack progesterone, are stuck at Tanner stage 4 breast growth and have “cone-shaped” breasts due to their absence of progesterone. In actuality however, there is no good evidence at this time that progesterone is required for normal pubertal breast development, that progesterone is needed to reach Tanner stage 5, or that it helps to round out the breasts. Such claims are contradicted by extensive available literature and evidence, including notably the literature on CAIS women themselves.
Women with CAIS are individuals who have a 46,XY karyotype (i.e., are genetically “male”), testes, and who would otherwise have physically developed as males, but did not because they have a mutation in the gene encoding the androgen receptor that makes them completely insensitive to the effects of androgens. There are also incomplete forms of the syndrome, like partial androgen insensitivity syndrome (PAIS) and mild androgen insensitivity syndrome (MAIS). CAIS women have a male-typical hormonal profile, generated by their testes, including high male-range levels of testosterone, low female-range estradiol levels, and negligible progesterone levels (Wiki; Table). Instead of developing physically as males however, CAIS women are perfectly phenotypically female, with a normal female body, vagina, and breasts (Wiki; Photo). Their testosterone has been unable to masculinize them, while their estradiol, unopposed by androgens, is able to fully feminize them. The internal reproductive system in CAIS women is essentially that of a highly underdeveloped male, with testes instead of ovaries, no uterus, fallopian tubes, or cervix, and no prostate gland or seminal vesicles. The testes are internally located, either intra-abdominally, inguinally, or labially. They are usually surgically removed by early adulthood, as they otherwise have a high risk of developing testicular cancer because of their location. The vagina in CAIS women is often short and is blind-ending, which is related to their lack of a uterus. In terms of behavior, gender, and sexuality, CAIS women are described as feminine.
Despite claims that CAIS women have generous breast sizes however, in actuality, some CAIS women have large breasts, while some have small breasts. One study found a wide range of breast size measurements of 16×14 cm to 41×31 cm, which equates to an almost 6-fold variation in breast size as quantified by area (Wisniewski et al., 2000). Moreover, the breasts of CAIS women have never been directly compared to those of normal women. Hence, there are no clear data at this time that the breasts of CAIS women are actually larger than average for women. The variation in breast growth in CAIS women parallels the same large variation in breast size between individuals that is seen in cisgender women in general. Here is a collection of photos of CAIS women and their breast development from published case reports and reviews throughout the literature. As can be seen from these photos, breast development in CAIS women is normal and often excellent, although subject to considerable variation between individuals in terms of breast size and shape as in women generally.
If CAIS women truly do have enhanced breast development and breast sizes compared to normal women, it may be that their androgen insensitivity, and hence lack of inhibition of estrogen-mediated breast development by androgens, is responsible for this (Wilson, 1968; Sobrinho, Kase, & Grunt, 1971; Andler & Zachmann, 1979; Zachmann et al., 1986; Patterson, McPhaul, & Hughes, 1994; Barbieri, 2019). Another theoretical possibility is that the high testosterone levels may be aromatized into greater amounts of estradiol locally within the breasts and other tissues in CAIS women and that this may somehow allow for enhanced breast development (Ladjouze & Donaldson, 2019). Interestingly, it has been claimed anecdotally by some researchers that breast development is much better in CAIS women who are allowed to naturally undergo puberty with their own endogenous hormones compared to CAIS women who undergo gonadectomy before puberty and have pubertal maturation induced with exogenous estrogen therapy (Dewhurst, 1972; Glenn, 1976; Dewhurst, 1981; Reindollar & McDonough, 1985; Shearman, 1985; Laufer, Goldstein, & Hendren, 2005). This is to the extent that some CAIS women who have had induced puberty have needed to undergo surgical breast augmentation due to poorly developed breasts (Dewhurst, 1981; Shearman, 1985). In relation to the preceding, it is usually standard clinical practice to delay gonadectomy in CAIS women until puberty has fully completed (Laufer, Goldstein, & Hendren, 2005). However, one clinical study reported good breast development rated as Tanner stage 5 in all cases in CAIS women who experienced either spontaneous or therapeutic puberty (Cheikhelard et al., 2008). It may be important to mimic normal pubertal estrogen exposure with puberty induction in CAIS females by employing low physiological estradiol levels that are slowly and gradually increased over a few years (Dewhurst, 1981; Cheikhelard et al., 2008; Bertelloni et al., 2011).
Baron evaluated a total of 41 people with androgen insensitivity syndrome (AIS) and found that 97% of CAIS women had normal breast development while 63% of individuals with “incomplete AIS” (likely PAIS) had normal breast development (Baron, 1993; Baron, 1994a; Baron, 1994b). In another earlier published study of 50 CAIS females, by Sir Christopher John Dewhurst, 76% were rated as having full breast development, 14% as having moderate breast development, 10% as having “mild” breast development, and 0% as having absent breast development (Dewhurst, 1971b). Hence, based on findings in large samples of CAIS females, most to almost all have normal or full breast development. That a minority of CAIS females have had less breast growth may be due to factors like low and inadequate estradiol levels in some individuals, young age at time of assessment by which point breast development has not fully completed, and/or a small subset of women in general having underdeveloped or small breasts.
CAIS women have never been described in the literature as having “cone-shaped”, “pointy”, or otherwise abnormal breasts. The only exception is that they are often said to have nipples and areolas that are described as “juvenile”, “infantile”, “small”, “pale”, and “non-pigmented” (e.g., Photo) (e.g., Morris, 1953; Morris & Mahesh, 1963; Simmer, Pion, & Dignam, 1965; Dewhurst, 1967; Khoo & Mackay, 1972; Perez-Palacios & Jaffe, 1972; Dewhurst & Spence, 1977). This has been said to be the case regardless of breast size or maturation (Khoo & Mackay, 1972). A possible reason for this phenomenon is that estradiol levels in CAIS women are relatively low, only about 35 pg/mL (130 pmol/L) on average (Wiki; Table). This is relevant as estrogens are known to concentration-dependently produce nipple and areolar pigmentation and enlargement (e.g., Davis et al., 1945 [Figure]; Kennedy & Nathanson, 1953). In contrast to estrogens, progestogens have not been implicated in nipple or areolar pigmentation. Hence, it seems that higher estrogen levels may be necessary for full adult-like nipple and areolar maturation.
Despite their often large breasts, CAIS women are said to have relatively little breast glandular tissue, as opposed to fat and connective tissue, and to have minimal breast lobuloalveolar development (Morris, 1953; Morris & Mahesh, 1963; Simmer, Pion, & Dignam, 1965; McMillan, 1966; Perez-Palacios & Jaffe, 1972; Dewhurst & Spence, 1977; Shapiro, 1982). This is in accordance with the lack of progesterone in CAIS women, since progesterone is important in mediating lobuloalveolar growth. The retained breast sizes of CAIS women despite reduced glandular and lobuloalveolar structures is consistent with the fact that the breasts are composed mostly of stromal adipose and connective tissue. Hence, as touched on previously in this article, greater glandular or lobuloalveolar formation in the breasts may not necessarily translate to greater breast size, which seems readily apparent in CAIS women.
The normal and excellent breast development of CAIS women is notable because these individuals, owing to their testes and hence absence of significant gonadal progesterone production, have very low and negligible levels of progesterone (Wiki; Table; Barbieri, 2019). CAIS womens’ normal breast development, often large breasts, and ability to reach complete breast maturation, as measured by the Tanner scale, are collectively suggestive that progesterone is not required for normal or complete pubertal breast development (Barbieri, 2019). In any case, it must be noted and cautioned again that the breasts of CAIS women have never been directly compared to those in normal women. In addition, quantitative studies of the breasts of CAIS women are very scarce, and much of our knowledge in this area is based on anecdotal clinical experience and subjective breast evaluation. This is in large part due to the rarity of CAIS women and the difficulty in obtaining decent samples of them for study. Furthermore, CAIS women also have other differences from regular women besides their lack of progesterone, for instance their relatively low circulating estradiol levels, high testosterone levels (which can be aromatized into estradiol within tissues like the breasts), androgen insensitivity, and XY karyotype, among others. Hence, the insights into breast development provided by CAIS women come with a variety of caveats.
Interestingly, in spite of their well-developed breasts, breast cancer has never been reported in CAIS women, and would appear to be very rare in these individuals (Aly, 2020b; Aly, 2020c). This may be related to factors like the lack of progesterone and lobuloalveolar maturation in CAIS women and/or their absence of a second X chromosome (Aly, 2020b; Aly, 2020c). CAIS women suggest that breast cancer is not an inherent eventual consequence of excellent breast development.
Menstrual Cycles and Temporary Cyclic Breast Enlargement
The enlargement of the breasts during the luteal phase of the menstrual cycle is believed to be due to temporary glandular and stromal tissue growth, luminal dilation of the ducts and alveoli, fluid retention in the glandular and stromal structures, and increased vascularization and blood flow (Scott et al., 1950; Drife, 1989; Fowler et al., 1990; Hussain et al., 1999; Alekseev, 2021; Biswas et al., 2022). However, studies suggest that most of the changes are merely due to water fluctuations and that change in breast glandular volume is relatively small (Rix et al., 2023). The breast changes during the menstrual cycle have been positively correlated with increased levels of estradiol and progesterone during the luteal phase (Jemström & Olsson, 1997; Clendenen et al., 2013; Rix et al., 2023). In addition, estrogen therapy has been found to reversibly increase breast size (e.g., Hartmann et al., 1998) and estradiol levels are positively associated with breast tenderness (e.g., de Lignières & Mauvais-Jarvis, 1981 [Figures]; Sitruk-Ware et al., 1984). Both estradiol and progesterone can promote water retention via distinct hormonal mechanisms as well as mediate breast glandular growth and changes (Rix et al., 2023). As such, the breast changes during the menstrual cycle are assumed to be due to changing levels of estradiol and progesterone, though it is noteworthy that progesterone has been particularly implicated owing to the breast volume increase occurring during the luteal phase (Lawrence & Lawrence, 2015; Rix et al., 2023). There is a delay in breast volume increases following the peaks of estradiol and progesterone levels during the menstrual cycle and hence the changes are not instantaneous (Rix et al., 2023).
Combined oral contraceptives, which are estrogen–progestogen preparations, as well as menopausal estrogen–progestogen hormone therapy, may produce temporary breast enlargement and feelings of breast fullness analogous to those that occur during the luteal phase of the menstrual cycle (Milligan, Drife, & Short, 1975; Dennerstein et al., 1980 [Figure]; Malini, Smith, & Goldzieher, 1985; Jemström & Olsson, 1997; Jernström et al., 2005). In one study, breast volume was around 100 mL greater (~30% higher) in women who were currently taking oral contraceptives relative to those who had not taken or had previously taken oral contraceptives (Jemström & Olsson, 1997). In some women, the increase in breast size with oral contraceptives was subjectively reported to be up to a single bra cup size in volume (Jemström & Olsson, 1997). However, in another study by the same group of researchers that had a much larger sample size (n=258 vs. n=65), breast volumes were not significantly different between current hormonal contraceptive users and non-users (Jernström et al., 2005). Additionally, another study found no significant differences in breast volume in women between different estrogen–progestogen oral contraceptives that had about 6-fold variation in dose of the same progestin (0.4 to 2.5 mg/day norethisterone) as well as non-users (Malini, Smith, & Goldzieher, 1985). However, this study was underpowered due to small sample sizes (n=5 to n=15 per group) (Malini, Smith, & Goldzieher, 1985).
Engman et al. (2008) conducted an RCT of treatment with mifepristone, a selective progesterone receptor modulator (SPRM) with predominantly antiprogestogenic effects, versus placebo for 3 months in normally cycling premenopausal cisgender women, and evaluated the effects of this progesterone receptor blockade on the breasts. They found that mifepristone significantly reduced Ki-67 index, a measure of cellular proliferation in the breasts, and reduced subjectively rated symptom scores on the Breast Symptom Index (BSI). More specifically, breast soreness, breast swelling, sense of increased breast volume, and the total breast symptoms score were all significantly reduced on the BSI. However, breast volume was not objectively measured in this study. A major limitation of this study is that mifepristone inhibits ovulation and modifies levels of estradiol and other hormones (Spitz et al., 1989; Spitz et al., 1994; Engman et al., 2008, Spitz, 2010). As such, it is unclear whether the effects observed by Engman and colleagues were specifically due to progesterone receptor antagonism in the breasts or due to disruption of the hypothalamic–pituitary–gonadal (HPG) axis, for instance lowered estradiol levels.
An interesting case report of an adult woman with CAIS documented a significant increase in breast volume with combined estrogen–progestogen therapy relative to estrogen monotherapy (Dijkman et al., 2023b). The woman was started on cyclic oral estradiol 2 mg/day and dydrogesterone 10 mg/day and subjectively experienced breast pain and fluctuations in breast volume of about one cup size while on this regimen. Subsequently, she was switched to oral estradiol valerate 3 mg/day monotherapy and the fluctuations in breast volume ceased. However, her overall breast volume was reduced as well, and the woman decided to resume combined estradiol and dydrogesterone therapy. Her clinicians proceeded to measure her breast volume using 3D body scanning. Her left breast was 758 mL and right breast was 673 mL with estrogen monotherapy, and her breasts increased to respective volumes of 875 mL and 784 mL during combined estrogen–progestogen therapy, giving net volume increases of 117 mL (+16%) and 111 mL (+17%). These differences in volume corresponded to an almost one bra cup difference in size. The researchers noted that estradiol and progesterone are associated with cyclical breast changes, and hypothesized that the changes in their patient were due to increased fluid retention in the breasts. Taken together, the case report demonstrates that progestogens can cause rapid and considerable reversible breast enlargement in some women analogous to that during the normal menstrual cycle.
Progesterone and Mammary Development in Animals
Progesterone and Pubertal Mammary Development in Animals
Although progesterone does not seem to be essential in normal pubertal mammary development in mice, studies have interestingly found that it is able to substitute for estrogen in mediating pubertal ductal mammary development in this species. Ruan, Monaco, & Kleinberg (2005) studied the effects of various combinations of exogenous estradiol, progesterone, and IGF-1 on mammary development in oophorectomized female IGF-1-knockout mice. In terms of stimulation of ductal development to occupy the mammary gland fat pad, the combination of progesterone and IGF-1 produced 92% occupation, estradiol and IGF-1 resulted in 92% occupation, estradiol, progesterone, and IGF-1 achieved 96% occupation, and IGF-1 alone resulted in only 28% occupation (Ruan, Monaco, & Kleinberg, 2005; Kleinberg & Ruan, 2008). In terms of gross anatomical appearance, the ductal tree with progesterone and IGF-1 was said to resemble that of a normal fully developed pubertal mammary gland (Ruan, Monaco, & Kleinberg, 2005). However, differences in mammary development between the combination of estradiol and IGF-1 and the combination of progesterone and IGF-1 were apparent, with estradiol and IGF-1 having greater effect on terminal end bud formation, ductal decorations, and slight alveolar maturation, and progesterone and IGF-1 having more effect on ductal formation, extension, and branching (Ruan, Monaco, & Kleinberg, 2005; Kleinberg & Ruan, 2008). The effects of progesterone on mammary development were reversed by the progesterone receptor antagonist mifepristone (Ruan, Monaco, & Kleinberg, 2005). Only the combination of estradiol, progesterone, and IGF-1 produced mammary development that resembled that during mid-pregnancy, with full maturation of secretory alveolar structures (Ruan, Monaco, & Kleinberg, 2005; Kleinberg & Ruan, 2008).
A limitation of studies that have used exogenous progesterone to stimulate pubertal ductal mammary development in mice is that the doses of progesterone employed, in conjunction with other hormones like estradiol, have been sufficient to mediate mammary growth to a level typical of pregnancy, with robust maturation of mammary lobuloalveolar structures (e.g., Škarda, Fremrová, & Bezecný, 1989; Ruan, Monaco, & Kleinberg, 2005). Pregnancy is a time when hormone levels are much higher than usual. Hence, the progesterone exposure in these studies may have been supraphysiological relative to normal puberty, and may have produced effects on mammary growth that would not otherwise occur during this time. Accordingly, Škarda, Fremrová, & Bezecný (1989) found that whereas untreated normal female mice naturally grew to a mammary gland area of 26.4 mm2 and normal female mice treated with exogenous estradiol grew to a mammary gland area of 25.3 mm2, normal female mice treated with exogenous estradiol and progesterone grew to a mammary gland area of 43.5 mm2 and with exogenous progesterone alone to a mammary gland area of 64.6 mm2. The untreated control mice did not show alveolar buds, whereas the progesterone-treated groups did have alveolar maturation, indicating supraphysiological and pregnancy-like development compared to non-pregnant mice (Škarda, Fremrová, & Bezecný, 1989). In any case, one study employed low doses of progesterone (0.1 mg/day), one-tenth of that used in most other studies (1 mg/day), and found that progesterone still stimulated significant ductal development in mice at these doses (Aupperlee et al., 2013; Berryhill, Trott, & Hovey, 2016). Hence, progesterone is still able to stimulate some level of ductal growth in mice even at lower levels.
Although progestogens by themselves can apparently stimulate normal pubertal mammary development in lieu of estrogen exposure in mice, it is not clear that they do so similarly in humans. It is well-known that progestogens alone, without concomitant estrogenic activity, do not generally produce breast development in humans. As an example, progestogens, for instance MPA and CPA, have been used as puberty blockers in boys and girls at very high doses, and do not produce breast development in this context, instead causing arrest and regression of breast development via gonadal suppression (Lyon, De Bruyn, & Grant, 1985; Fuqua & Eugster, 2022). Cases of gynecomastia in boys have occurred with CPA, but only in a minority and with this easily attributable to other causes than progestogenic activity, for instance the antiandrogenic activity of CPA and disruption of the HPG axis (Kauli et al., 1984; Laron & Kauli, 2000). Similarly, progestogens like MPA and CPA have been used at very high doses in men to treat prostate conditions and sexual disorders, and likewise do not usually produce gynecomastia under these circumstances. Rates of gynecomastia with CPA used in the treatment of prostate cancer are low and are not noticeably different from the rates with surgical or medical castration (~10%) (Fourcade & McLeod, 2004; Di Lorenzo et al., 2005). This is in major contrast to the high rates of gynecomastia with estrogens and nonsteroidal antiandrogens (up to 70–80%) (Fourcade & McLeod, 2004; Di Lorenzo et al., 2005; Deepinder & Braunstein, 2012). Species differences may be present such that progestogens can produce robust pubertal mammary development in mice but do not do so in humans.
Progesterone and Gestational Mammary Development in Animals
Therapeutic or pharmacological pseudopregnancy is a type of hormone therapy that attempts to replicate the hormonal mileu of pregnancy for certain medical indications in cisgender females by administering exogenous hormones. In practice, this has involved the administration of very high doses of estrogens and progestogens, with most other pregnancy hormones not included. Therapeutic pseudopregnancy was first developed in the 1950s and is largely no longer used in medicine today (Kaiser, 1993).
The effects of therapeutic pseudopregnancy on the breasts are of interest due to the breast changes that occur during pregnancy, for instance lobuloalveolar development and substantial reversible breast enlargement. In the 1980s, Lauritzen and colleagues conducted a study of therapeutic pseudopregnancy for treatment of breast hypoplasia (small/underdeveloped breasts) in cisgender women (Lauritzen, 1980; Lauritzen, 1982; Lauritzen, 1989; Göretzlehner & Lauritzen, 1992). They employed the estrogen estradiol valerate 40 mg/week and the progestogen hydroxyprogesterone caproate (OHPC) 250 to 500 mg/week both by intramuscular injection for 4 to 5 months. The estradiol valerate dosage employed was very high, with other studies by the same authors reporting that this dosage of estradiol valerate resulted in first-trimester pregnancy levels of estradiol in women (~3,000 pg/mL [~11,000 pmol/L]) (Ulrich, Pfeifer, & Lauritzen, 1994; Ulrich et al., 1995). These estradiol levels are roughly 30 times the normal concentrations outside of pregnancy (Aly, 2018b). Similarly, the OHPC doses were very high, with 250 to 500 mg per month being similar in strength to luteal-phase progestogenic exposure (Wiki). Hence, as the same OHPC doses were used weekly in the study, the doses were roughly around 4.5 times luteal-phase exposure and thus were analogously similar to first- or second-trimester progesterone levels in terms of strength (Aly, 2020d). The authors noted that they had initially tried lower hormone doses, similar to those originally used in the 1950s, but did not achieve significant breast growth with these doses, and so increased the dosage. Breast changes were measured in the study with a tape measure (applied horizontally and vertically to the breast area), photographs, breast imaging using mammography and sonography, and, later in the study, plasticine impressions/molds with determination of the filling volume.
Lauritzen and colleagues reported the study findings in four different publications with different follow-up times and growing sample sizes. In the final follow-up, a total of 221 women had been treated. In the second follow-up, when 78 women had been treated, it was noted that 29 of the cases (37%) were less than 18 years old. However, in the final follow-up of 221 women, the age range was listed as 18 to 42 years. The researchers found that breast volume increased by 10 to 30% above baseline in 65% of the women. This was also accompanied by breast tenderness in almost all of the women, though the breast tenderness progressively declined during the treatment period. Other breast-related side effects like pigmentation and stretch marks were rarely observed. Prolactin levels slightly increased to 14 to 28 pg/mL by the end of treatment. Breast imaging showed an increase in the density of breast glandular tissue. The researchers claimed that the increase in breast size in their study was due to increased adipose tissue, water retention, and moderate hypertrophy of the glandular tissue.
Following treatment discontinuation, the increases in breast volume gradually and partially regressed in 40% of the women, to an increase of 10 to 20% above baseline. However, the authors claimed that the regression in breast volume could be reduced with adequate-dose combined estrogen–progestogen birth control pills or with topical estrogen and progestogen therapy applied to the breasts. In addition, they noted that therapeutic pseudopregnancy could be repeated to increase breast volume again. This was performed in a subset of the women, with treatment repeated 1 to 2 times after 6 months. In the second follow-up, which had 78 women, it was noted that 12 women (15%) had undergone multiple treatments. Aside from Lauritzen and colleagues, many other researchers have also reported substantial or full regression in breast size following estrogen and/or progestogen therapy to increase breast size in cisgender women (e.g., Cernea, 1944; Müller, 1953; Anderson, 1962; Bruck & Müller, 1967; Keller, 1984; Kaiser & Leidenberger, 1991; Keller, 1995; Hartmann et al., 1998).
The findings of Lauritzen and colleagues were reported very informally, in the form of non-peer-reviewed book chapters, conference papers, and medical magazines, and were never published in a peer-reviewed journal article. In relation to this, the methodology and results of the study were only briefly and imprecisely described. There are also additional concerns related to study design, such as lack of controls, randomization, and the quality of the breast measurement methods. As a result of the preceding issues, it is difficult to fully interpret the results of the study and to have complete confidence in its findings. In any case, Lauritzen and colleages’ results suggest that treatment with high-dose combined estrogen–progestogen therapy, achieving earlier-pregnancy estrogenic and progestogenic exposure, may be able to produce a significant temporary increase in breast size and a smaller long-term increase. The findings of a permanent increase in breast size conflict with those of other researchers who have reported complete regression in breast changes following treatment discontinuation. Moreover, the results are contradicted by findings in pregnant women, who, as described previously, show complete reversion to pre-pregnancy breast size or to even slightly smaller breasts following cessation of lactation.
It is difficult to evaluate the relative roles of the estrogen and the progestogen in the findings of Lauritzen and colleagues, as there were no comparison groups employing estrogen or progestogen therapy alone in the study. Both estrogens and progestogens have been implicated in causing breast enlargement and plausibly could have contributed to the breast changes. As such, it is unclear to what extent the breast changes were specifically due to progestogenic exposure rather than to estrogenic exposure.
The breast size increases observed by Lauritzen and colleagues were seemingly more modest relative to those that occur normally during pregnancy. They also lacked certain characteristics of pregnancy-related breast changes, like nipple and areolar pigmentation. The reasons for this are not fully clear. The subject populations between these studies were different, for instance in terms of factors like initial breast size and age, which may be contributing reasons. Another possible contributing factor is that only estrogen and progestogen levels increased in the study, whereas levels of other pregnancy hormones, besides the slight increase in prolactin levels, did not increase. These other pregnancy hormones, for instance hPL and IGF-1, may also be involved in breast development during pregnancy. Finally, the treatment duration was only 4 to 5 months, and the estrogen and progestogen exposure was only similar to that during early-to-mid pregnancy, whereas normal pregnancy lasts 9 months and involves continued dramatic increases in estrogen and progesterone levels through to childbirth.
It should be noted that, owing to the highly supraphysiological estrogen and progestogen levels required, which can cause serious health complications like blood clots and cardiovascular problems (Aly, 2020e), as well as the small to negligible lasting increase in breast volume, therapeutic pseudopregnancy is inadvisable for transfeminine people and should not be pursued or employed. Nonetheless, the historical findings of therapeutic pseudopregnancy for increasing breast size in cisgender females are of significant theoretical interest in exploring the roles of estrogens and progestogens in breast growth.
Early Progestogen Exposure and the Possibility of Suboptimal Breast Development
While progestogens are typically sought after by transfeminine people for their potential in improving breast development, there have also been various suggestions in the literature that early or premature exposure to progestogens may result in suboptimal breast development and that progestogens may suppress or reduce estrogen-mediated breast development. These suggestions include progestogens having known antiestrogenic effects in the breasts, animal studies finding stunted mammary development with high doses of progestogens, clinical publications cautioning against premature introduction of progestogens in female puberty induction due to concerns about possibly stunted breast growth, clinical use of progestogens to treat macromastia in cisgender females, poor breast development with estrogen therapy in cisgender girls with a disorder of sexual development that results in high progesterone exposure, and breast development with estrogen and CPA (a very strong progestogen) typically being poor in transfeminine people. As with the question of whether progestogens can enhance breast development, it is currently unknown whether progestogens could worsen breast development. It is also unknown what dosage level and timing of introduction would be required for such an effect. In any case, for informational purposes, the preceding topics will each be discussed in the subsequent sections.
Antiestrogenic Effects of Progestogens in the Breasts
Stunted Mammary Growth with Progestogens in Animal Studies
Animal studies using progestogens including bioidentical progesterone and chlormadinone acetate (CMA), a progestin closely related to CPA, have found that high doses of these progestogens substantially stunt mammary gland development in rabbits, whereas lower doses do not do so (Lyons & McGinty, 1941; Beyer, Cruz, & Martinez-Manautou, 1970). See here for relevant literature excerpts as well as figures from these studies. Lyons & McGinty (1941) [Figure] found that estrogen alone induced ductal mammary development and estrogen plus progesterone 0.25 to 1 mg/day produced ductal development and slight to “fair” lobuloalveolar development. Conversely, estrogen plus progesterone 4 to 8 mg/day, which were 4- to 8-fold higher doses of progesterone than the most optimal dose, produced stunted mammary development with inhibited ductal development, only slight lobuloalveolar development, and, at the highest dosage, resulted in a much smaller mammary gland in terms of size than in the ≤1 mg/day groups. They concluded that high doses of progesterone are inhibitory and result in relatively poor mammary development. In the paper, doses of progesterone in international units (IU) were reported, but a citing review, Pfeiffer (1943), indicated that 1 IU progesterone is equal to 1 mg progesterone. As such, the milligram doses are listed above instead. Beyer, Cruz, & Martinez-Manautou (1970) [Figure] found that estrogen alone produced good ductal development without lobuloalveolar growth (mean mammary area = 376 mm2) and both estrogen plus CMA 0.5 mg/day and estrogen plus progesterone 2.5 mg/day produced optimal ductal and lobuloalveolar development (mean mammary area = 765 mm2 and mean mammary area = 688 mm2, respectively). Conversely, estrogen plus CMA 2.5 mg/day, a 5-fold higher dose of CMA than the optimal dose, resulted in dramatically reduced ductal development and mammary gland size albeit with significant lobuloalveolar growth (mean mammary area = 284 mm2). The authors concluded that moderate doses of progestogens stimulate mammary gland growth whereas large doses inhibit mammary gland development.
While these animal studies are suggestive that high doses of progestogens may be able to stunt breast development in humans, this is far from a certainty. There are species differences in hormone-mediated mammary development such that findings in one species, such as rabbits, may not translate to another species, like humans, or sometimes even to closely related species, like rats or guinea pigs (Bässler, 1970). As far as the present author is aware, stunted mammary development with high doses of progestogens has not been studied or reported in other animal species, for instance other rodent species or monkeys. It is also unclear that the doses employed in these animal studies are necessarily relevant to progestogen therapy in humans. This is because pregnancy levels of progesterone, which are much higher than luteal-phase progesterone levels, are necessary for substantial mammary lobuloalveolar development, and the doses of progestogens used in these studies were above that magnitude of progestogenic exposure. Hence, the doses may have corresponded to what in humans would be extremely high doses. However, such doses could still be relevant in the case of CPA used as an antiandrogen in humans, as CPA is used in this context at very high doses (see section below). The present author is unaware of any animal studies finding that physiological non-pregnancy levels of progesterone have any stunting or other adverse influence on mammary development, suggesting that only high doses of progestogens may have such effects. Finally, it seems notable that the estrogen and progestogen were initiated simultaneously in these animal studies and yet produced optimal pregnancy-like mammary development at the right doses. This suggests that early or immediate progestogen exposure might not be unfavorable in terms of breast development in humans. However, once again species differences may be present and confirmatory clinical studies are needed in humans.
Clinical Publications Cautioning Against Premature Introduction of Progestogens Due to Possibly Stunted Breast Development
A large number of clinical publications largely in the pediatric endocrinology literature have warned that premature exposure to progestogens during for instance puberty induction may result in suboptimal breast development in cisgender girls and/or transfeminine people (Zacharin, 2000; Bondy et al., 2007; Colvin, Devineni, & Ashraf, 2014; Wierckx, Gooren, & T’Sjoen, 2014; Kaiser & Ho, 2015; Bauman, Novello, & Kreitzer, 2016; Gawlik et al., 2016; Randolph, 2018; Donaldson et al., 2019; Heath & Wynne, 2019a; Heath & Wynne, 2019b; Iwamoto et al., 2019; Crowley & Pitteloud, 2020; Naseem, Lokman, & Fitzgerald, 2021; Federici et al., 2022; Lucien et al., 2022; Rothman & Iwamoto, 2022). The full relevant excerpts from these sources can be found here. In relation to these claims, and in order to mimic normal female puberty, a progestogen is not typically added to estrogen therapy during puberty induction in cisgender girls with delayed puberty until after about 2 to 3 years of treatment, by which point breast growth is generally considered complete. Additionally, progestogens are generally never added as part of puberty induction in transfeminine adolescents. Despite the preceding widespread literature statements and accepted clinical practices in the field of puberty induction however, it is important to note that the claims that premature introduction of progestogens might stunt breast development in this context are currently not based on any actual reliable clinical evidence and hence remain unsubstantiated. It is not even clear that these statements are based on anecdotal clinical experience as opposed to simple conjecture. The absence of data in this area may finally change in the future as more clinical studies of progestogens in puberty induction in cisgender girls are conducted (e.g., Rodari et al., 2023).
Rodari and colleagues studied optimization of puberty induction with estrogen therapy followed by eventual introduction of progestogen therapy in 49 cisgender girls with hypogonadism (e.g., Rodari et al., 2022; Rodari, 2022; Rodari et al., 2023). The researchers employed incrementally titrated low-dose transdermal estradiol to mimic the low and gradually increasing estradiol levels during normal puberty and added a progestogen only once menstrual bleeding began. The total duration of treatment was mean 2.65 ± 1 years, the time of first menstrual bleeding occurrence was 2.3 ± 1 years, and the time of progestogen introduction was median 2.22 years (IQR 1.56–2.87 years). Of the girls, 90% reached Tanner breast stage 4, but only 41% reached Tanner breast stage 5. Reaching the final Tanner breast stage was significantly associated with the number of estradiol dose increases (i.e., gradual estradiol dose titration) and the estradiol dose at progestogen introduction. The researchers interpreted the latter finding as progestogen exposure potentially hampering breast development. They questioned introducing progestogen therapy in the presence of incompletely developed breasts and suggested that instead of adding a progestogen upon onset of menstrual bleeding, clinicians should consider slightly reducing the estradiol dosage to delay progestogen introduction until the breasts complete maturation. While interesting, it must be noted that the findings of Rodari and colleagues are merely correlational, are open to multiple interpretations, and do not causally show that progestogens impair breast maturation.
Progestogens in the Treatment of Breast Hypertrophy
More recently, a couple of studies, both by the same group of researchers, assessed the impact of different types of hormonal contraception on macromastia in adolescent cisgender females with macromastia (Nuzzi et al., 2021; Nuzzi et al., 2022). They found that use of progestin-only contraceptives was associated with significantly more breast tissue removed upon surgical breast reduction (959.9 g/m2 vs. 735.9 g/m2 [+30%]; p = 0.04) and worse clinical symptoms (e.g., breast pain—odds ratio, 4.94, p = 0.005) relative to non-users of hormonal contraception (Nuzzi et al., 2021). Conversely, use of combined oral contraceptives, which are estrogen–progestogen preparations, was associated with significantly less breast tissue removed with breast reduction (639.5 g/m2 vs. 735.9 g/m2 [−13%]; p = 0.003), though not with any differences in clinical symptoms, relative to those naive to hormonal contraception (Nuzzi et al., 2022). It should be noted that progestin-only contraceptives suppress the HPG axis and result in low estradiol levels, whereas combined oral contraceptives suppress the HPG axis and lower estradiol production but simultaneously supplement estrogen signaling by delivering exogenous estrogen. This difference may somehow be responsible for the opposite influence of estrogen–progestogen therapy versus progestogen-alone therapy on macromastia severity. While the findings of Nuzzi and colleagues are interesting, it is noteworthy that the methodology and findings of their research were criticized on various grounds in a letter to the editor concerning one of the articles (Karp, 2022).
Santen et al. (2024), in a case series of cisgender girls with juvenile gigantomastia, noted that breast growth continues for only a number of years following onset and hence there must be some form of stop signal that is activated and that prevents further breast growth. They speculated that this signal may be related to apoptosis (programmed cell death). Santen and colleagues noted that in adult cisgender women, proliferation of breast cells is increased during the follicular phase of the menstrual cycle, whereas apoptosis in breast cells is increased during the luteal phase of the cycle. They hypothesized that the apoptosis during the luteal phase may block further breast development. Since progesterone is produced during the luteal phase and may mediate said apoptosis, this would substantiate the use of progestogens in the treatment of breast hypertrophy. However, the researchers noted that no data exist on apoptosis in the breasts of girls with juvenile gigantomastia. Moreover, an important point against the authors’ hypothesis is that estrogen-induced breast growth gradually slows and ceases in people who do not have menstrual cycles and luteal phases or progestogenic exposure just as it does in normal cisgender girls. Prominent examples of such individuals include CAIS women, transfeminine people, and cisgender men with prostate cancer treated with estrogen therapy.
Poor Breast Development in 17α-Hydroxylase/17,20-Lyase Deficiency
Non-Comparative Clinical Studies of Breast Development with Estrogen and Cyproterone Acetate in Transfeminine People
The possibility of suboptimal breast development with premature exposure to progestogens is of particular relevance in the case of CPA used as an antiandrogen in transfeminine people. This is because CPA is a potent progestogen in addition to antiandrogen, starts to be taken at the initiation of hormone therapy, and happens to be used in transfeminine people at doses that result in very strong to profound progestogenic exposure (Aly, 2019). In terms of progestogenic strength, CPA at a dosage of 2 mg/day is comparable to the progesterone exposure during the luteal phase of the menstrual cycle (Aly, 2019; Wiki). For comparison, CPA has been used in transfeminine people at doses ranging from 10 to 100 mg/day (Aly, 2019). This would mean that CPA provides roughly 6.25 times the progestogenic impact of luteal-phase progesterone exposure at a dosage of 12.5 mg/day, 12.5 times the impact at 25 mg/day, 25 times the impact at 50 mg/day, and 50 times the impact at 100 mg/day. Moreover, this does not consider the fact that progesterone is only produced during the luteal phase, or half of the menstrual cycle, whereas CPA is taken continuously every day of the month. The preceding magnitudes of progestogenic exposure with CPA are on par with and even beyond those during pregnancy. Only recently have lower doses of CPA (e.g., ≤12.5 mg/day) started to be used in transfeminine hormone therapy.
Studies in pubertal and adolescent transfeminine people given GnRH agonists to block puberty plus estrogen therapy have reported good breast development in these individuals as assessed by subjective clinical impression or Tanner staging (de Vries et al., 2010; Hannema et al., 2017). However, quality objective measures of breast development were not employed in these studies. Conversely, non-comparative studies using estrogen plus CPA in adult transfeminine people have commonly reported modest breast development, including incomplete breast development only to Tanner stage 2 to 4, small breast cup sizes, and small breast volumes (Kanhai et al., 1999; Sosa et al., 2003; Sosa et al., 2004; Wierckx et al., 2014; Fisher et al., 2016; Tack et al., 2017; de Blok et al., 2018; Reisman, Goldstein, & Safer, 2019; Meyer et al., 2020; de Blok et al., 2021). Additionally, breast sizes smaller than those in cisgender women have been reported (Asscheman & Gooren, 1992; Kanhai et al., 1999). In one study, breast development with estrogen plus CPA was also poor in late-adolescent transfeminine people (Tack et al., 2017). However, in this particular study, the estrogen dose used was likely too low and resulted in inadequate estradiol levels, as noted by the authors themselves, and this is a potential confounding factor in their findings (Tack et al., 2017). In any case, breast growth with estrogen plus CPA in transfeminine people would seem to consistently be poor. In contrast to the regimen of estrogen and CPA, breast development with other hormone therapy regimens, for instance estrogen with non-progestogenic antiandrogens like spironolactone, bicalutamide, and GnRH modulators, has not been nearly as well-studied in comparison, and hence comparisons of outcomes between regimens is difficult.
In one of the highest quality studies of estrogen and CPA and breast development in adult transfeminine people, breast volume measured with 3D body scanning (Vectra XT) was approximately mean 100 mL (95% CI ~75–125 mL; range up to ~750 mL), equating to less than an A cup size on average, after 3 years of hormone therapy with estrogen and CPA in 69 transfeminine people (de Blok et al., 2021 [Figure]). In this study, breast changes over time had clearly plateaued, suggesting that breast development was either complete or was nearly so (de Blok et al., 2021 [Figure]). Although most of the transfeminine people in this study had less than an A cup breast size (71%), a minority had cup sizes ranging from an A cup (9%), B cup (16%), C cup (3%), to E cup (1%) (de Blok et al., 2021 [Figure]). For comparison, a study of normative data on breast volumes in cisgender women, using a different 3D body scanning device (Artec Eva 3D), found breast volumes of median ~515 mL and mean ~650 mL (IQR ~310–850 mL; range ~50–3,100 mL) in 378 cisgender women (Coltman, Steele, & McGhee, 2017). As such, adult transfeminine people treated with estrogen and CPA would appear to have substantially smaller breasts than cisgender women. However, it must be emphasized that the preceding data come from separate clinical studies and hence are not directly comparative. It is noteworthy in this regard that breast volumes can vary considerably between different studies even using similar measurement methods (e.g., magnetic resonance imaging) (Sindi et al., 2019 [Table]). Hence, there is a need for studies directly comparing breast volumes in transfeminine people to those in cisgender women using the same measurement method in order to comparatively evaluate breast development.
Regardless of the preceding, transfeminine people could simply have poor breast development in general without this necessarily being related to CPA or progestogenic exposure. Indeed, a more recent study in transfeminine people who underwent pubertal suppression in adolescence, presumably with GnRH agonists and then estrogen therapy, found similarly poor breast development as has been reported in adults (Boogers et al., 2022; c.f. de Blok et al., 2021). This study used breast volume via 3D body scanning to measure breast development and found a mean breast volume of 114 mL (IQR 58–203 mL), equating to less than an A cup size, after 4.2 years of hormone therapy (Boogers et al., 2022). It was notably conducted by the same group of researchers who did the earlier higher-quality study in adult transfeminine people, and hence likely used the same 3D scanning method (de Blok et al., 2021).
No directly comparative studies of breast development with CPA versus other antiandrogens in transfeminine people are currently available. Hence, it’s not fully known whether the findings are specific to CPA or also generalize to other antiandrogens that are not also strongly progestogenic. The RCT of estradiol and spironolactone versus estradiol and CPA in transfeminine people by Ada Cheung and colleagues underway in Australia may provide more insight on this issue, as spironolactone is only a weakly or clinically non-progestogenic antiandrogen (Aly, 2018b; Wiki; update: see below).
Additional Considerations for Progestogen Therapy and Breast Development in Transfeminine People
Anecdotes About Progestogens and Breast Development
Many transfeminine people who have taken progestogens as part of hormone therapy have anedotally reported that the progestogens improved their breast development. At the same time, many other transfeminine people have anecdotally reported no benefit of progestogens to breast development. It must be cautioned in general that anecdotal reports are unreliable and represent a very low form of medical evidence. This is because subjective observations and attributions are often erroneous. Perceptions can be faulty and inaccurate, especially with slowly developing physical changes, and true physical changes can be due to coincidence and unrelated confounding factors rather than due to a person’s causal attributions. A couple notable examples of potential confounding factors with regard to progestogens and breast development include: (1) continued breast development from estrogen acting on its own; and (2) temporary breast enlargement due to local fluid retention, increased blood flow, and reversible lobuloalveolar growth caused by progestogens. Such factors have the potential to mislead, and may contribute significantly to anecdotal reports of enhanced breast development with progestogens in transfeminine people. Clinical studies that are well-designed, controlled, and employ reliable objective measures, with long-term follow-up and eventual discontinuation of the progestogen to control for reversible effects, are needed to properly evaluate the effects of progestogens on breast development.
Therapeutic Limitations of Oral Progesterone
Oral progesterone produces very low progesterone levels and has only weak progestogenic effects even at high doses (Aly, 2018a; Wiki). These low progesterone levels are likely to be inadequate in terms of desired physiological progestogenic effects, for instance in the breasts. Oral progesterone also uniquely has potent neurosteroid actions via active metabolites like allopregnanolone, which can result in prominent side effects such as alcohol-like central nervous system inhibition as well as mood swings (Aly, 2018b; Wiki; Wiki). These neurosteroid effects are dose-dependent and are more severe at high doses. Non-oral progesterone forms like rectal or injectable progesterone or progestins, which do not have the preceding problems, can be used instead to avoid such concerns (Aly, 2018a; Aly, 2018b).
Tolerability and Safety Considerations for Progestogens
Progestogens have a variety of tolerability issues and safety risks (Aly, 2018b). Examples of such risks variously include adverse mood changes, breast cancer, blood clots, cardiovascular complications, benignbrain tumors including prolactinomas and meningiomas, and off-target actions with undesirable effects (e.g., androgenic or glucocorticoid activity), among others (Aly, 2018b). CPA at high doses also uniquely has a significant risk of serious liver toxicity (Aly, 2018b). The risks of progestogens vary depending on the specific progestogen and dosage, but all progestogens, including even bioidentical progesterone, have significant known risks. The risks of progestogens, along with lack of evidence of beneficial effects in terms of feminization, well-being, and health, are why there are concerns about and hesitations on their use in transfeminine people (Aly, 2018b). However, cisgender women naturally have progesterone in their bodies, and the absolute risks of progestogens are low (Aly, 2018b). The risks of progestogens can be minimized by use for a limited duration of time (e.g., a few years), by using the lowest dosages expected to be effective in terms of desired effects, and by selection of progestogens with more favorable pharmacological profiles (Aly, 2018a; Aly, 2018b).
Updates
Update 1: Angus et al. (2023–2024)
It was previously reported in this article that an RCT assessing breast development with estradiol plus spironolactone versus estradiol plus CPA in transfeminine people was being conducted by Ada Cheung and colleagues. This study could provide more insight into breast development with progestogens, as CPA is a very potent progestogen whereas spironolactone is not meaningfully progestogenic. Cheung and colleagues’ study, led by Lachlan Angus, has now been published in the form of the following two conference abstracts, with a journal article also currently in the process of being published:
Angus, L. M., Leemaqz, S., Zajac, J. D., & Cheung, A. S. (November 2023). A randomised controlled trial of spironolactone versus cyproterone in trans people commencing estradiol. AusPATH 2023 Symposium. [URL] [PDF] [Trans Health Research Blog Post]
Angus, L. M., Leemaqz, S. Y., Zajac, J. D., & Cheung, A. S. (November 2023). The effect of cyproterone and spironolactone on breast development in transgender women: a randomised controlled trial. ESA/SRB/ENSA 2023 ASM 26-29 November, Brisbane, 54–55 (abstract no. 132). [URL] [PDF] [Full Abstract Book] [Trans Health Research Blog Post]
The study assessed estradiol plus spironolactone 100 mg/day versus estradiol plus CPA 12.5 mg/day in 55 transfeminine people, with 27 in the spironolactone group and 28 in the CPA group. Hormone therapy duration, at least at this follow-up point in the study, was 6 months. The measures of breast development included breast–chest difference (primary) and estimated breast volume (secondary).
Breast development, measured by breast–chest difference (mean ± SD), was 8.3 ± 2.7 cm with spironolactone and 9.2 ± 3.0 cm with CPA, with the differences between groups not statistically significant (p = 0.27). In addition, breast development, measured by estimated breast volume (mean ± SD), was 158 ± 112 mL with spironolactone and 190 ± 159 mL with CPA, with the differences between groups not statistically significant (p = 0.39). There was variability between individuals in estimated breast volume, with breast volume measurements ranging from 20 to 788 mL. Besides breast growth, the researchers found that CPA also resulted in a greater increase in body fat percentage and gynoid fat compared to spironolactone. Estradiol levels were comparable between antiandrogen groups, whereas total testosterone levels were (mean ± SD) 4.29 ± 5.44 nmol/L (124 ± 157 ng/dL) with spironolactone and 1.48 ± 3.45 nmol/L (43 ± 99 ng/dL) with CPA, a difference that was statistically significant (p = 0.04).
The researchers concluded that there was no difference in breast development with spironolactone versus CPA in their study and that antiandrogen choice should be individualized based on patient and clinician preference as well as consideration of associated side effects. Moreover, they concluded that further research is needed to optimize breast development in transfeminine people.
Angus, L., Mikolajczyk, M., Cheung, A., Zajac, J., Antoszewski, B., & Kasielska-Trojan, A. (2022). Estimation of breast volume in transgender women using 2D photography: validation of the BreastIdea Volume Estimator in men and transgender women. ESA/SRB/APEG/NZSE ASM 2022, November 13-16, Christchurch, Abstracts and Programme, 127–127 (abstract no. 279). [URL] [PDF] [Full Abstract Book]
In studies by the developers of the BreastIdea Volume Estimator, they reported breast volumes measured with the tool in cisgender women. These estimated breast volumes can provide comparison to the breast-volume findings in transfeminine people by Cheung and Angus and colleagues. The developers of the BreastIdea Volume Estimator reported that breast volume (mean ± SD) in cisgender women with normal breasts (n=30) was 283 ± 144 mL and in cisgender women with macromastia or gigantomastia (n=35) was 888 ± 277 mL (Kasielska-Trojan, Zawadzki, & Antoszewski, 2022). In another study, they reported that breast volume (mean ± SD) in cisgender women was 272 ± 150 mL, with a range of 99 to 694 mL (Kasielska-Trojan, Mikołajczyk, & Antoszewski, 2020).
Although the BreastIdea Volume Estimator is an interesting and promising tool for quantifying breast development, it has notable limitations, such as its resolution and accuracy being much less than that with 3D scanners like the Artec Eva and Vectra XT (Mikołajczyk, Kasielska-Trojan, & Antoszewski, 2019). Vectra and Artec 3D scanners have been and are being employed to measure breast development with hormone therapy in other studies in transfeminine people (de Blok et al., 2021; Boogers et al., 2022; Dijkman et al., 2023a; Dijkman et al., 2023b; Lopez et al., 2023). The accuracy limitations of the BreastIdea Volume Estimator may explain why the breast volume findings with it in transfeminine people and cisgender women were different from those seen in other studies that employed more advanced 3D scanning methods. Aside from the breast volume measurement, breast–chest difference also has limitations as a measure of breast development in transfeminine people, for instance failing to identify continued breast growth that can be detected with breast volume measurement (de Blok et al., 2021).
Besides the employed measurement methods for breast development, limitations of Lachlan Angus and colleagues’ RCT of breast development with spironolactone and CPA in transfeminine people include its limited duration of follow-up of only 6 months, the fact that testosterone levels were non-equivalent between the spironolactone and CPA groups, and its limited sample size. The incompletely suppressed testosterone levels with spironolactone are notable as androgens oppose estrogen-mediated breast development and could have reduced breast development in the spironolactone group. The limited sample size of the study was responsible for the numeric difference in breast measurements between antiandrogen groups not being statistically significant. In any case, Angus and colleagues’ findings are suggestive that CPA, which is highly progestogenic, neither enhances nor stunts breast development, at least relative to non-progestogenic spironolactone for up to 6 months of hormone therapy. It seems likely that the RCT will continue to longer follow-up times and durations of hormone therapy in the future.
Update 2: Flamant, Vervalcke, & T’Sjoen (2023) and Yang et al. (2024)
The following two recent studies provide additional information on the topic of breast development with progestogen exposure—specifically with CPA—in transfeminine people:
Flamant, T., Vervalcke, J., & T’Sjoen, G. (November 2023). Dose Reduction of Cyproterone Acetate in Trans Women and the Effect on Patient-reported Outcomes: Results from the ENIGI Study. Endocrine Abstracts, 97 [Belgian Endocrine Society 2023], 5–5 (abstract no. 007). [URL] [PDF]
Yang, W., Hong, T., Chang, X., Han, M., Gao, H., Pan, B., Zhao, Z., & Liu, Y. (2024). The efficacy of and user satisfaction with different antiandrogens in Chinese transgender women. International Journal of Transgender Health, advance online publication. [DOI:10.1080/26895269.2024.2323514]
In the first study, Flamant, Vervalcke, & T’Sjoen (2023), clinical outcomes in transfeminine people at the University of Ghent, Belgium clinic were compared in 72 people taking CPA at low doses (10–12.5 mg/day) or high doses (25–50 mg/day). Testosterone suppression was equivalent between the two dose groups. Breast development satisfaction, measured with the Body Image Scale, was not significantly different with low-dose CPA versus high-dose CPA following 1 year of hormone therapy (p = 0.078). However, the p-value indicates that there was almost a statistically significant difference between groups, though it was not stated which group was numerically higher in terms of satisfaction. In any case, the researchers stated that breast development satisfaction was “non-inferior” with low-dose CPA compared to high-dose CPA, which seems suggestive that satisfaction may have been higher in the high-dose CPA group. These findings suggest that higher doses of CPA may not stunt breast development relative to doses of CPA that are lower, although still quite high in terms of progestogenic activity.
In the second study, Yang et al. (2024), clinical outcomes in transfeminine people at the Peking University Third Hospital in China with estradiol plus spironolactone (n=43) versus estradiol plus CPA (n=53) were retrospectively compared. Testosterone levels were much higher in the spironolactone group relative to the CPA group (374 ng/dL [13.0 nmol/L] vs. 20 ng/dL [0.7 nmol/L]; p < 0.001) and duration of hormone therapy was shorter in the spironolactone group than in the CPA group (median 12 months vs. 18 months). Breast development satisfaction, measured with a visual analogue scale (VAS), was median 6.0 (IQR 4.0–7.0) with spironolactone and 6.0 (IQR 4.0–7.0) with CPA, and was not statistically different. On the other hand, the CPA group outperformed the spironolactone group in terms of several other VAS-based clinical-outcome measures, including figure feminization, testicular atrophy, decreased penile erections, and in terms of a composite overall satifaction score. These findings suggest, as with the RCT by Lachlan Angus and colleagues, that spironolactone and CPA result in similar breast development in transfeminine people despite differences in testosterone levels and other clinical outcomes.
Abduljalil, K., Furness, P., Johnson, T. N., Rostami-Hodjegan, A., & Soltani, H. (2012). Anatomical, Physiological and Metabolic Changes with Gestational Age during Normal Pregnancy. Clinical Pharmacokinetics, 51(6), 365–396. [DOI:10.2165/11597440-000000000-00000]
Adams, R. D., Kliman, B., Federman, D. D., Ulfelder, H. S., & Holmes, L. B. (1970). Syndromes of Testicular Feminization. Clinical Pediatrics, 9(3), 165–178. [DOI:10.1177/000992287000900312]
Alekseev, N. P. (2021). Origin and Development of the Mammary Glands. In Alekseev, N. P. Physiology of Human Female Lactation (pp. 11–66). Cham: Springer. [DOI:10.1007/978-3-030-66364-3_2]
Alex, A., Bhandary, E., & McGuire, K. P. (2020). Anatomy and Physiology of the Breast during Pregnancy and Lactation. In Alipour, S., & Omranipour, R. (Eds.). Diseases of the Breast during Pregnancy and Lactation (Advances in Experimental Medicine and Biology, Volume 1252) (pp. 3–7). Cham: Springer. [DOI:10.1007/978-3-030-41596-9]
Anderson, W. A. (1962). Experimental stimulation of breast development in the teen-age female. The Journal of the Medical Society of New Jersey, 59(10), 541–543. [Google Scholar] [PubMed] [PDF]
Andler, W., & Zachmann, M. (1979). Spontaneous breast development in an adolescent girl with testicular feminization after castration in early childhood. The Journal of Pediatrics, 94(2), 304–305. [DOI:10.1016/s0022-3476(79)80852-5]
Angus, L. M., Leemaqz, S., Zajac, J. D., & Cheung, A. S. (2023). A randomised controlled trial of spironolactone versus cyproterone in trans people commencing estradiol. AusPATH 2023 Symposium. [URL] [PDF] [Trans Health Research Blog Post]
Angus, L. M., Leemaqz, S. Y., Zajac, J. D., & Cheung, A. S. (2023). The effect of cyproterone and spironolactone on breast development in transgender women: a randomised controlled trial. ESA/SRB/ENSA 2023 ASM 26-29 November, Brisbane, 54–55 (abstract no. 132). [URL] [PDF] [Full Abstract Book] [Trans Health Research Blog Post]
Angus, L., Mikolajczyk, M., Cheung, A., Zajac, J., Antoszewski, B., & Kasielska-Trojan, A. (2022). Estimation of breast volume in transgender women using 2D photography: validation of the BreastIdea Volume Estimator in men and transgender women. ESA/SRB/APEG/NZSE ASM 2022, November 13-16, Christchurch, Abstracts and Programme, 127–127 (abstract no. 279). [URL] [PDF] [Full Abstract Book]
Apter, D. (1980). Serum steroids and pituitary hormones in female puberty: a partly longitudinal study. Clinical Endocrinology, 12(2), 107–120. [DOI:10.1111/j.1365-2265.1980.tb02125.x]
Apter, D., Räisänen, I., Ylöstalo, P., & Vihko, R. (1987). Follicular growth in relation to serum hormonal patterns in adolescent compared with adult menstrual cycles. Fertility and Sterility, 47(1), 82–88. [DOI:10.1016/s0015-0282(16)49940-1]
Aritaki, S., Miyazawa, H., Ogihara, M., Ushio, M., & Izumizawa, A. (1992). An Endocrinological Study of Persistent Pubertal Macromastia. The Tohoku Journal of Experimental Medicine, 167(3), 189–196. [DOI:10.1620/tjem.167.189]
Arya, S., Barnabas, R., Lila, A. R., Sarathi, V., Memon, S. S., Bhandare, V. V., Thakkar, K., Patil, V., Shah, N. S., Kunwar, A., & Bandgar, T. (2021). Clinical, Hormonal, Genetic, and Molecular Characteristics in Androgen Insensitivity Syndrome in an Asian Indian Cohort from a Single Centre in Western India. Sexual Development, 15(4), 253–261. [DOI:10.1159/000517763]
Asscheman, H., & Gooren, L. J. (1992). Hormone Treatment in Transsexuals. In Bocking, W. O., Coleman, E. (Eds). Gender Dysphoria: Interdisciplinary Approaches in Clinical Management (pp. 39–54). Binghamton: Haworth Press. / Journal of Psychology & Human Sexuality, 5(4), 39–54. [Google Scholar] [Google Books] [DOI:10.1300/J056v05n04_03]
Athanasoulia, A., Auer, M., Riepe, F., & Stalla, G. (2013). Rare Missense P450c17 (CYP17A1) Mutation in Exon 1 as a Cause of 46,XY Disorder of Sexual Development: Implications of Breast Tissue ‘Unresponsiveness’ despite Adequate Estradiol Substitution. Sexual Development, 7(4), 212–215. [DOI:10.1159/000348301]
Atwood, C., Hovey, R., Glover, J., Chepko, G., Ginsburg, E., Robison, W., & Vonderhaar, B. (2000). Progesterone induces side-branching of the ductal epithelium in the mammary glands of peripubertal mice. Journal of Endocrinology, 167(1), 39–52. [DOI:10.1677/joe.0.1670039]
Aupperlee, M. D., Leipprandt, J. R., Bennett, J. M., Schwartz, R. C., & Haslam, S. Z. (2013). Amphiregulin mediates progesterone-induced mammary ductal development during puberty. Breast Cancer Research, 15(3), R44. [DOI:10.1186/bcr3431]
Bahr, C., Ewald, J., Dragovich, R., & Gothard, M. D. (2024). Effects of progesterone on gender affirmation outcomes as part of feminizing hormone therapy. Journal of the American Pharmacists Association, 64(1), 268–272. [DOI:10.1016/j.japh.2023.08.001]
Baird, D., Hytten, F. E., & Thomson, A. M. (1958). Age and Human Reproduction. BJOG, 65(6), 865–876. [DOI:10.1111/j.1471-0528.1958.tb08582.x]
Baker, S. B., Burkey, B. A., Thornton, P., & LaRossa, D. (2001). Juvenile Gigantomastia: Presentation of Four Cases and Review of the Literature. Annals of Plastic Surgery, 46(5), 517–526. [DOI:10.1097/00000637-200105000-00011]
Bames, H. O. (1948). Reduction of massive breast hypertrophy. Plastic and Reconstructive Surgery, 3(5), 560–569. [DOI:10.1097/00006534-194809000-00006]
Barbieri, R. L. (2019). Breast. In Strauss, J. F., & Barbieri, R. L. (Eds.). Yen and Jaffe’s Reproductive Endocrinology: Physiology, Pathophysiology, and Clinical Management, 8th Edition (pp. 248–255.e3). Philadelphia: Elsevier. [Google Books] [DOI:10.1016/B978-0-323-47912-7.00010-X]
Baron, J. (1993). Zespół braku wrazliwości na androgeny. Studium kliniczne i endokrynologiczne 40 osobników [Androgen insensitivity syndrome. Clinical and endocrinologic study of 40 cases]. Endokrynologia Polska, 44(2), 175–186. [Google Scholar] [PubMed]
Baron, J. (1994). Klasyczne i niepełne zespoły braku wrazliwości na androgeny [Classical and incomplete androgen insensitivity syndromes]. Ginekologia Polska, 65(7), 377–386. [Google Scholar] [PubMed]
Baron, J. (1994). Niepełny lub cześciowy zespół braku wrazliwości na androgeny [Partial androgen insensitivity syndrome]. Ginekologia Polska, 65(6), 319–325. [Google Scholar] [PubMed]
Barrat, J., de Lignières, B., Marpeau, L., Larue, L., Fournier, S., Nahoul, K., Linares, G., Giorgi, H., & Contesso, G. (1990). Effet in vivo de l’administration locale de progestérone sur l’activité mitotique des galactophores humains. Résultat d’une étude pilote. [The in vivo effect of the local administration of progesterone on the mitotic activity of human ductal breast tissue. Results of a pilot study.] Journal de Gynecologie, Obstetrique et Biologie de la Reproduction, 19(3), 269–274. [Google Scholar 1] [Google Scholar 2] [PubMed]
Barrett, J. (2009). The clinical risks associated with the diagnosis and management of disorders of gender identity. Clinical Risk, 15(4), 131–134. [DOI:10.1258/cr.2008.080069]
Bässler, R. (1970). The Morphology of Hormone Induced Structural Changes in the Female Breast. In Altmann, H.-W., et al. (Eds.). Current Topics in Pathology: Ergebnisse der Pathology, Volume 53 (pp. 1–89). Heidelberg: Springer Berlin. [DOI:10.1007/978-3-662-30514-0_1]
Basson, R., & Prior, J. C. (1998). Hormonal Therapy of Gender Dysphoria: The Male-to-Female Transsexual. In Denny, D. (Ed.). Concepts in Transgender Identity (Garland Gay and Lesbian Studies, Volume 11) (pp. 277–296). New York: Garland Publishing Inc. [Google Scholar] [Google Books] [DOI:10.4324/9780203775134-19] [PDF]
Bauman, A., Novello, L., & Kreitzer, P. (2016). Endocrine Disorders and Delayed Puberty. In Appelbaum, H. (Ed.). Abnormal Female Puberty: A Clinical Casebook (pp. 87–107). Cham: Springer. [DOI:10.1007/978-3-319-27225-2_5]
Bayer, C. M., Bani, M. R., Schneider, M., Dammer, U., Raabe, E., Haeberle, L., Faschingbauer, F., Schneeberger, S., Renner, S. P., Fischer, D., Schulz-Wendtland, R., Fasching, P. A., Beckmann, M. W., & Jud, S. M. (2014). Assessment of breast volume changes during human pregnancy using a three-dimensional surface assessment technique in the prospective CGATE study. European Journal of Cancer Prevention, 23(3), 151–157. [DOI:10.1097/cej.0b013e3283651ccb]
Beck, P. (1972). Lactogenic Activity of Human Chorionic Somatomammotropin in Rhesus Monkeys. Experimental Biology and Medicine, 140(1), 183–187. [DOI:10.3181/00379727-140-36422]
Begley, D. J., Firth, J. A., & Hoult, J. R. (1980). The Breast and Lactation. In Begley, D. J., Firth, J. A., & Hoult, J. R. Human Reproduction and Developmental Biology (pp. 204–219). London: Macmillan Education UK. [DOI:10.1007/978-1-349-16260-4_14]
Bellwether, C. J. (2020). Why Should a Transfeminine Person Consider Progesterone? Google Docs. [URL]
Benjamin, H. (1966). Nonsurgical Management of Transsexualism. In Benjamin, H. The Transsexual Phenomenon (pp. 86–99). New York: Julian Press. [Google Scholar] [Google Books] [OpenLibrary] [WorldCat] [PDF]
Benjamin, H. (1967). Transvestism and Transsexualism in the male and female. Journal of Sex Research, 3(2), 107–127. [DOI:10.1080/00224496709550519]
Berliere, M., Coche, M., Lacroix, C., Riggi, J., Coyette, M., Coulie, J., Galant, C., Fellah, L., Leconte, I., Maiter, D., Duhoux, F. P., & François, A. (2022). Effects of Hormones on Breast Development and Breast Cancer Risk in Transgender Women. Cancers, 15(1), 245. [DOI:10.3390/cancers15010245]
Berryhill, G. E., Trott, J. F., & Hovey, R. C. (2016). Mammary gland development—It’s not just about estrogen. Journal of Dairy Science, 99(1), 875–883. [DOI:10.3168/jds.2015-10105]
Bertelloni, S., Dati, E., Baroncelli, G. I., & Hiort, O. (2011). Hormonal Management of Complete Androgen Insensitivity Syndrome from Adolescence Onward. Hormone Research in Paediatrics, 76(6), 428–433. [DOI:10.1159/000334162]
Bethea, C. L., Kohama, S. G., & Pecins-Thompson, M. (1997). Pituitary and Brain Actions of Estrogen and Progesterone in the Regulation of Primate Prolactin Secretion. In Pavlik, E. J. (Ed.). Estrogens, Progestins, and Their Antagonists: Functions and Mechanisms of Action (pp. 3–46). Boston: Birkhäuser. [DOI:10.1007/978-1-4612-2004-6_1]
Bevan, D. J. (2012). Progesterone for Breast Development? / Should Male-to-Female Transsexuals Take Progesterone as part of Hormone Therapy (HT) for Better Breast Development? Biopsychology of TSTG / Transgender Forum. [URL 1] [URL 2]
Bevan, D. J. (2019). Grow Your Own : Breast Development Update. Transgender Forum. [URL]
Beyer, C., Cruz, M. L., & Martinez-Manautou, J. (1970). Effect of Chlormadinone Acetate on Mammary Development and Lactation in the Rabbit. Endocrinology, 86(5), 1172–1174. [DOI:10.1210/endo-86-5-1172]
Biswas, S. K., Banerjee, S., Baker, G. W., Kuo, C., & Chowdhury, I. (2022). The Mammary Gland: Basic Structure and Molecular Signaling during Development. International Journal of Molecular Sciences, 23(7), 3883. [DOI:10.3390/ijms23073883]
Bland, K. I., Copeland, E. M., & Klimberg, V. S. (2018). Anatomy of the Breast, Axilla, Chest Wall, and Related Metastatic Sites. In Bland, K. I., Copeland, E. M., Klimberg, V. S., Gradishar, W. J., White, J., & Korourian, S. (Eds.). The Breast: Comprehensive Management of Benign and Malignant Diseases, 5th Edition (pp. 20–36.e2). Philadelphia: Elsevier. [DOI:10.1016/b978-0-323-35955-9.00002-7]
Bland, K. I., Harrison Howard, J., & Romrell, L. J. (2009). Congenital and Acquired Disturbances of Breast Development and Growth. In Bland, K. I., & Copeland, E. M. (Eds.). The Breast: Comprehensive Management of Benign and Malignant Diseases, 4th Edition (pp. 189–207). Philadelphia: Saunders/Elsevier. [Google Scholar] [Google Books] [OpenLibrary] [WorldCat]
Bondy, C. A., & Turner Syndrome Consensus Study Group. (2007). Care of girls and women with Turner syndrome: a guideline of the Turner Syndrome Study Group. The Journal of Clinical Endocrinology & Metabolism, 92(1), 10–25. [DOI:10.1210/jc.2006-1374]
Boogers, L., Infirri, S. S., Bouchareb, A., de Blok, C., Liberton, N., van Trotsenburg, P., Dreijerink, K., den Heijer, M., Wiepjes, C., & Hannema, S. (2022). The effect of timing of puberty suppression on breast development in trans girls; a cross-sectional study. Hormone Research in Paediatrics, 95(Suppl 2) [60th Annual Meeting of the European Society for Paediatric Endocrinology (ESPE), Rome, Italy, September 15–17, 2022], 390–391 (abstract no. P1-379). [Google Scholar] [DOI:10.1159/000525606] [URL] [PDF 1] [PDF 2]
Boyce, S. W., Hoffman, P. G., & Mathes, S. J. (1984). Recurrent Macromastia after Subcutaneous Mastectomy. Annals of Plastic Surgery, 13(6), 511–518. [DOI:10.1097/00000637-198412000-00008]
Bruck, H. G., & Müller, G. (1967). Zur Hormontherapie der Hypoplastischen Weiblichen Brust. [On Hormonal Therapy of the Hypoplastic Female Breast.] Ästhetische Medizin [Ästhetische Medizin : Kongreß-Organ der Deutschen Gesellschaft für die Ästhetische Medizin und ihre Grenzgebiete], 16(12), 365–366. [ISSN:0400-6755] [Google Scholar] [PubMed] [WorldCat] [PDF] [Translation]
Bryant, R., Underwood, A., Robinson, A., Stephenson, T., & Underwood, J. (1998). Determination of breast tissue composition for improved accuracy in estimating radiation doses and risks in mammographic screening. The Breast, 7(2), 95–98. [DOI:10.1016/s0960-9776(98)90064-9]
Buhimschi, C. S. (2004). Endocrinology of lactation. Obstetrics and Gynecology Clinics of North America, 31(4), 963–979. [DOI:10.1016/j.ogc.2004.08.002]
Camilletti, M. A., Abeledo-Machado, A., Faraoni, E. Y., Thomas, P., & Díaz-Torga, G. (2019). New insights into progesterone actions on prolactin secretion and prolactinoma development. Steroids, 152, 108496. [DOI:10.1016/j.steroids.2019.108496]
Çamtosun, E., Şıklar, Z., Ceylaner, S., Kocaay, P., & Berberoğlu, M. (2017). Delayed Diagnosis of a 17-Hydroxylase/17,20-Lyase Deficient Patient Presenting as a 46,XY Female: A Low Normal Potassium Level Can Be an Alerting Diagnostic Sign. Journal of Clinical Research in Pediatric Endocrinology, 9(2), 163–167. [DOI:10.4274/jcrpe.3839]
Capraro, V. J., & Dewhurst, C. J. (1975). Breast Disorders in Childhood and Adolescence. Clinical Obstetrics and Gynecology, 18(2), 25–50. [DOI:10.1097/00003081-197506000-00003]
Carlson, L. J., & Shaw, N. D. (2019). Development of Ovulatory Menstrual Cycles in Adolescent Girls. Journal of Pediatric and Adolescent Gynecology, 32(3), 249–253. [DOI:10.1016/j.jpag.2019.02.119]
Caro, T. M. (1987). Human breasts: Unsupported hypotheses reviewed. Human Evolution, 2(3), 271–282. [DOI:10.1007/bf03016112]
Ceriani, R. L. (1974). Hormones and Other Factors Controlling Growth in the Mammary Gland: A Review. Journal of Investigative Dermatology, 63(1), 93–108. [DOI:10.1111/1523-1747.ep12678104]
Cernea, R. (1944). Lokale Hormonbehandlung bei Mammaatrophie und Unterentwicklung. [Local Hormone Treatment in Mammary Atrophy and Underdevelopment.] Medizinische Klinik, 40(11/12), 169–170. [Google Scholar] [PDF] [Translation]
Chang, K., Lee, T. T., Linares-Cruz, G., Fournier, S., & de Ligniéres, B. (1995). Influences of percutaneous administration of estradiol and progesterone on human breast epithelial cell cycle in vivo. Fertility and Sterility, 63(4), 785–791. [DOI:10.1016/s0015-0282(16)57482-2]
Cheikhelard, A., Morel, Y., Thibaud, E., Lortat-Jacob, S., Jaubert, F., Polak, M., & Nihoul-Fekete, C. (2008). Long-Term Followup and Comparison Between Genotype and Phenotype in 29 Cases of Complete Androgen Insensitivity Syndrome. Journal of Urology, 180(4), 1496–1501. [DOI:10.1016/j.juro.2008.06.045]
Ciarloni, L., Mallepell, S., & Brisken, C. (2007). Amphiregulin is an essential mediator of estrogen receptor α function in mammary gland development. Proceedings of the National Academy of Sciences, 104(13), 5455–5460. [DOI:10.1073/pnas.0611647104]
Clendenen, T. V., Kim, S., Moy, L., Wan, L., Rusinek, H., Stanczyk, F. Z., Pike, M. C., & Zeleniuch-Jacquotte, A. (2013). Magnetic Resonance Imaging (MRI) of hormone-induced breast changes in young premenopausal women. Magnetic Resonance Imaging, 31(1), 1–9. [DOI:10.1016/j.mri.2012.06.022]
Cline, J. M., & Wood, C. E. (2006). Hormonal Effects on the Mammary Gland of Postmenopausal Nonhuman Primates. Breast Disease, 24(1), 59–70. [DOI:10.3233/bd-2006-24105]
Cline, J. M., & Wood, C. E. (2008). The Mammary Glands of Macaques. Toxicologic Pathology, 36(7 Suppl), 130S–141S. [DOI:10.1177/0192623308327411]
Cole, R. D., & Hopkins, T. R. (1962). A Biochemical Test of Artificial Mammogenesis and Lactogenesis As Models of the Natural Processes. Endocrinology, 70(3), 375–380. [DOI:10.1210/endo-70-3-375]
Coleman, E., Bockting, W., Botzer, M., Cohen-Kettenis, P., DeCuypere, G., Feldman, J., Fraser, L., Green, J., Knudson, G., Meyer, W. J., Monstrey, S., Adler, R. K., Brown, G. R., Devor, A. H., Ehrbar, R., Ettner, R., Eyler, E., Garofalo, R., Karasic, D. H., Lev, A. I., Mayer, G., Meyer-Bahlburg, H., Hall, B. P., Pfaefflin, F., Rachlin, K., Robinson, B., Schechter, L. S., Tangpricha, V., van Trotsenburg, M., Vitale, A., Winter, S., Whittle, S., Wylie, K. R., & Zucker, K. (2012). [World Professional Association for Transgender Health (WPATH)] Standards of Care for the Health of Transsexual, Transgender, and Gender-Nonconforming People, Version 7. International Journal of Transgenderism, 13(4), 165–232. [DOI:10.1080/15532739.2011.700873] [URL] [PDF]
Coleman, E., Radix, A. E., Bouman, W. P., Brown, G. R., de Vries, A. L., Deutsch, M. B., Ettner, R., Fraser, L., Goodman, M., Green, J., Hancock, A. B., Johnson, T. W., Karasic, D. H., Knudson, G. A., Leibowitz, S. F., Meyer-Bahlburg, H. F., Monstrey, S. J., Motmans, J., Nahata, L., … & Arcelus, J. (2022). [World Professional Association for Transgender Health (WPATH)] Standards of Care for the Health of Transgender and Gender Diverse People, Version 8. International Journal of Transgender Health, 23(Suppl 1), S1–S259. [DOI:10.1080/26895269.2022.2100644] [URL] [PDF]
Coltman, C. E., Steele, J. R., & McGhee, D. E. (2017). Breast volume is affected by body mass index but not age. Ergonomics, 60(11), 1576–1585. [DOI:10.1080/00140139.2017.1330968]
Colvin, C., Devineni, G., & Ashraf, A. P. (2014). Delayed Puberty. In Bandeira, F., Gharib, H., Golbert, A., Griz, L., & Faria, M. (Eds.). Endocrinology and Diabetes (pp. 203–217). New York: Springer. [DOI:10.1007/978-1-4614-8684-8_17]
Cowie, A. T., & Folley, S. J. (1961). The Mammary Gland and Lactation. In Young, W. C. (Ed.). Sex and Internal Secretions, 3rd Edition, Volume I (pp. 590–642). Baltimore: Williams & Wilkins. [Google Scholar] [Google Books] [OpenLibrary] [WorldCat] [Archive.org]
Cowie, A. T., Forsyth, I. A., & Hart, I. C. (1980). Growth and Development of the Mammary Gland. In Cowie, A. T., Forsyth, I. A., & Hart, I. C. Hormonal Control of Lactation (Monographs on Endocrinology, Volume 15) (pp. 58–145). Berlin/Heidelberg: Springer Berlin Heidelberg. [DOI:10.1007/978-3-642-81389-4_3]
Cox, D. B., Kent, J. C., Casey, T. M., Owens, R. A., & Hartmann, P. E. (1999). Breast Growth and the Urinary Excretion of Lactose During Human Pregnancy and Early Lactation: Endocrine Relationships. Experimental Physiology, 84(2), 421–434. [DOI:10.1111/j.1469-445x.1999.01807.x]
Cox, C. B., Kent, J. C., Owens, R., & Hartmann, P. E. (1994). Mammary morphological and functional changes during pregnancy in women. In Thompson, J. (Ed.). Proceedings of the Twenty-Sixth Annual Conference, Hilton Hotel, Brisbane, 26–28 September, 1994 [The Australian Society for Reproductive Biology Inc., Twenty Sixth Annual Conference, The Hilton Hotel, Brisbane, September 26 - 28 1994, Programme and Miniposters of Papers] (pp. 47–47). Australia: Australian Society for Reproductive Biology. [Google Scholar] [WorldCat] [URL] [PDF]
Coxon, J., & Seal, L. (2018). Hormone management of trans women. Trends in Urology & Men’s Health, 9(6), 10–14. [DOI:10.1002/tre.663]
Cregan, M. D., & Hartmann, P. E. (1999). Computerized Breast Measurement from Conception to Weaning: Clinical Implications. Journal of Human Lactation, 15(2), 89–96. [DOI:10.1177/089033449901500202]
Crowley, W. F., & Pitteloud, N. (2020). Approach to the patient with delayed puberty. UpToDate. [Google Scholar] [URL]
Cruz-Korchin, N., Korchin, L., González-Keelan, C., Climent, C., & Morales, I. (2002). Macromastia. Plastic and Reconstructive Surgery, 109(1), 64–68. [DOI:10.1097/00006534-200201000-00011]
Curtis, R. J. (2009 July 10). The Lowdown on Progesterone. London: The London Gender Clinic. [Google Scholar] [URL] [PDF]
Dallmann, A., Ince, I., Meyer, M., Willmann, S., Eissing, T., & Hempel, G. (2017). Gestation-Specific Changes in the Anatomy and Physiology of Healthy Pregnant Women: An Extended Repository of Model Parameters for Physiologically Based Pharmacokinetic Modeling in Pregnancy. Clinical Pharmacokinetics, 56(11), 1303–1330. [DOI:10.1007/s40262-017-0539-z]
Dancey, A., Khan, M., Dawson, J., & Peart, F. (2008). Gigantomastia – a classification and review of the literature. Journal of Plastic, Reconstructive & Aesthetic Surgery, 61(5), 493–502. [DOI:10.1016/j.bjps.2007.10.041]
Davajan, V., & Kletzky, O. A. (1979). Amenorrhea without Galactorrhea or Hirsutism. In Mishell, D. R., & Davajan, V. (Eds.). Reproductive Endocrinology, Infertility, and Contraception (pp. 219–248). Philadelphia: F. A. Davis Co. [Google Scholar] [Google Books] [OpenLibrary] [WorldCat] [Archive.org]
Davis, M. E., Boynton, M. W., Ferguson, J. H., & Rothman, S. (1945). Studies on Pigmentation of Endocrine Origin. The Journal of Clinical Endocrinology & Metabolism, 5(3), 138–146. [DOI:10.1210/jcem-5-3-138]
de Blok, C. J., Dijkman, B. A., Wiepjes, C. M., Staphorsius, A. S., Timmermans, F. W., Smit, J. M., Dreijerink, K. M., & den Heijer, M. (2021). Sustained Breast Development and Breast Anthropometric Changes in 3 Years of Gender-Affirming Hormone Treatment. The Journal of Clinical Endocrinology & Metabolism, 106(2), e782–e790. [DOI:10.1210/clinem/dgaa841]
de Blok, C. J., Klaver, M., Wiepjes, C. M., Nota, N. M., Heijboer, A. C., Fisher, A. D., Schreiner, T., T’Sjoen, G., & den Heijer, M. (2017). Breast Development in Transwomen After 1 Year of Cross-Sex Hormone Therapy: Results of a Prospective Multicenter Study. The Journal of Clinical Endocrinology & Metabolism, 103(2), 532–538. [DOI:10.1210/jc.2017-01927]
de Lignières, B. (2002). Effects of progestogens on the postmenopausal breast. Climacteric, 5(3), 229–235. [DOI:10.1080/cmt.5.3.229.235]
de Lignières, B., & Mauvais-Jarvis, P. (1981). Hormonal Dependence of Benign Breast Disease, Gynecomastia and Breast Cancer. In Hollman, K. H., Brux, J., & Verley, J. M. (Eds.). New Frontiers in Mammary Pathology (pp. 287–308). Boston: Springer US. [DOI:10.1007/978-1-4757-0019-0_17]
de Vries, A. L., Steensma, T. D., Wagemaar, E. C. F., Doreleijers, T. A., & Cohen-Kettenis, P. T. (2010). Puberty suppression followed by cross-sex hormones and gender reassignment surgery: A prospective follow-up of gender dysphoric adolescents into adulthood. In de Vries, A. L. (Ed.). Gender Dysphoria in Adolescents: Mental Health and Treatment Evaluation (pp. 91–106). (Doctoral thesis, Vrije Universiteit Amsterdam.) [Google Scholar] [URL] [PDF]
Deeb, A., Al Suwaidi, H., Attia, S., & Al Ameri, A. (2015). 17-hydroxylase/17,20-lyase deficiency due to a R96Q mutation causing hypertension and poor breast development. Endocrinology, Diabetes & Metabolism Case Reports, 2015(1), 15-0069. [DOI:10.1530/EDM-15-0069]
Deepinder, F., & Braunstein, G. D. (2012). Drug-induced gynecomastia: an evidence-based review. Expert Opinion on Drug Safety, 11(5), 779–795. [DOI:10.1517/14740338.2012.712109]
Dennerstein, L., Burrows, G. D., Hyman, G. J., & Sharpe, K. (1980). Some clinical effects of oestrogen-progestogen therapy in surgically castrated women. Maturitas, 2(1), 19–28. [DOI:10.1016/0378-5122(80)90056-0]
Dewhurst, C. J. (1971). Sex Chromosome Abnormalities and the Gynaecologist. BJOG, 78(12), 1058–1076. [DOI:10.1111/j.1471-0528.1971.tb00227.x]
Dewhurst, C. J. (1971). The XY female. American Journal of Obstetrics and Gynecology, 109(5) [Transactions of the Eighty-First Annual Meeting of the American Association of Obstetricians and Gynecologists], 675–688. [DOI:10.1016/0002-9378(71)90753-8]
Dewhurst, C. (1972). Amenorrhoea and the Paediatrician. Pediatric Clinics of North America, 19(3), 605–618. [DOI:10.1016/s0031-3955(16)32741-9]
Dewhurst, C. J., & Spence, J. E. (1977). The XY female. British Journal of Hospital Medicine, 17(5), 498, 501–506. [Google Scholar] [PubMed] [PDF]
Dewhurst, J. (1981). Breast Disorders in Children and Adolescents. Pediatric Clinics of North America, 28(2), 287–308. [DOI:10.1016/s0031-3955(16)33997-9]
Dewhurst, J. (1982). Breast Hypoplasia. In Bruni, V., Gasparri, F., Dewhurst, J., & Rey-Stocker, I. (Eds.). Pediatric and Adolescent Gynaecology [Proceedings of the IVth International Symposium, Florence, October 5-7, 1978] (pp. 205–212). Rome, Italy: Serono Symposia. [Google Scholar] [Google Books] [WorldCat] [PDF]
Di Lorenzo, G., Autorino, R., Perdonà, S., & De Placido, S. (2005). Management of gynaecomastia in patients with prostate cancer: a systematic review. The Lancet Oncology, 6(12), 972–979. [DOI:10.1016/s1470-2045(05)70464-2]
Dickson, L. M., & Hewer, E. E. (1950). The structure of the breast. In Saner, F. D. (Ed.). The Breast: Structure, Function, Disease (pp. 1–52). Baltimore: William & Wilins. [Google Scholar] [Google Books] [OpenLibrary] [WorldCat] [URL] [PDF]
Dijkman, B. A., Blok, C. J., Dreijerink, K. M., & den Heijer, M. (2023). Progestin-related breast volume changes in a woman with complete androgen insensitivity syndrome (CAIS). Endocrinology, Diabetes & Metabolism Case Reports, 2023(2), 22-0346. [DOI:10.1530/edm-22-0346]
Dijkman, B. A., Helder, D., Boogers, L. S., Gieles, N. C., van Heesewijk, J. O., Slaa, S. t., Liberton, N. P., Wiepjes, C. M., de Blok, C. J., den Heijer, M., & Dreijerink, K. M. (2023). Addition of progesterone to feminizing gender-affirming hormone therapy in transgender individuals for breast development: a randomized controlled trial. BMC Pharmacology and Toxicology, 24(1), 80. [DOI:10.1186/s40360-023-00724-4]
Dittrich, R., Binder, H., Cupisti, S., Hoffmann, I., Beckmann, M., & Mueller, A. (2005). Endocrine Treatment of Male-to-Female Transsexuals Using Gonadotropin-Releasing Hormone Agonist. Experimental and Clinical Endocrinology & Diabetes, 113(10), 586–592. [DOI:10.1055/s-2005-865900]
Donaldson, M., Kriström, B., Ankarberg-Lindgren, C., Verlinde, S., van Alfen-van der Velden, J., Gawlik, A., van Gelder, M., Sas, T., & (2019). Optimal Pubertal Induction in Girls with Turner Syndrome Using Either Oral or Transdermal Estradiol: A Proposed Modern Strategy. Hormone Research in Paediatrics, 91(3), 153–163. [DOI:10.1159/000500050]
Dorgan, J. F., Klifa, C., Deshmukh, S., Egleston, B. L., Shepherd, J. A., Kwiterovich, P. O., Van Horn, L., Snetselaar, L. G., Stevens, V. J., Robson, A. M., Lasser, N. L., & Hylton, N. M. (2013). Menstrual and reproductive characteristics and breast density in young women. Cancer Causes & Control, 24(11), 1973–1983. [DOI:10.1007/s10552-013-0273-2]
Döring, G. K. (1963). Über die relative Häufigkeit des anovulatorischen Cyclus im Leben der Frau. [On the relative frequency of the anovulatory cycle in women’s lives.] Archiv für Gynäkologie, 199(2), 115–123. [DOI:10.1007/bf00668062]
Drąsutis, J. (2017). Changes in breast morphological parameters, body size and shape, blood serum prolactin and lipids during pregnancy, multiple relationships of these indicators and morphological markers for health risk. (Doctoral dissertation, Vilniaus Universitetas.) [Google Scholar] [URL]
Drife, J. O. (1982). The effects of parity and the menstrual cycle on the normal mammary gland and their possible relationship to malignant change. (Doctoral dissertation, University of Edinburgh). [Google Scholar] [Google Books] [WorldCat] [URL] [PDF]
Drife, J. O. (1984). The pill and the breast. IPPF Medical Bulletin, 18(6), 1–2. [Google Scholar] [PubMed]
Drife, J. O. (1986). Breast Development in Puberty. Annals of the New York Academy of Sciences, 464(1) [Endocrinology of the Breast: Basic and Clinical Aspects], 58–65. [DOI:10.1111/j.1749-6632.1986.tb15993.x]
Drife, J. O. (1989). Breast modifications during the menstrual cycle. Supplement to International Journal of Gynecology and Obstetrics, 1, 19–24. / International Journal of Gynecology and Obstetrics, 1989(Suppl 1), 19–24. [Google Scholar] [PubMed] [Archive.org]
Drife, J. O. (1990). Premenopausal Hormone Therapy. In Drife, J. O., & Studd, J. W. W. (Eds.). HRT and Osteoporosis (pp. 351–362). London: Springer London. [DOI:10.1007/978-1-4471-1799-5_25]
Duncan, M. (2010). Sexual Selection and Human Breast Morphology. (Doctoral dissertation, Te Herenga Waka-Victoria University of Wellington.) [Google Scholar] [URL]
Edmonds, D. K. (1989). Normal Puberty. In Edmonds, D. K. Dewhurst’s Practical Paediatric and Adolescent Gynaecology, 2nd Edition (pp. 56–62). London: Butterworths. [Google Scholar] [Google Books] [OpenLibrary] [WorldCat] [URL] [Archive.org]
Elling, S. V., & Powell, F. C. (1997). Physiological changes in the skin during pregnancy. Clinics in Dermatology, 15(1), 35–43. [DOI:10.1016/s0738-081x(96)00108-3]
Engman, M., Skoog, L., Soderqvist, G., & Gemzell-Danielsson, K. (2008). The effect of mifepristone on breast cell proliferation in premenopausal women evaluated through fine needle aspiration cytology. Human Reproduction, 23(9), 2072–2079. [DOI:10.1093/humrep/den228]
Federici, S., Goggi, G., Quinton, R., Giovanelli, L., Persani, L., Cangiano, B., & Bonomi, M. (2021). New and Consolidated Therapeutic Options for Pubertal Induction in Hypogonadism: In-depth Review of the Literature. Endocrine Reviews, 43(5), 824–851. [DOI:10.1210/endrev/bnab043]
Fernández-Cancio, M., García-García, E., González-Cejudo, C., Martínez-Maestre, M., Mangas-Cruz, M., Guerra-Junior, G., Pandi de Mello, M., Arnhold, I. J., Nishi, M. Y., Bilharinho Mendonça, B., García-Arumí, E., Audí, L., Tizzano, E., & Carrascosa, A. (2017). Discordant Genotypic Sex and Phenotype Variations in Two Spanish Siblings with 17α-Hydroxylase/17,20-Lyase Deficiency Carrying the Most Prevalent Mutated CYP17A1 Alleles of Brazilian Patients. Sexual Development, 11(2), 70–77. [DOI:10.1159/000468160]
Fernandez-Valdivia, R., Mukherjee, A., Mulac-Jericevic, B., Conneely, O. M., DeMayo, F. J., Amato, P., & Lydon, J. P. (2005). Revealing Progesterone’s Role in Uterine and Mammary Gland Biology: Insights from the Mouse. Seminars in Reproductive Medicine, 23(1), 22–37. [DOI:10.1055/s-2005-864031]
Finkenzeller, D. A., & Loveless, M. B. (2007). Pediatric Gynecology. In Fortner, K. B., Szymanski, L. M., Fox, H. E., & Wallach, E. E. (Eds.). The Johns Hopkins Manual of Gynecology and Obstetrics, 3rd Edition (Spiral Manual Series) (pp. 363–379). Philadelphia: Lippincott Williams & Wilkins. [Google Scholar] [Google Books] [OpenLibrary] [WorldCat]
Fisher, A. D., Castellini, G., Ristori, J., Casale, H., Cassioli, E., Sensi, C., Fanni, E., Amato, A. M., Bettini, E., Mosconi, M., Dèttore, D., Ricca, V., & Maggi, M. (2016). Cross-Sex Hormone Treatment and Psychobiological Changes in Transsexual Persons: Two-Year Follow-Up Data. The Journal of Clinical Endocrinology & Metabolism, 101(11), 4260–4269. [DOI:10.1210/jc.2016-1276]
Foidart, J. M., Colin, C., Denoo, X., Desreux, J., Fournier, S., & de Linières, B. (1996). Influence of percutaneous administration of estradiol and progesterone on the proliferation of human breast epithelial cells. In Calvo, F., Crépin, M., & Magdelenat, H. (Eds.). Breast Cancer: Advances in Biology and Therapeutics [21st Meeting of the International Association for Breast Cancer Research, July 3-4-5, 1996, Paris] (pp. 329–334). Montrouge/Paris: John Libbey Eurotext. [Google Scholar] [Google Books] [OpenLibrary] [WorldCat]
Foidart, J., Colin, C., Denoo, X., Desreux, J., Béliard, A., Fournier, S., & de Lignières, B. (1998). Estradiol and Progesterone Regulate the Proliferation of Human Breast Epithelial Cells. Fertility and Sterility, 69(5), 963–969. [DOI:10.1016/s0015-0282(98)00042-9]
Folley, S. J. (1947). Endocrine Control of the Mammary Gland. British Medical Bulletin, 5(2–3), 130–134. [DOI:10.1093/oxfordjournals.bmb.a073121]
Folley, S. J. (1950). Lactational Physiology. In Bowes, K. (Ed.). Modern Trends in Obstetrics and Gynaecology (pp. 441–453). London: Butterworth. [Google Scholar] [Google Books] [OpenLibrary] [WorldCat] [PDF]
Folley, S. J. (1952). Lactation. In Parkes, A. S. (Ed.). Marshall’s Physiology of Reproduction, 3rd Edition, Volume II (pp. 525–647). Longmans, Green & Co.: London. [Google Scholar] [Google Books] [OpenLibrary] [WorldCat] [PDF]
Folley, S. J. (1956). Recent Studies on the Development of the Mammary Gland. In Folley, S. J. The Physiology and Biochemistry of Lactation, 1st Edition (pp. 1–22). Edinburgh: Oliver & Boyd. [Google Scholar] [Google Books] [OpenLibrary] [WorldCat]
Folley, S. J., & Malpress, F. H. (1948). Hormonal Control of Mammary Growth. In Pincus, G., & Thimann, K. V. (Eds.). The Hormones: Physiology, Chemistry and Applications, Volume I (pp. 695–743). New York: Academic Press. [Google Scholar] [Google Books] [OpenLibrary] [WorldCat] [PDF]
Fourcade, R., & McLeod, D. (2004). Tolerability of Antiandrogens in the Treatment of Prostate Cancer. UroOncology, 4(1), 5–13. [DOI:10.1080/1561095042000191655]
Fowler, P. A., Casey, C. E., Cameron, G. G., Foster, M. A., & Knight, C. H. (1990). Cyclic changes in composition and volume of the breast during the menstrual cycle, measured by magnetic resonance imaging. BJOG, 97(7), 595–602. [DOI:10.1111/j.1471-0528.1990.tb02546.x]
Fridriksdottir, A. J., Petersen, O. W., & Rnnov-Jessen, L. (2011). Mammary gland stem cells: current status and future challenges. The International Journal of Developmental Biology, 55(7–8–9), 719–729. [DOI:10.1387/ijdb.113373af]
Fuqua, J. S., & Eugster, E. A. (2022). History of Puberty: Normal and Precocious. Hormone Research in Paediatrics, 95(6), 568–578. [DOI:10.1159/000526464]
Gaede, P., Trolle, D., & Pedersen, H. (1978). Extremely low placental lactogen hormone (hpl) values in an otherwise uneventful pregnancy preceding delivery of a normal baby. Acta Obstetricia et Gynecologica Scandinavica, 57(3), 203–209. [DOI:10.3109/00016347809154883]
Galani, A., Kitsiou-Tzeli, S., Sofokleous, C., Kanavakis, E., & Kalpini-Mavrou, A. (2008). Androgen insensitivity syndrome: clinical features and molecular defects. Hormones, 7(3), 217–229. [DOI:10.14310/horm.2002.1201]
Galbarczyk, A. (2011). Unexpected changes in maternal breast size during pregnancy in relation to infant sex: An evolutionary interpretation. American Journal of Human Biology, 23(4), 560–562. [DOI:10.1002/ajhb.21177]
Gawlik, A., Hankus, M., Such, K., Drosdzol-Cop, A., Madej, P., Borkowska, M., Zachurzok, A., & Malecka-Tendera, E. (2016). Hypogonadism and Sex Steroid Replacement Therapy in Girls with Turner Syndrome. Journal of Pediatric and Adolescent Gynecology, 29(6), 542–550. [DOI:10.1016/j.jpag.2016.03.005]
Gershon-Cohen, J. (1970). The Normal Breast. In Gershon-Cohen, J. Atlas of Mammography (pp. 23–38). Berlin/Heidelberg: Springer. [DOI:10.1007/978-3-642-85678-5_4] [Google Books]
Gertig, D. M., Stillman, I. E., Byrne, C., Spiegelman, D., Schnitt, S. J., Connolly, J. L., Colditz, G. A., & Hunter, D. J. (1999). Association of age and reproductive factors with benign breast tissue composition. Cancer Epidemiology, Biomarkers & Prevention, 8(10), 873–879. [Google Scholar] [PubMed] [URL]
Geschickter, C. F. (1945). Endocrine Physiology of the Breast. In Geschickter, C. F. Diseases of the Breast: Diagnosis, Pathology, Treatment, 2nd Edition (pp. 42–81). Philadelphia: J.B. Lippincott. [Google Scholar] [Google Books] [OpenLibrary] [WorldCat] [PDF]
Glenn, J. F. (1976). Testicular feminization syndrome current clinical considerations. Urology, 7(6), 569–577. [DOI:10.1016/0090-4295(76)90079-0]
Gliosci, A., & Presutti, F. (1993). Virginal gigantomastia: Validity of combined surgical and hormonal treatments. Aesthetic Plastic Surgery, 17(1), 61–65. [DOI:10.1007/bf00455051]
Gompel, A., & Plu-Bureau, G. (2018). Progesterone, progestins and the breast in menopause treatment. Climacteric, 21(4), 326–332. [DOI:10.1080/13697137.2018.1476483]
Goodman, H. M. (2009). Hormonal Control of Pregnancy and Lactation. In Goodman, H. M. Basic Medical Endocrinology, 4th Edition (pp. 277–301). Amsterdam: Academic Press/Elsevier. [DOI:10.1016/b978-0-12-373975-9.00014-8]
Gooren, L. J. (2016). Hormone Treatment of Adult Transgender People. In Ettner, R., Monstrey, S., & Coleman, E. (Eds.). Principles of Transgender Medicine and Surgery, 2nd Edition (pp. 167–179). New York: Routledge. [Google Scholar] [Google Books] [DOI:10.4324/9781315718972-11]
Gordon, C. M., & Laufer, M. R. (2005) The Physiology of Puberty. In Emans, S. J., Laufer, M. R., & Goldstein, D. P. (Eds.). Pediatric and Adolescent Gynecology, 5th Edition (pp. 120–155). Philadelphia: Lippincott Williams & Wilkins. [Google Scholar] [Google Books] [OpenLibrary] [WorldCat] [Archive.org]
Göretzlehner, G. & Lauritzen, C. (1992). Hormontherapie bei Gynäkologischen Erkrankungen [Hormone Therapy for Gynecological Diseases]. In Göretzlehner, G. & Lauritzen, C. Praktische Hormontherapie in der Gynäkologie, 1. Auflage [Practical Hormone Therapy in Gynecology, 1st Edition] (pp. 245–299). Berlin/New York: de Gruyter. [DOI:10.1515/9783112417706-007] [Google Books] [PDF] [Translation]
Graham, J. D., & Clarke, C. L. (1997). Physiological Action of Progesterone in Target Tissues. Endocrine Reviews, 18(4), 502–519. [DOI:10.1210/edrv.18.4.0308]
Graham, S. J., Stanchev, P. L., Lloyd‐Smith, J. O., Bronskill, M. J., & Plewes, D. B. (1995). Changes in Fibroglandular Volume and Water Content of Breast Tissue During the Menstrual Cycle Observed by MR Imaging at 1.5 T. Journal of Magnetic Resonance Imaging, 5(6), 695–701. [DOI:10.1002/jmri.1880050613]
Greydanus, D. E., Omar, H. A., Matytsina, L. A., & Tsitsika, A. (2010). Breast Disorders in Children and Adolescents. In Omar, H. A., Greydanus, D. E., Tsitsika, A. K., Patel, D. R., & Merrick, J. (Eds.). Pediatric and Adolescent Sexuality and Gynecology: Principles for the Primary Care Clinician (pp. 245–316). Hauppauge: Nova Science Publishers. [Google Scholar] [Google Books] [URL] [OpenLibrary] [WorldCat] [PDF]
Guaragna-Filho, G., Guerra-Junior, G., Tadokoro-Cuccaro, R., Hughes, I. A., Barros, B. A., Hiort, O., Balsamo, A., Guran, T., Holterhus, P. M., Hannema, S., Poyrazoglu, S., Darendeliler, F., Bryce, J., Ahmed, S. F., & Quigley, C. A. (2023). Pubertal and Gonadal Outcomes in 46,XY Individuals with Partial Androgen Insensitivity Syndrome Raised as Girls. Sexual Development, 17(1), 16–25. [DOI:10.1159/000526997]
Gunn, H. M., Tsai, M., McRae, A., & Steinbeck, K. S. (2018). Menstrual Patterns in the First Gynecological Year: A Systematic Review. Journal of Pediatric and Adolescent Gynecology, 31(6), 557–565.e6. [DOI:10.1016/j.jpag.2018.07.009]
Günzel, P., Hasan, S. H., Düsterberg, B., Hümpel, M., Putz, B., & Lehmann, M. (1987). Zur toxikologischen Prüfung von Steroidhormonen. [For the Toxicological Testing of Steroid Hormones.] In Burger, O. K., Grosdanoff, P., Henschler, D., Kraupp, O., & Schnieders, B. (Eds.). Aktuelle Probleme der Biomedizin (pp. 93–112). Berlin/New York: De Gruyter. [Google Scholar] [Google Books] [DOI:10.1515/9783110898231-014]
Hagisawa, S., Shimura, N., & Arisaka, O. (2012). Effect of Excess Estrogen on Breast and External Genitalia Development in Growth Hormone Deficiency. Journal of Pediatric and Adolescent Gynecology, 25(3), e61–e63. [DOI:10.1016/j.jpag.2011.11.005]
Hamburger, C., & Benjamin, H. (1969). Endocrine Treatment of Male and Female Transsexualism / Appendix for the Practicing Physician: Suggestions and Guidelines for the Management of Transsexuals. In Green, R., & Money, J. (Eds.). Transsexualism and Sex Reassignment (pp. 291–307). Baltimore: John Hopkins University Press. [Google Scholar] [Google Books] [PDF]
Hannan, F. M., Elajnaf, T., Vandenberg, L. N., Kennedy, S. H., & Thakker, R. V. (2022). Hormonal regulation of mammary gland development and lactation. Nature Reviews Endocrinology, 19(1), 46–61. [DOI:10.1038/s41574-022-00742-y]
Hannema, S. E., Schagen, S. E., Cohen-Kettenis, P. T., & Delemarre-van de Waal, H. A. (2017). Efficacy and Safety of Pubertal Induction Using 17β-Estradiol in Transgirls. The Journal of Clinical Endocrinology & Metabolism, 102(7), 2356–2363. [DOI:10.1210/jc.2017-00373]
Hartmann, B. W., Laml, T., Albrecht, A. E., Huber, J. C., & Kirchengast, S. (1998). Hormonal Breast Augmentation: Prognostic Relevance of Insulin-Like Growth Factor-I. Gynecological Endocrinology, 12(2), 123–127. [DOI:10.3109/09513599809024960]
Hartmann, P. E., Owens, R. A., Cox, D. B., & Kent, J. C. (1996). Breast Development and Control of Milk Synthesis. Food and Nutrition Bulletin, 17(4), 1–12. [DOI:10.1177/156482659601700404]
Hasan, S. (1974). Steroid Hormone Levels During Pregnancy in Various Species. In Bernhard, S., & Raspé, G. (Ed.). Hormones and Embryonic Development (Advances in the Biosciences, Volume 13) (pp. 181–197). Oxford/New York: Pergamon Press. [Google Scholar] [Google Books] [DOI:10.1016/b978-0-08-018239-1.50014-3] [OpenLibrary] [Archive.org]
Hassiotou, F., & Geddes, D. (2012). Anatomy of the human mammary gland: Current status of knowledge. Clinical Anatomy, 26(1), 29–48. [DOI:10.1002/ca.22165]
Heath, R. A., & Wynne, K. (2019). Children and Adolescents. In Heath, R. A., & Wynne, K. A Guide to Transgender Health: State-of-the-art Information for Gender-Affirming People and Their Supporters (pp. 87–106). Santa Barbara: Praeger/ABC-CLIO. [Google Books]
Heath, R. A., & Wynne, K. (2019). Hormone and Surgical Therapies for Adults. In Heath, R. A., & Wynne, K. A Guide to Transgender Health: State-of-the-art Information for Gender-Affirming People and Their Supporters (pp. 107–146). Santa Barbara: Praeger/ABC-CLIO. [Google Books]
Hertz, R., Odell, W. D., & Ross, G. T. (1966). Diagnostic Implications of Primary Amenorrhea: Combined Clinical Staff Conference at the National Institutes of Health. Annals of Internal Medicine, 65(4), 800–820. [DOI:10.7326/0003-4819-65-4-800]
Hillard, P. J. A. (2007). Benign Diseases of the Female Reproductive Tract. In Berek, J. S., & Novak, E. (Eds.). Berek & Novak’s Gynecology, 14th Edition (pp. 431–496). Philadelphia: Lippincott Williams and Wilkins. [Google Scholar] [OpenLibrary] [WorldCat] [Archive.org]
Hoppe, I. C., Patel, P. P., Singer-Granick, C. J., & Granick, M. S. (2011). Virginal Mammary Hypertrophy: A Meta-Analysis and Treatment Algorithm. Plastic and Reconstructive Surgery, 127(6), 2224–2231. [DOI:10.1097/prs.0b013e3182131bd1]
Hovey, R. C., Trott, J. F., Ginsburg, E., Goldhar, A., Sasaki, M. M., Fountain, S. J., Sundararajan, K., & Vonderhaar, B. K. (2001). Transcriptional and spatiotemporal regulation of prolactin receptor mRNA and cooperativity with progesterone receptor function during ductal branch growth in the mammary gland. Developmental Dynamics, 222(2), 192–205. [DOI:10.1002/dvdy.1179]
Howard, B. A., & Gusterson, B. A. (2000). Human Breast Development. Journal of Mammary Gland Biology and Neoplasia, 5(2), 119–137. [DOI:10.1023/a:1026487120779]
Huffman, J., Dewhurst, C. J., & Capraro, V. J. (1981). The Breast and its Disorders in Childhood and Adolescence. In Huffman, J., Dewhurst, J., & Capraro, V. The Gynecology of Childhood and Adolescence, 2nd Edition (pp. 542–559). Philadelphia: Saunders. [Google Scholar] [Google Books] [OpenLibrary] [WorldCat] [Archive.org] [PDF]
Hussain, Z., Brooks, J., & Percy, D. (2008). Menstrual variation of breast volume and T2 relaxation times in cyclical mastalgia. Radiography, 14(1), 8–16. [DOI:10.1016/j.radi.2006.07.003]
Hussain, Z., Roberts, N., Whitehouse, G. H., García-Fiñana, M., & Percy, D. (1999). Estimation of breast volume and its variation during the menstrual cycle using MRI and stereology. The British Journal of Radiology, 72(855), 236–245. [DOI:10.1259/bjr.72.855.10396212]
Hutson, S. W., Cowen, P. N., & Bird, C. C. (1985). Morphometric studies of age related changes in normal human breast and their significance for evolution of mammary cancer. Journal of Clinical Pathology, 38(3), 281–287. [DOI:10.1136/jcp.38.3.281]
Hytten, F. E. (1954). Clinical and Chemical Studies in Human Lactation–VI. BMJ, 1(4867), 912–915. [DOI:10.1136/bmj.1.4867.912]
Hytten, F. E. (1976). The physiology of lactation. International Journal of Food Sciences and Nutrition, 30(4), 225–232. [DOI:10.3109/09637487609142745]
Hytten, F. E., & Baird, D. (1958). The Development of the Nipple in Pregnancy. The Lancet, 271(7032), 1201–1204. [DOI:10.1016/s0140-6736(58)91908-1]
Hytten, F. E., & Leitch, I. (1971). Preparations for Breast Feeding. In Hytten, F. E., & Leitch, I. The Physiology of Human Pregnancy, 2nd Edition (pp. 234–241). Oxford: Blackwell Scientific Publications. [Google Scholar] [Google Books] [OpenLibrary] [WorldCat] [Archive.org]
Hytten, F. E., & Leitch, I. (1971). Preparations for Breast Feeding. In Hytten, F. E., & Leitch, I. The Physiology of Human Pregnancy, 2nd Edition (pp. 234–241). Oxford: Blackwell Scientific Publications. [Google Scholar] [Google Books] [OpenLibrary] [WorldCat] [Archive.org]
Hytten, F. E., & Thomson, A. M. (1965). Pregnancy, childbirth and lactation. In Edholm, O. G., & Bacharach, A. L. (Eds.). The Physiology of Human Survival (pp. 327–350). London/New York: Academic Press. [Google Scholar] [Google Books] [OpenLibrary] [WorldCat] [Archive.org]
Hytten, F. E., & Thomson, A. M. (1968). Maternal physiological adjustments. In Assali, N. S. (Ed.). The Maternal Organism, Volume I (Biology of Gestation) (pp. 449–479). New York: Academic Press. [Google Scholar] [Google Books] [WorldCat]
Igo, J., & Visram, H. (2021). Progesterone Therapy Use and Safety in Male to Female Transgender Patients. Canadian Journal of Diabetes, 45(7 Suppl), S39–S39 (abstract no. 109). [DOI:10.1016/j.jcjd.2021.09.119] [URL]
Ingleby, H. (1949). Changes in breast volume in a group of normal young women. Bulletin of the International Association of Medical Museums, 29, 87–92. [Google Scholar] [Google Books] [HathiTrust]
Ingleby, H., Moore, L., & Gershon-Cohen, J. (1957). Gestational breast changes: x-ray studies of the human breast. Obstetrics & Gynecology, 10(2), 149–157. [Google Scholar] [PubMed] [URL]
Ismail, P. M., Amato, P., Soyal, S. M., DeMayo, F. J., Conneely, O. M., O’Malley, B. W., & Lydon, J. P. (2003). Progesterone involvement in breast development and tumorigenesis—as revealed by progesterone receptor “knockout” and “knockin” mouse models. Steroids, 68(10–13), 779–787. [DOI:10.1016/s0039-128x(03)00133-8]
Iwamoto, S. J., Defreyne, J., Rothman, M. S., Van Schuylenbergh, J., Van de Bruaene, L., Motmans, J., & T’Sjoen, G. (2019). Health considerations for transgender women and remaining unknowns: a narrative review. Therapeutic Advances in Endocrinology and Metabolism, 10, 204201881987116. [DOI:10.1177/2042018819871166]
Jacobsohn, D. (1961). Hormonal Regulation of Mammary Gland Growth. In Kon, S. K., & Cowie, A. T. (Eds.). Milk: The Mammary Gland and Its Secretion, Volume 1 (pp. 127–160). New York: Academic Press. [Google Scholar] [Google Books] [OpenLibrary] [WorldCat] [PDF]
Jain, J., Kwan, D., & Forcier, M. (2019). Medroxyprogesterone Acetate in Gender-Affirming Therapy for Transwomen: Results From a Retrospective Study. The Journal of Clinical Endocrinology & Metabolism, 104(11), 5148–5156. [DOI:10.1210/jc.2018-02253]
Jamal, N., Ng, K., McLean, D., Looi, L., & Moosa, F. (2004). Mammographic Breast Glandularity in Malaysian Women: Data Derived from Radiography. American Journal of Roentgenology, 182(3), 713–717. [DOI:10.2214/ajr.182.3.1820713]
Jemstrom, H., & Olsson, H. (1997). Breast Size in Relation to Endogenous Hormone Levels, Body Constitution, and Oral Contraceptive Use in Healthy Nulligravid Women Aged 19-25 Years. American Journal of Epidemiology, 145(7), 571–580. [DOI:10.1093/oxfordjournals.aje.a009153]
Jernström, H., Sandberg, T., Bågeman, E., Borg, Å., & Olsson, H. (2005). Insulin-like growth factor-1 (IGF1) genotype predicts breast volume after pregnancy and hormonal contraception and is associated with circulating IGF-1 levels: implications for risk of early-onset breast cancer in young women from hereditary breast cancer families. British Journal of Cancer, 92(5), 857–866. [DOI:10.1038/sj.bjc.6602389]
Jeruss, J. S. (2006). Molecular Basis of Breast Cancer. In Winchester, D. J., Winchester, D. P., Hudis, C. A., & Norton, L. (Eds.). Breast Cancer, 2nd Edition (pp. 83–95). Hamilton: B.C. Decker. [Google Scholar] [Google Books] [WorldCat]
Johnson, M. C., & Cutler, M. L. (2016). Anatomy and Physiology of the Breast. In Jatoi, I., & Rody, A. (Eds.). Management of Breast Diseases (pp. 1–39). Cham: Springer. [DOI:10.1007/978-3-319-46356-8_1]
Kaiser, R. (1993). Gestagen-Östrogen-Kombinationen in der Gynäkologie. Zur Geschichte, Dosierung und Anwendung eines Hormonprinzips. [Gestagen-Oestrogen Combinations in Gynaecology. History, Dosage and Use of a Hormonal Principle.] Geburtshilfe und Frauenheilkunde, 53(7), 503–513. [Google Scholar] [PubMed] [DOI:10.1055/s-2007-1022924]
Kaiser, R., & Leidenberger, F. (1991). Hormonbehandlung bei Benign Mammaerkrankungen: Mammahypoplasie. [Hormonal Treatment in Benign Breast Diseases: Breast Hypoplasia.] In Kaiser, R., & Leidenberger, F. Hormonbehandlung in der Gynäkologischen Praxis, 7. Auflage [Hormone Treatment in Gynecological Practice, 7th Edition] (pp. 138–138). Stuttgart: Georg Thieme Verlag. [Google Books] [OpenLibrary] [WorldCat] [PDF] [Translation]
Kaiser, U., & Ho, K. K. (2015). Pituitary Physiology and Diagnostic Evaluation. In Melmed, S., Polonsky, K. S., Larsen, P. R., Kronenberg, & H. M. (Eds.). Williams Textbook of Endocrinology, 13th Edition (pp. 176–231). Philadelphia: Elsevier. [DOI:10.1016/B978-0-323-29738-7.00008-3] [Google Books]
Kanhai, R. C., Hage, J. J., Asscheman, H., Mulder, W. J., & Hage, J. J. (1999). Augmentation Mammaplasty in Male-to-Female Transsexuals. Plastic and Reconstructive Surgery, 104(2), 542–549. [DOI:10.1097/00006534-199908000-00040]
Kanhai, R. C., Hage, J. J., van Diest, P. J., Bloemena, E., & Mulder, J. W. (2000). Short-Term and Long-Term Histologic Effects of Castration and Estrogen Treatment on Breast Tissue of 14 Male-to-Female Transsexuals in Comparison With Two Chemically Castrated Men. The American Journal of Surgical Pathology, 24(1), 74–80. [DOI:10.1097/00000478-200001000-00009]
Kardelen, A. D., Toksoy, G., Baş, F., Yavaş Abalı, Z., Gençay, G., Poyrazoğlu, Ş., Bundak, R., Altunoğlu, U., Avcı, Ş., Najaflı, A., Uyguner, O., Karaman, B., Başaran, S., & Darendeliler, F. (2018). A Rare Cause of Congenital Adrenal Hyperplasia: Clinical and Genetic Findings and Follow-up Characteristics of Six Patients with 17-Hydroxylase Deficiency Including Two Novel Mutations. Journal of Clinical Research in Pediatric Endocrinology, 10(3), 206–215. [DOI:10.4274/jcrpe.0032]
Kariagina, A., Xie, J., Leipprandt, J. R., & Haslam, S. Z. (2010). Amphiregulin Mediates Estrogen, Progesterone, and EGFR Signaling in the Normal Rat Mammary Gland and in Hormone-Dependent Rat Mammary Cancers. Hormones and Cancer, 1(5), 229–244. [DOI:10.1007/s12672-010-0048-0]
Karp, N. S. (2022). Discussion: The Impact of Combined Oral Contraceptives on Adolescents with Macromastia. Plastic & Reconstructive Surgery, 150(4), 739–740. [DOI:10.1097/prs.0000000000009514]
Kasielska-Trojan, A., Mikołajczyk, M., & Antoszewski, B. (2020). BreastIdea Volume Estimator: A New Tool for Breast Volume Estimation—Presentation and Validation for Women. Plastic & Reconstructive Surgery, 146(6), 744e–748e. [DOI:10.1097/prs.0000000000007373]
Kasielska-Trojan, A., Zawadzki, T., & Antoszewski, B. (2022). Breast Fluctuating Asymmetry in Women with Macromastia/Gigantomastia. International Journal of Environmental Research and Public Health, 19(24), 16895. [DOI:10.3390/ijerph192416895]
Kauli, R., Pertzelan, A., Ben‐Zeev, Z., Lewin, R. P., Kaufman, H., Schally, A. C., Schally, A. V., & Laron, Z. (1984). Treatment of precocious puberty with LHRH analogue in combination with cyproterone acetate—further experience. Clinical Endocrinology, 20(4), 377–387. [DOI:10.1111/j.1365-2265.1984.tb03433.x]
Keller, P. J. (1984). Diagnostik und Therapie wichtiger hormonaler Störungen: Mammahypoplasie. [Diagnosis and Treatment of Important Hormonal Disorders: Mammary Hypoplasia.] In Keller, P. J. Hormonale Störungen in der Gynäkologie: Diagnostik und Behandlung, 3. Auflage [Hormonal Disorders in Gynecology: Diagnosis and Treatment, 3rd Edition] (Kliniktaschenbücher) (pp. 133–134). Berlin/Heidelberg: Springer. [Google Books] [DOI:10.1007/978-3-662-00442-5_3]
Keller, P. J. (1995). Diagnostik und Therapie wichtiger Störungen: Mammahypoplasie. [Diagnosis and Treatment of Important Disorders: Mammary Hypoplasia.] In Keller, P. J. Hormon- und Fertilitätsstörungen in der Gynäkologie, 4. Auflage [Hormonal and Fertility Disorders in Gynecology, 4th Edition] (pp. 145–146). Berlin/Heidelberg: Springer. [Google Books] [DOI:10.1007/978-3-662-12026-2_3]
Kennedy, B. J. (1953). Effects of intensive sex steroid hormone therapy in advanced breast cancer. JAMA, 152(12), 1135–1141. [DOI:10.1001/jama.1953.63690120004013]
Kent, J. C., Mitoulas, L., Cox, D. B., Owens, R. A., & Hartmann, P. E. (1999). Breast Volume and Milk Production During Extended Lactation in Women. Experimental Physiology, 84(2), 435–447. [DOI:10.1111/j.1469-445x.1999.01808.x]
Khoo, S. K., & Mackay, E. V. (1972). Testicular Feminization: The Clinical Features, Endocrine Function and Gonadal Pathology in Six Patients. Australian and New Zealand Journal of Obstetrics and Gynaecology, 12(1), 1–13. [DOI:10.1111/j.1479-828x.1972.tb00721.x]
Klein, R., Aichinger, H., Dierker, J., Jansen, J. T., Joite-Barfuß, S., Säbel, M., Schulz-Wendtland, R., & Zoetelief, J. (1997). Determination of average glandular dose with modern mammography units for two large groups of patients. Physics in Medicine and Biology, 42(4), 651–671. [DOI:10.1088/0031-9155/42/4/004]
Kleinberg, D. L. (2006). Endocrinology of lactation. In DeGroot, L. J., & Jameson, J. L. (Eds). Endocrinology, 5th Edition (pp. 3461–3473). Philadelphia: Elsevier Saunders. [Google Scholar] [Google Books] [OpenLibrary] [WorldCat] [Archive.org]
Kleinberg, D. L., & Barcellos-Hoff, M. H. (2011). The Pivotal Role of Insulin-Like Growth Factor I in Normal Mammary Development. Endocrinology and Metabolism Clinics of North America, 40(3), 461–471. [DOI:10.1016/j.ecl.2011.06.001]
Kleinberg, D. L., & Ruan, W. (2008). IGF-I, GH, and Sex Steroid Effects in Normal Mammary Gland Development. Journal of Mammary Gland Biology and Neoplasia, 13(4), 353–360. [DOI:10.1007/s10911-008-9103-7]
Kleinberg, D. L., Wood, T. L., Furth, P. A., & Lee, A. V. (2008). Growth Hormone and Insulin-Like Growth Factor-I in the Transition from Normal Mammary Development to Preneoplastic Mammary Lesions. Endocrine Reviews, 30(1), 51–74. [DOI:10.1210/er.2008-0022]
Kühnel, W. (2000). IMMULITE® and IMMULITE® 2000 Reference Range Compendium, First English Edition. Los Angeles, California: Diagnostic Products Corporation. [Google Scholar] [URL] [PDF 1] [PDF 2]
Kustin, J., & Rebar, R. W. (1987). Menstrual Disorders in the Adolescent Age Group. Primary Care: Clinics in Office Practice, 14(1), 139–166. [DOI:10.1016/s0095-4543(21)01004-6]
Kutten, F., Malet, C., & Leygue, E. (1994). Antiestrogen action of progestogens in human breast cells. In Berg, G., & Hammar, M. (Eds.). The Modern Management of the Menopause: A Perspective for the 21st Century [The Proceedings of the VII International Congress on the Menopause, Stockholm, Sweden 1993] (pp. 419–433). Canforth: Parthenon. [Google Scholar] [Google Books] [OpenLibrary] [WorldCat] [Archive.org] [PDF]
Ladjouze, A., & Donaldson, M. (2019). Primary gonadal failure. Best Practice & Research Clinical Endocrinology & Metabolism, 33(3), 101295. [DOI:10.1016/j.beem.2019.101295]
Laessle, R. G., Tuschi, R. J., Schweiger, U., & Pirke, K. M. (1990). Mood changes and physical complaints during the normal menstrual cycle in healthy young women. Psychoneuroendocrinology, 15(2), 131–138. [DOI:10.1016/0306-4530(90)90021-z]
LaMarca, H. L., & Rosen, J. M. (2007). Estrogen regulation of mammary gland development and breast cancer: amphiregulin takes center stage. Breast Cancer Research, 9(4), 304. [DOI:10.1186/bcr1740]
Laron, Z., & Kauli, R. (2000). Experience with Cyproterone Acetate in the Treatment of Precocious Puberty. Journal of Pediatric Endocrinology and Metabolism, 13(Suppl 1), 805–810. [DOI:10.1515/jpem.2000.13.s1.805]
Laufer, M. R., Goldstein, D. P., & Hendren, W. H. (2005). Structural Abnormalities of the Female Reproductive Tract. In Emans, J. E., Laufer, M. R., & Goldstein, D. P. (Eds.). Pediatric and Adolescent Gynecology, 5th Edition (pp. 334–416). Philadelphia: Lippincott Williams and Wilkins. [Google Scholar] [Google Books] [OpenLibrary] [WorldCat] [Archive.org]
Lauritzen, C. (1980 October 27). Hormonkur Kann Hypoplastischer Mamma Aufhelfen. [Hormone Therapy Can Help Hypoplastic Breasts.] Selecta: Medizin aktuell; das Magazin für ärztliche Fortbildung [Selecta: Medicine Currently; the Magazine for Medical Training], 22(43), 3798–3801. Planegg: Selecta-Verlag. [ISSN:0582-4877] [WorldCat] [PDF] [Translation]
Lauritzen, C. (1982). Treatment of mammary- and uterus hypoplasia by estrogen-progestagen pseudopregnancy. In Richter, K., Huber, A., Terruhn, V. (Eds.) 1. Europäisches Symposium für Kinder- und Jugendgynäkologie. München 19.-21.3.1981, Band 2 [First European Symposium on Pediatric and Adolescent Gynaecology. München, March 19–21, 1981, Volume 2] (pp. 487–489). Friedrichsdorf/Taunus: Milupa-Aktiengesellschaft, Wissenschaftliche Abteilung. [Google Scholar] [PDF]
Lauritzen, C. (1989). Hormonelle Substitutionstherapie zur Brustvergrößerung. [Hormonal Substitution Therapy for Breast Enlargement.] In Beller, F. K. & Seitzer, D. (Eds.). 7. Siebte Wissenschaftliche Tagung der Deutschen Gesellschaft für Senologie, Münster, 25. - 27. September 1987: Ausgewählte Referate [7th Scientific Conference of the German Society for Senology, Münster, [Germany,] September 25–27, 1987: Selected Papers] (pp. 39–41). Mülheim, Germany: H.U.F. Verlag. [Google Scholar] [WorldCat 1] [WorldCat 2] [WorldCat 3] [Cited By 1] [Cited By 2] [Cited By 3] [PDF] [Translation]
Lawrence, R. A., & Lawrence, R. M. (2015). Physiology of Lactation. In Lawrence, R. A., & Lawrence, R. M. Breastfeeding: A Guide for the Medical Profession, 8th Edition (pp. 56–90). Philadelphia: Elsevier. [Google Scholar] [Google Books] [OpenLibrary] [WorldCat] [Archive.org]
Lee, H. J., & Ormandy, C. J. (2012). Interplay between progesterone and prolactin in mammary development and implications for breast cancer. Molecular and Cellular Endocrinology, 357(1–2), 101–107. [DOI:10.1016/j.mce.2011.09.020]
Lee, P. A. (2001). Physiology of Puberty. In Becker, K. L., Bilezikian, J. P., Bremner, W. J., Hung, W., Kahn, C. R., Loriaux, D. L., Nylén, E. S., Rebar, R. W., Robertson, G. L., Snider, R. H., Wartofsky, L. (Eds.). Principles and Practice of Endocrinology and Metabolism, 3rd Edition (pp. 885–893). Philadelphia: Lippincott Williams & Wilkins. [Google Scholar] [Google Books] [OpenLibrary] [WorldCat] [Archive.org]
Lee, S. W., Kwak, D. S., Jung, I. S., Kwak, J. H., Park, J. H., Hong, S. M., Lee, C. B., Park, Y. S., Kim, D. S., Choi, W. H., & Ahn, Y. H. (2015). Partial Androgen Insensitivity Syndrome Presenting with Gynecomastia. Endocrinology and Metabolism, 30(2), 226–230. [DOI:10.3803/enm.2015.30.2.226]
Lejour, M. (1994). Vertical Mammaplasty and Liposuction of the Breast. Plastic and Reconstructive Surgery, 94(1), 100–114. [DOI:10.1097/00006534-199407000-00010]
Lejour, M. (1997). Evaluation of Fat in Breast Tissue Removed by Vertical Mammaplasty. Plastic and Reconstructive Surgery, 99(2), 386–393. [DOI:10.1097/00006534-199702000-00012]
Lemarchand-Béraud, T., Zufferey, M., Reymond, M., & Rey, I. (1982). Maturation of the Hypothalamo-Pituitary-Ovarian Axis in Adolescent Girls. The Journal of Clinical Endocrinology & Metabolism, 54(2), 241–246. [DOI:10.1210/jcem-54-2-241]
Lewin, R. (2016). Breast Hypertrophy and Outcome of Breast Reduction Surgery. (Doctoral thesis, University of Gothenburg. Sahlgrenska Academy.) [Google Scholar] [URL]
Lim, L. Y., Ho, P. J., Liu, J., Chay, W. Y., Tan, M., Hartman, M., & Li, J. (2018). Determinants of breast size in Asian women. Scientific Reports, 8(1), 1201. [DOI:10.1038/s41598-018-19437-4]
Lloyd, C. W., & Leathem, J. H. (1964). Growth and development of the breast and lactation. In Lloyd, C. W. (Ed.). Human Reproduction and Sexual Behavior (pp. 117–134). Philadelphia: Lea & Febiger. [Google Scholar] [Google Books] [OpenLibrary] [WorldCat]
Lopez, X., Panton, J., Nagarkar, P., Preston, S., Abramowitz, J., & Amirlak, B. (2023). Initial Assessment of VECTRA Three-Dimensional Imaging to Accurately Simulate Breast Volume Changes in Transfeminine Patients: A Mannequin Study. Aesthetic Surgery Journal Open Forum, 5, online ahead of print. [DOI:10.1093/asjof/ojad015]
Lorincz, A. M., & Sukumar, S. (2006). Molecular links between obesity and breast cancer. Endocrine-Related Cancer, 13(2), 279–292. [DOI:10.1677/erc.1.00729]
Lucien, J. N., Ortega, M. T., Calvert, M. E., Smith, C., White, X., Rogers, H., Mosley, B., Agrawal, R., Drude, A., McGee, C., George, M., Brown, A., Downey, K., Wild, C., Njunge, A., Kuzmiak, C. M., Zava, D., Zava, T., Pollard, J., Francis, J., Beery, B. L., Harlin, M., Gonzalez, G. R., & Shaw, N. D. (2022). The Launch of A Girl’s First Period Study: Demystifying Reproductive Hormone Profiles in Adolescent Girls. Journal of Pediatric and Adolescent Gynecology, 35(4), 420–425. [DOI:10.1016/j.jpag.2021.12.018]
Lydon, J. P., DeMayo, F. J., Funk, C. R., Mani, S. K., Hughes, A. R., Montgomery, C. A., Shyamala, G., Conneely, O. M., & O’Malley, B. W. (1995). Mice lacking progesterone receptor exhibit pleiotropic reproductive abnormalities. Genes & Development, 9(18), 2266–2278. [DOI:10.1101/gad.9.18.2266]
Lyon, A. J., De Bruyn, R., & Grant, D. B. (1985). Isosexual Precocious Puberty in Girls. Acta Paediatrica, 74(6), 950–955. [DOI:10.1111/j.1651-2227.1985.tb10063.x]
Lyons, W. R. (1958). Hormonal synergism in mammary growth. Proceedings of the Royal Society of London. Series B - Biological Sciences, 149(936), 303–325. [DOI:10.1098/rspb.1958.0071]
Lyons, W. R., & McGinty, D. A. (1941). Effects of estrone and progesterone on male rabbit mammary glands. I. Varying doses of progesterone. Proceedings of the Society for Experimental Biology and Medicine, 48(1), 83–86. [DOI:10.3181/00379727-48-13227]
Lyons, W. R., Li, C. H., & Johnson, R. E. (1958). The Hormonal Control of Mammary Growth and Lactation. In Pincus, G. (Ed.). Recent Progress in Hormone Research, Volume 14 [Proceedings of the Laurentian Hormone Conference 1957, Held at Mont Tremblant, Quebec] (pp. 219–254). New York/London: Academic Press. [Google Scholar] [Google Books] [PubMed] [OpenLibrary] [WorldCat] [PDF]
MacBryde, C. M. (1939). The Production of Breast Growth in the Human Female. Journal of the American Medical Association, 112(11), 1045–1049. [DOI:10.1001/jama.1939.02800110025006]
Malet, C., Gompel, A., Yaneva, H., Cren, H., Fidji, N., Mowszowicz, I., Kuttenn, F., & Mauvais-Jarvis, P. (1991). Estradiol and Progesterone Receptors in Cultured Normal Human Breast Epithelial Cells and Fibroblasts: Immunocytochemical Studies. The Journal of Clinical Endocrinology & Metabolism, 73(1), 8–17. [DOI:10.1210/jcem-73-1-8]
Malini, S., Smith, E. O., & Goldzieher, J. W. (1985). Measurement of breast volume by ultrasound during normal menstrual cycles and with oral contraceptive use. Obstetrics and Gynecology, 66(4), 538–541. [Google Scholar] [PubMed] [URL] [PDF]
Marshall, W. A. (1978). Puberty. In Falkner, F., & Tanner, J. M. (Eds.). Human Growth: Postnatal Growth (pp. 141–181). Boston: Springer US. [DOI:10.1007/978-1-4684-2622-9_6]
Marshall, W. A., & Tanner, J. M. (1969). Variations in pattern of pubertal changes in girls. Archives of Disease in Childhood, 44(235), 291–303. [DOI:10.1136/adc.44.235.291]
Mauvais-Jarvis, P., Kuttenn, F., & Gompel, A. (1986). Antiestrogen action of progesterone in breast tissue. Breast Cancer Research and Treatment, 8(3), 179–188. [DOI:10.1007/bf01807330]
Mauvais-Jarvis, P., Kuttenn, F., & Gompel, A. (1986). Estradiol/Progesterone Interaction in Normal and Pathologic Breast Cells. Annals of the New York Academy of Sciences, 464(1), 152–167. [DOI:10.1111/j.1749-6632.1986.tb16002.x]
Mauvais-Jarvis, P., Kuttenn, F., & Gompel, A. (1987). Antiestrogen Action of Progesterone in Breast Tissue. Hormone Research, 28(2–4), 212–218. [DOI:10.1159/000180946]
Mauvais-Jarvis, P., Kuttenn, F., Gompel, A., & Benotmane, A. (1987). Action anti-estrogène de la progestérone dans le sein. [Antiestrogen action of progesterone in the breast]. Pathologie-Biologie, 35(7), 1081–1086. [Google Scholar 1] [Google Scholar 2] [PubMed]
Mauvais-Jarvis, P., Sitruk-Ware, R., & Kuttenn, F. (1981). Benign Breast Disease. In McGuire, W. L. (Ed.). Breast Cancer 4: Advances in Research and Treatment (pp. 51–94). Boston: Springer US. [DOI:10.1007/978-1-4615-6571-0_3]
McArthur, J. W. (1966). The Reproductive Endocrinology of Adolescence. In Heald, F. P. (Ed.). Adolescent Gynecology (pp. 9–20). Baltimore: Williams & Wilkins. [Google Scholar] [Google Books] [OpenLibrary] [WorldCat]
McBryan, J., Howlin, J., Napoletano, S., & Martin, F. (2008). Amphiregulin: Role in Mammary Gland Development and Breast Cancer. Journal of Mammary Gland Biology and Neoplasia, 13(2), 159–169. [DOI:10.1007/s10911-008-9075-7]
McDonough, P. G., Spicer, D. V., Ursin, G., & Pike, M. C. (1996). Progesterone Concentrations—Physiologic or Pharmacologic? Fertility and Sterility, 65(5), 1077–1078. [DOI:10.1016/s0015-0282(16)58295-8]
McMillan, M. (1966). Five cases of testicular feminisation including one with a teratoma of the testis. The Journal of Pathology and Bacteriology, 91(2), 417–427. [DOI:10.1002/path.1700910216]
McNally, S., & Stein, T. (2016). Overview of Mammary Gland Development: A Comparison of Mouse and Human. In Martin, F., Stein, T., & Howlin, J. (Eds.). Mammary Gland Development (Methods in Molecular Biology, Volume 1501) (pp. 1–17). New York: Springer New York. [DOI:10.1007/978-1-4939-6475-8_1]
McPhaul, M. J. (2002). Androgen receptor mutations and androgen insensitivity. Molecular and Cellular Endocrinology, 198(1–2), 61–67. [DOI:10.1016/s0303-7207(02)00369-6]
Mesiano, S. (2019). Endocrinology of Human Pregnancy and Fetal-Placental Neuroendocrine Development. In Strauss, J. F., & Barbieri, R. L. (Eds.). Yen and Jaffe’s Reproductive Endocrinology: Physiology, Pathophysiology, and Clinical Management, 8th Edition (pp. 256–284.e9). Philadelphia: Elsevier. [Google Books] [DOI:10.1016/b978-0-323-47912-7.00011-1]
Meyer, G., Mayer, M., Mondorf, A., Flügel, A. K., Herrmann, E., & Bojunga, J. (2020). Safety and rapid efficacy of guideline-based gender-affirming hormone therapy: an analysis of 388 individuals diagnosed with gender dysphoria. European Journal of Endocrinology, 182(2), 149–156. [DOI:10.1530/eje-19-0463]
Meyer, W. J., Finkelstein, J. W., Stuart, C. A., Webb, A., Smith, E. R., Payer, A. F., & Walker, P. A. (1981). Physical and hormonal evaluation of transsexual patients during hormonal therapy. Archives of Sexual Behavior, 10(4), 347–356. [DOI:10.1007/bf01565538]
Meyer, W. J., Webb, A., Stuart, C. A., Finkelstein, J. W., Lawrence, B., & Walker, P. A. (1986). Physical and hormonal evaluation of transsexual patients: A longitudinal study. Archives of Sexual Behavior, 15(2), 121–138. [DOI:10.1007/bf01542220]
Mikołajczyk, M., Kasielska-Trojan, A., & Antoszewski, B. (2019). A New Tool for Breast Anthropometric Measurements: Presentation and Validation for Women and Men. Aesthetic Plastic Surgery, 43(5), 1160–1170. [DOI:10.1007/s00266-019-01467-6]
Milionis, C., Ilias, I., & Koukkou, E. (2022). Progesterone in gender-affirming therapy of trans women. World Journal of Biological Chemistry, 13(3), 66–71. [DOI:10.4331/wjbc.v13.i3.66]
Milligan, D., Drife, J. O., & Short, R. V. (1975). Changes in breast volume during normal menstrual cycle and after oral contraceptives. BMJ, 4(5995), 494–496. [DOI:10.1136/bmj.4.5995.494]
Morris, J. M. (1953). The syndrome of testicular feminization in male pseudohermaphrodites. American Journal of Obstetrics and Gynecology, 65(6), 1192–1211. [DOI:10.1016/0002-9378(53)90359-7]
Morris, J. M., & Mahesh, V. B. (1963). Further observations on the syndrome, “testicular feminization”. American Journal of Obstetrics and Gynecology, 87(6), 731–748. [Google Scholar 1] [Google Scholar 2] [PubMed] [PDF]
Muallem, M. M., & Rubeiz, N. G. (2006). Physiological and biological skin changes in pregnancy. Clinics in Dermatology, 24(2), 80–83. [DOI:10.1016/j.clindermatol.2005.10.002]
Müller, C. (1953). Zur Hormonalen Kosmetik der Weiblichen Brust: Wirkung und Nebenwirkung Östrogenhaltiger Kosmetischer Präparate. [Hormonal Cosmetics of the Female Breast: Effects and Side Effects of Estrogen-Containing Cosmetic Preparations.] Schweizerische Medizinische Wochenschrift [Swiss Medical Weekly], 83(4), 81–84. [Google Scholar 1] [Google Scholar 2] [PubMed] [PDF] [Translation]
Muzaffar, F., Hussain, I., & Haroon, T. S. (1998). Physiologic skin changes during pregnancy: a study of 140 cases. International Journal of Dermatology, 37(6), 429–431. [DOI:10.1046/j.1365-4362.1998.00281.x]
Naik, M., Diwakar, R. K., Patre, S., & Singh, S. (2015). Gigantomastia: A Rare Complication In Pregnancy. Journal of Medical Science and Clinical Research, 3(7), 6873–6876. [Google Scholar] [URL] [PDF]
Naseem, H., Lokman, M., & Fitzgerald, C. (2021). Management of congenital hypogonadotropic hypogonadism in females. Human Fertility, 26(3), 622–631. [DOI:10.1080/14647273.2021.1998929]
Nelson, W. O. (1936). Endocrine Control of the Mammary Gland. Physiological Reviews, 16(3), 488–526. [DOI:10.1152/physrev.1936.16.3.488]
Nolan, B. J., Frydman, A. S., Leemaqz, S. Y., Carroll, M., Grossmann, M., Zajac, J. D., & Cheung, A. S. (2022). Effects of low-dose oral micronised progesterone on sleep, psychological distress, and breast development in transgender individuals undergoing feminising hormone therapy: a prospective controlled study. Endocrine Connections, 11(5), e220170. [DOI:10.1530/EC-22-0170]
Nolan, B. J., Frydman, A. S., Leemaqz, S. Y., Carroll, M., Grossmann, M., Zajac, J. D., & Cheung, A. S. (2022). Effects Of Low-dose Oral Micronised Progesterone On Sleep, Psychological Distress And Breast Development In Transgender Individuals Undergoing Feminising Hormone Therapy: A Prospective Controlled Study. Journal of the Endocrine Society, 6(Suppl 1), A653–A654 (abstract no. LBODP089). [DOI:10.1210/jendso/bvac150.1351]
Nussbaum, R., & Benedetto, A. V. (2006). Cosmetic aspects of pregnancy. Clinics in Dermatology, 24(2), 133–141. [DOI:10.1016/j.clindermatol.2005.10.007]
Nuzzi, L. C., Pramanick, T., Massey, G. G., Walsh, L. R., McNamara, C. T., Firriolo, J. M., DiVasta, A. D., & Labow, B. I. (2021). The Impact of Progestin-only Contraception on Adolescents with Macromastia. Plastic and Reconstructive Surgery - Global Open, 9(2), e3421. [DOI:10.1097/gox.0000000000003421]
Nuzzi, L. C., Pramanick, T., Massey, G. G., Walsh, L. R., McNamara, C. T., Firriolo, J. M., DiVasta, A. D., & Labow, B. I. (2022). The Impact of Combined Oral Contraceptives on Adolescents with Macromastia. Plastic and Reconstructive Surgery, 150(4), 731–738. [DOI:10.1097/prs.0000000000009513]
Oakes, M. B., Eyvazzadeh, A. D., Quint, E., & Smith, Y. R. (2008). Complete Androgen Insensitivity Syndrome—A Review. Journal of Pediatric and Adolescent Gynecology, 21(6), 305–310. [DOI:10.1016/j.jpag.2007.09.006]
Obr, A. E., & Edwards, D. P. (2012). The biology of progesterone receptor in the normal mammary gland and in breast cancer. Molecular and Cellular Endocrinology, 357(1–2), 4–17. [DOI:10.1016/j.mce.2011.10.030]
Olanrewaju, F., Onayemi, O., Olasode, O., Adeyemi, A., Oninla, A., Oripelaye, M., Ezejiofor, O., & Oke, O. (2017). Prevalence and Pattern of Pigmentary Changes among Primigravidae Attending a Tertiary Health Facility in South-Western Nigeria. British Journal of Medicine and Medical Research, 21(5), 1–9. [DOI:10.9734/bjmmr/2017/33382]
Orentreich, N., & Durr, N. P. (1974). Mammogenesis in Transsexuals. Journal of Investigative Dermatology, 63(1), 142–146. [DOI:10.1111/1523-1747.ep12678272]
Pandya, S., & Moore, R. G. (2011). Breast Development and Anatomy. Clinical Obstetrics & Gynecology, 54(1), 91–95. [DOI:10.1097/grf.0b013e318207ffe9]
Park, I. Y., Kim, M. R., Jo, H. H., Lee, M. K., & Kim, M. J. (2014). Association of the Nipple-Areola Complexes with Age, Parity, and Breastfeeding in Korean Premenopausal Women. Journal of Human Lactation, 30(4), 474–479. [DOI:10.1177/0890334414549049]
Pasqualini, J. R. (2007). Progestins and breast cancer. Gynecological Endocrinology, 23(Suppl 1), 32–41. [DOI:10.1080/09513590701585003]
Pasqualini, J. R. (2009). Breast cancer and steroid metabolizing enzymes: The role of progestogens. Maturitas, 65(Suppl 1), S17–S21. [DOI:10.1016/j.maturitas.2009.11.006]
Pasqualini, J. R., & Kincl, F. A. (1985). Hormone Production and Concentrations During Pregnancy in Humans and in Other Mammalian Species. In Pasqualini, J. R., & Kincl, F. A. Hormones and the Fetus, Volume I: Production, Concentration and Metabolism During Pregnancy (pp. 173–334). Oxford: Pergamon Press. [DOI:10.1016/b978-0-08-019708-1.50007-6]
Patel, H., Arruarana, V., Yao, L., Cui, X., & Ray, E. (2020). Effects of hormones and hormone therapy on breast tissue in transgender patients: a concise review. Endocrine, 68(1), 6–15. [DOI:10.1007/s12020-020-02197-5]
Patel, K. T., Adeel, S., Rodrigues Miragaya, J., & Tangpricha, V. (2022). Progestogen Use in Gender-Affirming Hormone Therapy: A Systematic Review. Endocrine Practice, 28(12), 1244–1252. [DOI:10.1016/j.eprac.2022.08.012]
Patterson, M. N., McPhaul, M. J., & Hughes, I. A. (1994). Androgen insensitivity syndrome. Baillière’s Clinical Endocrinology and Metabolism, 8(2), 379–404. [DOI:10.1016/s0950-351x(05)80258-7]
Pawłowski, B., & Żelaźniewicz, A. (2021). The evolution of perennially enlarged breasts in women: a critical review and a novel hypothesis. Biological Reviews, 96(6), 2794–2809. [DOI:10.1111/brv.12778]
Perez-Palacios, G., & Jaffe, R. B. (1972). The Syndrome of Testicular Feminization. Pediatric Clinics of North America, 19(3), 653–667. [DOI:10.1016/s0031-3955(16)32744-4]
Petrakis, N. (1978). Recurrent extreme breast involution following pregnancy and susceptibility to breast cancer: A hypothesis. Medical Hypotheses, 4(3), 268–272. [DOI:10.1016/0306-9877(78)90006-3]
Pfeiffer, C. A. (1943). Endocrinology of Reproduction. Annual Review of Physiology, 5(1), 413–452. [DOI:10.1146/annurev.ph.05.030143.002213]
Pipkin, F. B. (2019). Physiological Changes in Pregnancy. In Symonds, I. M., & Arulkumaran, S. (Eds.). Essential Obstetrics and Gynaecology, 6th Edition (pp. 22–40). Edinburgh: Elsevier. [Google Books] [OpenLibrary] [WorldCat]
Plu-Bureau, G., Touraine, P., & Mauvais-Jarvis, P. (1999). Interactions Between Estradiol and Progesterone in Normal Breast: Implications for Mammary Carcinogenesis. In Manni, A. (Ed.). Endocrinology of Breast Cancer (Contemporary Endocrinology, Volume 11) (pp. 21–37). Totowa, New Jersey: Humana Press. [DOI:10.1007/978-1-59259-699-7_2] [OpenLibrary] [Archive.org]
Pocock, G., Richards, C. D., & Richards, D. A. (2013). Fertilization, Pregnancy, and Lactation. In Pocock, G., Richards, C. D., & Richards, D. A. Human Physiology, 4th Edition (pp. 655–752). Oxford: Oxford University Press. [Google Scholar] [Google Books]
Polani, P. E. (1970). Hormonal and clinical aspects of hermaphroditism and the testicular feminizing syndrome in man. Philosophical Transactions of the Royal Society of London. B, Biological Sciences, 259(828), 187–206. [DOI:10.1098/rstb.1970.0058]
Price, S., McManus, J., & Barrett, J. (2019). The transgender population: improving awareness for gynaecologists and their role in the provision of care. The Obstetrician & Gynaecologist, 21(1), 11–20. [DOI:10.1111/tog.12521]
Prior, J. C. (2011). Progesterone for Symptomatic Perimenopause Treatment - Progesterone politics, physiology and potential for perimenopause. Facts, Views & Vision in ObGyn, 3(2), 109–120. [PubMed] [PubMed Central] [PDF]
Prior, J. C. (2019). Progesterone Is Important for Transgender Women’s Therapy—Applying Evidence for the Benefits of Progesterone in Ciswomen. The Journal of Clinical Endocrinology & Metabolism, 104(4), 1181–1186. [DOI:10.1210/jc.2018-01777]
Prior, J. C. (2019). Response to Letter to the Editor: “Progesterone Is Important for Transgender Women’s Therapy—Applying Evidence for the Benefits of Progesterone in Ciswomen”. The Journal of Clinical Endocrinology & Metabolism, 104(8), 3129–3130. [DOI:10.1210/jc.2019-00524]
Prior, J. C. (2020). Women’s Reproductive System as Balanced Estradiol and Progesterone Actions—A revolutionary, paradigm-shifting concept in women’s health. Drug Discovery Today: Disease Models, 32(Part B), 31–40. [DOI:10.1016/j.ddmod.2020.11.005]
Prior, J. C., Vigna, Y. M., & Watson, D. (1989). Spironolactone with physiological female steroids for presurgical therapy of male-to-female transsexualism. Archives of Sexual Behavior, 18(1), 49–57. [DOI:10.1007/bf01579291]
Prior, J. C., Vigna, Y. M., Watson, D., Diewold, P., & Robinow, O. (1986). Spironolactone in the presurgical therapy of male to female transsexuals: Philosophy and experience of the Vancouver Gender Dysphoria Clinic. Journal of Sex Information & Education Council of Canada, 1(1), 1–7. [Google Scholar] [PDF]
Quigley, C. A. (1998). The androgen receptor: Physiology and pathophysiology. In Nieschlag, E., & Behre, H. M. (Eds.). Testosterone: Action · Deficiency · Substitution, 2nd Edition (pp. 33–106). Berlin/Heidelberg: Springer. [DOI:10.1007/978-3-642-72185-4_2]
Quigley, C. A., Bellis, A. D., Marschke, K. B., El-Awady, M. K., Wilson, E. M., & French, F. S. (1995). Androgen Receptor Defects: Historical, Clinical, and Molecular Perspectives. Endocrine Reviews, 16(3), 271–321. [DOI:10.1210/edrv-16-3-271]
Radisky, D. C., & Hartmann, L. C. (2009). Mammary Involution and Breast Cancer Risk: Transgenic Models and Clinical Studies. Journal of Mammary Gland Biology and Neoplasia, 14(2), 181–191. [DOI:10.1007/s10911-009-9123-y]
Ramos, L., Chávez, B., Mares, L., Valdés, E., & Vilchis, F. (2018). Mutational analysis of the androgen receptor (NR3C4) gene in patients with 46,XY DSD. Gene, 641, 86–93. [DOI:10.1016/j.gene.2017.10.038]
Ramsay, D. T., Kent, J. C., Hartmann, R. A., & Hartmann, P. E. (2005). Anatomy of the lactating human breast redefined with ultrasound imaging. Journal of Anatomy, 206(6), 525–534. [DOI:10.1111/j.1469-7580.2005.00417.x]
Randolph, J. F. (2018). Gender-Affirming Hormone Therapy for Transgender Females. Clinical Obstetrics & Gynecology, 61(4), 705–721. [DOI:10.1097/grf.0000000000000396]
Rauh, C., Faschingbauer, F., Haeberle, L., Jud, S. M., Heusinger, K., Fasching, P. A., Goecke, T. W., Rajakaruna, N., Voigt, F., Bani, M. R., Lux, M. P., Renner, S. P., Loehberg, C. R., Hartmann, A., Schulz-Wendtland, R., Beckmann, M. W., & Bayer, C. M. (2013). Factors influencing breast changes after pregnancy. European Journal of Cancer Prevention, 22(3), 259–261. [DOI:10.1097/cej.0b013e328359cb81]
Rebar, R. W. (1988). The Ovaries. In Wyngaarden, J. B., & Smith, L. H. (Eds.). Cecil Textbook of Medicine, 18th Edition (pp. 1425–1446). Philadelphia: W. B. Saunders. [Google Books] [OpenLibrary] [WorldCat] [Archive.org]
Rebar, R. W. (1990). Disorders of Menstruation, Ovulation, and Sexual Response. In Becker, K. L., Bilezikian, J. P., Bremner, W. J., Hung, W., Kahn, C. R., Loriaux, D. L., Rebar, R. W., Robertson, G. L., & Wartofsky, L. (Eds.). Principles and Practice of Endocrinology and Metabolism, 1st Edition (pp. 798–814). Philadelphia: Lippincott. [Google Scholar—3rd/2001 Edition] [Google Books—3rd/2001 Edition] [OpenLibrary] [WorldCat] [Archive.org]
Rebar, R. W. (1993). Normal and Abnormal Sexual Differentiation and Pubertal Development. In Moore, T. R., Reiter, R. C., Rebar, R. W., & Baker, W. (Eds.). Gynecology & Obstetrics: A Longitudinal Approach (pp. 97–133). New York: Churchill Livingstone. [Google Books] [OpenLibrary] [WorldCat] [Archive.org]
Rebar, R. W. (1996). Puberty. In Berek, J. S., Adashi, E. Y., & Hillard, P. A. (Eds.). Novak’s Gynecology, 12th Edition (pp. 771–807). Baltimore: Williams & Wilkins. [Google Scholar] [Google Books] [OpenLibrary] [WorldCat] [Archive.org]
Reindollar, R. H., & McDonough, P. G. (1985). The Child with Ambiguous Genitalia. In Lavery, J. P., & Sanfilippo, J. S. (Eds.). Pediatric and Adolescent Obstetrics and Gynecology, 1st Edition (Clinical Perspective in Obstetrics and Gynecology) (pp. 38–60). New York: Springer. [DOI:10.1007/978-1-4612-5064-7_5]
Reisman, T., Goldstein, Z., & Safer, J. D. (2019). A Review of Breast Development in Cisgender Women and Implications for Transgender Women. Endocrine Practice, 25(12), 1338–1345. [DOI:10.4158/ep-2019-0183]
Richards, C., & Barrett, J. (2020). Physical Treatments for Trans People and Their Interactions with Psychiatric Treatments. In Richards, C., & Barrett, J. Trans and Non-binary Gender Healthcare for Psychiatrists, Psychologists, and Other Health Professionals (pp. 31–44). Cambridge: Cambridge University Press. [DOI:10.1017/9781108628419.003]
Richert, M. M., Schwertfeger, K. L., Ryder, J. W., & Anderson, S. M. (2000). An Atlas of Mouse Mammary Gland Development. Journal of Mammary Gland Biology and Neoplasia, 5(2), 227–241. [DOI:10.1023/a:1026499523505]
Rix, J., Mills, C., Ross, E., Allen, S., Lai, A., & Wakefield-Scurr, J. (2023). Breast volume fluctuations are associated with oestradiol and progesterone changes across the menstrual cycle. Research Square, preprint. [Google Scholar] [DOI:10.21203/rs.3.rs-3753080/v1] [PDF]
Rodari, G. (2022). Pubertal induction in girls with hypogonadism: estrogen replacement therapy outcomes and optimization of progesterone introduction. (Doctoral thesis, Università degli Studi di Milano.) [URL]
Rodari, G., Federici, S., Cattoni, A., Todisco, T., Ubertini, G., Giacchetti, F., Profka, E., Dall’Antonia, A., Cangiano, B., Arosio, M., Bonomi, M., Cappa, M., & Giavoli, C. (2022). Pubertal induction in girls with hypogonadism: insight into estrogen replacement therapy outcomes and optimization of progesterone introduction. Endocrine Abstracts, 81 [24th European Congress of Endocrinology 2022 21–24 May 2022, Milan, Italy], 107–107 (abstract no. RC12.7). [DOI:10.1530/endoabs.81.rc12.7] [PDF]
Rodari, G., Federici, S., Todisco, T., Ubertini, G., Cattoni, A., Pagano, M., Giacchetti, F., Profka, E., Citterio, V., Messetti, D., Collini, V., Soranna, D., Carbone, E., Arosio, M., Mantovani, G., Persani, L., Cappa, M., Bonomi, M., & Giavoli, C. (2023). Towards an individualized management of pubertal induction in girls with hypogonadism: insight into the best replacement outcomes from a large multicentre registry. European Journal of Endocrinology, 188(6), 467–476. [DOI:10.1093/ejendo/lvad056]
Rohn, R. D. (1989). Nipple (papilla) development in girls: III. Journal of Adolescent Health Care, 10(1), 39–40. [DOI:10.1016/0197-0070(89)90045-4]
Rosenfield, R. L. (2013). Adolescent Anovulation: Maturational Mechanisms and Implications. The Journal of Clinical Endocrinology & Metabolism, 98(9), 3572–3583. [DOI:10.1210/jc.2013-1770]
Rosenfield, R. L., Cooke, D. W., & Radovick, S. (2021). Puberty in the Female and Its Disorders. In Sperling, M. A., Majzoub, J. A., Menon, R. K., & Stratakis, C. A. (Eds.). Sperling Pediatric Endocrinology, 5th Edition (pp. 528–626). Philadelphia: Elsevier. [DOI:10.1016/B978-0-323-62520-3.00016-6]
Rothman, M. S., & Iwamoto, S. J. (2022). Feminizing Gender-Affirming Hormone Therapy: Special Considerations for Older Adults. In Davis, T. F. (Ed.). A Case-Based Guide to Clinical Endocrinology (pp. 513–523). Cham: Springer. [DOI:10.1007/978-3-030-84367-0_58]
Ruan, W., Monaco, M. E., & Kleinberg, D. L. (2005). Progesterone Stimulates Mammary Gland Ductal Morphogenesis by Synergizing with and Enhancing Insulin-Like Growth Factor-I Action. Endocrinology, 146(3), 1170–1178. [DOI:10.1210/en.2004-1360]
Rutgers, J. L., & Scully, R. E. (1991). The Androgen Insensitivity Syndrome (Testicular Feminization). International Journal of Gynecological Pathology, 10(2), 126–144. [DOI:10.1097/00004347-199104000-00002]
Ryan, R. F., & Pernoll, M. L. (1985). Virginal Hypertrophy. Plastic and Reconstructive Surgery, 75(5), 737–742. [DOI:10.1097/00006534-198505000-00024]
Saito, R., Yamamoto, Y., Goto, M., Araki, S., Kubo, K., Kawagoe, R., Kawada, Y., Kusuhara, K., Igarashi, M., & Fukami, M. (2014). Tamoxifen Treatment for Pubertal Gynecomastia in Two Siblings with Partial Androgen Insensitivity Syndrome. Hormone Research in Paediatrics, 81(3), 211–216. [DOI:10.1159/000356923]
Sandhu, R., Chollet-Hinton, L., Kirk, E. L., Midkiff, B., & Troester, M. A. (2016). Digital histologic analysis reveals morphometric patterns of age-related involution in breast epithelium and stroma. Human Pathology, 48, 60–68. [DOI:10.1016/j.humpath.2015.09.031]
Santen, R. J., Karaguzel, G., Livaoglu, M., Yue, W., Cline, J. M., Ratan, A., & Sasano, H. (2024). Role of ERα and aromatase in juvenile gigantomastia. The Journal of Clinical Endocrinology and Metabolism, online ahead of print. [DOI:10.1210/clinem/dgae019]
Sanuki, J., Fukuma, E., & Uchida, Y. (2008). Morphologic Study of Nipple-Areola Complex in 600 Breasts. Aesthetic Plastic Surgery, 33(3), 295–297. [DOI:10.1007/s00266-008-9194-y]
Satoh, K., Hovey, R. C., Malewski, T., Warri, A., Goldhar, A. S., Ginsburg, E., Saito, K., Lydon, J. P., & Vonderhaar, B. K. (2007). Progesterone enhances branching morphogenesis in the mouse mammary gland by increased expression of Msx2. Oncogene, 26(54), 7526–7534. [DOI:10.1038/sj.onc.1210555]
Schauffler, G. C. (1942). Disorders During Adolescence—The Onset of Menstruation. In Schauffler, G. C. Pediatric Gynecology; with Sections on Urology and Proctology, 1st Edition (pp. 169–211). Chicago: Year Book. [Google Scholar] [Google Books] [OpenLibrary] [WorldCat] [URL]
Schindler, A. E. (2010). Dydrogesterone and other progestins in benign breast disease: an overview. Archives of Gynecology and Obstetrics, 283(2), 369–371. [DOI:10.1007/s00404-010-1456-7]
Scott, P. P., Greene, R., Lane-Roberts, C. S., & Swain, V. (1950). The Function of the Breast. In Saner, F. D. (Ed.). The Breast: Structure, Function, Disease (pp. 53–86). Baltimore: Williams and Wilkins. [Google Scholar] [Google Books] [OpenLibrary] [WorldCat] [URL] [PDF]
Seal, L. (2017). Adult Endocrinology. In Richards, C., Bouman, W. P., & Barker, M.-J. (Eds.). Genderqueer and Non-Binary Genders (Critical and Applied Approaches in Sexuality, Gender and Identity) (pp. 183–223). London: Palgrave Macmillan UK. [DOI:10.1057/978-1-137-51053-2_10]
Seal, L. J., Franklin, S., Richards, C., Shishkareva, A., Sinclaire, C., & Barrett, J. (2012). Predictive Markers for Mammoplasty and a Comparison of Side Effect Profiles in Transwomen Taking Various Hormonal Regimens. The Journal of Clinical Endocrinology & Metabolism, 97(12), 4422–4428. [DOI:10.1210/jc.2012-2030]
Seibert, B., & Günzel, P. (1994). Animal toxicity studies performed for risk assessment of the once-a-month injectable contraceptive Mesigyna®. Contraception, 49(4), 303–333. [DOI:10.1016/0010-7824(94)90030-2]
Shapiro, L. R. (1982). Disorders of Female Sex Differentiation. In Blaustein, A. (Ed.). Pathology of the Female Genital Tract, 2nd Edition (pp. 479–510). New York: Springer New York. [DOI:10.1007/978-1-4757-1767-9_20]
Shearman, R. P. (1972). Ovarian Function and its Control. In Shearman, R. P. (Ed.). Human Reproductive Physiology, 1st Edition (pp. 45–90). Oxford: Blackwell Scientific Publications. [Google Scholar] [Google Books] [OpenLibrary] [WorldCat] [Archive.org]
Shearman, R. P. (1972). Primary Ammenorhoea. In Dewhurst, C. J. (Ed.). Integrated Obstetrics and Gynaecology for Postgraduates, 1st Edition (pp. 55–62). Oxford: Blackwell Scientific Publications. [Google Scholar] [Google Books] [OpenLibrary] [WorldCat] [Archive.org]
Shi, H. Y., Lydon, J. P., & Zhang, M. (2004). Hormonal Defect in Maspin Heterozygous Mice Reveals a Role of Progesterone in Pubertal Ductal Development. Molecular Endocrinology, 18(9), 2196–2207. [DOI:10.1210/me.2004-0052]
Shuttleworth, F. K. (1938). The Adolescent Period: A Graphic and Pictorial Atlas (Monographs of the Society for Research in Child Development, Volume 3, Number 3 / Serial No. 16). Washington, D. C.: Society for Research in Child Development. [Google Scholar] [Google Books] [DOI:10.2307/1165482]
Simmer, H. H., Pion, R. J., & Dignam, W. J. (1965). Testicular Feminization: Endocrine Function of Feminizing Testes, Comparison with Normal Testes. Springfield, Illinois: Thomas. [Google Scholar] [Google Books] [OpenLibrary] [WorldCat]
Simpson, J. L., & Rebar, R. W. (1990). Normal and Abnormal Sexual Differentiation and Development. In Becker, K. L., Bilezikian, J. P., Bremner, W. J., Hung, W., Kahn, C. R., Loriaux, D. L., Rebar, R. W., Robertson, G. L., & Wartofsky, L. (Eds.). Principles and Practice of Endocrinology and Metabolism, 1st Edition (pp. 710–739). Philadelphia: Lippincott. [Google Scholar] [Google Books—3rd/2001 Edition] [OpenLibrary] [WorldCat] [Archive.org]
Sindi, R., Sá Dos Reis, C., Bennett, C., Stevenson, G., & Sun, Z. (2019). Quantitative Measurements of Breast Density Using Magnetic Resonance Imaging: A Systematic Review and Meta-Analysis. Journal of Clinical Medicine, 8(5), 745. [DOI:10.3390/jcm8050745]
Sitruk-Ware, R., Basdevant, A., de Lignières, B., & Mauvais-Jarvis, P. (1984). Percutaneous oestrogen therapy. In van Herendael, H., van Herendael, B., Riphagen, F. E., Goessens, L., & van der Plas, H. (Eds.). The Climacteric: An Update: Proceedings of the fourth Jan Palfijn Symposium, European Conference on the Menopause, held in Antwerp, Belgium, on September 1–2, 1983, under the auspices of ‘De Vereniging voor Nederlandstalige gynecologen van België’ and ‘The International Menopause Society’ (pp. 127–139). Lancaster: MTP Press. [Google Scholar] [Google Books] [OpenLibrary] [WorldCat] [DOI:10.1007/978-94-009-5608-7_14]
Sizonenko, P. C. (1978). Endocrinology in Preadolescents and Adolescents. American Journal of Diseases of Children, 132(7), 704–712. [DOI:10.1001/archpedi.1978.02120320064015]
Škarda, J., Fremrová, V., & Bezecný, I. (1989). Progesterone alone is responsible for stimulation of the growth of ducts and of mammary alveolar structures in mice. Endocrinologia Experimentalis, 23(1), 17–28. [Google Scholar] [PubMed] [PDF]
Sobrinho, L. G., Kase, N., & Grunt, J. A. (1971). Spontaneous pubertal breast growth in a castrated patient with the syndrome of testicular feminization. The Yale Journal of Biology and Medicine, 44(2), 225–9. [Google Scholar] [PubMed] [PubMed Central] [PDF]
Sosa, M., Jódar, E., Arbelo, E., Domínguez, C., Saavedra, P., Torres, A., Salido, E., de Tejada, M. J., & Hernández, D. (2003). Bone Mass, Bone Turnover, Vitamin D, and Estrogen Receptor Gene Polymorphisms in Male to Female Transsexuals. Journal of Clinical Densitometry, 6(3), 297–304. [DOI:10.1385/jcd:6:3:297]
Sosa, M., Jódar, E., Arbelo, E., Domı́nguez, C., Saavedra, P., Torres, A., Salido, E., Limiñana, J., Gómez de Tejada, M. J., & Hernández, D. (2004). Serum lipids and estrogen receptor gene polymorphisms in male-to-female transsexuals: effects of estrogen treatment. European Journal of Internal Medicine, 15(4), 231–237. [DOI:10.1016/j.ejim.2004.04.009]
Soyal, S., Ismail, P. M., Li, J., Mulac-Jericevic, B., Conneely, O. M., & Lydon, J. P. (2002). Progesterone receptors - animal models and cell signaling in breast cancer: Progesterone’s role in mammary gland development and tumorigenesis as disclosed by experimental mouse genetics. Breast Cancer Research, 4(5), 191. [DOI:10.1186/bcr451]
Sperling, R. L., & Gold, J. J. (1973). Use of an anti-estrogen after a reduction mammaplasty to prevent recurrence of virginal hypertrophy of breasts. Plastic and Reconstructive Surgery, 52(4), 439–442. [DOI:10.1097/00006534-197352040-00030]
Spitz, I. M., Shoupe, D., Sitruk-Ware, R., & Mishell, D. R. (1989). Response to the antiprogestagen RU 486 (mifepristone) during early pregnancy and the menstrual cycle in women. Journal of Reproduction and Fertility Supplement, 37, 253–260. [Google Scholar] [PubMed]
Spitz, I., Croxatto, H., Lahteenmaki, P., Heikinheimo, O., & Bardin, C. (1994). Effect of mifepristone on inhibition of ovulation and induction of luteolysis. Human Reproduction, 9(Suppl 1), 69–76. [DOI:10.1093/humrep/9.suppl_1.69]
Spitz, I. M. (2010). Mifepristone: where do we come from and where are we going? Contraception, 82(5), 442–452. [DOI:10.1016/j.contraception.2009.12.012]
Sridhar, G. R., & Sinha, M. J. (1995). Macromastia in adolescent girls. Indian Pediatrics, 32(4), 496–499. [Google Scholar] [PubMed] [PDF]
Sun, B. Z., Kangarloo, T., Adams, J. M., Sluss, P. M., Welt, C. K., Chandler, D. W., Zava, D. T., McGrath, J. A., Umbach, D. M., Hall, J. E., & Shaw, N. D. (2018). Healthy Post-Menarchal Adolescent Girls Demonstrate Multi-Level Reproductive Axis Immaturity. The Journal of Clinical Endocrinology & Metabolism, 104(2), 613–623. [DOI:10.1210/jc.2018-00595]
Sun, S. X., Bostanci, Z., Kass, R. B., Mancino, A. T., Rosenbloom, A. L., Klimberg, V. S., & Bland, K. I. (2018). Breast Physiology: Normal and Abnormal Development and Function. In Bland, K. I., Copeland, E. M., Klimberg, V. S., Gradishar, W. J., White, J., & Korourian, S. (Eds.). The Breast: Comprehensive Management of Benign and Malignant Diseases, 5th Edition (pp. 37–56.e6). Philadelphia: Elsevier. [DOI:10.1016/b978-0-323-35955-9.00003-9]
Swelstad, M. R., Swelstad, B. B., Rao, V. K., & Gutowski, K. A. (2006). Management of Gestational Gigantomastia. Plastic and Reconstructive Surgery, 118(4), 840–848. [DOI:10.1097/01.prs.0000232364.40958.47]
Tack, L. J., Heyse, R., Craen, M., Dhondt, K., Bossche, H. V., Laridaen, J., & Cools, M. (2017). Consecutive Cyproterone Acetate and Estradiol Treatment in Late-Pubertal Transgender Female Adolescents. The Journal of Sexual Medicine, 14(5), 747–757. [DOI:10.1016/j.jsxm.2017.03.251]
Talbert, L. M., Hammond, M. G., Groff, T., & Udry, J. R. (1985). Relationship of age and pubertal development to ovulation in adolescent girls. Obstetrics & Gynecology, 66(4), 542–544. [Google Scholar] [PubMed] [URL]
Tanos, T., & Brisken, C. (2008). What Signals Operate in the Mammary Niche? Breast Disease, 29(1), 69–82. [DOI:10.3233/bd-2008-29108]
Thanaboonyawat, I., Chanprapaph, P., Lattalapkul, J., & Rongluen, S. (2013). Pilot Study of Normal Development of Nipples during Pregnancy. Journal of Human Lactation, 29(4), 480–483. [DOI:10.1177/0890334413493350]
Thody, A. J., & Smith, A. G. (1977). Hormones and Skin Pigmentation in the Mammal. International Journal of Dermatology, 16(8), 657–664. [DOI:10.1111/j.1365-4362.1977.tb01876.x]
Thoresen, M., & Wesche, J. (1988). Doppler measurements of changes in human mammary and uterine blood flow during pregnancy and lactation. Acta Obstetricia et Gynecologica Scandinavica, 67(8), 741–745. [DOI:10.3109/00016349809004301]
Tiefenbacher, K., & Daxenbichler, G. (2008). The Role of Androgens in Normal and Malignant Breast Tissue. Breast Care, 3(5), 325–331. [DOI:10.1159/000158055]
Tim, F., Jeroen, V., & T’Sjoen, G. (2023). Dose Reduction of Cyproterone Acetate in Trans Women and the Effect on Patient-reported Outcomes: Results from the ENIGI Study. Endocrine Abstracts, 97 [Belgian Endocrine Society 2023], 5–5 (abstract no. 007). [URL] [PDF]
Trabert, B., Sherman, M. E., Kannan, N., & Stanczyk, F. Z. (2019). Progesterone and Breast Cancer. Endocrine Reviews, 41(2), 320–344. [DOI:10.1210/endrev/bnz001]
Tucker, H. (2000). Hormones, Mammary Growth, and Lactation: a 41-Year Perspective. Journal of Dairy Science, 83(4), 874–884. [DOI:10.3168/jds.s0022-0302(00)74951-4]
Turan, S., Bereket, A., Guran, T., Akcay, T., Papari-Zareei, M., & Auchus, R. J. (2009). Puberty in a case with novel 17-hydroxylase mutation and the putative role of estrogen in development of pubic hair. European Journal of Endocrinology, 160(2), 325–330. [DOI:10.1530/eje-08-0632]
Turner, C. W. (1939). The Mammary Glands. In Allen, E., Danforth, C. H., & Doisy, E. A. (Eds.). Sex and Internal Secretions: A Survey of Recent Research, 2nd Edition (pp. 740–803). Baltimore: Williams & Wilkins. [Google Scholar] [Google Books] [OpenLibrary] [WorldCat]
Ulrich, U., Pfeifer, T., & Lauritzen, C. (1994). Rapid Increase in Lumbar Spine Bone Density in Osteopenic Women by High-Dose Intramuscular Estrogen-Progestogen Injections. Hormone and Metabolic Research, 26(9), 428–431. [DOI:10.1055/s-2007-1001723]
Ulrich, U., Pfeifer, T., Buck, G., Keckstein, J., & Lauritzen, C. (1995). High-dose estrogen-progestogen injections in gonadal dysgenesis, ovarian hypoplasia, and androgen insensitivity syndrome: Impact on bone density. Adolescent and Pediatric Gynecology, 8(1), 20–23. [DOI:10.1016/s0932-8610(12)80156-3]
Valentine, G. H. (1969). Chromosome Anomalies in the Female. In Valentine, G. H. The Chromosome Disorders: An Introduction for Clinicians, 2nd Edition (pp. 126–143). London: W. Heinemann Medical Books. [Google Scholar] [Google Books] [OpenLibrary] [WorldCat] [Archive.org]
van der Meulen, A. J. (1974). An unusual case of massive hypertrophy of the breasts. South African Medical Journal=Suid-Afrikaanse Tydskrif vir Geneeskunde, 48(34), 1465–1466. [Google Scholar] [PubMed] [URL 1] [URL 2]
Vandeweyer, E., & Hertens, D. (2002). Quantification of glands and fat in breast tissue: An experimental determination. Annals of Anatomy - Anatomischer Anzeiger, 184(2), 181–184. [DOI:10.1016/s0940-9602(02)80016-4]
Venturoli, S., Fabbri, R., Porcu, E., Paradisi, R., Orsini, L. F., Brondelli, L., Ruggeri, S., & Flamigni, C. (1989). Endocrine and ovarian parameters at various frequencies of ovulation in adolescents. Archives of Gynecology and Obstetrics, 246(2), 107–114. [DOI:10.1007/bf00934127]
Venturoli, S., Porcu, E., Fabbri, R., Magrini, O., Paradisi, R., Pallotti, G., Gammi, L., & Flamigni, C. (1987). Postmenarchal evolution of endocrine pattern and ovarian aspects in adolescents with menstrual irregularities. Fertility and Sterility, 48(1), 78–85. [DOI:10.1016/s0015-0282(16)59294-2]
Vorherr, H. (1974). Development of the Female Breast. In Vorherr, H. The Breast: Morphology, Physiology, and Lactation (pp. 1–19). New York: Academic Press. [Google Scholar] [Google Books] [OpenLibrary] [WorldCat]
Vorherr, H. (1974). Morphology of the Mature Female Breast. In Vorherr, H. The Breast: Morphology, Physiology, and Lactation (pp. 20–70). New York: Academic Press. [Google Scholar] [Google Books] [OpenLibrary] [WorldCat]
Wade, T. R., Wade, S. L., & Jones, H. E. (1978). Skin changes and diseases associated with pregnancy. Obstetrics and Gynecology, 52(2), 233–242. [Google Scholar] [PubMed] [URL]
Walker, M., Baker, G., & Lamb, M. (2013). Physiology of the Breast During Pregnancy and Lactation. In Mannel, R., Martens, P. J., & Walker, M. (Eds.). Core Curriculum for Lactation Consultant Practice, 3rd Edition (pp. 287–300). Burlington: Jones & Bartlett Learning. [Google Scholar] [Google Books—2013/3rd Edition] [Google Books—2008/2nd Edition] [OpenLibrary] [WorldCat]
Wang, C., Luan, J., Cheng, H., Chen, L., Li, Z., Panayi, A. C., & Liu, C. (2018). Menstrual Cycle-Related Fluctuations in Breast Volume Measured Using Three-Dimensional Imaging: Implications for Volumetric Evaluation in Breast Augmentation. Aesthetic Plastic Surgery, 43(1), 1–6. [DOI:10.1007/s00266-018-1243-6]
Wang, Q. A., & Scherer, P. E. (2019). Remodeling of Murine Mammary Adipose Tissue during Pregnancy, Lactation, and Involution. Journal of Mammary Gland Biology and Neoplasia, 24(3), 207–212. [DOI:10.1007/s10911-019-09434-2]
Weisberg, M. G., Malkasian, G. D., & Pratt, J. H. (1970). Testicular feminization syndrome. American Journal of Obstetrics and Gynecology, 107(8), 1181–1187. [DOI:10.1016/s0002-9378(15)30367-7]
Wellons, M. F., & Rebar, R. W. (2013). Amenorrhea. In Falcone, T., & Hurd, W. W. (Eds.). Clinical Reproductive Medicine and Surgery: A Practical Guide, 2nd Edition (pp. 105–112). New York: Springer New York. [DOI:10.1007/978-1-4614-6837-0_7]
Wellons, M. F., Weeber, K. M., & Rebar, R. W. (2017). Amenorrhea. In Falcone, T., & Hurd, W. W. (Eds.). Clinical Reproductive Medicine and Surgery, 3rd Edition (pp. 109–122). Cham: Springer International Publishing. [DOI:10.1007/978-3-319-52210-4_6]
Werner, A. A. (1935). Experiment to produce lactation in castrate women. Endocrinology, 19(2), 144–150. [DOI:10.1210/endo-19-2-144]
Whiteley, S. (1994). Predictors of Milk Production in Lactating Women. (Master’s thesis, The Open University.) [Google Scholar] [DOI:10.21954/ou.ro.0000fe02] [URL]
Wierckx, K., Gooren, L., & T’Sjoen, G. (2014). Clinical Review: Breast Development in Trans Women Receiving Cross-Sex Hormones. The Journal of Sexual Medicine, 11(5), 1240–1247. [DOI:10.1111/jsm.12487]
Wierckx, K., Van Caenegem, E., Schreiner, T., Haraldsen, I., Fisher, A., Toye, K., Kaufman, J. M., & T’Sjoen, G. (2014). Cross‐Sex Hormone Therapy in Trans Persons Is Safe and Effective at Short‐Time Follow‐Up: Results from the European Network for the Investigation of Gender Incongruence. The Journal of Sexual Medicine, 11(8), 1999–2011. [DOI:10.1111/jsm.12571]
Wilson, J. D. (1968 March 28). Medical Grand Rounds: Testicular Feminization. Parkland Memorial Hospital, UT Southwestern Medical Center. [Google Scholar] [URL] [PDF]
Wilson, C. L., Sims, A. H., Howell, A., Miller, C. J., & Clarke, R. B. (2006). Effects of oestrogen on gene expression in epithelium and stroma of normal human breast tissue. Endocrine-Related Cancer, 13(2), 617–628. [DOI:10.1677/erc.1.01165]
Winkler, U. H., Schindler, A. E., Brinkmann, U. S., Ebert, C., & Oberhoff, C. (2001). Cyclic progestin therapy for the management of mastopathy and mastodynia. Gynecological Endocrinology, 15(Suppl 6), 37–43. [DOI:10.1080/gye.15.s6.37.43]
Wisniewski, A. B., Migeon, C. J., Meyer-Bahlburg, H. F., Gearhart, J. P., Berkovitz, G. D., Brown, T. R., & Money, J. (2000). Complete Androgen Insensitivity Syndrome: Long-Term Medical, Surgical, and Psychosexual Outcome. The Journal of Clinical Endocrinology & Metabolism, 85(8), 2664–2669. [DOI:10.1210/jcem.85.8.6742]
Wong, R. C., & Ellis, C. N. (1984). Physiologic skin changes in pregnancy. Journal of the American Academy of Dermatology, 10(6), 929–940. [DOI:10.1016/s0190-9622(84)80305-9]
Wren, B. G., & Eden, J. A. (1996). Do Progestogens Reduce The Risk of Breast Cancer? A Review of the Evidence. Menopause, 3(1), 4–12. [DOI:10.1097/00042192-199603010-00003]
Wright, E. M. (2015). Breastfeeding and the Mother–Newborn Dyad (pp. 1157–1182). In King, T. L., Brucker, M. C., Kriebs, J. M., Fahey, J. O., Gegor, C. L., & Varney, H. (Eds.). Varney’s Midwifery, 5th Edition. Burlington: Jones & Bartlett Learning. [Google Scholar] [Google Books] [OpenLibrary] [WorldCat]
Xu, P., Ye, W., Zhong, S., Li, H., Feng, E., Lin, S. H., Kuo, C. T., Liu, J. Y., & Lin, Y. C. (2010). Leptin and zeranol up-regulate cyclin D1 expression in primary cultured normal human breast pre-adipocytes. Molecular Medicine Reports, 3(6), 983–990. [DOI:10.3892/mmr.2010.370]
Yang, W., Hong, T., Chang, X., Han, M., Gao, H., Pan, B., Zhao, Z., & Liu, Y. (2024). The efficacy of and user satisfaction with different antiandrogens in Chinese transgender women. International Journal of Transgender Health, advance online publication. [DOI:10.1080/26895269.2024.2323514]
Zacharin, M. (2000). Use of androgens and oestrogens in adolescents - A review of hormone replacement treatment. Journal of Pediatric Endocrinology and Metabolism, 13(1), 3–12. [DOI:10.1515/JPEM.2000.13.1.3]
Zachmann, M., Prader, A., Sobel, E. H., Crigler, J. F., Ritzén, E. M., Atarés, M., & Ferrandez, A. (1986). Pubertal growth in patients with androgen insensitivity: Indirect evidence for the importance of estrogens in pubertal growth of girls. The Journal of Pediatrics, 108(5), 694–697. [DOI:10.1016/s0022-3476(86)81043-5]
Żelaźniewicz, A., & Pawłowski, B. (2015). Breast size and asymmetry during pregnancy in dependence of a fetus’s sex. American Journal of Human Biology, 27(5), 690–696. [DOI:10.1002/ajhb.22716]
Żelaźniewicz, A., & Pawłowski, B. (2018). Maternal breast volume in pregnancy and lactation capacity. American Journal of Physical Anthropology, 168(1), 180–189. [DOI:10.1002/ajpa.23734]
Zhang, D., Yao, F., Tian, T., Deng, S., Luo, M., & Tian, Q. (2021). Clinical characteristics and molecular genetics of complete androgen insensitivity syndrome patients: a series study of 30 cases from a Chinese tertiary medical center. Fertility and Sterility, 115(5), 1270–1279. [DOI:10.1016/j.fertnstert.2020.12.008]
\ No newline at end of file
diff --git a/transfemscience.org/articles/shbg-unimportant/index.html b/transfemscience.org/articles/shbg-unimportant/index.html
index ff4ebc88..6b928bb2 100644
--- a/transfemscience.org/articles/shbg-unimportant/index.html
+++ b/transfemscience.org/articles/shbg-unimportant/index.html
@@ -1 +1 @@
-The Interactions of Sex Hormones with Sex Hormone-Binding Globulin and Relevance for Transfeminine Hormone Therapy - Transfeminine Science
The Interactions of Sex Hormones with Sex Hormone-Binding Globulin and Relevance for Transfeminine Hormone Therapy
By Aly | First published July 10, 2020 | Last modified March 25, 2023
Abstract / TL;DR
Sex hormones such as testosterone and estradiol bind to blood proteins like albumin and SHBG. This limits their biological activity by reducing their free fractions. Androgens decrease SHBG production while estrogens increase SHBG production. Hence, testosterone and estradiol can influence their own free fractions. Due to robust inactivation in the liver, testosterone and estradiol have relatively small influences on SHBG levels under normal physiological circumstances. At very high levels however, they can considerably influence SHBG levels. During pregnancy, when there are massive increases in estradiol levels (e.g., 100-fold), a maximal 5- to 10-fold elevation in SHBG levels occurs. Although large increases in SHBG levels can strongly limit the biological activity of testosterone, the situation with estradiol is different. In late pregnancy, the percentage of estradiol that is free appears to be decreased only to around 60% of that of non-pregnancy. Earlier in pregnancy, when estradiol levels are lower, the free fractions of estradiol are reduced to a lesser extent. At typical therapeutic levels of estradiol in transfeminine hormone therapy (<200 pg/mL), the limiting influence of SHBG on free estradiol is minimal. Oral estradiol has a greater influence on SHBG production than non-oral estradiol and may be a different case however. In any case, consequent lesser activity of oral estradiol is only theoretical, and available clinical studies so far haven’t reported important therapeutic differences relative to non-oral estradiol. Although SHBG may reduce free estradiol fractions in some contexts, only relatively low estradiol levels (<50 pg/mL) appear to be needed for maximal feminization and breast development in cisgender females and transfeminine people. In conclusion, the influence of SHBG on the effectiveness of estradiol isn’t something that should be a major source of concern in transfeminine hormone therapy.
Binding of Sex Hormones to Blood Proteins
Sex hormones bind to proteins in the blood called plasma proteins. This is a phenomenon known as plasma protein binding. In the case of androgens and estrogens, the plasma proteins they bind to are mainly albumin and sex hormone-binding globulin (SHBG). Plasma protein binding serves to prevent sex hormones from interacting with their target cells and hence from binding to and activating their receptors (Hammond, 2016). This is because plasma proteins are too large and lipid-insoluble to cross the lipid-rich cell membrane. As a result, they’re unable to diffuse through capillaries to exit the circulation and enter into tissues or to be taken up into cells. When the sex hormone is bound to plasma protein, it can’t reach target cells either. Hence, plasma protein binding limits the biological activity of sex hormones (Hammond, 2016). Binding to plasma proteins also serves to extend the biological half-lives of sex hormones. This is because protein-bound sex hormone is likewise unavailable for metabolism and elimination, processes that depend on cellular uptake.
There is only a single sex hormone binding site per molecule of SHBG (Moore & Bulbrook, 1988), whereas albumin has six binding sites for different substrates (Pardridge, 1988). Androgens and estradiol have high affinity for SHBG (nM) and low affinity for albumin (μM) (Moore & Bulbrook, 1988; Hammond, 2016). However, albumin levels are several orders of magnitude higher than SHBG levels (μM vs. nM), so this serves to balance out the fractions of sex hormone bound to each protein (Hammond, 2016). Androgens have higher affinities for SHBG than do estradiol or other estrogens. Estradiol has only about 10 to 20% of the affinity of dihydrotestosterone (DHT) and 33 to 50% of the affinity of testosterone for SHBG (Anderson, 1974; Ojasoo & Raynaud, 1978; Pugeat, Dunn, Nisula, 1981). As such, testosterone and DHT bind more strongly to SHBG than does estradiol.
The vast majority of sex hormone content in the blood is bound to plasma proteins; at any given time more than 97% of the testosterone, estradiol, and progesterone in the blood is plasma protein-bound (Strauss & FitzGerald, 2019). The fraction of sex hormone that isn’t bound to plasma proteins is known as the free or unbound fraction. This is the fraction that is available for diffusion into cells and hence is considered to be biologically active (Hammond, 2016). Total levels refer to both free/unbound and bound hormone. Bioavailable levels include both albumin-bound and free hormone levels. Due to their relatively weak affinity for albumin, sex hormones bound to albumin may to some extent be biologically active—hence the “bioavailable” descriptor (Nguyen et al., 2008). However, more research is needed to fully elucidate the biological activity of albumin-bound sex hormone fractions.
The relative calculated free and bound percentages of estradiol, testosterone, and DHT to albumin, SHBG, and another plasma protein known as corticosteroid-binding globulin (CBG) (only binds small fractions of the androgens and has no binding to estradiol) are shown in the table below.
Free sex hormone levels and percentages are often calculated from levels of total sex hormone, albumin, SHBG, and CBG with validated mathematical models constructed from data of published studies. This is because free sex hormone levels are usually very low (pM range) and are difficult to measure with routine blood testing methods. While generally in the vicinity of the true values, calculated results may not always be fully accurate (Rosner, 2015; Goldman et al., 2017; Handelsman, 2017; Keevil & Adaway, 2019). As such, measured levels, when feasible, are preferable.
Testosterone, DHT, and estradiol are strongly inactivated by the liver and have relatively weak effects in this part of the body under normal circumstances. As a result, they have much less relative impact on SHBG production than do synthetic hormonal agents. Accordingly, SHBG levels change only slightly over the course of the menstrual cycle in women despite substantial fluctuations in estradiol levels (Freymann et al., 1977b; Plymate et al., 1985; Schijf et al., 1993; Braunstein et al., 2011; Rothman et al., 2011; Fanelli et al., 2013; Rezaii et al., 2017). In one study, SHBG levels increased by about 6 to 13% (+2.9–5.3 nmol/L) going from the follicular phase to the luteal phase of the cycle (Braunstein et al., 2011). There is additionally only a small decrease in SHBG levels attributable to the sharp decline in estradiol with menopause (Burger et al., 2000; Guthrie et al., 2004). Nonetheless, estradiol therapy can more considerably influence the production of SHBG and other liver proteins as well under specific conditions (Kuhl, 1998). This is due to 1) use of oral estradiol, which because of the first pass through the liver has a greater impact on estrogen-sensitive liver synthesis than non-oral routes (Kuhl, 2005); and 2) use of high estradiol doses, for instance typical injectable doses. The table below shows SHBG increases from various studies with different estrogen routes, doses, and types.
Table 2: Relative increases in SHBG levels with some different estrogenic exposures:
a Estimated typical estradiol levels from various sources (e.g., Aly, 2020; Wiki). b Due to differences in molecular weight, EV has about 75% of the amount of estradiol as regular estradiol. Hence, 6 mg/day EV is approximately equivalent to 4.5 mg/day E2.
The influence of estradiol on SHBG levels is most relevant to pregnancy, when estradiol levels increase to far higher levels than usual. In late pregnancy, estradiol levels are generally around 15,000 to 25,000 pg/mL on average (Graphs; Troisi et al., 2003; Adamcová et al., 2018). These estradiol levels are on the order of 100-fold higher than normal menstrual cycle levels. In parallel with the massive increases in estradiol levels, SHBG levels increase by about 5- to 10-fold by late pregnancy (Anderson, 1974; Hammond, 2017). The dose–response curve of estrogens on SHBG production shows saturation, with most of the increase in SHBG levels happening at lower estradiol levels as well as limits to how much SHBG levels can be increased (Mean, Pellaton, & Magrini, 1977; O’Leary et al., 1991; Kerlan et al., 1994; Kuhl, 1999). The graphs below show SHBG levels throughout pregnancy.
Figure 1: SHBG and total estradiol levels during pregnancy in women (O’Leary et al., 1991). The lines are the mean and/or 95th percentile levels while the points are individual measurements.
Figure 2: Total sex hormone and SHBG levels during pregnancy in women (Kerlan et al., 1994).
Effects of SHBG Increase on Free Sex Hormone Levels
Changes in SHBG levels result in changes in SHBG-bound and free sex hormone levels. Aside from DHT, estradiol and testosterone are the hormones of the greatest interest in this regard.
SHBG Increase and Free Testosterone
EE-containing birth control pills, with their 4-fold increase in SHBG levels, substantially decrease the free percentage of testosterone (Graham et al., 2007; Zimmerman et al., 2014). In one study, an EE-containing birth control pill decreased the free testosterone fraction from 2.45% to 0.78% (a 3.2-fold decrease or to 32% of baseline) (Graham et al., 2007). Due to concomitant suppression of testosterone production and hence reduced total testosterone levels, free testosterone levels decreased from 0.89 pg/mL to 0.18 pg/mL (a 5-fold decrease, to 20% of baseline) (Graham et al., 2007). The influence of EE on SHBG levels contributes significantly to the antiandrogenic effects of EE-containing birth control pills, which are taken advantage of therapeutically to treat acne and hirsutism in women.
During pregnancy, testosterone levels increase to as much as 150 ng/dL (around 5-fold higher than non-pregnancy levels) (McClamrock, 2007). The increase in SHBG production during pregnancy serves an important function in that the higher SHBG levels neutralize the biological activity of the increased testosterone levels (Hammond, 2017). In one study, the free testosterone fraction was 6-fold lower in late pregnancy than in non-pregnant women (0.23% vs. 1.36%—or to 17% of non-pregnancy) (Dunn, Nisula, & Rodbard, 1981). Hence, despite substantial increases in total testosterone levels during pregnancy, free testosterone levels and by extension androgenic action in the body change minimally (Barini, Liberale, & Menini, 1993; Schuijt et al., 2019). A case report of marked hyperandrogenism due to severe SHBG deficiency in a pregnant woman evidences the role of SHBG in limiting the androgenic actions of testosterone during this time (Hogeveen et al., 2002; Hammond, 2017).
SHBG Increase and Free Estradiol
Endogenous and Non-Oral Estradiol
The research indicates that increases in SHBG levels and by extension decreases in the free estradiol fraction are minimal with physiological levels of estradiol (e.g., <200 pg/mL). This is the case whether the estradiol is endogenous or exogenous in origin—so long as it is taken non-orally. Such conclusions are based on both calculated and measured studies of free estradiol (e.g., Freymann et al., 1977b).
Increases in SHBG levels and decreases in the free estradiol fraction become more significant with supraphysiological levels of estradiol however, for instance during pregnancy and with very-high-dose estradiol therapy. Studies on changes in free estradiol with high doses of estradiol are few. This is especially true in the case of measured as opposed to calculated free estradiol. In any case, one can look at pregnancy to gain insight on the question of free estradiol with high estradiol levels. Moreover, due to the very high estradiol levels in pregnancy, free estradiol is more amenable to measurement during this time. Accordingly, multiple studies of measured free estradiol in pregnancy are available.
Although free estradiol percentages during pregnancy certainly decrease, the increases in estradiol are far from neutralized by SHBG. Hence, the situation with free estradiol in pregnancy is very different from that of testosterone. This is illustrated in the following excerpt (Rubinow et al., 2002):
Pregnancy is accompanied by a slow but sustained rise in the plasma levels of many steroid and peptide hormones and is followed by a precipitous drop in their levels over the first few days after delivery. By the third trimester of pregnancy, plasma progesterone levels average approximately 150 ng/ml and estradiol levels range from 10 to 15 ng/ml. These amounts represent a 10- and 50-fold increase, respectively, of maximum menstrual cycle levels (Tulchinsky et al., 1972). Although only a small fraction of these steroids are unbound, the amount of “free” (and thus biologically active) progesterone and estrogen also undergo similarly large increases during pregnancy (Heidrich et al., 1994).
In the study by Heidrich and colleagues cited in the excerpt, total estradiol levels at the time of delivery were 21,500 pg/mL and measured free estradiol levels were 232 pg/mL, with a resultant free estradiol fraction of 1.08% (Heidrich et al., 1994). For context, the free estradiol percentage in non-pregnant women ranges from 1.5 to 2.1% with RIA, while actual free estradiol levels are 0.30 to 4.1 pg/mL with RIA and 0.40 to 5.9 pg/mL with LC–MS/MS (Nakamoto, 2016). Hence, in this study free estradiol levels in late pregnancy were around 50-fold higher than maximal non-pregnancy levels.
Due to variable methodology, the findings of a single study may not be representative. As such, the table below provides measured free estradiol percentages in late pregnancy from several studies.
Table 3: Measured free estradiol percentages in late pregnancy (mean ± SD) (Perry et al., 1987):
As can be seen in the table, the free estradiol fraction in late pregnancy ranges from about 0.7 to 1.5%. Results for the free estradiol fraction from studies using calculated free estradiol levels in late pregnancy rather than measured levels are similar to measured findings, although sometimes a bit lower in comparison (e.g., 0.5%) (Dunn, Nisula, & Rodbard, 1981; Campino et al., 2001). The measured free estradiol percentage in late pregnancy can be cautiously compared to the fraction of 1.5 to 2.1% in non-pregnant women. Using middle values from these ranges, the free estradiol fraction in late pregnancy may be somewhere around 60% of that of non-pregnancy. This estimate is quite close to the actual findings of a study, which observed a decrease in the measured free estradiol percentage to 55% of that of non-pregnancy (Freymann et al., 1977a; Freymann et al., 1977b).
In contrast to estradiol, the free percentages of estrone and estriol are not different in late pregnancy when compared to non-pregnancy (Tulchinsky & Chopra, 1973; Steingold et al., 1987). This is attributable to the much lower affinities of estrone and estriol for SHBG relative to estradiol (Kuhl, 2005).
Studies have also assessed free estradiol fractions earlier in pregnancy, which might in theory differ from late pregnancy. The results of a study that measured free estradiol throughout pregnancy are shown in the table below (Freymann et al., 1977a; Freymann et al., 1977b).
In similar studies by another group of researchers, free estradiol fractions were measured in earlier pregnancy (weeks 7–16) and were found to be lower than those obtained by Freymann and colleagues (Bernstein et al., 1986; Depue et al., 1987; Bernstein et al., 1988). The free estradiol percentage was about 0.9 or 1.0% at 10 weeks and about 0.7% at 12 weeks (Bernstein et al., 1986; Depue et al., 1987; Bernstein et al., 1988). Hence, as with the results of Freymann and colleagues, the free estradiol fraction decreased as pregnancy progressed. The figure below provides a visualization of the findings.
Figure 3: Changes in total and free estradiol levels (pg/mL), free estradiol fraction (%), and SHBG binding capacity (μg/dL) during weeks 7 to 16 of pregnancy in women (Bernstein et al., 1986).
Free estradiol during pregnancy can also be calculated using total estradiol levels and SHBG levels. I roughly calculated the free estradiol fraction during pregnancy using the data from O’Leary et al. (1991) and a published calculator spreadsheet by Mazer (2009) (Aly, 2020). The results are shown below.
Figure 4: Average measured total estradiol and SHBG levels (O’Leary et al., 1991) and calculated free estradiol percentage (Mazer, 2009) throughout pregnancy in women. Another version of this graph scaled to only the first trimester of pregnancy (when estradiol levels are typically ≤2,000 pg/mL) is also provided (Graph).
The free estradiol fractions in the figure are merely rough estimations and hence should be given conservative consideration. In any case, they are similar to the findings of the available studies on measured free estradiol in earlier pregnancy just discussed—for instance in magnitude (relative to Bernstein et al.) and pattern of change throughout pregnancy (relative to both Bernstein et al. and Freymann et al.). As such, these calculated values offer a plausible and interesting model.
To summarize, there are profound increases in total estradiol levels and proportionally lower but still substantial increases in SHBG levels during pregnancy. In accordance with the marked increase in SHBG levels, the free estradiol fraction progressively decreases over the course of pregnancy. Studies are conflicting on the exact degrees to which free estradiol percentages decrease. In any case, the possibilities for the free estradiol fraction by late pregnancy range from about 0.5 to 1.5%. These figures can be compared to non-pregnancy free estradiol percentages of 1.5 to 2.1%. This may correspond to a maximal decrease in the free estradiol fraction in late pregnancy to around 60% of non-pregnancy. At the greatest extreme, the decrease may be to around 25% of non-pregnancy. Conversely, in earlier pregnancy, when estradiol levels are lower, free estradiol percentages are higher.
Despite the decreases in the free estradiol fraction during pregnancy, there are profound increases in free estradiol levels that parallel the massive increases in total estradiol. As such, the increase in estradiol levels during pregnancy markedly exceeds the limiting influences of the simultaneously elevated SHBG levels. For this reason, pregnancy is a profoundly hyperestrogenic state.
SHBG doesn’t impact estradiol like it does testosterone during pregnancy because the proportional increases in estradiol levels relative to SHBG levels are far greater in comparison and because of the relatively lower affinity of estradiol for SHBG. In general, it’s not possible for SHBG to limit the activity of estradiol in the way that it can with testosterone due to the inherent requirement for substantially increased SHBG production of much more highly increased estradiol levels.
Oral Estradiol
Oral estradiol may differ from non-oral estradiol when it comes to the issue of free estradiol. This is because oral estradiol undergoes a first pass that results in greater estradiol levels in the liver relative to the circulation. As a result, oral estradiol has disproportionate liver effects and increases SHBG levels to a proportionally greater extent than non-oral estradiol. Hence, the greater SHBG increases with oral estradiol may result in lower free estradiol fractions than with non-oral estradiol.
While this is probable, it is more difficult to determine the precise magnitudes of the differences between oral and non-oral estradiol in terms of free estradiol. Some data are available however. Clinical studies of low-dose oral estradiol in menopausal cisgender women have reported the limiting influence of the SHBG increase on calculated free estradiol to be modest (Nilsson, Holst, & von Schoultz, 1984; Nachtigall et al., 2000). Likewise, oral estradiol appears to have similar effectiveness for menopausal symptoms when compared to non-oral estradiol (Wiki; 2nd paragraph). Studies of higher doses of oral estradiol that provide data on SHBG or free estradiol levels are rare. In any case, a few studies by one group found that 6 mg/day oral estradiol valerate (a dose equivalent to approximately 4.5 mg/day oral estradiol) increased SHBG levels by about 2.5- to 3.0-fold in transgender women (Dittrich et al., 2005; Mueller et al., 2005; Mueller et al., 2006). Using the numbers from one of the studies for total estradiol and SHBG levels, it can be roughly calculated (Mazer, 2009) that the free estradiol fraction may have decreased from around 2.1% to 1.2% (a 43% reduction). Analogously, a study using oral conjugated estrogens (CEEs; Premarin) at a dose that increased SHBG levels by 2.3-fold reported that the calculated free estradiol percentage was 40% lower relative to an equivalent dose of transdermal estradiol (in terms of total estradiol levels) (Shifren et al., 2007). These findings suggest a non-trivial reduction in the free estradiol fraction with typical doses of oral estradiol in transfeminine people. Consequently, it’s possible that oral estradiol could be to a certain degree less potent at the same total estradiol levels relative to non-oral estradiol.
It’s important to be clear that it’s also not a certainty however. Levels of estrone are much higher with oral estradiol than with non-oral estradiol (~5-fold) (Kuhl, 2005), and estrone, although far less potent than estradiol, has significant intrinsic estrogenic activity similarly to estradiol (Kuhl, 2005). The degree to which estrone might add to the estrogenic activity of estradiol, if at all, is uncertain. In any case, it’s within the realm of possibility that estrone could contribute significantly to the estrogenic activity of oral estradiol (Pande et al., 2019). This additional estrogenic exposure could potentially serve to offset the impact of the higher SHBG levels and reduced free estradiol fractions that occur with oral estradiol. Further research is needed to evaluate such a possibility however. As another consideration, the higher SHBG levels with oral estradiol can be expected to reduce the free testosterone fraction in addition to that of estradiol (and to an even greater extent in comparison). This is important as testosterone suppression is a key therapeutic effect of estradiol in transfeminine people and the main justified reason for use of higher estradiol levels. Due to possibilities like these and the fact that free levels of hormones only theoretically represent their biological activity, it shouldn’t necessarily be assumed that oral estradiol is less potent or efficacious than non-oral estradiol. Only further clinical studies comparing oral estradiol to non-oral estradiol will be able to clarify this question.
Relevance for Transfeminine Hormone Therapy
Some have concerns that SHBG may substantially limit the effectiveness of estradiol and thereby hinder feminization and/or breast development. Some have even claimed that high levels of estradiol may be less effective than lower levels as a result of SHBG increases at higher levels. Before even touching on SHBG however, such notions are likely to be misguided. This is because low estradiol levels (<50 pg/mL) are known to be fully effective in terms of feminization and breast development. This is evidenced by normal and induced puberty in cisgender girls (Aly, 2020), as well as by the excellent secondary sexual development of women with complete androgen insensitivity syndrome (CAIS) (Aly, 2020; Wiki). No evidence exists at this time to indicate that higher estradiol levels are necessary or beneficial in terms of feminization or breast development (Nolan & Cheung, 2020). Available studies in fact suggest no relationship between estradiol levels and breast development in transfeminine people at typical therapeutic levels of estradiol (e.g., 50–200 pg/mL) (de Blok et al., 2017; Meyer et al., 2020; de Blok et al., 2020). This is in accordance with the concept of the maximal effect of estradiol on feminization and breast development being established at lower estradiol levels. Hence, besides the use of higher estradiol levels for testosterone suppression in transfeminine people, concerns about incomplete feminizing efficacy of estradiol consequent to inadequate estrogenic exposure have little basis.
If SHBG is nonetheless explored however, the research indicates that the role of SHBG in restricting free estradiol, and hence presumably the biological activity of estradiol, is only so considerable. Within physiological non-pregnancy ranges for estradiol (e.g., <200 pg/mL), changes in SHBG levels and free estradiol fractions due to endogenous or non-oral estradiol are minimal. Very high estradiol levels have greater influence on SHBG production than normal physiological levels however. During pregnancy, with the massive increases in estradiol and resultant 5- to 10-fold maximal elevation in SHBG levels, the free estradiol percentage may be decreased to around 60% of that of non-pregnancy. But actual free estradiol levels are nonetheless profoundly increased in pregnancy. Moreover, increases in SHBG levels and decreases in free estradiol fraction earlier in pregnancy are lower than in late pregnancy. Even with among the highest estradiol levels that would normally be encountered with non-oral estradiol therapy, the decreases in the free estradiol fraction due to SHBG are likely to be modest. The impact of such a reduction could easily be negated by a slightly greater estradiol dose.
While the preceding is applicable to non-oral estradiol, oral estradiol has a greater influence on SHBG production in comparison and hence the higher SHBG levels with oral estradiol could result in more significant limitation of free estradiol than with non-oral estradiol. The notion that this reduction in free estradiol corresponds to a decrease in the activity or potency of oral estradiol is only a theoretical possibility however. Therapeutically, oral estradiol has shown itself to be very effective. The decreases in free estradiol percentage with low-dose oral estradiol seem to be small. In addition, while no direct comparisons exist this time, higher doses of oral estradiol seem to show similar testosterone suppression as non-oral estradiol (Wiki; Graphs). Besides testosterone suppression, available studies have found no differences between oral and non-oral estradiol in terms of outcomes like breast development or feminization (Sam, 2020). As such, the differences between oral and non-oral estradiol in terms SHBG levels and free estradiol fraction may be of little therapeutic importance.
Aside from decreasing free estradiol fractions, increased SHBG levels also decrease free testosterone fractions to an even greater extent. This is advantageous in the case of transfeminine people.
Taken together, lower free estradiol due to increased SHBG levels, whether with non-oral or oral estradiol, isn’t something that should be a major source of concern in transfeminine hormone therapy.
Supplementary Material
See here for supplementary material for this article, including a spreadsheet and other calculators that can be used to estimate free hormone levels (e.g., Mazer, 2009).
References
Adamcová, K., Kolátorová, L., Škodová, T., Šimková, M., Pařízek, A., Stárka, L., & Dušková, M. (2018). Steroid hormone levels in the peripartum period – differences caused by fetal sex and delivery type. Physiological Research, 67(Suppl 3), S489–S497. [DOI:10.33549/physiolres.934019]
Anderson, P. J., Hancock, K. W., & Oakey, R. E. (1985). Non-protein-bound oestradiol and progesterone in human peripheral plasma before labour and delivery. Journal of Endocrinology, 104(1), 7–15. [DOI:10.1677/joe.0.1040007]
Barini, A., Liberale, I., & Menini, E. (1993). Simultaneous Determination of Free Testosterone and Testosterone Bound to Non-Sex-Hormone-Binding Globulin by Equilibrium Dialysis. Clinical Chemistry, 39(6), 936–941. [DOI:10.1093/clinchem/39.6.936]
Bernstein, L., Depue, R. H., Ross, R. K., Judd, H. L., Pike, M. C., & Henderson, B. E. (1986). Higher maternal levels of free estradiol in first compared to second pregnancy: early gestational differences. Journal of the National Cancer Institute, 76(6), 1035–1039. [DOI:10.1093/jnci/76.6.1035]
Bernstein, L., Pike, M., Depue, R., Ross, R., Moore, J., & Henderson, B. (1988). Maternal hormone levels in early gestation of cryptorchid males: a case-control study. British Journal of Cancer, 58(3), 379–381. [DOI:10.1038/bjc.1988.223]
Bland, L. B., Garzotto, M., DeLoughery, T. G., Ryan, C. W., Schuff, K. G., Wersinger, E. M., Lemmon, D., & Beer, T. M. (2005). Phase II study of transdermal estradiol in androgen-independent prostate carcinoma. Cancer, 103(4), 717–723. [DOI:10.1002/cncr.20857]
Braunstein, G. D., Reitz, R. E., Buch, A., Schnell, D., & Caulfield, M. P. (2011). Testosterone Reference Ranges in Normally Cycling Healthy Premenopausal Women. The Journal of Sexual Medicine, 8(10), 2924–2934. [DOI:10.1111/j.1743-6109.2011.02380.x]
Burger, H. G., Dudley, E. C., Cui, J., Dennerstein, L., & Hopper, J. L. (2000). A Prospective Longitudinal Study of Serum Testosterone, Dehydroepiandrosterone Sulfate, and Sex Hormone-Binding Globulin Levels through the Menopause Transition. The Journal of Clinical Endocrinology & Metabolism, 85(8), 2832–2838. [DOI:10.1210/jcem.85.8.6740]
Campino, C., Torres, C., Rioseco, A., Poblete, A., Pugin, E., Valdés, V., Catalán, S., Belmar, C., & Serón-Ferré, M. (2001). Plasma prolactin/oestradiol ratio at 38 weeks gestation predicts the duration of lactational amenorrhoea. Human Reproduction, 16(12), 2540–2545. [DOI:10.1093/humrep/16.12.2540]
de Blok, C. J., Klaver, M., Wiepjes, C. M., Nota, N. M., Heijboer, A. C., Fisher, A. D., Schreiner, T., T’Sjoen, G., & den Heijer, M. (2017). Breast Development in Transwomen After 1 Year of Cross-Sex Hormone Therapy: Results of a Prospective Multicenter Study. The Journal of Clinical Endocrinology & Metabolism, 103(2), 532–538. [DOI:10.1210/jc.2017-01927]
de Blok, C. J., Dijkman, B. A., Wiepjes, C. M., Staphorsius, A. S., Timmermans, F. W., Smit, J. M., Dreijerink, K. M., & den Heijer, M. (2020). Sustained Breast Development and Breast Anthropometric Changes in 3 Years of Gender-Affirming Hormone Treatment. The Journal of Clinical Endocrinology & Metabolism, 106(2), e782–e790. [DOI:10.1210/clinem/dgaa841]
Depue, R. H., Bernstein, L., Ross, R. K., Judd, H. L., & Henderson, B. E. (1987). Hyperemesis gravidarum in relation to estradiol levels, pregnancy outcome, and other maternal factors: A seroepidemiologic study. American Journal of Obstetrics and Gynecology, 156(5), 1137–1141. [DOI:10.1016/0002-9378(87)90126-8]
Derra, C. (1981). Hormonprofile unter Östrogen- und Antiandrogentherapie bei Patienten mit Prostatakarzinom: Östradiolundecylat versus Cyproteronacetat. [Hormone Profiles under Estrogen and Antiandrogen Therapy in Patients with Prostate Cancer: Estradiol Undecylate versus Cyproterone Acetate.] (Doctoral dissertation, University of Mainz.) [Google Scholar] [WorldCat] [PDF] [Translation]
Dittrich, R., Binder, H., Cupisti, S., Hoffmann, I., Beckmann, M., & Mueller, A. (2005). Endocrine Treatment of Male-to-Female Transsexuals Using Gonadotropin-Releasing Hormone Agonist. Experimental and Clinical Endocrinology & Diabetes, 113(10), 586–592. [DOI:10.1055/s-2005-865900]
Dunn, J. F., Nisula, B. C., & Rodbard, D. (1981). Transport of Steroid Hormones: Binding of 21 Endogenous Steroids to Both Testosterone-Binding Globulin and Corticosteroid-Binding Globulin in Human Plasma. The Journal of Clinical Endocrinology & Metabolism, 53(1), 58–68. [DOI:10.1210/jcem-53-1-58]
Fåhraeus, L., & Larsson-Cohn, U. (1982). Oestrogens, gonadotrophins and SHBG during oral and cutaneous administration of oestradiol-17β to menopausal women. Acta Endocrinologica, 101(4), 592–596. [DOI:10.1530/acta.0.1010592]
Fanelli, F., Gambineri, A., Belluomo, I., Repaci, A., Di Lallo, V. D., Di Dalmazi, G., Mezzullo, M., Prontera, O., Cuomo, G., Zanotti, L., Paccapelo, A., Morselli-Labate, A. M., Pagotto, U., & Pasquali, R. (2013). Androgen Profiling by Liquid Chromatography–Tandem Mass Spectrometry (LC-MS/MS) in Healthy Normal-Weight Ovulatory and Anovulatory Late Adolescent and Young Women. The Journal of Clinical Endocrinology & Metabolism, 98(7), 3058–3067. [DOI:10.1210/jc.2013-1381]
Freymann, E., Hubl, W., Büchner, M., & Belleée, H. (1977). Eine spezifische, radioimmunologische Bestimmung des Plasmaöstradiols ohne Chromatographie im Zyklus und in der Schwangerschaft und die Bestimmung des freien, nichtproteingebundenen Anteils mittels Dialyse. [A specific radioimmunologi determination of plasma estradiol without chromatography during the cycle and in pregnancy and determination of the free non-protein-bound fraction using dialysis.] Zentralblatt für Gynäkologie, 99(6), 321–329. [Google Scholar 1] [Google Scholar 2] [PubMed] [PDF]
Freymann, E., Hubl, W., Büchner, M., & Rohde, W. (1977). Plasma levels of apparent free estradiol during pregnancy. Endokrinologie, 69(2), 269–271. [Google Scholar] [PubMed] [PDF]
Gibney, J., Johannsson, G., Leung, K., & Ho, K. K. (2005). Comparison of the Metabolic Effects of Raloxifene and Oral Estrogen in Postmenopausal and Growth Hormone-Deficient Women. The Journal of Clinical Endocrinology & Metabolism, 90(7), 3897–3903. [DOI:10.1210/jc.2005-0173]
Goldman, A. L., Bhasin, S., Wu, F. C., Krishna, M., Matsumoto, A. M., & Jasuja, R. (2017). A Reappraisal of Testosterone’s Binding in Circulation: Physiological and Clinical Implications. Endocrine Reviews, 38(4), 302–324. [DOI:10.1210/er.2017-00025]
Graham, C. A., Bancroft, J., Doll, H. A., Greco, T., & Tanner, A. (2007). Does oral contraceptive-induced reduction in free testosterone adversely affect the sexuality or mood of women? Psychoneuroendocrinology, 32(3), 246–255. [DOI:10.1016/j.psyneuen.2006.12.011]
Guthrie, J., Dennerstein, L., Taffe, J., Lehert, P., & Burger, H. (2004). The menopausal transition: a 9-year prospective population-based study. The Melbourne Women’s Midlife Health Project. Climacteric, 7(4), 375–389. [DOI:10.1080/13697130400012163]
Hammond, G. L., Nisker, J. A., Jones, L. A., & Siiteri, P. K. (1980). Estimation of the percentage of free steroid in undiluted serum by centrifugal ultrafiltration-dialysis. Journal of Biological Chemistry, 255(11), 5023–5026. [DOI:10.1016/s0021-9258(19)70742-x]
Hammond, G. L. (2016). Plasma steroid-binding proteins: primary gatekeepers of steroid hormone action. Journal of Endocrinology, 230(1), R13–R25. [DOI:10.1530/joe-16-0070]
Hammond, G. L. (2017). Sex Hormone-Binding Globulin and the Metabolic Syndrome. In Winters, S. J., & Huhtaniemi, I. T. (Eds.). Male Hypogonadism: Basic, Clinical and Therapeutic Principles (pp. 305–324). Cham: Springer International Publishing. [DOI:10.1007/978-3-319-53298-1_15]
Handelsman, D. J. (2017). Free Testosterone: Pumping up the Tires or Ending the Free Ride? Endocrine Reviews, 38(4), 297–301. [DOI:10.1210/er.2017-00171]
Heidrich, A., Schleyer, M., Spingler, H., Albert, P., Knoche, M., Fritze, J., & Lanczik, M. (1994). Postpartum blues: Relationship between not-protein bound steroid hormones in plasma and postpartum mood changes. Journal of Affective Disorders, 30(2), 93–98. [DOI:10.1016/0165-0327(94)90036-1]
Heubner, A., Brockerhoff, P., Kreienberg, R., Grill, H., Rathgen, G., & Pollow, K. (1987). The influence of various dosages of megestrol acetate on SHBG, CBG and lipoprotein patterns. Journal of Steroid Biochemistry, 28(Suppl 1), 214S–214S (abstract no. 6). [DOI:10.1016/0022-4731(87)91680-3]
Hogeveen, K. N., Cousin, P., Pugeat, M., Dewailly, D., Soudan, B., & Hammond, G. L. (2002). Human sex hormone-binding globulin variants associated with hyperandrogenism and ovarian dysfunction. The Journal of Clinical Investigation, 109(7), 973–981. [DOI:10.1172/JCI14060]
Keevil, B. G., & Adaway, J. (2019). Assessment of free testosterone concentration. The Journal of Steroid Biochemistry and Molecular Biology, 190, 207–211. [DOI:10.1016/j.jsbmb.2019.04.008]
Kerlan, V., Nahoul, K., Martelot, M., & Bercovici, J. (1994). Longitudinal study of maternal plasma bioavailable testosterone and androstanediol glucuronide levels during pregnancy. Clinical Endocrinology, 40(2), 263–267. [DOI:10.1111/j.1365-2265.1994.tb02478.x]
Krause, A., Sinnecker, G., Hiort, O., Thamm, B., & Hoepffner, W. (2004). Applicability of the SHBG Androgen Sensitivity Test in the Differential Diagnosis of 46,XY Gonadal Dysgenesis, True Hermaphroditism, and Androgen Insensitivity Syndrome. Experimental and Clinical Endocrinology & Diabetes, 112(5), 236–240. [DOI:10.1055/s-2004-817969]
Kronawitter, D., Gooren, L. J., Zollver, H., Oppelt, P. G., Beckmann, M. W., Dittrich, R., & Mueller, A. (2009). Effects of transdermal testosterone or oral dydrogesterone on hypoactive sexual desire disorder in transsexual women: results of a pilot study. European Journal of Endocrinology, 161(2), 363–368. [DOI:10.1530/eje-09-0265] [Table]
Kuhl, H. (1997). Metabolische Effekte der Östrogene und Gestagene. [Metabolic Effects of Estrogens and Progestogens.] Der Gynäkologe, 30(4), 357–369. [DOI:10.1007/pl00003042]
Kuhl, H. (1998). Adverse effects of estrogen treatment: natural vs. synthetic estrogens. In Lippert, T. H., Mueck, A. O., & Ginsburg, J. (Eds.). Sex Steroids and the Cardiovascular System: The Proceedings of the 1st Interdisciplinary Workshop, Tuebingen, Germany, October 1996. Parthenon Publishing Group, New York, London (pp. 201–210). London/New York: Parthenon. [Google Scholar] [Google Books] [PDF]
Kuhl, H. (1999). Hormonal contraception. In Oettel, M., & Schillinger, E. (Eds.). Estrogens and Antiestrogens II: Pharmacology and Clinical Application of Estrogens and Antiestrogen (Handbook of Experimental Pharmacology, Volume 135, Part 2) (pp. 363–407). Berlin/Heidelberg: Springer. [DOI:10.1007/978-3-642-60107-1_18] [PDF]
Kuhl, H. (2005). Pharmacology of Estrogens and Progestogens: Influence of Different Routes of Administration. Climacteric, 8(Suppl 1), 3–63. [DOI:10.1080/13697130500148875] [PDF]
Lundgren, S., Lønning, P., Utaaker, E., Aakvaag, A., & Kvinnsland, S. (1990). Influence of progestins on serum hormone levels in postmenopausal women with advanced breast cancer—I. General findings. Journal of Steroid Biochemistry, 36(1–2), 99–104. [DOI:10.1016/0022-4731(90)90118-c]
Lundgren, S., & Lønning, P. (1990). Influence of progestins on serum hormone levels in postmenopausal women with advanced breast cancer—II. A differential effect of megestrol acetate and medroxyprogesterone acetate on serum estrone sulfate and sex hormone binding globulin. Journal of Steroid Biochemistry, 36(1–2), 105–109. [DOI:10.1016/0022-4731(90)90119-d]
Mazer, N. A. (2009). A novel spreadsheet method for calculating the free serum concentrations of testosterone, dihydrotestosterone, estradiol, estrone and cortisol: With illustrative examples from male and female populations. Steroids, 74(6), 512–519. [DOI:10.1016/j.steroids.2009.01.008] [Spreadsheet]
McClamrock, H. D. (2007). Pregnancy-Related Androgen Excess. In Azziz, R., Nestler, J. E., & Dewailly, D. (Eds.). Androgen Excess Disorders in Women: Polycystic Ovary Syndrome and Other Disorders, 2nd Edition (Contemporary Endocrinology) (pp. 107–119). Totowa, New Jersey: Humana Press. [Google Books] [DOI:10.1007/978-1-59745-179-6_9]
Mean, F., Pellaton, M., & Magrini, G. (1977). Study on the binding of dihydrotestosterone, testosterone and oestradiol with sex hormone binding globulin. Clinica Chimica Acta, 80(1), 171–180. [DOI:10.1016/0009-8981(77)90276-5]
Meyer, G., Mayer, M., Mondorf, A., Flügel, A. K., Herrmann, E., & Bojunga, J. (2020). Safety and rapid efficacy of guideline-based gender-affirming hormone therapy: an analysis of 388 individuals diagnosed with gender dysphoria. European Journal of Endocrinology, 182(2), 149–156. [DOI:10.1530/eje-19-0463] [PDF]
Moore, J. W., & Bulbrook, R. D. (1988). The epidemiology and function of sex hormone-binding globulin. Oxford Reviews of Reproductive Biology, 10, 180–236. [Google Scholar] [PubMed] [PDF]
Mueller, A., Dittrich, R., Binder, H., Kuehnel, W., Maltaris, T., Hoffmann, I., & Beckmann, M. W. (2005). High dose estrogen treatment increases bone mineral density in male-to-female transsexuals receiving gonadotropin-releasing hormone agonist in the absence of testosterone. European Journal of Endocrinology, 153(1), 107–113. [DOI:10.1530/eje.1.01943]
Mueller, A., Binder, H., Cupisti, S., Hoffmann, I., Beckmann, M., & Dittrich, R. (2006). Effects on the Male Endocrine System of Long-term Treatment with Gonadotropin-releasing Hormone Agonists and Estrogens in Male-to-Female Transsexuals. Hormone and Metabolic Research, 38(3), 183–187. [DOI:10.1055/s-2006-925198]
Mueller, A., Zollver, H., Kronawitter, D., Oppelt, P. G., Claassen, T., Hoffmann, I., Beckmann, M. W., & Dittrich, R. (2011). Body composition and bone mineral density in male-to-female transsexuals during cross-sex hormone therapy using gonadotrophin-releasing hormone agonist. Experimental and Clinical Endocrinology & Diabetes, 119(2), 95–100. [DOI:10.1055/s-0030-1255074] [Table]
Nachtigall, L. E., Raju, U., Banerjee, S., Wan, L., & Levitz, M. (2000). Serum Estradiol-Binding Profiles in Postmenopausal Women Undergoing Three Common Estrogen Replacement Therapies. Menopause, 7(4), 243–250. [DOI:10.1097/00042192-200007040-00006]
Nakamoto, J. (2016). Endocrine Testing. In Jameson, J. L., & De Groot, L. J. (Eds.). Endocrinology: Adult and Pediatric, 7th Edition (pp. 2655–2688.e1). Philadelphia: Saunders/Elsevier. [Google Books] [DOI:10.1016/B978-0-323-18907-1.00154-2]
Nguyen, T. D. T., Dolomie-Fagour, L., Georges, A., & Corcuff, J. B. (2008). Dosage des stéroïdes sexuels sériques: quelle place pour l’estradiol biodisponible? [What about bioavailable estradiol?] Annales de Biologie Clinique, 66(5), 493–497. [DOI:10.1684/abc.2008.0259]
Nilsson, B., Holst, J., & Schoultz, B. (1984). Serum levels of unbound 17β-oestradiol during oral and percutaneous postmenopausal replacement therapy. British Journal of Obstetrics and Gynaecology, 91(10), 1031–1036. [DOI:10.1111/j.1471-0528.1984.tb03683.x]
Nolan, B. J., & Cheung, A. S. (2021). Relationship Between Serum Estradiol Concentrations and Clinical Outcomes in Transgender Individuals Undergoing Feminizing Hormone Therapy: A Narrative Review. Transgender Health, 6(3), 125–131. [DOI:10.1089/trgh.2020.0077]
O’Leary, P., Boyne, P., Flett, P., Beilby, J., & James, I. (1991). Longitudinal assessment of changes in reproductive hormones during normal pregnancy. Clinical Chemistry, 37(5), 667–672. [DOI:10.1093/clinchem/37.5.667]
Odlind, V., Milsom, I., Persson, I., & Victor, A. (2002). Can changes in sex hormone binding globulin predict the risk of venous thromboembolism with combined oral contraceptive pills? Acta Obstetricia et Gynecologica Scandinavica, 81(6), 482–490. [DOI:10.1034/j.1600-0412.2002.810603.x]
Ojasoo, T., & Raynaud, J. P. (1978). Unique steroid congeners for receptor studies. Cancer Research, 38(11 Part 2), 4186–4198. [Google Scholar] [PubMed] [URL]
Pande, P., Fleck, S. C., Twaddle, N. C., Churchwell, M. I., Doerge, D. R., & Teeguarden, J. G. (2019). Comparative estrogenicity of endogenous, environmental and dietary estrogens in pregnant women II: Total estrogenicity calculations accounting for competitive protein and receptor binding and potency. Food and Chemical Toxicology, 125, 341–353. [DOI:10.1016/j.fct.2018.12.013]
Pardridge, W. M. (1988). Selective delivery of sex steroid hormones to tissues by albumin and by sex hormone-binding globulin. Oxford Reviews of Reproductive Biology, 10, 237–292. [Google Scholar] [PubMed] [PDF]
Perry, L., Wathen, N., & Chard, T. (1987). Saliva Levels of Oestradiol and Progesterone in Relation to Non-Protein-Bound Concentrations in Blood During Late Pregnancy. Hormone and Metabolic Research, 19(9), 444–447. [DOI:10.1055/s-2007-1011848]
Plymate, S. R., Moore, D. E., Cheng, C. Y., Bardin, C. W., Southworth, M. B., & Levinski, M. J. (1985). Sex Hormone-Binding Globulin Changes during the Menstrual Cycle. The Journal of Clinical Endocrinology & Metabolism, 61(5), 993–996. [DOI:10.1210/jcem-61-5-993]
Pugeat, M. M., Dunn, J. F., & Nisula, B. C. (1981). Transport of Steroid Hormones: Interaction of 70 Drugs with Testosterone-Binding Globulin and Corticosteroid-Binding Globulin in Human Plasma. The Journal of Clinical Endocrinology & Metabolism, 53(1), 69–75. [DOI:10.1210/jcem-53-1-69]
Rezaii, T., Gustafsson, T. P., Axelson, M., Zamani, L., Ernberg, M., Hirschberg, A. L., & Carlström, K. A. (2017). Circulating androgens and SHBG during the normal menstrual cycle in two ethnic populations. Scandinavian Journal of Clinical and Laboratory Investigation, 77(3), 184–189. [DOI:10.1080/00365513.2017.1286685]
Ropponen, A., Aittomäki, K., Vihma, V., Tikkanen, M. J., & Ylikorkala, O. (2005). Effects of Oral and Transdermal Estradiol Administration on Levels of Sex Hormone-Binding Globulin in Postmenopausal Women with and without a History of Intrahepatic Cholestasis of Pregnancy. The Journal of Clinical Endocrinology & Metabolism, 90(6), 3431–3434. [DOI:10.1210/jc.2005-0352]
Rosner, W. (2015). Free estradiol and sex hormone-binding globulin. Steroids, 99, 113–116. [DOI:10.1016/j.steroids.2014.08.005]
Rothman, M. S., Carlson, N. E., Xu, M., Wang, C., Swerdloff, R., Lee, P., Goh, V. H., Ridgway, E. C., & Wierman, M. E. (2011). Reexamination of testosterone, dihydrotestosterone, estradiol and estrone levels across the menstrual cycle and in postmenopausal women measured by liquid chromatography–tandem mass spectrometry. Steroids, 76(1–2), 177–182. [DOI:10.1016/j.steroids.2010.10.010]
Rubinow, D. R., Schmidt, P. J., Roca, C. A., & Daly, R. C. (2002). Gonadal Hormones and Behavior in Women: Concentrations versus Context. In Pfaff, D. W., Arnold, A. P., Etgen, A. M., Fahrbach, S. E., & Rubin, R. T. (Eds.). Hormones, Brain and Behavior, Volume 5 (pp. 37–73). Amsterdam: Academic Press. [Google Books] [DOI:10.1016/B978-012532104-4/50086-X]
Ruokonen, A., Alén, M., Bolton, N., & Vihko, R. (1985). Response of serum testosterone and its precursor steroids, SHBG and CBG to anabolic steroid and testosterone self-administration in man. Journal of Steroid Biochemistry, 23(1), 33–38. [DOI:10.1016/0022-4731(85)90257-2]
Schijf, C. P., van der Mooren, M. J., Doesburg, W. H., Thomas, C. M., & Rolland, R. (1993). Differences in serum lipids, lipoproteins, sex hormone binding globulin and testosterone between the follicular and the luteal phase of the menstrual cycle. Acta Endocrinologica, 129(2), 130–133. [DOI:10.1530/acta.0.1290130]
Schuijt, M. P., Sweep, C. G., van der Steen, R., Olthaar, A. J., Stikkelbroeck, N. M., Ross, H. A., & van Herwaarden, A. E. (2019). Validity of free testosterone calculation in pregnant women. Endocrine Connections, 8(6), 672–679. [DOI:10.1530/ec-19-0110]
Shifren, J. L., Desindes, S., McIlwain, M., Doros, G., & Mazer, N. A. (2007). A randomized, open-label, crossover study comparing the effects of oral versus transdermal estrogen therapy on serum androgens, thyroid hormones, and adrenal hormones in naturally menopausal women. Menopause, 14(6), 985–994. [DOI:10.1097/gme.0b013e31803867a]
Shifren, J. L., Rifai, N., Desindes, S., McIlwain, M., Doros, G., & Mazer, N. A. (2008). A Comparison of the Short-Term Effects of Oral Conjugated Equine Estrogens Versus Transdermal Estradiol on C-Reactive Protein, Other Serum Markers of Inflammation, and Other Hepatic Proteins in Naturally Menopausal Women. The Journal of Clinical Endocrinology & Metabolism, 93(5), 1702–1710. [DOI:10.1210/jc.2007-2193]
Smith, K., Galazi, M., Openshaw, M. R., Wilson, P., Sarker, S. J., O’Brien, N., Alifrangis, C., Stebbing, J., & Shamash, J. (2020). The Use of Transdermal Estrogen in Castrate-resistant, Steroid-refractory Prostate Cancer. Clinical Genitourinary Cancer, 18(3), e217–e223. [DOI:10.1016/j.clgc.2019.09.019]
Stege, R., Carlström, K., Collste, L., Eriksson, A., Henriksson, P., & Pousette, A. (1988). Single drug polyestradiol phosphate therapy in prostatic cancer. American Journal of Clinical Oncology, 11(Suppl 2), S101–S103. [DOI:10.1097/00000421-198801102-00024] [PDF]
Steingold, K. A., Pardridge, W. M., Judd, H. L., & Chaudhuri, G. (1987). The effects of membrane permeability and binding by human serum proteins on steroid influx into the rabbit uterus. American Journal of Obstetrics and Gynecology, 157(6), 1543–1549. [DOI:10.1016/s0002-9378(87)80260-0]
Strauss, J. F., & FitzGerald, G. A. (2019). Steroid Hormones and Other Lipid Molecules Involved in Human Reproduction. In Strauss, J. F., & Barbieri, R. L. (Eds.). Yen and Jaffe’s Reproductive Endocrinology: Physiology, Pathophysiology, and Clinical Management, 8th Edition (pp. 75–114.e7). Philadelphia: Elsevier. [Google Books] [DOI:10.1016/b978-0-323-47912-7.00004-4]
Troisi, R., Potischman, N., Roberts, J. M., Harger, G., Markovic, N., Cole, B., Lykins, D., Siiteri, P., & Hoover, R. N. (2003). Correlation of serum hormone concentrations in maternal and umbilical cord samples. Cancer Epidemiology, Biomarkers & Prevention, 12(5), 452–456. [Google Scholar] [PubMed] [URL]
Tulchinsky, D., & Chopra, I. J. (1973). Competitive Ligand-Binding Assay for Measurement of Sex Hormone-Binding Globulin (SHBG). The Journal of Clinical Endocrinology & Metabolism, 37(6), 873–881. [DOI:10.1210/jcem-37-6-873]
von Schoultz, B., Carlström, K., Collste, L., Eriksson, A., Henriksson, P., Pousette, Å., & Stege, R. (1989). Estrogen therapy and liver function—metabolic effects of oral and parenteral administration. The Prostate, 14(4), 389–395. [DOI:10.1002/pros.2990140410]
Zimmerman, Y., Eijkemans, M. J., Coelingh Bennink, H. J., Blankenstein, M. A., & Fauser, B. C. (2013). The effect of combined oral contraception on testosterone levels in healthy women: a systematic review and meta-analysis. Human Reproduction Update, 20(1), 76–105. [DOI:10.1093/humupd/dmt038]
\ No newline at end of file
+The Interactions of Sex Hormones with Sex Hormone-Binding Globulin and Relevance for Transfeminine Hormone Therapy - Transfeminine Science
The Interactions of Sex Hormones with Sex Hormone-Binding Globulin and Relevance for Transfeminine Hormone Therapy
By Aly | First published July 10, 2020 | Last modified March 25, 2023
Abstract / TL;DR
Sex hormones such as testosterone and estradiol bind to blood proteins like albumin and SHBG. This limits their biological activity by reducing their free fractions. Androgens decrease SHBG production while estrogens increase SHBG production. Hence, testosterone and estradiol can influence their own free fractions. Due to robust inactivation in the liver, testosterone and estradiol have relatively small influences on SHBG levels under normal physiological circumstances. At very high levels however, they can considerably influence SHBG levels. During pregnancy, when there are massive increases in estradiol levels (e.g., 100-fold), a maximal 5- to 10-fold elevation in SHBG levels occurs. Although large increases in SHBG levels can strongly limit the biological activity of testosterone, the situation with estradiol is different. In late pregnancy, the percentage of estradiol that is free appears to be decreased only to around 60% of that of non-pregnancy. Earlier in pregnancy, when estradiol levels are lower, the free fractions of estradiol are reduced to a lesser extent. At typical therapeutic levels of estradiol in transfeminine hormone therapy (<200 pg/mL), the limiting influence of SHBG on free estradiol is minimal. Oral estradiol has a greater influence on SHBG production than non-oral estradiol and may be a different case however. In any case, consequent lesser activity of oral estradiol is only theoretical, and available clinical studies so far haven’t reported important therapeutic differences relative to non-oral estradiol. Although SHBG may reduce free estradiol fractions in some contexts, only relatively low estradiol levels (<50 pg/mL) appear to be needed for maximal feminization and breast development in cisgender females and transfeminine people. In conclusion, the influence of SHBG on the effectiveness of estradiol isn’t something that should be a major source of concern in transfeminine hormone therapy.
Binding of Sex Hormones to Blood Proteins
Sex hormones bind to proteins in the blood called plasma proteins. This is a phenomenon known as plasma protein binding. In the case of androgens and estrogens, the plasma proteins they bind to are mainly albumin and sex hormone-binding globulin (SHBG). Plasma protein binding serves to prevent sex hormones from interacting with their target cells and hence from binding to and activating their receptors (Hammond, 2016). This is because plasma proteins are too large and lipid-insoluble to cross the lipid-rich cell membrane. As a result, they’re unable to diffuse through capillaries to exit the circulation and enter into tissues or to be taken up into cells. When the sex hormone is bound to plasma protein, it can’t reach target cells either. Hence, plasma protein binding limits the biological activity of sex hormones (Hammond, 2016). Binding to plasma proteins also serves to extend the biological half-lives of sex hormones. This is because protein-bound sex hormone is likewise unavailable for metabolism and elimination, processes that depend on cellular uptake.
There is only a single sex hormone binding site per molecule of SHBG (Moore & Bulbrook, 1988), whereas albumin has six binding sites for different substrates (Pardridge, 1988). Androgens and estradiol have high affinity for SHBG (nM) and low affinity for albumin (μM) (Moore & Bulbrook, 1988; Hammond, 2016). However, albumin levels are several orders of magnitude higher than SHBG levels (μM vs. nM), so this serves to balance out the fractions of sex hormone bound to each protein (Hammond, 2016). Androgens have higher affinities for SHBG than do estradiol or other estrogens. Estradiol has only about 10 to 20% of the affinity of dihydrotestosterone (DHT) and 33 to 50% of the affinity of testosterone for SHBG (Anderson, 1974; Ojasoo & Raynaud, 1978; Pugeat, Dunn, Nisula, 1981). As such, testosterone and DHT bind more strongly to SHBG than does estradiol.
The vast majority of sex hormone content in the blood is bound to plasma proteins; at any given time more than 97% of the testosterone, estradiol, and progesterone in the blood is plasma protein-bound (Strauss & FitzGerald, 2019). The fraction of sex hormone that isn’t bound to plasma proteins is known as the free or unbound fraction. This is the fraction that is available for diffusion into cells and hence is considered to be biologically active (Hammond, 2016). Total levels refer to both free/unbound and bound hormone. Bioavailable levels include both albumin-bound and free hormone levels. Due to their relatively weak affinity for albumin, sex hormones bound to albumin may to some extent be biologically active—hence the “bioavailable” descriptor (Nguyen et al., 2008). However, more research is needed to fully elucidate the biological activity of albumin-bound sex hormone fractions.
The relative calculated free and bound percentages of estradiol, testosterone, and DHT to albumin, SHBG, and another plasma protein known as corticosteroid-binding globulin (CBG) (only binds small fractions of the androgens and has no binding to estradiol) are shown in the table below.
Free sex hormone levels and percentages are often calculated from levels of total sex hormone, albumin, SHBG, and CBG with validated mathematical models constructed from data of published studies. This is because free sex hormone levels are usually very low (pM range) and are difficult to measure with routine blood testing methods. While generally in the vicinity of the true values, calculated results may not always be fully accurate (Rosner, 2015; Goldman et al., 2017; Handelsman, 2017; Keevil & Adaway, 2019). As such, measured levels, when feasible, are preferable.
Testosterone, DHT, and estradiol are strongly inactivated by the liver and have relatively weak effects in this part of the body under normal circumstances. As a result, they have much less relative impact on SHBG production than do synthetic hormonal agents. Accordingly, SHBG levels change only slightly over the course of the menstrual cycle in women despite substantial fluctuations in estradiol levels (Freymann et al., 1977b; Plymate et al., 1985; Schijf et al., 1993; Braunstein et al., 2011; Rothman et al., 2011; Fanelli et al., 2013; Rezaii et al., 2017). In one study, SHBG levels increased by about 6 to 13% (+2.9–5.3 nmol/L) going from the follicular phase to the luteal phase of the cycle (Braunstein et al., 2011). There is additionally only a small decrease in SHBG levels attributable to the sharp decline in estradiol with menopause (Burger et al., 2000; Guthrie et al., 2004). Nonetheless, estradiol therapy can more considerably influence the production of SHBG and other liver proteins as well under specific conditions (Kuhl, 1998). This is due to 1) use of oral estradiol, which because of the first pass through the liver has a greater impact on estrogen-sensitive liver synthesis than non-oral routes (Kuhl, 2005); and 2) use of high estradiol doses, for instance typical injectable doses. The table below shows SHBG increases from various studies with different estrogen routes, doses, and types.
Table 2: Relative increases in SHBG levels with some different estrogenic exposures:
a Estimated typical estradiol levels from various sources (e.g., Aly, 2020; Wiki). b Due to differences in molecular weight, EV has about 75% of the amount of estradiol as regular estradiol. Hence, 6 mg/day EV is approximately equivalent to 4.5 mg/day E2.
The influence of estradiol on SHBG levels is most relevant to pregnancy, when estradiol levels increase to far higher levels than usual. In late pregnancy, estradiol levels are generally around 15,000 to 25,000 pg/mL on average (Graphs; Troisi et al., 2003; Adamcová et al., 2018). These estradiol levels are on the order of 100-fold higher than normal menstrual cycle levels. In parallel with the massive increases in estradiol levels, SHBG levels increase by about 5- to 10-fold by late pregnancy (Anderson, 1974; Hammond, 2017). The dose–response curve of estrogens on SHBG production shows saturation, with most of the increase in SHBG levels happening at lower estradiol levels as well as limits to how much SHBG levels can be increased (Mean, Pellaton, & Magrini, 1977; O’Leary et al., 1991; Kerlan et al., 1994; Kuhl, 1999). The graphs below show SHBG levels throughout pregnancy.
Figure 1: SHBG and total estradiol levels during pregnancy in women (O’Leary et al., 1991). The lines are the mean and/or 95th percentile levels while the points are individual measurements.
Figure 2: Total sex hormone and SHBG levels during pregnancy in women (Kerlan et al., 1994).
Effects of SHBG Increase on Free Sex Hormone Levels
Changes in SHBG levels result in changes in SHBG-bound and free sex hormone levels. Aside from DHT, estradiol and testosterone are the hormones of the greatest interest in this regard.
SHBG Increase and Free Testosterone
EE-containing birth control pills, with their 4-fold increase in SHBG levels, substantially decrease the free percentage of testosterone (Graham et al., 2007; Zimmerman et al., 2014). In one study, an EE-containing birth control pill decreased the free testosterone fraction from 2.45% to 0.78% (a 3.2-fold decrease or to 32% of baseline) (Graham et al., 2007). Due to concomitant suppression of testosterone production and hence reduced total testosterone levels, free testosterone levels decreased from 0.89 pg/mL to 0.18 pg/mL (a 5-fold decrease, to 20% of baseline) (Graham et al., 2007). The influence of EE on SHBG levels contributes significantly to the antiandrogenic effects of EE-containing birth control pills, which are taken advantage of therapeutically to treat acne and hirsutism in women.
During pregnancy, testosterone levels increase to as much as 150 ng/dL (around 5-fold higher than non-pregnancy levels) (McClamrock, 2007). The increase in SHBG production during pregnancy serves an important function in that the higher SHBG levels neutralize the biological activity of the increased testosterone levels (Hammond, 2017). In one study, the free testosterone fraction was 6-fold lower in late pregnancy than in non-pregnant women (0.23% vs. 1.36%—or to 17% of non-pregnancy) (Dunn, Nisula, & Rodbard, 1981). Hence, despite substantial increases in total testosterone levels during pregnancy, free testosterone levels and by extension androgenic action in the body change minimally (Barini, Liberale, & Menini, 1993; Schuijt et al., 2019). A case report of marked hyperandrogenism due to severe SHBG deficiency in a pregnant woman evidences the role of SHBG in limiting the androgenic actions of testosterone during this time (Hogeveen et al., 2002; Hammond, 2017).
SHBG Increase and Free Estradiol
Endogenous and Non-Oral Estradiol
The research indicates that increases in SHBG levels and by extension decreases in the free estradiol fraction are minimal with physiological levels of estradiol (e.g., <200 pg/mL). This is the case whether the estradiol is endogenous or exogenous in origin—so long as it is taken non-orally. Such conclusions are based on both calculated and measured studies of free estradiol (e.g., Freymann et al., 1977b).
Increases in SHBG levels and decreases in the free estradiol fraction become more significant with supraphysiological levels of estradiol however, for instance during pregnancy and with very-high-dose estradiol therapy. Studies on changes in free estradiol with high doses of estradiol are few. This is especially true in the case of measured as opposed to calculated free estradiol. In any case, one can look at pregnancy to gain insight on the question of free estradiol with high estradiol levels. Moreover, due to the very high estradiol levels in pregnancy, free estradiol is more amenable to measurement during this time. Accordingly, multiple studies of measured free estradiol in pregnancy are available.
Although free estradiol percentages during pregnancy certainly decrease, the increases in estradiol are far from neutralized by SHBG. Hence, the situation with free estradiol in pregnancy is very different from that of testosterone. This is illustrated in the following excerpt (Rubinow et al., 2002):
Pregnancy is accompanied by a slow but sustained rise in the plasma levels of many steroid and peptide hormones and is followed by a precipitous drop in their levels over the first few days after delivery. By the third trimester of pregnancy, plasma progesterone levels average approximately 150 ng/ml and estradiol levels range from 10 to 15 ng/ml. These amounts represent a 10- and 50-fold increase, respectively, of maximum menstrual cycle levels (Tulchinsky et al., 1972). Although only a small fraction of these steroids are unbound, the amount of “free” (and thus biologically active) progesterone and estrogen also undergo similarly large increases during pregnancy (Heidrich et al., 1994).
In the study by Heidrich and colleagues cited in the excerpt, total estradiol levels at the time of delivery were 21,500 pg/mL and measured free estradiol levels were 232 pg/mL, with a resultant free estradiol fraction of 1.08% (Heidrich et al., 1994). For context, the free estradiol percentage in non-pregnant women ranges from 1.5 to 2.1% with RIA, while actual free estradiol levels are 0.30 to 4.1 pg/mL with RIA and 0.40 to 5.9 pg/mL with LC–MS/MS (Nakamoto, 2016). Hence, in this study free estradiol levels in late pregnancy were around 50-fold higher than maximal non-pregnancy levels.
Due to variable methodology, the findings of a single study may not be representative. As such, the table below provides measured free estradiol percentages in late pregnancy from several studies.
Table 3: Measured free estradiol percentages in late pregnancy (mean ± SD) (Perry et al., 1987):
As can be seen in the table, the free estradiol fraction in late pregnancy ranges from about 0.7 to 1.5%. Results for the free estradiol fraction from studies using calculated free estradiol levels in late pregnancy rather than measured levels are similar to measured findings, although sometimes a bit lower in comparison (e.g., 0.5%) (Dunn, Nisula, & Rodbard, 1981; Campino et al., 2001). The measured free estradiol percentage in late pregnancy can be cautiously compared to the fraction of 1.5 to 2.1% in non-pregnant women. Using middle values from these ranges, the free estradiol fraction in late pregnancy may be somewhere around 60% of that of non-pregnancy. This estimate is quite close to the actual findings of a study, which observed a decrease in the measured free estradiol percentage to 55% of that of non-pregnancy (Freymann et al., 1977a; Freymann et al., 1977b).
In contrast to estradiol, the free percentages of estrone and estriol are not different in late pregnancy when compared to non-pregnancy (Tulchinsky & Chopra, 1973; Steingold et al., 1987). This is attributable to the much lower affinities of estrone and estriol for SHBG relative to estradiol (Kuhl, 2005).
Studies have also assessed free estradiol fractions earlier in pregnancy, which might in theory differ from late pregnancy. The results of a study that measured free estradiol throughout pregnancy are shown in the table below (Freymann et al., 1977a; Freymann et al., 1977b).
In similar studies by another group of researchers, free estradiol fractions were measured in earlier pregnancy (weeks 7–16) and were found to be lower than those obtained by Freymann and colleagues (Bernstein et al., 1986; Depue et al., 1987; Bernstein et al., 1988). The free estradiol percentage was about 0.9 or 1.0% at 10 weeks and about 0.7% at 12 weeks (Bernstein et al., 1986; Depue et al., 1987; Bernstein et al., 1988). Hence, as with the results of Freymann and colleagues, the free estradiol fraction decreased as pregnancy progressed. The figure below provides a visualization of the findings.
Figure 3: Changes in total and free estradiol levels (pg/mL), free estradiol fraction (%), and SHBG binding capacity (μg/dL) during weeks 7 to 16 of pregnancy in women (Bernstein et al., 1986).
Free estradiol during pregnancy can also be calculated using total estradiol levels and SHBG levels. I roughly calculated the free estradiol fraction during pregnancy using the data from O’Leary et al. (1991) and a published calculator spreadsheet by Mazer (2009) (Aly, 2020). The results are shown below.
Figure 4: Average measured total estradiol and SHBG levels (O’Leary et al., 1991) and calculated free estradiol percentage (Mazer, 2009) throughout pregnancy in women. Another version of this graph scaled to only the first trimester of pregnancy (when estradiol levels are typically ≤2,000 pg/mL) is also provided (Graph).
The free estradiol fractions in the figure are merely rough estimations and hence should be given conservative consideration. In any case, they are similar to the findings of the available studies on measured free estradiol in earlier pregnancy just discussed—for instance in magnitude (relative to Bernstein et al.) and pattern of change throughout pregnancy (relative to both Bernstein et al. and Freymann et al.). As such, these calculated values offer a plausible and interesting model.
To summarize, there are profound increases in total estradiol levels and proportionally lower but still substantial increases in SHBG levels during pregnancy. In accordance with the marked increase in SHBG levels, the free estradiol fraction progressively decreases over the course of pregnancy. Studies are conflicting on the exact degrees to which free estradiol percentages decrease. In any case, the possibilities for the free estradiol fraction by late pregnancy range from about 0.5 to 1.5%. These figures can be compared to non-pregnancy free estradiol percentages of 1.5 to 2.1%. This may correspond to a maximal decrease in the free estradiol fraction in late pregnancy to around 60% of non-pregnancy. At the greatest extreme, the decrease may be to around 25% of non-pregnancy. Conversely, in earlier pregnancy, when estradiol levels are lower, free estradiol percentages are higher.
Despite the decreases in the free estradiol fraction during pregnancy, there are profound increases in free estradiol levels that parallel the massive increases in total estradiol. As such, the increase in estradiol levels during pregnancy markedly exceeds the limiting influences of the simultaneously elevated SHBG levels. For this reason, pregnancy is a profoundly hyperestrogenic state.
SHBG doesn’t impact estradiol like it does testosterone during pregnancy because the proportional increases in estradiol levels relative to SHBG levels are far greater in comparison and because of the relatively lower affinity of estradiol for SHBG. In general, it’s not possible for SHBG to limit the activity of estradiol in the way that it can with testosterone due to the inherent requirement for substantially increased SHBG production of much more highly increased estradiol levels.
Oral Estradiol
Oral estradiol may differ from non-oral estradiol when it comes to the issue of free estradiol. This is because oral estradiol undergoes a first pass that results in greater estradiol levels in the liver relative to the circulation. As a result, oral estradiol has disproportionate liver effects and increases SHBG levels to a proportionally greater extent than non-oral estradiol. Hence, the greater SHBG increases with oral estradiol may result in lower free estradiol fractions than with non-oral estradiol.
While this is probable, it is more difficult to determine the precise magnitudes of the differences between oral and non-oral estradiol in terms of free estradiol. Some data are available however. Clinical studies of low-dose oral estradiol in menopausal cisgender women have reported the limiting influence of the SHBG increase on calculated free estradiol to be modest (Nilsson, Holst, & von Schoultz, 1984; Nachtigall et al., 2000). Likewise, oral estradiol appears to have similar effectiveness for menopausal symptoms when compared to non-oral estradiol (Wiki; 2nd paragraph). Studies of higher doses of oral estradiol that provide data on SHBG or free estradiol levels are rare. In any case, a few studies by one group found that 6 mg/day oral estradiol valerate (a dose equivalent to approximately 4.5 mg/day oral estradiol) increased SHBG levels by about 2.5- to 3.0-fold in transgender women (Dittrich et al., 2005; Mueller et al., 2005; Mueller et al., 2006). Using the numbers from one of the studies for total estradiol and SHBG levels, it can be roughly calculated (Mazer, 2009) that the free estradiol fraction may have decreased from around 2.1% to 1.2% (a 43% reduction). Analogously, a study using oral conjugated estrogens (CEEs; Premarin) at a dose that increased SHBG levels by 2.3-fold reported that the calculated free estradiol percentage was 40% lower relative to an equivalent dose of transdermal estradiol (in terms of total estradiol levels) (Shifren et al., 2007). These findings suggest a non-trivial reduction in the free estradiol fraction with typical doses of oral estradiol in transfeminine people. Consequently, it’s possible that oral estradiol could be to a certain degree less potent at the same total estradiol levels relative to non-oral estradiol.
It’s important to be clear that it’s also not a certainty however. Levels of estrone are much higher with oral estradiol than with non-oral estradiol (~5-fold) (Kuhl, 2005), and estrone, although far less potent than estradiol, has significant intrinsic estrogenic activity similarly to estradiol (Kuhl, 2005). The degree to which estrone might add to the estrogenic activity of estradiol, if at all, is uncertain. In any case, it’s within the realm of possibility that estrone could contribute significantly to the estrogenic activity of oral estradiol (Pande et al., 2019). This additional estrogenic exposure could potentially serve to offset the impact of the higher SHBG levels and reduced free estradiol fractions that occur with oral estradiol. Further research is needed to evaluate such a possibility however. As another consideration, the higher SHBG levels with oral estradiol can be expected to reduce the free testosterone fraction in addition to that of estradiol (and to an even greater extent in comparison). This is important as testosterone suppression is a key therapeutic effect of estradiol in transfeminine people and the main justified reason for use of higher estradiol levels. Due to possibilities like these and the fact that free levels of hormones only theoretically represent their biological activity, it shouldn’t necessarily be assumed that oral estradiol is less potent or efficacious than non-oral estradiol. Only further clinical studies comparing oral estradiol to non-oral estradiol will be able to clarify this question.
Relevance for Transfeminine Hormone Therapy
Some have concerns that SHBG may substantially limit the effectiveness of estradiol and thereby hinder feminization and/or breast development. Some have even claimed that high levels of estradiol may be less effective than lower levels as a result of SHBG increases at higher levels. Before even touching on SHBG however, such notions are likely to be misguided. This is because low estradiol levels (<50 pg/mL) are known to be fully effective in terms of feminization and breast development. This is evidenced by normal and induced puberty in cisgender girls (Aly, 2020), as well as by the excellent secondary sexual development of women with complete androgen insensitivity syndrome (CAIS) (Aly, 2020; Wiki). No evidence exists at this time to indicate that higher estradiol levels are necessary or beneficial in terms of feminization or breast development (Nolan & Cheung, 2020). Available studies in fact suggest no relationship between estradiol levels and breast development in transfeminine people at typical therapeutic levels of estradiol (e.g., 50–200 pg/mL) (de Blok et al., 2017; Meyer et al., 2020; de Blok et al., 2020). This is in accordance with the concept of the maximal effect of estradiol on feminization and breast development being established at lower estradiol levels. Hence, besides the use of higher estradiol levels for testosterone suppression in transfeminine people, concerns about incomplete feminizing efficacy of estradiol consequent to inadequate estrogenic exposure have little basis.
If SHBG is nonetheless explored however, the research indicates that the role of SHBG in restricting free estradiol, and hence presumably the biological activity of estradiol, is only so considerable. Within physiological non-pregnancy ranges for estradiol (e.g., <200 pg/mL), changes in SHBG levels and free estradiol fractions due to endogenous or non-oral estradiol are minimal. Very high estradiol levels have greater influence on SHBG production than normal physiological levels however. During pregnancy, with the massive increases in estradiol and resultant 5- to 10-fold maximal elevation in SHBG levels, the free estradiol percentage may be decreased to around 60% of that of non-pregnancy. But actual free estradiol levels are nonetheless profoundly increased in pregnancy. Moreover, increases in SHBG levels and decreases in free estradiol fraction earlier in pregnancy are lower than in late pregnancy. Even with among the highest estradiol levels that would normally be encountered with non-oral estradiol therapy, the decreases in the free estradiol fraction due to SHBG are likely to be modest. The impact of such a reduction could easily be negated by a slightly greater estradiol dose.
While the preceding is applicable to non-oral estradiol, oral estradiol has a greater influence on SHBG production in comparison and hence the higher SHBG levels with oral estradiol could result in more significant limitation of free estradiol than with non-oral estradiol. The notion that this reduction in free estradiol corresponds to a decrease in the activity or potency of oral estradiol is only a theoretical possibility however. Therapeutically, oral estradiol has shown itself to be very effective. The decreases in free estradiol percentage with low-dose oral estradiol seem to be small. In addition, while no direct comparisons exist this time, higher doses of oral estradiol seem to show similar testosterone suppression as non-oral estradiol (Wiki; Graphs). Besides testosterone suppression, available studies have found no differences between oral and non-oral estradiol in terms of outcomes like breast development or feminization (Sam, 2020). As such, the differences between oral and non-oral estradiol in terms SHBG levels and free estradiol fraction may be of little therapeutic importance.
Aside from decreasing free estradiol fractions, increased SHBG levels also decrease free testosterone fractions to an even greater extent. This is advantageous in the case of transfeminine people.
Taken together, lower free estradiol due to increased SHBG levels, whether with non-oral or oral estradiol, isn’t something that should be a major source of concern in transfeminine hormone therapy.
Supplementary Material
See here for supplementary material for this article, including a spreadsheet and other calculators that can be used to estimate free hormone levels (e.g., Mazer, 2009).
References
Adamcová, K., Kolátorová, L., Škodová, T., Šimková, M., Pařízek, A., Stárka, L., & Dušková, M. (2018). Steroid hormone levels in the peripartum period – differences caused by fetal sex and delivery type. Physiological Research, 67(Suppl 3), S489–S497. [DOI:10.33549/physiolres.934019]
Anderson, P. J., Hancock, K. W., & Oakey, R. E. (1985). Non-protein-bound oestradiol and progesterone in human peripheral plasma before labour and delivery. Journal of Endocrinology, 104(1), 7–15. [DOI:10.1677/joe.0.1040007]
Barini, A., Liberale, I., & Menini, E. (1993). Simultaneous Determination of Free Testosterone and Testosterone Bound to Non-Sex-Hormone-Binding Globulin by Equilibrium Dialysis. Clinical Chemistry, 39(6), 936–941. [DOI:10.1093/clinchem/39.6.936]
Bernstein, L., Depue, R. H., Ross, R. K., Judd, H. L., Pike, M. C., & Henderson, B. E. (1986). Higher maternal levels of free estradiol in first compared to second pregnancy: early gestational differences. Journal of the National Cancer Institute, 76(6), 1035–1039. [DOI:10.1093/jnci/76.6.1035]
Bernstein, L., Pike, M., Depue, R., Ross, R., Moore, J., & Henderson, B. (1988). Maternal hormone levels in early gestation of cryptorchid males: a case-control study. British Journal of Cancer, 58(3), 379–381. [DOI:10.1038/bjc.1988.223]
Bland, L. B., Garzotto, M., DeLoughery, T. G., Ryan, C. W., Schuff, K. G., Wersinger, E. M., Lemmon, D., & Beer, T. M. (2005). Phase II study of transdermal estradiol in androgen-independent prostate carcinoma. Cancer, 103(4), 717–723. [DOI:10.1002/cncr.20857]
Braunstein, G. D., Reitz, R. E., Buch, A., Schnell, D., & Caulfield, M. P. (2011). Testosterone Reference Ranges in Normally Cycling Healthy Premenopausal Women. The Journal of Sexual Medicine, 8(10), 2924–2934. [DOI:10.1111/j.1743-6109.2011.02380.x]
Burger, H. G., Dudley, E. C., Cui, J., Dennerstein, L., & Hopper, J. L. (2000). A Prospective Longitudinal Study of Serum Testosterone, Dehydroepiandrosterone Sulfate, and Sex Hormone-Binding Globulin Levels through the Menopause Transition. The Journal of Clinical Endocrinology & Metabolism, 85(8), 2832–2838. [DOI:10.1210/jcem.85.8.6740]
Campino, C., Torres, C., Rioseco, A., Poblete, A., Pugin, E., Valdés, V., Catalán, S., Belmar, C., & Serón-Ferré, M. (2001). Plasma prolactin/oestradiol ratio at 38 weeks gestation predicts the duration of lactational amenorrhoea. Human Reproduction, 16(12), 2540–2545. [DOI:10.1093/humrep/16.12.2540]
de Blok, C. J., Klaver, M., Wiepjes, C. M., Nota, N. M., Heijboer, A. C., Fisher, A. D., Schreiner, T., T’Sjoen, G., & den Heijer, M. (2017). Breast Development in Transwomen After 1 Year of Cross-Sex Hormone Therapy: Results of a Prospective Multicenter Study. The Journal of Clinical Endocrinology & Metabolism, 103(2), 532–538. [DOI:10.1210/jc.2017-01927]
de Blok, C. J., Dijkman, B. A., Wiepjes, C. M., Staphorsius, A. S., Timmermans, F. W., Smit, J. M., Dreijerink, K. M., & den Heijer, M. (2020). Sustained Breast Development and Breast Anthropometric Changes in 3 Years of Gender-Affirming Hormone Treatment. The Journal of Clinical Endocrinology & Metabolism, 106(2), e782–e790. [DOI:10.1210/clinem/dgaa841]
Depue, R. H., Bernstein, L., Ross, R. K., Judd, H. L., & Henderson, B. E. (1987). Hyperemesis gravidarum in relation to estradiol levels, pregnancy outcome, and other maternal factors: A seroepidemiologic study. American Journal of Obstetrics and Gynecology, 156(5), 1137–1141. [DOI:10.1016/0002-9378(87)90126-8]
Derra, C. (1981). Hormonprofile unter Östrogen- und Antiandrogentherapie bei Patienten mit Prostatakarzinom: Östradiolundecylat versus Cyproteronacetat. [Hormone Profiles under Estrogen and Antiandrogen Therapy in Patients with Prostate Cancer: Estradiol Undecylate versus Cyproterone Acetate.] (Doctoral dissertation, University of Mainz.) [Google Scholar] [WorldCat] [PDF] [Translation]
Dittrich, R., Binder, H., Cupisti, S., Hoffmann, I., Beckmann, M., & Mueller, A. (2005). Endocrine Treatment of Male-to-Female Transsexuals Using Gonadotropin-Releasing Hormone Agonist. Experimental and Clinical Endocrinology & Diabetes, 113(10), 586–592. [DOI:10.1055/s-2005-865900]
Dunn, J. F., Nisula, B. C., & Rodbard, D. (1981). Transport of Steroid Hormones: Binding of 21 Endogenous Steroids to Both Testosterone-Binding Globulin and Corticosteroid-Binding Globulin in Human Plasma. The Journal of Clinical Endocrinology & Metabolism, 53(1), 58–68. [DOI:10.1210/jcem-53-1-58]
Fåhraeus, L., & Larsson-Cohn, U. (1982). Oestrogens, gonadotrophins and SHBG during oral and cutaneous administration of oestradiol-17β to menopausal women. Acta Endocrinologica, 101(4), 592–596. [DOI:10.1530/acta.0.1010592]
Fanelli, F., Gambineri, A., Belluomo, I., Repaci, A., Di Lallo, V. D., Di Dalmazi, G., Mezzullo, M., Prontera, O., Cuomo, G., Zanotti, L., Paccapelo, A., Morselli-Labate, A. M., Pagotto, U., & Pasquali, R. (2013). Androgen Profiling by Liquid Chromatography–Tandem Mass Spectrometry (LC-MS/MS) in Healthy Normal-Weight Ovulatory and Anovulatory Late Adolescent and Young Women. The Journal of Clinical Endocrinology & Metabolism, 98(7), 3058–3067. [DOI:10.1210/jc.2013-1381]
Freymann, E., Hubl, W., Büchner, M., & Belleée, H. (1977). Eine spezifische, radioimmunologische Bestimmung des Plasmaöstradiols ohne Chromatographie im Zyklus und in der Schwangerschaft und die Bestimmung des freien, nichtproteingebundenen Anteils mittels Dialyse. [A specific radioimmunologi determination of plasma estradiol without chromatography during the cycle and in pregnancy and determination of the free non-protein-bound fraction using dialysis.] Zentralblatt für Gynäkologie, 99(6), 321–329. [Google Scholar 1] [Google Scholar 2] [PubMed] [PDF]
Freymann, E., Hubl, W., Büchner, M., & Rohde, W. (1977). Plasma levels of apparent free estradiol during pregnancy. Endokrinologie, 69(2), 269–271. [Google Scholar] [PubMed] [PDF]
Gibney, J., Johannsson, G., Leung, K., & Ho, K. K. (2005). Comparison of the Metabolic Effects of Raloxifene and Oral Estrogen in Postmenopausal and Growth Hormone-Deficient Women. The Journal of Clinical Endocrinology & Metabolism, 90(7), 3897–3903. [DOI:10.1210/jc.2005-0173]
Goldman, A. L., Bhasin, S., Wu, F. C., Krishna, M., Matsumoto, A. M., & Jasuja, R. (2017). A Reappraisal of Testosterone’s Binding in Circulation: Physiological and Clinical Implications. Endocrine Reviews, 38(4), 302–324. [DOI:10.1210/er.2017-00025]
Graham, C. A., Bancroft, J., Doll, H. A., Greco, T., & Tanner, A. (2007). Does oral contraceptive-induced reduction in free testosterone adversely affect the sexuality or mood of women? Psychoneuroendocrinology, 32(3), 246–255. [DOI:10.1016/j.psyneuen.2006.12.011]
Guthrie, J., Dennerstein, L., Taffe, J., Lehert, P., & Burger, H. (2004). The menopausal transition: a 9-year prospective population-based study. The Melbourne Women’s Midlife Health Project. Climacteric, 7(4), 375–389. [DOI:10.1080/13697130400012163]
Hammond, G. L., Nisker, J. A., Jones, L. A., & Siiteri, P. K. (1980). Estimation of the percentage of free steroid in undiluted serum by centrifugal ultrafiltration-dialysis. Journal of Biological Chemistry, 255(11), 5023–5026. [DOI:10.1016/s0021-9258(19)70742-x]
Hammond, G. L. (2016). Plasma steroid-binding proteins: primary gatekeepers of steroid hormone action. Journal of Endocrinology, 230(1), R13–R25. [DOI:10.1530/joe-16-0070]
Hammond, G. L. (2017). Sex Hormone-Binding Globulin and the Metabolic Syndrome. In Winters, S. J., & Huhtaniemi, I. T. (Eds.). Male Hypogonadism: Basic, Clinical and Therapeutic Principles (pp. 305–324). Cham: Springer International Publishing. [DOI:10.1007/978-3-319-53298-1_15]
Handelsman, D. J. (2017). Free Testosterone: Pumping up the Tires or Ending the Free Ride? Endocrine Reviews, 38(4), 297–301. [DOI:10.1210/er.2017-00171]
Heidrich, A., Schleyer, M., Spingler, H., Albert, P., Knoche, M., Fritze, J., & Lanczik, M. (1994). Postpartum blues: Relationship between not-protein bound steroid hormones in plasma and postpartum mood changes. Journal of Affective Disorders, 30(2), 93–98. [DOI:10.1016/0165-0327(94)90036-1]
Heubner, A., Brockerhoff, P., Kreienberg, R., Grill, H., Rathgen, G., & Pollow, K. (1987). The influence of various dosages of megestrol acetate on SHBG, CBG and lipoprotein patterns. Journal of Steroid Biochemistry, 28(Suppl 1), 214S–214S (abstract no. 6). [DOI:10.1016/0022-4731(87)91680-3]
Hogeveen, K. N., Cousin, P., Pugeat, M., Dewailly, D., Soudan, B., & Hammond, G. L. (2002). Human sex hormone-binding globulin variants associated with hyperandrogenism and ovarian dysfunction. The Journal of Clinical Investigation, 109(7), 973–981. [DOI:10.1172/JCI14060]
Keevil, B. G., & Adaway, J. (2019). Assessment of free testosterone concentration. The Journal of Steroid Biochemistry and Molecular Biology, 190, 207–211. [DOI:10.1016/j.jsbmb.2019.04.008]
Kerlan, V., Nahoul, K., Martelot, M., & Bercovici, J. (1994). Longitudinal study of maternal plasma bioavailable testosterone and androstanediol glucuronide levels during pregnancy. Clinical Endocrinology, 40(2), 263–267. [DOI:10.1111/j.1365-2265.1994.tb02478.x]
Krause, A., Sinnecker, G., Hiort, O., Thamm, B., & Hoepffner, W. (2004). Applicability of the SHBG Androgen Sensitivity Test in the Differential Diagnosis of 46,XY Gonadal Dysgenesis, True Hermaphroditism, and Androgen Insensitivity Syndrome. Experimental and Clinical Endocrinology & Diabetes, 112(5), 236–240. [DOI:10.1055/s-2004-817969]
Kronawitter, D., Gooren, L. J., Zollver, H., Oppelt, P. G., Beckmann, M. W., Dittrich, R., & Mueller, A. (2009). Effects of transdermal testosterone or oral dydrogesterone on hypoactive sexual desire disorder in transsexual women: results of a pilot study. European Journal of Endocrinology, 161(2), 363–368. [DOI:10.1530/eje-09-0265] [Table]
Kuhl, H. (1997). Metabolische Effekte der Östrogene und Gestagene. [Metabolic Effects of Estrogens and Progestogens.] Der Gynäkologe, 30(4), 357–369. [DOI:10.1007/pl00003042]
Kuhl, H. (1998). Adverse effects of estrogen treatment: natural vs. synthetic estrogens. In Lippert, T. H., Mueck, A. O., & Ginsburg, J. (Eds.). Sex Steroids and the Cardiovascular System: The Proceedings of the 1st Interdisciplinary Workshop, Tuebingen, Germany, October 1996. Parthenon Publishing Group, New York, London (pp. 201–210). London/New York: Parthenon. [Google Scholar] [Google Books] [PDF]
Kuhl, H. (1999). Hormonal contraception. In Oettel, M., & Schillinger, E. (Eds.). Estrogens and Antiestrogens II: Pharmacology and Clinical Application of Estrogens and Antiestrogen (Handbook of Experimental Pharmacology, Volume 135, Part 2) (pp. 363–407). Berlin/Heidelberg: Springer. [DOI:10.1007/978-3-642-60107-1_18]
Kuhl, H. (2005). Pharmacology of Estrogens and Progestogens: Influence of Different Routes of Administration. Climacteric, 8(Suppl 1), 3–63. [DOI:10.1080/13697130500148875] [PDF]
Lundgren, S., Lønning, P., Utaaker, E., Aakvaag, A., & Kvinnsland, S. (1990). Influence of progestins on serum hormone levels in postmenopausal women with advanced breast cancer—I. General findings. Journal of Steroid Biochemistry, 36(1–2), 99–104. [DOI:10.1016/0022-4731(90)90118-c]
Lundgren, S., & Lønning, P. (1990). Influence of progestins on serum hormone levels in postmenopausal women with advanced breast cancer—II. A differential effect of megestrol acetate and medroxyprogesterone acetate on serum estrone sulfate and sex hormone binding globulin. Journal of Steroid Biochemistry, 36(1–2), 105–109. [DOI:10.1016/0022-4731(90)90119-d]
Mazer, N. A. (2009). A novel spreadsheet method for calculating the free serum concentrations of testosterone, dihydrotestosterone, estradiol, estrone and cortisol: With illustrative examples from male and female populations. Steroids, 74(6), 512–519. [DOI:10.1016/j.steroids.2009.01.008] [Spreadsheet]
McClamrock, H. D. (2007). Pregnancy-Related Androgen Excess. In Azziz, R., Nestler, J. E., & Dewailly, D. (Eds.). Androgen Excess Disorders in Women: Polycystic Ovary Syndrome and Other Disorders, 2nd Edition (Contemporary Endocrinology) (pp. 107–119). Totowa, New Jersey: Humana Press. [Google Books] [DOI:10.1007/978-1-59745-179-6_9]
Mean, F., Pellaton, M., & Magrini, G. (1977). Study on the binding of dihydrotestosterone, testosterone and oestradiol with sex hormone binding globulin. Clinica Chimica Acta, 80(1), 171–180. [DOI:10.1016/0009-8981(77)90276-5]
Meyer, G., Mayer, M., Mondorf, A., Flügel, A. K., Herrmann, E., & Bojunga, J. (2020). Safety and rapid efficacy of guideline-based gender-affirming hormone therapy: an analysis of 388 individuals diagnosed with gender dysphoria. European Journal of Endocrinology, 182(2), 149–156. [DOI:10.1530/eje-19-0463] [PDF]
Moore, J. W., & Bulbrook, R. D. (1988). The epidemiology and function of sex hormone-binding globulin. Oxford Reviews of Reproductive Biology, 10, 180–236. [Google Scholar] [PubMed] [PDF]
Mueller, A., Dittrich, R., Binder, H., Kuehnel, W., Maltaris, T., Hoffmann, I., & Beckmann, M. W. (2005). High dose estrogen treatment increases bone mineral density in male-to-female transsexuals receiving gonadotropin-releasing hormone agonist in the absence of testosterone. European Journal of Endocrinology, 153(1), 107–113. [DOI:10.1530/eje.1.01943]
Mueller, A., Binder, H., Cupisti, S., Hoffmann, I., Beckmann, M., & Dittrich, R. (2006). Effects on the Male Endocrine System of Long-term Treatment with Gonadotropin-releasing Hormone Agonists and Estrogens in Male-to-Female Transsexuals. Hormone and Metabolic Research, 38(3), 183–187. [DOI:10.1055/s-2006-925198]
Mueller, A., Zollver, H., Kronawitter, D., Oppelt, P. G., Claassen, T., Hoffmann, I., Beckmann, M. W., & Dittrich, R. (2011). Body composition and bone mineral density in male-to-female transsexuals during cross-sex hormone therapy using gonadotrophin-releasing hormone agonist. Experimental and Clinical Endocrinology & Diabetes, 119(2), 95–100. [DOI:10.1055/s-0030-1255074] [Table]
Nachtigall, L. E., Raju, U., Banerjee, S., Wan, L., & Levitz, M. (2000). Serum Estradiol-Binding Profiles in Postmenopausal Women Undergoing Three Common Estrogen Replacement Therapies. Menopause, 7(4), 243–250. [DOI:10.1097/00042192-200007040-00006]
Nakamoto, J. (2016). Endocrine Testing. In Jameson, J. L., & De Groot, L. J. (Eds.). Endocrinology: Adult and Pediatric, 7th Edition (pp. 2655–2688.e1). Philadelphia: Saunders/Elsevier. [Google Books] [DOI:10.1016/B978-0-323-18907-1.00154-2]
Nguyen, T. D. T., Dolomie-Fagour, L., Georges, A., & Corcuff, J. B. (2008). Dosage des stéroïdes sexuels sériques: quelle place pour l’estradiol biodisponible? [What about bioavailable estradiol?] Annales de Biologie Clinique, 66(5), 493–497. [DOI:10.1684/abc.2008.0259]
Nilsson, B., Holst, J., & Schoultz, B. (1984). Serum levels of unbound 17β-oestradiol during oral and percutaneous postmenopausal replacement therapy. British Journal of Obstetrics and Gynaecology, 91(10), 1031–1036. [DOI:10.1111/j.1471-0528.1984.tb03683.x]
Nolan, B. J., & Cheung, A. S. (2021). Relationship Between Serum Estradiol Concentrations and Clinical Outcomes in Transgender Individuals Undergoing Feminizing Hormone Therapy: A Narrative Review. Transgender Health, 6(3), 125–131. [DOI:10.1089/trgh.2020.0077]
O’Leary, P., Boyne, P., Flett, P., Beilby, J., & James, I. (1991). Longitudinal assessment of changes in reproductive hormones during normal pregnancy. Clinical Chemistry, 37(5), 667–672. [DOI:10.1093/clinchem/37.5.667]
Odlind, V., Milsom, I., Persson, I., & Victor, A. (2002). Can changes in sex hormone binding globulin predict the risk of venous thromboembolism with combined oral contraceptive pills? Acta Obstetricia et Gynecologica Scandinavica, 81(6), 482–490. [DOI:10.1034/j.1600-0412.2002.810603.x]
Ojasoo, T., & Raynaud, J. P. (1978). Unique steroid congeners for receptor studies. Cancer Research, 38(11 Part 2), 4186–4198. [Google Scholar] [PubMed] [URL]
Pande, P., Fleck, S. C., Twaddle, N. C., Churchwell, M. I., Doerge, D. R., & Teeguarden, J. G. (2019). Comparative estrogenicity of endogenous, environmental and dietary estrogens in pregnant women II: Total estrogenicity calculations accounting for competitive protein and receptor binding and potency. Food and Chemical Toxicology, 125, 341–353. [DOI:10.1016/j.fct.2018.12.013]
Pardridge, W. M. (1988). Selective delivery of sex steroid hormones to tissues by albumin and by sex hormone-binding globulin. Oxford Reviews of Reproductive Biology, 10, 237–292. [Google Scholar] [PubMed] [PDF]
Perry, L., Wathen, N., & Chard, T. (1987). Saliva Levels of Oestradiol and Progesterone in Relation to Non-Protein-Bound Concentrations in Blood During Late Pregnancy. Hormone and Metabolic Research, 19(9), 444–447. [DOI:10.1055/s-2007-1011848]
Plymate, S. R., Moore, D. E., Cheng, C. Y., Bardin, C. W., Southworth, M. B., & Levinski, M. J. (1985). Sex Hormone-Binding Globulin Changes during the Menstrual Cycle. The Journal of Clinical Endocrinology & Metabolism, 61(5), 993–996. [DOI:10.1210/jcem-61-5-993]
Pugeat, M. M., Dunn, J. F., & Nisula, B. C. (1981). Transport of Steroid Hormones: Interaction of 70 Drugs with Testosterone-Binding Globulin and Corticosteroid-Binding Globulin in Human Plasma. The Journal of Clinical Endocrinology & Metabolism, 53(1), 69–75. [DOI:10.1210/jcem-53-1-69]
Rezaii, T., Gustafsson, T. P., Axelson, M., Zamani, L., Ernberg, M., Hirschberg, A. L., & Carlström, K. A. (2017). Circulating androgens and SHBG during the normal menstrual cycle in two ethnic populations. Scandinavian Journal of Clinical and Laboratory Investigation, 77(3), 184–189. [DOI:10.1080/00365513.2017.1286685]
Ropponen, A., Aittomäki, K., Vihma, V., Tikkanen, M. J., & Ylikorkala, O. (2005). Effects of Oral and Transdermal Estradiol Administration on Levels of Sex Hormone-Binding Globulin in Postmenopausal Women with and without a History of Intrahepatic Cholestasis of Pregnancy. The Journal of Clinical Endocrinology & Metabolism, 90(6), 3431–3434. [DOI:10.1210/jc.2005-0352]
Rosner, W. (2015). Free estradiol and sex hormone-binding globulin. Steroids, 99, 113–116. [DOI:10.1016/j.steroids.2014.08.005]
Rothman, M. S., Carlson, N. E., Xu, M., Wang, C., Swerdloff, R., Lee, P., Goh, V. H., Ridgway, E. C., & Wierman, M. E. (2011). Reexamination of testosterone, dihydrotestosterone, estradiol and estrone levels across the menstrual cycle and in postmenopausal women measured by liquid chromatography–tandem mass spectrometry. Steroids, 76(1–2), 177–182. [DOI:10.1016/j.steroids.2010.10.010]
Rubinow, D. R., Schmidt, P. J., Roca, C. A., & Daly, R. C. (2002). Gonadal Hormones and Behavior in Women: Concentrations versus Context. In Pfaff, D. W., Arnold, A. P., Etgen, A. M., Fahrbach, S. E., & Rubin, R. T. (Eds.). Hormones, Brain and Behavior, Volume 5 (pp. 37–73). Amsterdam: Academic Press. [Google Books] [DOI:10.1016/B978-012532104-4/50086-X]
Ruokonen, A., Alén, M., Bolton, N., & Vihko, R. (1985). Response of serum testosterone and its precursor steroids, SHBG and CBG to anabolic steroid and testosterone self-administration in man. Journal of Steroid Biochemistry, 23(1), 33–38. [DOI:10.1016/0022-4731(85)90257-2]
Schijf, C. P., van der Mooren, M. J., Doesburg, W. H., Thomas, C. M., & Rolland, R. (1993). Differences in serum lipids, lipoproteins, sex hormone binding globulin and testosterone between the follicular and the luteal phase of the menstrual cycle. Acta Endocrinologica, 129(2), 130–133. [DOI:10.1530/acta.0.1290130]
Schuijt, M. P., Sweep, C. G., van der Steen, R., Olthaar, A. J., Stikkelbroeck, N. M., Ross, H. A., & van Herwaarden, A. E. (2019). Validity of free testosterone calculation in pregnant women. Endocrine Connections, 8(6), 672–679. [DOI:10.1530/ec-19-0110]
Shifren, J. L., Desindes, S., McIlwain, M., Doros, G., & Mazer, N. A. (2007). A randomized, open-label, crossover study comparing the effects of oral versus transdermal estrogen therapy on serum androgens, thyroid hormones, and adrenal hormones in naturally menopausal women. Menopause, 14(6), 985–994. [DOI:10.1097/gme.0b013e31803867a]
Shifren, J. L., Rifai, N., Desindes, S., McIlwain, M., Doros, G., & Mazer, N. A. (2008). A Comparison of the Short-Term Effects of Oral Conjugated Equine Estrogens Versus Transdermal Estradiol on C-Reactive Protein, Other Serum Markers of Inflammation, and Other Hepatic Proteins in Naturally Menopausal Women. The Journal of Clinical Endocrinology & Metabolism, 93(5), 1702–1710. [DOI:10.1210/jc.2007-2193]
Smith, K., Galazi, M., Openshaw, M. R., Wilson, P., Sarker, S. J., O’Brien, N., Alifrangis, C., Stebbing, J., & Shamash, J. (2020). The Use of Transdermal Estrogen in Castrate-resistant, Steroid-refractory Prostate Cancer. Clinical Genitourinary Cancer, 18(3), e217–e223. [DOI:10.1016/j.clgc.2019.09.019]
Stege, R., Carlström, K., Collste, L., Eriksson, A., Henriksson, P., & Pousette, A. (1988). Single drug polyestradiol phosphate therapy in prostatic cancer. American Journal of Clinical Oncology, 11(Suppl 2), S101–S103. [DOI:10.1097/00000421-198801102-00024] [PDF]
Steingold, K. A., Pardridge, W. M., Judd, H. L., & Chaudhuri, G. (1987). The effects of membrane permeability and binding by human serum proteins on steroid influx into the rabbit uterus. American Journal of Obstetrics and Gynecology, 157(6), 1543–1549. [DOI:10.1016/s0002-9378(87)80260-0]
Strauss, J. F., & FitzGerald, G. A. (2019). Steroid Hormones and Other Lipid Molecules Involved in Human Reproduction. In Strauss, J. F., & Barbieri, R. L. (Eds.). Yen and Jaffe’s Reproductive Endocrinology: Physiology, Pathophysiology, and Clinical Management, 8th Edition (pp. 75–114.e7). Philadelphia: Elsevier. [Google Books] [DOI:10.1016/b978-0-323-47912-7.00004-4]
Troisi, R., Potischman, N., Roberts, J. M., Harger, G., Markovic, N., Cole, B., Lykins, D., Siiteri, P., & Hoover, R. N. (2003). Correlation of serum hormone concentrations in maternal and umbilical cord samples. Cancer Epidemiology, Biomarkers & Prevention, 12(5), 452–456. [Google Scholar] [PubMed] [URL]
Tulchinsky, D., & Chopra, I. J. (1973). Competitive Ligand-Binding Assay for Measurement of Sex Hormone-Binding Globulin (SHBG). The Journal of Clinical Endocrinology & Metabolism, 37(6), 873–881. [DOI:10.1210/jcem-37-6-873]
von Schoultz, B., Carlström, K., Collste, L., Eriksson, A., Henriksson, P., Pousette, Å., & Stege, R. (1989). Estrogen therapy and liver function—metabolic effects of oral and parenteral administration. The Prostate, 14(4), 389–395. [DOI:10.1002/pros.2990140410]
Zimmerman, Y., Eijkemans, M. J., Coelingh Bennink, H. J., Blankenstein, M. A., & Fauser, B. C. (2013). The effect of combined oral contraception on testosterone levels in healthy women: a systematic review and meta-analysis. Human Reproduction Update, 20(1), 76–105. [DOI:10.1093/humupd/dmt038]
\ No newline at end of file
diff --git a/transfemscience.org/articles/spiro-testosterone/index.html b/transfemscience.org/articles/spiro-testosterone/index.html
index 0180669f..4dd40b61 100644
--- a/transfemscience.org/articles/spiro-testosterone/index.html
+++ b/transfemscience.org/articles/spiro-testosterone/index.html
@@ -1 +1 @@
-A Review of Studies on Spironolactone and Testosterone Suppression in Cisgender Men, Cisgender Women, and Transfeminine People - Transfeminine Science
A Review of Studies on Spironolactone and Testosterone Suppression in Cisgender Men, Cisgender Women, and Transfeminine People
By Aly | First published December 19, 2018 | Last modified April 5, 2024
Abstract / TL;DR
Spironolactone is an antiandrogen used in transfeminine hormone therapy which is especially employed in the United States. It is widely considered to act as an androgen receptor antagonist and as an androgen synthesis inhibitor, both blocking the actions of testosterone and lowering testosterone levels in transfeminine people. A literature search was conducted to review studies assessing the influence of spironolactone on testosterone levels in cisgender men, cisgender women, and transfeminine people. The results of these studies were mixed, but in most studies spironolactone showed no apparent influence on testosterone levels. These findings suggest that spironolactone has inconsistent and limited effects on testosterone levels. Moreover, these data, as well as studies of estradiol alone, indicate that estradiol is mainly responsible for lowered testosterone levels when the combination of estradiol and spironolactone is used for hormone therapy in transfeminine people. Besides testosterone suppression, spironolactone also acts as a direct antagonist of the androgen receptor, and this importantly contributes to its antiandrogenic efficacy as well. However, studies in cisgender women suggest that spironolactone is a relatively weak androgen receptor antagonist, and is likely best-suited for blocking relatively low testosterone levels. Taken together, the antiandrogenic effectiveness of spironolactone in transfeminine people appears to be limited. Other antiandrogenic approaches may be more effective in transfeminine people, and may be considered instead or as alternatives to spironolactone in those in whom testosterone levels with estradiol plus spironolactone remain inadequately suppressed.
Introduction
Spironolactone, also known by its major brand name Aldactone, is an antiandrogen which is commonly used in transfeminine hormone therapy. It is used in combination with estrogen in transfeminine people to help reduce the effects of testosterone. Spironolactone is used in transfeminine hormone therapy particularly in the United States, where another antiandrogen, cyproterone acetate (CPA; brand name Androcur), is unavailable. Conversely, CPA is the main antiandrogen used in transfeminine people in Europe and most of the rest of the world. Another type of medication, gonadotropin-releasing hormone (GnRH) agonists, are the major antiandrogens used in certain places like the United Kingdom. The combination of estradiol with CPA or a GnRH agonist in transfeminine people consistently suppresses testosterone levels into the normal female range (<50 ng/dL or <1.8 nmol/L) (Aly, 2018; Aly, 2019). Hence, both CPA and GnRH agonists are very effective antiandrogens in transfeminine people.
Spironolactone acts as an androgen receptor antagonist, but is also known to function as an androgen synthesis inhibitor. As an example, spironolactone has been shown in preclinical research to inhibit several enzymes involved in gonadal and adrenal androgen production, including CYP17A1 (17α-hydroxylase/17,20-lyase) among others, and to substantially decrease concentrations of androgens in these studies (Loriaux et al., 1976; Callan, 1988; McMullen & Van Herle, 1993). However, the steroid synthesis inhibition of spironolactone appears to only occur at very high doses and concentrations of spironolactone (Loriaux et al., 1976; McMullen & Van Herle, 1993). For example, spironolactone is used at 10- to 20-fold smaller doses by body weight in humans than in animal studies that have demonstrated substantial steroid synthesis inhibition with the agent (McMullen & Van Herle, 1993).
A widespread notion in the transgender community, as well as in the transgender health community and in the medical literature, is that spironolactone decreases testosterone levels and that this is a major part of how it works as an antiandrogen in transfeminine people. In actuality however, the clinical evidence to support this notion appears to be limited, and available data from studies appear to be highly conflicting. The purpose of this article is to review the available clinical studies on spironolactone and testosterone levels in cisgender men, cisgender women, and transfeminine people in order to help elucidate whether and to what extent spironolactone lowers testosterone levels in humans. In addition, the role of androgen receptor blockade in the antiandrogenic effects of spironolactone is briefly reviewed.
A total of 22 studies of spironolactone and sex hormone levels in cisgender males were identified (Table 1). These studies assessed pre-treatment versus post-treatment hormone levels with spironolactone, hormone levels with spironolactone versus a comparator group, or both. Within the identified studies, testosterone levels were not significantly changed in 12 of 22 studies (55%), decreased in 4 of 22 (18%) studies, increased in 1 of 22 (4.5%) studies, and mixed or unknown (e.g. divergences in changes of total versus free testosterone levels or didn’t actually report testosterone levels) in 4 of 22 (18%) studies. Most of the studies were very small (fewer than 10 people), with several exceptions. The studies were of highly variable lengths, with some being several days and others lasting for weeks or months. Few of the studies were RCTs. Most of the studies were very old, with a majority published in the 1970s and the rest published in the 1980s and 1990s. In relation to the preceding, the quality of data was limited.
Table 1: Studies of sex hormone levels with spironolactone alone in cisgender males:
Treatment and subjects
Findings
Source(s)
100 mg/day for 2 weeks in 7 healthy men (23–34 years)
T significantly decreased and LH significantly increased. No significant change in E1, E2, or E3. No change urinary total T excretion but significantly increased urinary total E excretion (including of E1 (7.72 to 10.54 µg/24 hrs), E2 (2.60 to 3.34 ug/24 hours), E3 (7.69 to 11.75 µg/24 hrs)). Slightly but significantly decreased excretion of 17-KS in urine.
400 mg/day for 5 days in 6 healthy men (21–33 years)
Significant increase in P4 and 17α-OHP (approximately doubled) for whole duration. Small and transient increases in LH (+20%) and FSH on the 2nd but not on the 3rd or 5th days (only other days measured). No significant changes in T, E2, or PRL. E2 and PRL non-significantly increased (+56% and +34% on the 5th day, respectively).
100 or 400 mg/day spironolactone for 8 weeks in 7 orchiectomized men (46–78 years) with metastatic prostate cancer
T, A4, and DHEA significantly decreased with both doses of spironolactone and of similar magnitude between doses. Influence more apparent after 2–3 weeks of treatment.
5 mg/kg/day for 1 week (275 mg/day for a 55 kg person) in 7 boys with delayed puberty (14–16 years)
Significant increase in LH (+60%) and non-significant increase in FSH (+60%); individual responses for FSH variable. Increased P4 and 17α-OHP. T and E2 not actually reported.
Initially 400 mg/day for 12 weeks; dosage later decreased in some due to hypotension (range 150–400 mg/day) in 5 men and 5 women (3 premenopausal, 2 postmenopausal) with normal or low renin hypertension
P4 and 17α-OHP increased by 2 to 4 times compared to pre-treatment and post-treatment. T, E2, LH, FSH, PRL, and 17-KS all unchanged.
200–400 mg/day for 4–13 months (mean 7 months) in 6 men with hypertension (35–61 years; mean 47 years) vs. 10 untreated male controls with hypertension (mean age 45 years)
Significantly greater LH and E2 (30 pg/mL vs. 13 pg/mL; +130%), significantly lower T (440 ng/dL vs. 270 ng/dL; –38%), no difference in FSH. Also, significantly greater metabolic clearance rate of T, significantly greater rate of peripheral conversion (conversion ratio and transfer constant) of T into E2, non-significantly greater metabolic clearance rate of E2, no difference in blood production rate of T, and significantly greater blood production rate of E2.
200–400 mg/day (mean 330 mg/day) for 20–27 days in 5 gonadally intact men (50–76 years) with prostate cancer
P4 increased significantly from 0.25 ± 0.10 ng/mL (mean ± SD) to maximum of 1.3 ± 0.31 ng/mL by 20 days (increase of 5.2-fold or 420%). T decreased significantly from 427 ± 74.3 ng/dL to 200 ± 80.3 ng/dL (–53.2%). No significant change in E2, LH, or FSH.
200 mg/day for 21 days in 4 healthy men (26–35 years)
No change in total T or E2. Unbound T and E2 slightly but significantly increased. Thought to be due to a direct interaction of spironolactone metabolites with the plasma protein binding of T and E2. But not due to binding to SHBG as T binding to SHBG was not significantly altered.
75–150 mg/day for 12 weeks in 6 men with essential hypertension (28–64 years; mean 48 years)
E1 significantly increased. E2 small, gradual, non-significant increase. T, LH, and PRL not significantly changed. PRL responses to TRH normal/not significantly changed.
150–300 mg/day for 40 weeks in 2 men with idiopathic hyperaldosteronism (23 and 44 years)
E1 increased. E2 fluctuated. E2 increased by 10-fold in one person by 16 weeks and this was associated with gynecomastia. T, LH, and PRL not altered significantly.
200 mg/day for 10 days (n=5) vs. placebo (n=5) in 10 healthy men (18–31 years) (RCT)
Significantly greater urinary A4, urinary EC, and urinary total E excretion. Differences in T, E2, LH, and FSH as well as urinary DHEA, LH, and FSH not significant. Examination of interaction between treatment and time showed significant changes in T, LH, and urinary DHEA. Concluded that there was a transient rise in T and urine DHEA for 2–4 days followed by increase in LH and normalization of T and DHEA excretion after 4–10 days.
300 mg/day for 7 days (n=5) vs. 200 mg/day triamterene (n=5) in 10 normal young men with diet-induced hyperaldosteronism (14 days of a diet modifying electrolyte intake)
P4, 17α-OHP, unchanged. T near-but-non-significantly decreased (704.6 ± 55.5 ng/dL (mean ± SEM) to 508.4 ± 45.9 ng/dL on day 6; p < 0.10). Also assessed endogenous corticosteroids.
100 mg/day for 3 months in treatment group of 47 men (age 60–80 years) with BPH; control group of 58 healthy men without BPH (also age 60–80 years)
In spiro/BPH group, T decreased from 650 ng/dL to 290 ng/dL and DHT decreased from 450 ng/dL to 150 ng/dL. In control/non-BPH group, T was 280 ng/dL and DHT was 90 ng/dL. P4, E2, and LH increased in spiro/BPH group. FSH also assessed. The authors stated that prostate gland can be a source of androgen production, implying that BPH can produce elevated androgen levels and that spironolactone can normalize elevated androgen levels in the condition.
150 mg/m2/day for 5 days in 6 boys with irregular puberty (11–13 years)
No significant changes in T or urinary 17-KS excretion, elevated LH (by 600%—likely typo of “60%” (?)), and slightly increased FSH (from 0.75 ng/mL to 0.86 ng/mL).
25–400 mg/day (median 100 mg/day) for 12 months in 32 males (59%) of a group of 54 males (17–64 years; mean 44 years) with non-alcoholic liver disease requiring liver transplantation vs. 469 healthy male controls (mean 31 years) with normal liver function
Significantly decreased T with spironolactone in men with moderate-severity liver disease but not with low- or high-severity liver disease. SHBG not influenced by spironolactone dosage. No influence on gonadotropin responses to GnRH stimulation.
Although the quality of these studies is limited, the findings of the studies, which are mixed but are overall more suggestive against spironolactone reducing testosterone levels than it doing so, are in notable contrast to similar studies of CPA and testosterone suppression in cisgender men that were published in the 1970s and 1980s. These studies consistently found that CPA suppressed testosterone levels by 40 to 70% on average (Aly, 2019). Subsequently, the findings were replicated in several more modern studies of CPA in cisgender men and transfeminine people, which likewise found that the drug given alone consistently suppressed testosterone levels by about 45 to 65% on average (Aly, 2019).
Spironolactone in Cisgender Women
Spironolactone has a long history of use in cisgender women in the treatment of androgen-dependent skin and hair conditions like acne, hirsutism, scalp hair loss, and hyperandrogenism (due to e.g. polycystic ovary syndrome (PCOS)). It has been used at similar doses for androgen-dependent conditions in cisgender women as it has in transfeminine people (e.g., 50–200 mg/day most typically). There are many dozens of studies of spironolactone as an antiandrogen in cisgender women (e.g., PubMed). Instead of attempting to individually review all of these studies, the present article will discuss the findings of several papers that have themselves reviewed substantial numbers of these studies and have summarized available findings on testosterone levels with spironolactone.
Callan (1988) reviewed the literature on spironolactone for treatment of acne and hirsutism in cisgender women and found that some clinical studies reported decreased levels of testosterone and/or other androgens with spironolactone (4 studies cited) whereas other studies reported no change in androgen levels (4 studies cited). The author cited several studies to support the claim that androgen receptor antagonism with spironolactone is more clinically important than any influence it has on androgen production (5 studies cited). For instance, clinical benefits against acne and hirsutism occurred with spironolactone both before androgen levels decrease as well as when androgen levels do not decrease.
McMullen & Van Herle (1993) reviewed 19 studies of spironolactone for treatment of androgen-dependent conditions in cisgender women, with a majority of these studies reporting long-term hormone levels. Most of the studies were open-label and uncontrolled, with only five studies having a control group and only two studies being double-blind placebo-controlled trials. Changes in hormone levels across studies were very heterogenous, with the majority of changes not reaching statistical significance. Only 1 of 7 (14%) studies found a decrease in DHEA-S levels. The review concluded that a clinically significant change in adrenal androgen levels with spironolactone in cisgender women was not supported. Conversely, testosterone levels were decreased with spironolactone in 13 of 16 (81%) of studies. However, in the only two RCTs, there were no differences in testosterone levels with spironolactone versus in the placebo control groups. As such, the review concluded that the decreased testosterone levels with spironolactone in cisgender women reported in many of the non-RCT studies may not actually be a real phenomenon. As with Callan (1988), the review noted that the major mechanism of action of spironolactone as an antiandrogen is likely to be androgen receptor blockade.
Bradstreet et al. (2007) cited and discussed a Cochrane review of spironolactone for treatment of acne and/or hirsutism in cisgender women (Farquhar et al., 2003). Cochrane reviews are rigorous high-quality systematic reviews of all of the available RCTs for a given medical intervention. The Cochrane review identified 19 RCTs, with 9 included in the review, 8 excluded due to methodological issues (e.g., with randomization), and two others which were described as “awaiting assessment” (Farquhar et al., 2003). Bradstreet and colleagues noted per the Cochrane review that spironolactone at a dosage of 100 mg/day had little influence on levels of DHEA, DHEA-S, or testosterone in the trials evaluated and said that this is because its mechanism of action as an antiandrogen is androgen receptor antagonism (Bradstreet et al., 2007). The Cochrane review itself did not discuss changes in androgen or testosterone levels with spironolactone in aggregate. An update of the Cochrane review was published in 2009, but with no new studies found and with the findings unchanged (Brown et al., 2009).
Layton et al. (2017) was a hybrid systematic review of spironolactone for acne in cisgender women. In a table discussing the mechanism of action of spironolactone and other antiandrogens for acne, the authors stated that “Data from over 50 articles reporting effects [of spironolactone] on serum androgens are equivocal” (i.e., ambiguous, uncertain, questionable) (Layton et al., 2017). The review further noted that inhibition of androgen synthesis by spironolactone in humans may be unlikely at therapeutic doses and may occur instead only at supraphysiological doses (with Menard et al. (1979) cited in support of these claims, presumably related to the very high doses required) (Layton et al., 2017).
Rozner et al. (2019) reviewed clinical studies of the endocrine effects of spironolactone in cisgender women to assess whether it is safe to use in women with past or present breast cancer receiving endocrine therapy. The review included 18 studies with 465 women (mostly having androgen-dependent conditions) assessing the influence of spironolactone on sex hormone levels. The assessed studies included retrospective cohort studies, case–control studies, and RCTs. Of the included studies, 10 (56%) studies (with 179 women) found no change in testosterone levels with spironolactone, 8 (44%) studies (with 253 women) found a decrease, and 1 (6%) study (with 33 women) found an increase in free but not total testosterone levels. Changes in levels of DHEA-S, androstenedione, and estrogen were also assessed and findings were similar, with no changes observed in majorities of studies for these hormones. The review concluded that there is no significant change in levels of androgens, estrogen, or gonadotropins with spironolactone in cisgender women.
Almalki et al. (2020) conducted a systematic review and network meta-analysis of RCTs on the comparative efficacy of several types of medications (statins, metformin, spironolactone, and combined birth control pills) on reducing testosterone levels in cisgender women specifically with PCOS. Nine RCTs including 613 women were included for all of the medications. The meta-analysis concluded that the statin atorvastatin was more effective than the other included medications in reducing testosterone levels. Only two of the included RCTs employed spironolactone, one of which was with spironolactone alone (n=34) versus metformin (n=35) (Ganie et al., 2004) and the other of which was with spironolactone plus metformin (n=62) versus spironolactone alone (n=51) versus metformin alone (n=56) (Ganie et al., 2013). Both of the included trials found that spironolactone alone significantly decreased testosterone levels in pre-treatment versus post-treatment comparisons (Ganie et al., 2004; Ganie et al., 2013). No trials of spironolactone versus placebo controls were included.
Taken together, the available studies of spironolactone and testosterone levels in cisgender women with androgen-dependent conditions are highly inconsistent and mixed, but with numerous studies finding no significant changes in testosterone levels. The reasons for the findings being so mixed are unclear, but may relate to study methodology and quality. Findings in this population seem particularly notable as regulation of the hypothalamic–pituitary–gonadal (HPG) axis by androgens in women is minimal to negligible, in turn making it such that androgen receptor antagonists will have little effect of upregulating gonadal sex hormone production as they can in cisgender men and transfeminine people. As a result, there is less homeostatic interference that could influence findings in evaluating the steroid synthesis inhibition of spironolactone in this sex, and hence these studies may provide a clearer picture of steroid synthesis inhibition as a possible clinical effect of spironolactone. However, as the findings are still so mixed, the results seem inconclusive. In any case, only a limited effect at best seems clear.
Spironolactone Alone in Transfeminine People
Only one study of spironolactone alone (without estrogen) and sex hormone levels in transfeminine people was identified (Table 2). It was conducted by Louis Gooren and colleagues of the Dutch Center of Expertise on Gender Dysphoria (CEGD) at the Vrije Universiteit Medical Center (VUMC) in Amsterdam, Netherlands in the 1980s. The study compared levels of testosterone, DHT, estradiol, LH, FSH, and prolactin before and after treatment with 200 mg/day spironolactone for 6 weeks in 6 young pre-hormone-therapy transfeminine people. It found slightly but significantly increased testosterone levels, increased prolactin levels, and no change in levels of estradiol, DHT, LH, or FSH.
Table 2: Studies of sex hormone levels with spironolactone alone in transfeminine people:
Treatment and subjects
Findings
Source(s)
200 mg/day for 6 weeks in 6 pre-hormone therapy transfeminine people (21–39 years)
T (mean ± SEM) increased significantly from 17.2 ± 0.8 nmol/L (496 ± 20 ng/dL) to 20.6 ± 1.7 nmol/L (594 ± 50 ng/dL) (+19.8%). No change in E2 (90 ± 20 pmol/L [25 ± 5.0 pg/mL] vs. 100 ± 30 pmol/L [27 ± 8.2 pg/mL] or 80 ± 20 pmol/L [22 ± 5.4 pg/mL]) or DHT (1.7 ± 0.8 nmol/L [49 ± 20 ng/dL] vs. 1.8 ± 0.9 nmol/L [52 ± 30 ng/dL]). LH, FSH, and GnRH-stimulated LH and FSH unchanged. PRL and TRH-stimulated PRL increased.
Abbreviations: T = testosterone; E2 = estradiol; DHT = dihydrotestosterone; LH = luteinizing hormone; FSH = follicle-stimulating hormone; GnRH = gonadotropin-releasing hormone; PRL = prolactin; TRH = thyrotropin-releasing hormone.
The fact that this study was done by the CEGD is notable as this institute is among the most prolific research centers on transgender hormone therapy in the world (Bakker, 2021), and, while they evaluated spironolactone as well as nilutamide as antiandrogens in studies in transfeminine people in the 1980s and 1990s (Wiki), the group ultimately settled on using only CPA instead. This was probably related to the lack of testosterone suppression with spironolactone and pure androgen receptor antagonists like nilutamide, as the researchers have touched on in other publications (e.g., Gooren, 1999).
Estrogen Plus Spironolactone in Transfeminine People
Eleven studies of the combination of estrogen and spironolactone and sex hormone levels in transfeminine people were identified (Table 3). The first study was conducted by Jerilynn Prior and colleagues in Canada in the 1980s. Subsequent studies were conducted over 25 years later by groups in the United States, Australia, Israel, and Thailand. All of the studies were retrospective chart reviews or prospective non-randomized studies, with the exception of a single RCT.
Table 3: Studies of testosterone levels with estrogen plus spironolactone in transfeminine people:
Treatment and subjects
Findings
Source(s)
Oral CEEs (0.625–5 mg/day cyclically—3 of 4 weeks per month), oral MPA (10–20 mg/day cyclically—3 of 4 weeks per month—or continuously—”if gonadotrophins increased or to aid in T reduction or breast development”), and spironolactone (100–600 mg/day continuously) for 12 months in 27 transfeminine people who had been on “high-dose” E alone for an extended duration (Group 1) and 23 transfeminine people who were pre-hormone-therapy (Group 2), or 50 transfeminine people total, at Vancouver General Hospital.
T decreased in Group 1 from mean 169 ng/dL to 87.4 ng/dL (–48.2%) and in Group 2 from mean 642 ng/dL to 49.2 ng/dL (–92.3%). In the groups combined, T following treatment would be mean 69.8 ng/dL. Per authors, spironolactone was intended to help reduce T and facilitate feminization while MPA was intended to help suppress gonadotropins and T and improve breast development. However, authors emphasized the decrease in T as being due to spironolactone despite inclusion of MPA, without data provided to substantiate this.
Sublingual estradiol (4 mg/day—2 mg b.i.d.) (n=14), transdermal estradiol patch (100 μg/day) (n=1), or injectable estradiol valerate (20 mg/2 weeks) (n=1) with spironolactone (100–200 mg/day) for 6 months in 16 transfeminine people at an LGBT community health center in Los Angeles, California.
T was median 405 ng/dL at baseline and 42 ng/dL after 6 months (–89.6%). Free T was median 11.4 ng/dL at baseline and 0.8 ng/dL at 6 months (–93.0%). 10 of 15 (66.7%) had total T in female range and 14 of 15 (93.3%) had free T in female range.
Oral E2 (1–8 mg/day) with or without spironolactone (200 mg/day) (n=61), finasteride (5 mg/day) (n=49), and/or MPA (2.5–10 mg/day) (n=38) for 0.3 to 10.5 years (mean 4.3 ± 3.1 years) in 156 transfeminine people at Albany Medical Center.
Oral E2 dose-dependently and substantially but incompletely suppressed T. Relative to E2 alone (at equivalent E2 levels), E2 plus spironolactone had no significant influence on T (+10.6 ± 16 ng/dL (mean ± SE); p = 0.5) and no greater likelihood of achieving better T suppression (<100 ng/dL) (OR = 0.75; 95% CI = 0.44–1.29). T levels with E2 alone were mean ~80 ng/dL and with E2 plus spironolactone were mean ~95 ng/dL per own re-analysis. Finasteride was also associated with greater T levels. MPA helped with T suppression in some (71% of subjects). More discussion and re-analysis including graphs (Aly, 2019).
Oral E2 (0.5–10 mg/day) (n=67) or oral CEEs (0.625–5 mg/day) (n=12) and spironolactone (25–400 mg/day; mean/median 145 mg/day) for 12 months in 98 transfeminine people at Boston Medical Center.
Combined E and spironolactone decreased T from median 385 ng/dL to 130 ng/dL (–66.2%). E alone vs. E and spironolactone not reported. No significant influence of spironolactone dosage on T. Incomplete suppression of T (>50 ng/dL) in all but the lowest quartile (25%) of individuals.
Oral EV (4–6 mg/day; median 5–6 mg/day) (88.3%) or transdermal E2 (11.7%) alone or in combination with CPA (25–50 mg/day; median 50 mg/day) or spironolactone (87.5–200 mg/day; median 100 mg/day) for 0.9 to 2.6 years (median 1.5 years) in 80 transfeminine people at two gender clinics in Melbourne, Australia.
T was median 10.5 nmol/L (303 ng/dL) with E2 only, 2.0 nmol/L (58 ng/dL) with E2 plus spironolactone, and 0.8 nmol/L (23 ng/dL) with E2 plus CPA. 90% of those on E2 plus CPA and 40% of those on E2 plus spironolactone had T of <2 nmol/L (<58 ng/dL). T significantly lower with E2 plus CPA compared to E2 plus spironolactone and E2 alone. T with E2 plus spironolactone lower than with E2 alone but non-significantly. No significant differences between groups in age, hormone therapy duration, or E2 dosage or levels. Graph that visually summarizes the results.
Sublingual estradiol (2–12 mg/day) and spironolactone (100–200 mg/day) with or without sublingual MPA (5–10 mg/day) or injectable MPA (150 mg/3 months) for 3.4 ± 1.7 years in 92 transfeminine people at Rhode Island Hospital.
T (mean ± SD) was 215 ± 29 ng/dL with E2 plus spironolactone and 79 ± 18 ng/dL with E2 plus spironolactone and MPA.
Oral E2 (2–8 mg/day) (84.2%) or other E forms (15.8%) with spironolactone (80.4%; n=107) or without spironolactone (19.6%) for more than 6 months in 133 transfeminine people at three clinics in Dallas, Texas.
T decreased from median 367 ng/dL (95% range 175–731 ng/dL) (n=70) at baseline to median 55 ng/dL (95% range 3–709 ng/dL) (n=131) in whole group (80.4% taking spironolactone). 65 of 133 (49%) had adequate T suppression (presumably <50 or <60 ng/dL) in whole group. T with E2 plus spironolactone at 25–75 mg/day (n=15) was mean 129.4 ng/dL (range <3—611 ng/dL), at 100–175 mg/day (n=61) was mean 180.4 ng/dL (range <3–1137 ng/dL), and at 200–300 mg/day (n=31) was mean 170.1 ng/dL (range <3–798 ng/dL). In the whole E2 plus spironolactone group (n=107), T would be mean 170.3 ng/dL.
Oral E2 (2–8 mg/day), transdermal E2 gel (2.5–5 mg/day), or transdermal E2 patches (50–200 μg/day) plus spironolactone (50–200 mg/day) (n=16), CPA (10–100 mg/day) (n=41), or a GnRH agonist (n=10) for 12 months in 67 transfeminine people at Tel Aviv-Sourasky Medical Center in Israel.
With spironolactone, T (mean ± SD) decreased from 15.2 ± 8.1 nmol/L (438 ± 230 ng/dL) at baseline to 10.2 ± 5.7 nmol/L (294 ± 164 ng/dL) at 3 months (–32.9%), 3.5 ± 1.2 nmol/L (100 ± 35 ng/dL) at 6 months (–77.0%), and 4 ± 7.1 nmol/L (120 ± 200 ng/dL) at 12 months (–73.7%). T was in the female range (<1.8 nmol/L [52 ng/dL]) at all follow-ups after baseline for both CPA and GnRH agonist (–92.0% to –96.4%).
Oral EV 4 mg/day plus spironolactone (100 mg/day) (n=26) or CPA (25 mg/day) (n=26) for 12 weeks in 52 transfeminine people at two clinics in Bangkok, Thailand (RCT).
With intention-to-treat analysis, T decreased with E2 plus spironolactone from median 645.0 ng/dL (IQR 466.7−1027.7 ng/dL) to 468.3 ng/dL (IQR 287.0−765.4 ng/dL) (–27.4%) and with E2 plus CPA from 655.5 ng/dL (402.6−872.7 ng/dL) to 9.3 ng/dL (IQR 5.5−310.4 ng/dL) (–98.6%). Adequate suppression of testosterone (<50 ng/dL) was achieved by 4 of 26 (15%) in the E2 plus spironolactone group and by 18 of 26 (69%) in the E2 plus CPA group. Study also assessed and reported E2, SHBG, and PRL levels.
E2 (sublingual, transdermal, or injectable) with spironolactone (n=39) or without spironolactone (n=37) for 12 months in 93 transfeminine people at two LGBTQ-oriented clinics in Seattle, Washington and Iowa City, Iowa.
T was median 11 to 18 ng/dL in different estradiol groups without spironolactone and median 10 to 12 ng/dL in different estradiol groups with spironolactone. T was significantly lower with spironolactone only for sublingual E2 group (median 11 ng/dL (IQR 6–35 ng/dL) [n=27] vs. median 18 ng/dL (IQR 13–205 ng/dL) [n=16]) and not for transdermal or injectable E2 groups.
Oral E2 (4–12 mg/day, median 6 mg/day) (n=27) or injectable EV (2–5 mg/week, median 4 mg/week) (n=6) with spironolactone (n=31) or without spironolactone (n=2) for median 6.2 months (range 0.6–28.2 months) (time on optimized E2 dose specifically) in 33 transfeminine people at Maine Medical Center.
T was median 13.0 ng/dL (range 2.7–559 ng/dL) for whole group (93.9% taking spironolactone). 28 of 33 (84.8%) of whole group had female-range T (<50 ng/dL). However, in earlier studies by the same group, similar T suppression with E2 alone was reported (Reardon et al., 2013; Spratt et al., 2014).
The data on the testosterone levels with estrogen plus spironolactone in transfeminine people from the 11 studies in the table can be roughly summarized. Some studies reported mean testosterone levels and some reported median testosterone levels, so these cases must be considered separately. In terms of reported mean testosterone levels across studies (4 studies), the median value of these study averages would be about 171 ng/dL and the range of study averages would be about 95 to 215 ng/dL. In terms of reported median testosterone levels across studies (7 studies), the median value of these study medians would be about 55 ng/dL and the range of study medians would be about 11 to 468 ng/dL. One study had to be excluded due to concomitant use of the progestogen medroxyprogesterone acetate (MPA) in all individuals (Prior, Vigna, & Watson, 1989; Prior et al., 1986). Insights from the preceding results include large variability in testosterone levels across studies and mean testosterone levels being much higher than median testosterone levels. Limitations of the preceding values include lack of equivalent estrogen and spironolactone dosages and levels across studies, lack of equivalent durations of hormone therapy across studies, lack of equivalent testosterone blood-testing methodologies across studies, lack of equivalent transfeminine patient samples, and, in the case of the study median testosterone values, two of the studies notably having almost all but not all individuals on spironolactone (80 and 94% rather than 100%). These limitations likely underlie the large variability in reported values across studies. In any case, these results suggest that estrogen plus spironolactone results in variably inadequate testosterone suppression in most transfeminine people, which is in notable major contrast to testosterone suppression with estrogen plus CPA or a GnRH agonist in transfeminine people.
Individual findings of the studies include inadequate testosterone suppression with estradiol plus spironolactone in most transfeminine people (Leinung et al., 2018; Liang et al., 2018; Jain, Kwan, & Forcier, 2019; Sofer et al., 2020; Burinkul et al., 2021), no difference in testosterone suppression with spironolactone versus without spironolactone (Leinung et al., 2018), lack of notable influence of spironolactone dosage on testosterone suppression (Liang et al., 2018; SoRelle et al., 2019), and inferior testosterone suppression with estradiol plus spironolactone compared to estradiol plus CPA or a GnRH agonist in transfeminine people (Angus et al., 2019; Sofer et al., 2020; Burinkul et al., 2021). Conversely, some studies have found adequate or near-adequate testosterone suppression with estradiol plus spironolactone in most or almost all transfeminine people (Deutsch, Bhakri, & Kubicek, 2015; Angus et al., 2019; SoRelle et al., 2019; Cirrincione et al., 2021; Pappas et al., 2021), and some studies have found indications of greater testosterone suppression with spironolactone versus without spironolactone (Angus et al., 2019; Cirrincione et al., 2021). On the other hand, some studies using estradiol alone without any antiandrogen at physiological estradiol levels (<200 pg/mL) have reported adequate testosterone suppression similarly to the preceding estradiol plus spironolactone studies (Reardon et al., 2013; Spratt et al., 2014; Cirrincione et al., 2021). One study was confounded by the concomitant use of MPA, which is known to suppress testosterone levels on its own, and hence reliable conclusions cannot not be drawn from this study (Prior, Vigna, & Watson, 1989; Prior et al., 1986). Indeed, it is notable that this study found lower mean testosterone levels with estrogen and spironolactone than any other study did. A couple of studies found that testosterone levels progressively decline with time (particularly over the first 12 months) with estradiol plus spironolactone in most transfeminine people (Liang et al., 2018; Sofer et al., 2020). Whether the decreases in testosterone levels with time were more related to estradiol or to spironolactone is unclear, though estradiol seems more likely (e.g., Wiki).
Taken together, the findings of available studies on estradiol plus spironolactone and testosterone suppression in transfeminine people are highly variable and mixed, although overall more studies support spironolactone having poor or no testosterone-suppressing effectiveness. The reasons underlying the differences in findings on testosterone suppression between studies are unclear, but contributing factors may include varying estradiol doses, routes, and levels, durations of hormone therapy, differing laboratory assays of testosterone levels, and other differences in study methodologies, as well as limitations in study and evidence quality. In any case, the conflicting nature of the findings is in major contrast to the almost invariably strong to maximal testosterone suppression in studies of estradiol plus CPA and estradiol plus GnRH agonists in transfeminine people.
Spironolactone, Androgen Receptor Antagonism, and Clinical Antiandrogenic Effectiveness
The clinical antiandrogenic effectiveness of spironolactone in cisgender women with androgen-dependent skin and hair conditions, like acne, hirsutism, and scalp hair loss, is well-established (Brown et al., 2009; van Zuuren & Fedorowicz, 2016; Layton et al., 2017; Barrionuevo et al., 2018; James, Jamerson, & Aguh, 2022; Wang et al., 2023). Conversely, the clinical antiandrogenic efficacy of spironolactone in transfeminine people has been very limitedly assessed to date and is largely unknown (Angus et al., 2021). Spironolactone does not appear to be very effective for decreasing testosterone levels in either cisgender women or transfeminine people based on the findings of the present review. However, spironolactone is a competitive antagonist of the androgen receptor in addition to its actions a weak androgen synthesis inhibitor, and hence it also directly blocks androgens from mediating their effects in the body (Loriaux et al., 1976; McMullen & Van Herle, 1993). Based on studies in populations besides transfeminine people, for instance cisgender women (discussed above) and cisgender boys with gonadotropin-independent precocious puberty (e.g., Holland, 1991), in which spironolactone has not decreased testosterone levels but has nonetheless been effective as an antiandrogen, the androgen receptor blockade of spironolactone is likely to be its main mechanism of action as an antiandrogen and may account for most or all of its therapeutic antiandrogenic effectiveness.
However, while spironolactone is clearly effective as an androgen receptor antagonist, it appears to be a relatively weak androgen receptor blocker at typical doses used in cisgender women and transfeminine people. Numerous publications in the literature describe spironolactone as being only a weak androgen receptor antagonist (Wiki; Wiki). In relation to this, animal studies have found that spironolactone is a far less potent androgen receptor antagonist than other antiandrogens like CPA, flutamide, and bicalutamide (Bonne & Raynaud, 1974; Hecker, Hasan, & Neumann, 1980; Sivelle, Underwood, & Jelly, 1982; Weissmann et al., 1985; Labrie et al., 1987; Snyder, Winneker, & Batzold, 1989 [Table]; Yamasaki et al., 2004 [Graph]). Moreover, in cisgender women, the population in which spironolactone is most widely used as an antiandrogen, testosterone levels are relatively low, on average about 20-fold lower than in cisgender men (around 30 ng/dL on average compared to about 600 ng/dL on average, respectively) (Aly, 2018). However, many cisgender women with androgen-dependent conditions have PCOS, which is associated with limitedly elevated testosterone levels (e.g., perhaps around 60 ng/dL on average) (Aly, 2018). The typical therapeutic dose range of spironolactone in cisgender women with androgen-dependent conditions is 50 to 200 mg/day, in which its effectiveness may be assumed to be dose-dependent, and this is roughly the same general dosage range used in transfeminine people (though up to 300–400 mg/day may be used and are allowed for by guidelines) (Aly, 2018; Aly, 2020).
A relatively small amount of dose-ranging data on spironolactone in cisgender women with androgen-dependent conditions exists, but in any case substantiates its dose-dependent effectiveness across its clinically used dose range (partially reviewed in Hammerstein (1990) and Shaw (1996)). One study compared spironolactone at doses of 50 to 200 mg/day with placebo for treatment of acne in cisgender women and reported progressive increases in effectiveness with spironolactone up to the 200 mg/day dosage (Goodfellow et al., 1984). Similarly, another study found that progressively increasing the dosage of spironolactone from 100 mg/day, to 150 mg/day, and up to 200 mg/day, resulted in increased effectiveness in the treatment of acne in cisgender women (Charny, Choi, & James, 2017). Spironolactone has been reported to be effective in the treatment of hirsutism in cisgender women at a dosage of as low as 50 mg/day (Diamanti-Kandarakis, Tolis, & Duleba, 1995). However, even a dosage of 100 mg/day did not appear to be maximally effective for hirsutism in a study that compared different doses of spironolactone; effectiveness was near-significantly greater at a dosage of 100 mg/day relative to a dosage of 200 mg/day (19% ± 8% and 30% ± 3% (mean ± SEM) reduction in hair shaft diameter, respectively; p = 0.07) (Lobo et al., 1985). Levels of free testosterone in this study were unchanged, suggesting that the effects of spironolactone was purely due to androgen receptor blockade. Finally, a 2022 systematic review of spironolactone for treatment of androgen-related scalp hair loss in cisgender women reported that the drug was “largely ineffective” at doses of less than 100 mg/day, whereas doses of 100 to 200 mg/day were effective (James, Jamerson, & Aguh, 2022).
Aside from dose-ranging studies, the antiandrogenic efficacy of spironolactone can be evaluated by comparing it to more potent antiandrogenic regimens. A study found that spironolactone 100 mg/day was significantly inferior to flutamide, a substantially more potent androgen receptor antagonist, in improving androgen-dependent skin and hair symptoms in cisgender women (Cusan et al., 1994). However, in other studies, there were no significant differences between spironolactone 100 mg/day and flutamide for hirsutism (Erenus et al., 1994; Moghetti et al., 2000; Inal, Yildirim, & Taner, 2005; Karakurt et al., 2008). Spironolactone and flutamide were variably taken together with an ethinylestradiol-containing combined birth control pill in these studies, which is likely to have limited detection of differences in effectiveness. This is because these birth control pills considerably suppress total and free testosterone levels and hence have substantial antiandrogenic effects themselves (Zimmerman et al., 2014; Amiri et al., 2018). In a biochemical study, spironolactone 100 mg/day was numerically inferior to flutamide in reducing levels of prostate-specific antigen (PSA) in cisgender women (Negri et al., 2000). This is notable as PSA is a systemic biomarker of androgen action (Negri et al., 2000). However, the study had small sample sizes, and the differences between groups were not statistically significant (Negri et al., 2000). A case report of a cisgender woman with female pattern hair loss and normal androgen levels found that treatment with spironolactone 200 mg/day for 5 years failed to improve or halt progression of her hair loss, in spite of almost complete loss of secondary sexual hair, but switching to flutamide resulted in a considerable improvement in hair loss after 12 months (Yazdabadi & Sinclair, 2011 [Figure]). Besides comparison with flutamide, a study found that spironolactone 100 mg/day was inferior to spironolactone 100 mg/day plus finasteride, a 5α-reductase inhibitor and hence functional antiandrogen, for hirsutism in cisgender women (–36.6% vs. –51.3% in scores; p < 0.005) (Unlühizarci et al., 2002; Keleştimur et al., 2004).
The preceding findings suggest that the clinical antiandrogenic effectiveness of spironolactone in cisgender women is not maximal at a dosage of below at least 200 mg/day despite the relatively low testosterone levels in these individuals. Put another way, spironolactone at typical doses seems best-suited for blocking female-range levels of testosterone. As many transfeminine people do not achieve female-range testosterone levels with estradiol plus spironolactone therapy, and in fact often have testosterone levels well above the normal female range or even in the male range, spironolactone may not be fully effective as an antiandrogen at the typical doses used in transfeminine hormone therapy. Higher doses of spironolactone, like 300 to 400 mg/day, may be to some degree more effective.
Summary, Discussion, and Conclusions
Numerous studies have assessed the influence of spironolactone on testosterone levels in cisgender men, cisgender women, and transfeminine people. Although the quality of these studies has often been limited, the studies have revealed highly inconsistent influences of spironolactone on testosterone levels in these populations, with many studies finding no changes, some studies finding decreases, and a small number of studies finding increases. The findings of studies of spironolactone and testosterone levels are in notable contrast to those of studies with estrogens, progestogens like CPA, and GnRH agonists, which consistently show substantial decreases in testosterone levels. This has been the case even in studies of similarly low quality to those of some of the included spironolactone studies (e.g., many of those in cisgender men). The fact that in the available studies testosterone levels with spironolactone have usually been unchanged, but have sometimes been decreased and have rarely been decreased, seems to suggest that spironolactone may be a clinically significant inhibitor of steroid hormone synthesis, but that it is only a weakly efficacious one, and that its effects may be variable depending on the individual and other clinical circumstances. In any case, the conflicting findings warrant more research with higher-quality study designs, particularly RCTs that have with spironolactone versus without comparison groups.
The notion that spironolactone decreases testosterone levels in transfeminine people, and the use of spironolactone in transfeminine hormone therapy in general, appear to have originated from the papers on spironolactone in transfeminine people published by Dr. Jerilynn Prior and colleagues in the 1980s (Prior, Vigna, & Watson, 1989; Prior et al., 1986). In their study, transfeminine people who were either already on high-dose estrogen therapy with inadequate testosterone suppression or had not yet started hormone therapy were put on physiological-dose estrogen therapy in combination with 200 to 600 mg/day spironolactone. Cyclic or continuous administration of the progestogen MPA at an oral dose of 10 mg/day was also given to all of the individuals. The authors reported that despite the lower estrogen dosage, testosterone levels decreased, from 169 ng/dL to 87 ng/dL (–49%) in those who had already been on hormone therapy and to 49 ng/dL in those who were pre-hormone therapy. Prior and her colleagues concluded that spironolactone helps to decrease testosterone levels in transfeminine people and that it can be used as a safer alternative to high doses of estrogen for this purpose.
However, the concomitant use of MPA in the study is a major confounding factor in terms of their results. This is because MPA is a progestogen, and progestogens, like estrogens, are antigonadotropins which are able to robustly suppress testosterone levels on their own (Aly, 2018; Aly, 2019). Indeed, MPA alone has been shown to dose-dependently lower testosterone levels in cisgender men (Wiki), and at a dosage of 10 mg/day, has been shown to considerably suppress testosterone levels in transfeminine people when added to estradiol and spironolactone therapy (Jain, Kwan, & Forcier, 2019). Hence, MPA may have been, and likely was, responsible for the decreases in testosterone levels seen in the study, rather than spironolactone. This point was also notably raised by other researchers, who were unable to replicate Prior and colleagues’ results on spironolactone and testosterone levels in transfeminine people (Leinung et al., 2018). Strangely, Prior and colleagues concluded that spironolactone was responsible for the decreased testosterone levels in their study even though they noted in their papers that MPA was also given to help suppress testosterone levels (as well as to help improve breast development). The work of Prior and colleagues likely resulted in the prominent and long-standing, but poorly supported, notion that spironolactone decreases testosterone levels in transfeminine people. Subsequent studies assessing the hypothesis that spironolactone decreases testosterone levels in transfeminine people were not published until 25 years after Prior and colleagues’ studies, with several of these studies, though not all of them, failing to replicate the earlier findings of Prior and colleagues.
Many people do not realize the capacity of estradiol to substantially and even completely suppress testosterone, and many mistakenly assume that it is the antiandrogen—which is often spironolactone—that is mostly or fully responsible for the decrease in testosterone levels seen with estradiol and antiandrogen therapy in transfeminine people. It is certainly true that antiandrogens like CPA and GnRH agonists play an important role in testosterone suppression in transfeminine people. However, as evidenced by the present review of studies of testosterone suppression with spironolactone, it is not necessarily always the case that the antiandrogen plays a major role—or potentially even any role—in reducing testosterone levels. This is notably also not the case with certain other antiandrogens besides spironolactone, for instance pure androgen receptor antagonists like bicalutamide, which likewise do not decrease testosterone levels but instead can actually increase them (Aly, 2019; Wiki). Clinicians and transfeminine people attributing observations of testosterone decreases to spironolactone rather than to estradiol with estradiol and spironolactone therapy may also have played a role in the perception that spironolactone considerably decreases testosterone levels in transfeminine people.
Due to its relatively weak strength as an androgen receptor antagonist and its limited efficacy in lowering testosterone levels, spironolactone is likely to be a limitedly effective antiandrogen in transfeminine people. Additionally, spironolactone is likely to be less effective than other antiandrogenic approaches used in transfeminine hormone therapy which either more robustly block androgens or more substantially reduce testosterone levels, for instance CPA, other progestogens (e.g., MPA, non-oral progesterone), GnRH agonists (and antagonists), bicalutamide, and high-dose parenteral estradiol monotherapy. These approaches can be used in transfeminine people instead of or in addition to spironolactone, or could be considered when testosterone suppression is inadequate with estradiol and spironolactone.
More studies are needed to evaluate the influence of spironolactone on testosterone levels, especially RCTs that compare estradiol alone versus estradiol plus spironolactone in transfeminine people. More research is also needed to clarify why some studies find highly inadequate testosterone suppression with estradiol alone or estradiol plus spironolactone while other studies find excellent or satisfactory testosterone suppression with these regimens. In any case, available data overall suggest that spironolactone does not consistently suppress testosterone levels, and that estradiol plus spironolactone produces inadequate testosterone suppression in many transfeminine people. Moreover, available data suggest that spironolactone is a relatively weak androgen receptor antagonist at the typical clinical doses used in cisgender women and transfeminine people, and is able to block only relatively low or female-range testosterone levels. Hence, spironolactone may not be fully effective in blocking the testosterone it fails to suppress, and may be particularly unsuitable for transfeminine people with testosterone levels that are well above the normal female range. In any case, more research is similarly needed to assess the androgen receptor antagonism and clinical antiandrogenic effectiveness of spironolactone.
Updates
Update 1: Spironolactone for Adult Female Acne (SAFA) Trial
A large new phase 3 RCT, the Spironolactone for Adult Female Acne (SAFA) trial, was published in May 2023 and assessed the effectiveness of spironolactone in the treatment of acne in cisgender women:
Santer, M., Lawrence, M., Renz, S., Eminton, Z., Stuart, B., Sach, T. H., Pyne, S., Ridd, M. J., Francis, N., Soulsby, I., Thomas, K., Permyakova, N., Little, P., Muller, I., Nuttall, J., Griffiths, G., Thomas, K. S., & Layton, A. M. (2023). Effectiveness of spironolactone for women with acne vulgaris (SAFA) in England and Wales: pragmatic, multicentre, phase 3, double blind, randomised controlled trial. BMJ, 381, e074349. [DOI:10.1136/bmj-2022-074349]
The trial included a total of 342 women, including 176 treated with spironolactone and 166 in the placebo control group. The dose of spironolactone employed was 50 mg/day for the first 6 weeks and then 100 mg/day thereafter. The trial was 24 weeks (5.5 months) in duration. Women who might become pregnant were required to use a hormonal or barrier method of contraception.
Spironolactone significantly outperformed placebo in terms of improvement in mean Acne-QoL symptom scores (higher is better). Significant improvement was apparent within 12 weeks of treatment (+45% in scores with spironolactone, +38% with placebo) and was highest at 24 weeks (+61% in scores with spironolactone, +35% with placebo). There was no difference in the rates of women who reported improvement in acne scores at 12 weeks (72% with spironolactone, 68% with placebo), but there was a significant difference at 24 weeks (82% with spironolactone, 63% with placebo). In terms of the Investigator’s Global Assessment (IGA), treatment success at 12 weeks was 19% with spironolactone and 6% with placebo. Rates of hormonal contraceptive use in the spironolactone and placebo groups were not reported. Testosterone levels were also not reported. A small subset of the women had PCOS (15% in the spironolactone group, 23% in the placebo group).
Adverse effects occurred only slightly more often with spironolactone than with placebo (64% vs. 51%, p = 0.01). The only side effect that occurred significantly more often with spironolactone than with placebo was headache (20% vs. 12%; p = 0.02). However, a few other side effects trended towards occurring significantly more frequently with spironolactone than with placebo: “other” (17% vs. 11%; p = 0.06), dizziness/vertigo/lightheadness (19% vs. 12%; p = 0.07), vomiting/being sick (2% vs. 1%; p = 0.16), and polyuria (urinary frequency) (31% vs. 25%; p = 0.18). Rates of other potentially relevant side effects, like abdominal pain, breast enlargement, breast tenderness, drowsiness/sleepiness, fatigue/tiredness, menstrual irregularity, and reduced libido, were all not different between spironolactone and placebo. There were no serious adverse reactions in the trial. Rates of compliance were similar between the spironolactone and placebo groups, suggesting that spironolactone was well-tolerated.
This trial is the largest and most rigorous RCT of spironolactone in the treatment of androgen-dependent skin and hair conditions in cisgender women that has been conducted to date. Although spironolactone was found to be effective in this study and was about twice as effective as placebo in terms of Acne-QoL symptom scores and three times as effective as placebo in terms of IGA treatment success rates, the effectiveness of spironolactone was seemingly less than in previous clinical studies of spironolactone for acne. This may be related to the relatively low doses of spironolactone used in this study (50–100 mg/day), to the more rigorous and less-risk-of-bias design of the study (large phase 3 RCT), to a possibly too-short treatment duration (24 weeks/5.5 months), and to concomitant hormonal contraceptive use possibly blunting the degree of potential improvement. The latter is relevant as hormonal contraceptives containing ethinylestradiol provide a considerable improvement in acne via functional antiandrogenic effects all on their own. A final possibility however is that spironolactone is simply a less effective antiandrogen even in cisgender women than has been previously thought. On the other hand, similarly to findings in previous clinical studies, spironolactone was well-tolerated and produced few side effects.
Update 2: New Spironolactone and Testosterone Suppression Studies
The following new studies have additionally assessed and found inadequate testosterone suppression in transfeminine people treated with estradiol and spironolactone:
Angus, L. M., Leemaqz, S., Zajac, J. D., & Cheung, A. S. (November 2023). A randomised controlled trial of spironolactone versus cyproterone in trans people commencing estradiol. AusPATH 2023 Symposium. [URL] [PDF] [Trans Health Research Blog Post]
Angus, L. M., Leemaqz, S. Y., Zajac, J. D., & Cheung, A. S. (November 2023). The effect of cyproterone and spironolactone on breast development in transgender women: a randomised controlled trial. ESA/SRB/ENSA 2023 ASM 26-29 November, Brisbane, 54–55 (abstract no. 132). [URL] [PDF] [Full Abstract Book] [Trans Health Research Blog Post]
Miro, E., Rizzone, K., Ho, T., Mark, B., Sullivan, E., & Cushman, D. (2024). 2024 AMSSM Research Podium Presentations: Testosterone Levels Among Transgender Women on Gender-affirming Hormone Therapy. Clinical Journal of Sports Medicine, 34(2), 152–152. [DOI:10.1097/JSM.0000000000001212]
Yang, W., Hong, T., Chang, X., Han, M., Gao, H., Pan, B., Zhao, Z., & Liu, Y. (2024). The efficacy of and user satisfaction with different antiandrogens in Chinese transgender women. International Journal of Transgender Health, advance online publication. [DOI:10.1080/26895269.2024.2323514]
Angus et al. (2023) and Yang et al. (2024) compared estradiol plus spironolactone to estradiol plus CPA and are described in-depth in a section of a different article located here. Yang et al. (2024) found that in addition to spironolactone resulting in much less testosterone suppression than CPA, it was also less effective than CPA as an antiandrogen on multiple clinical measures of demasculinization.
References
Abshagen, U., Spörl, S., Schöneshöfer, M., L’age, M., & Oelkers, W. (1978). Interference of spironolactone therapy with adrenal steroid metabolism in secondary hyperaldosteronism. [Zum Einfluß einer Spironolaktonbehandlung auf den adrenalen Steroidstoffwechsel bei sekundärem Hyperaldosteronismus.] Klinische Wochenschrift, 56(7), 341–349. [DOI:10.1007/bf01477394]
Aizawa, H., & Niimura, M. (1992). Oral Spironolactone Therapy in Male Patients with Rosacea. The Journal of Dermatology, 19(5), 293–297. [DOI:10.1111/j.1346-8138.1992.tb03227.x]
Allen, A. N., Jiao, R., Day, P., Pagels, P., Gimpel, N., & SoRelle, J. A. (2020). Dynamic Impact of Hormone Therapy on Laboratory Values in Transgender Patients over Time. The Journal of Applied Laboratory Medicine, 6(1), 27–40. [DOI:10.1093/jalm/jfaa192]
Almalki, H. H., Alshibani, T. M., Alhifany, A. A., & Almohammed, O. A. (2020). Comparative efficacy of statins, metformin, spironolactone and combined oral contraceptives in reducing testosterone levels in women with polycystic ovary syndrome: a network meta-analysis of randomized clinical trials. BMC Women’s Health, 20(1), 68. [DOI:10.1186/s12905-020-00919-5]
Amiri, M., Kabir, A., Nahidi, F., Shekofteh, M., & Ramezani Tehrani, F. (2018). Effects of combined oral contraceptives on the clinical and biochemical parameters of hyperandrogenism in patients with polycystic ovary syndrome: a systematic review and meta-analysis. The European Journal of Contraception & Reproductive Health Care, 23(1), 64–77. [DOI:10.1080/13625187.2018.1435779]
Angus, L., Leemaqz, S., Ooi, O., Cundill, P., Silberstein, N., Locke, P., Zajac, J. D., & Cheung, A. S. (2019). Cyproterone acetate or spironolactone in lowering testosterone concentrations for transgender individuals receiving oestradiol therapy. Endocrine Connections, 8(7), 935–940. [DOI:10.1530/ec-19-0272]
Angus, L. M., Leemaqz, S., Zajac, J. D., & Cheung, A. S. (2023). A randomised controlled trial of spironolactone versus cyproterone in trans people commencing estradiol. AusPATH 2023 Symposium. [URL] [PDF] [Trans Health Research Blog Post]
Angus, L. M., Leemaqz, S. Y., Zajac, J. D., & Cheung, A. S. (2023). The effect of cyproterone and spironolactone on breast development in transgender women: a randomised controlled trial. ESA/SRB/ENSA 2023 ASM 26-29 November, Brisbane, 54–55 (abstract no. 132). [URL] [PDF] [Full Abstract Book] [Trans Health Research Blog Post]
Angus, L. M., Nolan, B. J., Zajac, J. D., & Cheung, A. S. (2021). A systematic review of antiandrogens and feminization in transgender women. Clinical Endocrinology, 94(5), 743–752. [DOI:10.1111/cen.14329]
Baba, S. (1977). Antiandrogenic effect of spironolactone. The Japanese Journal of Urology, 68(12), 1184–1192. [DOI:10.5980/jpnjurol1928.68.12_1184]
Baba, S., Murai, M., Jitsukawa, S., Hata, M., & Tazaki, H. (1978). Antiandrogenic Effects of Spironolactone: Hormonal and Ultrastructural Studies in Dogs and Men. Journal of Urology, 119(3), 375–380. [DOI:10.1016/s0022-5347(17)57495-9]
Bakker, A. (2021). Een halve eeuw transgenderzorg aan de VU [Half a Century of Transgender Care at the VU]. Amsterdam: Boom. [Google Books] [WorldCat] [URL]
Barrionuevo, P., Nabhan, M., Altayar, O., Wang, Z., Erwin, P. J., Asi, N., Martin, K. A., & Murad, M. H. (2018). Treatment Options for Hirsutism: A Systematic Review and Network Meta-Analysis. The Journal of Clinical Endocrinology & Metabolism, 103(4), 1258–1264. [DOI:10.1210/jc.2017-02052]
Bonne, C., & Raynaud, J. (1974). Mode of spironolactone anti-androgenic action: Inhibition of androstanolone binding to rat prostate androgen receptor. Molecular and Cellular Endocrinology, 2(1), 59–67. [DOI:10.1016/0303-7207(74)90012-4]
Bonzagni, A. F. (2014). Understanding the effects of long-term hormone therapy in transgender individuals being provided care at Boston Medical Center Endocrinology Clinic: a quality assurance project. (Doctoral dissertation, Boston University.) [Google Scholar] [URL] [PDF]
Bradstreet, J. J., Smith, S., Granpeesheh, D., El-Dahr, J. M., & Rossignol, D. (2007). Spironolactone might be a desirable immunologic and hormonal intervention in autism spectrum disorders. Medical Hypotheses, 68(5), 979–987. [DOI:10.1016/j.mehy.2006.10.015]
Brown, J., Farquhar, C., Lee, O., Toomath, R., & Jepson, R. G. (2003). Spironolactone versus placebo or in combination with steroids for hirsutism and/or acne. Cochrane Database of Systematic Reviews, 2003(4), CD000194. [DOI:10.1002/14651858.cd000194]
Brown, J., Farquhar, C., Lee, O., Toomath, R., & Jepson, R. G. (2009). Spironolactone versus placebo or in combination with steroids for hirsutism and/or acne. Cochrane Database of Systematic Reviews, 2009(2), CD000194. [DOI:10.1002/14651858.cd000194.pub2]
Burinkul, S., Panyakhamlerd, K., Suwan, A., Tuntiviriyapun, P., & Wainipitapong, S. (2021). Anti-Androgenic Effects Comparison Between Cyproterone Acetate and Spironolactone in Transgender Women: A Randomized Controlled Trial. The Journal of Sexual Medicine, 18(7), 1299–1307. [DOI:10.1016/j.jsxm.2021.05.003] [PDF]
Callan, A. W. (1988). Spironolactone therapy in hirsutism and acne. Australasian Journal of Dermatology, 29(3), 135–139. [DOI:10.1111/j.1440-0960.1988.tb00385.x]
Caminos-Torres, R., MA, L., & Snyder, P. J. (1977). Gynecomastia and Semen Abnormalities Induced by Spironolactone in Normal Men. The Journal of Clinical Endocrinology & Metabolism, 45(2), 255–260. [DOI:10.1210/jcem-45-2-255]
Charny, J., Choi, J., & James, W. (2017). Spironolactone for the treatment of acne in women, a retrospective study of 110 patients. International Journal of Women’s Dermatology, 3(2), 111–115. [DOI:10.1016/j.ijwd.2016.12.002]
Cheung, A. S., Ooi, O., Davidoff, D., Leemaqz, S. Y., Cundill, P., Silberstein, N., Bretherton, I., Grossmann, M., & Zajac, J. D. (2018). Cyproterone vs spironolactone as anti-androgen therapy for transgender females receiving oestradiol therapy. Clinical Endocrinology, 89(S1) [Abstracts of the Endocrine Society of Australia’s Annual Scientific Meeting 2017], 14–14 (abstract no. 62). [Google Scholar] [DOI:10.1111/cen.13727] [URL 1] [URL 2] [PDF]
Cirrincione, L. R., Winston McPherson, G., Rongitsch, J., Sadilkova, K., Drees, J. C., Krasowski, M. D., Dickerson, J. A., & Greene, D. N. (2021). Sublingual Estradiol Is Associated with Higher Estrone Concentrations than Transdermal or Injectable Preparations in Transgender Women and Gender Nonbinary Adults. LGBT Health, 8(2), 125–132. [DOI:10.1089/lgbt.2020.0249]
Corvol, P., Mahoudeau, J. A., Valcke, J. C., Ménard, J., & Bricaire, H. (1976). Effets sexuels secondaires des spirolactones. Mécanismes possibles de l’action antiandrogène. [Sexual side-effects of spironolactones. Possible mechanisms of their anti-androgen action]. La Nouvelle Presse Medicale, 5(11), 691–694. [Google Scholar 1] [Google Scholar 2] [PubMed] [PDF]
Cusan, L., Dupont, A., Gomez, J., Tremblay, R. R., & Labrie, F. (1994). Comparison of flutamide and spironolactone in the treatment of hirsutism: a randomized controlled trial. Fertility and Sterility, 61(2), 281–287. [DOI:10.1016/s0015-0282(16)56518-2]
Deutsch, M. B., Bhakri, V., & Kubicek, K. (2015). Effects of Cross-Sex Hormone Treatment on Transgender Women and Men. Obstetrics & Gynecology, 125(3), 605–610. [DOI:10.1097/aog.0000000000000692]
Diamanti-Kandarakis, E., Tolis, G., & Duleba, A. J. (1995). Androgens and Therapeutic Aspects of Antiandrogens in Women. Journal of the Society for Gynecologic Investigation, 2(4), 577–592. [DOI:10.1177/107155769500200401]
Dymling, J., Nilsson, K. O., & Hökfelt, B. (1972). The effect of Soldactona® (canrenoate potassium) on plasma testosterone and androstenedione and urinary 17-ketosteroids and 17-hydroxycorticosteroids. Acta Endocrinologica, 70(1), 104–112. [DOI:10.1530/acta.0.0700104]
Dymling, J. F., & Hökfelt, B. (1973). Reduced plasma testosterone following spirolactone in man. Acta Endocrinologica, 73(Suppl 177) [9th Acta Endocrinologica Congress], 53–53 (abstract no. 53). [Google Scholar] [PDF 1] [PDF 2]
Dymling, J. F. (1978). The effect of spirolactone and spironolactone on plasma testosterone in man. In Addison, G. M., Asmussen, N. W., Corvol, P., Kloppernborg, P. W. C., Norman, N., Schroder, R., & Robertson, J. I. C. (Eds.). Aldosterone Antagonists in Clinical Medicine: Proceedings of the Searle Symposium, Nice, April 13–15, 1978 (pp. 297–302). Amsterdam: Excerpta Medica. [Google Scholar] [Google Books] [WorldCat] [PDF 1] [PDF 2]
Erbler, H. C. (1974). Suppression by the spironolactone metabolite canrenone of plasma testosterone in man. Naunyn-Schmiedeberg’s Archives of Pharmacology, 285(4), 403–406. [DOI:10.1007/bf00501468]
Erenus, M., Gürbüz, O., Durmuşoğlu, F., Demirçay, Z., & Pekin, S. (1994). Comparison of the efficacy of spironolactone versus flutamide in the treatment of hirsutism. Fertility and Sterility, 61(4), 613–616. [DOI:10.1016/s0015-0282(16)56634-5]
Ganie, M. A., Khurana, M. L., Eunice, M., Gulati, M., Dwivedi, S. N., & Ammini, A. C. (2004). Comparison of Efficacy of Spironolactone with Metformin in the Management of Polycystic Ovary Syndrome: An Open-Labeled Study. The Journal of Clinical Endocrinology & Metabolism, 89(6), 2756–2762. [DOI:10.1210/jc.2003-031780]
Ganie, M. A., Khurana, M. L., Nisar, S., Shah, P. A., Shah, Z. A., Kulshrestha, B., Gupta, N., Zargar, M. A., Wani, T. A., Mudasir, S., Mir, F. A., & Taing, S. (2013). Improved Efficacy of Low-Dose Spironolactone and Metformin Combination Than Either Drug Alone in the Management of Women With Polycystic Ovary Syndrome (PCOS): A Six-Month, Open-Label Randomized Study. The Journal of Clinical Endocrinology & Metabolism, 98(9), 3599–3607. [DOI:10.1210/jc.2013-1040]
Goodfellow, A., Alaghband-Zadeh, J., Carter, G., Cream, J., Holland, S., Scully, J., & Wise, P. (1984). Oral spironolactone improves acne vulgaris and reduces sebum excretion. British Journal of Dermatology, 111(2), 209–214. [DOI:10.1111/j.1365-2133.1984.tb04045.x]
Gooren, L. J., Veen, E. A., Kessel, H., Harmsen-Louman, W., & Wiegel, A. R. (1984). Prolactin secretion in the human male is increased by endogenous oestrogens and decreased by exogenous/endogenous androgens. International Journal of Andrology, 7(1), 53–60. [DOI:10.1111/j.1365-2605.1984.tb00759.x]
Gooren, L., Veen, E., Kessel, H., Harmsen-Louman, W., & Wiegel, A. (1984). Androgens in the Feedback Regulation of Gonadotropin Secretion in Men: Effects of Administration of Dihydrotestosterone to Eugonadal and Agonadal Subjects and of Spironolactone to Eugonadal Subjects. Andrologia, 16(4), 289–298. [DOI:10.1111/j.1439-0272.1984.tb00286.x]
Gooren, L. J. G. (1999). Hormonal Sex Reassignment. International Journal of Transgenderism, 3(3), 1–7. [Google Scholar] [URL 1] [URL 2]
Hammerstein, J. (1990). Antiandrogens: Clinical Aspects. In Orfanos, C. E., & Happle, R. (Eds.). Hair and Hair Diseases (pp. 827–886). Berlin/Heidelberg: Springer. [DOI:10.1007/978-3-642-74612-3_35]
Handelsman, D. J., Strasser, S., McDonald, J. A., Conway, A. J., & McCaughan, G. W. (1995). Hypothalamic-pituitary-testicular function in end-stage non-alcoholic liver disease before and after liver transplantation. Clinical Endocrinology, 43(3), 331–337. [DOI:10.1111/j.1365-2265.1995.tb02040.x]
Hecker, A., Hasan, S. H., & Neumann, F. (1980). Disturbances in sexual differentiation of rat foetuses following spironolactone treatment. Acta Endocrinologica, 95(4), 540–545. [DOI:10.1530/acta.0.0950540]
Holland, F. J. (1991). Gonadotropin-lndependent Precocious Puberty. Endocrinology and Metabolism Clinics of North America, 20(1), 191–210. [DOI:10.1016/s0889-8529(18)30288-3]
Horth, C., Lobo, P., Shelton, J., Asbury, M., Clarke, J., & Venning, G. (1977). Effects of spironolaetone on the plasma binding and unbound levels of testosterone and oestradiol in healthy men. Journal of Steroid Biochemistry, 8(12), xx–xx. [DOI:10.1016/0022-4731(77)90178-9]
Horth, C. E., Lobo, P. J., Shelton, J. R., Asbury, M. J., Clarke, J. M., & Venning, G. R. (1979). Effects of spironolactone on the plasma binding and unbound levels of testosterone and oestradiol in healthy men. In Klopper, A., Lerner, L., van der Molen, H. J., & Sciarra, F. (Eds.). Research on Steroids: Proceedings of the International Study Group for Steroid Hormones, Volume 8 / Research on Steroids Transactions of the Eighth Meeting of the International Study Group for Steroid Hormones (Proceedings of the Serono Symposia, Volume 21) (pp. 313–315). London/New York/San Francisco: Academic Press. [Google Scholar]
Huffman, D. H., Kampmann, J. P., Hignite, C. E., & Azarnoff, D. L. (1978). Gynecomastia induced in normal males by spironolactone. Clinical Pharmacology & Therapeutics, 24(4), 465–473. [DOI:10.1002/cpt1978244465]
Inal, M. M., Yildirim, Y., & Taner, C. E. (2005). Comparison of the clinical efficacy of flutamide and spironolactone plus Diane 35 in the treatment of idiopathic hirsutism: a randomized controlled study. Fertility and Sterility, 84(6), 1693–1697. [DOI:10.1016/j.fertnstert.2005.05.051]
Jain, J., Kwan, D., & Forcier, M. (2019). Medroxyprogesterone Acetate in Gender-Affirming Therapy for Transwomen: Results From a Retrospective Study. The Journal of Clinical Endocrinology & Metabolism, 104(11), 5148–5156. [DOI:10.1210/jc.2018-02253]
James, J. F., Jamerson, T. A., & Aguh, C. (2022). Efficacy and safety profile of oral spironolactone use for androgenic alopecia: A systematic review. Journal of the American Academy of Dermatology, 86(2), 425–429. [DOI:10.1016/j.jaad.2021.07.048]
Karakurt, F., Sahin, I., Güler, S., Demirbas, B., Culha, C., Serter, R., Aral, Y., & Bavbek, N. (2008). Comparison of the clinical efficacy of flutamide and spironolactone plus ethinyloestradiol/cyproterone acetate in the treatment of hirsutism: A randomised controlled study. Advances in Therapy, 25(4), 321–328. [DOI:10.1007/s12325-008-0039-5]
Keleştimur, F., Everest, H., Unlühizarci, K., Bayram, F., & Șahin, Y. (2004). A comparison between spironolactone and spironolactone plus finasteride in the treatment of hirsutism. European Journal of Endocrinology, 150(3), 351–354. [DOI:10.1530/eje.0.1500351]
Labrie, C., Cusan, L., Plante, M., Lapointe, S., & Labrie, F. (1987). Analysis of the androgenic activity of synthetic “progestins” currently used for the treatment of prostate cancer. Journal of Steroid Biochemistry, 28(4), 379–384. [DOI:10.1016/0022-4731(87)91054-5]
Layton, A. M., Eady, E. A., Whitehouse, H., Del Rosso, J. Q., Fedorowicz, Z., & van Zuuren, E. J. (2017). Oral Spironolactone for Acne Vulgaris in Adult Females: A Hybrid Systematic Review. American Journal of Clinical Dermatology, 18(2), 169–191. [DOI:10.1007/s40257-016-0245-x]
Leinung, M. C., Feustel, P. J., & Joseph, J. (2018). Hormonal Treatment of Transgender Women with Oral Estradiol. Transgender Health, 3(1), 74–81. [DOI:10.1089/trgh.2017.0035]
Liang, J. J., Jolly, D., Chan, K. J., & Safer, J. D. (2018). Testosterone Levels Achieved by Medically Treated Transgender Women in a United States Endocrinology Clinic Cohort. Endocrine Practice, 24(2), 135–142. [DOI:10.4158/ep-2017-0116]
Lobo, R. A., Shoupe, D., Serafini, P., Brinton, D., & Horton, R. (1985). The effects of two doses of spironolactone on serum androgens and anagen hair in hirsute women. Fertility and Sterility, 43(2), 200–205. [DOI:10.1016/s0015-0282(16)48373-1]
Loriaux, D. L. (1976). Spironolactone and Endocrine Dysfunction. Annals of Internal Medicine, 85(5), 630–630. [DOI:10.7326/0003-4819-85-5-630]
McMullen, G. R., & Van Herle, A. J. (1993). Hirsutism and the effectiveness of spironolactone in its management. Journal of Endocrinological Investigation, 16(11), 925–932. [DOI:10.1007/bf03348960]
Menard, R., Guenthner, T., Kon, H., & Gillette, J. (1979). Studies on the destruction of adrenal and testicular cytochrome P-450 by spironolactone. Requirement for the 7α-thio group and evidence for the loss of the heme and apoproteins of cytochrome P-450. Journal of Biological Chemistry, 254(5), 1726–1733. [DOI:10.1016/s0021-9258(17)37833-x]
Miro, E., Rizzone, K., Ho, T., Mark, B., Sullivan, E., & Cushman, D. (2024). 2024 AMSSM Research Podium Presentations: Testosterone Levels Among Transgender Women on Gender-affirming Hormone Therapy. Clinical Journal of Sports Medicine, 34(2), 152–152. [DOI:10.1097/JSM.0000000000001212]
Miyatake, A., Noma, K., Nakao, K., Morimoto, Y., & Yamamura, Y. (1978). Increased serum oestrone and oestradiol following spironolactone administration in hypertensive men. Clinical Endocrinology, 9(6), 523–533. [DOI:10.1111/j.1365-2265.1978.tb01510.x]
Moghetti, P., Tosi, F., Tosti, A., Negri, C., Misciali, C., Perrone, F., Caputo, M., Muggeo, M., & Castello, R. (2000). Comparison of Spironolactone, Flutamide, and Finasteride Efficacy in the Treatment of Hirsutism: A Randomized, Double Blind, Placebo-Controlled Trial. The Journal of Clinical Endocrinology & Metabolism, 85(1), 89–94. [DOI:10.1210/jcem.85.1.6245]
Negri, C., Tosi, F., Dorizzi, R., Fortunato, A., Spiazzi, G. G., Muggeo, M., Castello, R., & Moghetti, P. (2000). Antiandrogen Drugs Lower Serum Prostate-Specific Antigen (PSA) Levels in Hirsute Subjects: Evidence That Serum PSA Is a Marker of Androgen Action in Women. The Journal of Clinical Endocrinology & Metabolism, 85(1), 81–84. [DOI:10.1210/jcem.85.1.6230]
Pappas, I. I., Craig, W. Y., Spratt, L. V., & Spratt, D. I. (2020). Efficacy of Sex Steroid Therapy Without Progestin or GnRH Agonist for Gonadal Suppression in Adult Transgender Patients. The Journal of Clinical Endocrinology & Metabolism, 106(3), e1290–e1300. [DOI:10.1210/clinem/dgaa884]
Pappas, I. I., Craig, W., Spratt, L. V., & Spratt, D. I. (2020). Testosterone (T) and estradiol (E2) therapy alone can suppress gonadal function in transgender patients. Costas T. Lambrew Research Retreat 2020, 47. [Google Scholar] [URL] [PDF]
Pentikäinen, P. J., Pentikäinen, L. A., Huffman, D. H., & Azarnoff, D. L. (1974). The effect of spironolactone on plasma levels and excretion of testosterone and oestrogens in the urine in males. (A preliminary report). The Journal of International Medical Research, 2(6), 439–443. [Google Scholar] [PubMed] [PDF]
Prior, J. C., Vigna, Y. M., Watson, D., Diewold, P., & Robinow, O. (1986). Spironolactone in the presurgical therapy of male to female transsexuals: Philosophy and experience of the Vancouver Gender Dysphoria Clinic. Journal of Sex Information & Education Council of Canada, 1(1), 1–7. [Google Scholar] [PDF]
Prior, J. C., Vigna, Y. M., & Watson, D. (1989). Spironolactone with physiological female steroids for presurgical therapy of male-to-female transsexualism. Archives of Sexual Behavior, 18(1), 49–57. [DOI:10.1007/bf01579291]
Reardon, E., Farnell, P., Langzettel, J., & Spratt, D. (2013). Efficacy of single agent hormonal therapy in transgender patients to suppress endogenous hypothalamic-pituitary-gonadal (HPG) activity. Fertility and Sterility, 100(3 Suppl) [Scientific Program Supplement: Oral and Poster Session Abstracts 12 October 2013 - 17 October 2013], S333–S333 (abstract no. P-640). [Google Scholar] [DOI:10.1016/j.fertnstert.2013.07.914]
Rose, L. I. (1977). Pathophysiology of Spironolactone-Induced Gynecomastia. Annals of Internal Medicine, 87(4), 398–403. [DOI:10.7326/0003-4819-87-4-398]
Rozner, R. N., Freites-Martinez, A., Shapiro, J., Geer, E. B., Goldfarb, S., & Lacouture, M. E. (2018). Safety of 5α-reductase inhibitors and spironolactone in breast cancer patients receiving endocrine therapies. Breast Cancer Research and Treatment, 174(1), 15–26. [DOI:10.1007/s10549-018-4996-3]
Santen, R. J., Kulin, H. E., Loriaux, D. L., & Friend, J. (1976). Spironolactone Stimulation of Gonadotropin Secretion in Boys with Delayed Adolescence. The Journal of Clinical Endocrinology & Metabolism, 43(6), 1386–1390. [DOI:10.1210/jcem-43-6-1386]
Santer, M., Lawrence, M., Renz, S., Eminton, Z., Stuart, B., Sach, T. H., Pyne, S., Ridd, M. J., Francis, N., Soulsby, I., Thomas, K., Permyakova, N., Little, P., Muller, I., Nuttall, J., Griffiths, G., Thomas, K. S., & Layton, A. M. (2023). Effectiveness of spironolactone for women with acne vulgaris (SAFA) in England and Wales: pragmatic, multicentre, phase 3, double blind, randomised controlled trial. BMJ, 381, e074349. [DOI:10.1136/bmj-2022-074349]
Shaw, J. C. (1996). Antiandrogen and hormonal treatment of acne. Dermatologic Clinics, 14(4), 803–811. [DOI:10.1016/s0733-8635(05)70405-8]
Sivelle, P. C., Underwood, A. H., & Jelly, J. A. (1982). The effects of histamine H2 receptor antagonists on androgen action in vivo and dihydrotestosterone binding to the rat prostate androgen receptor in vitro. Biochemical Pharmacology, 31(5), 677–684. [DOI:10.1016/0006-2952(82)90449-x]
Skorodok, L. M., Savchenko, O. N., & Liss, V. L. (1983). Hypothalamo-hypophyseal-gonadal function in boys with irregular puberty. Neuroscience and Behavioral Physiology, 13(2), 141–145. [DOI:10.1007/bf01190800]
Snyder, B. W., Winneker, R. C., & Batzold, F. H. (1989). Endocrine profile of win 49596 in the rat: A novel androgen receptor antagonist. Journal of Steroid Biochemistry, 33(6), 1127–1132. [DOI:10.1016/0022-4731(89)90419-6]
Sofer, Y., Yaish, I., Yaron, M., Bach, M. Y., Stern, N., & Greenman, Y. (2020). Differential Endocrine and Metabolic Effects of Testosterone Suppressive Agents in Transgender Women. Endocrine Practice, 26(8), 883–890. [DOI:10.4158/ep-2020-0032]
SoRelle, J. A., Jiao, R., Gao, E., Veazey, J., Frame, I., Quinn, A. M., Day, P., Pagels, P., Gimpel, N., & Patel, K. (2019). Impact of Hormone Therapy on Laboratory Values in Transgender Patients. Clinical Chemistry, 65(1), 170–179. [DOI:10.1373/clinchem.2018.292730]
Spörl, S. (1978/1979). Über den Einfluß von Spironolacton (Aldactone®) auf den Stoffwechsel von Nebennierenrindenhormonen und von Testosteron bei Gesunden mit diätinduziertem Hyperaldosterismus. [On the influence of spironolactone (Aldactone®) on the metabolism of adrenocortical hormones and testosterone in healthy individuals with diet-induced hyperaldosteronism.] (Doctoral dissertation, Freie Universität, Berlin.) [Google Scholar] [Google Books] [WorldCat] [PDF]
Spratt, L. V., Reardon, E., Olshan, J. S., & Eimicke, T. (2014). Efficacy of Testosterone (T) or Estradiol (E2) Therapy without a GnRH Agonist or Progestin to Suppress Endogenous Gonadal Activity in Transsexual Patients. Endocrine Reviews, 35(Suppl 1) [Endocrine Society’s 96th Annual Meeting and Expo, June 21–24, 2014 – Chicago], ?–? (abstract no. OR42-2). [DOI:10.1093/edrv/35.supp.1] [URL]
Stewart, I., Spratt, L., Craig, W., Olshan, J., & Spratt, D. (2018). The efficacy of testosterone or estradiol therapy without a GnRH agonist or progestin to suppress endogenous gonadal activity in transgender patients. Fertility and Sterility, 110(4 Suppl) [Scientific Congress Supplement: Oral and Poster Session Abstracts 06 October 2018 - 10 October 2018], e21–e21 (abstract no. O-44). [Google Scholar] [DOI:10.1016/j.fertnstert.2018.07.075]
Stripp, B., Taylor, A. A., Bartter, F. C., Gillette, J. R., Loriaux, D. L., Easley, R., & Menard, R. H. (1975). Effect of Spironolactone on Sex Hormones in Man. The Journal of Clinical Endocrinology & Metabolism, 41(4), 777–781. [DOI:10.1210/jcem-41-4-777]
Taylor, A. A., Rollins, D., Snodgrass, W., & Bartter, F. (1976). Effect of spironolactone (S) on adrenal and gonadal steroids in man. Clinical Research, 24(3), A279–A279. [Google Scholar] [PDF]
Unlühizarci, K., Everest, H., Bayram, F., & Keleştimur, F. (2002). Comparison of spironolactone and spironolactone plus finasteride in the treatment of hirsutism. Fertility and Sterility, 78(6), 1331–1333. [DOI:10.1016/s0015-0282(02)04294-2]
Tidd, M. J., Horth, C. E., Ramsay, L. E., Shelton, J. R., & Palmer, R. F. (1978). Endocrine effects of spironolactone in man. Clinical Endocrinology, 9(5), 389–399. [DOI:10.1111/j.1365-2265.1978.tb03578.x]
van Zuuren, E., & Fedorowicz, Z. (2016). Interventions for hirsutism excluding laser and photoepilation therapy alone: abridged Cochrane systematic review including GRADE assessments. British Journal of Dermatology, 175(1), 45–61. [DOI:10.1111/bjd.14486]
Walsh, P. C., & Siiteri, P. K. (1975). Suppression of Plasma Androgens by Spironolactone in Castrated Men with Carcinoma of the Prostate. Journal of Urology, 114(2), 254–256. [DOI:10.1016/s0022-5347(17)67001-0]
Wang, C., Du, Y., Bi, L., Lin, X., Zhao, M., & Fan, W. (2023). The Efficacy and Safety of Oral and Topical Spironolactone in Androgenetic Alopecia Treatment: A Systematic Review. Clinical, Cosmetic and Investigational Dermatology, 16, 603–612. [DOI:10.2147/ccid.s398950]
Weissmann, A. (1985). Antiandrogenic Effects of Topically Applied Spironolactone on the Hamster Flank Organ. Archives of Dermatology, 121(1), 57–62. [DOI:10.1001/archderm.1985.01660010061019]
Yamasaki, K., Sawaki, M., Noda, S., Muroi, T., Takakura, S., Mitoma, H., Sakamoto, S., Nakai, M., & Yakabe, Y. (2004). Comparison of the Hershberger assay and androgen receptor binding assay of twelve chemicals. Toxicology, 195(2–3), 177–186. [DOI:10.1016/j.tox.2003.09.012]
Yang, W., Hong, T., Chang, X., Han, M., Gao, H., Pan, B., Zhao, Z., & Liu, Y. (2024). The efficacy of and user satisfaction with different antiandrogens in Chinese transgender women. International Journal of Transgender Health, advance online publication. [DOI:10.1080/26895269.2024.2323514]
Yazdabadi, A., & Sinclair, R. (2011). Treatment of female pattern hair loss with the androgen receptor antagonist flutamide. The Australasian Journal of Dermatology, 52(2), 132–134. [DOI:10.1111/j.1440-0960.2010.00735.x]
Zgliczynski, S., Baranowska, B., & Szymanowski, J. (1981). L’influence du spironolactone sur la concentration des gonatrophines et des hormones gonadiques dans l’hypertrophie prostatique. [The influence of spironolactone on the concentration of gonadotrophins and gonadal hormones in prostatic hypertrophy]. Journal d’Urologie, 87(9), 635–638. [Google Scholar 1] [Google Scholar 2] [PubMed] [PDF] [Translation]
Zimmerman, Y., Eijkemans, M. J., Coelingh Bennink, H. J., Blankenstein, M. A., & Fauser, B. C. (2013). The effect of combined oral contraception on testosterone levels in healthy women: a systematic review and meta-analysis. Human Reproduction Update, 20(1), 76–105. [DOI:10.1093/humupd/dmt038]
\ No newline at end of file
+A Review of Studies on Spironolactone and Testosterone Suppression in Cisgender Men, Cisgender Women, and Transfeminine People - Transfeminine Science
A Review of Studies on Spironolactone and Testosterone Suppression in Cisgender Men, Cisgender Women, and Transfeminine People
By Aly | First published December 19, 2018 | Last modified April 5, 2024
Abstract / TL;DR
Spironolactone is an antiandrogen used in transfeminine hormone therapy which is especially employed in the United States. It is widely considered to act as an androgen receptor antagonist and as an androgen synthesis inhibitor, both blocking the actions of testosterone and lowering testosterone levels in transfeminine people. A literature search was conducted to review studies assessing the influence of spironolactone on testosterone levels in cisgender men, cisgender women, and transfeminine people. The results of these studies were mixed, but in most studies spironolactone showed no apparent influence on testosterone levels. These findings suggest that spironolactone has inconsistent and limited effects on testosterone levels. Moreover, these data, as well as studies of estradiol alone, indicate that estradiol is mainly responsible for lowered testosterone levels when the combination of estradiol and spironolactone is used for hormone therapy in transfeminine people. Besides testosterone suppression, spironolactone also acts as a direct antagonist of the androgen receptor, and this importantly contributes to its antiandrogenic efficacy as well. However, studies in cisgender women suggest that spironolactone is a relatively weak androgen receptor antagonist, and is likely best-suited for blocking relatively low testosterone levels. Taken together, the antiandrogenic effectiveness of spironolactone in transfeminine people appears to be limited. Other antiandrogenic approaches may be more effective in transfeminine people, and may be considered instead or as alternatives to spironolactone in those in whom testosterone levels with estradiol plus spironolactone remain inadequately suppressed.
Introduction
Spironolactone, also known by its major brand name Aldactone, is an antiandrogen which is commonly used in transfeminine hormone therapy. It is used in combination with estrogen in transfeminine people to help reduce the effects of testosterone. Spironolactone is used in transfeminine hormone therapy particularly in the United States, where another antiandrogen, cyproterone acetate (CPA; brand name Androcur), is unavailable. Conversely, CPA is the main antiandrogen used in transfeminine people in Europe and most of the rest of the world. Another type of medication, gonadotropin-releasing hormone (GnRH) agonists, are the major antiandrogens used in certain places like the United Kingdom. The combination of estradiol with CPA or a GnRH agonist in transfeminine people consistently suppresses testosterone levels into the normal female range (<50 ng/dL or <1.8 nmol/L) (Aly, 2018; Aly, 2019). Hence, both CPA and GnRH agonists are very effective antiandrogens in transfeminine people.
Spironolactone acts as an androgen receptor antagonist, but is also known to function as an androgen synthesis inhibitor. As an example, spironolactone has been shown in preclinical research to inhibit several enzymes involved in gonadal and adrenal androgen production, including CYP17A1 (17α-hydroxylase/17,20-lyase) among others, and to substantially decrease concentrations of androgens in these studies (Loriaux et al., 1976; Callan, 1988; McMullen & Van Herle, 1993). However, the steroid synthesis inhibition of spironolactone appears to only occur at very high doses and concentrations of spironolactone (Loriaux et al., 1976; McMullen & Van Herle, 1993). For example, spironolactone is used at 10- to 20-fold smaller doses by body weight in humans than in animal studies that have demonstrated substantial steroid synthesis inhibition with the agent (McMullen & Van Herle, 1993).
A widespread notion in the transgender community, as well as in the transgender health community and in the medical literature, is that spironolactone decreases testosterone levels and that this is a major part of how it works as an antiandrogen in transfeminine people. In actuality however, the clinical evidence to support this notion appears to be limited, and available data from studies appear to be highly conflicting. The purpose of this article is to review the available clinical studies on spironolactone and testosterone levels in cisgender men, cisgender women, and transfeminine people in order to help elucidate whether and to what extent spironolactone lowers testosterone levels in humans. In addition, the role of androgen receptor blockade in the antiandrogenic effects of spironolactone is briefly reviewed.
A total of 22 studies of spironolactone and sex hormone levels in cisgender males were identified (Table 1). These studies assessed pre-treatment versus post-treatment hormone levels with spironolactone, hormone levels with spironolactone versus a comparator group, or both. Within the identified studies, testosterone levels were not significantly changed in 12 of 22 studies (55%), decreased in 4 of 22 (18%) studies, increased in 1 of 22 (4.5%) studies, and mixed or unknown (e.g. divergences in changes of total versus free testosterone levels or didn’t actually report testosterone levels) in 4 of 22 (18%) studies. Most of the studies were very small (fewer than 10 people), with several exceptions. The studies were of highly variable lengths, with some being several days and others lasting for weeks or months. Few of the studies were RCTs. Most of the studies were very old, with a majority published in the 1970s and the rest published in the 1980s and 1990s. In relation to the preceding, the quality of data was limited.
Table 1: Studies of sex hormone levels with spironolactone alone in cisgender males:
Treatment and subjects
Findings
Source(s)
100 mg/day for 2 weeks in 7 healthy men (23–34 years)
T significantly decreased and LH significantly increased. No significant change in E1, E2, or E3. No change urinary total T excretion but significantly increased urinary total E excretion (including of E1 (7.72 to 10.54 µg/24 hrs), E2 (2.60 to 3.34 ug/24 hours), E3 (7.69 to 11.75 µg/24 hrs)). Slightly but significantly decreased excretion of 17-KS in urine.
400 mg/day for 5 days in 6 healthy men (21–33 years)
Significant increase in P4 and 17α-OHP (approximately doubled) for whole duration. Small and transient increases in LH (+20%) and FSH on the 2nd but not on the 3rd or 5th days (only other days measured). No significant changes in T, E2, or PRL. E2 and PRL non-significantly increased (+56% and +34% on the 5th day, respectively).
100 or 400 mg/day spironolactone for 8 weeks in 7 orchiectomized men (46–78 years) with metastatic prostate cancer
T, A4, and DHEA significantly decreased with both doses of spironolactone and of similar magnitude between doses. Influence more apparent after 2–3 weeks of treatment.
5 mg/kg/day for 1 week (275 mg/day for a 55 kg person) in 7 boys with delayed puberty (14–16 years)
Significant increase in LH (+60%) and non-significant increase in FSH (+60%); individual responses for FSH variable. Increased P4 and 17α-OHP. T and E2 not actually reported.
Initially 400 mg/day for 12 weeks; dosage later decreased in some due to hypotension (range 150–400 mg/day) in 5 men and 5 women (3 premenopausal, 2 postmenopausal) with normal or low renin hypertension
P4 and 17α-OHP increased by 2 to 4 times compared to pre-treatment and post-treatment. T, E2, LH, FSH, PRL, and 17-KS all unchanged.
200–400 mg/day for 4–13 months (mean 7 months) in 6 men with hypertension (35–61 years; mean 47 years) vs. 10 untreated male controls with hypertension (mean age 45 years)
Significantly greater LH and E2 (30 pg/mL vs. 13 pg/mL; +130%), significantly lower T (440 ng/dL vs. 270 ng/dL; –38%), no difference in FSH. Also, significantly greater metabolic clearance rate of T, significantly greater rate of peripheral conversion (conversion ratio and transfer constant) of T into E2, non-significantly greater metabolic clearance rate of E2, no difference in blood production rate of T, and significantly greater blood production rate of E2.
200–400 mg/day (mean 330 mg/day) for 20–27 days in 5 gonadally intact men (50–76 years) with prostate cancer
P4 increased significantly from 0.25 ± 0.10 ng/mL (mean ± SD) to maximum of 1.3 ± 0.31 ng/mL by 20 days (increase of 5.2-fold or 420%). T decreased significantly from 427 ± 74.3 ng/dL to 200 ± 80.3 ng/dL (–53.2%). No significant change in E2, LH, or FSH.
200 mg/day for 21 days in 4 healthy men (26–35 years)
No change in total T or E2. Unbound T and E2 slightly but significantly increased. Thought to be due to a direct interaction of spironolactone metabolites with the plasma protein binding of T and E2. But not due to binding to SHBG as T binding to SHBG was not significantly altered.
75–150 mg/day for 12 weeks in 6 men with essential hypertension (28–64 years; mean 48 years)
E1 significantly increased. E2 small, gradual, non-significant increase. T, LH, and PRL not significantly changed. PRL responses to TRH normal/not significantly changed.
150–300 mg/day for 40 weeks in 2 men with idiopathic hyperaldosteronism (23 and 44 years)
E1 increased. E2 fluctuated. E2 increased by 10-fold in one person by 16 weeks and this was associated with gynecomastia. T, LH, and PRL not altered significantly.
200 mg/day for 10 days (n=5) vs. placebo (n=5) in 10 healthy men (18–31 years) (RCT)
Significantly greater urinary A4, urinary EC, and urinary total E excretion. Differences in T, E2, LH, and FSH as well as urinary DHEA, LH, and FSH not significant. Examination of interaction between treatment and time showed significant changes in T, LH, and urinary DHEA. Concluded that there was a transient rise in T and urine DHEA for 2–4 days followed by increase in LH and normalization of T and DHEA excretion after 4–10 days.
300 mg/day for 7 days (n=5) vs. 200 mg/day triamterene (n=5) in 10 normal young men with diet-induced hyperaldosteronism (14 days of a diet modifying electrolyte intake)
P4, 17α-OHP, unchanged. T near-but-non-significantly decreased (704.6 ± 55.5 ng/dL (mean ± SEM) to 508.4 ± 45.9 ng/dL on day 6; p < 0.10). Also assessed endogenous corticosteroids.
100 mg/day for 3 months in treatment group of 47 men (age 60–80 years) with BPH; control group of 58 healthy men without BPH (also age 60–80 years)
In spiro/BPH group, T decreased from 650 ng/dL to 290 ng/dL and DHT decreased from 450 ng/dL to 150 ng/dL. In control/non-BPH group, T was 280 ng/dL and DHT was 90 ng/dL. P4, E2, and LH increased in spiro/BPH group. FSH also assessed. The authors stated that prostate gland can be a source of androgen production, implying that BPH can produce elevated androgen levels and that spironolactone can normalize elevated androgen levels in the condition.
150 mg/m2/day for 5 days in 6 boys with irregular puberty (11–13 years)
No significant changes in T or urinary 17-KS excretion, elevated LH (by 600%—likely typo of “60%” (?)), and slightly increased FSH (from 0.75 ng/mL to 0.86 ng/mL).
25–400 mg/day (median 100 mg/day) for 12 months in 32 males (59%) of a group of 54 males (17–64 years; mean 44 years) with non-alcoholic liver disease requiring liver transplantation vs. 469 healthy male controls (mean 31 years) with normal liver function
Significantly decreased T with spironolactone in men with moderate-severity liver disease but not with low- or high-severity liver disease. SHBG not influenced by spironolactone dosage. No influence on gonadotropin responses to GnRH stimulation.
Although the quality of these studies is limited, the findings of the studies, which are mixed but are overall more suggestive against spironolactone reducing testosterone levels than it doing so, are in notable contrast to similar studies of CPA and testosterone suppression in cisgender men that were published in the 1970s and 1980s. These studies consistently found that CPA suppressed testosterone levels by 40 to 70% on average (Aly, 2019). Subsequently, the findings were replicated in several more modern studies of CPA in cisgender men and transfeminine people, which likewise found that the drug given alone consistently suppressed testosterone levels by about 45 to 65% on average (Aly, 2019).
Spironolactone in Cisgender Women
Spironolactone has a long history of use in cisgender women in the treatment of androgen-dependent skin and hair conditions like acne, hirsutism, scalp hair loss, and hyperandrogenism (due to e.g. polycystic ovary syndrome (PCOS)). It has been used at similar doses for androgen-dependent conditions in cisgender women as it has in transfeminine people (e.g., 50–200 mg/day most typically). There are many dozens of studies of spironolactone as an antiandrogen in cisgender women (e.g., PubMed). Instead of attempting to individually review all of these studies, the present article will discuss the findings of several papers that have themselves reviewed substantial numbers of these studies and have summarized available findings on testosterone levels with spironolactone.
Callan (1988) reviewed the literature on spironolactone for treatment of acne and hirsutism in cisgender women and found that some clinical studies reported decreased levels of testosterone and/or other androgens with spironolactone (4 studies cited) whereas other studies reported no change in androgen levels (4 studies cited). The author cited several studies to support the claim that androgen receptor antagonism with spironolactone is more clinically important than any influence it has on androgen production (5 studies cited). For instance, clinical benefits against acne and hirsutism occurred with spironolactone both before androgen levels decrease as well as when androgen levels do not decrease.
McMullen & Van Herle (1993) reviewed 19 studies of spironolactone for treatment of androgen-dependent conditions in cisgender women, with a majority of these studies reporting long-term hormone levels. Most of the studies were open-label and uncontrolled, with only five studies having a control group and only two studies being double-blind placebo-controlled trials. Changes in hormone levels across studies were very heterogenous, with the majority of changes not reaching statistical significance. Only 1 of 7 (14%) studies found a decrease in DHEA-S levels. The review concluded that a clinically significant change in adrenal androgen levels with spironolactone in cisgender women was not supported. Conversely, testosterone levels were decreased with spironolactone in 13 of 16 (81%) of studies. However, in the only two RCTs, there were no differences in testosterone levels with spironolactone versus in the placebo control groups. As such, the review concluded that the decreased testosterone levels with spironolactone in cisgender women reported in many of the non-RCT studies may not actually be a real phenomenon. As with Callan (1988), the review noted that the major mechanism of action of spironolactone as an antiandrogen is likely to be androgen receptor blockade.
Bradstreet et al. (2007) cited and discussed a Cochrane review of spironolactone for treatment of acne and/or hirsutism in cisgender women (Farquhar et al., 2003). Cochrane reviews are rigorous high-quality systematic reviews of all of the available RCTs for a given medical intervention. The Cochrane review identified 19 RCTs, with 9 included in the review, 8 excluded due to methodological issues (e.g., with randomization), and two others which were described as “awaiting assessment” (Farquhar et al., 2003). Bradstreet and colleagues noted per the Cochrane review that spironolactone at a dosage of 100 mg/day had little influence on levels of DHEA, DHEA-S, or testosterone in the trials evaluated and said that this is because its mechanism of action as an antiandrogen is androgen receptor antagonism (Bradstreet et al., 2007). The Cochrane review itself did not discuss changes in androgen or testosterone levels with spironolactone in aggregate. An update of the Cochrane review was published in 2009, but with no new studies found and with the findings unchanged (Brown et al., 2009).
Layton et al. (2017) was a hybrid systematic review of spironolactone for acne in cisgender women. In a table discussing the mechanism of action of spironolactone and other antiandrogens for acne, the authors stated that “Data from over 50 articles reporting effects [of spironolactone] on serum androgens are equivocal” (i.e., ambiguous, uncertain, questionable) (Layton et al., 2017). The review further noted that inhibition of androgen synthesis by spironolactone in humans may be unlikely at therapeutic doses and may occur instead only at supraphysiological doses (with Menard et al. (1979) cited in support of these claims, presumably related to the very high doses required) (Layton et al., 2017).
Rozner et al. (2019) reviewed clinical studies of the endocrine effects of spironolactone in cisgender women to assess whether it is safe to use in women with past or present breast cancer receiving endocrine therapy. The review included 18 studies with 465 women (mostly having androgen-dependent conditions) assessing the influence of spironolactone on sex hormone levels. The assessed studies included retrospective cohort studies, case–control studies, and RCTs. Of the included studies, 10 (56%) studies (with 179 women) found no change in testosterone levels with spironolactone, 8 (44%) studies (with 253 women) found a decrease, and 1 (6%) study (with 33 women) found an increase in free but not total testosterone levels. Changes in levels of DHEA-S, androstenedione, and estrogen were also assessed and findings were similar, with no changes observed in majorities of studies for these hormones. The review concluded that there is no significant change in levels of androgens, estrogen, or gonadotropins with spironolactone in cisgender women.
Almalki et al. (2020) conducted a systematic review and network meta-analysis of RCTs on the comparative efficacy of several types of medications (statins, metformin, spironolactone, and combined birth control pills) on reducing testosterone levels in cisgender women specifically with PCOS. Nine RCTs including 613 women were included for all of the medications. The meta-analysis concluded that the statin atorvastatin was more effective than the other included medications in reducing testosterone levels. Only two of the included RCTs employed spironolactone, one of which was with spironolactone alone (n=34) versus metformin (n=35) (Ganie et al., 2004) and the other of which was with spironolactone plus metformin (n=62) versus spironolactone alone (n=51) versus metformin alone (n=56) (Ganie et al., 2013). Both of the included trials found that spironolactone alone significantly decreased testosterone levels in pre-treatment versus post-treatment comparisons (Ganie et al., 2004; Ganie et al., 2013). No trials of spironolactone versus placebo controls were included.
Taken together, the available studies of spironolactone and testosterone levels in cisgender women with androgen-dependent conditions are highly inconsistent and mixed, but with numerous studies finding no significant changes in testosterone levels. The reasons for the findings being so mixed are unclear, but may relate to study methodology and quality. Findings in this population seem particularly notable as regulation of the hypothalamic–pituitary–gonadal (HPG) axis by androgens in women is minimal to negligible, in turn making it such that androgen receptor antagonists will have little effect of upregulating gonadal sex hormone production as they can in cisgender men and transfeminine people. As a result, there is less homeostatic interference that could influence findings in evaluating the steroid synthesis inhibition of spironolactone in this sex, and hence these studies may provide a clearer picture of steroid synthesis inhibition as a possible clinical effect of spironolactone. However, as the findings are still so mixed, the results seem inconclusive. In any case, only a limited effect at best seems clear.
Spironolactone Alone in Transfeminine People
Only one study of spironolactone alone (without estrogen) and sex hormone levels in transfeminine people was identified (Table 2). It was conducted by Louis Gooren and colleagues of the Dutch Center of Expertise on Gender Dysphoria (CEGD) at the Vrije Universiteit Medical Center (VUMC) in Amsterdam, Netherlands in the 1980s. The study compared levels of testosterone, DHT, estradiol, LH, FSH, and prolactin before and after treatment with 200 mg/day spironolactone for 6 weeks in 6 young pre-hormone-therapy transfeminine people. It found slightly but significantly increased testosterone levels, increased prolactin levels, and no change in levels of estradiol, DHT, LH, or FSH.
Table 2: Studies of sex hormone levels with spironolactone alone in transfeminine people:
Treatment and subjects
Findings
Source(s)
200 mg/day for 6 weeks in 6 pre-hormone therapy transfeminine people (21–39 years)
T (mean ± SEM) increased significantly from 17.2 ± 0.8 nmol/L (496 ± 20 ng/dL) to 20.6 ± 1.7 nmol/L (594 ± 50 ng/dL) (+19.8%). No change in E2 (90 ± 20 pmol/L [25 ± 5.0 pg/mL] vs. 100 ± 30 pmol/L [27 ± 8.2 pg/mL] or 80 ± 20 pmol/L [22 ± 5.4 pg/mL]) or DHT (1.7 ± 0.8 nmol/L [49 ± 20 ng/dL] vs. 1.8 ± 0.9 nmol/L [52 ± 30 ng/dL]). LH, FSH, and GnRH-stimulated LH and FSH unchanged. PRL and TRH-stimulated PRL increased.
Abbreviations: T = testosterone; E2 = estradiol; DHT = dihydrotestosterone; LH = luteinizing hormone; FSH = follicle-stimulating hormone; GnRH = gonadotropin-releasing hormone; PRL = prolactin; TRH = thyrotropin-releasing hormone.
The fact that this study was done by the CEGD is notable as this institute is among the most prolific research centers on transgender hormone therapy in the world (Bakker, 2021), and, while they evaluated spironolactone as well as nilutamide as antiandrogens in studies in transfeminine people in the 1980s and 1990s (Wiki), the group ultimately settled on using only CPA instead. This was probably related to the lack of testosterone suppression with spironolactone and pure androgen receptor antagonists like nilutamide, as the researchers have touched on in other publications (e.g., Gooren, 1999).
Estrogen Plus Spironolactone in Transfeminine People
Eleven studies of the combination of estrogen and spironolactone and sex hormone levels in transfeminine people were identified (Table 3). The first study was conducted by Jerilynn Prior and colleagues in Canada in the 1980s. Subsequent studies were conducted over 25 years later by groups in the United States, Australia, Israel, and Thailand. All of the studies were retrospective chart reviews or prospective non-randomized studies, with the exception of a single RCT.
Table 3: Studies of testosterone levels with estrogen plus spironolactone in transfeminine people:
Treatment and subjects
Findings
Source(s)
Oral CEEs (0.625–5 mg/day cyclically—3 of 4 weeks per month), oral MPA (10–20 mg/day cyclically—3 of 4 weeks per month—or continuously—”if gonadotrophins increased or to aid in T reduction or breast development”), and spironolactone (100–600 mg/day continuously) for 12 months in 27 transfeminine people who had been on “high-dose” E alone for an extended duration (Group 1) and 23 transfeminine people who were pre-hormone-therapy (Group 2), or 50 transfeminine people total, at Vancouver General Hospital.
T decreased in Group 1 from mean 169 ng/dL to 87.4 ng/dL (–48.2%) and in Group 2 from mean 642 ng/dL to 49.2 ng/dL (–92.3%). In the groups combined, T following treatment would be mean 69.8 ng/dL. Per authors, spironolactone was intended to help reduce T and facilitate feminization while MPA was intended to help suppress gonadotropins and T and improve breast development. However, authors emphasized the decrease in T as being due to spironolactone despite inclusion of MPA, without data provided to substantiate this.
Sublingual estradiol (4 mg/day—2 mg b.i.d.) (n=14), transdermal estradiol patch (100 μg/day) (n=1), or injectable estradiol valerate (20 mg/2 weeks) (n=1) with spironolactone (100–200 mg/day) for 6 months in 16 transfeminine people at an LGBT community health center in Los Angeles, California.
T was median 405 ng/dL at baseline and 42 ng/dL after 6 months (–89.6%). Free T was median 11.4 ng/dL at baseline and 0.8 ng/dL at 6 months (–93.0%). 10 of 15 (66.7%) had total T in female range and 14 of 15 (93.3%) had free T in female range.
Oral E2 (1–8 mg/day) with or without spironolactone (200 mg/day) (n=61), finasteride (5 mg/day) (n=49), and/or MPA (2.5–10 mg/day) (n=38) for 0.3 to 10.5 years (mean 4.3 ± 3.1 years) in 156 transfeminine people at Albany Medical Center.
Oral E2 dose-dependently and substantially but incompletely suppressed T. Relative to E2 alone (at equivalent E2 levels), E2 plus spironolactone had no significant influence on T (+10.6 ± 16 ng/dL (mean ± SE); p = 0.5) and no greater likelihood of achieving better T suppression (<100 ng/dL) (OR = 0.75; 95% CI = 0.44–1.29). T levels with E2 alone were mean ~80 ng/dL and with E2 plus spironolactone were mean ~95 ng/dL per own re-analysis. Finasteride was also associated with greater T levels. MPA helped with T suppression in some (71% of subjects). More discussion and re-analysis including graphs (Aly, 2019).
Oral E2 (0.5–10 mg/day) (n=67) or oral CEEs (0.625–5 mg/day) (n=12) and spironolactone (25–400 mg/day; mean/median 145 mg/day) for 12 months in 98 transfeminine people at Boston Medical Center.
Combined E and spironolactone decreased T from median 385 ng/dL to 130 ng/dL (–66.2%). E alone vs. E and spironolactone not reported. No significant influence of spironolactone dosage on T. Incomplete suppression of T (>50 ng/dL) in all but the lowest quartile (25%) of individuals.
Oral EV (4–6 mg/day; median 5–6 mg/day) (88.3%) or transdermal E2 (11.7%) alone or in combination with CPA (25–50 mg/day; median 50 mg/day) or spironolactone (87.5–200 mg/day; median 100 mg/day) for 0.9 to 2.6 years (median 1.5 years) in 80 transfeminine people at two gender clinics in Melbourne, Australia.
T was median 10.5 nmol/L (303 ng/dL) with E2 only, 2.0 nmol/L (58 ng/dL) with E2 plus spironolactone, and 0.8 nmol/L (23 ng/dL) with E2 plus CPA. 90% of those on E2 plus CPA and 40% of those on E2 plus spironolactone had T of <2 nmol/L (<58 ng/dL). T significantly lower with E2 plus CPA compared to E2 plus spironolactone and E2 alone. T with E2 plus spironolactone lower than with E2 alone but non-significantly. No significant differences between groups in age, hormone therapy duration, or E2 dosage or levels. Graph that visually summarizes the results.
Sublingual estradiol (2–12 mg/day) and spironolactone (100–200 mg/day) with or without sublingual MPA (5–10 mg/day) or injectable MPA (150 mg/3 months) for 3.4 ± 1.7 years in 92 transfeminine people at Rhode Island Hospital.
T (mean ± SD) was 215 ± 29 ng/dL with E2 plus spironolactone and 79 ± 18 ng/dL with E2 plus spironolactone and MPA.
Oral E2 (2–8 mg/day) (84.2%) or other E forms (15.8%) with spironolactone (80.4%; n=107) or without spironolactone (19.6%) for more than 6 months in 133 transfeminine people at three clinics in Dallas, Texas.
T decreased from median 367 ng/dL (95% range 175–731 ng/dL) (n=70) at baseline to median 55 ng/dL (95% range 3–709 ng/dL) (n=131) in whole group (80.4% taking spironolactone). 65 of 133 (49%) had adequate T suppression (presumably <50 or <60 ng/dL) in whole group. T with E2 plus spironolactone at 25–75 mg/day (n=15) was mean 129.4 ng/dL (range <3—611 ng/dL), at 100–175 mg/day (n=61) was mean 180.4 ng/dL (range <3–1137 ng/dL), and at 200–300 mg/day (n=31) was mean 170.1 ng/dL (range <3–798 ng/dL). In the whole E2 plus spironolactone group (n=107), T would be mean 170.3 ng/dL.
Oral E2 (2–8 mg/day), transdermal E2 gel (2.5–5 mg/day), or transdermal E2 patches (50–200 μg/day) plus spironolactone (50–200 mg/day) (n=16), CPA (10–100 mg/day) (n=41), or a GnRH agonist (n=10) for 12 months in 67 transfeminine people at Tel Aviv-Sourasky Medical Center in Israel.
With spironolactone, T (mean ± SD) decreased from 15.2 ± 8.1 nmol/L (438 ± 230 ng/dL) at baseline to 10.2 ± 5.7 nmol/L (294 ± 164 ng/dL) at 3 months (–32.9%), 3.5 ± 1.2 nmol/L (100 ± 35 ng/dL) at 6 months (–77.0%), and 4 ± 7.1 nmol/L (120 ± 200 ng/dL) at 12 months (–73.7%). T was in the female range (<1.8 nmol/L [52 ng/dL]) at all follow-ups after baseline for both CPA and GnRH agonist (–92.0% to –96.4%).
Oral EV 4 mg/day plus spironolactone (100 mg/day) (n=26) or CPA (25 mg/day) (n=26) for 12 weeks in 52 transfeminine people at two clinics in Bangkok, Thailand (RCT).
With intention-to-treat analysis, T decreased with E2 plus spironolactone from median 645.0 ng/dL (IQR 466.7−1027.7 ng/dL) to 468.3 ng/dL (IQR 287.0−765.4 ng/dL) (–27.4%) and with E2 plus CPA from 655.5 ng/dL (402.6−872.7 ng/dL) to 9.3 ng/dL (IQR 5.5−310.4 ng/dL) (–98.6%). Adequate suppression of testosterone (<50 ng/dL) was achieved by 4 of 26 (15%) in the E2 plus spironolactone group and by 18 of 26 (69%) in the E2 plus CPA group. Study also assessed and reported E2, SHBG, and PRL levels.
E2 (sublingual, transdermal, or injectable) with spironolactone (n=39) or without spironolactone (n=37) for 12 months in 93 transfeminine people at two LGBTQ-oriented clinics in Seattle, Washington and Iowa City, Iowa.
T was median 11 to 18 ng/dL in different estradiol groups without spironolactone and median 10 to 12 ng/dL in different estradiol groups with spironolactone. T was significantly lower with spironolactone only for sublingual E2 group (median 11 ng/dL (IQR 6–35 ng/dL) [n=27] vs. median 18 ng/dL (IQR 13–205 ng/dL) [n=16]) and not for transdermal or injectable E2 groups.
Oral E2 (4–12 mg/day, median 6 mg/day) (n=27) or injectable EV (2–5 mg/week, median 4 mg/week) (n=6) with spironolactone (n=31) or without spironolactone (n=2) for median 6.2 months (range 0.6–28.2 months) (time on optimized E2 dose specifically) in 33 transfeminine people at Maine Medical Center.
T was median 13.0 ng/dL (range 2.7–559 ng/dL) for whole group (93.9% taking spironolactone). 28 of 33 (84.8%) of whole group had female-range T (<50 ng/dL). However, in earlier studies by the same group, similar T suppression with E2 alone was reported (Reardon et al., 2013; Spratt et al., 2014).
The data on the testosterone levels with estrogen plus spironolactone in transfeminine people from the 11 studies in the table can be roughly summarized. Some studies reported mean testosterone levels and some reported median testosterone levels, so these cases must be considered separately. In terms of reported mean testosterone levels across studies (4 studies), the median value of these study averages would be about 171 ng/dL and the range of study averages would be about 95 to 215 ng/dL. In terms of reported median testosterone levels across studies (7 studies), the median value of these study medians would be about 55 ng/dL and the range of study medians would be about 11 to 468 ng/dL. One study had to be excluded due to concomitant use of the progestogen medroxyprogesterone acetate (MPA) in all individuals (Prior, Vigna, & Watson, 1989; Prior et al., 1986). Insights from the preceding results include large variability in testosterone levels across studies and mean testosterone levels being much higher than median testosterone levels. Limitations of the preceding values include lack of equivalent estrogen and spironolactone dosages and levels across studies, lack of equivalent durations of hormone therapy across studies, lack of equivalent testosterone blood-testing methodologies across studies, lack of equivalent transfeminine patient samples, and, in the case of the study median testosterone values, two of the studies notably having almost all but not all individuals on spironolactone (80 and 94% rather than 100%). These limitations likely underlie the large variability in reported values across studies. In any case, these results suggest that estrogen plus spironolactone results in variably inadequate testosterone suppression in most transfeminine people, which is in notable major contrast to testosterone suppression with estrogen plus CPA or a GnRH agonist in transfeminine people.
Individual findings of the studies include inadequate testosterone suppression with estradiol plus spironolactone in most transfeminine people (Leinung et al., 2018; Liang et al., 2018; Jain, Kwan, & Forcier, 2019; Sofer et al., 2020; Burinkul et al., 2021), no difference in testosterone suppression with spironolactone versus without spironolactone (Leinung et al., 2018), lack of notable influence of spironolactone dosage on testosterone suppression (Liang et al., 2018; SoRelle et al., 2019), and inferior testosterone suppression with estradiol plus spironolactone compared to estradiol plus CPA or a GnRH agonist in transfeminine people (Angus et al., 2019; Sofer et al., 2020; Burinkul et al., 2021). Conversely, some studies have found adequate or near-adequate testosterone suppression with estradiol plus spironolactone in most or almost all transfeminine people (Deutsch, Bhakri, & Kubicek, 2015; Angus et al., 2019; SoRelle et al., 2019; Cirrincione et al., 2021; Pappas et al., 2021), and some studies have found indications of greater testosterone suppression with spironolactone versus without spironolactone (Angus et al., 2019; Cirrincione et al., 2021). On the other hand, some studies using estradiol alone without any antiandrogen at physiological estradiol levels (<200 pg/mL) have reported adequate testosterone suppression similarly to the preceding estradiol plus spironolactone studies (Reardon et al., 2013; Spratt et al., 2014; Cirrincione et al., 2021). One study was confounded by the concomitant use of MPA, which is known to suppress testosterone levels on its own, and hence reliable conclusions cannot not be drawn from this study (Prior, Vigna, & Watson, 1989; Prior et al., 1986). Indeed, it is notable that this study found lower mean testosterone levels with estrogen and spironolactone than any other study did. A couple of studies found that testosterone levels progressively decline with time (particularly over the first 12 months) with estradiol plus spironolactone in most transfeminine people (Liang et al., 2018; Sofer et al., 2020). Whether the decreases in testosterone levels with time were more related to estradiol or to spironolactone is unclear, though estradiol seems more likely (e.g., Wiki).
Taken together, the findings of available studies on estradiol plus spironolactone and testosterone suppression in transfeminine people are highly variable and mixed, although overall more studies support spironolactone having poor or no testosterone-suppressing effectiveness. The reasons underlying the differences in findings on testosterone suppression between studies are unclear, but contributing factors may include varying estradiol doses, routes, and levels, durations of hormone therapy, differing laboratory assays of testosterone levels, and other differences in study methodologies, as well as limitations in study and evidence quality. In any case, the conflicting nature of the findings is in major contrast to the almost invariably strong to maximal testosterone suppression in studies of estradiol plus CPA and estradiol plus GnRH agonists in transfeminine people.
Spironolactone, Androgen Receptor Antagonism, and Clinical Antiandrogenic Effectiveness
The clinical antiandrogenic effectiveness of spironolactone in cisgender women with androgen-dependent skin and hair conditions, like acne, hirsutism, and scalp hair loss, is well-established (Brown et al., 2009; van Zuuren & Fedorowicz, 2016; Layton et al., 2017; Barrionuevo et al., 2018; James, Jamerson, & Aguh, 2022; Wang et al., 2023). Conversely, the clinical antiandrogenic efficacy of spironolactone in transfeminine people has been very limitedly assessed to date and is largely unknown (Angus et al., 2021). Spironolactone does not appear to be very effective for decreasing testosterone levels in either cisgender women or transfeminine people based on the findings of the present review. However, spironolactone is a competitive antagonist of the androgen receptor in addition to its actions a weak androgen synthesis inhibitor, and hence it also directly blocks androgens from mediating their effects in the body (Loriaux et al., 1976; McMullen & Van Herle, 1993). Based on studies in populations besides transfeminine people, for instance cisgender women (discussed above) and cisgender boys with gonadotropin-independent precocious puberty (e.g., Holland, 1991), in which spironolactone has not decreased testosterone levels but has nonetheless been effective as an antiandrogen, the androgen receptor blockade of spironolactone is likely to be its main mechanism of action as an antiandrogen and may account for most or all of its therapeutic antiandrogenic effectiveness.
However, while spironolactone is clearly effective as an androgen receptor antagonist, it appears to be a relatively weak androgen receptor blocker at typical doses used in cisgender women and transfeminine people. Numerous publications in the literature describe spironolactone as being only a weak androgen receptor antagonist (Wiki; Wiki). In relation to this, animal studies have found that spironolactone is a far less potent androgen receptor antagonist than other antiandrogens like CPA, flutamide, and bicalutamide (Bonne & Raynaud, 1974; Hecker, Hasan, & Neumann, 1980; Sivelle, Underwood, & Jelly, 1982; Weissmann et al., 1985; Labrie et al., 1987; Snyder, Winneker, & Batzold, 1989 [Table]; Yamasaki et al., 2004 [Graph]). Moreover, in cisgender women, the population in which spironolactone is most widely used as an antiandrogen, testosterone levels are relatively low, on average about 20-fold lower than in cisgender men (around 30 ng/dL on average compared to about 600 ng/dL on average, respectively) (Aly, 2018). However, many cisgender women with androgen-dependent conditions have PCOS, which is associated with limitedly elevated testosterone levels (e.g., perhaps around 60 ng/dL on average) (Aly, 2018). The typical therapeutic dose range of spironolactone in cisgender women with androgen-dependent conditions is 50 to 200 mg/day, in which its effectiveness may be assumed to be dose-dependent, and this is roughly the same general dosage range used in transfeminine people (though up to 300–400 mg/day may be used and are allowed for by guidelines) (Aly, 2018; Aly, 2020).
A relatively small amount of dose-ranging data on spironolactone in cisgender women with androgen-dependent conditions exists, but in any case substantiates its dose-dependent effectiveness across its clinically used dose range (partially reviewed in Hammerstein (1990) and Shaw (1996)). One study compared spironolactone at doses of 50 to 200 mg/day with placebo for treatment of acne in cisgender women and reported progressive increases in effectiveness with spironolactone up to the 200 mg/day dosage (Goodfellow et al., 1984). Similarly, another study found that progressively increasing the dosage of spironolactone from 100 mg/day, to 150 mg/day, and up to 200 mg/day, resulted in increased effectiveness in the treatment of acne in cisgender women (Charny, Choi, & James, 2017). Spironolactone has been reported to be effective in the treatment of hirsutism in cisgender women at a dosage of as low as 50 mg/day (Diamanti-Kandarakis, Tolis, & Duleba, 1995). However, even a dosage of 100 mg/day did not appear to be maximally effective for hirsutism in a study that compared different doses of spironolactone; effectiveness was near-significantly greater at a dosage of 100 mg/day relative to a dosage of 200 mg/day (19% ± 8% and 30% ± 3% (mean ± SEM) reduction in hair shaft diameter, respectively; p = 0.07) (Lobo et al., 1985). Levels of free testosterone in this study were unchanged, suggesting that the effects of spironolactone was purely due to androgen receptor blockade. Finally, a 2022 systematic review of spironolactone for treatment of androgen-related scalp hair loss in cisgender women reported that the drug was “largely ineffective” at doses of less than 100 mg/day, whereas doses of 100 to 200 mg/day were effective (James, Jamerson, & Aguh, 2022).
Aside from dose-ranging studies, the antiandrogenic efficacy of spironolactone can be evaluated by comparing it to more potent antiandrogenic regimens. A study found that spironolactone 100 mg/day was significantly inferior to flutamide, a substantially more potent androgen receptor antagonist, in improving androgen-dependent skin and hair symptoms in cisgender women (Cusan et al., 1994). However, in other studies, there were no significant differences between spironolactone 100 mg/day and flutamide for hirsutism (Erenus et al., 1994; Moghetti et al., 2000; Inal, Yildirim, & Taner, 2005; Karakurt et al., 2008). Spironolactone and flutamide were variably taken together with an ethinylestradiol-containing combined birth control pill in these studies, which is likely to have limited detection of differences in effectiveness. This is because these birth control pills considerably suppress total and free testosterone levels and hence have substantial antiandrogenic effects themselves (Zimmerman et al., 2014; Amiri et al., 2018). In a biochemical study, spironolactone 100 mg/day was numerically inferior to flutamide in reducing levels of prostate-specific antigen (PSA) in cisgender women (Negri et al., 2000). This is notable as PSA is a systemic biomarker of androgen action (Negri et al., 2000). However, the study had small sample sizes, and the differences between groups were not statistically significant (Negri et al., 2000). A case report of a cisgender woman with female pattern hair loss and normal androgen levels found that treatment with spironolactone 200 mg/day for 5 years failed to improve or halt progression of her hair loss, in spite of almost complete loss of secondary sexual hair, but switching to flutamide resulted in a considerable improvement in hair loss after 12 months (Yazdabadi & Sinclair, 2011 [Figure]). Besides comparison with flutamide, a study found that spironolactone 100 mg/day was inferior to spironolactone 100 mg/day plus finasteride, a 5α-reductase inhibitor and hence functional antiandrogen, for hirsutism in cisgender women (–36.6% vs. –51.3% in scores; p < 0.005) (Unlühizarci et al., 2002; Keleştimur et al., 2004).
The preceding findings suggest that the clinical antiandrogenic effectiveness of spironolactone in cisgender women is not maximal at a dosage of below at least 200 mg/day despite the relatively low testosterone levels in these individuals. Put another way, spironolactone at typical doses seems best-suited for blocking female-range levels of testosterone. As many transfeminine people do not achieve female-range testosterone levels with estradiol plus spironolactone therapy, and in fact often have testosterone levels well above the normal female range or even in the male range, spironolactone may not be fully effective as an antiandrogen at the typical doses used in transfeminine hormone therapy. Higher doses of spironolactone, like 300 to 400 mg/day, may be to some degree more effective.
Summary, Discussion, and Conclusions
Numerous studies have assessed the influence of spironolactone on testosterone levels in cisgender men, cisgender women, and transfeminine people. Although the quality of these studies has often been limited, the studies have revealed highly inconsistent influences of spironolactone on testosterone levels in these populations, with many studies finding no changes, some studies finding decreases, and a small number of studies finding increases. The findings of studies of spironolactone and testosterone levels are in notable contrast to those of studies with estrogens, progestogens like CPA, and GnRH agonists, which consistently show substantial decreases in testosterone levels. This has been the case even in studies of similarly low quality to those of some of the included spironolactone studies (e.g., many of those in cisgender men). The fact that in the available studies testosterone levels with spironolactone have usually been unchanged, but have sometimes been decreased and have rarely been decreased, seems to suggest that spironolactone may be a clinically significant inhibitor of steroid hormone synthesis, but that it is only a weakly efficacious one, and that its effects may be variable depending on the individual and other clinical circumstances. In any case, the conflicting findings warrant more research with higher-quality study designs, particularly RCTs that have with spironolactone versus without comparison groups.
The notion that spironolactone decreases testosterone levels in transfeminine people, and the use of spironolactone in transfeminine hormone therapy in general, appear to have originated from the papers on spironolactone in transfeminine people published by Dr. Jerilynn Prior and colleagues in the 1980s (Prior, Vigna, & Watson, 1989; Prior et al., 1986). In their study, transfeminine people who were either already on high-dose estrogen therapy with inadequate testosterone suppression or had not yet started hormone therapy were put on physiological-dose estrogen therapy in combination with 200 to 600 mg/day spironolactone. Cyclic or continuous administration of the progestogen MPA at an oral dose of 10 mg/day was also given to all of the individuals. The authors reported that despite the lower estrogen dosage, testosterone levels decreased, from 169 ng/dL to 87 ng/dL (–49%) in those who had already been on hormone therapy and to 49 ng/dL in those who were pre-hormone therapy. Prior and her colleagues concluded that spironolactone helps to decrease testosterone levels in transfeminine people and that it can be used as a safer alternative to high doses of estrogen for this purpose.
However, the concomitant use of MPA in the study is a major confounding factor in terms of their results. This is because MPA is a progestogen, and progestogens, like estrogens, are antigonadotropins which are able to robustly suppress testosterone levels on their own (Aly, 2018; Aly, 2019). Indeed, MPA alone has been shown to dose-dependently lower testosterone levels in cisgender men (Wiki), and at a dosage of 10 mg/day, has been shown to considerably suppress testosterone levels in transfeminine people when added to estradiol and spironolactone therapy (Jain, Kwan, & Forcier, 2019). Hence, MPA may have been, and likely was, responsible for the decreases in testosterone levels seen in the study, rather than spironolactone. This point was also notably raised by other researchers, who were unable to replicate Prior and colleagues’ results on spironolactone and testosterone levels in transfeminine people (Leinung et al., 2018). Strangely, Prior and colleagues concluded that spironolactone was responsible for the decreased testosterone levels in their study even though they noted in their papers that MPA was also given to help suppress testosterone levels (as well as to help improve breast development). The work of Prior and colleagues likely resulted in the prominent and long-standing, but poorly supported, notion that spironolactone decreases testosterone levels in transfeminine people. Subsequent studies assessing the hypothesis that spironolactone decreases testosterone levels in transfeminine people were not published until 25 years after Prior and colleagues’ studies, with several of these studies, though not all of them, failing to replicate the earlier findings of Prior and colleagues.
Many people do not realize the capacity of estradiol to substantially and even completely suppress testosterone, and many mistakenly assume that it is the antiandrogen—which is often spironolactone—that is mostly or fully responsible for the decrease in testosterone levels seen with estradiol and antiandrogen therapy in transfeminine people. It is certainly true that antiandrogens like CPA and GnRH agonists play an important role in testosterone suppression in transfeminine people. However, as evidenced by the present review of studies of testosterone suppression with spironolactone, it is not necessarily always the case that the antiandrogen plays a major role—or potentially even any role—in reducing testosterone levels. This is notably also not the case with certain other antiandrogens besides spironolactone, for instance pure androgen receptor antagonists like bicalutamide, which likewise do not decrease testosterone levels but instead can actually increase them (Aly, 2019; Wiki). Clinicians and transfeminine people attributing observations of testosterone decreases to spironolactone rather than to estradiol with estradiol and spironolactone therapy may also have played a role in the perception that spironolactone considerably decreases testosterone levels in transfeminine people.
Due to its relatively weak strength as an androgen receptor antagonist and its limited efficacy in lowering testosterone levels, spironolactone is likely to be a limitedly effective antiandrogen in transfeminine people. Additionally, spironolactone is likely to be less effective than other antiandrogenic approaches used in transfeminine hormone therapy which either more robustly block androgens or more substantially reduce testosterone levels, for instance CPA, other progestogens (e.g., MPA, non-oral progesterone), GnRH agonists (and antagonists), bicalutamide, and high-dose parenteral estradiol monotherapy. These approaches can be used in transfeminine people instead of or in addition to spironolactone, or could be considered when testosterone suppression is inadequate with estradiol and spironolactone.
More studies are needed to evaluate the influence of spironolactone on testosterone levels, especially RCTs that compare estradiol alone versus estradiol plus spironolactone in transfeminine people. More research is also needed to clarify why some studies find highly inadequate testosterone suppression with estradiol alone or estradiol plus spironolactone while other studies find excellent or satisfactory testosterone suppression with these regimens. In any case, available data overall suggest that spironolactone does not consistently suppress testosterone levels, and that estradiol plus spironolactone produces inadequate testosterone suppression in many transfeminine people. Moreover, available data suggest that spironolactone is a relatively weak androgen receptor antagonist at the typical clinical doses used in cisgender women and transfeminine people, and is able to block only relatively low or female-range testosterone levels. Hence, spironolactone may not be fully effective in blocking the testosterone it fails to suppress, and may be particularly unsuitable for transfeminine people with testosterone levels that are well above the normal female range. In any case, more research is similarly needed to assess the androgen receptor antagonism and clinical antiandrogenic effectiveness of spironolactone.
Updates
Update 1: Spironolactone for Adult Female Acne (SAFA) Trial
A large new phase 3 RCT, the Spironolactone for Adult Female Acne (SAFA) trial, was published in May 2023 and assessed the effectiveness of spironolactone in the treatment of acne in cisgender women:
Santer, M., Lawrence, M., Renz, S., Eminton, Z., Stuart, B., Sach, T. H., Pyne, S., Ridd, M. J., Francis, N., Soulsby, I., Thomas, K., Permyakova, N., Little, P., Muller, I., Nuttall, J., Griffiths, G., Thomas, K. S., & Layton, A. M. (2023). Effectiveness of spironolactone for women with acne vulgaris (SAFA) in England and Wales: pragmatic, multicentre, phase 3, double blind, randomised controlled trial. BMJ, 381, e074349. [DOI:10.1136/bmj-2022-074349]
The trial included a total of 342 women, including 176 treated with spironolactone and 166 in the placebo control group. The dose of spironolactone employed was 50 mg/day for the first 6 weeks and then 100 mg/day thereafter. The trial was 24 weeks (5.5 months) in duration. Women who might become pregnant were required to use a hormonal or barrier method of contraception.
Spironolactone significantly outperformed placebo in terms of improvement in mean Acne-QoL symptom scores (higher is better). Significant improvement was apparent within 12 weeks of treatment (+45% in scores with spironolactone, +38% with placebo) and was highest at 24 weeks (+61% in scores with spironolactone, +35% with placebo). There was no difference in the rates of women who reported improvement in acne scores at 12 weeks (72% with spironolactone, 68% with placebo), but there was a significant difference at 24 weeks (82% with spironolactone, 63% with placebo). In terms of the Investigator’s Global Assessment (IGA), treatment success at 12 weeks was 19% with spironolactone and 6% with placebo. Rates of hormonal contraceptive use in the spironolactone and placebo groups were not reported. Testosterone levels were also not reported. A small subset of the women had PCOS (15% in the spironolactone group, 23% in the placebo group).
Adverse effects occurred only slightly more often with spironolactone than with placebo (64% vs. 51%, p = 0.01). The only side effect that occurred significantly more often with spironolactone than with placebo was headache (20% vs. 12%; p = 0.02). However, a few other side effects trended towards occurring significantly more frequently with spironolactone than with placebo: “other” (17% vs. 11%; p = 0.06), dizziness/vertigo/lightheadness (19% vs. 12%; p = 0.07), vomiting/being sick (2% vs. 1%; p = 0.16), and polyuria (urinary frequency) (31% vs. 25%; p = 0.18). Rates of other potentially relevant side effects, like abdominal pain, breast enlargement, breast tenderness, drowsiness/sleepiness, fatigue/tiredness, menstrual irregularity, and reduced libido, were all not different between spironolactone and placebo. There were no serious adverse reactions in the trial. Rates of compliance were similar between the spironolactone and placebo groups, suggesting that spironolactone was well-tolerated.
This trial is the largest and most rigorous RCT of spironolactone in the treatment of androgen-dependent skin and hair conditions in cisgender women that has been conducted to date. Although spironolactone was found to be effective in this study and was about twice as effective as placebo in terms of Acne-QoL symptom scores and three times as effective as placebo in terms of IGA treatment success rates, the effectiveness of spironolactone was seemingly less than in previous clinical studies of spironolactone for acne. This may be related to the relatively low doses of spironolactone used in this study (50–100 mg/day), to the more rigorous and less-risk-of-bias design of the study (large phase 3 RCT), to a possibly too-short treatment duration (24 weeks/5.5 months), and to concomitant hormonal contraceptive use possibly blunting the degree of potential improvement. The latter is relevant as hormonal contraceptives containing ethinylestradiol provide a considerable improvement in acne via functional antiandrogenic effects all on their own. A final possibility however is that spironolactone is simply a less effective antiandrogen even in cisgender women than has been previously thought. On the other hand, similarly to findings in previous clinical studies, spironolactone was well-tolerated and produced few side effects.
Update 2: New Spironolactone and Testosterone Suppression Studies
The following new studies have additionally assessed and found inadequate testosterone suppression in transfeminine people treated with estradiol and spironolactone:
Angus, L. M., Leemaqz, S., Zajac, J. D., & Cheung, A. S. (November 2023). A randomised controlled trial of spironolactone versus cyproterone in trans people commencing estradiol. AusPATH 2023 Symposium. [URL] [PDF] [Trans Health Research Blog Post]
Angus, L. M., Leemaqz, S. Y., Zajac, J. D., & Cheung, A. S. (November 2023). The effect of cyproterone and spironolactone on breast development in transgender women: a randomised controlled trial. ESA/SRB/ENSA 2023 ASM 26-29 November, Brisbane, 54–55 (abstract no. 132). [URL] [PDF] [Full Abstract Book] [Trans Health Research Blog Post]
Miro, E., Rizzone, K., Ho, T., Mark, B., Sullivan, E., & Cushman, D. (2024). 2024 AMSSM Research Podium Presentations: Testosterone Levels Among Transgender Women on Gender-affirming Hormone Therapy. Clinical Journal of Sports Medicine, 34(2), 152–152. [DOI:10.1097/JSM.0000000000001212]
Yang, W., Hong, T., Chang, X., Han, M., Gao, H., Pan, B., Zhao, Z., & Liu, Y. (2024). The efficacy of and user satisfaction with different antiandrogens in Chinese transgender women. International Journal of Transgender Health, advance online publication. [DOI:10.1080/26895269.2024.2323514]
Angus et al. (2023) and Yang et al. (2024) compared estradiol plus spironolactone to estradiol plus CPA and are described in-depth in a section of a different article located here. Yang et al. (2024) found that in addition to spironolactone resulting in much less testosterone suppression than CPA, it was also less effective than CPA as an antiandrogen on multiple clinical measures of demasculinization.
References
Abshagen, U., Spörl, S., Schöneshöfer, M., L’age, M., & Oelkers, W. (1978). Interference of spironolactone therapy with adrenal steroid metabolism in secondary hyperaldosteronism. [Zum Einfluß einer Spironolaktonbehandlung auf den adrenalen Steroidstoffwechsel bei sekundärem Hyperaldosteronismus.] Klinische Wochenschrift, 56(7), 341–349. [DOI:10.1007/bf01477394]
Aizawa, H., & Niimura, M. (1992). Oral Spironolactone Therapy in Male Patients with Rosacea. The Journal of Dermatology, 19(5), 293–297. [DOI:10.1111/j.1346-8138.1992.tb03227.x]
Allen, A. N., Jiao, R., Day, P., Pagels, P., Gimpel, N., & SoRelle, J. A. (2020). Dynamic Impact of Hormone Therapy on Laboratory Values in Transgender Patients over Time. The Journal of Applied Laboratory Medicine, 6(1), 27–40. [DOI:10.1093/jalm/jfaa192]
Almalki, H. H., Alshibani, T. M., Alhifany, A. A., & Almohammed, O. A. (2020). Comparative efficacy of statins, metformin, spironolactone and combined oral contraceptives in reducing testosterone levels in women with polycystic ovary syndrome: a network meta-analysis of randomized clinical trials. BMC Women’s Health, 20(1), 68. [DOI:10.1186/s12905-020-00919-5]
Amiri, M., Kabir, A., Nahidi, F., Shekofteh, M., & Ramezani Tehrani, F. (2018). Effects of combined oral contraceptives on the clinical and biochemical parameters of hyperandrogenism in patients with polycystic ovary syndrome: a systematic review and meta-analysis. The European Journal of Contraception & Reproductive Health Care, 23(1), 64–77. [DOI:10.1080/13625187.2018.1435779]
Angus, L., Leemaqz, S., Ooi, O., Cundill, P., Silberstein, N., Locke, P., Zajac, J. D., & Cheung, A. S. (2019). Cyproterone acetate or spironolactone in lowering testosterone concentrations for transgender individuals receiving oestradiol therapy. Endocrine Connections, 8(7), 935–940. [DOI:10.1530/ec-19-0272]
Angus, L. M., Leemaqz, S., Zajac, J. D., & Cheung, A. S. (2023). A randomised controlled trial of spironolactone versus cyproterone in trans people commencing estradiol. AusPATH 2023 Symposium. [URL] [PDF] [Trans Health Research Blog Post]
Angus, L. M., Leemaqz, S. Y., Zajac, J. D., & Cheung, A. S. (2023). The effect of cyproterone and spironolactone on breast development in transgender women: a randomised controlled trial. ESA/SRB/ENSA 2023 ASM 26-29 November, Brisbane, 54–55 (abstract no. 132). [URL] [PDF] [Full Abstract Book] [Trans Health Research Blog Post]
Angus, L. M., Nolan, B. J., Zajac, J. D., & Cheung, A. S. (2021). A systematic review of antiandrogens and feminization in transgender women. Clinical Endocrinology, 94(5), 743–752. [DOI:10.1111/cen.14329]
Baba, S. (1977). Antiandrogenic effect of spironolactone. The Japanese Journal of Urology, 68(12), 1184–1192. [DOI:10.5980/jpnjurol1928.68.12_1184]
Baba, S., Murai, M., Jitsukawa, S., Hata, M., & Tazaki, H. (1978). Antiandrogenic Effects of Spironolactone: Hormonal and Ultrastructural Studies in Dogs and Men. Journal of Urology, 119(3), 375–380. [DOI:10.1016/s0022-5347(17)57495-9]
Bakker, A. (2021). Een halve eeuw transgenderzorg aan de VU [Half a Century of Transgender Care at the VU]. Amsterdam: Boom. [Google Books] [WorldCat] [URL]
Barrionuevo, P., Nabhan, M., Altayar, O., Wang, Z., Erwin, P. J., Asi, N., Martin, K. A., & Murad, M. H. (2018). Treatment Options for Hirsutism: A Systematic Review and Network Meta-Analysis. The Journal of Clinical Endocrinology & Metabolism, 103(4), 1258–1264. [DOI:10.1210/jc.2017-02052]
Bonne, C., & Raynaud, J. (1974). Mode of spironolactone anti-androgenic action: Inhibition of androstanolone binding to rat prostate androgen receptor. Molecular and Cellular Endocrinology, 2(1), 59–67. [DOI:10.1016/0303-7207(74)90012-4]
Bonzagni, A. F. (2014). Understanding the effects of long-term hormone therapy in transgender individuals being provided care at Boston Medical Center Endocrinology Clinic: a quality assurance project. (Doctoral dissertation, Boston University.) [Google Scholar] [URL] [PDF]
Bradstreet, J. J., Smith, S., Granpeesheh, D., El-Dahr, J. M., & Rossignol, D. (2007). Spironolactone might be a desirable immunologic and hormonal intervention in autism spectrum disorders. Medical Hypotheses, 68(5), 979–987. [DOI:10.1016/j.mehy.2006.10.015]
Brown, J., Farquhar, C., Lee, O., Toomath, R., & Jepson, R. G. (2003). Spironolactone versus placebo or in combination with steroids for hirsutism and/or acne. Cochrane Database of Systematic Reviews, 2003(4), CD000194. [DOI:10.1002/14651858.cd000194]
Brown, J., Farquhar, C., Lee, O., Toomath, R., & Jepson, R. G. (2009). Spironolactone versus placebo or in combination with steroids for hirsutism and/or acne. Cochrane Database of Systematic Reviews, 2009(2), CD000194. [DOI:10.1002/14651858.cd000194.pub2]
Burinkul, S., Panyakhamlerd, K., Suwan, A., Tuntiviriyapun, P., & Wainipitapong, S. (2021). Anti-Androgenic Effects Comparison Between Cyproterone Acetate and Spironolactone in Transgender Women: A Randomized Controlled Trial. The Journal of Sexual Medicine, 18(7), 1299–1307. [DOI:10.1016/j.jsxm.2021.05.003]
Callan, A. W. (1988). Spironolactone therapy in hirsutism and acne. Australasian Journal of Dermatology, 29(3), 135–139. [DOI:10.1111/j.1440-0960.1988.tb00385.x]
Caminos-Torres, R., MA, L., & Snyder, P. J. (1977). Gynecomastia and Semen Abnormalities Induced by Spironolactone in Normal Men. The Journal of Clinical Endocrinology & Metabolism, 45(2), 255–260. [DOI:10.1210/jcem-45-2-255]
Charny, J., Choi, J., & James, W. (2017). Spironolactone for the treatment of acne in women, a retrospective study of 110 patients. International Journal of Women’s Dermatology, 3(2), 111–115. [DOI:10.1016/j.ijwd.2016.12.002]
Cheung, A. S., Ooi, O., Davidoff, D., Leemaqz, S. Y., Cundill, P., Silberstein, N., Bretherton, I., Grossmann, M., & Zajac, J. D. (2018). Cyproterone vs spironolactone as anti-androgen therapy for transgender females receiving oestradiol therapy. Clinical Endocrinology, 89(S1) [Abstracts of the Endocrine Society of Australia’s Annual Scientific Meeting 2017], 14–14 (abstract no. 62). [Google Scholar] [DOI:10.1111/cen.13727] [URL 1] [URL 2] [PDF]
Cirrincione, L. R., Winston McPherson, G., Rongitsch, J., Sadilkova, K., Drees, J. C., Krasowski, M. D., Dickerson, J. A., & Greene, D. N. (2021). Sublingual Estradiol Is Associated with Higher Estrone Concentrations than Transdermal or Injectable Preparations in Transgender Women and Gender Nonbinary Adults. LGBT Health, 8(2), 125–132. [DOI:10.1089/lgbt.2020.0249]
Corvol, P., Mahoudeau, J. A., Valcke, J. C., Ménard, J., & Bricaire, H. (1976). Effets sexuels secondaires des spirolactones. Mécanismes possibles de l’action antiandrogène. [Sexual side-effects of spironolactones. Possible mechanisms of their anti-androgen action]. La Nouvelle Presse Medicale, 5(11), 691–694. [Google Scholar 1] [Google Scholar 2] [PubMed] [PDF]
Cusan, L., Dupont, A., Gomez, J., Tremblay, R. R., & Labrie, F. (1994). Comparison of flutamide and spironolactone in the treatment of hirsutism: a randomized controlled trial. Fertility and Sterility, 61(2), 281–287. [DOI:10.1016/s0015-0282(16)56518-2]
Deutsch, M. B., Bhakri, V., & Kubicek, K. (2015). Effects of Cross-Sex Hormone Treatment on Transgender Women and Men. Obstetrics & Gynecology, 125(3), 605–610. [DOI:10.1097/aog.0000000000000692]
Diamanti-Kandarakis, E., Tolis, G., & Duleba, A. J. (1995). Androgens and Therapeutic Aspects of Antiandrogens in Women. Journal of the Society for Gynecologic Investigation, 2(4), 577–592. [DOI:10.1177/107155769500200401]
Dymling, J., Nilsson, K. O., & Hökfelt, B. (1972). The effect of Soldactona® (canrenoate potassium) on plasma testosterone and androstenedione and urinary 17-ketosteroids and 17-hydroxycorticosteroids. Acta Endocrinologica, 70(1), 104–112. [DOI:10.1530/acta.0.0700104]
Dymling, J. F., & Hökfelt, B. (1973). Reduced plasma testosterone following spirolactone in man. Acta Endocrinologica, 73(Suppl 177) [9th Acta Endocrinologica Congress], 53–53 (abstract no. 53). [Google Scholar] [PDF 1] [PDF 2]
Dymling, J. F. (1978). The effect of spirolactone and spironolactone on plasma testosterone in man. In Addison, G. M., Asmussen, N. W., Corvol, P., Kloppernborg, P. W. C., Norman, N., Schroder, R., & Robertson, J. I. C. (Eds.). Aldosterone Antagonists in Clinical Medicine: Proceedings of the Searle Symposium, Nice, April 13–15, 1978 (pp. 297–302). Amsterdam: Excerpta Medica. [Google Scholar] [Google Books] [WorldCat] [PDF 1] [PDF 2]
Erbler, H. C. (1974). Suppression by the spironolactone metabolite canrenone of plasma testosterone in man. Naunyn-Schmiedeberg’s Archives of Pharmacology, 285(4), 403–406. [DOI:10.1007/bf00501468]
Erenus, M., Gürbüz, O., Durmuşoğlu, F., Demirçay, Z., & Pekin, S. (1994). Comparison of the efficacy of spironolactone versus flutamide in the treatment of hirsutism. Fertility and Sterility, 61(4), 613–616. [DOI:10.1016/s0015-0282(16)56634-5]
Ganie, M. A., Khurana, M. L., Eunice, M., Gulati, M., Dwivedi, S. N., & Ammini, A. C. (2004). Comparison of Efficacy of Spironolactone with Metformin in the Management of Polycystic Ovary Syndrome: An Open-Labeled Study. The Journal of Clinical Endocrinology & Metabolism, 89(6), 2756–2762. [DOI:10.1210/jc.2003-031780]
Ganie, M. A., Khurana, M. L., Nisar, S., Shah, P. A., Shah, Z. A., Kulshrestha, B., Gupta, N., Zargar, M. A., Wani, T. A., Mudasir, S., Mir, F. A., & Taing, S. (2013). Improved Efficacy of Low-Dose Spironolactone and Metformin Combination Than Either Drug Alone in the Management of Women With Polycystic Ovary Syndrome (PCOS): A Six-Month, Open-Label Randomized Study. The Journal of Clinical Endocrinology & Metabolism, 98(9), 3599–3607. [DOI:10.1210/jc.2013-1040]
Goodfellow, A., Alaghband-Zadeh, J., Carter, G., Cream, J., Holland, S., Scully, J., & Wise, P. (1984). Oral spironolactone improves acne vulgaris and reduces sebum excretion. British Journal of Dermatology, 111(2), 209–214. [DOI:10.1111/j.1365-2133.1984.tb04045.x]
Gooren, L. J., Veen, E. A., Kessel, H., Harmsen-Louman, W., & Wiegel, A. R. (1984). Prolactin secretion in the human male is increased by endogenous oestrogens and decreased by exogenous/endogenous androgens. International Journal of Andrology, 7(1), 53–60. [DOI:10.1111/j.1365-2605.1984.tb00759.x]
Gooren, L., Veen, E., Kessel, H., Harmsen-Louman, W., & Wiegel, A. (1984). Androgens in the Feedback Regulation of Gonadotropin Secretion in Men: Effects of Administration of Dihydrotestosterone to Eugonadal and Agonadal Subjects and of Spironolactone to Eugonadal Subjects. Andrologia, 16(4), 289–298. [DOI:10.1111/j.1439-0272.1984.tb00286.x]
Gooren, L. J. G. (1999). Hormonal Sex Reassignment. International Journal of Transgenderism, 3(3), 1–7. [Google Scholar] [URL 1] [URL 2]
Hammerstein, J. (1990). Antiandrogens: Clinical Aspects. In Orfanos, C. E., & Happle, R. (Eds.). Hair and Hair Diseases (pp. 827–886). Berlin/Heidelberg: Springer. [DOI:10.1007/978-3-642-74612-3_35]
Handelsman, D. J., Strasser, S., McDonald, J. A., Conway, A. J., & McCaughan, G. W. (1995). Hypothalamic-pituitary-testicular function in end-stage non-alcoholic liver disease before and after liver transplantation. Clinical Endocrinology, 43(3), 331–337. [DOI:10.1111/j.1365-2265.1995.tb02040.x]
Hecker, A., Hasan, S. H., & Neumann, F. (1980). Disturbances in sexual differentiation of rat foetuses following spironolactone treatment. Acta Endocrinologica, 95(4), 540–545. [DOI:10.1530/acta.0.0950540]
Holland, F. J. (1991). Gonadotropin-lndependent Precocious Puberty. Endocrinology and Metabolism Clinics of North America, 20(1), 191–210. [DOI:10.1016/s0889-8529(18)30288-3]
Horth, C., Lobo, P., Shelton, J., Asbury, M., Clarke, J., & Venning, G. (1977). Effects of spironolaetone on the plasma binding and unbound levels of testosterone and oestradiol in healthy men. Journal of Steroid Biochemistry, 8(12), xx–xx. [DOI:10.1016/0022-4731(77)90178-9]
Horth, C. E., Lobo, P. J., Shelton, J. R., Asbury, M. J., Clarke, J. M., & Venning, G. R. (1979). Effects of spironolactone on the plasma binding and unbound levels of testosterone and oestradiol in healthy men. In Klopper, A., Lerner, L., van der Molen, H. J., & Sciarra, F. (Eds.). Research on Steroids: Proceedings of the International Study Group for Steroid Hormones, Volume 8 / Research on Steroids Transactions of the Eighth Meeting of the International Study Group for Steroid Hormones (Proceedings of the Serono Symposia, Volume 21) (pp. 313–315). London/New York/San Francisco: Academic Press. [Google Scholar]
Huffman, D. H., Kampmann, J. P., Hignite, C. E., & Azarnoff, D. L. (1978). Gynecomastia induced in normal males by spironolactone. Clinical Pharmacology & Therapeutics, 24(4), 465–473. [DOI:10.1002/cpt1978244465]
Inal, M. M., Yildirim, Y., & Taner, C. E. (2005). Comparison of the clinical efficacy of flutamide and spironolactone plus Diane 35 in the treatment of idiopathic hirsutism: a randomized controlled study. Fertility and Sterility, 84(6), 1693–1697. [DOI:10.1016/j.fertnstert.2005.05.051]
Jain, J., Kwan, D., & Forcier, M. (2019). Medroxyprogesterone Acetate in Gender-Affirming Therapy for Transwomen: Results From a Retrospective Study. The Journal of Clinical Endocrinology & Metabolism, 104(11), 5148–5156. [DOI:10.1210/jc.2018-02253]
James, J. F., Jamerson, T. A., & Aguh, C. (2022). Efficacy and safety profile of oral spironolactone use for androgenic alopecia: A systematic review. Journal of the American Academy of Dermatology, 86(2), 425–429. [DOI:10.1016/j.jaad.2021.07.048]
Karakurt, F., Sahin, I., Güler, S., Demirbas, B., Culha, C., Serter, R., Aral, Y., & Bavbek, N. (2008). Comparison of the clinical efficacy of flutamide and spironolactone plus ethinyloestradiol/cyproterone acetate in the treatment of hirsutism: A randomised controlled study. Advances in Therapy, 25(4), 321–328. [DOI:10.1007/s12325-008-0039-5]
Keleştimur, F., Everest, H., Unlühizarci, K., Bayram, F., & Șahin, Y. (2004). A comparison between spironolactone and spironolactone plus finasteride in the treatment of hirsutism. European Journal of Endocrinology, 150(3), 351–354. [DOI:10.1530/eje.0.1500351]
Labrie, C., Cusan, L., Plante, M., Lapointe, S., & Labrie, F. (1987). Analysis of the androgenic activity of synthetic “progestins” currently used for the treatment of prostate cancer. Journal of Steroid Biochemistry, 28(4), 379–384. [DOI:10.1016/0022-4731(87)91054-5]
Layton, A. M., Eady, E. A., Whitehouse, H., Del Rosso, J. Q., Fedorowicz, Z., & van Zuuren, E. J. (2017). Oral Spironolactone for Acne Vulgaris in Adult Females: A Hybrid Systematic Review. American Journal of Clinical Dermatology, 18(2), 169–191. [DOI:10.1007/s40257-016-0245-x]
Leinung, M. C., Feustel, P. J., & Joseph, J. (2018). Hormonal Treatment of Transgender Women with Oral Estradiol. Transgender Health, 3(1), 74–81. [DOI:10.1089/trgh.2017.0035]
Liang, J. J., Jolly, D., Chan, K. J., & Safer, J. D. (2018). Testosterone Levels Achieved by Medically Treated Transgender Women in a United States Endocrinology Clinic Cohort. Endocrine Practice, 24(2), 135–142. [DOI:10.4158/ep-2017-0116]
Lobo, R. A., Shoupe, D., Serafini, P., Brinton, D., & Horton, R. (1985). The effects of two doses of spironolactone on serum androgens and anagen hair in hirsute women. Fertility and Sterility, 43(2), 200–205. [DOI:10.1016/s0015-0282(16)48373-1]
Loriaux, D. L. (1976). Spironolactone and Endocrine Dysfunction. Annals of Internal Medicine, 85(5), 630–630. [DOI:10.7326/0003-4819-85-5-630]
McMullen, G. R., & Van Herle, A. J. (1993). Hirsutism and the effectiveness of spironolactone in its management. Journal of Endocrinological Investigation, 16(11), 925–932. [DOI:10.1007/bf03348960]
Menard, R., Guenthner, T., Kon, H., & Gillette, J. (1979). Studies on the destruction of adrenal and testicular cytochrome P-450 by spironolactone. Requirement for the 7α-thio group and evidence for the loss of the heme and apoproteins of cytochrome P-450. Journal of Biological Chemistry, 254(5), 1726–1733. [DOI:10.1016/s0021-9258(17)37833-x]
Miro, E., Rizzone, K., Ho, T., Mark, B., Sullivan, E., & Cushman, D. (2024). 2024 AMSSM Research Podium Presentations: Testosterone Levels Among Transgender Women on Gender-affirming Hormone Therapy. Clinical Journal of Sports Medicine, 34(2), 152–152. [DOI:10.1097/JSM.0000000000001212]
Miyatake, A., Noma, K., Nakao, K., Morimoto, Y., & Yamamura, Y. (1978). Increased serum oestrone and oestradiol following spironolactone administration in hypertensive men. Clinical Endocrinology, 9(6), 523–533. [DOI:10.1111/j.1365-2265.1978.tb01510.x]
Moghetti, P., Tosi, F., Tosti, A., Negri, C., Misciali, C., Perrone, F., Caputo, M., Muggeo, M., & Castello, R. (2000). Comparison of Spironolactone, Flutamide, and Finasteride Efficacy in the Treatment of Hirsutism: A Randomized, Double Blind, Placebo-Controlled Trial. The Journal of Clinical Endocrinology & Metabolism, 85(1), 89–94. [DOI:10.1210/jcem.85.1.6245]
Negri, C., Tosi, F., Dorizzi, R., Fortunato, A., Spiazzi, G. G., Muggeo, M., Castello, R., & Moghetti, P. (2000). Antiandrogen Drugs Lower Serum Prostate-Specific Antigen (PSA) Levels in Hirsute Subjects: Evidence That Serum PSA Is a Marker of Androgen Action in Women. The Journal of Clinical Endocrinology & Metabolism, 85(1), 81–84. [DOI:10.1210/jcem.85.1.6230]
Pappas, I. I., Craig, W. Y., Spratt, L. V., & Spratt, D. I. (2020). Efficacy of Sex Steroid Therapy Without Progestin or GnRH Agonist for Gonadal Suppression in Adult Transgender Patients. The Journal of Clinical Endocrinology & Metabolism, 106(3), e1290–e1300. [DOI:10.1210/clinem/dgaa884]
Pappas, I. I., Craig, W., Spratt, L. V., & Spratt, D. I. (2020). Testosterone (T) and estradiol (E2) therapy alone can suppress gonadal function in transgender patients. Costas T. Lambrew Research Retreat 2020, 47. [Google Scholar] [URL] [PDF]
Pentikäinen, P. J., Pentikäinen, L. A., Huffman, D. H., & Azarnoff, D. L. (1974). The effect of spironolactone on plasma levels and excretion of testosterone and oestrogens in the urine in males. (A preliminary report). The Journal of International Medical Research, 2(6), 439–443. [Google Scholar] [PubMed] [PDF]
Prior, J. C., Vigna, Y. M., Watson, D., Diewold, P., & Robinow, O. (1986). Spironolactone in the presurgical therapy of male to female transsexuals: Philosophy and experience of the Vancouver Gender Dysphoria Clinic. Journal of Sex Information & Education Council of Canada, 1(1), 1–7. [Google Scholar] [PDF]
Prior, J. C., Vigna, Y. M., & Watson, D. (1989). Spironolactone with physiological female steroids for presurgical therapy of male-to-female transsexualism. Archives of Sexual Behavior, 18(1), 49–57. [DOI:10.1007/bf01579291]
Reardon, E., Farnell, P., Langzettel, J., & Spratt, D. (2013). Efficacy of single agent hormonal therapy in transgender patients to suppress endogenous hypothalamic-pituitary-gonadal (HPG) activity. Fertility and Sterility, 100(3 Suppl) [Scientific Program Supplement: Oral and Poster Session Abstracts 12 October 2013 - 17 October 2013], S333–S333 (abstract no. P-640). [Google Scholar] [DOI:10.1016/j.fertnstert.2013.07.914]
Rose, L. I. (1977). Pathophysiology of Spironolactone-Induced Gynecomastia. Annals of Internal Medicine, 87(4), 398–403. [DOI:10.7326/0003-4819-87-4-398]
Rozner, R. N., Freites-Martinez, A., Shapiro, J., Geer, E. B., Goldfarb, S., & Lacouture, M. E. (2018). Safety of 5α-reductase inhibitors and spironolactone in breast cancer patients receiving endocrine therapies. Breast Cancer Research and Treatment, 174(1), 15–26. [DOI:10.1007/s10549-018-4996-3]
Santen, R. J., Kulin, H. E., Loriaux, D. L., & Friend, J. (1976). Spironolactone Stimulation of Gonadotropin Secretion in Boys with Delayed Adolescence. The Journal of Clinical Endocrinology & Metabolism, 43(6), 1386–1390. [DOI:10.1210/jcem-43-6-1386]
Santer, M., Lawrence, M., Renz, S., Eminton, Z., Stuart, B., Sach, T. H., Pyne, S., Ridd, M. J., Francis, N., Soulsby, I., Thomas, K., Permyakova, N., Little, P., Muller, I., Nuttall, J., Griffiths, G., Thomas, K. S., & Layton, A. M. (2023). Effectiveness of spironolactone for women with acne vulgaris (SAFA) in England and Wales: pragmatic, multicentre, phase 3, double blind, randomised controlled trial. BMJ, 381, e074349. [DOI:10.1136/bmj-2022-074349]
Shaw, J. C. (1996). Antiandrogen and hormonal treatment of acne. Dermatologic Clinics, 14(4), 803–811. [DOI:10.1016/s0733-8635(05)70405-8]
Sivelle, P. C., Underwood, A. H., & Jelly, J. A. (1982). The effects of histamine H2 receptor antagonists on androgen action in vivo and dihydrotestosterone binding to the rat prostate androgen receptor in vitro. Biochemical Pharmacology, 31(5), 677–684. [DOI:10.1016/0006-2952(82)90449-x]
Skorodok, L. M., Savchenko, O. N., & Liss, V. L. (1983). Hypothalamo-hypophyseal-gonadal function in boys with irregular puberty. Neuroscience and Behavioral Physiology, 13(2), 141–145. [DOI:10.1007/bf01190800]
Snyder, B. W., Winneker, R. C., & Batzold, F. H. (1989). Endocrine profile of win 49596 in the rat: A novel androgen receptor antagonist. Journal of Steroid Biochemistry, 33(6), 1127–1132. [DOI:10.1016/0022-4731(89)90419-6]
Sofer, Y., Yaish, I., Yaron, M., Bach, M. Y., Stern, N., & Greenman, Y. (2020). Differential Endocrine and Metabolic Effects of Testosterone Suppressive Agents in Transgender Women. Endocrine Practice, 26(8), 883–890. [DOI:10.4158/ep-2020-0032]
SoRelle, J. A., Jiao, R., Gao, E., Veazey, J., Frame, I., Quinn, A. M., Day, P., Pagels, P., Gimpel, N., & Patel, K. (2019). Impact of Hormone Therapy on Laboratory Values in Transgender Patients. Clinical Chemistry, 65(1), 170–179. [DOI:10.1373/clinchem.2018.292730]
Spörl, S. (1978/1979). Über den Einfluß von Spironolacton (Aldactone®) auf den Stoffwechsel von Nebennierenrindenhormonen und von Testosteron bei Gesunden mit diätinduziertem Hyperaldosterismus. [On the influence of spironolactone (Aldactone®) on the metabolism of adrenocortical hormones and testosterone in healthy individuals with diet-induced hyperaldosteronism.] (Doctoral dissertation, Freie Universität, Berlin.) [Google Scholar] [Google Books] [WorldCat] [PDF]
Spratt, L. V., Reardon, E., Olshan, J. S., & Eimicke, T. (2014). Efficacy of Testosterone (T) or Estradiol (E2) Therapy without a GnRH Agonist or Progestin to Suppress Endogenous Gonadal Activity in Transsexual Patients. Endocrine Reviews, 35(Suppl 1) [Endocrine Society’s 96th Annual Meeting and Expo, June 21–24, 2014 – Chicago], ?–? (abstract no. OR42-2). [DOI:10.1093/edrv/35.supp.1] [URL]
Stewart, I., Spratt, L., Craig, W., Olshan, J., & Spratt, D. (2018). The efficacy of testosterone or estradiol therapy without a GnRH agonist or progestin to suppress endogenous gonadal activity in transgender patients. Fertility and Sterility, 110(4 Suppl) [Scientific Congress Supplement: Oral and Poster Session Abstracts 06 October 2018 - 10 October 2018], e21–e21 (abstract no. O-44). [Google Scholar] [DOI:10.1016/j.fertnstert.2018.07.075]
Stripp, B., Taylor, A. A., Bartter, F. C., Gillette, J. R., Loriaux, D. L., Easley, R., & Menard, R. H. (1975). Effect of Spironolactone on Sex Hormones in Man. The Journal of Clinical Endocrinology & Metabolism, 41(4), 777–781. [DOI:10.1210/jcem-41-4-777]
Taylor, A. A., Rollins, D., Snodgrass, W., & Bartter, F. (1976). Effect of spironolactone (S) on adrenal and gonadal steroids in man. Clinical Research, 24(3), A279–A279. [Google Scholar] [PDF]
Unlühizarci, K., Everest, H., Bayram, F., & Keleştimur, F. (2002). Comparison of spironolactone and spironolactone plus finasteride in the treatment of hirsutism. Fertility and Sterility, 78(6), 1331–1333. [DOI:10.1016/s0015-0282(02)04294-2]
Tidd, M. J., Horth, C. E., Ramsay, L. E., Shelton, J. R., & Palmer, R. F. (1978). Endocrine effects of spironolactone in man. Clinical Endocrinology, 9(5), 389–399. [DOI:10.1111/j.1365-2265.1978.tb03578.x]
van Zuuren, E., & Fedorowicz, Z. (2016). Interventions for hirsutism excluding laser and photoepilation therapy alone: abridged Cochrane systematic review including GRADE assessments. British Journal of Dermatology, 175(1), 45–61. [DOI:10.1111/bjd.14486]
Walsh, P. C., & Siiteri, P. K. (1975). Suppression of Plasma Androgens by Spironolactone in Castrated Men with Carcinoma of the Prostate. Journal of Urology, 114(2), 254–256. [DOI:10.1016/s0022-5347(17)67001-0]
Wang, C., Du, Y., Bi, L., Lin, X., Zhao, M., & Fan, W. (2023). The Efficacy and Safety of Oral and Topical Spironolactone in Androgenetic Alopecia Treatment: A Systematic Review. Clinical, Cosmetic and Investigational Dermatology, 16, 603–612. [DOI:10.2147/ccid.s398950]
Weissmann, A. (1985). Antiandrogenic Effects of Topically Applied Spironolactone on the Hamster Flank Organ. Archives of Dermatology, 121(1), 57–62. [DOI:10.1001/archderm.1985.01660010061019]
Yamasaki, K., Sawaki, M., Noda, S., Muroi, T., Takakura, S., Mitoma, H., Sakamoto, S., Nakai, M., & Yakabe, Y. (2004). Comparison of the Hershberger assay and androgen receptor binding assay of twelve chemicals. Toxicology, 195(2–3), 177–186. [DOI:10.1016/j.tox.2003.09.012]
Yang, W., Hong, T., Chang, X., Han, M., Gao, H., Pan, B., Zhao, Z., & Liu, Y. (2024). The efficacy of and user satisfaction with different antiandrogens in Chinese transgender women. International Journal of Transgender Health, advance online publication. [DOI:10.1080/26895269.2024.2323514]
Yazdabadi, A., & Sinclair, R. (2011). Treatment of female pattern hair loss with the androgen receptor antagonist flutamide. The Australasian Journal of Dermatology, 52(2), 132–134. [DOI:10.1111/j.1440-0960.2010.00735.x]
Zgliczynski, S., Baranowska, B., & Szymanowski, J. (1981). L’influence du spironolactone sur la concentration des gonatrophines et des hormones gonadiques dans l’hypertrophie prostatique. [The influence of spironolactone on the concentration of gonadotrophins and gonadal hormones in prostatic hypertrophy]. Journal d’Urologie, 87(9), 635–638. [Google Scholar 1] [Google Scholar 2] [PubMed] [PDF] [Translation]
Zimmerman, Y., Eijkemans, M. J., Coelingh Bennink, H. J., Blankenstein, M. A., & Fauser, B. C. (2013). The effect of combined oral contraception on testosterone levels in healthy women: a systematic review and meta-analysis. Human Reproduction Update, 20(1), 76–105. [DOI:10.1093/humupd/dmt038]
\ No newline at end of file
diff --git a/transfemscience.org/articles/sublingual-e2-transfem/index.html b/transfemscience.org/articles/sublingual-e2-transfem/index.html
index 67bec7c2..cbf58167 100644
--- a/transfemscience.org/articles/sublingual-e2-transfem/index.html
+++ b/transfemscience.org/articles/sublingual-e2-transfem/index.html
@@ -1 +1 @@
-An Exploration of Sublingual Estradiol as an Alternative to Oral Estradiol in Transfeminine People - Transfeminine Science
An Exploration of Sublingual Estradiol as an Alternative to Oral Estradiol in Transfeminine People
By Sam | First published June 11, 2021 | Last modified March 30, 2024
Abstract / TL;DR
Despite being less well characterised in the medical literature than other formulations, sublingually administered estradiol has been used successfully by several gender clinics around the world. While there may be practical shortcomings associated with the sublingual route, clinical experience and best judgement would suggest it to be effective and affordable when dosed correctly. Sublingual administration of estradiol may be a useful alternative to oral administration for some transfeminine people and can be used for feminising hormone therapy instead.
Introduction
Although the most common way to administer medication in the form of pills or tablets is by the oral route, oral estradiol formulations can otherwise be taken sublingually or buccally (Kuhl, 2005). Sublingual administration refers to the placing of the pill or tablet under the tongue to dissolve and be absorbed into the bloodstream. Buccal administration is similar and refers to placing the medication between the cheek and gums, where it also quickly dissolves and is absorbed (Gass et al., 2004; Bartlett & Maarschalk, 2012).
Many transfeminine people wonder or ask questions on online forums about the sublingual route of administration for estradiol. Some of the most common queries are “What doses of sublingual estradiol should I take?”, “How often should I take sublingual estradiol?”, “Is sublingual estradiol better than oral estradiol?” and so on.
Previously, I reviewed the literature in a comparison of oral and transdermal estradiol (Sam, 2020a). Although many transfeminine people experiment with sublingual estradiol and its use appears to be commonplace among those who self-medicate with estrogens, I did not discuss sublingual or buccal routes of administration in this review. In part, the reason for this was because few studies exist concerning the use of sublingual estradiol compared to conventional and more widely used routes. This is likely also the reason that sublingual estradiol is not discussed in many clinical practice guidelines (Aly, 2020a). Moreover, I wanted to focus specifically on oral estradiol. Since the time of publication of that article, however, several new studies of sublingual estradiol in transfeminine people have been published. In light of this new information, and on account of the many questions asked by transfeminine people online, I believe an in-depth look at this route of administration is warranted. So this is intended to be an overview of the published medical literature regarding sublingual estradiol, with a specific focus on its use in transgender care, aiming to answer some of these questions.
It is of note that, although the sublingual and buccal administration are distinct routes of administration, they are very similar to each other in how they are performed and in their pharmacology (Perloff, 1950; Chandrasekhara et al., 2002). As such, although I have ostensibly chosen to make use of the term “sublingual” in this literature review, much of the content here is applicable to buccal administration of estradiol as well.
Pharmacology of Sublingual Estradiol
While sublingual estradiol has not been as widely used in clinical practice as oral estradiol and other formulations, a number of studies have examined its pharmacology. These studies include both samples of postmenopausal cisgender women and transfeminine people as well as other patient populations (Casper & Yen, 1981; Serhal & Craft, 1989; Deutsch, Bhakri, & Kubicek, 2015; Cirrincione et al., 2021). Both oral estradiol and oral estradiol valerate tablets can be taken sublingually (Serhal, 1990).
After the administration of a dose of oral estradiol, the medication is heavily metabolised and inactivated into estrogen conjugates by the liver (Kuhl, 2005). In turn, these metabolites are gradually converted back into estradiol, which serves to prolong its half life (to approximately 13–20 hours) (Stanczyk, Archer, & Bhavnani, 2013). In contrast to oral estradiol, sublingual estradiol does not pass extensively through the liver and is not significantly deactivated by hepatic metabolism into estrogen metabolites. Instead, sublingually administered estradiol is rapidly absorbed into the bloodstream and directly enters circulation. Consequently, sublingual estradiol has greater bioavailability than oral estradiol, meaning that lower doses are needed to achieve similar AUC estradiol levels (Kuhl, 2005) (Figures 1 and 2). This is an advantage of sublingual estradiol over oral estradiol, as it allows for lower doses to be used and for reduced medication costs.
Because accidental swallowing of some of the estradiol seems probable, the sublingual route is, most likely, actually a combination of sublingual and oral delivery of estradiol (Lobo, 1987; Kuhl, 2005). A preliminary report from an ongoing study of transfeminine people reported that a single 1 mg dose of sublingual estradiol caused an average rise in the level of estradiol up to a maximum of at least 179 pg/mL (657 pmol/L) within one to two hours of administration. In contrast, a peak concentration of just 36 pg/mL (130 pmol/L) was found with the same 1 mg dose administered orally (Doll et al., 2020). Thereafter, estradiol levels decreased rapidly. This response has also been found in other studies of postmenopausal women where a wide range of peak concentrations have been observed (Burnier et al., 1981; Price et al., 1997; Wren et al., 2003). Estradiol levels are found to rapidly rise on the order of ten times that of the peak of oral estradiol, then rapidly decline with an elimination half-life of a few hours (Kuhl, 2005). Sublingual estradiol is somewhat analogous in this respect to intravenously administered estradiol, which also is associated with a rapid increase in estradiol levels and a very short elimination half-life following a dose (Kuhnz, Gansau, & Mahler, 1993). Another route of administration that is similar in this regard is intranasal administration (Devissaguet et al., 1999). Owing to the spikiness and short duration of sublingual estradiol, sublingual estradiol does not achieve as stable of concentrations as other formulations do. As such, this is a marked difference to other formulations of estradiol, such as oral estradiol, that produce much more stable hormone levels that do not fluctuate as much over the course of the day.
A range of estimates have been reported for the relative bioavailability of sublingual estradiol. One small randomised study of postmenopausal women found approximately 2.5-fold higher area-under-the-curve (AUC) levels of estradiol with sublingual estradiol than with the same doses of oral estradiol (Price et al., 1997). Other studies have reported relative bioavailability estimates for sublingual estradiol of up to five times that of oral estradiol (Pines et al., 1999). A study in marmoset monkeys found that the absolute bioavailability of sublingual estradiol was 10%; approximately twice that of conventional absolute bioavailability estimates of oral estradiol (5%, though with a wide range of 0.1 to 12%) (Kuhnz, Blode, & Zimmermann, 1993). Therefore, with respect to AUC levels of estradiol, the sublingual route appears to have between approximately two and five times higher estradiol levels compared to oral estradiol when given at the same doses. Based on these findings, approximate doses of sublingual estradiol for use in transfeminine hormone therapy can be derived (Table 1). It is of note that, at this time, the comparative potency of sublingual estradiol remains to be properly characterised due to a lack of research.
Table 1: Approximately comparable doses of estradiol (E2) and estradiol valerate (EV) administered by the oral and sublingual routes in terms of total estradiol exposure (Price et al., 1997; Pines et al., 1999):
Low Dose
Moderate Dose
High Dose
Very-High Dose
Oral E2
2 mg/day
4 mg/day
8 mg/day
10 mg/day
Sublingual E2a
0.5–1 mg/day
1–2 mg/day
2–4 mg/day
2.5–5 mg/day
Oral EV
3 mg/day
6 mg/day
10 mg/day
12 mg/day
Sublingual EVa
0.75–1.5 mg/day
1.5–3 mg/day
2.5–5 mg/day
3–6 mg/day
a Range calculated by dividing oral doses by two and four to reflect differences in absolute bioavailability and rounding to the nearest 0.25 mg. * Bioidentical estradiol has wide interindividual variation in its pharmacology and the effects of doses may vary significantly between individuals. EV has greater molecular weight and therefore contains less medication for the same amount/dose by weight. It should be noted that estimates for the relative bioavailability of EV are extrapolated from formulations with no valeric ester attached (i.e., E2).
Sublingually Administered Estradiol and Feminisation
The very short half-life of sublingually and buccally administered estradiol relative to other forms raises a few questions for its potential use of sublingual estradiol in feminising hormone therapy. One of the most commonly asked questions on online forums is regarding which gender-affirming hormone therapy regimens might be most “effective” with respect to the feminising effects of estrogens. These include, but are not limited to, outcomes such as breast development and fat distribution.
In contrast to oral and trandermal estradiol, no data exist describing the extent of feminisation with sublingual estradiol (Sam, 2020a). However, as discussed previously, oral and non-oral estradiol have not been found to differ in their effects on breast development or other feminising outcomes in transfeminine people or cisgender hypogondal girls (Rosenfield et al., 2005; Shah et al., 2014; Klaver et al., 2018; de Blok et al., 2021). In consideration of this, differences in efficacy might not be expected for sublingual estradiol either. The fact that several gender clinics have employed sublingual estradiol is also encouraging and suggests that sublingual estradiol is effective for inducing feminization (Deutsch, Bhakri, & Kubicek, 2015; Lim et al., 2019; Cirrincione et al., 2021). Nevertheless, as no studies have been conducted comparing the feminising efficacy of sublingual estradiol with objective measures, it is not possible to say for certain whether or not there is any difference in feminisation outcomes between oral and sublingual estradiol. Hopefully, studies in the future will shed more light on this.
Testosterone Suppressing Efficacy of Sublingually Administered Estradiol
Another question that might be raised by the short half-life of sublingual estradiol is how it might compare to more conventional routes of administration in terms of its ability to suppress testosterone and other androgens.
Estrogens were first characterised for their use as antigonadotrophic antiandrogens in the 1940s, in the form of oral synthetic estrogens, namely diethylstilbestrol (DES), to treat men with prostate cancer (Huggins & Hodges, 1941). Estrogens given in the form of oral ethinylestradiol (EE), long-acting estradiol esters, such as polyestradiol phosphate, and transdermal estradiol patches have been studied. Their efficacy for this indication is well established (Stege et al., 1996; Kohli, 2006; Sciarra et al., 2015). As data are more limited for testosterone suppression with estrogens in transfeminine people, these data are valuable for informing transfeminine hormone therapy. Sublingual estradiol, on the other hand, has never been used as therapy for prostatic cancer and, consequently, no such data exist on the same scale to show the ability of sublingual estradiol in this capacity.
Recent data from some studies have found that physiologic levels of estradiol (i.e., 100–200 pg/mL [367–734 pmol/L]) from non-sublingual estradiol alone result in rapid and near complete, if not complete, suppression of testosterone levels to the female range in many transfeminine people (Leinung, Feustel, & Joseph, 2018; Pappas et al., 2020). Additionally, new data from around 900 men enrolled in the ongoing Prostate Adenocarcinoma TransCutaneous Hormones (PATCH) study, a multicentre randomised controlled trial in the United Kingdom, show that sustained median estradiol levels of between 215 to 250 pg/mL (789–918 pmol/L) from transdermal patches were similarly effective (~95%) to GnRH analogues in reducing testosterone levels to the castrate range (<50 ng/dL [<1.7 nmol/L]) (Langley et al., 2021). However, because of the markedly different pharmacokinetics of sublingual estradiol, it is plausible that estradiol administered in this way might result in sub-par suppression at doses with similar AUC levels of estradiol. Put another way, sustained estradiol levels may be more efficacious with respect to testosterone suppression than the frequent and short-lived “spikes” in estradiol levels that occur with the sublingual route.
There is some weak evidence from pharmacological studies of estradiol that support this possibility. One line of evidence is that some studies of both sublingual and intravenous administration have reported rapid but limited suppression of the gonadotropins (follicle-stimulating hormone and luteinising hormone) in women despite sufficiently elevated estradiol levels for several hours (Tsai & Yen, 1971; Burnier et al., 1981; Casper & Yen, 1981; Hoon et al., 1993). These studies are low quality and indirect since testosterone suppression itself was not measured and they were performed in cisgender women. Another problem is that all were single dose studies and their findings may not translate to multiple dosing. It may be the case that full gonadotropin suppression becomes apparent with repeated physiologic doses of sublingual estradiol. Nevertheless, these studies might suggest a limited effect of sublingual estradiol to fully suppress gonadal function in transfeminine people without the use of excessive doses that would lead to greater health risks or the additional use of other antiandrogens.
It could be the case that monotherapy with sublingual estradiol may not be as effective at comparable doses to the typically employed doses in studies of prostatic cancer (e.g., two to four 100 μg/24 hours transdermal patches). Transdermal patches, gels and parenteral estradiol esters, such as estradiol valerate, injected intramuscularly or subcutaneously might therefore be more reliable choices for monotherapy regimens. On the other hand, sublingual estradiol has been studied in transfeminine people in combination with and without the low-dose use of the progestin medroxyprogesterone acetate (MPA) (Jain, Kwan, & Forcier, 2019). In this study, at least reasonably high rates of testosterone levels within the female range (<50 ng/dL [<1.7 nmol/L]) were achieved by the transfeminine people who took sublingual estradiol together with medroxyprogesterone acetate, showing that sublingual estradiol taken together with other antiandrogens (e.g., 10 mg/day cyproterone acetate) is very likely to be viable for achieving effective testosterone suppression (Aly, 2019).
Monitoring of Estradiol Levels with Sublingual Administration
A further consideration regarding the rapid changes in estradiol levels that occur with the use of sublingual estradiol is the relevance of monitoring of estradiol levels through bloodwork. Currently, consensus guidelines do not recommend a specific time for monitoring of the blood relative to the time of a last dose (Deutsch, 2016; Cheung et al., 2019; T’Sjoen et al., 2020). This may be in part due to practical reasons, or because there is currently no robust data from randomised controlled trials to guide the specifics of dosing in transgender hormone therapy (Haupt et al., 2020). Nevertheless, because estradiol levels vary so significantly with sublingual estradiol, knowledge of how long after the last dose blood was drawn is important to ensure proper interpretation of laboratory results.
For instance, measuring hormone levels just after a dose of sublingual estradiol has been taken might lead to the misinterpretation that levels of estradiol are excessively high and that one’s dosage should be reduced to achieve a more sensible concentration of estradiol in the blood. In reality, this would be a misunderstanding caused by the pharmacology of sublingual estradiol as the point of measurement would be right around the time when estradiol levels are most likely to be at their highest. These estradiol levels would not be indicative of the average amount of exposure, which is the more accurate measure of overall estrogenicity. Similarly, on the opposite end of the scale, drawing blood just before the administration of a new dose might lead to the belief that estrogen levels are too low and, consequently, lead to the use of excessive doses of estrogens. The latter misinterpretation may be more common among people unfamiliar with the pharmacology of sublingual estradiol as levels of estradiol only remain very high in the first few hours after a dose of sublingual estradiol has been taken before falling rapidly.
This oversight may also have implications in studies of sublingual estradiol. For instance, in the previously mentioned respective analysis of the use of sublingual estradiol for gender-affirming hormone therapy, the frequency of administration and time of measurement relative to the last dose were not specified in their results (Jain, Kwan, & Forcier, 2019). Although this data is much needed and is valuable to ongoing research to characterise sublingual estradiol in in transfeminine people, a significant problem is not knowing at what time estradiol levels were measured after the medication was administered. It is difficult to say much about the estradiol levels recorded in this study. Moreover, it is impossible to use this data to help derive equivalent doses of sublingual and oral estradiol.
A possible solution to the problem of rapidly changing hormone levels associated with the sublingual route might simply be to measure when estradiol levels are most likely to be closest to their average. In the case of sublingual estradiol, studies generally find this to be approximately four hours after the administration of a dose, although there is likely to be considerable variation between individuals (Kuhl, 2005). Nevertheless, this approach may give the most representative “snapshot” of overall estrogenic exposure and might help to avoid misleading laboratory data in users of sublingual estradiol.
Administration of Multiple Sublingual Doses Per Day
In order to compensate for the short half-life of sublingually administered estradiol, multiple doses of estrogens can be administered in smaller quantities per day to maintain hormone levels that are somewhat more consistent (Ahokas, Kaukoranta, & Aito, 1999).
In one study of premenopausal women with high-dose estrogen therapy, 2 mg of sublingual estradiol was administered three or four times per day (a total of 6–8 mg/day), resulting in significantly more stable hormone levels than would be expected with a single dose per day (Serhal & Craft, 1989). This was replicated in another study where estradiol was administered three to eight times per day (Ahokas et al., 2001). Conversely, a third study investigating low-dose buccal estradiol found little difference between the “steady-state” estradiol concentrations with a once-daily and twice-daily 0.25 mg dose of buccal estradiol over a 12 hour observation period (Wren et al., 2003). These findings may indicate that sublingual and buccal estradiol needs to be taken at least thrice per day in order to achieve concentrations of estradiol that are more stable.
For the reasons outlined in the subsections above, it would seem advantageous that transfeminine people using sublingual estradiol employ this approach and take sublingual estradiol in divided doses throughout the day; perhaps ideally at least three or four times per day. For instance, instead of taking a 2 mg dose every 24 hours, it would be better to take four 0.5 mg doses in the space of 24 hours (as evenly spaced as practical). Administering sublingual estradiol multiple times throughout the day might be less convenient, but is likely to provide at least somewhat more balanced estradiol levels and potentially better testosterone suppression. The administration of multiple doses every day could be regarded as optimal for the use of sublingually administered estradiol.
Safety and Tolerability
Unfortunately, as with the pharmacokinetics of sublingually and buccally estradiol, the published medical literature concerning the safety and tolerability of this route of administration leaves much to be desired. No long term safety data exist for sublingually administered estradiol in the same way that both oral and transdermal estradiol have been rigorously studied in menopausal women (Rovinski et al., 2018; CGHFBC, 2019).
Adverse Health Effects of Estrogens
With sufficient exposure, owing to their effects in the liver, estrogens are associated with an increased risk of blood clots (Kuhl, 2005; Aly, 2020b). Additionally, under certain circumstances, estrogens can be associated with other cardiovascular complications (Anderson et al., 2004; Mikkola et al., 2005). Although the absolute risk is low in the short-term, these are the most significant health concerns associated with gender-affirming hormone therapy.
A limited number of studies have assessed the effects of sublingually administered estradiol on the liver (Pines et al., 1999; Lim et al., 2019). These data found similar effects on lipids and cholesterol to other estrogens. One line of evidence that indicates sublingual estradiol has greater hepatic impact than other non-oral forms such as trandermal estradiol is the significantly greater quantities of estrone and estrone sulphate that are generated by this route; a marker of estrogenic exposure in the liver (Burnier et al., 1981; Cirrincione et al., 2021). Intense estrogenic activation in the liver is the mechanism by which non-oral estradiol induces a hypercoagulable state at high doses (Sam, 2020b; Sam, 2020c).
While a large body of research does exist concerning the short and long term health effects of estrogens, none of these studies have investigated sublingual or buccal estradiol (Oliver-Williams et al., 2019; Mishra et al., 2021). Given that oral estradiol has greater risks than non-oral estradiol, and that sublingual administration partially but not fully avoids first-pass metabolism, it may be the case that its own risk would be no higher than the risk observed with oral estradiol but no lower than the risk observed with non-oral routes. A retrospective cohort study in the United States found that the incidence of thromboembolism in transfeminine people with an average dose of 4 mg/day oral estradiol was approximately twice that of cisgender controls not taking hormone therapy after adjusting for confounders (HR 2.0, 95% CI 1.4–2.8 versus reference women) (Getahun et al., 2018). These increases in risks are much lower compared to regimens in transfeminine people in the past that included high doses of synthetic estrogens, but it’s important to remember that even such increases can significantly increase morbidity and mortality (Morimont, Dogné, & Douxfils, 2020). It would be advisable to limit doses of sublingual and buccal estradiol so that they are not excessive (i.e., <6 mg/day) in the interest of harm reduction and the balancing of the risks and benefits of gender-affirming hormone therapy.
Non-compliance
A practical obstacle to the use of sublingual estradiol in transfeminine people is that it may be highly inconvenient to have to administer doses thrice, four times or perhaps even more often throughout the duration of a single day. It has been found in observational studies that, in general, the number of prescribed medications and doses per day are positively associated with patient non-compliance and the number of missed doses (Jin et al., 2008; Toh et al., 2014). These findings are especially of relevance to transfeminine people as, in most cases, we require decades of hormone therapy. While missing one dose from time to time may be of little consequence, missing doses repeatedly could be more problematic.
In contrast to sublingual estradiol, the half-life of oral estradiol and transdermal gel is long enough to enable once-daily administration (Wiegratz et al., 2001; Potts & Lobo, 2005). In the case of transdermal patches and parenteral estradiol, these forms only have to be replenished every few days or after even longer intervals of time (Thurman et al., 2013; Wisner et al., 2015). Therefore, when considering the use of sublingual estradiol versus other forms, whether or not it would be practical or convenient to consistently take medication several times a day should probably also be an important consideration for transfeminine people. If not, then another formulation may be preferable for the person in question. This may be especially true for long term use.
Summary and Conclusions
There is much less research investigating sublingual and buccal estradiol than other forms of estrogen. These forms, namely oral and transdermal estrogens, are used in the alleviation of the menopause and for other indications that have historically been more widely used. As a result, they have received much more attention and characterisation than sublingual estradiol has for transfeminine hormone therapy. However, several recent studies have added to our knowledge of sublingual estradiol. Clinical practice guidelines for transgender care that have historically not discussed the use of sublingual estradiol may be adjusted accordingly if more information becomes available.
Sublingual estradiol is different in its pharmacology to other formulations. The main difference is that it is associated with a rapid rise and fall in estradiol levels. It has between two and four times the bioavailability of oral estradiol and hence provides the same total estradiol exposure at doses that are two to four times lower. This is a particular advantage because sublingual estradiol, therefore, is cheaper than oral estradiol, and the higher estradiol levels at the same dose may be helpful for testosterone suppression.
While no evidence exists to show or suggest that sublingual estradiol results in better or inferior feminisation to that experienced with other routes of administration, it is plausible that sublingual estradiol may to some degree result in less testosterone suppression at the same total estradiol exposure. Sublingual estradiol has, nonetheless, been shown to be effective with respect to testosterone suppression when paired with other antiandrogens. Care should be taken with sublingual estradiol when monitoring estradiol levels to ensure correct interpretation. In order to help minimise these potential problems, sublingual estradiol can be taken in multiple doses divided throughout the day.
The health risks of sublingual estradiol have not been quantified in large observational or randomised studies. Therefore, although the partial bypassing of the first pass through the liver is reassuring in this respect, its cardiovascular risk profile is unknown. Sublingual estradiol may be inconvenient and other formulations can be used instead if preferred, particularly for more long-term therapy.
Taken together, although much more research is clearly needed to properly characterise the route, sublingual estradiol may have a number of advantageous properties and may be a useful alternative to oral estradiol in transfeminine hormone therapy.
Updates
Update 1: New Sublingual Estradiol Studies (Added By Aly)
Since this article was first published, the following new relevant studies and papers on sublingual estradiol in transfeminine people have been published:
Doll, E., Gunsolus, I., Thorgerson, A., Tangpricha, V., Lamberton, N., & Sarvaideo, J. L. (2022). Pharmacokinetics of Sublingual Versus Oral Estradiol in Transgender Women. Endocrine Practice, 28(3), 237–242. [DOI:10.1016/j.eprac.2021.11.081]
Safer, J. D. (2022). Are the Pharmacokinetics of Sublingual Estradiol Superior or Inferior to Those of Oral Estradiol? Endocrine Practice, 28(3), 351–352. [DOI:10.1016/j.eprac.2021.12.018]
Sarvaideo, J., Doll, E., & Tangpricha, V. (2022). More Studies Are Needed to Establish the Safety and Efficacy of Sublingual Estradiol in Transgender Women. Endocrine Practice, 28(3), 353–354. [DOI:10.1016/j.eprac.2022.01.004]
Cortez, S., Moog, D., Lewis, C., Williams, K., Herrick, C., Fields, M., Gray, T., Guo, Z., Nicol, G., & Baranski, T. (2023). Effectiveness and Safety of Different Estradiol Regimens in Transgender Women (TREAT Study): Protocol for a Randomized Controlled Trial. JMIR Research Protocols, 12, e53092. [DOI:10.2196/53092]
Jalal, E., & Baldwin, C. (2023). Supratherapeutic Estrogen Levels in Transgender Women Likely From Sublingual Estradiol. Journal of the Endocrine Society, 7(Suppl 1) [ENDO 2023 Abstracts Annual Meeting of the Endocrine Society], A1095–A1096 (abstract no. SAT391/bvad114.2062). [DOI:10.1210/jendso/bvad114.2062] [PDF]
Yaish, I., Gindis, G., Greenman, Y., Moshe, Y., Arbiv, M., Buch, A., Sofer, Y., Shefer, G., & Tordjman, K. (2023). Sublingual Estradiol Offers No Apparent Advantage Over Combined Oral Estradiol and Cyproterone Acetate for Gender-Affirming Hormone Therapy of Treatment-Naive Trans Women: Results of a Prospective Pilot Study. Transgender Health, 8(6), 485–493. [DOI:10.1089/trgh.2023.0022]
Gindis, G., Yaish, I., Greenman, Y., Moshe, Y., Arbiv, M., Buch, A., Sofer, Y., Shefer, G., & Tordjman, K. (May 2023). Sublingual estradiol only, offers no apparent advantage over combined oral estradiol and cyproterone acetate, for Gender Affirming Hormone Therapy (GAHT) of treatment-naive transwomen: Results of a prospective pilot study. Endocrine Abstracts, 90 [25th European Congress of Endocrinology 2023, 13–16 May 2023, Istanbul, Turkey], 274–274 (abstract no. P182). [DOI:10.1530/endoabs.90.p182] [PDF]
Yaish, I., Gindis, G., Greenman, Y., Shefer, G., Buch, A., Arbiv, M., Moshe, Y., Sofer, Y., & Tordjman, K. M. (October 2023). Sublingual Estradiol Only, Compared To Combined Oral Estradiol And Cyproterone Acetate,Offers No Apparent Advantage For Gender Affirming Hormone Therapy (GHAT), In Treatment Naïve Transwomen: Results Of A Prospective Pilot Study. Journal of the Endocrine Society, 7(Suppl 1) [ENDO 2023 Abstracts Annual Meeting of the Endocrine Society], A1104–A1105 (abstract no. SAT409/bvad114.2080). [DOI:10.1210/jendso/bvad114.2080] [PDF]
Kariyawasam, N. M., Ahmad, T., Sarma, S., & Fung, R. (2024). Comparison of Estrone/Estradiol Ratio and Levels in Transfeminine Individuals on Different Routes of Estradiol. Transgender Health, online ahead of print. [DOI:10.1089/trgh.2023.0138]
References
Ahokas, A., Kaukoranta, J., & Aito, M. (1999). Effect of oestradiol on postpartum depression. Psychopharmacology, 146(1), 108–110. [DOI:10.1007/s002130051095]
Ahokas, A., Kaukoranta, J., Wahlbeck, K., & Aito, M. (2001). Estrogen deficiency in severe postpartum depression: successful treatment with sublingual physiologic 17β-estradiol: a preliminary study. Journal of Clinical Psychiatry, 62(5), 332–336. [DOI:10.4088/jcp.v62n0504] [PDF]
Anderson, G. L., Limacher, M., Assaf, A. R., Bassford, T., Beresford, S. A., Black, H., Bonds, D., Brunner, R., Brzyski, R., Caan, B., Chlebowski, R., Curb, D., Gass, M., Hays, J., Heiss, G., Hendrix, S., Howard, B. V., Hsia, J., Hubbell, A., Jackson, R., … & Women’s Health Initiative Steering Committee. (2004). Effects of Conjugated Equine Estrogen in Postmenopausal Women With Hysterectomy: The Women’s Health Initiative Randomized Controlled Trial. JAMA, 291(14), 1701–1712. [DOI:10.1001/jama.291.14.1701]
Bartlett, J. A., & van der Voort Maarschalk, K. (2012). Understanding the oral mucosal absorption and resulting clinical pharmacokinetics of asenapine. AAPS Pharmscitech, 13(4), 1110–1115. [DOI:10.1208/s12249-012-9839-7]
Burnier, A. M., Martin, P. L., Yen, S. S., & Brooks, P. (1981). Sublingual absorption of micronized 17β-estradiol. American Journal of Obstetrics and Gynecology, 140(2), 146–150. [DOI:10.1016/0002-9378(81)90101-0]
Casper, R. F., & Yen, S. S. (1981). Rapid absorption of micronized estradiol-17β following sublingual administration. Obstetrics and Gynecology, 57(1), 62–64. [Google Scholar] [PubMed] [URL] [PDF]
Chandrasekhara, D. S., Ali, V., Prost, H. M., & Nader-Estekhari, S. (2002). Buccal estrogen in toothpaste study: systemic absorption of estradiol in postmenopausal or surgically menopausal women when administered as a component in toothpaste. Fertility and Sterility, 78(Suppl 1), S98–S98 (O-258). [DOI:10.1016/S0015-0282(02)03639-7]
Cheung, A. S., Wynne, K., Erasmus, J., Murray, S., & Zajac, J. D. (2019). Position statement on the hormonal management of adult transgender and gender diverse individuals. Medical Journal of Australia, 211(3), 127–133. [DOI:10.5694/mja2.50259]
Cirrincione, L. R., Winston McPherson, G., Rongitsch, J., Sadilkova, K., Drees, J. C., Krasowski, M. D., Dickerson, J. A., & Greene, D. N. (2021). Sublingual Estradiol Is Associated with Higher Estrone Concentrations than Transdermal or Injectable Preparations in Transgender Women and Gender Nonbinary Adults. LGBT Health, 8(2), 125–132. [DOI:10.1089/lgbt.2020.0249]
Collaborative Group on Hormonal Factors in Breast Cancer. (2019). Type and timing of menopausal hormone therapy and breast cancer risk: individual participant meta-analysis of the worldwide epidemiological evidence. The Lancet, 394(10204), 1159–1168. [DOI:10.1016/S0140-6736(19)31709-X]
Cortez, S., Moog, D., Lewis, C., Williams, K., Herrick, C., Fields, M., Gray, T., Guo, Z., Nicol, G., & Baranski, T. (2023). Effectiveness and Safety of Different Estradiol Regimens in Transgender Women (TREAT Study): Protocol for a Randomized Controlled Trial. JMIR Research Protocols, 12, e53092. [DOI:10.2196/53092]
de Blok, C., Dijkman, B., Wiepjes, C. M., Staphorsius, A. S., Timmermans, F. W., Smit, J. M., Dreijerink, K., & den Heijer, M. (2021). Sustained Breast Development and Breast Anthropometric Changes in 3 Years of Gender-Affirming Hormone Treatment. The Journal of Clinical Endocrinology & Metabolism, 106(2), e782–e790. [DOI:10.1210/clinem/dgaa841]
Deutsch, M. B., Bhakri, V., & Kubicek, K. (2015). Effects of cross-sex hormone treatment on transgender women and men. Obstetrics and Gynecology, 125(3), 605–610. [DOI:10.1097/AOG.0000000000000692]
Deutsch, M. B. (Ed.). (2016). Guidelines for the Primary and Gender-Affirming Care of Transgender and Gender Nonbinary People, 2nd Edition. San Francisco: University of California, San Francisco/UCSF Transgender Care. [URL] [PDF]
Devissaguet, J. P., Brion, N., Lhote, O., & Deloffre, P. (1999). Pulsed estrogen therapy: pharmacokinetics of intranasal 17-beta-estradiol (S21400) in postmenopausal women and comparison with oral and transdermal formulations. European Journal of Drug Metabolism and Pharmacokinetics, 24(3), 265–271. [DOI:10.1007/BF03190030]
Doll, E. E., Gunsolus, I., Lamberton, N., Tangpricha, V., & Sarvaideo, J. L. (2020). Pharmacokinetics of Sublingual Versus Oral Estradiol in Transgender Women. Journal of the Endocrine Society, 4(Suppl 1), A1128–A1128 (SUN-LB9). [DOI:10.1210/jendso/bvaa046.2237]
Doll, E., Gunsolus, I., Thorgerson, A., Tangpricha, V., Lamberton, N., & Sarvaideo, J. L. (2022). Pharmacokinetics of Sublingual Versus Oral Estradiol in Transgender Women. Endocrine Practice, 28(3), 237–242. [DOI:10.1016/j.eprac.2021.11.081]
Fiet, J., Hermano, M., Witte, J., Villette, J. M., Haimart, M., Gourmel, B., Tabuteau, F., Rouffy, J., & Dreux, C. (1982). Post-menopausal concentrations of plasma oestradiol, oestrone, FSH and LH and of total urinary oestradiol and oestrone after a single sublingual dose of oestradiol-17β. Acta Endocrinologica, 101(1), 93–97. [DOI:10.1530/acta.0.1010093]
Gass, M. S., Rebar, R. W., Cuffie-Jackson, C., Cedars, M. I., Lobo, R. A., Shoupe, D., Judd, H. L., Buyalos, R. P., & Clisham, P. R. (2004). A short study in the treatment of hot flashes with buccal administration of 17-β estradiol. Maturitas, 49(2), 140–147. [DOI:10.1016/j.maturitas.2003.12.004]
Getahun, D., Nash, R., Flanders, W. D., Baird, T. C., Becerra-Culqui, T. A., Cromwell, L., Hunkeler, E., Lash, T. L., Millman, A., Quinn, V. P., Robinson, B., Roblin, D., Silverberg, M. J., Safer, J., Slovis, J., Tangpricha, V., & Goodman, M. (2018). Cross-sex hormones and acute cardiovascular events in transgender persons: a cohort study. Annals of Internal Medicine, 169(4), 205–213. [DOI:10.7326/M17-2785]
Gindis, G., Yaish, I., Greenman, Y., Moshe, Y., Arbiv, M., Buch, A., Sofer, Y., Shefer, G., & Tordjman, K. (May 2023). Sublingual estradiol only, offers no apparent advantage over combined oral estradiol and cyproterone acetate, for Gender Affirming Hormone Therapy (GAHT) of treatment-naive transwomen: Results of a prospective pilot study. Endocrine Abstracts, 90 [25th European Congress of Endocrinology 2023, 13–16 May 2023, Istanbul, Turkey], 274–274 (abstract no. P182). [DOI:10.1530/endoabs.90.p182] [PDF]
Haupt, C., Henke, M., Kutschmar, A., Hauser, B., Baldinger, S., Saenz, S. R., & Schreiber, G. (2020). Antiandrogen or estradiol treatment or both during hormone therapy in transitioning transgender women. Cochrane Database of Systematic Reviews, 11(11), CD013138. [DOI:10.1002/14651858.CD013138.pub2]
Hoon, T. J., Dawood, M. Y., Khan‐Dawood, F. S., Ramos, J., & Batenhorst, R. L. (1993). Bioequivalence of a 17β‐Estradiol Hydroxypropyl‐β‐Cyclodextrin Complex in Postmenopausal Women. The Journal of Clinical Pharmacology, 33(11), 1116–1121. [DOI:10.1002/j.1552-4604.1993.tb01949.x]
Huggins, C., & Hodges, C. V. (1941). Studies on prostatic cancer. I. The effect of castration, of estrogen and of androgen injection on serum phosphatases in metastatic carcinoma of the prostate. Cancer Research, 1(4), 293–297. [DOI:10.3322/canjclin.22.4.232]
Jain, J., Kwan, D., & Forcier, M. (2019). Medroxyprogesterone acetate in Gender-Affirming therapy for Transwomen: results from a retrospective study. The Journal of Clinical Endocrinology & Metabolism, 104(11), 5148–5156. [DOI:10.1210/jc.2018-02253]
Jalal, E., & Baldwin, C. (2023). Supratherapeutic Estrogen Levels in Transgender Women Likely From Sublingual Estradiol. Journal of the Endocrine Society, 7(Suppl 1) [ENDO 2023 Abstracts Annual Meeting of the Endocrine Society], A1095–A1096 (abstract no. SAT391/bvad114.2062). [DOI:10.1210/jendso/bvad114.2062] [PDF]
Jin, J., Sklar, G. E., Oh, V. M. S., & Li, S. C. (2008). Factors affecting therapeutic compliance: A review from the patient’s perspective. Therapeutics and Clinical Risk Management, 4(1), 269–286. [DOI:10.2147/TCRM.S1458]
Kariyawasam, N. M., Ahmad, T., Sarma, S., & Fung, R. (2024). Comparison of Estrone/Estradiol Ratio and Levels in Transfeminine Individuals on Different Routes of Estradiol. Transgender Health, online ahead of print. [DOI:10.1089/trgh.2023.0138]
Klaver, M., de Blok, C. J. M., Wiepjes, C. M., Nota, N. M., Dekker, M. J., de Mutsert, R., Schreiner, T., Fisher, A. D., T’Sjoen, G., & den Heijer, M. (2018). Changes in regional body fat, lean body mass and body shape in trans persons using cross-sex hormonal therapy: results from a multicenter prospective study. European Journal of Endocrinology, 178(2), 163–171. [DOI:10.1530/EJE-17-0496]
Kohli, M. (2006). Phase II study of transdermal estradiol in androgen‐independent prostate carcinoma. Cancer, 106(1), 234–235. [DOI:10.1002/cncr.21528]
Kuhl, H. (2005). Pharmacology of estrogens and progestogens: influence of different routes of administration. Climacteric, 8(Suppl 1), 3–63. [DOI:10.1080/13697130500148875] [PDF]
Kuhnz, W., Blode, H., & Zimmermann, H. (1993). Pharmacokinetics of exogenous natural and synthetic estrogens and antiestrogens. In Oettel, M., & Schillinger, E. (Eds.). Estrogens and Antiestrogens II: Pharmacology and Clinical Application of Estrogens and Antiestrogen (Handbook of Experimental Pharmacology, Volume 135, Part 2) (pp. 261–322). Berlin/Heidelberg: Springer. [DOI:10.1007/978-3-642-60107-1_15]
Kuhnz, W., Gansau, C., & Mahler, M. (1993). Pharmacokinetics of estradiol, free and total estrone, in young women following single intravenous and oral administration of 17β-estradiol. Arzneimittelforschung, 43(9), 966–973. [Google Scholar] [PubMed] [PDF]
Langley, R. E., Gilbert, D. C., Duong, T., Clarke, N. W., Nankivell, M., Rosen, S. D., Mangar, S., Macnair, A., Sundaram, S. K., Laniado, M. E., Dixit, S., Madaan, S., Manetta, C., Pope, A., Scrase, C. D., Mckay, S., Muazzam, I. A., Collins, G. N., Worlding, J., Williams, S. T., … & Parmar, M. (2021). Transdermal oestradiol for androgen suppression in prostate cancer: long-term cardiovascular outcomes from the randomised Prostate Adenocarcinoma Transcutaneous Hormone (PATCH) trial programme. The Lancet, 397(10274), 581–591. [DOI:10.1016/S0140-6736(21)00100-8]
Leinung, M. C., Feustel, P. J., & Joseph, J. (2018). Hormonal treatment of transgender women with oral estradiol. Transgender Health, 3(1), 74–81. [DOI:10.1089/trgh.2017.0035]
Lim, H. H., Jang, Y. H., Choi, G. Y., Lee, J. J., & Lee, E. S. (2019). Gender affirmative care of transgender people: a single center’s experience in Korea. Obstetrics & Gynecology Science, 62(1), 46–55. [DOI:10.5468/ogs.2019.62.1.46]
Lobo, R. A. (1987). Absorption and metabolic effects of different types of estrogens and progestogens. Obstetrics and Gynecology Clinics of North America, 14(1), 143–167. [PubMed] [DOI:10.1016/S0889-8545(21)00577-5] [URL] [PDF]
Mikkola, A., Aro, J., Rannikko, S., Oksanen, H., Ruutu, M., & Finnprostate Group. (2005). Cardiovascular complications in patients with advanced prostatic cancer treated by means of orchiectomy or polyestradiol phosphate. Scandinavian Journal of Urology and Nephrology, 39(4), 294–300. [DOI:10.1080/00365590510031228]
Mishra, S. R., Chung, H. F., Waller, M., & Mishra, G. D. (2021). Duration of estrogen exposure during reproductive years, age at menarche and age at Menopause, and risk of cardiovascular disease events, all‐cause and cardiovascular mortality: a systematic review and meta‐analysis. BJOG: An International Journal of Obstetrics & Gynaecology, 128(5), 809–821. [DOI:10.1111/1471-0528.16524]
Morimont, L., Dogné, J. M., & Douxfils, J. (2020). Letter to the Editors-in-Chief in response to the article of Abou-Ismail, et al. entitled “Estrogen and thrombosis: A bench to bedside review” (Thrombosis Research 192 (2020) 40–51). Thrombosis Research, 193, 221–223. [DOI:10.1016/j.thromres.2020.08.006]
Oliver-Williams, C., Glisic, M., Shahzad, S., Brown, E., Pellegrino Baena, C., Chadni, M., Chowdhury, R., Franco, O. H., & Muka, T. (2019). The route of administration, timing, duration and dose of postmenopausal hormone therapy and cardiovascular outcomes in women: a systematic review. Human Reproduction Update, 25(2), 257–271. [DOI:10.1093/humupd/dmy039]
Pappas, I. I., Craig, W. Y., Spratt, L. V., & Spratt, D. I. (2021). Efficacy of Sex Steroid Therapy Without Progestin or GnRH Agonist for Gonadal Suppression in Adult Transgender Patients. The Journal of Clinical Endocrinology & Metabolism, 106(3), e1290–e1300. [DOI:10.1210/clinem/dgaa884]
Perloff, W. H. (1950). Estradiol buccal tablets in the treatment of the menopause. American Journal of Obstetrics and Gynecology, 59(1), 223–225. [DOI:10.1016/0002-9378(50)90390-5]
Pickar, J. H., Bon, C., Amadio, J. M., Mirkin, S., & Bernick, B. (2015). Pharmacokinetics of the first combination 17β-estradiol/progesterone capsule in clinical development for menopausal hormone therapy. Menopause, 22(12), 1308–1316. [DOI:10.1097/GME.0000000000000467]
Pines, A., Averbuch, M., Fisman, E. Z., & Rosano, G. M. (1999). The acute effects of sublingual 17β-estradiol on the cardiovascular system. Maturitas, 33(1), 81–85. [DOI:10.1016/S0378-5122(99)00036-5]
Potts, R. O., & Lobo, R. A. (2005). Transdermal drug delivery: clinical considerations for the obstetrician–gynecologist. Obstetrics & Gynecology, 105(5), 953–961. [DOI:10.1097/01.AOG.0000161958.70059.db]
Price, T. M., Blauer, K. L., Hansen, M., Stanczyk, F., Lobo, R., & Bates, G. W. (1997). Single-dose pharmacokinetics of sublingual versus oral administration of micronized 17β-estradiol. Obstetrics & Gynecology, 89(3), 340–345. [DOI:10.1016/S0029-7844(96)00513-3]
Rosenfield, R. L., Devine, N., Hunold, J. J., Mauras, N., Moshang Jr, T., & Root, A. W. (2005). Salutary effects of combining early very low-dose systemic estradiol with growth hormone therapy in girls with Turner syndrome. The Journal of Clinical Endocrinology & Metabolism, 90(12), 6424–6430. [DOI:10.1210/jc.2005-1081]
Rovinski, D., Ramos, R. B., Fighera, T. M., Casanova, G. K., & Spritzer, P. M. (2018). Risk of venous thromboembolism events in postmenopausal women using oral versus non-oral hormone therapy: a systematic review and meta-analysis. Thrombosis Research, 168, 83–95. [DOI:10.1016/j.thromres.2018.06.014]
Safer, J. D. (2022). Are the Pharmacokinetics of Sublingual Estradiol Superior or Inferior to Those of Oral Estradiol? Endocrine Practice, 28(3), 351–352. [DOI:10.1016/j.eprac.2021.12.018]
Sarvaideo, J., Doll, E., & Tangpricha, V. (2022). More Studies Are Needed to Establish the Safety and Efficacy of Sublingual Estradiol in Transgender Women. Endocrine Practice, 28(3), 353–354. [DOI:10.1016/j.eprac.2022.01.004]
Sciarra, A., Gentile, V., Cattarino, S., Gentilucci, A., Alfarone, A., D’Eramo, G., & Salciccia, S. (2015). Oral ethinylestradiol in castration‐resistant prostate cancer: a 10‐year experience. International Journal of Urology, 22(1), 98–103. [DOI:10.1111/iju.12613]
Serhal, P., & Craft, I. (1989). Oocyte donation in 61 patients. The Lancet, 333(8648), 1185–1187. [DOI:10.1016/S0140-6736(89)92762-1]
Shah, S., Forghani, N., Durham, E., & Neely, E. K. (2014). A randomized trial of transdermal and oral estrogen therapy in adolescent girls with hypogonadism. International Journal of Pediatric Endocrinology, 2014(1), 12. [DOI:10.1186/1687-9856-2014-12]
Stanczyk, F. Z., Archer, D. F., & Bhavnani, B. R. (2013). Ethinyl estradiol and 17β-estradiol in combined oral contraceptives: pharmacokinetics, pharmacodynamics and risk assessment. Contraception, 87(6), 706–727. [DOI:10.1016/j.contraception.2012.12.011]
Stege, R., Gunnarsson, P. O., Johansson, C. J., Olsson, P., Pousette, Å., & Carlström, K. (1996). Pharmacokinetics and testosterone suppression of a single dose of polyestradiol phosphate (Estradurin®) in prostatic cancer patients. The Prostate, 28(5), 307–310. [DOI:10.1002/(SICI)1097-0045(199605)28:5<307::AID-PROS6>3.0.CO;2-8]
T’Sjoen, G., Arcelus, J., De Vries, A. L., Fisher, A. D., Nieder, T. O., Özer, M., & Motmans, J. (2020). European Society for Sexual Medicine position statement “assessment and hormonal management in adolescent and adult trans people, with attention for sexual function and satisfaction”. The Journal of Sexual Medicine, 17(4), 570–584. [DOI:10.1016/j.jsxm.2020.01.012]
Thurman, A., Kimble, T., Hall, P., Schwartz, J. L., & Archer, D. F. (2013). Medroxyprogesterone acetate and estradiol cypionate injectable suspension (Cyclofem) monthly contraceptive injection: steady-state pharmacokinetics. Contraception, 87(6), 738–743. [DOI:10.1016/j.contraception.2012.11.010]
Toh, M. R., Teo, V., Kwan, Y. H., Raaj, S., Tan, S. Y. D., & Tan, J. Z. Y. (2014). Association between number of doses per day, number of medications and patient’s non-compliance, and frequency of readmissions in a multi-ethnic Asian population. Preventive Medicine Reports, 1, 43–47. [DOI:10.1016/j.pmedr.2014.10.001]
Tsai, C. C., & Yen, S. S. C. (1971). Acute effects of intravenous infusion of 17β-estradiol on gonadotropin release in pre-and post-menopausal women. The Journal of Clinical Endocrinology & Metabolism, 32(6), 766–771. [DOI:10.1210/jcem-32-6-766]
Verdonk, S. J., Vesper, H. W., Martens, F., Sluss, P. M., Hillebrand, J. J., & Heijboer, A. C. (2019). Estradiol reference intervals in women during the menstrual cycle, postmenopausal women and men using an LC-MS/MS method. Clinica Chimica Acta, 495, 198–204. [DOI:10.1016/j.cca.2019.04.062]
Wiegratz, I., Fink, T., Rohr, U. D., Lang, E., Leukel, P., & Kuhl, H. (2001). Überkreuz-Vergleich der Pharmakokinetik von Estradiol unter der Hormonsubstitution mit Estradiolvalerat oder mikronisiertem Estradiol. [Cross-over comparison of the pharmacokinetics of estradiol during hormone replacement therapy with estradiol valerate or micronized estradiol.] Zentralblatt für Gynäkologie, 123(9), 505–512. [PubMed] [DOI:10.1055/s-2001-18223]
Wisner, K. L., Sit, D. K., Moses-Kolko, E. L., Driscoll, K. E., Prairie, B. A., Stika, C. S., Eng, H. F., Dills, J. L., Luther, J. F., & Wisniewski, S. R. (2015). Transdermal estradiol treatment for postpartum depression: a pilot randomized trial. Journal of Clinical Psychopharmacology, 35(4), 389–395. [DOI:10.1097/JCP.0000000000000351]
Wren, B. G., Day, R. O., McLachlan, A. J., & Williams, K. M. (2003). Pharmacokinetics of estradiol, progesterone, testosterone and dehydroepiandrosterone after transbuccal administration to postmenopausal women. Climacteric, 6(2), 104–111. [DOI:10.1080/cmt.6.2.104.111]
Yaish, I., Gindis, G., Greenman, Y., Moshe, Y., Arbiv, M., Buch, A., Sofer, Y., Shefer, G., & Tordjman, K. (2023). Sublingual Estradiol Offers No Apparent Advantage Over Combined Oral Estradiol and Cyproterone Acetate for Gender-Affirming Hormone Therapy of Treatment-Naive Trans Women: Results of a Prospective Pilot Study. Transgender Health, 8(6), 485–493. [DOI:10.1089/trgh.2023.0022]
Yaish, I., Gindis, G., Greenman, Y., Shefer, G., Buch, A., Arbiv, M., Moshe, Y., Sofer, Y., & Tordjman, K. M. (2023). Sublingual Estradiol Only, Compared To Combined Oral Estradiol And Cyproterone Acetate,Offers No Apparent Advantage For Gender Affirming Hormone Therapy (GHAT), In Treatment Naïve Transwomen: Results Of A Prospective Pilot Study. Journal of the Endocrine Society, 7(Suppl 1) [ENDO 2023 Abstracts Annual Meeting of the Endocrine Society], A1104–A1105 (abstract no. SAT409/bvad114.2080). [DOI:10.1210/jendso/bvad114.2080] [PDF]
\ No newline at end of file
+An Exploration of Sublingual Estradiol as an Alternative to Oral Estradiol in Transfeminine People - Transfeminine Science
An Exploration of Sublingual Estradiol as an Alternative to Oral Estradiol in Transfeminine People
By Sam | First published June 11, 2021 | Last modified March 30, 2024
Abstract / TL;DR
Despite being less well characterised in the medical literature than other formulations, sublingually administered estradiol has been used successfully by several gender clinics around the world. While there may be practical shortcomings associated with the sublingual route, clinical experience and best judgement would suggest it to be effective and affordable when dosed correctly. Sublingual administration of estradiol may be a useful alternative to oral administration for some transfeminine people and can be used for feminising hormone therapy instead.
Introduction
Although the most common way to administer medication in the form of pills or tablets is by the oral route, oral estradiol formulations can otherwise be taken sublingually or buccally (Kuhl, 2005). Sublingual administration refers to the placing of the pill or tablet under the tongue to dissolve and be absorbed into the bloodstream. Buccal administration is similar and refers to placing the medication between the cheek and gums, where it also quickly dissolves and is absorbed (Gass et al., 2004; Bartlett & Maarschalk, 2012).
Many transfeminine people wonder or ask questions on online forums about the sublingual route of administration for estradiol. Some of the most common queries are “What doses of sublingual estradiol should I take?”, “How often should I take sublingual estradiol?”, “Is sublingual estradiol better than oral estradiol?” and so on.
Previously, I reviewed the literature in a comparison of oral and transdermal estradiol (Sam, 2020a). Although many transfeminine people experiment with sublingual estradiol and its use appears to be commonplace among those who self-medicate with estrogens, I did not discuss sublingual or buccal routes of administration in this review. In part, the reason for this was because few studies exist concerning the use of sublingual estradiol compared to conventional and more widely used routes. This is likely also the reason that sublingual estradiol is not discussed in many clinical practice guidelines (Aly, 2020a). Moreover, I wanted to focus specifically on oral estradiol. Since the time of publication of that article, however, several new studies of sublingual estradiol in transfeminine people have been published. In light of this new information, and on account of the many questions asked by transfeminine people online, I believe an in-depth look at this route of administration is warranted. So this is intended to be an overview of the published medical literature regarding sublingual estradiol, with a specific focus on its use in transgender care, aiming to answer some of these questions.
It is of note that, although the sublingual and buccal administration are distinct routes of administration, they are very similar to each other in how they are performed and in their pharmacology (Perloff, 1950; Chandrasekhara et al., 2002). As such, although I have ostensibly chosen to make use of the term “sublingual” in this literature review, much of the content here is applicable to buccal administration of estradiol as well.
Pharmacology of Sublingual Estradiol
While sublingual estradiol has not been as widely used in clinical practice as oral estradiol and other formulations, a number of studies have examined its pharmacology. These studies include both samples of postmenopausal cisgender women and transfeminine people as well as other patient populations (Casper & Yen, 1981; Serhal & Craft, 1989; Deutsch, Bhakri, & Kubicek, 2015; Cirrincione et al., 2021). Both oral estradiol and oral estradiol valerate tablets can be taken sublingually (Serhal, 1990).
After the administration of a dose of oral estradiol, the medication is heavily metabolised and inactivated into estrogen conjugates by the liver (Kuhl, 2005). In turn, these metabolites are gradually converted back into estradiol, which serves to prolong its half life (to approximately 13–20 hours) (Stanczyk, Archer, & Bhavnani, 2013). In contrast to oral estradiol, sublingual estradiol does not pass extensively through the liver and is not significantly deactivated by hepatic metabolism into estrogen metabolites. Instead, sublingually administered estradiol is rapidly absorbed into the bloodstream and directly enters circulation. Consequently, sublingual estradiol has greater bioavailability than oral estradiol, meaning that lower doses are needed to achieve similar AUC estradiol levels (Kuhl, 2005) (Figures 1 and 2). This is an advantage of sublingual estradiol over oral estradiol, as it allows for lower doses to be used and for reduced medication costs.
Because accidental swallowing of some of the estradiol seems probable, the sublingual route is, most likely, actually a combination of sublingual and oral delivery of estradiol (Lobo, 1987; Kuhl, 2005). A preliminary report from an ongoing study of transfeminine people reported that a single 1 mg dose of sublingual estradiol caused an average rise in the level of estradiol up to a maximum of at least 179 pg/mL (657 pmol/L) within one to two hours of administration. In contrast, a peak concentration of just 36 pg/mL (130 pmol/L) was found with the same 1 mg dose administered orally (Doll et al., 2020). Thereafter, estradiol levels decreased rapidly. This response has also been found in other studies of postmenopausal women where a wide range of peak concentrations have been observed (Burnier et al., 1981; Price et al., 1997; Wren et al., 2003). Estradiol levels are found to rapidly rise on the order of ten times that of the peak of oral estradiol, then rapidly decline with an elimination half-life of a few hours (Kuhl, 2005). Sublingual estradiol is somewhat analogous in this respect to intravenously administered estradiol, which also is associated with a rapid increase in estradiol levels and a very short elimination half-life following a dose (Kuhnz, Gansau, & Mahler, 1993). Another route of administration that is similar in this regard is intranasal administration (Devissaguet et al., 1999). Owing to the spikiness and short duration of sublingual estradiol, sublingual estradiol does not achieve as stable of concentrations as other formulations do. As such, this is a marked difference to other formulations of estradiol, such as oral estradiol, that produce much more stable hormone levels that do not fluctuate as much over the course of the day.
A range of estimates have been reported for the relative bioavailability of sublingual estradiol. One small randomised study of postmenopausal women found approximately 2.5-fold higher area-under-the-curve (AUC) levels of estradiol with sublingual estradiol than with the same doses of oral estradiol (Price et al., 1997). Other studies have reported relative bioavailability estimates for sublingual estradiol of up to five times that of oral estradiol (Pines et al., 1999). A study in marmoset monkeys found that the absolute bioavailability of sublingual estradiol was 10%; approximately twice that of conventional absolute bioavailability estimates of oral estradiol (5%, though with a wide range of 0.1 to 12%) (Kuhnz, Blode, & Zimmermann, 1993). Therefore, with respect to AUC levels of estradiol, the sublingual route appears to have between approximately two and five times higher estradiol levels compared to oral estradiol when given at the same doses. Based on these findings, approximate doses of sublingual estradiol for use in transfeminine hormone therapy can be derived (Table 1). It is of note that, at this time, the comparative potency of sublingual estradiol remains to be properly characterised due to a lack of research.
Table 1: Approximately comparable doses of estradiol (E2) and estradiol valerate (EV) administered by the oral and sublingual routes in terms of total estradiol exposure (Price et al., 1997; Pines et al., 1999):
Low Dose
Moderate Dose
High Dose
Very-High Dose
Oral E2
2 mg/day
4 mg/day
8 mg/day
10 mg/day
Sublingual E2a
0.5–1 mg/day
1–2 mg/day
2–4 mg/day
2.5–5 mg/day
Oral EV
3 mg/day
6 mg/day
10 mg/day
12 mg/day
Sublingual EVa
0.75–1.5 mg/day
1.5–3 mg/day
2.5–5 mg/day
3–6 mg/day
a Range calculated by dividing oral doses by two and four to reflect differences in absolute bioavailability and rounding to the nearest 0.25 mg. * Bioidentical estradiol has wide interindividual variation in its pharmacology and the effects of doses may vary significantly between individuals. EV has greater molecular weight and therefore contains less medication for the same amount/dose by weight. It should be noted that estimates for the relative bioavailability of EV are extrapolated from formulations with no valeric ester attached (i.e., E2).
Sublingually Administered Estradiol and Feminisation
The very short half-life of sublingually and buccally administered estradiol relative to other forms raises a few questions for its potential use of sublingual estradiol in feminising hormone therapy. One of the most commonly asked questions on online forums is regarding which gender-affirming hormone therapy regimens might be most “effective” with respect to the feminising effects of estrogens. These include, but are not limited to, outcomes such as breast development and fat distribution.
In contrast to oral and trandermal estradiol, no data exist describing the extent of feminisation with sublingual estradiol (Sam, 2020a). However, as discussed previously, oral and non-oral estradiol have not been found to differ in their effects on breast development or other feminising outcomes in transfeminine people or cisgender hypogondal girls (Rosenfield et al., 2005; Shah et al., 2014; Klaver et al., 2018; de Blok et al., 2021). In consideration of this, differences in efficacy might not be expected for sublingual estradiol either. The fact that several gender clinics have employed sublingual estradiol is also encouraging and suggests that sublingual estradiol is effective for inducing feminization (Deutsch, Bhakri, & Kubicek, 2015; Lim et al., 2019; Cirrincione et al., 2021). Nevertheless, as no studies have been conducted comparing the feminising efficacy of sublingual estradiol with objective measures, it is not possible to say for certain whether or not there is any difference in feminisation outcomes between oral and sublingual estradiol. Hopefully, studies in the future will shed more light on this.
Testosterone Suppressing Efficacy of Sublingually Administered Estradiol
Another question that might be raised by the short half-life of sublingual estradiol is how it might compare to more conventional routes of administration in terms of its ability to suppress testosterone and other androgens.
Estrogens were first characterised for their use as antigonadotrophic antiandrogens in the 1940s, in the form of oral synthetic estrogens, namely diethylstilbestrol (DES), to treat men with prostate cancer (Huggins & Hodges, 1941). Estrogens given in the form of oral ethinylestradiol (EE), long-acting estradiol esters, such as polyestradiol phosphate, and transdermal estradiol patches have been studied. Their efficacy for this indication is well established (Stege et al., 1996; Kohli, 2006; Sciarra et al., 2015). As data are more limited for testosterone suppression with estrogens in transfeminine people, these data are valuable for informing transfeminine hormone therapy. Sublingual estradiol, on the other hand, has never been used as therapy for prostatic cancer and, consequently, no such data exist on the same scale to show the ability of sublingual estradiol in this capacity.
Recent data from some studies have found that physiologic levels of estradiol (i.e., 100–200 pg/mL [367–734 pmol/L]) from non-sublingual estradiol alone result in rapid and near complete, if not complete, suppression of testosterone levels to the female range in many transfeminine people (Leinung, Feustel, & Joseph, 2018; Pappas et al., 2020). Additionally, new data from around 900 men enrolled in the ongoing Prostate Adenocarcinoma TransCutaneous Hormones (PATCH) study, a multicentre randomised controlled trial in the United Kingdom, show that sustained median estradiol levels of between 215 to 250 pg/mL (789–918 pmol/L) from transdermal patches were similarly effective (~95%) to GnRH analogues in reducing testosterone levels to the castrate range (<50 ng/dL [<1.7 nmol/L]) (Langley et al., 2021). However, because of the markedly different pharmacokinetics of sublingual estradiol, it is plausible that estradiol administered in this way might result in sub-par suppression at doses with similar AUC levels of estradiol. Put another way, sustained estradiol levels may be more efficacious with respect to testosterone suppression than the frequent and short-lived “spikes” in estradiol levels that occur with the sublingual route.
There is some weak evidence from pharmacological studies of estradiol that support this possibility. One line of evidence is that some studies of both sublingual and intravenous administration have reported rapid but limited suppression of the gonadotropins (follicle-stimulating hormone and luteinising hormone) in women despite sufficiently elevated estradiol levels for several hours (Tsai & Yen, 1971; Burnier et al., 1981; Casper & Yen, 1981; Hoon et al., 1993). These studies are low quality and indirect since testosterone suppression itself was not measured and they were performed in cisgender women. Another problem is that all were single dose studies and their findings may not translate to multiple dosing. It may be the case that full gonadotropin suppression becomes apparent with repeated physiologic doses of sublingual estradiol. Nevertheless, these studies might suggest a limited effect of sublingual estradiol to fully suppress gonadal function in transfeminine people without the use of excessive doses that would lead to greater health risks or the additional use of other antiandrogens.
It could be the case that monotherapy with sublingual estradiol may not be as effective at comparable doses to the typically employed doses in studies of prostatic cancer (e.g., two to four 100 μg/24 hours transdermal patches). Transdermal patches, gels and parenteral estradiol esters, such as estradiol valerate, injected intramuscularly or subcutaneously might therefore be more reliable choices for monotherapy regimens. On the other hand, sublingual estradiol has been studied in transfeminine people in combination with and without the low-dose use of the progestin medroxyprogesterone acetate (MPA) (Jain, Kwan, & Forcier, 2019). In this study, at least reasonably high rates of testosterone levels within the female range (<50 ng/dL [<1.7 nmol/L]) were achieved by the transfeminine people who took sublingual estradiol together with medroxyprogesterone acetate, showing that sublingual estradiol taken together with other antiandrogens (e.g., 10 mg/day cyproterone acetate) is very likely to be viable for achieving effective testosterone suppression (Aly, 2019).
Monitoring of Estradiol Levels with Sublingual Administration
A further consideration regarding the rapid changes in estradiol levels that occur with the use of sublingual estradiol is the relevance of monitoring of estradiol levels through bloodwork. Currently, consensus guidelines do not recommend a specific time for monitoring of the blood relative to the time of a last dose (Deutsch, 2016; Cheung et al., 2019; T’Sjoen et al., 2020). This may be in part due to practical reasons, or because there is currently no robust data from randomised controlled trials to guide the specifics of dosing in transgender hormone therapy (Haupt et al., 2020). Nevertheless, because estradiol levels vary so significantly with sublingual estradiol, knowledge of how long after the last dose blood was drawn is important to ensure proper interpretation of laboratory results.
For instance, measuring hormone levels just after a dose of sublingual estradiol has been taken might lead to the misinterpretation that levels of estradiol are excessively high and that one’s dosage should be reduced to achieve a more sensible concentration of estradiol in the blood. In reality, this would be a misunderstanding caused by the pharmacology of sublingual estradiol as the point of measurement would be right around the time when estradiol levels are most likely to be at their highest. These estradiol levels would not be indicative of the average amount of exposure, which is the more accurate measure of overall estrogenicity. Similarly, on the opposite end of the scale, drawing blood just before the administration of a new dose might lead to the belief that estrogen levels are too low and, consequently, lead to the use of excessive doses of estrogens. The latter misinterpretation may be more common among people unfamiliar with the pharmacology of sublingual estradiol as levels of estradiol only remain very high in the first few hours after a dose of sublingual estradiol has been taken before falling rapidly.
This oversight may also have implications in studies of sublingual estradiol. For instance, in the previously mentioned respective analysis of the use of sublingual estradiol for gender-affirming hormone therapy, the frequency of administration and time of measurement relative to the last dose were not specified in their results (Jain, Kwan, & Forcier, 2019). Although this data is much needed and is valuable to ongoing research to characterise sublingual estradiol in in transfeminine people, a significant problem is not knowing at what time estradiol levels were measured after the medication was administered. It is difficult to say much about the estradiol levels recorded in this study. Moreover, it is impossible to use this data to help derive equivalent doses of sublingual and oral estradiol.
A possible solution to the problem of rapidly changing hormone levels associated with the sublingual route might simply be to measure when estradiol levels are most likely to be closest to their average. In the case of sublingual estradiol, studies generally find this to be approximately four hours after the administration of a dose, although there is likely to be considerable variation between individuals (Kuhl, 2005). Nevertheless, this approach may give the most representative “snapshot” of overall estrogenic exposure and might help to avoid misleading laboratory data in users of sublingual estradiol.
Administration of Multiple Sublingual Doses Per Day
In order to compensate for the short half-life of sublingually administered estradiol, multiple doses of estrogens can be administered in smaller quantities per day to maintain hormone levels that are somewhat more consistent (Ahokas, Kaukoranta, & Aito, 1999).
In one study of premenopausal women with high-dose estrogen therapy, 2 mg of sublingual estradiol was administered three or four times per day (a total of 6–8 mg/day), resulting in significantly more stable hormone levels than would be expected with a single dose per day (Serhal & Craft, 1989). This was replicated in another study where estradiol was administered three to eight times per day (Ahokas et al., 2001). Conversely, a third study investigating low-dose buccal estradiol found little difference between the “steady-state” estradiol concentrations with a once-daily and twice-daily 0.25 mg dose of buccal estradiol over a 12 hour observation period (Wren et al., 2003). These findings may indicate that sublingual and buccal estradiol needs to be taken at least thrice per day in order to achieve concentrations of estradiol that are more stable.
For the reasons outlined in the subsections above, it would seem advantageous that transfeminine people using sublingual estradiol employ this approach and take sublingual estradiol in divided doses throughout the day; perhaps ideally at least three or four times per day. For instance, instead of taking a 2 mg dose every 24 hours, it would be better to take four 0.5 mg doses in the space of 24 hours (as evenly spaced as practical). Administering sublingual estradiol multiple times throughout the day might be less convenient, but is likely to provide at least somewhat more balanced estradiol levels and potentially better testosterone suppression. The administration of multiple doses every day could be regarded as optimal for the use of sublingually administered estradiol.
Safety and Tolerability
Unfortunately, as with the pharmacokinetics of sublingually and buccally estradiol, the published medical literature concerning the safety and tolerability of this route of administration leaves much to be desired. No long term safety data exist for sublingually administered estradiol in the same way that both oral and transdermal estradiol have been rigorously studied in menopausal women (Rovinski et al., 2018; CGHFBC, 2019).
Adverse Health Effects of Estrogens
With sufficient exposure, owing to their effects in the liver, estrogens are associated with an increased risk of blood clots (Kuhl, 2005; Aly, 2020b). Additionally, under certain circumstances, estrogens can be associated with other cardiovascular complications (Anderson et al., 2004; Mikkola et al., 2005). Although the absolute risk is low in the short-term, these are the most significant health concerns associated with gender-affirming hormone therapy.
A limited number of studies have assessed the effects of sublingually administered estradiol on the liver (Pines et al., 1999; Lim et al., 2019). These data found similar effects on lipids and cholesterol to other estrogens. One line of evidence that indicates sublingual estradiol has greater hepatic impact than other non-oral forms such as trandermal estradiol is the significantly greater quantities of estrone and estrone sulphate that are generated by this route; a marker of estrogenic exposure in the liver (Burnier et al., 1981; Cirrincione et al., 2021). Intense estrogenic activation in the liver is the mechanism by which non-oral estradiol induces a hypercoagulable state at high doses (Sam, 2020b; Sam, 2020c).
While a large body of research does exist concerning the short and long term health effects of estrogens, none of these studies have investigated sublingual or buccal estradiol (Oliver-Williams et al., 2019; Mishra et al., 2021). Given that oral estradiol has greater risks than non-oral estradiol, and that sublingual administration partially but not fully avoids first-pass metabolism, it may be the case that its own risk would be no higher than the risk observed with oral estradiol but no lower than the risk observed with non-oral routes. A retrospective cohort study in the United States found that the incidence of thromboembolism in transfeminine people with an average dose of 4 mg/day oral estradiol was approximately twice that of cisgender controls not taking hormone therapy after adjusting for confounders (HR 2.0, 95% CI 1.4–2.8 versus reference women) (Getahun et al., 2018). These increases in risks are much lower compared to regimens in transfeminine people in the past that included high doses of synthetic estrogens, but it’s important to remember that even such increases can significantly increase morbidity and mortality (Morimont, Dogné, & Douxfils, 2020). It would be advisable to limit doses of sublingual and buccal estradiol so that they are not excessive (i.e., <6 mg/day) in the interest of harm reduction and the balancing of the risks and benefits of gender-affirming hormone therapy.
Non-compliance
A practical obstacle to the use of sublingual estradiol in transfeminine people is that it may be highly inconvenient to have to administer doses thrice, four times or perhaps even more often throughout the duration of a single day. It has been found in observational studies that, in general, the number of prescribed medications and doses per day are positively associated with patient non-compliance and the number of missed doses (Jin et al., 2008; Toh et al., 2014). These findings are especially of relevance to transfeminine people as, in most cases, we require decades of hormone therapy. While missing one dose from time to time may be of little consequence, missing doses repeatedly could be more problematic.
In contrast to sublingual estradiol, the half-life of oral estradiol and transdermal gel is long enough to enable once-daily administration (Wiegratz et al., 2001; Potts & Lobo, 2005). In the case of transdermal patches and parenteral estradiol, these forms only have to be replenished every few days or after even longer intervals of time (Thurman et al., 2013; Wisner et al., 2015). Therefore, when considering the use of sublingual estradiol versus other forms, whether or not it would be practical or convenient to consistently take medication several times a day should probably also be an important consideration for transfeminine people. If not, then another formulation may be preferable for the person in question. This may be especially true for long term use.
Summary and Conclusions
There is much less research investigating sublingual and buccal estradiol than other forms of estrogen. These forms, namely oral and transdermal estrogens, are used in the alleviation of the menopause and for other indications that have historically been more widely used. As a result, they have received much more attention and characterisation than sublingual estradiol has for transfeminine hormone therapy. However, several recent studies have added to our knowledge of sublingual estradiol. Clinical practice guidelines for transgender care that have historically not discussed the use of sublingual estradiol may be adjusted accordingly if more information becomes available.
Sublingual estradiol is different in its pharmacology to other formulations. The main difference is that it is associated with a rapid rise and fall in estradiol levels. It has between two and four times the bioavailability of oral estradiol and hence provides the same total estradiol exposure at doses that are two to four times lower. This is a particular advantage because sublingual estradiol, therefore, is cheaper than oral estradiol, and the higher estradiol levels at the same dose may be helpful for testosterone suppression.
While no evidence exists to show or suggest that sublingual estradiol results in better or inferior feminisation to that experienced with other routes of administration, it is plausible that sublingual estradiol may to some degree result in less testosterone suppression at the same total estradiol exposure. Sublingual estradiol has, nonetheless, been shown to be effective with respect to testosterone suppression when paired with other antiandrogens. Care should be taken with sublingual estradiol when monitoring estradiol levels to ensure correct interpretation. In order to help minimise these potential problems, sublingual estradiol can be taken in multiple doses divided throughout the day.
The health risks of sublingual estradiol have not been quantified in large observational or randomised studies. Therefore, although the partial bypassing of the first pass through the liver is reassuring in this respect, its cardiovascular risk profile is unknown. Sublingual estradiol may be inconvenient and other formulations can be used instead if preferred, particularly for more long-term therapy.
Taken together, although much more research is clearly needed to properly characterise the route, sublingual estradiol may have a number of advantageous properties and may be a useful alternative to oral estradiol in transfeminine hormone therapy.
Updates
Update 1: New Sublingual Estradiol Studies (Added By Aly)
Since this article was first published, the following new relevant studies and papers on sublingual estradiol in transfeminine people have been published:
Doll, E., Gunsolus, I., Thorgerson, A., Tangpricha, V., Lamberton, N., & Sarvaideo, J. L. (2022). Pharmacokinetics of Sublingual Versus Oral Estradiol in Transgender Women. Endocrine Practice, 28(3), 237–242. [DOI:10.1016/j.eprac.2021.11.081]
Safer, J. D. (2022). Are the Pharmacokinetics of Sublingual Estradiol Superior or Inferior to Those of Oral Estradiol? Endocrine Practice, 28(3), 351–352. [DOI:10.1016/j.eprac.2021.12.018]
Sarvaideo, J., Doll, E., & Tangpricha, V. (2022). More Studies Are Needed to Establish the Safety and Efficacy of Sublingual Estradiol in Transgender Women. Endocrine Practice, 28(3), 353–354. [DOI:10.1016/j.eprac.2022.01.004]
Cortez, S., Moog, D., Lewis, C., Williams, K., Herrick, C., Fields, M., Gray, T., Guo, Z., Nicol, G., & Baranski, T. (2023). Effectiveness and Safety of Different Estradiol Regimens in Transgender Women (TREAT Study): Protocol for a Randomized Controlled Trial. JMIR Research Protocols, 12, e53092. [DOI:10.2196/53092]
Jalal, E., & Baldwin, C. (2023). Supratherapeutic Estrogen Levels in Transgender Women Likely From Sublingual Estradiol. Journal of the Endocrine Society, 7(Suppl 1) [ENDO 2023 Abstracts Annual Meeting of the Endocrine Society], A1095–A1096 (abstract no. SAT391/bvad114.2062). [DOI:10.1210/jendso/bvad114.2062] [PDF]
Yaish, I., Gindis, G., Greenman, Y., Moshe, Y., Arbiv, M., Buch, A., Sofer, Y., Shefer, G., & Tordjman, K. (2023). Sublingual Estradiol Offers No Apparent Advantage Over Combined Oral Estradiol and Cyproterone Acetate for Gender-Affirming Hormone Therapy of Treatment-Naive Trans Women: Results of a Prospective Pilot Study. Transgender Health, 8(6), 485–493. [DOI:10.1089/trgh.2023.0022]
Gindis, G., Yaish, I., Greenman, Y., Moshe, Y., Arbiv, M., Buch, A., Sofer, Y., Shefer, G., & Tordjman, K. (May 2023). Sublingual estradiol only, offers no apparent advantage over combined oral estradiol and cyproterone acetate, for Gender Affirming Hormone Therapy (GAHT) of treatment-naive transwomen: Results of a prospective pilot study. Endocrine Abstracts, 90 [25th European Congress of Endocrinology 2023, 13–16 May 2023, Istanbul, Turkey], 274–274 (abstract no. P182). [DOI:10.1530/endoabs.90.p182] [PDF]
Yaish, I., Gindis, G., Greenman, Y., Shefer, G., Buch, A., Arbiv, M., Moshe, Y., Sofer, Y., & Tordjman, K. M. (October 2023). Sublingual Estradiol Only, Compared To Combined Oral Estradiol And Cyproterone Acetate,Offers No Apparent Advantage For Gender Affirming Hormone Therapy (GHAT), In Treatment Naïve Transwomen: Results Of A Prospective Pilot Study. Journal of the Endocrine Society, 7(Suppl 1) [ENDO 2023 Abstracts Annual Meeting of the Endocrine Society], A1104–A1105 (abstract no. SAT409/bvad114.2080). [DOI:10.1210/jendso/bvad114.2080] [PDF]
Kariyawasam, N. M., Ahmad, T., Sarma, S., & Fung, R. (2024). Comparison of Estrone/Estradiol Ratio and Levels in Transfeminine Individuals on Different Routes of Estradiol. Transgender Health, online ahead of print. [DOI:10.1089/trgh.2023.0138]
References
Ahokas, A., Kaukoranta, J., & Aito, M. (1999). Effect of oestradiol on postpartum depression. Psychopharmacology, 146(1), 108–110. [DOI:10.1007/s002130051095]
Ahokas, A., Kaukoranta, J., Wahlbeck, K., & Aito, M. (2001). Estrogen deficiency in severe postpartum depression: successful treatment with sublingual physiologic 17β-estradiol: a preliminary study. Journal of Clinical Psychiatry, 62(5), 332–336. [DOI:10.4088/jcp.v62n0504]
Anderson, G. L., Limacher, M., Assaf, A. R., Bassford, T., Beresford, S. A., Black, H., Bonds, D., Brunner, R., Brzyski, R., Caan, B., Chlebowski, R., Curb, D., Gass, M., Hays, J., Heiss, G., Hendrix, S., Howard, B. V., Hsia, J., Hubbell, A., Jackson, R., … & Women’s Health Initiative Steering Committee. (2004). Effects of Conjugated Equine Estrogen in Postmenopausal Women With Hysterectomy: The Women’s Health Initiative Randomized Controlled Trial. JAMA, 291(14), 1701–1712. [DOI:10.1001/jama.291.14.1701]
Bartlett, J. A., & van der Voort Maarschalk, K. (2012). Understanding the oral mucosal absorption and resulting clinical pharmacokinetics of asenapine. AAPS Pharmscitech, 13(4), 1110–1115. [DOI:10.1208/s12249-012-9839-7]
Burnier, A. M., Martin, P. L., Yen, S. S., & Brooks, P. (1981). Sublingual absorption of micronized 17β-estradiol. American Journal of Obstetrics and Gynecology, 140(2), 146–150. [DOI:10.1016/0002-9378(81)90101-0]
Casper, R. F., & Yen, S. S. (1981). Rapid absorption of micronized estradiol-17β following sublingual administration. Obstetrics and Gynecology, 57(1), 62–64. [Google Scholar] [PubMed] [URL] [PDF]
Chandrasekhara, D. S., Ali, V., Prost, H. M., & Nader-Estekhari, S. (2002). Buccal estrogen in toothpaste study: systemic absorption of estradiol in postmenopausal or surgically menopausal women when administered as a component in toothpaste. Fertility and Sterility, 78(Suppl 1), S98–S98 (O-258). [DOI:10.1016/S0015-0282(02)03639-7]
Cheung, A. S., Wynne, K., Erasmus, J., Murray, S., & Zajac, J. D. (2019). Position statement on the hormonal management of adult transgender and gender diverse individuals. Medical Journal of Australia, 211(3), 127–133. [DOI:10.5694/mja2.50259]
Cirrincione, L. R., Winston McPherson, G., Rongitsch, J., Sadilkova, K., Drees, J. C., Krasowski, M. D., Dickerson, J. A., & Greene, D. N. (2021). Sublingual Estradiol Is Associated with Higher Estrone Concentrations than Transdermal or Injectable Preparations in Transgender Women and Gender Nonbinary Adults. LGBT Health, 8(2), 125–132. [DOI:10.1089/lgbt.2020.0249]
Collaborative Group on Hormonal Factors in Breast Cancer. (2019). Type and timing of menopausal hormone therapy and breast cancer risk: individual participant meta-analysis of the worldwide epidemiological evidence. The Lancet, 394(10204), 1159–1168. [DOI:10.1016/S0140-6736(19)31709-X]
Cortez, S., Moog, D., Lewis, C., Williams, K., Herrick, C., Fields, M., Gray, T., Guo, Z., Nicol, G., & Baranski, T. (2023). Effectiveness and Safety of Different Estradiol Regimens in Transgender Women (TREAT Study): Protocol for a Randomized Controlled Trial. JMIR Research Protocols, 12, e53092. [DOI:10.2196/53092]
de Blok, C., Dijkman, B., Wiepjes, C. M., Staphorsius, A. S., Timmermans, F. W., Smit, J. M., Dreijerink, K., & den Heijer, M. (2021). Sustained Breast Development and Breast Anthropometric Changes in 3 Years of Gender-Affirming Hormone Treatment. The Journal of Clinical Endocrinology & Metabolism, 106(2), e782–e790. [DOI:10.1210/clinem/dgaa841]
Deutsch, M. B., Bhakri, V., & Kubicek, K. (2015). Effects of cross-sex hormone treatment on transgender women and men. Obstetrics and Gynecology, 125(3), 605–610. [DOI:10.1097/AOG.0000000000000692]
Deutsch, M. B. (Ed.). (2016). Guidelines for the Primary and Gender-Affirming Care of Transgender and Gender Nonbinary People, 2nd Edition. San Francisco: University of California, San Francisco/UCSF Transgender Care. [URL] [PDF]
Devissaguet, J. P., Brion, N., Lhote, O., & Deloffre, P. (1999). Pulsed estrogen therapy: pharmacokinetics of intranasal 17-beta-estradiol (S21400) in postmenopausal women and comparison with oral and transdermal formulations. European Journal of Drug Metabolism and Pharmacokinetics, 24(3), 265–271. [DOI:10.1007/BF03190030]
Doll, E. E., Gunsolus, I., Lamberton, N., Tangpricha, V., & Sarvaideo, J. L. (2020). Pharmacokinetics of Sublingual Versus Oral Estradiol in Transgender Women. Journal of the Endocrine Society, 4(Suppl 1), A1128–A1128 (SUN-LB9). [DOI:10.1210/jendso/bvaa046.2237]
Doll, E., Gunsolus, I., Thorgerson, A., Tangpricha, V., Lamberton, N., & Sarvaideo, J. L. (2022). Pharmacokinetics of Sublingual Versus Oral Estradiol in Transgender Women. Endocrine Practice, 28(3), 237–242. [DOI:10.1016/j.eprac.2021.11.081]
Fiet, J., Hermano, M., Witte, J., Villette, J. M., Haimart, M., Gourmel, B., Tabuteau, F., Rouffy, J., & Dreux, C. (1982). Post-menopausal concentrations of plasma oestradiol, oestrone, FSH and LH and of total urinary oestradiol and oestrone after a single sublingual dose of oestradiol-17β. Acta Endocrinologica, 101(1), 93–97. [DOI:10.1530/acta.0.1010093]
Gass, M. S., Rebar, R. W., Cuffie-Jackson, C., Cedars, M. I., Lobo, R. A., Shoupe, D., Judd, H. L., Buyalos, R. P., & Clisham, P. R. (2004). A short study in the treatment of hot flashes with buccal administration of 17-β estradiol. Maturitas, 49(2), 140–147. [DOI:10.1016/j.maturitas.2003.12.004]
Getahun, D., Nash, R., Flanders, W. D., Baird, T. C., Becerra-Culqui, T. A., Cromwell, L., Hunkeler, E., Lash, T. L., Millman, A., Quinn, V. P., Robinson, B., Roblin, D., Silverberg, M. J., Safer, J., Slovis, J., Tangpricha, V., & Goodman, M. (2018). Cross-sex hormones and acute cardiovascular events in transgender persons: a cohort study. Annals of Internal Medicine, 169(4), 205–213. [DOI:10.7326/M17-2785]
Gindis, G., Yaish, I., Greenman, Y., Moshe, Y., Arbiv, M., Buch, A., Sofer, Y., Shefer, G., & Tordjman, K. (May 2023). Sublingual estradiol only, offers no apparent advantage over combined oral estradiol and cyproterone acetate, for Gender Affirming Hormone Therapy (GAHT) of treatment-naive transwomen: Results of a prospective pilot study. Endocrine Abstracts, 90 [25th European Congress of Endocrinology 2023, 13–16 May 2023, Istanbul, Turkey], 274–274 (abstract no. P182). [DOI:10.1530/endoabs.90.p182] [PDF]
Haupt, C., Henke, M., Kutschmar, A., Hauser, B., Baldinger, S., Saenz, S. R., & Schreiber, G. (2020). Antiandrogen or estradiol treatment or both during hormone therapy in transitioning transgender women. Cochrane Database of Systematic Reviews, 11(11), CD013138. [DOI:10.1002/14651858.CD013138.pub2]
Hoon, T. J., Dawood, M. Y., Khan‐Dawood, F. S., Ramos, J., & Batenhorst, R. L. (1993). Bioequivalence of a 17β‐Estradiol Hydroxypropyl‐β‐Cyclodextrin Complex in Postmenopausal Women. The Journal of Clinical Pharmacology, 33(11), 1116–1121. [DOI:10.1002/j.1552-4604.1993.tb01949.x]
Huggins, C., & Hodges, C. V. (1941). Studies on prostatic cancer. I. The effect of castration, of estrogen and of androgen injection on serum phosphatases in metastatic carcinoma of the prostate. Cancer Research, 1(4), 293–297. [DOI:10.3322/canjclin.22.4.232]
Jain, J., Kwan, D., & Forcier, M. (2019). Medroxyprogesterone acetate in Gender-Affirming therapy for Transwomen: results from a retrospective study. The Journal of Clinical Endocrinology & Metabolism, 104(11), 5148–5156. [DOI:10.1210/jc.2018-02253]
Jalal, E., & Baldwin, C. (2023). Supratherapeutic Estrogen Levels in Transgender Women Likely From Sublingual Estradiol. Journal of the Endocrine Society, 7(Suppl 1) [ENDO 2023 Abstracts Annual Meeting of the Endocrine Society], A1095–A1096 (abstract no. SAT391/bvad114.2062). [DOI:10.1210/jendso/bvad114.2062] [PDF]
Jin, J., Sklar, G. E., Oh, V. M. S., & Li, S. C. (2008). Factors affecting therapeutic compliance: A review from the patient’s perspective. Therapeutics and Clinical Risk Management, 4(1), 269–286. [DOI:10.2147/TCRM.S1458]
Kariyawasam, N. M., Ahmad, T., Sarma, S., & Fung, R. (2024). Comparison of Estrone/Estradiol Ratio and Levels in Transfeminine Individuals on Different Routes of Estradiol. Transgender Health, online ahead of print. [DOI:10.1089/trgh.2023.0138]
Klaver, M., de Blok, C. J. M., Wiepjes, C. M., Nota, N. M., Dekker, M. J., de Mutsert, R., Schreiner, T., Fisher, A. D., T’Sjoen, G., & den Heijer, M. (2018). Changes in regional body fat, lean body mass and body shape in trans persons using cross-sex hormonal therapy: results from a multicenter prospective study. European Journal of Endocrinology, 178(2), 163–171. [DOI:10.1530/EJE-17-0496]
Kohli, M. (2006). Phase II study of transdermal estradiol in androgen‐independent prostate carcinoma. Cancer, 106(1), 234–235. [DOI:10.1002/cncr.21528]
Kuhl, H. (2005). Pharmacology of estrogens and progestogens: influence of different routes of administration. Climacteric, 8(Suppl 1), 3–63. [DOI:10.1080/13697130500148875] [PDF]
Kuhnz, W., Blode, H., & Zimmermann, H. (1993). Pharmacokinetics of exogenous natural and synthetic estrogens and antiestrogens. In Oettel, M., & Schillinger, E. (Eds.). Estrogens and Antiestrogens II: Pharmacology and Clinical Application of Estrogens and Antiestrogen (Handbook of Experimental Pharmacology, Volume 135, Part 2) (pp. 261–322). Berlin/Heidelberg: Springer. [DOI:10.1007/978-3-642-60107-1_15]
Kuhnz, W., Gansau, C., & Mahler, M. (1993). Pharmacokinetics of estradiol, free and total estrone, in young women following single intravenous and oral administration of 17β-estradiol. Arzneimittelforschung, 43(9), 966–973. [Google Scholar] [PubMed] [PDF]
Langley, R. E., Gilbert, D. C., Duong, T., Clarke, N. W., Nankivell, M., Rosen, S. D., Mangar, S., Macnair, A., Sundaram, S. K., Laniado, M. E., Dixit, S., Madaan, S., Manetta, C., Pope, A., Scrase, C. D., Mckay, S., Muazzam, I. A., Collins, G. N., Worlding, J., Williams, S. T., … & Parmar, M. (2021). Transdermal oestradiol for androgen suppression in prostate cancer: long-term cardiovascular outcomes from the randomised Prostate Adenocarcinoma Transcutaneous Hormone (PATCH) trial programme. The Lancet, 397(10274), 581–591. [DOI:10.1016/S0140-6736(21)00100-8]
Leinung, M. C., Feustel, P. J., & Joseph, J. (2018). Hormonal treatment of transgender women with oral estradiol. Transgender Health, 3(1), 74–81. [DOI:10.1089/trgh.2017.0035]
Lim, H. H., Jang, Y. H., Choi, G. Y., Lee, J. J., & Lee, E. S. (2019). Gender affirmative care of transgender people: a single center’s experience in Korea. Obstetrics & Gynecology Science, 62(1), 46–55. [DOI:10.5468/ogs.2019.62.1.46]
Lobo, R. A. (1987). Absorption and metabolic effects of different types of estrogens and progestogens. Obstetrics and Gynecology Clinics of North America, 14(1), 143–167. [PubMed] [DOI:10.1016/S0889-8545(21)00577-5] [URL]
Mikkola, A., Aro, J., Rannikko, S., Oksanen, H., Ruutu, M., & Finnprostate Group. (2005). Cardiovascular complications in patients with advanced prostatic cancer treated by means of orchiectomy or polyestradiol phosphate. Scandinavian Journal of Urology and Nephrology, 39(4), 294–300. [DOI:10.1080/00365590510031228]
Mishra, S. R., Chung, H. F., Waller, M., & Mishra, G. D. (2021). Duration of estrogen exposure during reproductive years, age at menarche and age at Menopause, and risk of cardiovascular disease events, all‐cause and cardiovascular mortality: a systematic review and meta‐analysis. BJOG: An International Journal of Obstetrics & Gynaecology, 128(5), 809–821. [DOI:10.1111/1471-0528.16524]
Morimont, L., Dogné, J. M., & Douxfils, J. (2020). Letter to the Editors-in-Chief in response to the article of Abou-Ismail, et al. entitled “Estrogen and thrombosis: A bench to bedside review” (Thrombosis Research 192 (2020) 40–51). Thrombosis Research, 193, 221–223. [DOI:10.1016/j.thromres.2020.08.006]
Oliver-Williams, C., Glisic, M., Shahzad, S., Brown, E., Pellegrino Baena, C., Chadni, M., Chowdhury, R., Franco, O. H., & Muka, T. (2019). The route of administration, timing, duration and dose of postmenopausal hormone therapy and cardiovascular outcomes in women: a systematic review. Human Reproduction Update, 25(2), 257–271. [DOI:10.1093/humupd/dmy039]
Pappas, I. I., Craig, W. Y., Spratt, L. V., & Spratt, D. I. (2021). Efficacy of Sex Steroid Therapy Without Progestin or GnRH Agonist for Gonadal Suppression in Adult Transgender Patients. The Journal of Clinical Endocrinology & Metabolism, 106(3), e1290–e1300. [DOI:10.1210/clinem/dgaa884]
Perloff, W. H. (1950). Estradiol buccal tablets in the treatment of the menopause. American Journal of Obstetrics and Gynecology, 59(1), 223–225. [DOI:10.1016/0002-9378(50)90390-5]
Pickar, J. H., Bon, C., Amadio, J. M., Mirkin, S., & Bernick, B. (2015). Pharmacokinetics of the first combination 17β-estradiol/progesterone capsule in clinical development for menopausal hormone therapy. Menopause, 22(12), 1308–1316. [DOI:10.1097/GME.0000000000000467]
Pines, A., Averbuch, M., Fisman, E. Z., & Rosano, G. M. (1999). The acute effects of sublingual 17β-estradiol on the cardiovascular system. Maturitas, 33(1), 81–85. [DOI:10.1016/S0378-5122(99)00036-5]
Potts, R. O., & Lobo, R. A. (2005). Transdermal drug delivery: clinical considerations for the obstetrician–gynecologist. Obstetrics & Gynecology, 105(5), 953–961. [DOI:10.1097/01.AOG.0000161958.70059.db]
Price, T. M., Blauer, K. L., Hansen, M., Stanczyk, F., Lobo, R., & Bates, G. W. (1997). Single-dose pharmacokinetics of sublingual versus oral administration of micronized 17β-estradiol. Obstetrics & Gynecology, 89(3), 340–345. [DOI:10.1016/S0029-7844(96)00513-3]
Rosenfield, R. L., Devine, N., Hunold, J. J., Mauras, N., Moshang Jr, T., & Root, A. W. (2005). Salutary effects of combining early very low-dose systemic estradiol with growth hormone therapy in girls with Turner syndrome. The Journal of Clinical Endocrinology & Metabolism, 90(12), 6424–6430. [DOI:10.1210/jc.2005-1081]
Rovinski, D., Ramos, R. B., Fighera, T. M., Casanova, G. K., & Spritzer, P. M. (2018). Risk of venous thromboembolism events in postmenopausal women using oral versus non-oral hormone therapy: a systematic review and meta-analysis. Thrombosis Research, 168, 83–95. [DOI:10.1016/j.thromres.2018.06.014]
Safer, J. D. (2022). Are the Pharmacokinetics of Sublingual Estradiol Superior or Inferior to Those of Oral Estradiol? Endocrine Practice, 28(3), 351–352. [DOI:10.1016/j.eprac.2021.12.018]
Sarvaideo, J., Doll, E., & Tangpricha, V. (2022). More Studies Are Needed to Establish the Safety and Efficacy of Sublingual Estradiol in Transgender Women. Endocrine Practice, 28(3), 353–354. [DOI:10.1016/j.eprac.2022.01.004]
Sciarra, A., Gentile, V., Cattarino, S., Gentilucci, A., Alfarone, A., D’Eramo, G., & Salciccia, S. (2015). Oral ethinylestradiol in castration‐resistant prostate cancer: a 10‐year experience. International Journal of Urology, 22(1), 98–103. [DOI:10.1111/iju.12613]
Serhal, P., & Craft, I. (1989). Oocyte donation in 61 patients. The Lancet, 333(8648), 1185–1187. [DOI:10.1016/S0140-6736(89)92762-1]
Shah, S., Forghani, N., Durham, E., & Neely, E. K. (2014). A randomized trial of transdermal and oral estrogen therapy in adolescent girls with hypogonadism. International Journal of Pediatric Endocrinology, 2014(1), 12. [DOI:10.1186/1687-9856-2014-12]
Stanczyk, F. Z., Archer, D. F., & Bhavnani, B. R. (2013). Ethinyl estradiol and 17β-estradiol in combined oral contraceptives: pharmacokinetics, pharmacodynamics and risk assessment. Contraception, 87(6), 706–727. [DOI:10.1016/j.contraception.2012.12.011]
Stege, R., Gunnarsson, P. O., Johansson, C. J., Olsson, P., Pousette, Å., & Carlström, K. (1996). Pharmacokinetics and testosterone suppression of a single dose of polyestradiol phosphate (Estradurin®) in prostatic cancer patients. The Prostate, 28(5), 307–310. [DOI:10.1002/(SICI)1097-0045(199605)28:5<307::AID-PROS6>3.0.CO;2-8]
T’Sjoen, G., Arcelus, J., De Vries, A. L., Fisher, A. D., Nieder, T. O., Özer, M., & Motmans, J. (2020). European Society for Sexual Medicine position statement “assessment and hormonal management in adolescent and adult trans people, with attention for sexual function and satisfaction”. The Journal of Sexual Medicine, 17(4), 570–584. [DOI:10.1016/j.jsxm.2020.01.012]
Thurman, A., Kimble, T., Hall, P., Schwartz, J. L., & Archer, D. F. (2013). Medroxyprogesterone acetate and estradiol cypionate injectable suspension (Cyclofem) monthly contraceptive injection: steady-state pharmacokinetics. Contraception, 87(6), 738–743. [DOI:10.1016/j.contraception.2012.11.010]
Toh, M. R., Teo, V., Kwan, Y. H., Raaj, S., Tan, S. Y. D., & Tan, J. Z. Y. (2014). Association between number of doses per day, number of medications and patient’s non-compliance, and frequency of readmissions in a multi-ethnic Asian population. Preventive Medicine Reports, 1, 43–47. [DOI:10.1016/j.pmedr.2014.10.001]
Tsai, C. C., & Yen, S. S. C. (1971). Acute effects of intravenous infusion of 17β-estradiol on gonadotropin release in pre-and post-menopausal women. The Journal of Clinical Endocrinology & Metabolism, 32(6), 766–771. [DOI:10.1210/jcem-32-6-766]
Verdonk, S. J., Vesper, H. W., Martens, F., Sluss, P. M., Hillebrand, J. J., & Heijboer, A. C. (2019). Estradiol reference intervals in women during the menstrual cycle, postmenopausal women and men using an LC-MS/MS method. Clinica Chimica Acta, 495, 198–204. [DOI:10.1016/j.cca.2019.04.062]
Wiegratz, I., Fink, T., Rohr, U. D., Lang, E., Leukel, P., & Kuhl, H. (2001). Überkreuz-Vergleich der Pharmakokinetik von Estradiol unter der Hormonsubstitution mit Estradiolvalerat oder mikronisiertem Estradiol. [Cross-over comparison of the pharmacokinetics of estradiol during hormone replacement therapy with estradiol valerate or micronized estradiol.] Zentralblatt für Gynäkologie, 123(9), 505–512. [PubMed] [DOI:10.1055/s-2001-18223]
Wisner, K. L., Sit, D. K., Moses-Kolko, E. L., Driscoll, K. E., Prairie, B. A., Stika, C. S., Eng, H. F., Dills, J. L., Luther, J. F., & Wisniewski, S. R. (2015). Transdermal estradiol treatment for postpartum depression: a pilot randomized trial. Journal of Clinical Psychopharmacology, 35(4), 389–395. [DOI:10.1097/JCP.0000000000000351]
Wren, B. G., Day, R. O., McLachlan, A. J., & Williams, K. M. (2003). Pharmacokinetics of estradiol, progesterone, testosterone and dehydroepiandrosterone after transbuccal administration to postmenopausal women. Climacteric, 6(2), 104–111. [DOI:10.1080/cmt.6.2.104.111]
Yaish, I., Gindis, G., Greenman, Y., Moshe, Y., Arbiv, M., Buch, A., Sofer, Y., Shefer, G., & Tordjman, K. (2023). Sublingual Estradiol Offers No Apparent Advantage Over Combined Oral Estradiol and Cyproterone Acetate for Gender-Affirming Hormone Therapy of Treatment-Naive Trans Women: Results of a Prospective Pilot Study. Transgender Health, 8(6), 485–493. [DOI:10.1089/trgh.2023.0022]
Yaish, I., Gindis, G., Greenman, Y., Shefer, G., Buch, A., Arbiv, M., Moshe, Y., Sofer, Y., & Tordjman, K. M. (2023). Sublingual Estradiol Only, Compared To Combined Oral Estradiol And Cyproterone Acetate,Offers No Apparent Advantage For Gender Affirming Hormone Therapy (GHAT), In Treatment Naïve Transwomen: Results Of A Prospective Pilot Study. Journal of the Endocrine Society, 7(Suppl 1) [ENDO 2023 Abstracts Annual Meeting of the Endocrine Society], A1104–A1105 (abstract no. SAT409/bvad114.2080). [DOI:10.1210/jendso/bvad114.2080] [PDF]
\ No newline at end of file
diff --git a/transfemscience.org/articles/sublingual-ev/index.html b/transfemscience.org/articles/sublingual-ev/index.html
index 8de44344..7e22a7d2 100644
--- a/transfemscience.org/articles/sublingual-ev/index.html
+++ b/transfemscience.org/articles/sublingual-ev/index.html
@@ -1 +1 @@
-Sublingual Administration of Oral Estradiol Valerate Tablets for Transfeminine People - Transfeminine Science
Sublingual Administration of Oral Estradiol Valerate Tablets for Transfeminine People
By Aly | First published January 5, 2019 | Last modified November 28, 2022
Abstract / TL;DR
Oral estradiol tablets can be taken sublingually instead of orally and this allows for greater bioavailability and higher estradiol levels than with oral use. For this reason, sublingual estradiol is frequently used in transfeminine people. Oral estradiol valerate tablets also exist in some parts of the world and it’s often inquired by transfeminine people whether this form of estradiol is likewise effective sublingually. Research in this area is limited and no direct comparisons exist, but at least one study in cisgender women has shown that oral estradiol valerate tablets taken sublingually can result in high estradiol levels and gonadal suppression analogously to sublingual estradiol. In addition, at least one gender-affirming hormone therapy clinic has reported use of sublingual estradiol valerate in transfeminine people. Hence, sublingual estradiol valerate appears to be an effective means of estradiol delivery similarly to sublingual estradiol. One difference between these forms of estradiol is that estradiol valerate contains less estradiol than estradiol by weight and hence should be taken at slightly higher doses. While they can be effective, oral estradiol tablets and oral estradiol valerate tablets were not intended or designed for sublingual use, and formulations of these tablets vary. The implications of this in terms of clinical properties, if any, are unknown. However, it does seem apparent that different tablet formulations may require substantially different amounts of time to dissolve when used sublingually. As a result, some formulations of oral estradiol and oral estradiol valerate may be better-suited for sublingual use than others. Additional characteristics of these formulations like micronization and lipophilicity could also differentially influence their pharmacokinetics in ways that have not been studied. It may be advisable to choose sublingual estradiol over sublingual estradiol valerate where possible simply because sublingual estradiol is much better-characterized in comparison and there are fewer unknowns with it. However, sublingual estradiol valerate can be a clearly effective form of estradiol for transfeminine people as well if needed.
Introduction
Oral estradiol tablets (e.g., Estrace and Estrofem among other brand names) are indicated for oral administration (i.e., taken by mouth/swallowed) and this is how they are normally taken. As an alternative to the standard oral route however, these tablets can be taken sublingually (held under the tongue) or buccally (held in the cheek or lips/gums). Sublingual or buccal administration of oral estradiol tablets allows for much greater bioavailability and estradiol levels in comparison to oral administration (Sam, 2021; Wiki; Graphs; Wiki). Transfeminine people often use sublingual estradiol as the estrogen component of hormone therapy. In various countries, for instance many European countries, estradiol is also provided in oral form as estradiol valerate (EV) tablets (e.g., Progynova among other brand names). It is frequently inquired by transfeminine people whether estradiol valerate tablets can be taken sublingually similarly to estradiol tablets and whether there are any differences between these two estradiol forms for this route. This article is intended to explore and shed some light on these questions.
Effectiveness of Sublingual Estradiol Valerate
Estradiol valerate is an estradiol ester and a prodrug of estradiol. Estradiol esters themselves are pharmacologically inactive prior to conversion into estradiol. Estradiol valerate and other related estradiol esters are cleaved into estradiol by various esteraseenzymes. These esterases are widely expressed throughout the body, and the metabolism of estradiol esters into estradiol occurs not only in the liver but has also been shown to take place rapidly in blood and other tissues (Wiki). Hence, estradiol esters like estradiol valerate do not require the first pass through the liver that occurs with oral administration to become pharmacologically active as estrogens. As such, transformation of estradiol valerate into estradiol should not be an impediment in terms of non-oral administration of estradiol valerate, for instance via sublingual administration (as well as in the form of depot injectables of course).
Studies of estradiol tablets administered sublingually instead of orally are limited, and studies on estradiol valerate tablets used sublingually are extremely scarce. No direct comparisons have been made between sublingual use of estradiol tablets versus sublingual use of estradiol valerate tablets. Hence, we currently don’t have reliable data on how sublingual estradiol valerate compares to sublingual estradiol in terms of pharmacokinetics (e.g., bioavailability, estradiol levels, concentration–time curve, etc.).
Only one study seems to have researched and characterized sublingual administration of oral estradiol valerate tablets. This study assessed the use of oral estradiol valerate tablets (brand name Progynova [Schering]) administered sublingually 3 to 4 times per day in a group of premenopausal cisgender women. The researchers reported the findings of their study in the following two publications:
Serhal, P., & Craft, I. (1989). Oocyte donation in 61 patients. The Lancet, 333(8648), 1185–1187. [DOI:10.1016/S0140-6736(89)92762-1]
The results in terms of hormone levels with sublingual estradiol valerate were as follows (top plot is a control menstrual cycle in untreated women, bottom plot is a cycle with sublingual estradiol valerate):
Figure 1: Levels of estradiol (E2), progesterone (P4), luteinizing hormone (LH), and follicle-stimulating hormone (FSH) with 2 mg oral micronized estradiol valerate tablets (Progynova) administered sublingually (SL) 3 or 4 times per day in a group of premenopausal women (bottom). The normal menstrual cycle in a control group of premenopausal women is also shown (top). The time of blood collection following administration was not specified.
As can be seen in the figure, estradiol levels with sublingual estradiol valerate were much higher than in normally cycling control women. In addition, levels of other hormones were suppressed, which is in accordance with the high estradiol levels exhibiting negative feedback on the hypothalamic–pituitary–gonadal axis and suppressing hormone production. These findings indicate that sublingual estradiol valerate is well-absorbed and is able to achieve high estradiol levels analogously to sublingual estradiol. In other words, although we still don’t have direct comparisons between the two, sublingual estradiol valerate appears to be a highly effective means of estradiol delivery similarly to sublingual estradiol.
It’s notable that at least one gender-affirming hormone therapy clinic, located in South Korea, uses sublingual estradiol valerate in transfeminine people. These clinicians have briefly described their experience with sublingual estradiol valerate and their rationale for using it over oral estradiol in a recent publication (Lim et al., 2019). While they don’t provide actual pharmacokinetic data on sublingual estradiol valerate (e.g., estradiol levels), it seems apparent based on their clinical experience that sublingual use is a therapeutically effective route of administration for this form of estradiol.
Formulation of Estradiol and Estradiol Valerate Tablets and Implications for Sublingual Use
Micronization of Oral Estradiol Valerate Tablets
Micronization is a manufacturing process in which solid particles of a substance are reduced to smaller sizes. Micronization can modify the pharmacokinetics of medications by altering their rate and extent of absorption. Oral estradiol tablets were originally non-micronized and had lower estrogenic potency than those used today, but in the 1970s micronized oral estradiol tablets were introduced and replaced the previous formulations (Wiki; Wiki). It appears that micronization of estradiol crystals to a defined particle size range improves the absorption and bioavailability of oral estradiol tablets by several-fold (Wiki). All modern oral estradiol tablets available today are assumed to be micronized.
Questions arise as to what influence micronization has on sublingual administration (rather than oral administration) of hormonal agents like estradiol and estradiol valerate and whether oral estradiol valerate tablets are micronized similarly to oral estradiol tablets. The influence of micronization on the sublingual absorption and pharmacokinetic characteristics of estradiol and its esters, as well as other hormonal agents like progesterone and testosterone, does not seem to have been studied and hence is unknown. It could be assumed that micronization might improve the rate and extent of absorption with sublingual administration similarly to oral administration and hence may be important however, as touched on by the following literature excerpt (Sayeed & Ashraf, 2014):
The drugs that are administered sublingually generally have low solubility. Therefore, to enhance dissolution, it is crucial to reduce and control the particle size of the [active pharmaceutical ingredient]. This attribute is important in the case of all drugs with low solubility. However, a tighter control on particle size of [active pharmaceutical ingredient] is desirable in sublingual drug products to maintain the reproducible quality and performance of the drug product in view of the limited window of dissolution and absorption time.
As to whether oral estradiol valerate tablets are micronized, some formulations of oral estradiol valerate clearly indicate that they are micronized in their packaging or manufacturer information (Photo), whereas other formulations of oral estradiol valerate do not. The oral estradiol valerate tablets used in the study by Serhal and Craft (Progynova [Schering]) as well as certain other publications (e.g., Devroey & Pados, 1998) have been explicitly noted to be micronized. Considering the similar doses and apparently comparable clinical properties of all oral estradiol valerate tablets used today, it may be the case that all oral estradiol valerate formulations are micronized but that this simply isn’t always explicitly stated. Indeed, the original form of oral estradiol valerate introduced in the late 1960s is said to have been micronized (Wiki). An alternative but perhaps less likely possibility is that micronization might not influence the properties of oral estradiol valerate similarly to how it does with oral estradiol.
The University of California, San Francisco (UCSF) transgender care guidelines state that only micronized oral estradiol tablets can be used sublingually and imply that not all oral estradiol tablets are micronized (Deutsch, 2016). These statements may be assumed to also apply to oral estradiol valerate tablets. However, as discussed in this article, support for these notions is lacking at present.
Physicochemical Properties of Estradiol versus Estradiol Valerate
Estradiol valerate is more lipophilic (fat-soluble) than estradiol due to its fatty acid ester moiety (i.e., valeric acid). Lipophilicity is known to modify the sublingual and buccal absorption of medications (Smart, 2005; Batheja, Thakur, & Michniak, 2006). How the differing lipophilicities of estradiol versus estradiol valerate may influence their pharmacokinetics when used sublingually has not been studied. Hence, the therapeutic implications of this physicochemical difference for this route are unknown. It’s also known however that esterases are present in the oral mucosa and saliva and can cleave carboxylic acid esters like estradiol valerate into their unesterified forms (Yamahara & Lee, 1993; Rathbone, Drummond, & Tucker, 1994). This might serve to reduce the importance of the physicochemical differences between estradiol valerate and estradiol in terms of sublingual and buccal administration.
Another difference between estradiol and estradiol valerate is that estradiol valerate has a higher molecular weight than estradiol due to its ester component and hence estradiol valerate contains less estradiol than estradiol for the same dose of substance. The molecular weight of estradiol valerate is about 131% of that of estradiol and hence estradiol valerate contains 76% of the estradiol as an equal amount of estradiol (Table). This difference has been shown to translate to pharmacokinetic studies of oral estradiol versus oral estradiol valerate, with estradiol levels being around 25% lower with oral estradiol valerate compared to oral estradiol at equal doses (Wiki). This is likely also the case for other routes of administration of these forms of estradiol, including sublingual administration. Hence, slightly higher doses (e.g., 2 mg versus 1.5 mg) are likely needed and should be used for estradiol valerate relative to estradiol for equivalent estradiol levels and therapeutic estrogenic effect (Sam, 2021).
Formulation and Dissolution of Oral Estradiol Valerate Tablets
Oral estradiol and estradiol valerate tablets were intended and designed for oral administration and not specifically for sublingual administration. Although many of these tablets do clearly work quite well when used sublingually, different tablet formulations vary in their coating and their compositions and excipients. It is possible that differences between formulations of these tablets may influence their properties when used sublingually, as touched on in the following literature excerpt (Sayeed & Ashraf, 2014):
The conditions prevailing in the oral cavity for disintegration and dissolution of sublingual tablets are markedly different from the tablets that are orally ingested. […] Other specialized [oral] tablets, such as modified-release or enteric-coated tablets, may also partly release the drug in the stomach. In contrast, sublingual tablets are designed to completely disintegrate and dissolve in the oral cavity under the tongue.
One particular issue is that different oral tablets of estradiol and estradiol valerate may dissolve at very different rates. One study of oral estradiol tablets used sublingually reported that they dissolved within 1 or 2 minutes (Burnier, 1981). Anecdotally this has been the case similarly with one brand of generic sugar-coated oral estradiol tablets in the United States (Photo), which dissolve and disappear sublingually within a few minutes at most. Some transfeminine people on social media sites like Reddit however have reported their tablets taking much longer to dissolve, for instance about an hour, when used sublingually or buccally. In any case, dissolution rates of oral estradiol and estradiol valerate tablets may vary depending on the formulation, and some forms of oral estradiol and oral estradiol valerate may be better-suited for sublingual use than others. If tablets take a long time to dissolve when used sublingually, switching to another brand may be considered.
Estradiol or Estradiol Valerate for Sublingual Use?
Sublingual administration of oral estradiol tablets has been much better researched and characterized than sublingual administration of oral estradiol valerate tablets. Because of this, it may be advisable to select oral estradiol tablets with the intention of sublingual use over oral estradiol valerate tablets simply because there are fewer unknowns with them. However, oral estradiol tablets may not always be available in a given market, a person may be prescribed oral estradiol valerate tablets instead of oral estradiol tablets, or other considerations may make oral estradiol tablets a less feasible option. In this regard, it is clear based on available literature that sublingual estradiol valerate can be a highly effective means of delivering estradiol similarly to sublingual estradiol and can be used instead if needed.
References
Batheja, P., Thakur, R., & Michniak, B. (2006). Basic Biopharmaceutics of Buccal and Sublingual Absorption. In Touitou, E., & Barry, B. W. (Eds.). Enhancement in Drug Delivery (pp. 175–202). Boca Raton/London/New York: CRC Press. [Google Scholar] [Google Books] [DOI:10.1201/9781420004816-17] [PDF]
Burnier, A. M., Martin, P. L., Yen, S. S., & Brooks, P. (1981). Sublingual absorption of micronized 17β-estradiol. American Journal of Obstetrics and Gynecology, 140(2), 146–150. [DOI:10.1016/0002-9378(81)90101-0]
Deutsch, M. B. (2016). Overview of feminizing hormone therapy. In Deutsch, M. B. (Ed.). Guidelines for the Primary and Gender-Affirming Care of Transgender and Gender Nonbinary People, 2nd Edition (pp. 26–48). San Francisco: University of California, San Francisco/UCSF Transgender Care. [Google Scholar] [URL] [PDF]
Devroey, P., & Pados, G. (1998). Preparation of endometrium for egg donation. Human Reproduction Update, 4(6), 856–861. [DOI:10.1093/humupd/4.6.856]
Lim, H. H., Jang, Y. H., Choi, G. Y., Lee, J. J., & Lee, E. S. (2019). Gender affirmative care of transgender people: a single center’s experience in Korea. Obstetrics & Gynecology Science, 62(1), 46–55. [DOI:10.5468/ogs.2019.62.1.46]
Rathbone, M. J., Drummond, B. K., & Tucker, I. G. (1994). The oral cavity as a site for systemic drug delivery. Advanced Drug Delivery Reviews, 13(1–2), 1–22. [DOI:10.1016/0169-409X(94)90024-8]
Sayeed, V. A., & Ashraf, M. (2014). Considerations in Developing Sublingual Tablets—An Overview. Pharmaceutical Technology, 38(11), 34–72. [Google Scholar] [URL] [PDF]
Serhal, P., & Craft, I. (1989). Oocyte donation in 61 patients. The Lancet, 333(8648), 1185–1187. [DOI:10.1016/S0140-6736(89)92762-1]
Smart, J. D. (2005). Buccal drug delivery. Expert Opinion on Drug Delivery, 2(3), 507–517. [DOI:10.1517/17425247.2.3.507]
Yamahara, H., & Lee, V. H. (1993). Drug metabolism in the oral cavity. Advanced Drug Delivery Reviews, 12(1–2), 25–39. [DOI:10.1016/0169-409X(93)90039-7]
\ No newline at end of file
+Sublingual Administration of Oral Estradiol Valerate Tablets for Transfeminine People - Transfeminine Science
Sublingual Administration of Oral Estradiol Valerate Tablets for Transfeminine People
By Aly | First published January 5, 2019 | Last modified November 28, 2022
Abstract / TL;DR
Oral estradiol tablets can be taken sublingually instead of orally and this allows for greater bioavailability and higher estradiol levels than with oral use. For this reason, sublingual estradiol is frequently used in transfeminine people. Oral estradiol valerate tablets also exist in some parts of the world and it’s often inquired by transfeminine people whether this form of estradiol is likewise effective sublingually. Research in this area is limited and no direct comparisons exist, but at least one study in cisgender women has shown that oral estradiol valerate tablets taken sublingually can result in high estradiol levels and gonadal suppression analogously to sublingual estradiol. In addition, at least one gender-affirming hormone therapy clinic has reported use of sublingual estradiol valerate in transfeminine people. Hence, sublingual estradiol valerate appears to be an effective means of estradiol delivery similarly to sublingual estradiol. One difference between these forms of estradiol is that estradiol valerate contains less estradiol than estradiol by weight and hence should be taken at slightly higher doses. While they can be effective, oral estradiol tablets and oral estradiol valerate tablets were not intended or designed for sublingual use, and formulations of these tablets vary. The implications of this in terms of clinical properties, if any, are unknown. However, it does seem apparent that different tablet formulations may require substantially different amounts of time to dissolve when used sublingually. As a result, some formulations of oral estradiol and oral estradiol valerate may be better-suited for sublingual use than others. Additional characteristics of these formulations like micronization and lipophilicity could also differentially influence their pharmacokinetics in ways that have not been studied. It may be advisable to choose sublingual estradiol over sublingual estradiol valerate where possible simply because sublingual estradiol is much better-characterized in comparison and there are fewer unknowns with it. However, sublingual estradiol valerate can be a clearly effective form of estradiol for transfeminine people as well if needed.
Introduction
Oral estradiol tablets (e.g., Estrace and Estrofem among other brand names) are indicated for oral administration (i.e., taken by mouth/swallowed) and this is how they are normally taken. As an alternative to the standard oral route however, these tablets can be taken sublingually (held under the tongue) or buccally (held in the cheek or lips/gums). Sublingual or buccal administration of oral estradiol tablets allows for much greater bioavailability and estradiol levels in comparison to oral administration (Sam, 2021; Wiki; Graphs; Wiki). Transfeminine people often use sublingual estradiol as the estrogen component of hormone therapy. In various countries, for instance many European countries, estradiol is also provided in oral form as estradiol valerate (EV) tablets (e.g., Progynova among other brand names). It is frequently inquired by transfeminine people whether estradiol valerate tablets can be taken sublingually similarly to estradiol tablets and whether there are any differences between these two estradiol forms for this route. This article is intended to explore and shed some light on these questions.
Effectiveness of Sublingual Estradiol Valerate
Estradiol valerate is an estradiol ester and a prodrug of estradiol. Estradiol esters themselves are pharmacologically inactive prior to conversion into estradiol. Estradiol valerate and other related estradiol esters are cleaved into estradiol by various esteraseenzymes. These esterases are widely expressed throughout the body, and the metabolism of estradiol esters into estradiol occurs not only in the liver but has also been shown to take place rapidly in blood and other tissues (Wiki). Hence, estradiol esters like estradiol valerate do not require the first pass through the liver that occurs with oral administration to become pharmacologically active as estrogens. As such, transformation of estradiol valerate into estradiol should not be an impediment in terms of non-oral administration of estradiol valerate, for instance via sublingual administration (as well as in the form of depot injectables of course).
Studies of estradiol tablets administered sublingually instead of orally are limited, and studies on estradiol valerate tablets used sublingually are extremely scarce. No direct comparisons have been made between sublingual use of estradiol tablets versus sublingual use of estradiol valerate tablets. Hence, we currently don’t have reliable data on how sublingual estradiol valerate compares to sublingual estradiol in terms of pharmacokinetics (e.g., bioavailability, estradiol levels, concentration–time curve, etc.).
Only one study seems to have researched and characterized sublingual administration of oral estradiol valerate tablets. This study assessed the use of oral estradiol valerate tablets (brand name Progynova [Schering]) administered sublingually 3 to 4 times per day in a group of premenopausal cisgender women. The researchers reported the findings of their study in the following two publications:
Serhal, P., & Craft, I. (1989). Oocyte donation in 61 patients. The Lancet, 333(8648), 1185–1187. [DOI:10.1016/S0140-6736(89)92762-1]
The results in terms of hormone levels with sublingual estradiol valerate were as follows (top plot is a control menstrual cycle in untreated women, bottom plot is a cycle with sublingual estradiol valerate):
Figure 1: Levels of estradiol (E2), progesterone (P4), luteinizing hormone (LH), and follicle-stimulating hormone (FSH) with 2 mg oral micronized estradiol valerate tablets (Progynova) administered sublingually (SL) 3 or 4 times per day in a group of premenopausal women (bottom). The normal menstrual cycle in a control group of premenopausal women is also shown (top). The time of blood collection following administration was not specified.
As can be seen in the figure, estradiol levels with sublingual estradiol valerate were much higher than in normally cycling control women. In addition, levels of other hormones were suppressed, which is in accordance with the high estradiol levels exhibiting negative feedback on the hypothalamic–pituitary–gonadal axis and suppressing hormone production. These findings indicate that sublingual estradiol valerate is well-absorbed and is able to achieve high estradiol levels analogously to sublingual estradiol. In other words, although we still don’t have direct comparisons between the two, sublingual estradiol valerate appears to be a highly effective means of estradiol delivery similarly to sublingual estradiol.
It’s notable that at least one gender-affirming hormone therapy clinic, located in South Korea, uses sublingual estradiol valerate in transfeminine people. These clinicians have briefly described their experience with sublingual estradiol valerate and their rationale for using it over oral estradiol in a recent publication (Lim et al., 2019). While they don’t provide actual pharmacokinetic data on sublingual estradiol valerate (e.g., estradiol levels), it seems apparent based on their clinical experience that sublingual use is a therapeutically effective route of administration for this form of estradiol.
Formulation of Estradiol and Estradiol Valerate Tablets and Implications for Sublingual Use
Micronization of Oral Estradiol Valerate Tablets
Micronization is a manufacturing process in which solid particles of a substance are reduced to smaller sizes. Micronization can modify the pharmacokinetics of medications by altering their rate and extent of absorption. Oral estradiol tablets were originally non-micronized and had lower estrogenic potency than those used today, but in the 1970s micronized oral estradiol tablets were introduced and replaced the previous formulations (Wiki; Wiki). It appears that micronization of estradiol crystals to a defined particle size range improves the absorption and bioavailability of oral estradiol tablets by several-fold (Wiki). All modern oral estradiol tablets available today are assumed to be micronized.
Questions arise as to what influence micronization has on sublingual administration (rather than oral administration) of hormonal agents like estradiol and estradiol valerate and whether oral estradiol valerate tablets are micronized similarly to oral estradiol tablets. The influence of micronization on the sublingual absorption and pharmacokinetic characteristics of estradiol and its esters, as well as other hormonal agents like progesterone and testosterone, does not seem to have been studied and hence is unknown. It could be assumed that micronization might improve the rate and extent of absorption with sublingual administration similarly to oral administration and hence may be important however, as touched on by the following literature excerpt (Sayeed & Ashraf, 2014):
The drugs that are administered sublingually generally have low solubility. Therefore, to enhance dissolution, it is crucial to reduce and control the particle size of the [active pharmaceutical ingredient]. This attribute is important in the case of all drugs with low solubility. However, a tighter control on particle size of [active pharmaceutical ingredient] is desirable in sublingual drug products to maintain the reproducible quality and performance of the drug product in view of the limited window of dissolution and absorption time.
As to whether oral estradiol valerate tablets are micronized, some formulations of oral estradiol valerate clearly indicate that they are micronized in their packaging or manufacturer information (Photo), whereas other formulations of oral estradiol valerate do not. The oral estradiol valerate tablets used in the study by Serhal and Craft (Progynova [Schering]) as well as certain other publications (e.g., Devroey & Pados, 1998) have been explicitly noted to be micronized. Considering the similar doses and apparently comparable clinical properties of all oral estradiol valerate tablets used today, it may be the case that all oral estradiol valerate formulations are micronized but that this simply isn’t always explicitly stated. Indeed, the original form of oral estradiol valerate introduced in the late 1960s is said to have been micronized (Wiki). An alternative but perhaps less likely possibility is that micronization might not influence the properties of oral estradiol valerate similarly to how it does with oral estradiol.
The University of California, San Francisco (UCSF) transgender care guidelines state that only micronized oral estradiol tablets can be used sublingually and imply that not all oral estradiol tablets are micronized (Deutsch, 2016). These statements may be assumed to also apply to oral estradiol valerate tablets. However, as discussed in this article, support for these notions is lacking at present.
Physicochemical Properties of Estradiol versus Estradiol Valerate
Estradiol valerate is more lipophilic (fat-soluble) than estradiol due to its fatty acid ester moiety (i.e., valeric acid). Lipophilicity is known to modify the sublingual and buccal absorption of medications (Smart, 2005; Batheja, Thakur, & Michniak, 2006). How the differing lipophilicities of estradiol versus estradiol valerate may influence their pharmacokinetics when used sublingually has not been studied. Hence, the therapeutic implications of this physicochemical difference for this route are unknown. It’s also known however that esterases are present in the oral mucosa and saliva and can cleave carboxylic acid esters like estradiol valerate into their unesterified forms (Yamahara & Lee, 1993; Rathbone, Drummond, & Tucker, 1994). This might serve to reduce the importance of the physicochemical differences between estradiol valerate and estradiol in terms of sublingual and buccal administration.
Another difference between estradiol and estradiol valerate is that estradiol valerate has a higher molecular weight than estradiol due to its ester component and hence estradiol valerate contains less estradiol than estradiol for the same dose of substance. The molecular weight of estradiol valerate is about 131% of that of estradiol and hence estradiol valerate contains 76% of the estradiol as an equal amount of estradiol (Table). This difference has been shown to translate to pharmacokinetic studies of oral estradiol versus oral estradiol valerate, with estradiol levels being around 25% lower with oral estradiol valerate compared to oral estradiol at equal doses (Wiki). This is likely also the case for other routes of administration of these forms of estradiol, including sublingual administration. Hence, slightly higher doses (e.g., 2 mg versus 1.5 mg) are likely needed and should be used for estradiol valerate relative to estradiol for equivalent estradiol levels and therapeutic estrogenic effect (Sam, 2021).
Formulation and Dissolution of Oral Estradiol Valerate Tablets
Oral estradiol and estradiol valerate tablets were intended and designed for oral administration and not specifically for sublingual administration. Although many of these tablets do clearly work quite well when used sublingually, different tablet formulations vary in their coating and their compositions and excipients. It is possible that differences between formulations of these tablets may influence their properties when used sublingually, as touched on in the following literature excerpt (Sayeed & Ashraf, 2014):
The conditions prevailing in the oral cavity for disintegration and dissolution of sublingual tablets are markedly different from the tablets that are orally ingested. […] Other specialized [oral] tablets, such as modified-release or enteric-coated tablets, may also partly release the drug in the stomach. In contrast, sublingual tablets are designed to completely disintegrate and dissolve in the oral cavity under the tongue.
One particular issue is that different oral tablets of estradiol and estradiol valerate may dissolve at very different rates. One study of oral estradiol tablets used sublingually reported that they dissolved within 1 or 2 minutes (Burnier, 1981). Anecdotally this has been the case similarly with one brand of generic sugar-coated oral estradiol tablets in the United States (Photo), which dissolve and disappear sublingually within a few minutes at most. Some transfeminine people on social media sites like Reddit however have reported their tablets taking much longer to dissolve, for instance about an hour, when used sublingually or buccally. In any case, dissolution rates of oral estradiol and estradiol valerate tablets may vary depending on the formulation, and some forms of oral estradiol and oral estradiol valerate may be better-suited for sublingual use than others. If tablets take a long time to dissolve when used sublingually, switching to another brand may be considered.
Estradiol or Estradiol Valerate for Sublingual Use?
Sublingual administration of oral estradiol tablets has been much better researched and characterized than sublingual administration of oral estradiol valerate tablets. Because of this, it may be advisable to select oral estradiol tablets with the intention of sublingual use over oral estradiol valerate tablets simply because there are fewer unknowns with them. However, oral estradiol tablets may not always be available in a given market, a person may be prescribed oral estradiol valerate tablets instead of oral estradiol tablets, or other considerations may make oral estradiol tablets a less feasible option. In this regard, it is clear based on available literature that sublingual estradiol valerate can be a highly effective means of delivering estradiol similarly to sublingual estradiol and can be used instead if needed.
References
Batheja, P., Thakur, R., & Michniak, B. (2006). Basic Biopharmaceutics of Buccal and Sublingual Absorption. In Touitou, E., & Barry, B. W. (Eds.). Enhancement in Drug Delivery (pp. 175–202). Boca Raton/London/New York: CRC Press. [Google Scholar] [Google Books] [DOI:10.1201/9781420004816-17]
Burnier, A. M., Martin, P. L., Yen, S. S., & Brooks, P. (1981). Sublingual absorption of micronized 17β-estradiol. American Journal of Obstetrics and Gynecology, 140(2), 146–150. [DOI:10.1016/0002-9378(81)90101-0]
Deutsch, M. B. (2016). Overview of feminizing hormone therapy. In Deutsch, M. B. (Ed.). Guidelines for the Primary and Gender-Affirming Care of Transgender and Gender Nonbinary People, 2nd Edition (pp. 26–48). San Francisco: University of California, San Francisco/UCSF Transgender Care. [Google Scholar] [URL] [PDF]
Devroey, P., & Pados, G. (1998). Preparation of endometrium for egg donation. Human Reproduction Update, 4(6), 856–861. [DOI:10.1093/humupd/4.6.856]
Lim, H. H., Jang, Y. H., Choi, G. Y., Lee, J. J., & Lee, E. S. (2019). Gender affirmative care of transgender people: a single center’s experience in Korea. Obstetrics & Gynecology Science, 62(1), 46–55. [DOI:10.5468/ogs.2019.62.1.46]
Rathbone, M. J., Drummond, B. K., & Tucker, I. G. (1994). The oral cavity as a site for systemic drug delivery. Advanced Drug Delivery Reviews, 13(1–2), 1–22. [DOI:10.1016/0169-409X(94)90024-8]
Sayeed, V. A., & Ashraf, M. (2014). Considerations in Developing Sublingual Tablets—An Overview. Pharmaceutical Technology, 38(11), 34–72. [Google Scholar] [URL] [PDF]
Serhal, P., & Craft, I. (1989). Oocyte donation in 61 patients. The Lancet, 333(8648), 1185–1187. [DOI:10.1016/S0140-6736(89)92762-1]
Smart, J. D. (2005). Buccal drug delivery. Expert Opinion on Drug Delivery, 2(3), 507–517. [DOI:10.1517/17425247.2.3.507]
Yamahara, H., & Lee, V. H. (1993). Drug metabolism in the oral cavity. Advanced Drug Delivery Reviews, 12(1–2), 25–39. [DOI:10.1016/0169-409X(93)90039-7]
\ No newline at end of file
diff --git a/transfemscience.org/articles/transfem-intro/index.html b/transfemscience.org/articles/transfem-intro/index.html
index afc82b4e..1d7473ee 100644
--- a/transfemscience.org/articles/transfem-intro/index.html
+++ b/transfemscience.org/articles/transfem-intro/index.html
@@ -1 +1 @@
-An Introduction to Hormone Therapy for Transfeminine People - Transfeminine Science
An Introduction to Hormone Therapy for Transfeminine People
By Aly | First published August 4, 2018 | Last modified June 26, 2024
Abstract / TL;DR
Sex hormones such as estrogen, testosterone, and progesterone are produced by the gonads. The sex hormones mediate the development of the secondary sexual characteristics. Testosterone causes masculinization, while estradiol causes feminization and breast development. Males have high amounts of testosterone, while females have low testosterone but high amounts of estradiol. These hormonal differences are responsible for the physical differences between males and females. Sex hormones and other hormonal medications are used in transfeminine people to shift the hormonal profile from a male-typical one to a female-typical profile. This causes feminization and demasculinization and allows for alleviation of gender dysphoria. The changes caused by transfeminine hormone therapy occur over a period of months to years. There are many different types and forms of hormonal medications, and these medications can be administered by a variety of different routes. Examples include as pills taken by mouth, as patches or gel applied to the skin, and as injections, among others. Different hormonal medications, routes, and doses have differences in efficacy, side effects, risks, costs, convenience, and availability. Hormone therapy should ideally be regularly monitored in transfeminine people with blood tests to ensure effectiveness and safety and to allow for adjustment as necessary.
The Sex Hormones
Types and Effects
The sex hormones include the estrogens (E), progestogens (P), and androgens. A person’s hormonal profile is a product of the type of gonads that they are born with. Natal males have testes while natal females have ovaries. Testes produce large amounts of androgens and small amounts of estrogens whereas ovaries produce high amounts of estrogens and progesterone and low amounts of androgens.
Progestogens have essentially no known role in feminization or pubertal breast development. Rather than acting as mediators of feminization, progestogens have important effects in the female reproductive system and are essential hormones during pregnancy (Wiki). They also oppose the actions of estrogens in certain parts of the body, such as the uterus, vagina, and breasts (Wiki).
In addition to their effects on the body, sex hormones have actions in the brain. These actions influence cognition, emotions, and behavior. For instance, androgens produce pronounced sexual desire and arousal (including spontaneous erections) in men, while estrogens appear to be the major hormones responsible for sexual desire in women (Cappelletti & Wallen, 2016). As another example, testosterone levels have been negatively associated with agreeableness, whereas estrogen levels have been positively associated with this characteristic (Treleaven et al., 2013). Sex hormones also have important effects on health, which can be both positive and negative. For instance, estrogens maintain bone strength and likely protect against heart disease in cisgender women (NAMS, 2022), but also increase the risk of breast cancer (Aly, 2020) and can increase the risk of blood clots (Aly, 2020).
Estrogens, progestogens, and androgens also have antigonadotropic effects. That is, they inhibit the gonadotropin-releasing hormone (GnRH)-induced secretion of the gonadotropins, luteinizing hormone (LH) and follicle-stimulating hormone (FSH), from the pituitary gland in the brain. The gonadotropins signal the gonads to make sex hormones and to supply the sperm and egg cells necessary for fertility. Hence, lower levels of the gonadotropins will result in reduced gonadal sex hormone production and diminished fertility. If gonadotropin levels are sufficiently suppressed, the gonads will no longer make sex hormones at all and fertility will cease. The vast majorities of the quantities of estradiol, testosterone, and progesterone in the body are produced by the gonads. Most of the small remaining amounts of these hormones are produced via the adrenal glands of the kidneys.
Normal Hormone Levels
In cisgender females, the sex hormones are largely absent during childhood, gradually ramp up in production in late childhood and adolescence, are present in a cyclical manner during adulthood, and then largely stop being produced following the menopause. Hormone levels vary substantially but in a predictable manner during the normal menstrual cycle in adult premenopausal women. The menstrual cycle lasts about 28 days on average and consists of the following parts:
Luteal phase—latter half of the cycle or days 14–28
Hormone levels during the menstrual cycle are shown in the following graph:
Figure 1: Median estradiol and progesterone levels throughout the menstrual cycle in premenopausal cisgender women (Stricker et al., 2006; Abbott, 2009). The horizontal dashed lines are the average levels over the spanned periods. Other figures available elsewhere show variation between individuals (Graph; Graph; Graph).
As can be seen in the graph, estradiol levels are relatively low and progesterone levels are very low during the follicular phase; estradiol but not progesterone levels briefly surge to very high levels and trigger ovulation during mid-cycle; and estradiol and progesterone levels both undergo a bump and are relatively high during the luteal phase (though estradiol is not as high as during the mid-cycle peak).
The table below shows the circulating levels and production rates of estradiol, progesterone, and testosterone in women and men and allows for comparison between them.
Table 1: Ranges for circulating levelsa and estimated production ratesb of the major sex hormones:
Mean integrated estradiol levels are around 100 pg/mL (367 pmol/L) in premenopausal women and around 25 pg/mL (92 pmol/L) in men. The 95% range for mean estradiol levels in women is around 50 to 250 pg/mL (180–918 pmol/L) (e.g., Abbott, 2009 (Graph); Verdonk et al., 2019 (Graph)). The average production of estradiol by the ovaries in premenopausal women is about 6 mg over the course of one menstrual cycle (i.e., one month) (Rosenfield et al., 2008). This corresponds to a mean rate of about 200 μg/day. Estradiol levels increase slowly during normal female puberty, when breast development and feminization take place. Mean estradiol levels during the different stages of female puberty are quite low—less than about 50 to 60 pg/mL (180–220 pmol/L) until late puberty (Aly, 2020). In postmenopausal women, whose ovaries no longer produce considerable quantities of estrogens, estradiol levels are generally less than 10 to 20 pg/mL (37–73 pmol/L) (Nakamoto, 2016). Estradiol levels below 50 pg/mL (184 pmol/L) in adults are concentration-dependently associated with menopausal symptoms, including hot flashes, depressive mood changes, defeminization (e.g., breast atrophy, loss of feminine fat distribution), accelerated skin aging, and bone density loss with increased risk of bone fracture.
Mean testosterone levels are around 30 ng/dL (1.0 nmol/L) in women and 600 ng/dL (21 nmol/L) in men. Based on these values, testosterone levels are on average about 20-fold higher in men than in women. In men who have undergone gonadectomy (castration or surgical gonadal removal), testosterone levels are similar to those in women (<50 ng/dL [1.7 nmol/L]) (Nishiyama, 2014; Itty & Getzenberg, 2020). The mean or median levels of testosterone in women with polycystic ovary syndrome (PCOS), who often have clinically significant symptoms of androgen excess (e.g., excessive facial/body hair growth), range from 41 to 75 ng/dL (1.4–2.6 nmol/L) per different studies (Balen et al., 1995; Steinberger et al., 1998; Legro et al., 2010; Loh et al., 2020). Hence, it appears that even testosterone levels that are marginally elevated relative to normal female levels may produce undesirable androgenic effects.
The goal of hormone therapy for transfeminine people, otherwise known as feminizing hormone therapy (FHT) or (more in the past) as male-to-female (MtF) hormone replacement therapy (HRT), is to produce feminization and demasculinization of the body as well as alleviation of gender dysphoria. Medication therapy with sex hormones and other sex-hormonal medications is used to mediate these changes. Transfeminine people are given estrogens, progestogens, and antiandrogens (AAs) to supersede gonadal sex hormone production and shift the hormonal profile from male-typical to female-typical.
Transfeminine hormone therapy aims to achieve estradiol and testosterone levels within the normal female range. Commonly recommended ranges for transfeminine people in the literature are 100 to 200 pg/mL (367–734 pmol/L) for estradiol levels and less than 50 ng/dL (1.7 nmol/L) for testosterone levels (Table). However, higher estradiol levels of more than 200 pg/mL (734 pmol/L) can be useful in transfeminine hormone therapy to help suppress testosterone levels. Lower estradiol levels (≤50–60 pg/mL [≤180–220 pmol/L]) are recommended and more appropriate for pubertal and adolescent transfeminine individuals. Sex hormone levels in the blood can be measured with blood tests, in which blood is drawn from a vein using a needle and then analyzed in a laboratory. This is useful in transfeminine people to ensure that the hormonal profile has been satisfactorily altered in line with therapeutic goals—specifically that hormone levels are within female ranges.
Gonadal Suppression
At sufficiently high exposure, estrogens and androgens are able to completely suppress gonadal sex hormone production, while progestogens by themselves are able to partially but substantially suppress gonadal sex hormone production. More specifically, studies in cisgender men and transfeminine people have found that estradiol levels of around 200 pg/mL (734 pmol/L) suppress testosterone levels by about 90% on average (to ~50 ng/dL [1.7 nmol/L]), while estradiol levels of around 500 pg/mL (1,840 pmol/L) suppress testosterone levels by about 95% on average (to ~20–30 ng/dL [0.7–1.0 nmol/L]) (Gooren et al., 1984 [Graph]; Herndon et al., 2023 [Discussion]; Wiki; Graphs). Estradiol levels of below 200 pg/mL (734 pmol/L) also suppress testosterone levels, although to a reduced extent compared to higher levels (Aly, 2019; Krishnamurthy et al., 2023; Slack et al., 2023). In one large study in transfeminine people, the rates of adequate testosterone suppression (to testosterone levels of <50 ng/dL or <1.7 nmol/L) were 24% of individuals at estradiol levels of <100 pg/mL (367 pmol/L), 58% at 100 to 200 pg/mL (367–734 pmol/L), and 77% at >200 pg/mL (>734 pmol/L) (Krishnamurthy et al., 2023).
Figure 2: Estradiol and testosterone levels after a single injection of 320 mg polyestradiol phosphate (PEP) (a long-acting prodrug of estradiol) in men with prostate cancer (Stege et al., 1996). The maximal decrease in testosterone levels occurred with estradiol levels of greater than 200 pg/mL (734 pmol/L) and was about 90% (to roughly 50 ng/dL [1.7 nmol/L]). This figure demonstrates the ability of estradiol to concentration-dependently suppress gonadal testosterone production and circulating testosterone levels in people with testes.
Progestogens on their own are able to maximally suppress testosterone levels by about 50 to 70% (to ~150–300 ng/dL [5.2–10.4 nmol/L] on average) (Aly, 2019; Wiki). In combination with relatively small amounts of estrogen however, there is synergism in the antigonadotropic effect—the suppression of gonadal testosterone production with maximally effective doses of progestogens becomes complete, and testosterone levels are reduced by about 95% (to ~20–30 ng/dL [0.7–1.0 nmol/L]) (Aly, 2019). Hence, the combination of an estrogen and a progestogen can be used to achieve maximal testosterone suppression at lower doses than would be necessary if an estrogen or progestogen were used alone.
The antigonadotropic effects of estrogens and progestogens are taken advantage of in transfeminine hormone therapy to suppress gonadal testosterone production and attain testosterone levels that are more consistent with those in cisgender women. It should be noted that the preceding numbers on testosterone suppression with estrogens and progestogens are averages and there is significant variation between individuals in terms of testosterone suppression. In other words, some may need more or less in terms of hormonal dosages to achieve the same decrease in testosterone levels.
Timeline of Effects
During normal puberty in both males and females, sex hormone exposure increases slowly over a period of several years (Aly, 2020). In relation to this, sexual maturation occurs gradually during normal puberty. In non-adolescent transgender people, adult or higher amounts of hormones are generally administered right away, and this can result in changes in secondary sex characteristics happening more quickly. The table below is reproduced from literature sources with slight modification and is commonly cited as a timeline for the effects of hormone therapy in transfeminine people (Table). It is based on a mixture of anecdotal clinical experience, expert opinion, and available clinical studies of hormone therapy in transfeminine people. Due to limited research characterizing the effects of transfeminine hormone therapy at present, the table may or may not be completely accurate.
Table 2: Effects of hormone therapy at typical doses in adult transfeminine people (Wiki):
Effect
Onseta
Completiona
Permanency
Breast development
2–6 months
2–3 years
Permanent
Reduced and slowed growth of facial and body hair
3–12 months
>3 yearsb
Reversible
Cessation and reversal of scalp hair loss
1–3 months
1–2 years
Reversible
Softening of skin and decreased skin oiliness and acne
3–6 months
Unknown
Reversible
Redistribution of body fat in a feminine pattern
3–6 months
2–5 years
Reversible
Decreased muscle mass and strength
3–6 months
1–2 yearsc
Reversible
Widening and rounding of the pelvisd
Unknown
Unknown
Permanent
Changes in mood, emotionality, and behavior
Immediate
Unknown
Reversible
Decreased sex drive and spontaneous erections
1–3 months
3–6 months
Reversible
Erectile dysfunction and decreased ejaculate volume
1–3 months
Variable
Reversible
Decreased sperm production and infertility
Unknown
>3 years
Mixede
Decreased testicular volume
3–6 months
2–3 years
Unknown
Voice changes (e.g., decreased pitch/resonance)
Nonef
N/A
N/A
a May vary significantly between individuals due to factors like genetics, diet/nutrition, hormone levels, etc. b Hormone therapy usually has little influence on facial hair density in transfeminine people. Complete removal of facial and body hair can be achieved with laser hair removal and electrolysis. Temporary hair removal can be achieved with shaving, epilating, waxing, and other methods. c May vary significantly depending on amount of physical exercise. d Occurs only in young individuals who have not yet completed growth plate closure (may not occur at all in post-adolescent people). e Only estrogens, particularly at high doses, seem to have the potential for long-lasting or irreversible infertility; impaired fertility caused by antiandrogens is usually readily reversible with discontinuation. fVoice training can be an effective means of feminizing the voice.
Breast development is one of the most anticipated effects of feminizing hormone therapy in transfeminine people (Masumori et al., 2021; Grock et al., 2024). Some review content on breast development in transfeminine people exists on this site (e.g., Aly, 2020). Breast growth can notably be measured and tracked with a variety of methods (Wiki). For see real-life photographic timelines of breast development (as well as feminization in general) with feminizing hormone therapy in transfeminine people, see the r/TransBreastTimelines community on the social media website Reddit.
Specific Hormonal Medications
The medications that are used in transfeminine hormone therapy include estrogens, progestogens, and antiandrogens. Estrogens produce feminization and testosterone suppression. Progestogens and antiandrogens do not mediate feminization themselves but further suppress and/or block testosterone. Testosterone suppression causes demasculinization and disinhibition of estrogen-mediated feminization. Androgens are sometimes used at low doses in transfeminine people who have low testosterone levels, although they are not required and benefits are uncertain. There are many different types of these hormonal medications available for transfeminine hormone therapy, with different benefits and risks.
Estrogens, progestogens, and antiandrogens are available in a variety of different formulations and for use by many different routes of administration in transfeminine people. The route of administration influences the absorption, distribution, metabolism, and elimination of the hormone in the body, resulting in significant differences between routes in terms of bioavailability, hormone levels in blood and specific tissues, and patterns of metabolites. These differences can have important therapeutic consequences.
Table 3: Major routes of administration of hormonal medications for transfeminine people:
Insertion via surgical incision into fat under skin
Pellet
Vaginal administration is a major additional route of administration of hormonal medications in cisgender women. While vaginal administration via a natal vagina is of course not possible in transfeminine people, neovaginal administration is a possiblility in those who have undergone vaginoplasty. However, the lining of the neovagina is not the vaginal epithelium of natal females but instead is usually skin or colon—depending on the type of vaginoplasty performed (penile inversion or sigmoid colon vaginoplasty, respectively). For this reason, neovaginal administration in transfeminine people is likely more similar in its properties to transdermal and rectal administration—depending on the type of neovagina—than to vaginal administration in cisgender women. It is noteworthy that the vaginal and rectal routes are said to be similar in their properties for hormonal medications however (Goletiani, Keith, & Gorsky, 2007; Wiki). Moreover, absorption of estradiol via neovaginas constructed from peritoneum (internal abdominal lining)—a less commonly employed vaginoplasty approach in transfeminine people—was reported in one study to be similar to that with vaginal administration of estradiol in cisgender women (Willemsen et al., 1985). As such, neovaginal administration may be an additional possible route for certain transfeminine people depending on the circumstances. However, this route still remains to be more adequately characterized.
Estrogens
Estradiol, the primary bioidentical form normally found in the human body, is the main estrogen that is used in transfeminine hormone therapy. Estradiol hemihydrate (EH) is another form that is essentially identical to and interchangeable with estradiol. Estradiol esters are also sometimes used in place of estradiol. They are prodrugs of estradiol (i.e., are converted into estradiol in the body) and have essentially identical biological activity to estradiol. However, they have longer durations when used by injection due to slower absorption from the injection site, and this allows them to be administered less often. Some examples of major estradiol esters include estradiol valerate (EV; Progynova, Progynon Depot, Delestrogen) and estradiol cypionate (EC; Depo-Estradiol). Polyestradiol phosphate (PEP; Estradurin) is an injectable estradiol prodrug in the form of a polymer (i.e., linked chain of estradiol molecules) which is metabolized slowly and has a very long duration.
Non-bioidentical estrogens such as ethinylestradiol (EE; found in birth control pills), conjugated estrogens (CEEs; Premarin; used in menopausal hormone therapy), and diethylstilbestrol (DES; widely used previously but now abandoned) are resistant to metabolism in the liver and have disproportionate effects on estrogen-modulated liver synthesis when compared to bioidentical estrogens like estradiol (Aly, 2020). As a result, they have stronger influence on coagulation and greater risk of certain health problems like blood clots and associated cardiovascular issues (Aly, 2020). For this reason, as well as the fact that relatively high doses of estrogens may be needed for testosterone suppression, non-bioidentical estrogens should ideally never be used in transfeminine hormone therapy.
Estradiol dose-dependently suppresses testosterone levels in people with testes. Physiological and guideline-based levels of estradiol (<200 pg/mL or <734 pmol/L) are often not sufficient to suppress testosterone levels into the female range in transfeminine people who have not had their gonads removed (e.g., Liang et al., 2018; Krishnamurthy et al., 2023; Slack et al., 2023). As a result, estradiol is generally used in combination with an antiandrogen or progestogen in transfeminine hormone therapy (Hembree et al., 2017; Coleman et al., 2022; Rose et al., 2023). This results in partial suppression of testosterone levels by estradiol and further suppression or blockade of the remaining testosterone by the antiandrogen or progestogen. While combination therapy can be effective in fully suppressing or blocking testosterone (e.g., Aly, 2019; Aly, 2020), testosterone suppression can also still remain incomplete with antiandrogens and progestogens in certain forms (e.g., Aly, 2018; Jain, Kwan, & Forcier, 2019). In contrast to physiological estradiol levels, supraphysiological levels of estradiol are able to consistently and fully suppress testosterone levels into the normal female range with estradiol alone in transfeminine people (e.g., Gooren et al., 1984 [Graph]; Igo & Visram, 2021; Herndon et al., 2023 [Discussion]). This alternative approach, often referred to as high-dose estradiol monotherapy, has the advantage of avoiding the side effects, risks, and costs of antiandrogens and progestogens. However, it has the disadvantage of exposure to supraphysiological estradiol levels that are above those recommended by guidelines and that may have greater health risks. Physiological estradiol doses and combination therapy are more often used in transfeminine people treated by clinicians, whereas high-dose estradiol monotherapy is more frequently encountered in transfeminine people on DIY hormone therapy.
The feminizing effects of estradiol appear to be maximal at relatively low levels in the absence of androgens. Higher doses of estradiol and supraphysiological estradiol levels, aside from allowing for greater testosterone suppression, are not known to result in better feminization in transfeminine people (Deutsch, 2016; Nolan & Cheung, 2021). In fact, there is some indication that higher estrogen doses early into hormone therapy could actually result in worse breast development. Hence, the therapeutic emphasis in transfeminine hormone therapy is more on testosterone suppression than on achieving a specific estradiol level, at least above a certain low threshold level. Higher doses of estrogens, including of estradiol, also have a greater risk of adverse health effects such as blood clots and cardiovascular problems (Aly, 2020). As such, the use of physiological doses of estradiol is optimal in transfeminine people. At the same time however, high estrogen doses can be useful for improving testosterone suppression when it is inadequate, and the absolute risks, in the case of non-oral bioidentical estradiol, are low and are more important in people with specific risk factors (e.g., older age, physical inactivity, obesity, concomitant progestogen use, smoking, surgery, and rare thrombophilic abnormalities). If more adequate testosterone suppression is necessary, limitedly supraphysiological doses of non-oral estradiol may have a reasonable ratio of benefit to risk in this context, at least in those without relevant risk factors for estrogen-related complications (e.g., many healthy young people) (Aly, 2020).
Estradiol and estradiol esters are usually used orally, sublingually, transdermally, by injection (intramuscularly or subcutaneously), or by implant in transfeminine hormone therapy (Wiki).
Oral Estradiol
Estradiol is used orally in the form of tablets of estradiol (Wiki; Graphs). Alternatively, oral estradiol valerate tablets are used in some countries, for instance in many European countries. The only real differences between these oral estradiol forms is that estradiol valerate contains slightly less estradiol by weight (~76%) due to its ester component and hence requires somewhat higher doses (~1.3-fold) in comparison for equivalent estradiol levels (Wiki; Table). Oral estradiol has a duration suitable for once-daily administration. Oral administration of estradiol is a very convenient and inexpensive route, which makes it the most popular and widely used form of estradiol in transfeminine people. Oral estradiol has relatively low bioavailability (~5%), and there is substantial variability between people in terms of estradiol levels achieved with the same dose. Hence, in some transfeminine people estradiol levels may be low with oral estradiol, and testosterone suppression may be inadequate depending on the antiandrogen.
A major drawback of oral estradiol is that it results in excessive levels of estradiol in the liver due to the first pass that occurs with oral administration and has a disproportionate impact on estrogen-modulated liver synthesis (Aly, 2020). This in turn increases coagulation and the risk of associated health complications like blood clots and cardiovascular problems (Aly, 2020). These particular health concerns are largely allayed if estradiol is taken non-orally at reasonable and non-excessive doses. Hence non-oral forms of estradiol, like transdermal estradiol, although less convenient and often more expensive than oral estradiol, are preferable in transfeminine hormone therapy. It is recommended that all transfeminine people who are over 40 to 45 years of age use non-oral routes due to the greater risk of blood clots and cardiovascular problems that occurs with age (Aly, 2020; Coleman et al., 2022). Oral estradiol is not a good choice for high-dose estradiol monotherapy in transfeminine people due to the high estradiol levels required and the greater risks than with non-oral routes. In addition to its disproportionate liver impact, oral estradiol results in unphysiological levels of estradiol metabolites like estrone and estrone sulfate when compared to non-oral forms. The clinical implications of this, if any, are unknown. Oral and non-oral estradiol have in any case been found to have similar effectiveness in terms of feminization and breast development in transfeminine people in available studies (Sam, 2020).
Sublingual Estradiol
Oral estradiol tablets can be taken sublingually instead of orally. Sublingual use of estradiol tablets has several-fold higher bioavailability relative to oral administration and hence achieves much higher overall estradiol levels in comparison (Sam, 2021; Wiki; Graphs). Sublingual use of oral estradiol tablets can be employed instead of oral administration to reduce doses and hence medication costs or to produce higher estradiol levels for the purpose of achieving better testosterone suppression when needed. However, sublingual estradiol is very spiky in terms of estradiol levels when compared to oral estradiol and has a short duration of highly elevated estradiol levels. As such, it may be advisable for sublingual estradiol to be used in divided doses multiple times throughout the day in order to maintain at least somewhat steadier estradiol levels. The therapeutic implications for transfeminine people of the spikiness of sublingual estradiol, for instance in terms of testosterone suppression and health risks, have been little-studied and are mostly unknown. In any case, when used as a form of high-dose estradiol monotherapy and taken multiple times per day, strong though still incomplete testosterone suppression has been observed (Yaish et al., 2023). Oral estradiol valerate tablets can be taken sublingually instead of orally similarly to estradiol and are likewise highly effective when used in this way (Aly, 2019; Wiki). Due to partial swallowing of tablets, sublingual estradiol may in practice be a mixture of sublingual and oral administration and may have some of the same health risks of oral estradiol (Wiki). Buccal administration of estradiol appears to have similar properties as sublingual administration but is much less researched in comparison and is not used as often in transfeminine people (Wiki).
Transdermal Estradiol
Transdermal estradiol is available in the form of patches, gel, emulsions, and sprays (Wiki). These forms are usually applied to skin areas such as the arms, abdomen, or buttocks. Gel, emulsions, and sprays are applied and left to dry for a short period, whereas patches are applied and remain adhesed to the skin for a specified amount of time. Due to rate-limited absorption through the skin, there is a depot effect with transdermal estradiol and this route has a long duration with very steady estradiol levels. As a result, estradiol gel, emulsions, and sprays are all suitable for once-daily use. Patches stay applied and continuously deliver estradiol for either 3–4 days or 7 days depending on the patch brand (Table). Transdermal estradiol is more expensive than oral estradiol. Gel, emulsions, and sprays may be less convenient than oral administration, but patches can be more convenient due to their infrequent application. However, patches can sometimes cause application site problems like redness and irritation and can occasionally come off prematurely due to adhesive failure. As with oral estradiol, there is substantial variability in estradiol levels with transdermal estradiol, and some transfeminine people may have poor absorption, low estradiol levels, and inadequate testosterone suppression with this route. Estradiol sprays, such as Lenzetto, have been found to achieve very low estradiol levels that are probably not therapeutically adequate for use in transfeminine hormone therapy (Aly, 2020; Graph).
Transdermal estradiol is the form of estradiol most commonly used in transfeminine people who are over 40 years of age due to its lower health risks relative to oral estradiol. Transdermal estradiol gel is not a favorable option for high-dose estradiol monotherapy as it has difficulty achieving the high estradiol levels needed for adequate testosterone suppression (Aly, 2019). On the other hand, transdermal estradiol patches can be an effective option for high-dose estradiol monotherapy if multiple 100 μg/day patches are used, although this can require the use of many patches and can be expensive (Wiki). Different skin sites absorb transdermal estradiol to different extents (Wiki). Genital application of transdermal estradiol, specifically to the scrotum or neolabia, is particularly better-absorbed than conventional skin sites and can result in much higher estradiol levels than usual (Aly, 2019). This can be useful for reducing doses and hence medication costs or for achieving higher estradiol levels for better testosterone suppression when needed, for instance in the context of high-dose estradiol monotherapy. Transdermal estradiol should not be applied to the breasts as this is not known to result in improved breast development and the potential health consequences of doing so are unknown (e.g., influence on breast cancer risk).
Injectable Estradiol
Injectable estradiol preparations can be administered via either intramuscular or subcutaneous injection (Wiki; Wiki; Graphs). There is a depot effect with injection of estradiol esters such that they are slowly absorbed from the injection site and have a prolonged duration. This ranges from days to months depending on the ester. Commonly used injectable estradiol esters, which all have short to moderate durations, include estradiol valerate (EV), estradiol cypionate (EC), estradiol enanthate (EEn), and estradiol benzoate (EB). Longer-acting injectable estradiol esters, such as estradiol undecylate (EU) and polyestradiol phosphate (PEP), have been discontinued and are no longer pharmaceutically available. In the case of intramuscular injection, common injection sites include the deltoid muscle (upper arm), vastus lateralis and rectus femoris muscles (thigh), and ventrogluteal muscle (buttocks). Subcutaneous injection of estradiol injectables, while less commonly used, has comparable pharmacokinetics to intramuscular injection, and is easier, less painful, and more convenient in comparison (Wiki). However, the maximum volume that can be safely and comfortably injected subcutaneously is less than that which can be injected intramuscularly (depending on the site up to 1.5–3 mL and up to 2–5 mL, respectively) (Hopkins, & Arias, 2013; Usach et al., 2019). Injectable estradiol tends to be fairly inexpensive, but may be less convenient than other routes due to the need for regular injections. There may also be a risk of internal scar tissue build-up long-term. Estradiol injectables have been discontinued in many parts of the world (e.g., most of Europe), and their availability is limited. In recent years, many transfeminine people have turned to black market homebrewed injectable estradiol preparations to use this route.
Injectable estradiol preparations are typically used at higher doses than other forms of estradiol, and can easily achieve very high levels of estradiol. This can be useful for testosterone suppression, making this form of estradiol likely the best choice for high-dose estradiol monotherapy in transfeminine people. However, the high doses that are possible with injectable estradiol preparations can also easily lead to overdosage and unnecessarily increased risks (e.g., Aly, 2020). Resources are available on this site for guiding selection of appropriate doses and intervals of injectable estradiol esters in transfeminine people. This includes a simulator and informal meta-analysis of estradiol levels with these preparations (Aly, 2021; Aly, 2021) and a table providing approximate equivalent doses between injectable estradiol esters and other estradiol routes and forms (Aly, 2020). It is notable and unfortunate that currently recommended doses and intervals for injectable estradiol esters by transgender care guidelines (e.g., 10–40 mg/2 weeks estradiol valerate) appear to be highly excessive and too widely spaced, and are likely to be therapeutically inadvisable (Aly, 2021). Doses and intervals of injectable estradiol esters recommended by the present author for use as a means of high-dose estradiol monotherapy, targeting mean estradiol levels of around 300 pg/mL (1,100 pmol/L), are provided below (Table 4).
Table 4: Recommended doses and intervals of injectable estradiol esters for high-dose estradiol monotherapy (targeting estradiol levels of around 300 pg/mL [1,100 pmol/L]):
a Doses and intervals for estradiol undecylate are extrapolated and hypothetical (Aly, 2021).
These doses and intervals should be considered a starting point, and should be fine-tuned as necessary based on blood tests. In terms of injection intervals, the shorter interval, the more stable the estradiol levels, but the more often that injections need to be done. Doses may be increased if estradiol levels are too low and testosterone suppression is inadequate, and doses may be decreased if estradiol levels are too high so long as adequate testosterone suppression is maintained. Doses should be lower (targeting mean estradiol levels of 100–200 pg/mL [367–734 pmol/L]) if combined with an antiandrogen or progestogen as these agents will help with testosterone suppression. Similarly, doses should be lower following surgical gonadal removal as testosterone suppression will no longer be necessary.
Estradiol Pellets
Estradiol implants are pellets of pure crystalline hormone and are surgically placed into subcutaneous fat by a physician (Wiki). They are slowly absorbed by the body following implantation, and new implants are given once every 4 to 6 months. Due to the need for minor surgery, their high cost, and limited availability, estradiol implants are not as commonly used as other estradiol routes. Notably, almost all pharmaceutical estradiol implants throughout the world have been discontinued, and the implants that remain available are almost exclusively compounded products provided by compounding pharmacies. Dosage adjustment with estradiol implants is also more difficult than with other estradiol routes. Despite their various practical limitations however, estradiol implants allow for very steady estradiol levels, and their very long duration can allow for unusual convenience among available estradiol forms.
Additional Notes
Table 5: Available forms and recommended doses of estradiol for adulta transfeminine people:
a Estradiol doses in pubertal adolescent transfeminine people should be lower to mimic estradiol exposure during normal female puberty (Aly, 2020). b May be advisable to use divided doses 2 to 4 times per day (i.e., once every 6 to 12 hours) instead of once per day (Sam, 2021). c This estradiol form achieves very low estradiol levels at typical doses that don’t appear to be well-suited for transfeminine hormone therapy (Aly, 2020; Graph). d Estradiol valerate contains about 75% of the same amount of estradiol as estradiol so doses are about 1.3-fold higher for the same estradiol levels (Aly, 2019; Sam, 2021). e Doses and intervals for estradiol undecylate are extrapolated and hypothetical (Aly, 2021). f A higher initial loading dose of e.g., 240 or 320 mg polyestradiol phosphate can be used for the first one or two injections to reach steady-state estradiol levels more quickly. However, this preparation has recently been discontinued and appears to no longer be available.
Additional informational resources are available in terms of estradiol levels (Wiki; Table) and approximate equivalent doses (Aly, 2020) with different forms, routes, and doses of estradiol.
There is high variability between individuals in the levels of estradiol achieved during estradiol therapy. That is, estradiol levels during treatment with the same dosage of estradiol can differ substantially between individuals. This variability is greatest with oral and transdermal estradiol but is also considerable even with injectable estradiol preparations and other estradiol forms. As such, estradiol doses are not absolute and should be individualized on a case-by-case basis in conjunction with blood work as a guide. It should also be noted that due to fluctuations in estradiol concentrations with certain routes, levels of estradiol can vary considerably from one blood test to another. This is most notable with sublingual estradiol and injectable estradiol. The fluctuations in estradiol levels with these routes are predictable and must be understood when interpreting blood work results. Differences in blood test results can be minimized with informed and consistent timing of blood draws.
If or when the gonads are surgically removed, testosterone suppression is no longer needed in transfeminine people. As a result, estradiol doses, if they are high or supraphysiological, can be lowered to more closely approximate normal physiological levels in cisgender women.
Progestogens
Progestogens include progesterone and progestins. Progestins are synthetic progestogens derived from structural modification of progesterone or testosterone. There are dozens of different progestins and these progestins can be divided into a variety of different structural classes with varying properties (Table). Examples of some major progestins of different classes include the 17α-hydroxyprogesterone derivative medroxyprogesterone acetate (MPA; Provera, Depo-Provera), the 19-nortestosterone derivative norethisterone (NET; many brand names), the retroprogesterone derivative dydrogesterone (Duphaston), and the 17α-spirolactone derivative drospirenone (Slynd, Yasmin). Progestins were developed because they have a more favorable disposition in the body than progesterone for use as medications. Only a few clinically used progestins have been used in transfeminine hormone therapy. However, progestogens largely produce the same progestogenic effects, with a few exceptions, and theoretically almost any progestogen could be employed.
Besides helping with testosterone suppression, progestogens are of no clear or known benefit for feminization or breast development in transfeminine people. While some transfeminine people anecdotally claim to experience improved breast development with progestogens, an involvement of progestogens in improving breast size or shape is controversial and is not supported by theory nor evidence at present (Wiki; Aly, 2020). It is possible that premature introduction of progestogens, particularly at high doses, could actually have an unfavorable influence on breast development (Aly, 2020). Many transfeminine people have also anecdotally claimed that progestogens have a beneficial effect on their sexual desire. However, a review of the literature by the present author found that neither progesterone nor progestins positively influence sexual desire in humans (Aly, 2020). Instead, the available evidence suggests either a neutral influence or an inhibitory effect of progestogens on sexual desire, although the latter may be specific only to high doses of progestogens (Aly, 2020). Claims have been made that progesterone may have beneficial effects on mood in transfeminine people as well, but clinical support for such notions is likewise lacking at this time (Coleman et al., 2022; Nolan et al., 2022). It is notable that progesterone at luteal-phase levels, due to its neurosteroid metabolites like allopregnanolone, actually appears to worsen mood in around 30% of cisgender women, and produces more overt negative reactions, which constitute the diagnoses of premenstrual syndrome (PMS) and premenstrual dysphoric disorder (PMDD), in around 2 to 10% of women (Bäckström et al., 2011; Edler Schiller, Schmidt, & Rubinow, 2014; Sundström-Poromaa et al., 2020). More research is needed to evaluate the possible beneficial effects of progestogens in transfeminine people.
Most clinically used progestogens have off-target activities in addition to their progestogenic activity, and these activities may be desirable or undesirable depending on the action in question (Kuhl, 2005; Stanczyk et al., 2013; Wiki; Table). Progesterone has a variety of neurosteroid as well as other activities that can result in central nervous system effects among others which are not shared by progestins. MPA as well as NET and its derivatives have weak androgenic activity, which is unfavorable in the context of transfeminine hormone therapy. NET and certain related progestins produce ethinylestradiol as a metabolite at high doses and hence can produce ethinylestradiol-like estrogenic effects, including increased risk of blood clots and associated cardiovascular problems. Other off-target actions of progestogens include antiandrogenic, glucocorticoid, and antimineralocorticoid activities. These actions can result in differences in therapeutic effectiveness (e.g., androgen suppression or blockade) as well as side effects and health risks. Some notable progestins without undesirable off-target activities (i.e., androgenic or glucocorticoid activity) include low-dose CPA, drospirenone (DRSP), dienogest, nomegestrol acetate (NOMAC), dydrogesterone, and hydroxyprogesterone caproate (OHPC). However, of these progestins, only CPA has been considerably used and studied in transfeminine people.
The addition of progestogens to estrogen therapy has been associated with a number of unfavorable health effects. These include increased risk of blood clots (Wiki; Aly, 2020), coronary heart disease (Wiki), and breast cancer (Wiki; Aly, 2020). High doses of progestogens are also associated with increased risk of certain non-cancerousbrain tumors including meningiomas and prolactinomas (Wiki; Aly, 2020). The coronary heart disease risk may be due to changes in blood lipids caused by the weak androgenic activity of certain progestogens, but the rest of the aforementioned risks are probably due to their progestogenic activity (Stanczyk et al., 2013; Jiang & Tian, 2017). Aside from health risks, progestogens have also been associated with adverse mood changes (Wiki; Wiki). However, besides the case of progesterone and its neurosteroid metabolites, these effects of progestogens are controversial and are not well-supported by evidence (Wiki; Wiki). Progestogens are otherwise generally well-tolerated and are regarded as producing little in the way of side effects.
In contrast to certain progestins, progesterone has no unfavorable off-target activities. Due to its lack of androgenic activity, progesterone has no adverse influence on blood lipids and is not expected to raise the risk of coronary heart disease. The addition of oral progesterone to estrogen therapy notably has not been associated with increased risk of blood clots (Wiki). In addition, oral progesterone seems to have less risk of breast cancer than progestins with short-term therapy, although this is notably not the case with longer-term exposure (Wiki; Aly, 2020). Consequently, it has been suggested that progesterone, for reasons that have yet to be fully elucidated, may be a safer progestogen than progestins and that it should be the preferred progestogen for hormone therapy in cisgender women and transfeminine people. However, there are also theoretical arguments against such notions. Oral progesterone is known to produce very low progesterone levels and to have only weak progestogenic effects at typical doses (Aly, 2018; Wiki). The seemingly better safety of oral progesterone may simply be an artifact of the low progesterone levels that occur with it, and hence of progestogenic dosage. Non-oral progesterone, at doses resulting in physiological and full progestogenic strength, has never been properly evaluated in terms of health outcomes, and may have similar risks as progestins (Aly, 2018; Wiki).
Due to their lack of known influence on feminization and breast development and their known and possible adverse effects and risks, progestogens are not routinely used in transfeminine hormone therapy at present. Major transgender health guidelines note the limitations of the available evidence on progestogens for transfeminine people and have mixed attitudes on their use, either explictly recommending against their use (Coleman et al., 2022—WPATH SOC8), taking a more neutral stance (Hembree et al., 2017—Endocrine Society guidelines), or being permissive of their use (Deutsch, 2016—UCSF guidelines). There is however a very major exception to the preceding in the form of CPA, an antiandrogen which is widely used in transfeminine hormone therapy to suppress testosterone production and which happens to be a powerful progestogen at the typical doses used in transfeminine people. CPA will be described below in the section on antiandrogens. Although progestogens have various health risks, cisgender women of course have progesterone, and the absolute risks of progestogens are very low in healthy young people. Risks like breast cancer also are exposure-dependent and take many years to develop. The testosterone suppression provided by progestogens can furthermore be very useful in transfeminine people, as is widely taken advantage of with CPA. Given these considerations, a limited duration of progestogen therapy in transfeminine people, for instance a few years to help suppress testosterone levels before surgical gonadal removal, may be considered quite acceptable.
Progesterone can be used in transfeminine people by oral administration, sublingual administration, rectal administration, or by intramuscular or subcutaneous injection (Wiki). Progestins are usually used via oral administration, but certain progestins are also available in injectable formulations (Wiki).
Oral Progesterone
Progesterone is most commonly taken orally. It is used by this route in the form of oil-filled capsules containing 100 or 200 mg micronized progesterone under brand names such as Prometrium, Utrogestan, and Microgest (Wiki). Despite its widespread use, levels of progesterone via oral administration have been found using state-of-the-art assays (LC–MS) to be very low (<2 ng/mL [<6.4 nmol/L] at 100 mg/day) and inadequate for satisfactory progestogenic effects in various areas (Aly, 2018; Wiki). In relation to this, even high doses of oral progesterone (400 mg/day) showed no antigonadotropic effect or testosterone suppression in cisgender men (Aly, 2018; Wiki). This is in major contrast to non-oral forms of progesterone and to progestins, which produce dose-dependent and robust testosterone suppression (Aly, 2019; Wiki). In addition to its low progestogenic potency, oral progesterone is excessively converted into neurosteroid metabolites like allopregnanolone and pregnanolone. These metabolites act as potent GABAA receptor positive allosteric modulators, and can produce undesirable alcohol-like side effects such as sedation, cognitive, memory, and motor impairment, and mood changes (Wiki; Wiki). As such, while inconvenient, non-oral routes are greatly preferable for progesterone.
Sublingual Progesterone
Sublingual progesterone tablets exist and are marketed under the brand name Luteina but today are only available in Poland and Ukraine (Wiki). Oral progesterone could theoretically be taken sublingually, analogously to sublingual use of oral estradiol. However, because oral progesterone is formulated as oil-filled capsules, this makes it difficult and unpleasant to use by sublingual administration. Buccal progesterone, which would be expected to have similar characteristics to those of sublingual progesterone, has been used in medicine in the past, but is no longer marketed today (Wiki).
Rectal Progesterone
Progesterone is approved for use by rectal administration in the form of suppositories under the brand name Cyclogest (Wiki). This product is marketed in only a limited number of countries however, although it is available in the United Kingdom (Wiki). While not approved for use by rectal administration, oral progesterone capsules can be taken rectally instead of orally, and using them in this way may allow for much higher progesterone levels than would be achieved by oral administration due to avoidance of most first-pass metabolism. Rectal administration of oral progesterone capsules has not been formally studied, but oral progesterone capsules have been administered vaginally in cisgender women with success (Miles et al., 1994; Wang et al., 2019), and the vaginal and rectal routes are said to have similar pharmacokinetics in general (Goletiani, Keith, & Gorsky, 2007; Wiki). Hence, there is good theoretical basis for rectal administration of oral progesterone capsules being an effective route of administration of progesterone. Whereas oral progesterone achieves very low levels of progesterone, rectal progesterone can readily achieve normal luteal-phase levels of progesterone (Wiki). Although inconvenient, rectal administration may be the overall best route of administration of progesterone for transfeminine people.
Injectable Progesterone
Progesterone by injection is available as an oil solution for intramuscular injection under brand names such as Proluton, Progestaject, and Gestone (Wiki) and as an aqueous solution for subcutaneous injection under the brand name Prolutex (Wiki). Oil solutions of progesterone for intramuscular injection are widely available, whereas the aqueous solution of progesterone for subcutaneous injection is available only in some European countries (Wiki). Injectable progesterone, regardless of route, has a relatively short duration and must be injected once every one to three days (Wiki; Wiki). This makes it too inconvenient to use for most people. Unlike with estradiol, progesterone esters with longer durations than progesterone itself by injection are not chemically possible as progesterone has no hydroxyl groups available for esterification (Wiki). Injectable aqueous suspensions of microcrystalline progesterone were previously marketed and had a duration of 1 to 2 weeks, but these preparations were associated with pain at the injection site and were eventually discontinued (Aly, 2019; Wiki).
Other Progesterone Routes
Other progesterone routes, such as transdermal progesterone and subcutaneous progesterone pellets, are also known, but are not available as pharmaceutical drugs and are little-used medically (Wiki). This is related to the low potency of progesterone and difficulty achieving progesterone levels high enough for adequate therapeutic effects with these routes (Wiki; Wiki). In addition, progesterone pellets tend to be extruded at high rates (Wiki). In any case, certain compounding pharmacies may make forms of progesterone that could be used by these routes.
Oral and Injectable Progestins
Most progestins are taken orally in the form of solid tablets (Wiki). In contrast to progesterone, progestins, owing to their synthetic nature, are resistant to metabolism in the intestines and liver and have high oral bioavailability. In addition, unlike the case of the estrogen receptors, the progesterone receptors are expressed minimally or not at all in the liver, and there is no known first pass influence of progestogenic activity on liver synthesis (Lax, 1987; Stanczyk, Mathews, & Cortessis, 2017). As a result, there are no apparent problems with oral administration in the case of purely progestogenic progestins. However, some progestins have liver-impacting off-target hormonal actions, such as androgenic, estrogenic, and/or glucocorticoid activity, and this can result in adverse effects like unfavorable lipid changes or procoagulation—which may be augmented by the first pass with oral administration.
A selection of progestins are available in injectable formulations, including for intramuscular or subcutaneous injection (Wiki). Some of the more notable ones include medroxyprogesterone acetate (MPA), norethisterone enanthate (NETE), hydroxyprogesterone caproate (OHPC), and algestone acetophenide (dihydroxyprogesterone acetophenide; DHPA) (Wiki). In addition to being used alone, injectable progestins are used together with estradiol esters in combined injectable contraceptives (Wiki). These preparations are often used as a means of hormone therapy by transfeminine people in Latin America. Whereas injectable progesterone has a duration measured in days, injectable progestins have durations ranging from weeks to months, and can be injected much less often in comparison (Table).
Additional Notes
Table 6: Available forms and recommended doses of progestogens for transfeminine people:
For progesterone levels with different forms, routes, and doses of progesterone, see the table here (only LC–MS and IA + CS assays for oral progesterone) and the graphs here.
As with estradiol, there is high variability between individuals in progesterone levels. Conversely, there is less variability between individuals in the case of progestins.
After removal of the gonads, progestogen doses can be lowered or adjusted to approximate normal female physiological exposure or they can be discontinued entirely.
Antiandrogens
Aside from estrogens and progestogens, there is another class of hormonal medications used in transfeminine hormone therapy known as antiandrogens (AAs). These medications reduce the effects of androgens in the body by either decreasing androgen production and thereby lowering androgen levels or by directly blocking the actions of androgens. They work via a variety of different mechanisms of action, and include androgen receptor antagonists, antigonadotropins, and androgen synthesis inhibitors.
Androgen receptor antagonists act by directly blocking the effects of androgens, including testosterone, DHT, and other androgens, at the level of their biological target. They bind to the androgen receptor without activating it, thereby displacing androgens from the receptor. Due to the nature of their mechanism of action as competitive blockers of androgens, the antiandrogenic efficacy of androgen receptor antagonists is both highly dose-dependent and fundamentally dependent on testosterone levels. They do not act by lowering testosterone levels, although some androgen receptor antagonists may have additional antiandrogenic actions that result in decreased testosterone levels. Because androgen receptor antagonists do not work by lowering testosterone levels, blood work can be less informative for them compared to antiandrogens that suppress testosterone levels. Androgen receptor antagonists include steroidal antiandrogens (SAAs) like spironolactone (Aldactone) and cyproterone acetate (CPA; Androcur) and nonsteroidal antiandrogens (NSAAs) like bicalutamide (Casodex).
Antigonadotropins suppress the gonadal production of androgens by inhibiting the GnRH-mediated secretion of gonadotropins from the pituitary gland. They include estrogens and progestogens. In addition, GnRH agonists such as leuprorelin (Lupron) and GnRH antagonists such as elagolix (Orilissa) act similarly and could likewise be described as antigonadotropins.
Androgen synthesis inhibitors inhibit the enzyme-mediated synthesis of androgens. They include 5α-reductase inhibitors (5α-RIs) like finasteride (Propecia) and dutasteride (Avodart). There are also other types of androgen synthesis inhibitors, for instance potent 17α-hydroxylase/17,20-lyase inhibitors like ketoconazole (Nizoral) and abiraterone acetate (Zytiga). However, these agents have limitations (e.g., toxicity, high cost, and lack of experience) and have not been used in transfeminine hormone therapy.
Although antigonadotropins and androgen synthesis inhibitors have antiandrogenic effects secondary to decreased androgen levels, they are not usually referred to as “antiandrogens”. Instead, this term is most commonly reserved to refer specifically to androgen receptor antagonists. However, antigonadotropins and androgen synthesis inhibitors may nonetheless be described as antiandrogens as well.
After removal of the gonads, antiandrogens can be discontinued. If unwanted androgen-dependent symptoms, such as acne, seborrhea, or scalp hair loss, persist despite full suppression or ablation of gonadal testosterone, then a lower dose of an androgen receptor antagonist, such as 100 to 200 mg/day spironolactone or 12.5 to 25 mg/day bicalutamide, can be continued to treat these symptoms.
Table 7: Available forms and recommended doses of antiandrogens for transfeminine people:
a For CPA, this dose range is specifically one-quarter of a 10-mg tablet to one full 10-mg tablet per day (2.5–10 mg/day) or a quarter of a 50-mg tablet every other day or every 2 to 3 days (4.2–12.5 mg/day). A dosage of 5–10 mg/day or 6.25–12.5 mg/day is likely to ensure maximal testosterone suppression, while lower doses may be less effective (Aly, 2019). b For spironolactone and bicalutamide, it is assumed that testosterone levels are substantially suppressed (≤200 ng/dL [<6.9 nmol/L]). If testosterone levels are not suppressed to this range, then higher doses may be warranted. c Spironolactone and its metabolites have relatively short half-lives, and twice-daily administration in divided doses (e.g., 100–200 mg twice per day) is recommended.
Figure 3: Suppression of gonadal testosterone production and circulating testosterone levels (ng/dL) with estradiol in combination with different antiandrogens over one year of hormone therapy in transfeminine people (Sofer et al., 2020). The estradiol forms included oral tablets 2–8 mg/day, transdermal gel 2.5–5 mg/day, and transdermal patches 50–200 μg/day. The antiandrogens included spironolactone 50–200 mg/day (n=16), cyproterone acetate (n=41), and GnRH agonists (specifically triptorelin 3.75 mg/month or goserelin 3.6 mg/month by injection) (n=10) (Sofer et al., 2020). It should be noted that lower doses of cyproterone acetate (10–12.5 mg/day) show equal testosterone suppression to higher doses (25–100 mg/day) and higher doses should no longer be used (Aly, 2019). The dashed horizontal line corresponds to the upper limit of the normal female range for testosterone levels.
As an antiandrogen, CPA has a dual mechanism of action of suppressing testosterone levels via its progestogenic and hence antigonadotropic activity and of acting as an androgen receptor antagonist (Aly, 2019). The progestogenic activity of CPA is of far greater potency than its androgen receptor antagonism however (Aly, 2019). The dose of CPA used as a progestogen in cisgender women is about 2 mg per day, which produces similar progestogenic effects to those of physiological luteal-phase levels of progesterone (e.g., suppression of gonadotropin secretion, ovulation inhibition, and endometrial transformation and protection) (Aly, 2019). Conversely, much higher doses of CPA of 50 to 300 mg/day have typically been used for androgen-dependent indications (Aly, 2019). These high doses of CPA result in profound progestogenic overdosage and associated side effects and risks (Aly, 2019). In transfeminine people, CPA has historically been used at doses of 50 to 150 mg/day (Aly, 2019). However, CPA doses have dramatically fallen in recent years, and today doses of no more than 10 to 12.5 mg/day are recommended (Aly, 2019; Coleman et al., 2022—WPATH SOC8). These lower doses of CPA still produce strong progestogenic effects, and in combination with estradiol, are equally effective as higher doses in suppressing testosterone levels (Aly, 2019; Meyer et al., 2020; Even Zohar et al., 2021; Kuijpers et al., 2021; Coleman et al., 2022). Even lower doses of CPA, for instance 5 to 6.25 mg/day, are currently being studied, and may still be fully effective (Aly, 2019).
Given by itself without estrogen, CPA typically suppresses testosterone levels in people with testes by about 50 to 70%, down to about 150 to 300 ng/dL (5.2–10.4 nmol/L) (Meriggiola et al., 2002; Toorians et al., 2003; Giltay et al., 2004; T’Sjoen et al., 2005; Tack et al., 2017; Zitzmann et al., 2017; Aly, 2019). Lower doses of CPA alone (e.g., 10 mg/day) show the same degree of testosterone suppression as higher doses of CPA alone (e.g., 50–100 mg/day), indicating that the antigonadotropic effects of CPA are maximal at relatively low therapeutic doses of this medication (Aly, 2019). This is on the order of about 5 to 10 times the ovulation-inhibiting dosage of CPA in cisgender women, a dose–response relationship that has also been observed with a number of other progestogens (Aly, 2019). Per the preceding, CPA alone, regardless of dosage, is unable to reduce testosterone levels into the normal female range (<50 ng/dL [<1.7 nmol/L]). But when CPA is combined with estradiol, even at relatively small doses of estradiol, it consistently suppresses testosterone levels into the normal female range (Aly, 2019; Angus et al., 2019; Gava et al., 2020; Sofer et al., 2020; Collet et al., 2022). However, it appears that a certain minimum level of estradiol, perhaps around 60 pg/mL (220 pmol/L) on average, is required for this to occur (Aly, 2019). Estradiol levels lower than this threshold in those taking CPA, which can occasionally be encountered in transfeminine people due to estradiol being dosed too low, have the potential to compromise full testosterone suppression (Aly, 2019).
In addition to testosterone suppression, CPA can dose-dependently block the androgen receptor (Aly, 2019). However, relatively high doses of CPA are needed to considerably antagonize the androgen receptor (e.g., 50–300 mg/day), and lower doses (e.g., ≤12.5 mg/day) may not be able to do this to a meaningful degree (Aly, 2019). As such, lower doses of CPA may essentially be purely progestogenic, with minimal or no androgen receptor antagonism. In this regard, referring to CPA at such doses as an “antiandrogen”—rather than as a “progestogen”—may be considered somewhat of a misnomer. Higher doses of CPA (>12.5 mg/day) can no longer be considered safe due to the massive progestogenic overdosage that occurs with them, and should no longer be used in transfeminine people. Moreover, as testosterone levels are usually suppressed into the normal female range in transfeminine people taking estradiol plus CPA, there is no actual need for any additional androgen receptor blockade (Aly, 2019).
CPA has been reported to produce various side effects. Some of these side effects include fatigue and a degree of weight gain (Belisle & Love, 1986; Hammerstein, 1990; Martinez-Martin et al., 2022). CPA might be able to produce a magnitude of sexual dysfunction (e.g., reduced sexual desire) beyond that expected with testosterone suppression alone (Wiki; Aly, 2019). It may also have a small risk of depressive mood changes (Wiki). In transfeminine people, CPA has been documented to produce pregnancy-like breast changes (i.e., lobuloalveolar development of the mammary glands) (Kanhai et al., 2000). In relation to this, CPA sometimes causes lactation as a side effect (Gooren, Harmsen-Louman, & van Kessel, 1985; Schlatterer et al., 1998; Bazarra-Castro, 2009). Concerns have been raised about premature introduction of progestogens—particularly at high doses like with CPA—and possible adverse influence on breast development (Aly, 2020). However, little data exists in humans to substantiate such concerns at present. The side effects of CPA are assumed to be dose-dependent, and using the lowest effective doses is expected to minimize its side effects.
CPA is usually taken orally in the form of tablets (e.g., 10, 50, and 100 mg) (Wiki). Under the brand name Androcur Depot, it is also available as a long-lasting 300 mg depot injectable in some countries (Wiki). However, this formulation is not commonly used in transfeminine people, and happens to correspond to very high doses in terms of CPA exposure. A pill cutter (Amazon) can be used to split CPA tablets and achieve lower doses (e.g., 12.5 mg doses with 50-mg tablets). CPA has a relatively long elimination half-life of about 1.6 to 4.3 days (Wiki; Aly, 2019). As such, it can be taken once daily, or even as infrequently as once every 2 or 3 days, if needed (Aly, 2019). In addition to splitting of CPA tablets, dosing CPA once every 2 or 3 days can also be useful for achieving lower doses (Aly, 2019).
As already described, CPA is a powerful progestogen even at the relatively low doses now used in transfeminine people (e.g., 5–12.5 mg/day). As such, there is no need, nor point, in adding another progestogen, for instance progesterone, in those who are taking CPA—at least if the goal of doing so is to produce progestogenic effects. This is something that is often overlooked in people taking CPA, and can result in increased costs, side effects, and inconvenience without any expected benefit.
Spironolactone
Spironolactone (Aldactone) is an antiandrogen and antimineralocorticoid. It is widely used as an antiandrogen in cisgender women for treatment of androgen-dependent hair and skin conditions like acne, hirsutism (excessive facial/body hair growth), and scalp hair loss, in cisgender women for treatment of hyperandrogenism (high androgen levels) due to polycystic ovary syndrome (PCOS), and in transfeminine people as a component of hormone therapy. Spironolactone is particularly widely used in transfeminine people in the United States, where it is the most commonly used antiandrogen in this population. As an antimineralocorticoid, the original and primary use of spironolactone in medicine, it is used to treat heart failure, high blood pressure, high mineralocorticoid levels, low potassium levels, and conditions of excess fluid retention like nephrotic syndrome and ascites, among others (Wiki). In terms of its antiandrogenic actions, spironolactone is a relatively weak androgen receptor antagonist as well as a weak androgen synthesis inhibitor (Wiki). The androgen synthesis inhibition of spironolactone is mediated specifically via inhibition of 17α-hydroxylase and 17,20-lyase (Wiki). Spironolactone does not appear to have meaningful progestogenic activity, 5α-reductase inhibition, or direct estrogenic activity (Wiki). However, indirect estrogenic effects secondary to its antiandrogenic activity (e.g., breast development and feminization) can occur with it at sufficiently high doses (Wiki).
Spironolactone shows limited and highly inconsistent effects on testosterone levels in clinical studies in cisgender men, cisgender women, and transfeminine people, with most studies finding no change in levels, some studies finding a decrease in levels, and a small number even finding an increase in levels (Aly, 2018). In spite of this, studies commonly find that spironolactone still produces antiandrogenic effects even when androgen levels remain unchanged. Hence, the primary mechanism of action of spironolactone as an antiandrogen appears to be androgen receptor blockade. In relation to this, in transfeminine people taking spironolactone as an antiandrogen, the estrogen component of the regimen is likely to be the main or possibly sole agent suppressing testosterone production. This is in part based on studies in transfeminine people comparing estradiol plus spironolactone to estradiol alone (e.g., Leinung, 2014; Leinung, Feustel, & Joseph, 2018; Angus et al., 2019) and on studies comparing testosterone levels with different doses of spironolactone (e.g., Liang et al., 2018; SoRelle et al., 2019; Allen et al., 2021). Due to the minimal influence of spironolactone on testosterone production, testosterone levels are not usually suppressed into the female range in transfeminine people taking estradiol plus spironolactone, with testosterone levels often remaining well above this range (e.g., 50–450 ng/dL [1.7–15.6 nmol/L] on average) (Leinung, 2014; Leinung, Feustel, & Joseph, 2018; Liang et al., 2018; Angus et al., 2019; Jain, Kwan, & Forcier, 2019; SoRelle et al., 2019; Sofer et al., 2020; Burinkul et al., 2021). However, testosterone levels do tend to decline gradually over time in transfeminine people on this regimen (e.g., Liang et al., 2018; Sofer et al., 2020 (Graph); Allen et al., 2021).
Due to its relatively weak androgen receptor antagonism, spironolactone is likely best-suited for blocking female-range or somewhat-higher testosterone levels (e.g., <100 ng/dL [<3.5 nmol/L]) (Aly, 2018). This is based on clinical dose-ranging studies of spironolactone (typically using 50–200 mg/day) in healthy cisgender women and cisgender women with PCOS (Goodfellow et al., 1984; Lobo et al., 1985; Hammerstein, 1990; James, Jamerson, & Aguh, 2022) as well as comparative studies of spironolactone against the more-potent antiandrogen flutamide (Cusan et al., 1994; Erenus et al., 1994; Shaw, 1996). The clinical antiandrogenic efficacy of spironolactone has been very limitedly assessed in transfeminine people to date, and is largely unknown (Angus et al., 2021). In any case, the antiandrogenic efficacy of spironolactone in cisgender women with androgen-dependent hair and skin conditions is well-established, and the medication thus does appear to be effective so long as testosterone levels are not too high (Brown et al., 2009; van Zuuren & Fedorowicz, 2016; Layton et al., 2017; Barrionuevo et al., 2018; James, Jamerson, & Aguh, 2022). In addition, higher doses of spironolactone (e.g., 300–400 mg/day) may be more useful for blocking higher testosterone levels in transfeminine people, and are allowed for by transgender care guidelines (Aly, 2020).
Consequent to spironolactone’s limited and inconsistent influence on testosterone levels and its relatively weak androgen receptor antagonism, estradiol plus spironolactone regimens will likely not be fully effective in terms of testosterone suppression for many transfeminine people. This is liable to result in suboptimal demasculinization, feminization, and breast development in these individuals. Other antiandrogenic approaches, such as bicalutamide, CPA, GnRH modulators, and high-dose estradiol monotherapy, will likely be more effective in these cases owing either to their ability to more potently block androgens or their capacity to reliably reduce testosterone levels into the female range. If testosterone levels are still too high with estradiol plus spironolactone, a switch to a different antiandrogen, increasing to a higher dosage of estradiol, or addition of a clinically antigonadotropic progestogen (e.g., non-oral progesterone or a progestin) should be considered.
Spironolactone is a strong antimineralocorticoid, or antagonist of the mineralocorticoid receptor, the biological target of the mineralocorticoid steroid hormones aldosterone and 11-deoxycorticosterone. This is an action that spironolactone shares with progesterone, although spironolactone is a much more potent antimineralocorticoid than progesterone. The mineralocorticoid receptor is involved in regulating electrolyte and fluid balances, among other roles. Spironolactone is associated with modestly lowered blood pressure, which may be considered a beneficial effect of its antimineralocorticoid activity (Martinez-Martin et al., 2022). Although spironolactone is usually well-tolerated, it can sometimes produce antimineralocorticoid side effects such as excessively lowered blood pressure, dizziness, fatigue, urinary frequency, and increased cortisol levels, among others (Kellner & Wiedemann, 2008; Kim & Del Rosso, 2012; Zaenglein et al., 2016; Layton et al., 2017; James, Jamerson, & Aguh, 2022). It has been argued by some in the online transgender community that spironolactone, via its antimineralocorticoid activity and increased cortisol levels, may increase visceral fat in transfeminine people (Aly, 2020). However, evidence does not support this hypothetical side effect at present (Aly, 2020). Available data also do not support spironolactone stunting breast development in transfeminine people or producing serious neuropsychiatric side effects, such as prominent depressive mood changes.
In people who are at-risk for hyperkalemia, dietary restriction to limit intake of potassium-rich foods is often recommended (Roscioni et al., 2012; Cupisti et al., 2018). This is often encountered in transgender health as transfeminine people being told “not to eat bananas”, which are said to be high in potassium. However, limiting dietary potassium with spironolactone to avoid hyperkalemia is theoretical and not actually evidence-based, with data so far contradicting its efficacy (St-Jules, Goldfarb, & Sevick, 2016; St-Jules & Fouque, 2021; Babich, Kalantar-Zadeh, & Joshi, 2022; St-Jules & Fouque, 2022). As such, routine restriction of dietary potassium with spironolactone may not be warranted.
Aside from its antimineralocorticoid activity, spironolactone has been reported to increase levels of LDL (“bad”) cholesterol levels and to decrease levels of HDL (“good”) cholesterol in women with PCOS (Nakhjavani et al., 2009). However, findings appear to be conflicting, with other studies not finding unfavorable influences on cholesterol levels with spironolactone (Polyzos et al., 2011). Long-term, adverse effects on cholesterol levels could result in an increase in the risk of coronary heart disease.
Spironolactone is taken orally in the form of tablets (e.g., 25, 50, and 100 mg) (Wiki). It is a prodrug of several active metabolites, including 7α-thiomethylspironolactone, 6β-hydroxy-7α-thiomethylspironolactone, and canrenone (7α-desthioacetyl-δ6-spironolactone) (Wiki). Spironolactone and these active metabolites have elimination half-lives of 1.4 hours, 13.8 hours, 15.0 hours, and 16.5 hours, respectively (Wiki). Due to the relatively short duration of elevated drug levels with spironolactone and its active metabolites (Graph), twice-daily administration of spironolactone in divided doses may be more optimal than once-daily intake and is advised (Reiter et al., 2010).
Bicalutamide
Bicalutamide (Casodex) is a nonsteroidal antiandrogen (NSAA) which acts as a potent and highly selective androgen receptor antagonist (Wiki). It is primarily used in the treatment of prostate cancer in cisgender men. Prostate cancer is an androgen-dependent cancer which antiandrogens can help to slow the progression of, and this use constitutes the vast majority of prescriptions for bicalutamide (Wiki). In addition to prostate cancer, although to a much lesser extent, bicalutamide has been used in the treatment of hirsutism (excessive facial/body hair growth), scalp hair loss, and polycystic ovary syndrome (PCOS) in cisgender women, peripheral or gonadotropin-independent precocious puberty (a rare form of precocious puberty in which antigonadotropins such as GnRH agonists are not effective) in cisgender boys, and priapism in cisgender men (Wiki). Bicalutamide is also becoming increasingly adopted for use as an antiandrogen in transfeminine people (Aly, 2020; Wiki). However, its use in transgender health is still very limited, and well-regarded transgender care guidelines either recommend against its use (Deutsch, 2016—UCSF guidelines; Coleman et al., 2022—WPATH SOC8) or are only cautiously permissive of its use (Thompson et al., 2021—Fenway Health guidelines). This is due to a lack of studies of bicalutamide in transfeminine people and its potential risks. Nonetheless, a small but growing number of clinicians are using bicalutamide in transfeminine people or are willing to prescribe it, with these clinicians located particularly in the United States. A single small clinical study has assessed bicalutamide in transfeminine people so far, specifically as a puberty blocker in 13 transfeminine adolescents who were denied insurance coverage for GnRH agonists (Neyman, Fuqua, & Eugster, 2019). (Update: More studies of bicalutamide in transfeminine people have since been published, see Aly (2020).)
Bicalutamide is a much more potent androgen receptor antagonist than either spironolactone or CPA (Wiki; Neyman, Fuqua, & Eugster, 2019). It is typically used in transfeminine people at a dosage of 25 to 50 mg/day, although this dosage has been arbitrarily selected and is not based on clinical data. Nonetheless, due to its relatively high potency as an androgen receptor antagonist and concomitant suppression of testosterone levels by estradiol, these doses may be adequate for testosterone blockade for many transfeminine people. At higher doses (>50 mg/day), bicalutamide is able to substantially block male-range testosterone levels (>300 ng/dL [>10.4 nmol/L]) based on studies of bicalutamide monotherapy in cisgender men with prostate cancer (Wiki). This is something that spironolactone and CPA are not capable of in the same way. Owing to its selectivity for the androgen receptor, bicalutamide has no off-target hormonal activity and produces almost no side effects in women (Wiki; Erem, 2013; Moretti et al., 2018). The only apparent side effect of bicalutamide in a rigorous clinical trial of the drug for hirsutism in cisgender women was significantly increased total and LDL (“bad”) cholesterol levels (Moretti et al., 2018). Hence, bicalutamide tends to be very well-tolerated. The relative lack of side effects with bicalutamide is contrast in to other antiandrogens like spironolactone and CPA, which are not pure androgen receptor antagonists and have off-target hormonal actions like antimineralocorticoid activity or strong progestogenic activity with consequent side effects and risks.
As a selective androgen receptor antagonist, bicalutamide taken by itself does not decrease testosterone production or levels but rather increases them (Wiki). This is due to a loss of androgen receptor-mediated negative feedback on gonadotropin secretion and a consequent compensatory upregulation of gonadal testosterone production (Wiki). Bicalutamide more than blocks the effects of any increase in testosterone it causes, and in fact fundamentally cannot increase testosterone levels more than it can block them (Wiki). In addition, increases in testosterone levels with bicalutamide will be blunted or abolished if it is combined with an adequate dose of an antigonadotropin such as estradiol (Wiki; Wiki). Since estradiol is made from testosterone in the body, bicalutamide taken alone also preserves and increases estradiol production and levels (Wiki). Because of this, although bicalutamide has no other important intrinsic hormonal activity besides its antiandrogenic activity, it produces robust indirect estrogenic effects including feminization and breast development even when it is not combined with estrogen (Wiki; Wiki; Neyman, Fuqua, & Eugster, 2019). This has important implications for the use of bicalutamide as a puberty blocker in transfeminine adolescents, as bicalutamide does not actually block puberty like conventional puberty blockers (GnRH agonists) but instead has the effect of dose-dependently converting male puberty into female puberty (Wiki; Neyman, Fuqua, & Eugster, 2019).
Bicalutamide has certain health risks, which has been a major reason that it has not been more readily adopted in transfeminine hormone therapy (Aly, 2020). It has a small risk of liver toxicity (Wiki; Aly, 2020) and of lung toxicity (Wiki). Abnormal liver function tests (LFTs), such as elevated liver enzymes and elevated bilirubin, occurred in about 3.4% of men with bicalutamide monotherapy plus standard care versus 1.9% of men with placebo plus standard care in the Early Prostate Trial (EPC) clinical programme after 3.0 years of follow-up (Wiki). In clinical trials, treatment with bicalutamide had to be discontinued in about 0.3 to 1.5% of men due to LFTs that became too highly elevated and could have progressed to serious liver toxicity (Wiki). To date, there are around 10 published case reports of serious liver toxicity, including cases of death, with bicalutamide, all of which have been in men with prostate cancer (Wiki; Table; Aly, 2020). There have also been a few unpublished reports of serious liver toxicity including deaths with bicalutamide in transfeminine people (Aly, 2020). However, these reports have not been confirmed, and they may or may not be reliable. In addition to the preceding reports, hundreds of additional instances of liver complications in people taking bicalutamide exist in the United States FDA Adverse Event Reporting System (FAERS) database (Wiki; FDA). Abnormal LFTs with bicalutamide usually occur within the first 3 to 6 months of treatment (Kolvenbag & Blackledge, 1996; Casodex FDA Label), and all case reports of liver toxicity with bicalutamide have had an onset of less than 6 months (Table). The liver toxicity of bicalutamide is not known to be dose-dependent across its clinically used dose range (Wiki). Abnormal LFTs have occurred with bicalutamide (at rates of 2.9% to 11.4%) even at relatively low doses in cisgender women (e.g., 10–50 mg/day) (de Melo Carvalho, 2022). Due to its risk of liver toxicity, periodic liver monitoring is strongly advised with bicalutamide, especially within the first 6 months of treatment. Possible signs of liver toxicity include nausea, vomiting, abdominal pain, fatigue, appetite loss, flu-like symptoms, dark urine, and jaundice (yellowing of the skin/eyes) (Wiki).
In terms of its lung toxicity risk, bicalutamide has been associated rarely with interstitial pneumonitis, which can lead to pulmonary fibrosis and can be fatal, and also less often with eosinophilic lung disease (Wiki; Table). As of writing, 15 published case reports of interstitial pneumonitis and 2 case reports of eosinophilic lung disease in association with bicalutamide therapy exist, likewise all in men with prostate cancer (Table). As with liver toxicity, hundreds of additional cases of interstitial pneumonitis in people taking bicalutamide exist in the United States FAERS database (Wiki; FDA). It has been estimated that interstitial pneumonitis with bicalutamide occurs at a rate of around 1 in 10,000 people, although this may be an underestimate due to under-reporting (Wiki; Ahmad & Graham, 2003). Asian people may be especially likely to experience lung toxicity with bicalutamide and other NSAAs, as much higher incidences have been observed in this population (Mahler et al., 1996; Wu et al., 2022). There is no laboratory test for routine monitoring of lung changes with bicalutamide. Possible signs of relevant lung toxicity include dyspnea (difficulty breathing or shortness of breath), coughing, and pharyngitis (inflammation of the throat, typically manifesting as sore throat) (Wiki).
Aside from liver and lung toxicity, bicalutamide monotherapy has been found in cisgender men with prostate cancer to increase the risk of death due to causes other than prostate cancer (Iversen et al., 2004; Iversen et al., 2006; Wellington & Keam, 2006; Jia & Spratt, 2022; Wiki). This led to marketing authorization of bicalutamide for treatment of the earliest stage of prostate cancer being revoked and to the drug being abandoned for this use (Wiki). Bicalutamide remains approved and used for treatment of later stages of prostate cancer, as the antiandrogenic benefits of bicalutamide against prostate cancer outweigh any adverse influence it has on non-prostate-cancer mortality in these more severe stages. The mechanisms underlying the increase in risk of death with bicalutamide in men are unknown (Wiki). It is also unclear whether bicalutamide could likewise increase the risk of death in transfeminine people. Limitations of generalizing these studies to transfeminine people include the men in the trials being relatively old and ill, a relatively high dosage of bicalutamide (150 mg/day) being used in the trials for an extended duration (e.g., 5 years), the question of whether the risks were due to androgen deprivation or to specific drug-related toxicity of bicalutamide, and estradiol levels with bicalutamide monotherapy in men with prostate cancer being only about 30 to 50 pg/mL (110–184 pmol/L) (Wiki). The preceding estradiol levels are well above castrate levels and are sufficient for a substantial degree of estrogenic effect, but are nonetheless below those recommended for transfeminine people and potentially needed for full sex-hormone replacement (which are ≥50 pg/mL [≥184 pmol/L]). In any case, as the specific mechanisms underlying the increased mortality risk with bicalutamide seen in men with prostate cancer are uncertain, and as clinical safety data showing that the risk does not generalize do not exist, it remains a possibility that bicalutamide could also increase the risk of death in transfeminine people.
Bicalutamide is taken orally in the form of tablets (e.g., 50 and 150 mg) (Wiki). Due to saturation of absorption in the gastrointestinal tract, the oral bioavailability of bicalutamide progressively starts to decrease above a dosage of about 150 mg/day, and there is no further increase in bicalutamide levels above 300 mg/day (Wiki; Graph). Bicalutamide has a very long elimination half-life of about 6 to 10 days (Wiki; Graphs). As a result, it does not necessarily have to be taken daily, and can be dosed less often (in proportionally higher doses)—for instance twice weekly or even once weekly—if this is more convenient or otherwise desired. Due to its long half-life, bicalutamide requires about 4 to 12 weeks to fully reach steady-state levels (Wiki; Graph; Wiki). However, about 50% of steady state is reached within 1 week of administration of bicalutamide, and about 80 to 90% of steady state is reached after 3 to 4 weeks (Wiki; Graph; Wiki). Loading doses of bicalutamide can be taken to reach steady state more quickly if desired. Animal studies originally suggested that bicalutamide did not cross the blood–brain barrier and hence was peripherally selective (i.e., did not block androgen receptors in the brain) (Wiki). However, subsequent clinical studies found that this was not similarly the case in humans, in whom bicalutamide shows clear and robust centrally mediated antiandrogenic effects (Wiki).
Older NSAAs related to bicalutamide like flutamide (Eulexin) and nilutamide (Anandron, Nilandron) have much greater risks in comparison to bicalutamide and should not be used in transfeminine people. Nilutamide was previously characterized as an antiandrogen in transfeminine people in several studies, but was not further pursued probably due to its very high incidence of lung toxicity and other side effects (Aly, 2020; Wiki; Wiki). Flutamide has been used limitedly as an antiandrogen in transfeminine people in the past, but should no longer be used due to a much higher risk of liver toxicity than bicalutamide as well as other side effects and drawbacks (Aly, 2020; Wiki). Other newer and more-potent NSAAs like enzalutamide (Xtandi), apalutamide (Erleada), and darolutamide (Nubeqa) also have risks and have been studied and used little outside of prostate cancer to date.
5α-Reductase Inhibitors
Testosterone is converted into DHT within certain tissues in the body (Swerdloff et al., 2017). DHT is an androgen metabolite of testosterone with several-fold higher activity than testosterone. The transformation of testosterone into DHT is mediated by the enzyme 5α-reductase. The tissues in which 5α-reductase is present and testosterone is converted into DHT are limited but most importantly include the skin, hair follicles, and prostate gland. Although DHT is more potent than testosterone, it is thought to have minimal biological role as a circulating hormone (Horton, 1992; Swerdloff et al., 2017). Instead, testosterone serves as the main circulating androgen, and the role of DHT is thought to be mainly via local metabolism and potentiation of testosterone into DHT within certain tissues.
5α-Reductase inhibitors (5α-RIs), such as finasteride (Proscar, Propecia) and dutasteride (Avodart), inhibit 5α-reductase and thereby block the conversion of testosterone into DHT. This results in marked decreases in circulating and within-tissue levels of DHT. Due to the primary role of DHT as a mediator in tissues rather than as circulating hormone, the antiandrogenic efficacy of 5α-RIs is limited. This is evidenced by the fact that they are well-tolerated in cisgender men and do not cause notable demasculinization in these individuals (Hirshburg, 2016). The medical use of 5α-RIs is mainly restricted to the treatment of scalp hair loss in men and women, hirsutism (excessive facial/body hair) in women, and prostate enlargement in men. They might also be useful for acne in women, but evidence of this is very limited (Wiki). Due to their specificity, 5α-RIs are inappropriate as general antiandrogens in transfeminine people. Moreover, DHT levels decrease in tandem with testosterone levels with suppression of testosterone production in transfeminine hormone therapy, and routine use of 5α-RIs in transfeminine people with testosterone levels within the female range is of limited usefulness and can be considered unnecessary (Gooren et al., 2016; Irwig, 2020; Prince & Safer, 2020; Glintborg et al., 2021). In any case, 5α-RIs may be useful in transfeminine people on hormone therapy who have persistent body hair growth or scalp hair loss—as they have been shown to be in cisgender women (Barrionuevo et al., 2018; Prince & Safer, 2020). However, it is notable that evidence of effectiveness in cisgender women is better for androgen receptor antagonists for such indications (van Zuuren et al., 2015). This is intuitive as androgen receptor antagonists block both testosterone and DHT whereas 5α-RIs only prevent conversion of testosterone into DHT. Hence, although 5α-RIs strongly reduce or eliminate DHT and their net effect is antiandrogenic, they do not decrease testosterone levels and in fact increase them.
There are three subtypes of 5α-reductase. Dutasteride inhibits all three subtypes of 5α-reductase whereas finasteride only inhibits two of the subtypes. As a result of this, dutasteride is a more complete 5α-RI than finasteride. Dutasteride decreases DHT levels in the blood by up to 98% while finasteride can only decrease them by around 65 to 70%. As nearly all circulating DHT originates from synthesis in peripheral tissues, these decreases indicate parallel reductions in tissue DHT production (Horton, 1992). In accordance with these findings, dutasteride has been found to be more effective than finasteride in the treatment of scalp hair loss in men (Zhou et al., 2018; Dhurat et al., 2020; Wiki). For these reasons, although both finasteride and dutasteride are effective 5α-RIs, dutasteride may be the preferable choice if a 5α-RI is used (Zhou et al., 2018; Dhurat et al., 2020).
A potentially undesirable effect of 5α-RIs in transfeminine people is that they may increase circulating testosterone levels to a degree in those in whom testosterone production isn’t fully suppressed (Leinung, Feustel, & Joseph, 2018; Aly, 2019; Traish et al., 2019; Irwig, 2020; Glintborg et al., 2021). It appears that DHT adds significantly to negative feedback on gonadotropin secretion in the pituitary gland in people with testes who have low testosterone levels relative to the normal male range (Traish et al., 2019). The therapeutic implications of this for transfeminine people, if any, are uncertain.
Clinical dose-ranging studies have found that lower doses of finasteride and dutasteride than are typically used still provide substantial or near-maximal 5α-reductase inhibition (Gormley et al., 1990; Vermeulen et al., 1991; Sudduth & Koronkowski, 1993; Drake et al., 1999; Roberts et al., 1999; Clark et al., 2004; Frye, 2006; Olsen et al., 2006; Harcha et al., 2014; Kuhl & Wiegratz, 2017). In one study with finasteride for instance, DHT levels decreased by 49.5% at 0.05 mg/day, 68.6% at 0.2 mg/day, 71.4% at 1 mg/day, and 72.2% at 5 mg/day (Drake et al., 1999). Parallel reductions in DHT levels were seen locally in the scalp (Drake et al., 1999). In a study with dutasteride, DHT levels were decreased by 52.9% at 0.05 mg/day, 94.7% at 0.5 mg/day, 97.7% at 2.5 mg/day, and 98.4% at 5 mg/day (Clark et al., 2004). Based on these findings, 5α-RIs can potentially be taken at lower doses to help reduce medication costs if needed. Finasteride tablets can be split to achieve smaller doses. Conversely, dutasteride cannot be split as it is formulated as an oil capsule. However, dutasteride has a long half-life, and instead of dividing pills, it can be taken less frequently (e.g., once every few days) as a means of reducing dosage.
5α-Reductase inhibitors are taken orally in the form of tablets and capsules. Compoundedtopical formulations of finasteride also exist (Marks et al., 2020). However, caution is advised with these preparations as they have been found to be excessively dosed and to produce equivalent systemic DHT suppression as oral finasteride formulations (Marks et al., 2020). Lower-concentration formulations of topical finsteride on the other hand may be more locally selective (Marks et al., 2020).
Table 8: Available forms and recommended doses of 5α-reductase inhibitors for transfeminine people:
GnRH agonists and antagonists (GnRHa), also known as GnRH receptor agonists and antagonists or GnRH modulators, are antiandrogens which work by preventing the effects of GnRH in the pituitary gland and thereby suppressing LH and FSH secretion. Receptor agonists normally activate receptors while receptor antagonists block and thereby inhibit the activation of receptors. Due to a physiological quirk however, GnRH agonists and antagonists have the same effects in the pituitary gland. This is because GnRH is secreted in pulses under normal physiological circumstances, and when the GnRH receptor is unnaturally activated in a continuous manner, as with exogenous GnRH agonists, the GnRH receptor in the pituitary gland is strongly desensitized to the point of becoming inactive. Consequently, both GnRH agonists and GnRH antagonists have the effect of abolishing gonadal sex hormone production. This, in turn, reduces testosterone levels into the castrate or normal female range (both <50 ng/dL or <1.7 nmol/L) in people with testes. GnRHa are like a reversible gonadectomy, and for this reason, are also sometimes referred to as “medical castration”. Provided that an estrogen is taken in combination with a GnRHa to prevent sex hormone deficiency, these medications have essentially no known side effects or risks. For these reasons, GnRHa are the ideal antiandrogens for use in transfeminine people.
GnRHa are widely used to suppess puberty in adolescent transgender individuals. Unfortunately however, they are very expensive (e.g., ~US$10,000 per year) and medical insurance does not usually cover them for adult transgender people. Consequently, GnRHa are not commonly used in adult transfeminine people at this time. An exception is in the United Kingdom, where GnRH agonists are covered for all adult transgender people by the National Health Service (NHS). Another exception is buserelin (Suprefact), which has become available very inexpensively in its nasal spray form from certain Eastern European online pharmacies in recent years (Aly, 2018).
GnRH agonists cause a brief flare in testosterone levels at the start of therapy prior to the GnRH receptors in the pituitary gland becoming desensitized (Wiki). Testosterone levels increase by up to about 1.5- to 2-fold for about 1 week and then decrease thereafter (Wiki). Castrate or female-range levels of testosterone are generally reached within 2 to 4 weeks (Wiki). In contrast to GnRH agonists, there is no testosterone flare with GnRH antagonists and testosterone levels start decreasing immediately, reaching castrate levels within a few days (Wiki; Graph). This is because GnRH antagonists work by blocking the GnRH receptor without initially activating it, and hence desensitization of the receptor is not necessary for their action. If desired, the testosterone flare at the initiation of GnRH agonist therapy can be prevented or blunted with the use of antigonadotropins, for instance estrogens and progestogens, as well as with potent androgen receptor antagonists such as bicalutamide (Wiki).
GnRH agonists must be injected subcutaneously or intramuscularly once per day or once every one to six months depending on the formulation employed (buserelin, goserelin, leuprorelin, triptorelin). Alternatively, they can be surgically implanted once a year (histrelin, leuprorelin) or used as a nasal spray two to three times per day (buserelin, nafarelin). The first GnRH antagonists were developed for use by once-monthly intramuscular or subcutaneous injection (abarelix, degarelix). More recently, orally administered GnRH antagonists such as elagolix and relugolix have been introduced for medical use. They are taken in the form of tablets once or twice daily.
Table 9: Available forms and recommended doses of GnRH agonists for transfeminine people:
a 500 μg 3x/day for the first week then 200 μg/day. b 800 μg 3x/day for the first week then 400 μg 3x/day. c 500 μg 2x/day can be used instead of 400 μg 3x/day but is less effective (70% decrease in testosterone levels (to ~180 ng/dL [6.2 nmol/L]) instead of 90% decrease (to ~50 ng/dL [1.7 nmol/L]) per available studies of buserelin in men with prostate cancer) (Aly, 2018; Wiki).
Table 10: Available forms and recommended doses of GnRH antagonists for transfeminine people:
a First month is 240 mg then 80 mg per month thereafter. b 150 mg 1x/day is less effective than 200 mg 2x/day (which provides full gonadal sex-hormone suppression in cisgender women) (Wiki). c 80–120 mg/day for full gonadal sex-hormone suppression and 20–40 mg/day for substantial but partial gonadal sex-hormone suppression (MacLean et al., 2015; DailyMed).
Other Hormonal Medications
Androgens and Anabolic Steroids
In addition to estrogens, progestogens, and antiandrogens, androgens/anabolic steroids (AAS) are sometimes added to transfeminine hormone therapy. This is when testosterone levels are low (e.g., below the female average of 30 ng/dL [1.0 nmol/L]) and androgen replacement is desired. It has been proposed that adequate levels of testosterone may provide benefits such as increased sexual desire, improved mood and energy, positive effects on skin health and cellulite (Avram, 2004), and increased muscle size and strength (Huang & Basaria, 2017). However, there is insufficient clinical evidence to support such benefits at present, and androgens can produce adverse effects in cisgender women and transfeminine people, for instance acne, hirsutism, scalp hair loss, and masculinization (Wiki). For transfeminine people who nonetheless desire androgen replacement therapy, possible options for androgen medications include testosterone and its esters, dehydroepiandrosterone (DHEA; prasterone), and nandroloneesters such as nandrolone decanoate (ND) (Aly, 2020; Table), among others.
Monitoring of Therapy
Transfeminine people on hormone therapy should undergo regular laboratory monitoring in the form of blood work to assess efficacy and monitor for safety. Total estradiol levels and total testosterone levels should be measured to assess the effectiveness of therapy—that is, whether hormone levels are in appropriate ranges for cisgender females—and determine whether medication adjustments may be necessary. Levels of free testosterone, free estradiol, estrone (E1), dihydrotestosterone (DHT), luteinizing hormone (LH), follicle-stimulating hormone (FSH), and sex hormone-binding globulin (SHBG) can also be measured to provide further information although they’re not absolutely necessary. If progesterone is used as a part of hormone therapy, progesterone levels can be measured to provide insight on the degree of progesterone exposure. In addition to hormone blood tests, transfeminine people can monitor their physical changes with hormone therapy, such as breast development and other aspects of feminization, using various physical and digital measurement methods (e.g., Wiki).
Certain therapeutic situations can result in inaccurate lab blood work results. Monitoring of progesterone levels with oral progesterone using immunoassay-based blood tests can result in falsely high readings for progesterone levels due to cross-reactivity with high levels of progesterone metabolites such as allopregnanolone (Aly, 2018; Wiki). Instead of immunoassay-based tests, mass spectrometry-based tests should be used to determine progesterone levels with oral progesterone (Aly, 2018; Wiki). Conversely, either type of test may be used to measure progesterone levels with non-oral progesterone therapy. High-dose biotin (vitamin B7) supplements can interfere with the accuracy of immunoassay-based hormone blood tests, causing falsely low or falsely high readings (Samarasinghe et al., 2017; Avery, 2019; Bowen et al., 2019; FDA, 2019; Luong, Male, & Glennon, 2019). Transdermal estradiol formulations applied to the arm can result in contamination of blood draws taken from the same arm and can result in falsely high readings for estradiol levels (Vihtamäkia, Luukkaala, & Tuimala, 2004).
Certain cancers are known to be hormone-sensitive and their incidence can be influenced by hormone therapy. Screening for breast and prostate cancer is recommended in transfeminine people (Sterling & Garcia, 2020; Iwamoto et al., 2021). The risk of breast cancer appears to be dramatically increased with transfeminine hormone therapy, perhaps especially with progestogens (Aly, 2020). However, the risk still remains lower than in cisgender women (Aly, 2020). The incidence of prostate cancer is greatly decreased with hormone therapy in transfeminine people as a consequence of androgen deprivation, but the risk is not abolished and prostate cancer can still occur (de Nie et al., 2020). The prostate gland is not removed with vaginoplasty, so transfeminine people who have undergone vaginoplasty will also require monitoring for prostate cancer still. Testicular cancer is not known to be a hormone-dependent cancer and its incidence does not appear to be increased with hormone therapy in transfeminine people (Bensley et al., 2021; de Nie et al., 2021; Jacoby et al., 2021).
Ahmad, S. R., & Graham, D. J. (2003). Pneumonitis with Antiandrogens. Annals of Internal Medicine, 139(6), 528–529. [DOI:10.7326/0003-4819-139-6-200309160-00023]
Allen, A. N., Jiao, R., Day, P., Pagels, P., Gimpel, N., & SoRelle, J. A. (2020). Dynamic Impact of Hormone Therapy on Laboratory Values in Transgender Patients over Time. The Journal of Applied Laboratory Medicine, 6(1), 27–40. [DOI:10.1093/jalm/jfaa192]
Angus, L., Leemaqz, S., Ooi, O., Cundill, P., Silberstein, N., Locke, P., Zajac, J. D., & Cheung, A. S. (2019). Cyproterone acetate or spironolactone in lowering testosterone concentrations for transgender individuals receiving oestradiol therapy. Endocrine Connections, 8(7), 935–940. [DOI:10.1530/ec-19-0272]
Angus, L. M., Nolan, B. J., Zajac, J. D., & Cheung, A. S. (2020). A systematic review of antiandrogens and feminization in transgender women. Clinical Endocrinology, 94(5), 743–752. [DOI:10.1111/cen.14329]
Antoniou, T., Gomes, T., Mamdani, M. M., Yao, Z., Hellings, C., Garg, A. X., Weir, M. A., & Juurlink, D. N. (2011). Trimethoprim-sulfamethoxazole induced hyperkalaemia in elderly patients receiving spironolactone: nested case-control study. BMJ, 343, d5228. [DOI:10.1136/bmj.d5228]
Antoniou, T., Hollands, S., Macdonald, E. M., Gomes, T., Mamdani, M. M., & Juurlink, D. N. (2015). Trimethoprim–sulfamethoxazole and risk of sudden death among patients taking spironolactone. Canadian Medical Association Journal, 187(4), E138–E143. [DOI:10.1503/cmaj.140816]
Aufrère, M. B., & Benson, H. (1976). Progesterone: An overview and recent advances. Journal of Pharmaceutical Sciences, 65(6), 783–800. [DOI:10.1002/jps.2600650602]
Avery, G. (2019). Biotin interference in immunoassay: a review for the laboratory scientist. Annals of Clinical Biochemistry: International Journal of Laboratory Medicine, 56(4), 424–430. [DOI:10.1177/0004563219842231]
Avram, M. M. (2004). Cellulite: a review of its physiology and treatment. Journal of Cosmetic and Laser Therapy, 6(4), 181–185. [DOI:10.1080/14764170410003057]
Babich, J. S., Kalantar-Zadeh, K., & Joshi, S. (2022). Taking the Kale out of Hyperkalemia: Plant Foods and Serum Potassium in Patients With Kidney Disease. Journal of Renal Nutrition, 32(6), 641–649. [DOI:10.1053/j.jrn.2022.01.013]
Bäckström, T., Haage, D., Löfgren, M., Johansson, I., Strömberg, J., Nyberg, S., Andréen, L., Ossewaarde, L., van Wingen, G., Turkmen, S., & Bengtsson, S. (2011). Paradoxical effects of GABA-A modulators may explain sex steroid induced negative mood symptoms in some persons. Neuroscience, 191, 46–54. [DOI:10.1016/j.neuroscience.2011.03.061]
Barrionuevo, P., Nabhan, M., Altayar, O., Wang, Z., Erwin, P. J., Asi, N., Martin, K. A., & Murad, M. H. (2018). Treatment Options for Hirsutism: A Systematic Review and Network Meta-Analysis. The Journal of Clinical Endocrinology & Metabolism, 103(4), 1258–1264. [DOI:10.1210/jc.2017-02052]
Bazarra-Castro, M. A. (2009). Etiological aspects, therapy regimes, side effects and treatment satisfaction of transsexual patients. (Doctoral dissertation, Ludwig Maximilian University of Munich.) [DOI:10.5282/edoc.9984] [URN:urn:nbn:de:bvb:19-99840] [PDF]
Belisle, S., & Love, E. J. (1986). Clinical efficacy and safety of cyproterone acetate in severe hirsutism: results of a multicentered Canadian study. Fertility and Sterility, 46(6), 1015–1020. [DOI:10.1016/s0015-0282(16)49873-0]
Ben Salem, C., Badreddine, A., Fathallah, N., Slim, R., & Hmouda, H. (2014). Drug-Induced Hyperkalemia. Drug Safety, 37(9), 677–692. [DOI:10.1007/s40264-014-0196-1]
Bensley, J. G., Cheung, A. S., Grossmann, M., & Papa, N. (2022). Testicular Cancer in Trans People Using Feminising Hormone Therapy–A Brief Review. Urology, 160, 1–4. [DOI:10.1016/j.urology.2021.11.014]
Bessone, F., Lucena, M., Roma, M. G., Stephens, C., Medina-Cáliz, I., Frider, B., Tsariktsian, G., Hernández, N., Bruguera, M., Gualano, G., Fassio, E., Montero, J., Reggiardo, M. V., Ferretti, S., Colombato, L., Tanno, F., Ferrer, J., Zeno, L., Tanno, H., & Andrade, R. J. (2015). Cyproterone acetate induces a wide spectrum of acute liver damage including corticosteroid-responsive hepatitis: report of 22 cases. Liver International, 36(2), 302–310. [DOI:10.1111/liv.12899]
Bowen, R., Benavides, R., Colón-Franco, J. M., Katzman, B. M., Muthukumar, A., Sadrzadeh, H., Straseski, J., Klause, U., & Tran, N. (2019). Best practices in mitigating the risk of biotin interference with laboratory testing. Clinical Biochemistry, 74, 1–11. [DOI:10.1016/j.clinbiochem.2019.08.012]
Brown, J., Farquhar, C., Lee, O., Toomath, R., & Jepson, R. G. (2009). Spironolactone versus placebo or in combination with steroids for hirsutism and/or acne. Cochrane Database of Systematic Reviews, 2009(2), CD000194. [DOI:10.1002/14651858.cd000194.pub2]
Burinkul, S., Panyakhamlerd, K., Suwan, A., Tuntiviriyapun, P., & Wainipitapong, S. (2021). Anti-Androgenic Effects Comparison Between Cyproterone Acetate and Spironolactone in Transgender Women: A Randomized Controlled Trial. The Journal of Sexual Medicine, 18(7), 1299–1307. [DOI:10.1016/j.jsxm.2021.05.003] [PDF]
Callen-Lorde Community Health Center. (2018). Protocols for the Provision of Hormone Therapy. New York City: Callen-Lorde Community Health Center. [URL] [PDF]
Cappelletti, M., & Wallen, K. (2016). Increasing women’s sexual desire: The comparative effectiveness of estrogens and androgens. Hormones and Behavior, 78, 178–193. [DOI:10.1016/j.yhbeh.2015.11.003]
Carmina, E., Stanczyk, F. Z., & Lobo, R. A. (2019). Evaluation of Hormonal Status. In Strauss, J. F., & Barbieri, R. L. (Eds.). Yen and Jaffe’s Reproductive Endocrinology: Physiology, Pathophysiology, and Clinical Management, 8th Edition (pp. 887–915.e4). Philadelphia: Elsevier. [DOI:10.1016/b978-0-323-47912-7.00034-2]
Carvalho, R. d., Santos, L. D., Ramos, P. M., Machado, C. J., Acioly, P., Frattini, S. C., Barcaui, C. B., Donda, A. L., & Melo, D. F. (2022). Bicalutamide and the new perspectives for female pattern hair loss treatment: What dermatologists should know. Journal of Cosmetic Dermatology, 21(10), 4171–4175. [DOI:10.1111/jocd.14773]
Clark, R. V., Hermann, D. J., Cunningham, G. R., Wilson, T. H., Morrill, B. B., & Hobbs, S. (2004). Marked Suppression of Dihydrotestosterone in Men with Benign Prostatic Hyperplasia by Dutasteride, a Dual 5α-Reductase Inhibitor. The Journal of Clinical Endocrinology & Metabolism, 89(5), 2179–2184. [DOI:10.1210/jc.2003-030330]
Coleman, E., Radix, A. E., Bouman, W. P., Brown, G. R., de Vries, A. L., Deutsch, M. B., Ettner, R., Fraser, L., Goodman, M., Green, J., Hancock, A. B., Johnson, T. W., Karasic, D. H., Knudson, G. A., Leibowitz, S. F., Meyer-Bahlburg, H. F., Monstrey, S. J., Motmans, J., Nahata, L., … & Arcelus, J. (2022). [World Professional Association for Transgender Health (WPATH)] Standards of Care for the Health of Transgender and Gender Diverse People, Version 8. International Journal of Transgender Health, 23(Suppl 1), S1–S259. [DOI:10.1080/26895269.2022.2100644] [URL] [PDF]
Collaborative Group on Hormonal Factors in Breast Cancer. (2019). Type and timing of menopausal hormone therapy and breast cancer risk: individual participant meta-analysis of the worldwide epidemiological evidence. The Lancet, 394(10204), 1159–1168. [DOI:10.1016/s0140-6736(19)31709-x]
Collet, S., Gieles, N. C., Wiepjes, C. M., Heijboer, A. C., Reyns, T., Fiers, T., Lapauw, B., den Heijer, M., & T’Sjoen, G. (2022). Changes in Serum Testosterone and Adrenal Androgen Levels in Transgender Women With and Without Gonadectomy. The Journal of Clinical Endocrinology & Metabolism, 108(2), 331–338. [DOI:10.1210/clinem/dgac576]
Connors, J. M., & Middeldorp, S. (2019). Transgender patients and the role of the coagulation clinician. Journal of Thrombosis and Haemostasis, 17(11), 1790–1797. [DOI:10.1111/jth.14626]
Cupisti, A., Kovesdy, C., D’Alessandro, C., & Kalantar-Zadeh, K. (2018). Dietary Approach to Recurrent or Chronic Hyperkalaemia in Patients with Decreased Kidney Function. Nutrients, 10(3), 261–261. [DOI:10.3390/nu10030261]
Cusan, L., Dupont, A., Gomez, J., Tremblay, R. R., & Labrie, F. (1994). Comparison of flutamide and spironolactone in the treatment of hirsutism: a randomized controlled trial. Fertility and Sterility, 61(2), 281–287. [DOI:10.1016/s0015-0282(16)56518-2]
de Blok, C. J., Wiepjes, C. M., Nota, N. M., van Engelen, K., Adank, M. A., Dreijerink, K. M., Barbé, E., Konings, I. R., & den Heijer, M. (2019). Breast cancer risk in transgender people receiving hormone treatment: nationwide cohort study in the Netherlands. BMJ, 365, l1652. [DOI:10.1136/bmj.l1652]
de Nie, I., de Blok, C. J., van der Sluis, T. M., Barbé, E., Pigot, G. L., Wiepjes, C. M., Nota, N. M., van Mello, N. M., Valkenburg, N. E., Huirne, J., Gooren, L. J., van Moorselaar, R. J., Dreijerink, K. M., & den Heijer, M. (2020). Prostate Cancer Incidence under Androgen Deprivation: Nationwide Cohort Study in Trans Women Receiving Hormone Treatment. The Journal of Clinical Endocrinology & Metabolism, 105(9), e3293–e3299. [DOI:10.1210/clinem/dgaa412]
Deng, T., Duan, X., He, Z., Zhao, Z., & Zeng, G. (2020). Association Between 5-Alpha Reductase Inhibitor Use and The Risk of Depression: A Meta-Analysis. Urology Journal, 18(2), 144–150. [DOI:10.22037/uj.v16i7.5866]
Deutsch, M. B. (2016). Overview of feminizing hormone therapy. In Deutsch, M. B. (Ed.). Guidelines for the Primary and Gender-Affirming Care of Transgender and Gender Nonbinary People, 2nd Edition (pp. 26–48). San Francisco: University of California, San Francisco/UCSF Transgender Care. [URL] [PDF]
Dhurat, R., Sharma, A., Rudnicka, L., Kroumpouzos, G., Kassir, M., Galadari, H., Wollina, U., Lotti, T., Golubovic, M., Binic, I., Grabbe, S., & Goldust, M. (2020). 5‐Alpha reductase inhibitors in androgenetic alopecia: Shifting paradigms, current concepts, comparative efficacy, and safety. Dermatologic Therapy, 33(3), e13379. [DOI:10.1111/dth.13379]
Drake, L., Hordinsky, M., Fiedler, V., Swinehart, J., Unger, W. P., Cotterill, P. C., Thiboutot, D. M., Lowe, N., Jacobson, C., Whiting, D., Stieglitz, S., Kraus, S. J., Griffin, E. I., Weiss, D., Carrington, P., Gencheff, C., Cole, G. W., Pariser, D. M., Epstein, E. S., Tanaka, W., Dallob, A., Vandormael, K., Geissler, L., & Waldsteicher, J. (1999). The effects of finasteride on scalp skin and serum androgen levels in men with androgenetic alopecia. Journal of the American Academy of Dermatology, 41(4), 550–554. [DOI:10.1016/s0190-9622(99)80051-6]
Dyson, T. E., Cantrell, M. A., & Lund, B. C. (2020). Lack of Association between 5α-Reductase Inhibitors and Depression. Journal of Urology, 204(4), 793–798. [DOI:10.1097/ju.0000000000001079]
Erem, C. (2013). Update on idiopathic hirsutism: diagnosis and treatment. Acta Clinica Belgica, 68(4), 268–274. [DOI:10.2143/acb.3267]
Erenus, M., Gürbüz, O., Durmuşoğlu, F., Demirçay, Z., & Pekin, S. (1994). Comparison of the efficacy of spironolactone versus flutamide in the treatment of hirsutism. Fertility and Sterility, 61(4), 613–616. [DOI:10.1016/s0015-0282(16)56634-5]
Esoterix/LabCorp. (2020). Endocrinology Expected Values and S.I. Unit Conversion Tables. LabCorp/Endocrine Sciences. [PDF]
Even Zohar, N., Sofer, Y., Yaish, I., Serebro, M., Tordjman, K., & Greenman, Y. (2021). Low-Dose Cyproterone Acetate Treatment for Transgender Women. The Journal of Sexual Medicine, 18(7), 1292–1298. [DOI:10.1016/j.jsxm.2021.04.008]
Fertig, R., Shapiro, J., Bergfeld, W., & Tosti, A. (2016). Investigation of the Plausibility of 5-Alpha-Reductase Inhibitor Syndrome. Skin Appendage Disorders, 2(3–4), 120–129. [DOI:10.1159/000450617]
Food and Drug Administration. (2019). UPDATE: The FDA Warns that Biotin May Interfere with Lab Tests: FDA Safety Communication. Food and Drug Administration. [URL]
Fournier, A., Berrino, F., & Clavel-Chapelon, F. (2007). Unequal risks for breast cancer associated with different hormone replacement therapies: results from the E3N cohort study. Breast Cancer Research and Treatment, 107(1), 103–111. [DOI:10.1007/s10549-007-9523-x]
Frye, S. (2006). Discovery and Clinical Development of Dutasteride, a Potent Dual 5α-Reductase Inhibitor. Current Topics in Medicinal Chemistry, 6(5), 405–421. [DOI:10.2174/156802606776743101]
Gava, G., Mancini, I., Alvisi, S., Seracchioli, R., & Meriggiola, M. C. (2020). A comparison of 5-year administration of cyproterone acetate or leuprolide acetate in combination with estradiol in transwomen. European Journal of Endocrinology, 183(6), 561–569. [DOI:10.1530/eje-20-0370]
Getzenberg, R., & Itty, S. (2020). How do we define “castration” in men on androgen deprivation therapy? Asian Journal of Andrology, 22(5), 441–446. [DOI:10.4103/aja.aja_139_19]
Giltay, E. J., Gooren, L. J., Toorians, A. W., Katan, M. B., & Zock, P. L. (2004). Docosahexaenoic acid concentrations are higher in women than in men because of estrogenic effects. The American Journal of Clinical Nutrition, 80(5), 1167–1174. [DOI:10.1093/ajcn/80.5.1167]
Glintborg, D., T’Sjoen, G., Ravn, P., & Andersen, M. S. (2021). MANAGEMENT OF ENDOCRINE DISEASE: Optimal feminizing hormone treatment in transgender people. European Journal of Endocrinology, 185(2), R49–R63. [DOI:10.1530/eje-21-0059]
Goletiani, N. V., Keith, D. R., & Gorsky, S. J. (2007). Progesterone: Review of safety for clinical studies. Experimental and Clinical Psychopharmacology, 15(5), 427–444. [DOI:10.1037/1064-1297.15.5.427]
Goodfellow, A., Alaghband-Zadeh, J., Carter, G., Cream, J., Holland, S., Scully, J., & Wise, P. (1984). Oral spironolactone improves acne vulgaris and reduces sebum excretion. British Journal of Dermatology, 111(2), 209–214. [DOI:10.1111/j.1365-2133.1984.tb04045.x]
Gooren, L. J. (2016). The Endocrinology of Sexual Behavior and Gender Identity. In Jameson, J. L., & De Groot, L. J. (Eds.). Endocrinology: Adult and Pediatric, 7th Edition, Volume 2 (pp. 2163–2176.e4). Philadelphia: Saunders/Elsevier. [Google Books] [DOI:10.1016/B978-0-323-18907-1.00124-4]
Gooren, L. J., Harmsen-Louman, W., & Kessel, H. (1985). Follow-up of prolactin levels in long-term oestrogen-treated male-to-female transsexuals with regard to prolactinoma induction. Clinical Endocrinology, 22(2), 201–207. [DOI:10.1111/j.1365-2265.1985.tb01081.x]
Gooren, L., Rao, B., van Kessel, H., & Harmsen-Louman, W. (1984). Estrogen positive feedback on LH secretion in transsexuality. Psychoneuroendocrinology, 9(3), 249–259. [DOI:10.1016/0306-4530(84)90004-0]
Gormley, G. J., Stoner, E., Rittmaster, R. S., Gregg, H., Thompson, D. L., Lasseter, K. C., Vlasses, P. H., & Stein, E. A. (1990). Effects of Finasteride (MK-906), a 5α-Reductase Inhibitor, on Circulating Androgens in Male Volunteers. The Journal of Clinical Endocrinology & Metabolism, 70(4), 1136–1141. [DOI:10.1210/jcem-70-4-1136]
Grock, S., Weinreb, J., Williams, K. C., Weimer, A., Fadich, S., Patel, R., Geft, A., & Korenman, S. (2024). Priorities for efficacy trials of gender-affirming hormone therapy with estrogen: collaborative design and results of a community survey. Hormones, online ahead of print. [DOI:10.1007/s42000-024-00532-3]
Gubelin Harcha, W., Barboza Martínez, J., Tsai, T., Katsuoka, K., Kawashima, M., Tsuboi, R., Barnes, A., Ferron-Brady, G., & Chetty, D. (2014). A randomized, active- and placebo-controlled study of the efficacy and safety of different doses of dutasteride versus placebo and finasteride in the treatment of male subjects with androgenetic alopecia. Journal of the American Academy of Dermatology, 70(3), 489–498.e3. [DOI:10.1016/j.jaad.2013.10.049]
Gupta, P., Suppakitjanusant, P., Stevenson, M., Goodman, M., & Tangpricha, V. (2022). Potassium Concentrations in Transgender Women Using Spironolactone: A Retrospective Chart Review. Endocrine Practice, 28(11), 1113–1117. [DOI:10.1016/j.eprac.2022.08.007]
Hammerstein, J. (1990). Antiandrogens: Clinical Aspects. In Orfanos, C. E., & Happle, R. (Eds.). Hair and Hair Diseases (pp. 827–886). Berlin/Heidelberg: Springer. [DOI:10.1007/978-3-642-74612-3_35]
Hayes, H., Russell, R., Haugen, A., Nagavally, S., & Sarvaideo, J. (2022). The Utility of Monitoring Potassium in Transgender, Gender Diverse, and Nonbinary Individuals on Spironolactone. Journal of the Endocrine Society, 6(11), bvac133. [DOI:10.1210/jendso/bvac133]
Heinemann, L. A., Will-Shahab, L., van Kesteren, P., Gooren, L. J., & (1997). Safety of Cyproterone Acetate: Report of Active Surveillance. Pharmacoepidemiology and Drug Safety, 6(3), 169–178. [DOI:10.1002/(sici)1099-1557(199705)6:3<169::aid-pds263>3.0.co;2-3]
Hembree, W. C., Cohen-Kettenis, P. T., Gooren, L., Hannema, S. E., Meyer, W. J., Murad, M. H., Rosenthal, S. M., Safer, J. D., Tangpricha, V., & T’Sjoen, G. G. (2017). Endocrine Treatment of Gender-Dysphoric/Gender-Incongruent Persons: An Endocrine Society Clinical Practice Guideline. The Journal of Clinical Endocrinology and Metabolism, 102(11), 3869–3903. [DOI:10.1210/jc.2017-01658] [PDF]
Herndon, J. S., Maheshwari, A. K., Nippoldt, T. B., Carlson, S. J., Davidge-Pitts, C. J., & Chang, A. Y. (2023). Comparison of the Subcutaneous and Intramuscular Estradiol Regimens as Part of Gender-Affirming Hormone Therapy. Endocrine Practice, 29(5), 356–361. [DOI:10.1016/j.eprac.2023.02.006]
Hirshburg, J. M., Kelsey, P. A., Therrien, C. A., Gavino, A. C., & Reichenberg, J. S. (2016). Adverse Effects and Safety of 5-alpha Reductase Inhibitors (Finasteride, Dutasteride): A Systematic Review. The Journal of Clinical and Aesthetic Dermatology, 9(7), 56–62. [PubMed] [PubMed Central]
Hopkins, U., & Arias, C. Y. (2013). Large-volume IM injections: a review of best practices. Oncology Nurse Advisor, 4(1), 32–37. [Google Scholar] [URL] [PDF]
Horton, R. (1992). Dihydrotestosterone Is a Peripheral Paracrine Hormone. Journal of Andrology, 13(1), 23–27. [DOI:10.1002/j.1939-4640.1992.tb01621.x]
Huang, G., & Basaria, S. (2017). The Case for Androgens in Menopausal Women: When and How? In Pal, L., & Sayegh, R. A. (Eds.). Essentials of Menopause Management: A Case-Based Approach (pp. 173–196). Cham: Springer International Publishing. [DOI:10.1007/978-3-319-42451-4_10]
Igo, J., & Visram, H. (2021). Testosterone Suppression With Injectable Estrogen Therapy Alone in Male to Female Transgender Patients. Canadian Journal of Diabetes, 45(7 Suppl), S40–S40 (abstract no. 114). [DOI:10.1016/j.jcjd.2021.09.124] [URL] [PDF]
Irwig, M. S. (2020). Is there a role for 5α‐reductase inhibitors in transgender individuals? Andrology, 9(6), 1729–1731. [DOI:10.1111/andr.12881]
Iversen, P., Johansson, J. E., Lodding, P., Lukkarinen, O., Lundmo, P., Klarskov, P., Tammela, T. L., Tasdemir, I., Morris, T., Carroll, K., & Scandinavian Prostatic Cancer Group. (2004). Bicalutamide (150 mg) versus placebo as immediate therapy alone or as adjuvant to therapy with curative intent for early nonmetastatic prostate cancer: 5.3-year median followup from the Scandinavian Prostate Cancer Group Study Number 6. The Journal of Urology, 172(5 Part 1), 1871–1876. [DOI:10.1097/01.ju.0000139719.99825.54]
Iversen, P., Johansson, J., Lodding, P., Kylmälä, T., Lundmo, P., Klarskov, P., Tammela, T. L., Tasdemir, I., Morris, T., Armstrong, J., & (2006). Bicalutamide 150 mg in addition to standard care for patients with early non-metastatic prostate cancer Updated results from the Scandinavian Prostate Cancer Period Group-6 Study after a median follow-up period of 7.1 years. Scandinavian Journal of Urology and Nephrology, 40(6), 441–452. [DOI:10.1080/00365590601017329]
Iwamoto, S. J., Defreyne, J., Rothman, M. S., Van Schuylenbergh, J., Van de Bruaene, L., Motmans, J., & T’Sjoen, G. (2019). Health considerations for transgender women and remaining unknowns: a narrative review. Therapeutic Advances in Endocrinology and Metabolism, 10, 204201881987116. [DOI:10.1177/2042018819871166]
Iwamoto, S. J., Grimstad, F., Irwig, M. S., & Rothman, M. S. (2021). Routine Screening for Transgender and Gender Diverse Adults Taking Gender-Affirming Hormone Therapy: a Narrative Review. Journal of General Internal Medicine, 36(5), 1380–1389. [DOI:10.1007/s11606-021-06634-7]
Jacoby, A., Rifkin, W., Zhao, L. C., & Bluebond-Langner, R. (2020). Incidence of Cancer and Premalignant Lesions in Surgical Specimens of Transgender Patients. Plastic & Reconstructive Surgery, 147(1), 194–198. [DOI:10.1097/prs.0000000000007452]
Jain, J., Kwan, D., & Forcier, M. (2019). Medroxyprogesterone Acetate in Gender-Affirming Therapy for Transwomen: Results From a Retrospective Study. The Journal of Clinical Endocrinology & Metabolism, 104(11), 5148–5156. [DOI:10.1210/jc.2018-02253]
James, J. F., Jamerson, T. A., & Aguh, C. (2022). Efficacy and safety profile of oral spironolactone use for androgenic alopecia: A systematic review. Journal of the American Academy of Dermatology, 86(2), 425–429. [DOI:10.1016/j.jaad.2021.07.048]
Jia, A. Y., & Spratt, D. E. (2022). Bicalutamide Monotherapy With Radiation Therapy for Localized Prostate Cancer: A Non-Evidence-Based Alternative. International Journal of Radiation Oncology*Biology*Physics, 113(2), 316–319. [DOI:10.1016/j.ijrobp.2022.01.037]
Jiang, Y., & Tian, W. (2017). The effects of progesterones on blood lipids in hormone replacement therapy. Lipids in Health and Disease, 16(1), 219. [DOI:10.1186/s12944-017-0612-5]
Kanhai, R. C., Hage, J. J., van Diest, P. J., Bloemena, E., & Mulder, J. W. (2000). Short-Term and Long-Term Histologic Effects of Castration and Estrogen Treatment on Breast Tissue of 14 Male-to-Female Transsexuals in Comparison With Two Chemically Castrated Men. The American Journal of Surgical Pathology, 24(1), 74–80. [DOI:10.1097/00000478-200001000-00009]
Kellner, M., & Wiedemann, K. (2008). Mineralocorticoid receptors in brain, in health and disease: Possibilities for new pharmacotherapy. European Journal of Pharmacology, 583(2–3), 372–378. [DOI:10.1016/j.ejphar.2007.07.072]
Kim, G. K., & Del Rosso, J. Q. (2012). Oral Spironolactone in Post-teenage Female Patients with Acne Vulgaris: Practical Considerations for the Clinician Based on Current Data and Clinical Experience. The Journal of Clinical and Aesthetic Dermatology, 5(3), 37–50. [PubMed] [PubMed Central]
King, S. R. (2012). Neurosteroids and the Nervous System. In King, S. R. Neurosteroids and the Nervous System (pp. 1–122). New York: Springer New York. [DOI:10.1007/978-1-4614-5559-2_1]
Krishnamurthy, N., Slack, D., Kyweluk, M., Kirkley, J., Trakhtenberg, E., Contreras-Castro, F., & Safer, J. (2023). Not All Transfeminine Individuals on Estradiol Can Reach Both Target Testosterone and Target Estradiol Levels—Time to Revisit Treatment Guidelines? USPATH Scientific Symposium, November 1-5, 2023, The Westin Westminster, Westminster, Colorado, Abstract Submissions, 94–94 (abstract no. SAT-B2-T4). [Symposium Schedule] [PDF] [Full Abstract Book]
Kolvenbag, G. J., & Blackledge, G. R. (1996). Worldwide activity and safety of bicalutamide: a summary review. Urology, 47(1), 70–79. [DOI:10.1016/s0090-4295(96)80012-4]
Kuhl, H. (2003). Östrogene für den Mann? [Estrogen for men?] Blickpunkt der Mann, 1(3), 6–12. [Google Scholar] [URL] [PDF]
Kuhl, H. (2005). Pharmacology of estrogens and progestogens: influence of different routes of administration. Climacteric, 8(Suppl 1), 3–63. [DOI:10.1080/13697130500148875] [PDF]
Kuhl, H., & Wiegratz, I. (2017). Das Post-Finasterid-Syndrom. [Post Finasteride Syndrome.] Gynäkologische Endokrinologie, 15(2), 153–163. [DOI:10.1007/s10304-017-0126-2]
Kuijpers, S. M., Wiepjes, C. M., Conemans, E. B., Fisher, A. D., T’Sjoen, G., & den Heijer, M. (2021). Toward a Lowest Effective Dose of Cyproterone Acetate in Trans Women: Results From the ENIGI Study. The Journal of Clinical Endocrinology & Metabolism, 106(10), e3936–e3945. [DOI:10.1210/clinem/dgab427]
Kumar, P., Reddy, S., Kulkarni, A., Sharma, M., & Rao, P. N. (2021). Cyproterone Acetate–Induced Acute Liver Failure: A Case Report and Review of the Literature. Journal of Clinical and Experimental Hepatology, 11(6), 739–741. [DOI:10.1016/j.jceh.2021.01.003]
Lauritzen, C. (1988). Natürliche und synthetische Sexualhormone – Biologische Grundlagen und Behandlungsprinzipien. [Natural and Synthetic Sexual Hormones – Biological Basis and Medical Treatment Principles.] In Lauritzen, C., Schneider, H. P. G., & Nieschlag, E. (Eds.). Grundlagen und Klinik der Menschlichen Fortpflanzung [Foundations and Clinic of Human Reproduction] (pp. 229–306). Berlin: de Gruyter. [Google Scholar] [Google Books] [OpenLibrary] [WorldCat] [URL] [PDF] [Translation]
Lax, E. (1987). Mechanisms of physiological and pharmacological sex hormone action on the mammalian liver. Journal of Steroid Biochemistry, 27(4–6), 1119–1128. [DOI:10.1016/0022-4731(87)90198-1]
Layton, A. M., Eady, E. A., Whitehouse, H., Del Rosso, J. Q., Fedorowicz, Z., & van Zuuren, E. J. (2017). Oral Spironolactone for Acne Vulgaris in Adult Females: A Hybrid Systematic Review. American Journal of Clinical Dermatology, 18(2), 169–191. [DOI:10.1007/s40257-016-0245-x]
Legro, R. S., Schlaff, W. D., Diamond, M. P., Coutifaris, C., Casson, P. R., Brzyski, R. G., Christman, G. M., Trussell, J. C., Krawetz, S. A., Snyder, P. J., Ohl, D., Carson, S. A., Steinkampf, M. P., Carr, B. R., McGovern, P. G., Cataldo, N. A., Gosman, G. G., Nestler, J. E., Myers, E. R., Santoro, N., Eisenberg, E., Zhang, M., & Zhang, H. (2010). Total Testosterone Assays in Women with Polycystic Ovary Syndrome: Precision and Correlation with Hirsutism. The Journal of Clinical Endocrinology & Metabolism, 95(12), 5305–5313. [DOI:10.1210/jc.2010-1123]
Leinung, M. C., Feustel, P. J., & Joseph, J. (2018). Hormonal Treatment of Transgender Women with Oral Estradiol. Transgender Health, 3(1), 74–81. [DOI:10.1089/trgh.2017.0035]
Liang, J. J., Jolly, D., Chan, K. J., & Safer, J. D. (2018). Testosterone Levels Achieved by Medically Treated Transgender Women in a United States Endocrinology Clinic Cohort. Endocrine Practice, 24(2), 135–142. [DOI:10.4158/ep-2017-0116]
Lobo, R. A., Shoupe, D., Serafini, P., Brinton, D., & Horton, R. (1985). The effects of two doses of spironolactone on serum androgens and anagen hair in hirsute women. Fertility and Sterility, 43(2), 200–205. [DOI:10.1016/s0015-0282(16)48373-1]
Loh, H. H., Yee, A., Loh, H. S., Kanagasundram, S., Francis, B., & Lim, L. (2020). Sexual dysfunction in polycystic ovary syndrome: a systematic review and meta-analysis. Hormones, 19(3), 413–423. [DOI:10.1007/s42000-020-00210-0]
Luong, J. H., Male, K. B., & Glennon, J. D. (2019). Biotin interference in immunoassays based on biotin-strept(avidin) chemistry: An emerging threat. Biotechnology Advances, 37(5), 634–641. [DOI:10.1016/j.biotechadv.2019.03.007]
MacLean, D. B., Shi, H., Faessel, H. M., & Saad, F. (2015). Medical Castration Using the Investigational Oral GnRH Antagonist TAK-385 (Relugolix): Phase 1 Study in Healthy Males. The Journal of Clinical Endocrinology & Metabolism, 100(12), 4579–4587. [DOI:10.1210/jc.2015-2770]
Mahler, C. (1996). A Review of the Clinical Studies with Nilutamide. In Denis, L. (Ed.). Antiandrogens in Prostate Cancer: A Key to Tailored Endocrine Treatment (ESO Monographs) (pp. 105–111). Berlin/Heidelberg: Springer Berlin Heidelberg. [DOI:10.1007/978-3-642-45745-6_10]
Maksym, R. B., Kajdy, A., & Rabijewski, M. (2019). Post-finasteride syndrome – does it really exist? The Aging Male, 22(4), 250–259. [DOI:10.1080/13685538.2018.1548589]
Marks, D. H., Prasad, S., De Souza, B., Burns, L. J., & Senna, M. M. (2019). Topical Antiandrogen Therapies for Androgenetic Alopecia and Acne Vulgaris. American Journal of Clinical Dermatology, 21(2), 245–254. [DOI:10.1007/s40257-019-00493-z]
Martinez-Martin, F. J., Kuzior, A., Hernandez-Lazaro, A., de Leon-Durango, R. J., Rios-Gomez, C., Santana-Ojeda, B., Perez-Rivero, J. M., Fernandez-Trujillo-Comenge, P. M., Gonzalez-Diaz, P., Arnas-Leon, C., Acosta-Calero, C., Perdomo-Herrera, E., Tocino-Hernandez, A. L., del Sol Sanchez-Bacaicoa, M., & del Pino Perez-Garcia, M. (2022). Incidence of hypertension in young transgender people after a 5-year follow-up: association with gender-affirming hormonal therapy. Hypertension Research, 46(1), 219–225. [DOI:10.1038/s41440-022-01067-z]
Masumori, N., Baba, T., Abe, T., & Niwa, K. (2021). What is the most anticipated change induced by treatment using gender‐affirming hormones in individuals with gender incongruence?. International Journal of Urology, 28(5), 526–529. [DOI:10.1111/iju.14499]
McFarlane, T., Zajac, J. D., & Cheung, A. S. (2018). Gender-affirming hormone therapy and the risk of sex hormone-dependent tumours in transgender individuals—A systematic review. Clinical Endocrinology, 89(6), 700–711. [DOI:10.1111/cen.13835]
Meriggiola, M. C., Bremner, W. J., Costantino, A., Bertaccini, A., Morselli-Labate, A. M., Huebler, D., Kaufmann, G., Oettel, M., & Flamigni, C. (2002). Twenty-One Day Administration of Dienogest Reversibly Suppresses Gonadotropins and Testosterone in Normal Men. The Journal of Clinical Endocrinology & Metabolism, 87(5), 2107–2113. [DOI:10.1210/jcem.87.5.8514]
Meyer, G., Mayer, M., Mondorf, A., Flügel, A. K., Herrmann, E., & Bojunga, J. (2020). Safety and rapid efficacy of guideline-based gender-affirming hormone therapy: an analysis of 388 individuals diagnosed with gender dysphoria. European Journal of Endocrinology, 182(2), 149–156. [DOI:10.1530/eje-19-0463]
Miles, R. A., Paulson, R. J., Lobo, R. A., Press, M. F., Dahmoush, L., & Sauer, M. V. (1994). Pharmacokinetics and endometrial tissue levels of progesterone after administration by intramuscular and vaginal routes: a comparative study. Fertility and Sterility, 62(3), 485–490. [DOI:10.1016/s0015-0282(16)56935-0]
Millington, K., Liu, E., & Chan, Y. (2019). The Utility of Potassium Monitoring in Gender-Diverse Adolescents Taking Spironolactone. Journal of the Endocrine Society, 3(5), 1031–1038. [DOI:10.1210/js.2019-00030]
Millward, C. P., Keshwara, S. M., Islim, A. I., Jenkinson, M. D., Alalade, A. F., & Gilkes, C. E. (2022). Development and Growth of Intracranial Meningiomas in Transgender Women Taking Cyproterone Acetate as Gender-Affirming Progestogen Therapy: A Systematic Review. Transgender Health, 7(6), 473–483. [DOI:10.1089/trgh.2021.0025]
Moretti, C., Guccione, L., Di Giacinto, P., Simonelli, I., Exacoustos, C., Toscano, V., Motta, C., De Leo, V., Petraglia, F., & Lenzi, A. (2017). Combined Oral Contraception and Bicalutamide in Polycystic Ovary Syndrome and Severe Hirsutism: A Double-Blind Randomized Controlled Trial. The Journal of Clinical Endocrinology & Metabolism, 103(3), 824–838. [DOI:10.1210/jc.2017-01186]
Nakamoto, J. (2016). Endocrine Testing. In Jameson, J. L., & De Groot, L. J. (Eds.). Endocrinology: Adult and Pediatric, 7th Edition (pp. 2655–2688.e1). Philadelphia: Saunders/Elsevier. [DOI:10.1016/B978-0-323-18907-1.00154-2]
Nakhjavani, M., Hamidi, S., Esteghamati, A., Abbasi, M., Nosratian-Jahromi, S., & Pasalar, P. (2009). Short term effects of spironolactone on blood lipid profile: a 3-month study on a cohort of young women with hirsutism. British Journal of Clinical Pharmacology, 68(4), 634–637. [DOI:10.1111/j.1365-2125.2009.03483.x]
Neyman, A., Fuqua, J. S., & Eugster, E. A. (2019). Bicalutamide as an Androgen Blocker With Secondary Effect of Promoting Feminization in Male-to-Female Transgender Adolescents. Journal of Adolescent Health, 64(4), 544–546. [DOI:10.1016/j.jadohealth.2018.10.296]
Nguyen, D., Marchese, M., Cone, E. B., Paciotti, M., Basaria, S., Bhojani, N., & Trinh, Q. (2021). Investigation of Suicidality and Psychological Adverse Events in Patients Treated With Finasteride. JAMA Dermatology, 157(1), 35–42. [DOI:10.1001/jamadermatol.2020.3385]
Nie, I., Wiepjes, C. M., Blok, C. J., Moorselaar, R. J., Pigot, G. L., Sluis, T. M., Barbé, E., Voorn, P., Mello, N. M., Huirne, J., & Heijer, M. (2021). Incidence of testicular cancer in trans women using gender‐affirming hormonal treatment: a nationwide cohort study. BJU International, 129(4), 491–497. [DOI:10.1111/bju.15575]
Nieschlag, E., Zitzmann, M., & Kamischke, A. (2003). Use of progestins in male contraception. Steroids, 68(10–13), 965–972. [DOI:10.1016/s0039-128x(03)00135-1]
Nieschlag, E. (2010). Clinical trials in male hormonal contraception. Contraception, 82(5), 457–470. [DOI:10.1016/j.contraception.2010.03.020]
Nieschlag, E., & Behre, H. M. (2012). The essential role of testosterone in hormonal male contraception. In Nieschlag, E., Behre, H. M., & Nieschlag, S. (Eds.). Testosterone: Action · Deficiency · Substitution, 4th Edition (pp. 470–493). Cambridge/New York: Cambridge University Press. [DOI:10.1017/cbo9781139003353.023]
Nishiyama, T. (2014). Serum testosterone levels after medical or surgical androgen deprivation: A comprehensive review of the literature. Urologic Oncology: Seminars and Original Investigations, 32(1), 38.e17–38.e28. [DOI:10.1016/j.urolonc.2013.03.007]
Nolan, B. J., & Cheung, A. S. (2021). Relationship Between Serum Estradiol Concentrations and Clinical Outcomes in Transgender Individuals Undergoing Feminizing Hormone Therapy: A Narrative Review. Transgender Health, 6(3), 125–131. [DOI:10.1089/trgh.2020.0077]
Nolan, B. J., Frydman, A. S., Leemaqz, S. Y., Carroll, M., Grossmann, M., Zajac, J. D., & Cheung, A. S. (2022). Effects of low-dose oral micronised progesterone on sleep, psychological distress, and breast development in transgender individuals undergoing feminising hormone therapy: a prospective controlled study. Endocrine Connections, 11(5), e220170. [DOI:10.1530/EC-22-0170]
Norman, A. W., & Henry, H. L. (2015). Androgens. In Norman, A. W., & Henry, H. L. Hormones, 3rd Edition (pp. 255–273). London: Academic Press/Elsevier. [DOI:10.1016/b978-0-08-091906-5.00012-4]
Norman, A. W., & Henry, H. L. (2015). Estrogens and Progestins. In Norman, A. W., & Henry, H. L. Hormones, 3rd Edition (pp. 275–296). London: Academic Press/Elsevier. [DOI:10.1016/b978-0-08-091906-5.00013-6]
Nota, N. M., Wiepjes, C. M., de Blok, C. J., Gooren, L. J., Peerdeman, S. M., Kreukels, B. P., & den Heijer, M. (2018). The occurrence of benign brain tumours in transgender individuals during cross-sex hormone treatment. Brain, 141(7), 2047–2054. [DOI:10.1093/brain/awy108]
North American Menopause Society. (2022). The 2022 hormone therapy position statement of The North American Menopause Society. Menopause, 29(7), 767–794. [DOI:10.1097/gme.0000000000002028]
O’Connell, M. B. (1995). Pharmacokinetic and Pharmacologic Variation Between Different Estrogen Products. The Journal of Clinical Pharmacology, 35(9S), 18S–24S. [DOI:10.1002/j.1552-4604.1995.tb04143.x]
Olsen, E. A., Hordinsky, M., Whiting, D., Stough, D., Hobbs, S., Ellis, M. L., Wilson, T., & Rittmaster, R. S. (2006). The importance of dual 5α-reductase inhibition in the treatment of male pattern hair loss: Results of a randomized placebo-controlled study of dutasteride versus finasteride. Journal of the American Academy of Dermatology, 55(6), 1014–1023. [DOI:10.1016/j.jaad.2006.05.007]
Plovanich, M., Weng, Q. Y., & Mostaghimi, A. (2015). Low Usefulness of Potassium Monitoring Among Healthy Young Women Taking Spironolactone for Acne. JAMA Dermatology, 151(9), 941–944. [DOI:10.1001/jamadermatol.2015.34]
Polyzos, S. A., Kountouras, J., Zavos, C., & Deretzi, G. (2011). Spironolactone Revisited. The Journal of Clinical Hypertension, 13(10), 783–784. [DOI:10.1111/j.1751-7176.2011.00484.x]
Powers, M. S., Schenkel, L., Darley, P. E., Good, W. R., Balestra, J. C., & Place, V. A. (1985). Pharmacokinetics and pharmacodynamics of transdermal dosage forms of 17β-estradiol: Comparison with conventional oral estrogens used for hormone replacement. American Journal of Obstetrics and Gynecology, 152(8), 1099–1106. [DOI:10.1016/0002-9378(85)90569-1]
Prince, J. C., & Safer, J. D. (2020). Endocrine treatment of transgender individuals: current guidelines and strategies. Expert Review of Endocrinology & Metabolism, 15(6), 395–403. [DOI:10.1080/17446651.2020.1825075]
Reiter, E. O., Mauras, N., McCormick, K., Kulshreshtha, B., Amrhein, J., De Luca, F., O’Brien, S., Armstrong, J., & Melezinkova, H. (2010). Bicalutamide plus Anastrozole for the Treatment of Gonadotropin-Independent Precocious Puberty in Boys with Testotoxicosis: A Phase II, Open-Label Pilot Study (BATT). Journal of Pediatric Endocrinology and Metabolism, 23(10), 999–1009. [DOI:10.1515/jpem.2010.161]
Rezende, H. D., Dias, M. F. R. G., & Trüeb, R. M. (2018). A Comment on the Post-Finasteride Syndrome. International Journal of Trichology, 10(6), 255–261. [PubMed] [PubMed Central] [DOI:10.4103/ijt.ijt_61_18]
Roberts, J. L., Fiedler, V., Imperato-McGinley, J., Whiting, D., Olsen, E., Shupack, J., Stough, D., DeVillez, R., Rietschel, R., Savin, R., Bergfeld, W., Swinehart, J., Funicella, T., Hordinsky, M., Lowe, N., Katz, I., Lucky, A., Drake, L., Price, V. H., Weiss, D., Whitmore, E., Millikan, L., Muller, S., Gencheff, C., Carrington, P., Binkowitz, B., Kotey, P., He, W., Bruno, K., Jacobsen, C., Terranella, L., Gormley, G. J., & Kaufman, K. D. (1999). Clinical dose ranging studies with finasteride, a type 2 5α-reductase inhibitor, in men with male pattern hair loss. Journal of the American Academy of Dermatology, 41(4), 555–563. [DOI:10.1016/s0190-9622(99)80052-8]
Roscioni, S. S., de Zeeuw, D., Bakker, S. J., & Lambers Heerspink, H. J. (2012). Management of hyperkalaemia consequent to mineralocorticoid-receptor antagonist therapy. Nature Reviews Nephrology, 8(12), 691–699. [DOI:10.1038/nrneph.2012.217]
Rose, A. J., Hughto, J. M., Dunbar, M. S., Quinn, E. K., Deutsch, M., Feldman, J., Radix, A., Safer, J. D., Shipherd, J. C., Thompson, J., & Jasuja, G. K. (2023). Trends in Feminizing Hormone Therapy for Transgender Patients, 2006–2017. Transgender Health, 8(2), 188–194. [DOI:10.1089/trgh.2021.0041]
Rosenfield, R. L., Cooke, D. W., & Radovick, S. (2008). Puberty and its disorders in the female. In Sperling, M. A. (Ed.). Pediatric Endocrinology, 3rd Edition (pp. 530–609). Philadelphia: Saunders. [Google Scholar] [Google Books] [OpenLibrary] [WorldCat]
Rosenfield, R. L., Cooke, D. W., & Radovick, S. (2021). Puberty in the Female and Its Disorders. In Sperling, M. A., Majzoub, J. A., Menon, R. K., & Stratakis, C. A. (Eds.). Sperling Pediatric Endocrinology, 5th Edition (pp. 528–626). Philadelphia: Elsevier. [DOI:10.1016/B978-0-323-62520-3.00016-6]
Samarasinghe, S., Meah, F., Singh, V., Basit, A., Emanuele, N., Emanuele, M. A., Mazhari, A., & Holmes, E. W. (2017). Biotin Interference with Routine Clinical Immunoassays: Understand the Causes and Mitigate the Risks. Endocrine Practice, 23(8), 989–998. [DOI:10.4158/ep171761.ra]
Schiller, C. E., Schmidt, P. J., & Rubinow, D. R. (2014). Allopregnanolone as a mediator of affective switching in reproductive mood disorders. Psychopharmacology, 231(17), 3557–3567. [DOI:10.1007/s00213-014-3599-x]
Schlatterer, K., Yassouridis, A., Werder, K. V., Poland, D., Kemper, J., & Stalla, G. K. (1998). Archives of Sexual Behavior, 27(5), 475–492. [DOI:10.1023/a:1018704630036]
Seaman, H. E., Langley, S. E., Farmer, R. D., & de Vries, C. S. (2007). Venous thromboembolism and cyproterone acetate in men with prostate cancer: a study using the General Practice Research Database. BJU International, 99(6), 1398–1403. [DOI:10.1111/j.1464-410x.2007.06859.x]
Shackleton, C. (2010). Clinical steroid mass spectrometry: A 45-year history culminating in HPLC–MS/MS becoming an essential tool for patient diagnosis. The Journal of Steroid Biochemistry and Molecular Biology, 121(3–5), 481–490. [DOI:10.1016/j.jsbmb.2010.02.017]
Shaw, J. C. (1996). Antiandrogen and hormonal treatment of acne. Dermatologic Clinics, 14(4), 803–811. [DOI:10.1016/s0733-8635(05)70405-8]
Slack, D., Krishnamurthy, N., Contreras-Castro, F., & Safer, J. D. (2023). Achieving Both Target Testosterone And Target Estradiol Levels May Not Be Practical In All Trans Feminine Users Of Estradiol - Which To Prioritize? Journal of the Endocrine Society, 7(Suppl 1), A1102–A1102 (abstract no. SAT404/bvad114.2075). [DOI:10.1210/jendso/bvad114.2075] [PubMed Central]
Sofer, Y., Yaish, I., Yaron, M., Bach, M. Y., Stern, N., & Greenman, Y. (2020). Differential Endocrine and Metabolic Effects of Testosterone Suppressive Agents in Transgender Women. Endocrine Practice, 26(8), 883–890. [DOI:10.4158/ep-2020-0032] [PDF]
SoRelle, J. A., Jiao, R., Gao, E., Veazey, J., Frame, I., Quinn, A. M., Day, P., Pagels, P., Gimpel, N., & Patel, K. (2019). Impact of Hormone Therapy on Laboratory Values in Transgender Patients. Clinical Chemistry, 65(1), 170–179. [DOI:10.1373/clinchem.2018.292730]
St-Jules, D. E., Goldfarb, D. S., & Sevick, M. A. (2016). Nutrient Non-equivalence: Does Restricting High-Potassium Plant Foods Help to Prevent Hyperkalemia in Hemodialysis Patients? Journal of Renal Nutrition, 26(5), 282–287. [DOI:10.1053/j.jrn.2016.02.005]
St-Jules, D. E., & Fouque, D. (2020). Is it time to abandon the nutrient-based renal diet model? Nephrology Dialysis Transplantation, 36(4), 574–577. [DOI:10.1093/ndt/gfaa257]
St-Jules, D. E., & Fouque, D. (2022). Etiology-based dietary approach for managing hyperkalemia in people with chronic kidney disease. Nutrition Reviews, 80(11), 2198–2205. [DOI:10.1093/nutrit/nuac026]
Stanczyk, F. Z., & Clarke, N. J. (2010). Advantages and challenges of mass spectrometry assays for steroid hormones. The Journal of Steroid Biochemistry and Molecular Biology, 121(3–5), 491–495. [DOI:10.1016/j.jsbmb.2010.05.001]
Stanczyk, F. Z., Hapgood, J. P., Winer, S., & Mishell, D. R. (2012). Progestogens Used in Postmenopausal Hormone Therapy: Differences in Their Pharmacological Properties, Intracellular Actions, and Clinical Effects. Endocrine Reviews, 34(2), 171–208. [DOI:10.1210/er.2012-1008]
Stanczyk, F. Z., Mathews, B. W., & Cortessis, V. K. (2017). Does the type of progestin influence the production of clotting factors? Contraception, 95(2), 113–116. [DOI:10.1016/j.contraception.2016.07.007]
Stege, R., Gunnarsson, P. O., Johansson, C., Olsson, P., Pousette, Å., & Carlström, K. (1996). Pharmacokinetics and testosterone suppression of a single dose of polyestradiol phosphate (Estradurin®) in prostatic cancer patients. The Prostate, 28(5), 307–310. [DOI:10.1002/(sici)1097-0045(199605)28:5<307::aid-pros6>3.0.co;2-8]
Steinberger, E., Ayala, C., Hsi, B., Smith, K. D., Rodriguez-Rigau, L. J., Weidman, E. R., & Reimondo, G. G. (1998). Utilization of Commercial Laboratory Results in Management of Hyperandrogenism in Women. Endocrine Practice, 4(1), 1–10. [DOI:10.4158/ep.4.1.1]
Sterling, J., & Garcia, M. M. (2020). Cancer screening in the transgender population: a review of current guidelines, best practices, and a proposed care model. Translational Andrology and Urology, 9(6), 2771–2785. [DOI:10.21037/tau-20-954]
Strauss, J. F., & FitzGerald, G. A. (2019). Steroid Hormones and Other Lipid Molecules Involved in Human Reproduction. In Strauss, J. F., & Barbieri, R. L. (Eds.). Yen and Jaffe’s Reproductive Endocrinology: Physiology, Pathophysiology, and Clinical Management, 8th Edition (pp. 75–114.e7). Philadelphia: Elsevier. [Google Books] [DOI:10.1016/b978-0-323-47912-7.00004-4]
Stricker, R., Eberhart, R., Chevailler, M., Quinn, F. A., Bischof, P., & Stricker, R. (2006). Establishment of detailed reference values for luteinizing hormone, follicle stimulating hormone, estradiol, and progesterone during different phases of the menstrual cycle on the Abbott ARCHITECT® analyzer. Clinical Chemistry and Laboratory Medicine (CCLM), 44(7), 883–887. [DOI:10.1515/cclm.2006.160]
Styne, D. M. (2016). Laboratory Values for Pediatric Endocrinology. In Styne, D. M. Pediatric Endocrinology: A Clinical Handbook (pp. 385–434). Cham: Springer International Publishing. [DOI:10.1007/978-3-319-18371-8_16]
Sudduth, S. L., & Koronkowski, M. J. (1993). Finasteride: The First 5α-Reductase Inhibitor. Pharmacotherapy: The Journal of Human Pharmacology and Drug Therapy, 13(4), 309–329. [DOI:10.1002/j.1875-9114.1993.tb02739.x]
Sundström-Poromaa, I., Comasco, E., Sumner, R., & Luders, E. (2020). Progesterone – Friend or foe? Frontiers in Neuroendocrinology, 59, 100856. [DOI:10.1016/j.yfrne.2020.100856]
Swerdloff, R. S., Dudley, R. E., Page, S. T., Wang, C., & Salameh, W. A. (2017). Dihydrotestosterone: Biochemistry, Physiology, and Clinical Implications of Elevated Blood Levels. Endocrine Reviews, 38(3), 220–254. [DOI:10.1210/er.2016-1067]
T’Sjoen, G. G., Beguin, Y., Feyen, E., Rubens, R., Kaufman, J., & Gooren, L. (2005). Influence of exogenous oestrogen or (anti-) androgen administration on soluble transferrin receptor in human plasma. Journal of Endocrinology, 186(1), 61–67. [DOI:10.1677/joe.1.06112]
T’Sjoen, G., Arcelus, J., Gooren, L., Klink, D. T., & Tangpricha, V. (2018). Endocrinology of Transgender Medicine. Endocrine Reviews, 40(1), 97–117. [DOI:10.1210/er.2018-00011]
Tack, L. J., Heyse, R., Craen, M., Dhondt, K., Bossche, H. V., Laridaen, J., & Cools, M. (2017). Consecutive Cyproterone Acetate and Estradiol Treatment in Late-Pubertal Transgender Female Adolescents. The Journal of Sexual Medicine, 14(5), 747–757. [DOI:10.1016/j.jsxm.2017.03.251]
Thompson, J., Hopwood, R. A., deNormand, S., & Cavanaugh, T. (2021). Medical Care of Trans and Gender Diverse Adults. Boston: Fenway Health. [URL] [PDF]
Toorians, A. W., Thomassen, M. C., Zweegman, S., Magdeleyns, E. J., Tans, G., Gooren, L. J., & Rosing, J. (2003). Venous Thrombosis and Changes of Hemostatic Variables during Cross-Sex Hormone Treatment in Transsexual People. The Journal of Clinical Endocrinology & Metabolism, 88(12), 5723–5729. [DOI:10.1210/jc.2003-030520]
Traish, A. M., Krakowsky, Y., Doros, G., & Morgentaler, A. (2019). Do 5α-Reductase Inhibitors Raise Circulating Serum Testosterone Levels? A Comprehensive Review and Meta-Analysis to Explaining Paradoxical Results. Sexual Medicine Reviews, 7(1), 95–114. [DOI:10.1016/j.sxmr.2018.06.002]
Traish, A. M. (2020). Post-finasteride syndrome: a surmountable challenge for clinicians. Fertility and Sterility, 113(1), 21–50. [DOI:10.1016/j.fertnstert.2019.11.030]
Treleaven, M. M., Jackowich, R. A., Roberts, L., Wassersug, R. J., & Johnson, T. (2013). Castration and personality: Correlation of androgen deprivation and estrogen supplementation with the Big Five factor personality traits of adult males. Journal of Research in Personality, 47(4), 376–379. [DOI:10.1016/j.jrp.2013.03.005]
Usach, I., Martinez, R., Festini, T., & Peris, J. (2019). Subcutaneous Injection of Drugs: Literature Review of Factors Influencing Pain Sensation at the Injection Site. Advances in Therapy, 36(11), 2986–2996. [DOI:10.1007/s12325-019-01101-6]
van Zuuren, E. J., Fedorowicz, Z., Carter, B., & Pandis, N. (2015). Interventions for hirsutism (excluding laser and photoepilation therapy alone). Cochrane Database of Systematic Reviews, 2015, CD010334. [DOI:10.1002/14651858.cd010334.pub2]
Verdonk, S. J., Vesper, H. W., Martens, F., Sluss, P. M., Hillebrand, J. J., & Heijboer, A. C. (2019). Estradiol reference intervals in women during the menstrual cycle, postmenopausal women and men using an LC-MS/MS method. Clinica Chimica Acta, 495, 198–204. [DOI:10.1016/j.cca.2019.04.062]
Vermeulen, A., Giagulli, V., De Schepper, P., & Buntinx, A. (1991). Hormonal Effects of a 5α-Reductase Inhibitor (Finasteride) onHormonal Levels in Normal Men and in Patients withBenign Prostatic Hyperplasia. European Urology, 20(1), 82–86. [DOI:10.1159/000471752]
Vihtamäki, T., Luukkaala, T., & Tuimala, R. (2004). Skin contamination by oestradiol gel—a remarkable source of error in plasma oestradiol measurements during percutaneous hormone replacement therapy. Maturitas, 48(4), 347–353. [DOI:10.1016/s0378-5122(03)00043-4]
Wang, H., Liu, M., Fu, Q., & Deng, C. (2019). Pharmacokinetics of hard micronized progesterone capsules via vaginal or oral route compared with soft micronized capsules in healthy postmenopausal women: a randomized open-label clinical study. Drug Design, Development and Therapy, 13, 2475–2482. [DOI:10.2147/dddt.s204624]
Wang, Y., & Lipner, S. R. (2020). Retrospective analysis of adverse events with spironolactone in females reported to the United States Food and Drug Administration. International Journal of Women’s Dermatology, 6(4), 272–276. [DOI:10.1016/j.ijwd.2020.05.002]
Weill, A., Nguyen, P., Labidi, M., Cadier, B., Passeri, T., Duranteau, L., Bernat, A., Yoldjian, I., Fontanel, S., Froelich, S., & Coste, J. (2021). Use of High Dose Cyproterone Acetate and Risk of Intracranial Meningioma in Women: Cohort Study. BMJ, 372, n37. [DOI:10.1136/bmj.n37]
Welk, B., McArthur, E., Ordon, M., Anderson, K. K., Hayward, J., & Dixon, S. (2017). Association of Suicidality and Depression With 5α-Reductase Inhibitors. JAMA Internal Medicine, 177(5), 683–691. [DOI:10.1001/jamainternmed.2017.0089]
Wellington, K., & Keam, S. J. (2006). Bicalutamide 150mg: A Review of its Use in the Treatment of Locally Advanced Prostate Cancer. Drugs, 66(6), 837–850. [DOI:10.2165/00003495-200666060-00007]
Willemsen, W. N., Mastboom, J. L., Thomas, C. M., & Rolland, R. (1985). Absorption of 17β-estradiol in a neovagina constructed from the peritoneum. European Journal of Obstetrics & Gynecology and Reproductive Biology, 19(4), 247–253. [DOI:10.1016/0028-2243(85)90036-x]
Wilson, L. M., Baker, K. E., Sharma, R., Dukhanin, V., McArthur, K., & Robinson, K. A. (2020). Effects of antiandrogens on prolactin levels among transgender women on estrogen therapy: A systematic review. International Journal of Transgender Health, 21(4), 391–402. [DOI:10.1080/15532739.2020.1819505]
Wu, B., Shen, P., Yin, X., Yu, L., Wu, F., Chen, C., Li, J., & Xu, T. (2022). Analysis of adverse event of interstitial lung disease in men with prostate cancer receiving hormone therapy using the Food and Drug Administration Adverse Event Reporting System. British Journal of Clinical Pharmacology, 89(2), 440–448. [DOI:10.1111/bcp.15336]
Wu, F. C., Balasubramanian, R., Mulders, T. M., & Coelingh-Bennink, H. J. (1999). Oral Progestogen Combined with Testosterone as a Potential Male Contraceptive: Additive Effects between Desogestrel and Testosterone Enanthate in Suppression of Spermatogenesis, Pituitary-Testicular Axis, and Lipid Metabolism. The Journal of Clinical Endocrinology & Metabolism, 84(1), 112–122. [DOI:10.1210/jcem.84.1.5412]
Yaish, I., Gindis, G., Greenman, Y., Moshe, Y., Arbiv, M., Buch, A., Sofer, Y., Shefer, G., & Tordjman, K. (2023). Sublingual Estradiol Offers No Apparent Advantage Over Combined Oral Estradiol and Cyproterone Acetate for Gender-Affirming Hormone Therapy of Treatment-Naive Trans Women: Results of a Prospective Pilot Study. Transgender Health, 8(6), 485–493. [DOI:10.1089/trgh.2023.0022]
Zaenglein, A. L., Pathy, A. L., Schlosser, B. J., Alikhan, A., Baldwin, H. E., Berson, D. S., Bowe, W. P., Graber, E. M., Harper, J. C., Kang, S., Keri, J. E., Leyden, J. J., Reynolds, R. V., Silverberg, N. B., Stein Gold, L. F., Tollefson, M. M., Weiss, J. S., Dolan, N. C., Sagan, A. A., Stern, M., Boyer, K. M., & Bhushan, R. (2016). Guidelines of care for the management of acne vulgaris. Journal of the American Academy of Dermatology, 74(5), 945–973.e33. [DOI:10.1016/j.jaad.2015.12.037]
Zhang, J., & Stanczyk, F. Z. (2013). LC-MS Bioanalysis of Steroids. In Li, W., Zhang, J., & Tse, F. L. S. (Eds.). Handbook of LC-MS Bioanalysis: Best Practices, Experimental Protocols, and Regulations (pp. 573–590). Hoboken, New Jersey: John Wiley & Sons. [DOI:10.1002/9781118671276.ch45]
Zhou, Z., Song, S., Gao, Z., Wu, J., Ma, J., & Cui, Y. (2019). The efficacy and safety of dutasteride compared with finasteride in treating men with androgenetic alopecia: a systematic review and meta-analysis. Clinical Interventions in Aging, 14, 399–406. [DOI:10.2147/cia.s192435]
Zitzmann, M., Rohayem, J., Raidt, J., Kliesch, S., Kumar, N., Sitruk-Ware, R., & Nieschlag, E. (2017). Impact of various progestins with or without transdermal testosterone on gonadotropin levels for non-invasive hormonal male contraception: a randomized clinical trial. Andrology, 5(3), 516–526. [DOI:10.1111/andr.12328]
Zuuren, E., & Fedorowicz, Z. (2016). Interventions for hirsutism excluding laser and photoepilation therapy alone: abridged Cochrane systematic review including GRADE assessments. British Journal of Dermatology, 175(1), 45–61. [DOI:10.1111/bjd.14486]
\ No newline at end of file
+An Introduction to Hormone Therapy for Transfeminine People - Transfeminine Science
An Introduction to Hormone Therapy for Transfeminine People
By Aly | First published August 4, 2018 | Last modified May 8, 2025
Abstract / TL;DR
Sex hormones such as estrogen, testosterone, and progesterone are produced by the gonads. The sex hormones mediate the development of the secondary sexual characteristics. Testosterone causes masculinization, while estradiol causes feminization and breast development. Males have high amounts of testosterone, while females have low testosterone but high amounts of estradiol. These hormonal differences are responsible for the physical differences between males and females. Sex hormones and other hormonal medications are used in transfeminine people to shift the hormonal profile from a male-typical one to a female-typical profile. This causes feminization and demasculinization and allows for alleviation of gender dysphoria. The changes caused by transfeminine hormone therapy occur over a period of months to years. There are many different types and forms of hormonal medications, and these medications can be administered by a variety of different routes. Examples include as pills taken by mouth, as patches or gel applied to the skin, and as injections, among others. Different hormonal medications, routes, and doses have differences in efficacy, side effects, risks, costs, convenience, and availability. Hormone therapy should ideally be regularly monitored in transfeminine people with blood tests to ensure effectiveness and safety and to allow for adjustment as necessary.
The Sex Hormones
Types and Effects
The sex hormones include the estrogens (E), progestogens (P), and androgens. A person’s hormonal profile is a product of the type of gonads that they are born with. Natal males have testes while natal females have ovaries. Testes produce large amounts of androgens and small amounts of estrogens whereas ovaries produce high amounts of estrogens and progesterone and low amounts of androgens.
Progestogens have essentially no known role in feminization or pubertal breast development. Rather than acting as mediators of feminization, progestogens have important effects in the female reproductive system and are essential hormones during pregnancy (Wiki). They also oppose the actions of estrogens in certain parts of the body, such as the uterus, vagina, and breasts (Wiki).
In addition to their effects on the body, sex hormones have actions in the brain. These actions influence cognition, emotions, and behavior. For instance, androgens produce pronounced sexual desire and arousal (including spontaneous erections) in men, while estrogens appear to be the major hormones responsible for sexual desire in women (Cappelletti & Wallen, 2016). As another example, testosterone levels have been negatively associated with agreeableness, whereas estrogen levels have been positively associated with this characteristic (Treleaven et al., 2013). Sex hormones also have important effects on health, which can be both positive and negative. For instance, estrogens maintain bone strength and likely protect against heart disease in cisgender women (NAMS, 2022), but also increase the risk of breast cancer (Aly, 2020) and can increase the risk of blood clots (Aly, 2020).
Estrogens, progestogens, and androgens also have antigonadotropic effects. That is, they inhibit the gonadotropin-releasing hormone (GnRH)-induced secretion of the gonadotropins, luteinizing hormone (LH) and follicle-stimulating hormone (FSH), from the pituitary gland in the brain. The gonadotropins signal the gonads to make sex hormones and to supply the sperm and egg cells necessary for fertility. Hence, lower levels of the gonadotropins will result in reduced gonadal sex hormone production and diminished fertility. If gonadotropin levels are sufficiently suppressed, the gonads will no longer make sex hormones at all and fertility will cease. The vast majorities of the quantities of estradiol, testosterone, and progesterone in the body are produced by the gonads. Most of the small remaining amounts of these hormones are produced via the adrenal glands of the kidneys.
Normal Hormone Levels
In cisgender females, the sex hormones are largely absent during childhood, gradually ramp up in production in late childhood and adolescence, are present in a cyclical manner during adulthood, and then largely stop being produced following the menopause. Hormone levels vary substantially but in a predictable manner during the normal menstrual cycle in adult premenopausal women. The menstrual cycle lasts about 28 days on average and consists of the following parts:
Luteal phase—latter half of the cycle or days 14–28
Hormone levels during the menstrual cycle are shown in the following graph:
Figure 1: Median estradiol and progesterone levels throughout the menstrual cycle in premenopausal cisgender women (Stricker et al., 2006; Abbott, 2009). The horizontal dashed lines are the average levels over the spanned periods. Other figures available elsewhere show variation between individuals (Graph; Graph; Graph).
As can be seen in the graph, estradiol levels are relatively low and progesterone levels are very low during the follicular phase; estradiol but not progesterone levels briefly surge to very high levels and trigger ovulation during mid-cycle; and estradiol and progesterone levels both undergo a bump and are relatively high during the luteal phase (though estradiol is not as high as during the mid-cycle peak).
The table below shows the circulating levels and production rates of estradiol, progesterone, and testosterone in women and men and allows for comparison between them.
Table 1: Ranges for circulating levelsa and estimated production ratesb of the major sex hormones:
Mean integrated estradiol levels are around 100 pg/mL (367 pmol/L) in premenopausal women and around 25 pg/mL (92 pmol/L) in men. The 95% range for mean estradiol levels in women is around 50 to 250 pg/mL (180–918 pmol/L) (e.g., Abbott, 2009 (Graph); Verdonk et al., 2019 (Graph)). The average production of estradiol by the ovaries in premenopausal women is about 6 mg over the course of one menstrual cycle (i.e., one month) (Rosenfield et al., 2008). This corresponds to a mean rate of about 200 μg/day. Estradiol levels increase slowly during normal female puberty, when breast development and feminization take place. Mean estradiol levels during the different stages of female puberty are quite low—less than about 50 to 60 pg/mL (180–220 pmol/L) until late puberty (Aly, 2020). In postmenopausal women, whose ovaries no longer produce considerable quantities of estrogens, estradiol levels are generally less than 10 to 20 pg/mL (37–73 pmol/L) (Nakamoto, 2016). Estradiol levels below 50 pg/mL (184 pmol/L) in adults are concentration-dependently associated with menopausal symptoms, including hot flashes, depressive mood changes, defeminization (e.g., breast atrophy, loss of feminine fat distribution), accelerated skin aging, and bone density loss with increased risk of bone fracture.
Mean testosterone levels are around 30 ng/dL (1.0 nmol/L) in women and 600 ng/dL (21 nmol/L) in men. Based on these values, testosterone levels are on average about 20-fold higher in men than in women. In men who have undergone gonadectomy (castration or surgical gonadal removal), testosterone levels are similar to those in women (<50 ng/dL [1.7 nmol/L]) (Nishiyama, 2014; Itty & Getzenberg, 2020). The mean or median levels of testosterone in women with polycystic ovary syndrome (PCOS), who often have clinically significant symptoms of androgen excess (e.g., excessive facial/body hair growth), range from 41 to 75 ng/dL (1.4–2.6 nmol/L) per different studies (Balen et al., 1995; Steinberger et al., 1998; Legro et al., 2010; Loh et al., 2020). Hence, it appears that even testosterone levels that are marginally elevated relative to normal female levels may produce undesirable androgenic effects.
The goal of hormone therapy for transfeminine people, otherwise known as feminizing hormone therapy (FHT) or (more in the past) as male-to-female (MtF) hormone replacement therapy (HRT), is to produce feminization and demasculinization of the body as well as alleviation of gender dysphoria. Medication therapy with sex hormones and other sex-hormonal medications is used to mediate these changes. Transfeminine people are given estrogens, progestogens, and antiandrogens (AAs) to supersede gonadal sex hormone production and shift the hormonal profile from male-typical to female-typical.
Transfeminine hormone therapy aims to achieve estradiol and testosterone levels within the normal female range. Commonly recommended ranges for transfeminine people in the literature are 100 to 200 pg/mL (367–734 pmol/L) for estradiol levels and less than 50 ng/dL (1.7 nmol/L) for testosterone levels (Table). However, higher estradiol levels of more than 200 pg/mL (734 pmol/L) can be useful in transfeminine hormone therapy to help suppress testosterone levels. Lower estradiol levels (≤50–60 pg/mL [≤180–220 pmol/L]) are recommended and more appropriate for pubertal and adolescent transfeminine individuals. Sex hormone levels in the blood can be measured with blood tests, in which blood is drawn from a vein using a needle and then analyzed in a laboratory. This is useful in transfeminine people to ensure that the hormonal profile has been satisfactorily altered in line with therapeutic goals—specifically that hormone levels are within female ranges.
Gonadal Suppression
At sufficiently high exposure, estrogens and androgens are able to completely suppress gonadal sex hormone production, while progestogens by themselves are able to partially but substantially suppress gonadal sex hormone production. More specifically, studies in cisgender men and transfeminine people have found that estradiol levels of around 200 pg/mL (734 pmol/L) suppress testosterone levels by about 90% on average (to ~50 ng/dL [1.7 nmol/L]), while estradiol levels of around 500 pg/mL (1,840 pmol/L) suppress testosterone levels by about 95% on average (to ~20–30 ng/dL [0.7–1.0 nmol/L]) (Gooren et al., 1984 [Graph]; Herndon et al., 2023 [Discussion]; Wiki; Graphs). Estradiol levels of below 200 pg/mL (734 pmol/L) also suppress testosterone levels, although to a reduced extent compared to higher levels (Aly, 2019; Krishnamurthy et al., 2023; Slack et al., 2023). In one large study in transfeminine people, the rates of adequate testosterone suppression (to testosterone levels of <50 ng/dL or <1.7 nmol/L) were 24% of individuals at estradiol levels of <100 pg/mL (367 pmol/L), 58% at 100 to 200 pg/mL (367–734 pmol/L), and 77% at >200 pg/mL (>734 pmol/L) (Krishnamurthy et al., 2023).
Figure 2: Estradiol and testosterone levels after a single injection of 320 mg polyestradiol phosphate (PEP) (a long-acting prodrug of estradiol) in men with prostate cancer (Stege et al., 1996). The maximal decrease in testosterone levels occurred with estradiol levels of greater than 200 pg/mL (734 pmol/L) and was about 90% (to roughly 50 ng/dL [1.7 nmol/L]). This figure demonstrates the ability of estradiol to concentration-dependently suppress gonadal testosterone production and circulating testosterone levels in people with testes.
Progestogens on their own are able to maximally suppress testosterone levels by about 50 to 70% (to ~150–300 ng/dL [5.2–10.4 nmol/L] on average) (Aly, 2019; Wiki). In combination with relatively small amounts of estrogen however, there is synergism in the antigonadotropic effect—the suppression of gonadal testosterone production with maximally effective doses of progestogens becomes complete, and testosterone levels are reduced by about 95% (to ~20–30 ng/dL [0.7–1.0 nmol/L]) (Aly, 2019). Hence, the combination of an estrogen and a progestogen can be used to achieve maximal testosterone suppression at lower doses than would be necessary if an estrogen or progestogen were used alone.
The antigonadotropic effects of estrogens and progestogens are taken advantage of in transfeminine hormone therapy to suppress gonadal testosterone production and attain testosterone levels that are more consistent with those in cisgender women. It should be noted that the preceding numbers on testosterone suppression with estrogens and progestogens are averages and there is significant variation between individuals in terms of testosterone suppression. In other words, some may need more or less in terms of hormonal dosages to achieve the same decrease in testosterone levels.
Effects and Timeline
During normal puberty in both males and females, sex hormone exposure increases slowly over a period of several years (Aly, 2020). In relation to this, sexual maturation occurs gradually during normal puberty. In non-adolescent transgender people, adult or higher amounts of hormones are generally administered right away, and this can result in changes in secondary sex characteristics happening more quickly. Most of the effects of feminizing hormone therapy in transfeminine people onset within 1 to 6 months of commencing treatment and complete within 1 to 3 years. The table below is reproduced from literature sources with slight modification and is commonly cited as a timeline of the effects (Table). It is based on a mixture of anecdotal clinical experience, expert opinion, and available clinical studies of hormone therapy in transfeminine people. Due to limited research characterizing the effects of transfeminine hormone therapy at present, the table may or may not be completely accurate.
Table 2: Effects of hormone therapy at typical doses in adult transfeminine people (Wiki):
Effect
Onseta
Completiona
Permanency
Breast development
2–6 months
2–3 years
Permanent
Reduced and slowed growth of facial and body hair
3–12 months
>3 yearsb
Reversible
Cessation and reversal of scalp hair loss
1–3 months
1–2 years
Reversible
Softening of skin and decreased skin oiliness and acne
3–6 months
Unknown
Reversible
Redistribution of body fat in a feminine pattern
3–6 months
2–5 years
Reversible
Decreased muscle mass and strength
3–6 months
1–2 yearsc
Reversible
Widening and rounding of the pelvisd
Unknown
Unknown
Permanent
Changes in mood, emotionality, and behavior
Immediate
Unknown
Reversible
Decreased sex drive and spontaneous erections
1–3 months
3–6 months
Reversible
Erectile dysfunction and decreased ejaculate volume
1–3 months
Variable
Reversible
Decreased sperm production and infertility
Unknown
>3 years
Mixede
Decreased testicular volume
3–6 months
2–3 years
Unknown
Voice changes (e.g., decreased pitch/resonance)
Nonef
N/A
N/A
a May vary significantly between individuals due to factors like genetics, diet/nutrition, hormone levels, etc. b Hormone therapy usually has little influence on facial hair density in transfeminine people. Complete removal of facial and body hair can be achieved with laser hair removal and electrolysis. Temporary hair removal can be achieved with shaving, epilating, waxing, and other methods. c May vary significantly depending on amount of physical exercise. d Occurs only in young individuals who have not yet completed growth plate closure (may not occur at all in post-adolescent people). e Only estrogens, particularly at high doses, seem to have the potential for long-lasting or irreversible infertility; impaired fertility caused by antiandrogens is usually readily reversible with discontinuation. fVoice training can be an effective means of feminizing the voice.
Breast Development
Breast development is among the most anticipated effects of hormone therapy in transfeminine people (Masumori et al., 2021; Grock et al., 2024). This relates to the key significance of breasts as a feminine characteristic, component of sexual attractiveness, and signal of sex and gender. Breast growth in transfeminine people usually starts within 1 to 6 months and completes over a period of 1 to 3 years (e.g., de Blok et al., 2021). The developed breasts of transfeminine people are highly variable in terms of size and shape, as with natal women (de Blok et al., 2021). Based on available high-quality clinical studies, transfeminine people tend to have much smaller mature breasts than those of natal women on average, and this appears to be the case regardless of hormonal regimen or age at which hormone therapy is commenced (e.g., de Blok et al., 2021; Boogers et al., 2025). The reasons for this are unknown, but one key possibility, observed in animals, is that prenatal androgen exposure limits subsequent breast growth potential. Despite usually modest breast development, many transfeminine people still express overall satisfaction with their breasts (de Blok et al., 2021; Boogers et al., 2025).
Beyond ensuring adequate testosterone suppression and maintaining sufficient estradiol levels above a specific low threshold, there are currently no known or substantiated methods to permanently enhance or optimize breast development. However, research suggests that avoiding high or excessive doses of estradiol and progestogens may be beneficial. In addition, high levels of estradiol, progesterone, and/or prolactin, as with the normal menstrual cycle and pregnancy, are known to induce temporary and reversible breast tenderness and enlargement, for instance due to local fluid retention and lobuloalveolar maturation (Aly, 2020). However, the breast size increases are modest, and high hormone levels come with health risks (Aly, 2020). Surgical breast augmentation is an option to increase breast size if it is unsatisfactory. Some transfeminine people, for instance many non-binary individuals, may wish to avoid or minimize breast growth, and there are possible therapeutic approaches in this area (Aly, 2019).
Additional review content on breast development in transfeminine people exists on this site (e.g., Aly, 2020; Aly, 2020). Breast growth can be measured and tracked with a variety of methods for individuals who are interested in monitoring their progress (Wiki). Photographs and timelines of breast development and feminization with hormone therapy in transfeminine people are available in communities like r/TransTimelines and r/TransBreastTimelines on the social media website Reddit.
Specific Hormonal Medications
The medications that are used in transfeminine hormone therapy include estrogens, progestogens, and antiandrogens. Estrogens produce feminization and testosterone suppression. Progestogens and antiandrogens do not mediate feminization themselves but further suppress and/or block testosterone. Testosterone suppression causes demasculinization and disinhibition of estrogen-mediated feminization. Androgens are sometimes used at low doses in transfeminine people who have low testosterone levels, although they are not required and benefits are uncertain. There are many different types of these hormonal medications available for transfeminine hormone therapy, with different benefits and risks.
Estrogens, progestogens, and antiandrogens are available in a variety of different formulations and for use by many different routes of administration in transfeminine people. The route of administration influences the absorption, distribution, metabolism, and elimination of the hormone in the body, resulting in significant differences between routes in terms of bioavailability, hormone levels in blood and specific tissues, and patterns of metabolites. These differences can have important therapeutic consequences.
Table 3: Major routes of administration of hormonal medications for transfeminine people:
Insertion via surgical incision into fat under skin
Pellet
Vaginal administration is a major additional route of administration of hormonal medications in cisgender women. While vaginal administration via a natal vagina is of course not possible in transfeminine people, neovaginal administration is a possiblility in those who have undergone vaginoplasty. However, the lining of the neovagina is not the vaginal epithelium of natal females but instead is usually skin or colon—depending on the type of vaginoplasty performed (penile inversion or sigmoid colon vaginoplasty, respectively). For this reason, neovaginal administration in transfeminine people is likely more similar in its properties to transdermal and rectal administration—depending on the type of neovagina—than to vaginal administration in cisgender women. It is noteworthy that the vaginal and rectal routes are said to be similar in their properties for hormonal medications however (Goletiani, Keith, & Gorsky, 2007; Wiki). Moreover, absorption of estradiol via neovaginas constructed from peritoneum (internal abdominal lining)—a less commonly employed vaginoplasty approach in transfeminine people—was reported in one study to be similar to that with vaginal administration of estradiol in cisgender women (Willemsen et al., 1985). As such, neovaginal administration may be an additional possible route for certain transfeminine people depending on the circumstances. However, this route still remains to be more adequately characterized.
An often-encountered question from people who take hormonal medications is whether there is an optimal time of the day to take them (Colonnello et al., 2025). As of present, there is little research in this area, and the answer to the question is essentially unknown (Colonnello et al., 2025). In any case, there is currently no evidence or persuasive theoretical basis to favor specific times of day to take these medications (Colonnello et al., 2025). In all likelihood, it makes little or no difference.
Estrogens
Estradiol, the primary bioidentical form normally found in the human body, is the main estrogen that is used in transfeminine hormone therapy. Estradiol hemihydrate (EH) is another form that is essentially identical to and interchangeable with estradiol. Estradiol esters are also sometimes used in place of estradiol. They are prodrugs of estradiol (i.e., are converted into estradiol in the body) and have essentially identical biological activity to estradiol. However, they have longer durations when used by injection due to slower absorption from the injection site, and this allows them to be administered less often. Some examples of major estradiol esters include estradiol valerate (EV; Progynova, Progynon Depot, Delestrogen) and estradiol cypionate (EC; Depo-Estradiol). Polyestradiol phosphate (PEP; Estradurin) is an injectable estradiol prodrug in the form of a polymer (i.e., linked chain of estradiol molecules) which is metabolized slowly and has a very long duration.
Non-bioidentical estrogens such as ethinylestradiol (EE; found in birth control pills), conjugated estrogens (CEEs; Premarin; used in menopausal hormone therapy), and diethylstilbestrol (DES; widely used previously but now abandoned) are resistant to metabolism in the liver and have disproportionate effects on estrogen-modulated liver synthesis when compared to bioidentical estrogens like estradiol (Aly, 2020). As a result, they have stronger influence on coagulation and greater risk of certain health problems like blood clots and associated cardiovascular issues (Aly, 2020). For this reason, as well as the fact that relatively high doses of estrogens may be needed for testosterone suppression, non-bioidentical estrogens should ideally never be used in transfeminine hormone therapy.
Estradiol dose-dependently suppresses testosterone levels in people with testes. Physiological and guideline-based levels of estradiol (<200 pg/mL or <734 pmol/L) are often not sufficient to suppress testosterone levels into the female range in transfeminine people who have not had their gonads removed (e.g., Liang et al., 2018; Krishnamurthy et al., 2023; Slack et al., 2023). As a result, estradiol is generally used in combination with an antiandrogen or progestogen in transfeminine hormone therapy (Hembree et al., 2017; Coleman et al., 2022; Rose et al., 2023). This results in partial suppression of testosterone levels by estradiol and further suppression or blockade of the remaining testosterone by the antiandrogen or progestogen. While combination therapy can be effective in fully suppressing or blocking testosterone (e.g., Aly, 2019; Aly, 2020), testosterone suppression can also still remain incomplete with antiandrogens and progestogens in certain forms (e.g., Aly, 2018; Jain, Kwan, & Forcier, 2019). In contrast to physiological estradiol levels, supraphysiological levels of estradiol are able to consistently and fully suppress testosterone levels into the normal female range with estradiol alone in transfeminine people (e.g., Gooren et al., 1984 [Graph]; Igo & Visram, 2021; Herndon et al., 2023 [Discussion]). This alternative approach, often referred to as high-dose estradiol monotherapy, has the advantage of avoiding the side effects, risks, and costs of antiandrogens and progestogens. However, it has the disadvantage of exposure to supraphysiological estradiol levels that are above those recommended by guidelines and that may have greater health risks. Physiological estradiol doses and combination therapy are more often used in transfeminine people treated by clinicians, whereas high-dose estradiol monotherapy is more frequently encountered in transfeminine people on DIY hormone therapy.
The feminizing effects of estradiol appear to be maximal at relatively low levels in the absence of androgens. Higher doses of estradiol and supraphysiological estradiol levels, aside from allowing for greater testosterone suppression, are not known to result in better feminization in transfeminine people (Deutsch, 2016; Nolan & Cheung, 2021). In fact, there is some indication that higher estrogen doses early into hormone therapy could actually result in worse breast development. Hence, the therapeutic emphasis in transfeminine hormone therapy is more on testosterone suppression than on achieving a specific estradiol level, at least above a certain low threshold level. Higher doses of estrogens, including of estradiol, also have a greater risk of adverse health effects such as blood clots and cardiovascular problems (Aly, 2020). As such, the use of physiological doses of estradiol is optimal in transfeminine people. At the same time however, high estrogen doses can be useful for improving testosterone suppression when it is inadequate, and the absolute risks, in the case of non-oral bioidentical estradiol, are low and are more important in people with specific risk factors (e.g., older age, physical inactivity, obesity, concomitant progestogen use, smoking, surgery, and rare thrombophilic abnormalities). If more adequate testosterone suppression is necessary, limitedly supraphysiological doses of non-oral estradiol may have a reasonable ratio of benefit to risk in this context, at least in those without relevant risk factors for estrogen-related complications (e.g., many healthy young people) (Aly, 2020).
Estradiol and estradiol esters are usually used orally, sublingually, transdermally, by injection (intramuscularly or subcutaneously), or by implant in transfeminine hormone therapy (Wiki).
Oral Estradiol
Estradiol is used orally in the form of tablets of estradiol (Wiki; Graphs). Alternatively, oral estradiol valerate tablets are used in some countries, for instance in many European countries. The only real difference between these oral estradiol forms is that estradiol valerate contains slightly less estradiol by weight (~76% of that of estradiol) due to its ester component and hence requires somewhat higher doses (~1.3-fold) in comparison for equivalent estradiol levels (Wiki; Table). Oral estradiol has a duration suitable for once-daily administration. Oral administration of estradiol is a very convenient and inexpensive route, which makes it the most popular and widely used form of estradiol in transfeminine people. Oral estradiol has relatively low bioavailability (~5%), and there is substantial variability between people in terms of estradiol levels achieved with the same dose. Hence, in some transfeminine people estradiol levels may be low with oral estradiol, and testosterone suppression may be inadequate depending on the antiandrogen.
A major drawback of oral estradiol is that it results in excessive levels of estradiol in the liver due to the first pass that occurs with oral administration and has a disproportionate impact on estrogen-modulated liver synthesis (Aly, 2020). This in turn increases coagulation and the risk of associated health complications like blood clots and cardiovascular problems (Aly, 2020). These particular health concerns are largely allayed if estradiol is taken non-orally at reasonable and non-excessive doses. Hence non-oral forms of estradiol, like transdermal estradiol, although less convenient and often more expensive than oral estradiol, are preferable in transfeminine hormone therapy. It is recommended that all transfeminine people who are over 40 to 45 years of age use non-oral routes due to the greater risk of blood clots and cardiovascular problems that occurs with age (Aly, 2020; Coleman et al., 2022). Oral estradiol is not a good choice for high-dose estradiol monotherapy in transfeminine people due to the high estradiol levels required and the greater risks than with non-oral routes. In addition to its disproportionate liver impact, oral estradiol results in unphysiological levels of estradiol metabolites like estrone and estrone sulfate when compared to non-oral forms. The clinical implications of this, if any, are unknown. Oral and non-oral estradiol have in any case been found to have similar effectiveness in terms of feminization and breast development in transfeminine people in available studies (Sam, 2020).
Sublingual Estradiol
Oral estradiol tablets can be taken sublingually instead of orally. Sublingual use of estradiol tablets has several-fold higher bioavailability relative to oral administration and hence achieves much higher overall estradiol levels in comparison (Sam, 2021; Wiki; Graphs). Sublingual use of oral estradiol tablets can be employed instead of oral administration to reduce doses and hence medication costs or to produce higher estradiol levels for the purpose of achieving better testosterone suppression when needed. However, sublingual estradiol is very spiky in terms of estradiol levels when compared to oral estradiol and has a short duration of highly elevated estradiol levels. As such, it may be advisable for sublingual estradiol to be used in divided doses multiple times throughout the day in order to maintain at least somewhat steadier estradiol levels. The therapeutic implications for transfeminine people of the spikiness of sublingual estradiol, for instance in terms of testosterone suppression and health risks, have been little-studied and are mostly unknown. In any case, when used as a form of high-dose estradiol monotherapy and taken multiple times per day, strong though still incomplete testosterone suppression has been observed (Yaish et al., 2023). Oral estradiol valerate tablets can be taken sublingually instead of orally similarly to estradiol and are likewise highly effective when used in this way (Aly, 2019; Wiki). Due to partial swallowing of tablets, sublingual estradiol may in practice be a mixture of sublingual and oral administration and may have some of the same health risks of oral estradiol (Wiki). Buccal administration of estradiol appears to have similar properties as sublingual administration but is much less researched in comparison and is not used as often in transfeminine people (Wiki).
Transdermal Estradiol
Transdermal estradiol is available in the form of patches, gel, emulsions, and sprays (Wiki). These forms are usually applied to skin areas such as the arms, abdomen, or buttocks. Gel, emulsions, and sprays are applied and left to dry for a short period, whereas patches are applied and remain adhesed to the skin for a specified amount of time. Due to rate-limited absorption through the skin, there is a depot effect with transdermal estradiol and this route has a long duration with very steady estradiol levels. As a result, estradiol gel, emulsions, and sprays are all suitable for once-daily use. Patches stay applied and continuously deliver estradiol for either 3–4 days or 7 days depending on the patch brand (Table). Transdermal estradiol is more expensive than oral estradiol. Gel, emulsions, and sprays may be less convenient than oral administration, but patches can be more convenient due to their infrequent application. However, patches can sometimes cause application site problems like redness and irritation and can occasionally come off prematurely due to adhesive failure. As with oral estradiol, there is substantial variability in estradiol levels with transdermal estradiol, and some transfeminine people may have poor absorption, low estradiol levels, and inadequate testosterone suppression with this route. Estradiol sprays, such as Lenzetto, have been found to achieve very low estradiol levels that are probably not therapeutically adequate for use in transfeminine hormone therapy (Aly, 2020; Graph).
Transdermal estradiol is the form of estradiol most commonly used in transfeminine people who are over 40 years of age due to its lower health risks relative to oral estradiol. Transdermal estradiol gel is not a favorable option for high-dose estradiol monotherapy as it has difficulty achieving the high estradiol levels needed for adequate testosterone suppression (Aly, 2019). On the other hand, transdermal estradiol patches can be an effective option for high-dose estradiol monotherapy if multiple 100 μg/day patches are used, although this can require the use of many patches and can be expensive (Wiki). Different skin sites absorb transdermal estradiol to different extents (Wiki). Genital application of transdermal estradiol, specifically to the scrotum or neolabia, is particularly better-absorbed than conventional skin sites and can result in much higher estradiol levels than usual (Aly, 2019). This can be useful for reducing doses and hence medication costs or for achieving higher estradiol levels for better testosterone suppression when needed, for instance in the context of high-dose estradiol monotherapy. Transdermal estradiol should not be applied to the breasts as this is not known to result in improved breast development and the potential health consequences of doing so are unknown (e.g., influence on breast cancer risk).
Injectable Estradiol
Injectable estradiol preparations can be administered via either intramuscular or subcutaneous injection (Wiki; Wiki; Graphs). There is a depot effect with injection of estradiol esters such that they are slowly absorbed from the injection site and have a prolonged duration. This ranges from days to months depending on the ester. Commonly used injectable estradiol esters, which all have short to moderate durations, include estradiol valerate (EV), estradiol cypionate (EC), estradiol enanthate (EEn), and estradiol benzoate (EB). Longer-acting injectable estradiol esters, such as estradiol undecylate (EU) and polyestradiol phosphate (PEP), have been discontinued and are no longer pharmaceutically available. In the case of intramuscular injection, common injection sites include the deltoid muscle (upper arm), vastus lateralis and rectus femoris muscles (thigh), and ventrogluteal muscle (buttocks). Subcutaneous injection of estradiol injectables, while less commonly used, has comparable pharmacokinetics to intramuscular injection, and is easier, less painful, and more convenient in comparison (Wiki). However, the maximum volume that can be safely and comfortably injected subcutaneously (1.5–3 mL) is less than that which can be injected intramuscularly (2–5 mL) (Hopkins, & Arias, 2013; Usach et al., 2019). Injectable estradiol tends to be fairly inexpensive, but may be less convenient than other routes due to the need for regular injections. There may also be a risk of internal scar tissue build-up long-term. Estradiol injectables have been discontinued in many parts of the world (e.g., most of Europe), and their availability is limited. In recent years, many transfeminine people have turned to black market homebrewed injectable estradiol preparations to use this route.
Injectable estradiol preparations are typically used at higher doses than other forms of estradiol, and can easily achieve very high levels of estradiol. This can be useful for testosterone suppression, making this form of estradiol likely the best choice for high-dose estradiol monotherapy in transfeminine people. However, the high doses that are possible with injectable estradiol preparations can also easily lead to overdosage and unnecessarily increased risks (e.g., Aly, 2020). Resources are available on this site for guiding selection of appropriate doses and intervals of injectable estradiol esters in transfeminine people. This includes a simulator and informal meta-analysis of estradiol levels with these preparations (Aly, 2021; Aly, 2021) and a table providing approximate equivalent doses between injectable estradiol esters and other estradiol routes and forms (Aly, 2020). It is notable and unfortunate that currently recommended doses and intervals for injectable estradiol esters by transgender care guidelines (e.g., 10–40 mg/2 weeks estradiol valerate) appear to be highly excessive and too widely spaced, and are likely to be therapeutically inadvisable (Aly, 2021). Doses and intervals of injectable estradiol esters recommended by the present author for use as a means of high-dose estradiol monotherapy, targeting mean estradiol levels of around 300 pg/mL (1,100 pmol/L), are provided below (Table 4).
Table 4: Recommended doses and intervals of injectable estradiol esters for high-dose estradiol monotherapy (targeting estradiol levels of around 300 pg/mL [1,100 pmol/L]):
a Injection interval. b Doses and intervals for estradiol undecylate are extrapolated and hypothetical (Aly, 2021).
These doses and intervals should be considered a starting point, and should be fine-tuned as necessary based on blood tests. In terms of injection intervals, the shorter interval, the more stable the estradiol levels, but the more often that injections need to be done. Doses may be increased if estradiol levels are too low and testosterone suppression is inadequate, and doses may be decreased if estradiol levels are too high so long as adequate testosterone suppression is maintained. Doses should be lower (targeting mean estradiol levels of 100–200 pg/mL [367–734 pmol/L]) if combined with an antiandrogen or progestogen as these agents will help with testosterone suppression. Similarly, doses should be lower following surgical gonadal removal as testosterone suppression will no longer be necessary.
Estradiol Pellets
Estradiol implants are pellets of pure crystalline hormone and are surgically placed into subcutaneous fat by a physician (Wiki). They are slowly absorbed by the body following implantation, and new implants are given once every 4 to 6 months. Due to the need for minor surgery, their high cost, and limited availability, estradiol implants are not as commonly used as other estradiol routes. Notably, almost all pharmaceutical estradiol implants throughout the world have been discontinued, and the implants that remain available are almost exclusively compounded products provided by compounding pharmacies. Dosage adjustment with estradiol implants is also more difficult than with other estradiol routes. Despite their various practical limitations however, estradiol implants allow for very steady estradiol levels, and their very long duration can allow for unusual convenience among available estradiol forms.
Additional Notes
Table 5: Available forms and recommended doses of estradiol for adulta transfeminine people:
a Estradiol doses in pubertal adolescent transfeminine people should be lower to mimic estradiol exposure during normal female puberty (Aly, 2020). b May be advisable to use divided doses 2 to 4 times per day (i.e., once every 6 to 12 hours) instead of once per day (Sam, 2021). c This estradiol form achieves very low estradiol levels at typical doses that don’t appear to be well-suited for transfeminine hormone therapy (Aly, 2020; Graph). d Estradiol valerate contains about 75% of the same amount of estradiol as estradiol so doses are about 1.3-fold higher for the same estradiol levels (Aly, 2019; Sam, 2021). e Doses and intervals for estradiol undecylate are extrapolated and hypothetical (Aly, 2021). f A higher initial loading dose of e.g., 240 or 320 mg polyestradiol phosphate can be used for the first one or two injections to reach steady-state estradiol levels more quickly. However, this preparation has recently been discontinued and appears to no longer be available.
Additional informational resources are available in terms of estradiol levels (Wiki; Table) and approximate equivalent doses (Aly, 2020) with different forms, routes, and doses of estradiol.
There is high variability between individuals in the levels of estradiol achieved during estradiol therapy. That is, estradiol levels during treatment with the same dosage of estradiol can differ substantially between individuals. This variability is greatest with oral and transdermal estradiol but is also considerable even with injectable estradiol preparations and other estradiol forms. As such, estradiol doses are not absolute and should be individualized on a case-by-case basis in conjunction with blood work as a guide. It should also be noted that due to fluctuations in estradiol concentrations with certain routes, levels of estradiol can vary considerably from one blood test to another. This is most notable with sublingual estradiol and injectable estradiol. The fluctuations in estradiol levels with these routes are predictable and must be understood when interpreting blood work results. Differences in blood test results can be minimized with informed and consistent timing of blood draws.
If or when the gonads are surgically removed, testosterone suppression is no longer needed in transfeminine people. As a result, estradiol doses, if they are high or supraphysiological, can be lowered to more closely approximate normal physiological levels in cisgender women.
Progestogens
Progestogens include progesterone and progestins. Progestins are synthetic progestogens derived from structural modification of progesterone or testosterone. There are dozens of different progestins and these progestins can be divided into a variety of different structural classes with varying properties (Table). Examples of some major progestins of different classes include the 17α-hydroxyprogesterone derivative medroxyprogesterone acetate (MPA; Provera, Depo-Provera), the 19-nortestosterone derivative norethisterone (NET; many brand names), the retroprogesterone derivative dydrogesterone (Duphaston), and the 17α-spirolactone derivative drospirenone (Slynd, Yasmin). Progestins were developed because they have a more favorable disposition in the body than progesterone for use as medications. Only a few clinically used progestins have been employed in transfeminine hormone therapy. However, progestogens largely produce the same progestogenic effects, with a few exceptions, and theoretically almost any progestogen could be used.
Besides helping with testosterone suppression, progestogens are of no clear or known benefit for feminization or breast development in transfeminine people. While some transfeminine people anecdotally claim to experience improved breast development with progestogens, an involvement of progestogens in improving breast size or shape is controversial and is not supported by theory nor evidence at present (Wiki; Aly, 2020). It is possible that premature introduction of progestogens, particularly at high doses, could actually have an unfavorable influence on breast development (Aly, 2020). Many transfeminine people have also anecdotally claimed that progestogens have a beneficial effect on their sexual desire. However, a review of the literature by the present author found that neither progesterone nor progestins positively influence sexual desire in humans (Aly, 2020). Instead, the available evidence suggests either a neutral influence or an inhibitory effect of progestogens on sexual desire, although the latter may be specific only to high doses of progestogens (Aly, 2020). Claims have been made that progesterone may have beneficial effects on mood in transfeminine people as well, but clinical support for such notions is likewise lacking at this time (Coleman et al., 2022; Nolan et al., 2022). It is notable that progesterone at luteal-phase levels, due to its neurosteroid metabolites like allopregnanolone, actually appears to worsen mood in around 30% of cisgender women, and produces more overt negative reactions, which constitute the diagnoses of premenstrual syndrome (PMS) and premenstrual dysphoric disorder (PMDD), in around 2 to 10% of women (Bäckström et al., 2011; Edler Schiller, Schmidt, & Rubinow, 2014; Sundström-Poromaa et al., 2020). More research is needed to evaluate the possible beneficial effects of progestogens in transfeminine people.
Most clinically used progestogens have off-target activities in addition to their progestogenic activity, and these activities may be desirable or undesirable depending on the action in question (Kuhl, 2005; Stanczyk et al., 2013; Wiki; Table). Progesterone has a variety of neurosteroid as well as other activities that can result in central nervous system effects among others which are not shared by progestins. MPA as well as NET and its derivatives have weak androgenic activity, which is unfavorable in the context of transfeminine hormone therapy. NET and certain related progestins produce ethinylestradiol as a metabolite at high doses and hence can produce ethinylestradiol-like estrogenic effects, including increased risk of blood clots and associated cardiovascular problems. Other off-target actions of progestogens include antiandrogenic, glucocorticoid, and antimineralocorticoid activities. These actions can result in differences in therapeutic effectiveness (e.g., androgen suppression or blockade) as well as side effects and health risks. Some notable progestins without undesirable off-target activities (i.e., androgenic or glucocorticoid activity) include low-dose CPA, drospirenone (DRSP), dienogest, nomegestrol acetate (NOMAC), dydrogesterone, and hydroxyprogesterone caproate (OHPC). However, of these progestins, only CPA has been considerably used and studied in transfeminine people.
The addition of progestogens to estrogen therapy has been associated with a number of unfavorable health effects. These include increased risk of blood clots (Wiki; Aly, 2020), coronary heart disease (Wiki), and breast cancer (Wiki; Aly, 2020). High doses of progestogens are also associated with increased risk of certain non-cancerousbrain tumors including meningiomas and prolactinomas (Wiki; Aly, 2020). The coronary heart disease risk may be due to changes in blood lipids caused by the weak androgenic activity of certain progestogens, but the rest of the aforementioned risks are probably due to their progestogenic activity (Stanczyk et al., 2013; Jiang & Tian, 2017). Aside from health risks, progestogens have also been associated with adverse mood changes (Wiki; Wiki). However, besides the case of progesterone and its neurosteroid metabolites, these effects of progestogens are controversial and are not well-supported by evidence (Wiki; Wiki). Progestogens are otherwise generally well-tolerated and are regarded as producing little in the way of side effects.
In contrast to certain progestins, progesterone has no unfavorable off-target hormonal activities. Due to its lack of androgenic activity, progesterone has no adverse influence on blood lipids and is not expected to raise the risk of coronary heart disease. The addition of oral progesterone to estrogen therapy notably has not been associated with increased risk of blood clots (Wiki). In addition, oral progesterone seems to have less risk of breast cancer than progestins with shorter-term therapy, although this is notably not the case with longer-term exposure (Wiki; Aly, 2020). Consequently, it has been suggested that progesterone, for reasons that have yet to be fully elucidated, may be a safer progestogen than progestins and that it should be the preferred progestogen for hormone therapy in cisgender women and transfeminine people. However, there are also theoretical arguments against such notions. Oral progesterone is known to produce very low progesterone levels and to have only weak progestogenic effects at typical doses (Aly, 2018; Wiki). The seemingly better safety of oral progesterone may simply be an artifact of the low progesterone levels that occur with it, and hence of progestogenic dosage. Non-oral progesterone, at doses resulting in physiological and full progestogenic strength, has never been properly evaluated in terms of health outcomes, and may have similar risks as progestins (Aly, 2018; Wiki).
Due to their lack of known influence on feminization and breast development and their known and possible adverse effects and risks, progestogens are not routinely used in transfeminine hormone therapy at present. Major transgender health guidelines note the limitations of the available evidence on progestogens for transfeminine people and have mixed attitudes on their use, either explictly recommending against their use (Coleman et al., 2022—WPATH SOC8), taking a more neutral stance (Hembree et al., 2017—Endocrine Society guidelines), or being permissive of their use (Deutsch, 2016—UCSF guidelines). There is however a very major exception to the preceding in the form of CPA, an antiandrogen which is widely used in transfeminine hormone therapy to suppress testosterone production and which happens to be a powerful progestogen at the typical doses used in transfeminine people. CPA will be described below in the section on antiandrogens. Although progestogens have various health risks, cisgender women of course have progesterone, and the absolute risks of progestogens are very low in healthy young people. Risks like breast cancer also are exposure-dependent and take many years to develop. The testosterone suppression provided by progestogens can furthermore be very useful in transfeminine people, as is widely taken advantage of with CPA. Given these considerations, a limited duration of progestogen therapy in transfeminine people, for instance a few years to help suppress testosterone levels before surgical gonadal removal, may be considered quite acceptable.
Progesterone can be used in transfeminine people by oral administration, sublingual administration, rectal administration, or by intramuscular or subcutaneous injection (Wiki). Progestins are usually used via oral administration, but certain progestins are also available in injectable formulations (Wiki).
Oral Progesterone
Progesterone is most commonly taken orally. It is used by this route in the form of oil-filled capsules containing 100 or 200 mg micronized progesterone under brand names such as Prometrium, Utrogestan, and Microgest (Wiki). Despite its widespread use, levels of progesterone via oral administration have been found using state-of-the-art assays (LC–MS) to be very low (<2 ng/mL [<6.4 nmol/L] at 100 mg/day) and inadequate for satisfactory progestogenic effects in various areas (Aly, 2018; Wiki). In relation to this, even high doses of oral progesterone (400 mg/day) showed no antigonadotropic effect or testosterone suppression in cisgender men (Aly, 2018; Wiki). This is in major contrast to non-oral forms of progesterone and to progestins, which produce dose-dependent and robust testosterone suppression (Aly, 2019; Wiki). In addition to its low progestogenic potency, oral progesterone is excessively converted into neurosteroid metabolites like allopregnanolone and pregnanolone. These metabolites act as potent GABAA receptor positive allosteric modulators, and can produce undesirable alcohol-like side effects such as sedation, cognitive, memory, and motor impairment, and mood changes (Wiki; Wiki). As such, while inconvenient, non-oral routes are greatly preferable for progesterone.
Sublingual Progesterone
Sublingual progesterone tablets exist and are marketed under the brand name Luteina but today are only available in Poland and Ukraine (Wiki). Oral progesterone could theoretically be taken sublingually, analogously to sublingual use of oral estradiol. However, because oral progesterone is formulated as oil-filled capsules, this makes it difficult and unpleasant to use by sublingual administration. Buccal progesterone, which would be expected to have similar characteristics to those of sublingual progesterone, has been used in medicine in the past, but is no longer marketed today (Wiki).
Rectal Progesterone
Progesterone is approved for use by rectal administration in the form of suppositories under the brand name Cyclogest (Wiki). This product is marketed in only a limited number of countries however, although it is available in the United Kingdom (Wiki). While not approved for use by rectal administration, oral progesterone capsules can be taken rectally instead of orally, and using them in this way may allow for much higher progesterone levels than would be achieved by oral administration due to avoidance of most first-pass metabolism. Rectal administration of oral progesterone capsules has not been formally studied, but oral progesterone capsules have been administered vaginally in cisgender women with success (Miles et al., 1994; Wang et al., 2019), and the vaginal and rectal routes are said to have similar pharmacokinetics in general (Goletiani, Keith, & Gorsky, 2007; Wiki). Hence, there is good theoretical basis for rectal administration of oral progesterone capsules being an effective route of progesterone. Whereas oral progesterone achieves very low levels of progesterone, rectal progesterone can readily achieve normal luteal-phase levels of progesterone (Wiki). Although inconvenient, rectal administration may be the overall best route of administration of progesterone for transfeminine people. A significant subset of transfeminine people on progestogens take progesterone rectally (Chang et al., 2024).
Injectable Progesterone
Progesterone by injection is available as an oil solution for intramuscular injection under brand names such as Proluton, Progestaject, and Gestone (Wiki) and as an aqueous solution for subcutaneous injection under the brand name Prolutex (Wiki). Oil solutions of progesterone for intramuscular injection are widely available, whereas the aqueous solution of progesterone for subcutaneous injection is available only in some European countries (Wiki). Injectable progesterone, regardless of route, has a relatively short duration and must be injected once every one to three days (Wiki; Wiki). This makes it too inconvenient to use for most people. Unlike with estradiol, progesterone esters with longer durations than progesterone itself by injection are not chemically possible as progesterone has no hydroxyl groups available for esterification (Wiki). Injectable aqueous suspensions of microcrystalline progesterone were previously marketed and had a duration of 1 to 2 weeks, but these preparations were associated with pain at the injection site and were eventually discontinued (Aly, 2019; Wiki).
Other Progesterone Routes
Other progesterone routes, such as transdermal progesterone and subcutaneous progesterone pellets, are also known, but are not available as pharmaceutical drugs and are little-used medically (Wiki). This is related to the low potency of progesterone and difficulty achieving progesterone levels high enough for adequate therapeutic effects with these routes (Wiki; Wiki). In addition, progesterone pellets tend to be extruded at high rates (Wiki). In any case, certain compounding pharmacies may make forms of progesterone that could be used by these routes.
Oral and Injectable Progestins
Most progestins are taken orally in the form of solid tablets (Wiki). In contrast to progesterone, progestins, owing to their synthetic nature, are resistant to metabolism in the intestines and liver and have high oral bioavailability. In addition, unlike the case of the estrogen receptors, the progesterone receptors are expressed minimally or not at all in the liver, and there is no known first pass influence of progestogenic activity on liver synthesis (Lax, 1987; Stanczyk, Mathews, & Cortessis, 2017). As a result, there are no apparent problems with oral administration in the case of purely progestogenic progestins. However, some progestins have liver-impacting off-target hormonal actions, such as androgenic, estrogenic, and/or glucocorticoid activity, and this can result in adverse effects like unfavorable lipid changes or procoagulation—which may be augmented by the first pass with oral administration.
A selection of progestins are available in injectable formulations, including for intramuscular or subcutaneous injection (Wiki). Some of the more notable ones include medroxyprogesterone acetate (MPA), norethisterone enanthate (NETE), hydroxyprogesterone caproate (OHPC), and algestone acetophenide (dihydroxyprogesterone acetophenide; DHPA) (Wiki). In addition to being used alone, injectable progestins are used together with estradiol esters in combined injectable contraceptives (Wiki). These preparations are often used as a means of hormone therapy by transfeminine people in Latin America. Whereas injectable progesterone has a duration measured in days, injectable progestins have durations ranging from weeks to months, and can be injected much less often in comparison (Table).
Additional Notes
Table 6: Available forms and recommended doses of progestogens for transfeminine people:
For progesterone levels with different forms, routes, and doses of progesterone, see the table here (only LC–MS and IA + CS assays for oral progesterone) and the graphs here.
As with estradiol, there is high variability between individuals in progesterone levels. Conversely, there is less variability between individuals in the case of progestins.
After removal of the gonads, progestogen doses can be lowered or adjusted to approximate normal female physiological exposure or they can be discontinued entirely.
Antiandrogens
Aside from estrogens and progestogens, there is another class of hormonal medications used in transfeminine hormone therapy known as antiandrogens (AAs). These medications reduce the effects of androgens in the body by either decreasing androgen production and thereby lowering androgen levels or by directly blocking the actions of androgens. They work via a variety of different mechanisms of action, and include androgen receptor antagonists, antigonadotropins, and androgen synthesis inhibitors.
Androgen receptor antagonists act by directly blocking the effects of androgens, including testosterone, DHT, and other androgens, at the level of their biological target. They bind to the androgen receptor without activating it, thereby displacing androgens from the receptor. Due to the nature of their mechanism of action as competitive blockers of androgens, the antiandrogenic efficacy of androgen receptor antagonists is both highly dose-dependent and fundamentally dependent on testosterone levels. They do not act by lowering testosterone levels, although some androgen receptor antagonists may have additional antiandrogenic actions that result in decreased testosterone levels. Because androgen receptor antagonists do not work by lowering testosterone levels, blood work can be less informative for them compared to antiandrogens that suppress testosterone levels. Androgen receptor antagonists include steroidal antiandrogens (SAAs) like spironolactone (Aldactone) and cyproterone acetate (CPA; Androcur) and nonsteroidal antiandrogens (NSAAs) like bicalutamide (Casodex).
Antigonadotropins suppress the gonadal production of androgens by inhibiting the GnRH-mediated secretion of gonadotropins from the pituitary gland. They include estrogens and progestogens. In addition, GnRH agonists such as leuprorelin (Lupron) and GnRH antagonists such as elagolix (Orilissa) act similarly and could likewise be described as antigonadotropins.
Androgen synthesis inhibitors inhibit the enzyme-mediated synthesis of androgens. They include 5α-reductase inhibitors (5α-RIs) like finasteride (Propecia) and dutasteride (Avodart). There are also other types of androgen synthesis inhibitors, for instance potent 17α-hydroxylase/17,20-lyase inhibitors like ketoconazole (Nizoral) and abiraterone acetate (Zytiga). However, these agents have limitations (e.g., toxicity, high cost, and lack of experience) and have not been used in transfeminine hormone therapy.
Although antigonadotropins and androgen synthesis inhibitors have antiandrogenic effects secondary to decreased androgen levels, they are not usually referred to as “antiandrogens”. Instead, this term is most commonly reserved to refer specifically to androgen receptor antagonists. However, antigonadotropins and androgen synthesis inhibitors may nonetheless be described as antiandrogens as well.
After removal of the gonads, antiandrogens can be discontinued. If unwanted androgen-dependent symptoms, such as acne, seborrhea, or scalp hair loss, persist despite full suppression or ablation of gonadal testosterone, then a lower dose of an androgen receptor antagonist, such as 100 to 200 mg/day spironolactone or 12.5 to 25 mg/day bicalutamide, can be continued to treat these symptoms.
Table 7: Available forms and recommended doses of antiandrogens for transfeminine people:
a For CPA, this dose range is specifically one-quarter of a 10-mg tablet to one full 10-mg tablet per day (2.5–10 mg/day) or a quarter of a 50-mg tablet every other day or every 2 to 3 days (4.2–12.5 mg/day). A dosage of 5–10 mg/day or 6.25–12.5 mg/day is likely to ensure maximal testosterone suppression, while lower doses may be less effective (Aly, 2019). b For spironolactone and bicalutamide, it is assumed that testosterone levels are substantially suppressed (≤200 ng/dL [<6.9 nmol/L]). If testosterone levels are not suppressed to this range, then higher doses may be warranted. c Spironolactone and its metabolites have relatively short half-lives, and twice-daily administration in divided doses (e.g., 100–200 mg twice per day) is recommended.
Figure 3: Suppression of gonadal testosterone production and circulating testosterone levels (ng/dL) with estradiol in combination with different antiandrogens over one year of hormone therapy in transfeminine people (Sofer et al., 2020). The estradiol forms included oral tablets 2–8 mg/day, transdermal gel 2.5–5 mg/day, and transdermal patches 50–200 μg/day. The antiandrogens included spironolactone 50–200 mg/day (n=16), cyproterone acetate (n=41), and GnRH agonists (specifically triptorelin 3.75 mg/month or goserelin 3.6 mg/month by injection) (n=10) (Sofer et al., 2020). It should be noted that lower doses of cyproterone acetate (10–12.5 mg/day) show equal testosterone suppression to higher doses (25–100 mg/day) and higher doses should no longer be used (Aly, 2019). The dashed horizontal line corresponds to the upper limit of the normal female range for testosterone levels.
As an antiandrogen, CPA has a dual mechanism of action of suppressing testosterone levels via its progestogenic and hence antigonadotropic activity and of acting as an androgen receptor antagonist (Aly, 2019). The progestogenic activity of CPA is of far greater potency than its androgen receptor antagonism however (Aly, 2019). The dose of CPA used as a progestogen in cisgender women is about 2 mg per day, which produces similar progestogenic effects to those of physiological luteal-phase levels of progesterone (e.g., suppression of gonadotropin secretion, ovulation inhibition, and endometrial transformation and protection) (Aly, 2019). Conversely, much higher doses of CPA of 50 to 300 mg/day have typically been used for androgen-dependent indications (Aly, 2019). These high doses of CPA result in profound progestogenic overdosage and associated side effects and risks (Aly, 2019). In transfeminine people, CPA has historically been used at doses of 50 to 150 mg/day (Aly, 2019). However, CPA doses have dramatically fallen in recent years, and today doses of no more than 10 to 12.5 mg/day are recommended (Aly, 2019; Coleman et al., 2022—WPATH SOC8). These lower doses of CPA still produce strong progestogenic effects, and in combination with estradiol, are equally effective as higher doses in suppressing testosterone levels (Aly, 2019; Meyer et al., 2020; Even Zohar et al., 2021; Kuijpers et al., 2021; Coleman et al., 2022). Even lower doses of CPA, for instance 5 to 6.25 mg/day, are currently being studied, and may still be fully effective (Aly, 2019).
Given by itself without estrogen, CPA typically suppresses testosterone levels in people with testes by about 50 to 70%, down to about 150 to 300 ng/dL (5.2–10.4 nmol/L) (Meriggiola et al., 2002; Toorians et al., 2003; Giltay et al., 2004; T’Sjoen et al., 2005; Tack et al., 2017; Zitzmann et al., 2017; Aly, 2019). Lower doses of CPA alone (e.g., 10 mg/day) show the same degree of testosterone suppression as higher doses of CPA alone (e.g., 50–100 mg/day), indicating that the antigonadotropic effects of CPA are maximal at relatively low therapeutic doses of this medication (Aly, 2019). This is on the order of about 5 to 10 times the ovulation-inhibiting dosage of CPA in cisgender women, a dose–response relationship that has also been observed with a number of other progestogens (Aly, 2019). Per the preceding, CPA alone, regardless of dosage, is unable to reduce testosterone levels into the normal female range (<50 ng/dL [<1.7 nmol/L]). But when CPA is combined with estradiol, even at relatively small doses of estradiol, it consistently suppresses testosterone levels into the normal female range (Aly, 2019; Angus et al., 2019; Gava et al., 2020; Sofer et al., 2020; Collet et al., 2022). However, it appears that a certain minimum level of estradiol, perhaps around 60 pg/mL (220 pmol/L) on average, is required for this to occur (Aly, 2019). Estradiol levels lower than this threshold in those taking CPA, which can occasionally be encountered in transfeminine people due to estradiol being dosed too low, have the potential to compromise full testosterone suppression (Aly, 2019).
In addition to testosterone suppression, CPA can dose-dependently block the androgen receptor (Aly, 2019). However, relatively high doses of CPA are needed to considerably antagonize the androgen receptor (e.g., 50–300 mg/day), and lower doses (e.g., ≤12.5 mg/day) may not be able to do this to a meaningful degree (Aly, 2019). As such, lower doses of CPA may essentially be purely progestogenic, with minimal or no androgen receptor antagonism. In this regard, referring to CPA at such doses as an “antiandrogen”—rather than as a “progestogen”—may be considered somewhat of a misnomer. Higher doses of CPA (>12.5 mg/day) can no longer be considered safe due to the massive progestogenic overdosage that occurs with them, and should no longer be used in transfeminine people. Moreover, as testosterone levels are usually suppressed into the normal female range in transfeminine people taking estradiol plus CPA, there is no actual need for any additional androgen receptor blockade (Aly, 2019).
CPA has been reported to produce various side effects. Some of these side effects include fatigue and a degree of weight gain (Belisle & Love, 1986; Hammerstein, 1990; Martinez-Martin et al., 2022). CPA might be able to produce a magnitude of sexual dysfunction (e.g., reduced sexual desire) beyond that expected with testosterone suppression alone (Wiki; Aly, 2019). It may also have a small risk of depressive mood changes (Wiki). In transfeminine people, CPA has been documented to produce pregnancy-like breast changes (i.e., lobuloalveolar development of the mammary glands) (Kanhai et al., 2000). In relation to this, CPA sometimes causes lactation as a side effect (Gooren, Harmsen-Louman, & van Kessel, 1985; Schlatterer et al., 1998; Bazarra-Castro, 2009). Concerns have been raised about premature introduction of progestogens—particularly at high doses like with CPA—and possible adverse influence on breast development (Aly, 2020). However, little data exists in humans to substantiate such concerns at present. The side effects of CPA are assumed to be dose-dependent, and using the lowest effective doses is expected to minimize its side effects.
CPA is usually taken orally in the form of tablets (e.g., 10, 50, and 100 mg) (Wiki). Under the brand name Androcur Depot, it is also available as a long-lasting 300 mg depot injectable in some countries (Wiki). However, this formulation is not commonly used in transfeminine people, and happens to correspond to very high doses in terms of CPA exposure. A pill cutter (Amazon) can be used to split CPA tablets and achieve lower doses (e.g., 12.5 mg doses with 50-mg tablets). CPA has a relatively long elimination half-life of about 1.6 to 4.3 days (Wiki; Aly, 2019). As such, it can be taken once daily, or even as infrequently as once every 2 or 3 days, if needed (Aly, 2019). In addition to splitting of CPA tablets, dosing CPA once every 2 or 3 days can also be useful for achieving lower doses (Aly, 2019).
As already described, CPA is a powerful progestogen even at the relatively low doses now used in transfeminine people (e.g., 5–12.5 mg/day). As such, there is no need, nor point, in adding another progestogen, for instance progesterone, in those who are taking CPA—at least if the goal of doing so is to produce progestogenic effects. This is something that is often overlooked in people taking CPA, and can result in increased costs, side effects, and inconvenience without any expected benefit.
Spironolactone
Spironolactone (Aldactone) is an antiandrogen and antimineralocorticoid. It is widely used as an antiandrogen in cisgender women for treatment of androgen-dependent hair and skin conditions like acne, hirsutism (excessive facial/body hair growth), and scalp hair loss, in cisgender women for treatment of hyperandrogenism (high androgen levels) due to polycystic ovary syndrome (PCOS), and in transfeminine people as a component of hormone therapy. Spironolactone is particularly widely used in transfeminine people in the United States, where it is the most commonly used antiandrogen in this population. As an antimineralocorticoid, the original and primary use of spironolactone in medicine, it is used to treat heart failure, high blood pressure, high mineralocorticoid levels, low potassium levels, and conditions of excess fluid retention like nephrotic syndrome and ascites, among others (Wiki). In terms of its antiandrogenic actions, spironolactone is a relatively weak androgen receptor antagonist as well as a weak androgen synthesis inhibitor (Wiki). The androgen synthesis inhibition of spironolactone is mediated specifically via inhibition of 17α-hydroxylase and 17,20-lyase (Wiki). Spironolactone does not appear to have meaningful progestogenic activity, 5α-reductase inhibition, or direct estrogenic activity (Wiki). However, indirect estrogenic effects secondary to its antiandrogenic activity (e.g., breast development and feminization) can occur with it at sufficiently high doses (Wiki).
Spironolactone shows limited and highly inconsistent effects on testosterone levels in clinical studies in cisgender men, cisgender women, and transfeminine people, with most studies finding no change in levels, some studies finding a decrease in levels, and a small number even finding an increase in levels (Aly, 2018). In spite of this, studies commonly find that spironolactone still produces antiandrogenic effects even when androgen levels remain unchanged. Hence, the primary mechanism of action of spironolactone as an antiandrogen appears to be androgen receptor blockade. In relation to this, in transfeminine people taking spironolactone as an antiandrogen, the estrogen component of the regimen is likely to be the main or possibly sole agent suppressing testosterone production. This is in part based on studies in transfeminine people comparing estradiol plus spironolactone to estradiol alone (e.g., Leinung, 2014; Leinung, Feustel, & Joseph, 2018; Angus et al., 2019) and on studies comparing testosterone levels with different doses of spironolactone (e.g., Liang et al., 2018; SoRelle et al., 2019; Allen et al., 2021). Due to the minimal influence of spironolactone on testosterone production, testosterone levels are not usually suppressed into the female range in transfeminine people taking estradiol plus spironolactone, with testosterone levels often remaining well above this range (e.g., 50–450 ng/dL [1.7–15.6 nmol/L] on average) (Leinung, 2014; Leinung, Feustel, & Joseph, 2018; Liang et al., 2018; Angus et al., 2019; Jain, Kwan, & Forcier, 2019; SoRelle et al., 2019; Sofer et al., 2020; Burinkul et al., 2021). However, testosterone levels do tend to decline gradually over time in transfeminine people on this regimen (e.g., Liang et al., 2018; Sofer et al., 2020 (Graph); Allen et al., 2021).
Due to its relatively weak androgen receptor antagonism, spironolactone is likely best-suited for blocking female-range or somewhat-higher testosterone levels (e.g., <100 ng/dL [<3.5 nmol/L]) (Aly, 2018). This is based on clinical dose-ranging studies of spironolactone (typically using 50–200 mg/day) in healthy cisgender women and cisgender women with PCOS (Goodfellow et al., 1984; Lobo et al., 1985; Hammerstein, 1990; James, Jamerson, & Aguh, 2022) as well as comparative studies of spironolactone against the more-potent antiandrogen flutamide (Cusan et al., 1994; Erenus et al., 1994; Shaw, 1996). The clinical antiandrogenic efficacy of spironolactone has been very limitedly assessed in transfeminine people to date, and is largely unknown (Angus et al., 2021). In any case, the antiandrogenic efficacy of spironolactone in cisgender women with androgen-dependent hair and skin conditions is well-established, and the medication thus does appear to be effective so long as testosterone levels are not too high (Brown et al., 2009; van Zuuren & Fedorowicz, 2016; Layton et al., 2017; Barrionuevo et al., 2018; James, Jamerson, & Aguh, 2022). In addition, higher doses of spironolactone (e.g., 300–400 mg/day) may be more useful for blocking higher testosterone levels in transfeminine people, and are allowed for by transgender care guidelines (Aly, 2020).
Consequent to spironolactone’s limited and inconsistent influence on testosterone levels and its relatively weak androgen receptor antagonism, estradiol plus spironolactone regimens will likely not be fully effective in terms of testosterone suppression for many transfeminine people. This is liable to result in suboptimal demasculinization, feminization, and breast development in these individuals. Other antiandrogenic approaches, such as bicalutamide, CPA, GnRH modulators, and high-dose estradiol monotherapy, will likely be more effective in these cases owing either to their ability to more potently block androgens or their capacity to reliably reduce testosterone levels into the female range. If testosterone levels are still too high with estradiol plus spironolactone, a switch to a different antiandrogen, increasing to a higher dosage of estradiol, or addition of a clinically antigonadotropic progestogen (e.g., non-oral progesterone or a progestin) should be considered.
Spironolactone is a strong antimineralocorticoid, or antagonist of the mineralocorticoid receptor, the biological target of the mineralocorticoid steroid hormones aldosterone and 11-deoxycorticosterone. This is an action that spironolactone shares with progesterone, although spironolactone is a much more potent antimineralocorticoid than progesterone. The mineralocorticoid receptor is involved in regulating electrolyte and fluid balances, among other roles. Spironolactone is associated with modestly lowered blood pressure, which may be considered a beneficial effect of its antimineralocorticoid activity (Martinez-Martin et al., 2022). Although spironolactone is usually well-tolerated, it can sometimes produce antimineralocorticoid side effects such as excessively lowered blood pressure, dizziness, fatigue, urinary frequency, and increased cortisol levels, among others (Kellner & Wiedemann, 2008; Kim & Del Rosso, 2012; Zaenglein et al., 2016; Layton et al., 2017; James, Jamerson, & Aguh, 2022). It has been argued by some in the online transgender community that spironolactone, via its antimineralocorticoid activity and increased cortisol levels, may increase visceral fat in transfeminine people (Aly, 2020). However, evidence does not support this hypothetical side effect at present (Aly, 2020). Available data also do not support spironolactone stunting breast development in transfeminine people or producing serious neuropsychiatric side effects, such as prominent depressive mood changes.
In people who are at-risk for hyperkalemia, dietary restriction to limit intake of potassium-rich foods is often recommended (Roscioni et al., 2012; Cupisti et al., 2018). This is often encountered in transgender health as transfeminine people being told “not to eat bananas”, which are said to be high in potassium. However, limiting dietary potassium with spironolactone to avoid hyperkalemia is theoretical and not actually evidence-based, with data so far contradicting its efficacy (St-Jules, Goldfarb, & Sevick, 2016; St-Jules & Fouque, 2021; Babich, Kalantar-Zadeh, & Joshi, 2022; St-Jules & Fouque, 2022). As such, routine restriction of dietary potassium with spironolactone may not be warranted.
Aside from its antimineralocorticoid activity, spironolactone has been reported to increase levels of LDL (“bad”) cholesterol levels and to decrease levels of HDL (“good”) cholesterol in women with PCOS (Nakhjavani et al., 2009). However, findings appear to be conflicting, with other studies not finding unfavorable influences on cholesterol levels with spironolactone (Polyzos et al., 2011). Long-term, adverse effects on cholesterol levels could result in an increase in the risk of coronary heart disease.
Spironolactone is taken orally in the form of tablets (e.g., 25, 50, and 100 mg) (Wiki). It is a prodrug of several active metabolites, including 7α-thiomethylspironolactone, 6β-hydroxy-7α-thiomethylspironolactone, and canrenone (7α-desthioacetyl-δ6-spironolactone) (Wiki). Spironolactone and these active metabolites have elimination half-lives of 1.4 hours, 13.8 hours, 15.0 hours, and 16.5 hours, respectively (Wiki). Due to the relatively short duration of elevated drug levels with spironolactone and its active metabolites (Graph), twice-daily administration of spironolactone in divided doses may be more optimal than once-daily intake and is advised (Reiter et al., 2010).
Bicalutamide
Bicalutamide (Casodex) is a nonsteroidal antiandrogen (NSAA) which acts as a potent and highly selective androgen receptor antagonist (Wiki). It is primarily used in the treatment of prostate cancer in cisgender men. Prostate cancer is an androgen-dependent cancer which antiandrogens can help to slow the progression of, and this use constitutes the vast majority of prescriptions for bicalutamide (Wiki). In addition to prostate cancer, although to a much lesser extent, bicalutamide has been used in the treatment of hirsutism (excessive facial/body hair growth), scalp hair loss, and polycystic ovary syndrome (PCOS) in cisgender women, peripheral or gonadotropin-independent precocious puberty (a rare form of precocious puberty in which antigonadotropins such as GnRH agonists are not effective) in cisgender boys, and priapism in cisgender men (Wiki). Bicalutamide is also becoming increasingly adopted for use as an antiandrogen in transfeminine people (Aly, 2020; Wiki). However, its use in transgender health is still very limited, and well-regarded transgender care guidelines either recommend against its use (Deutsch, 2016—UCSF guidelines; Coleman et al., 2022—WPATH SOC8) or are only cautiously permissive of its use (Thompson et al., 2021—Fenway Health guidelines). This is due to a lack of studies of bicalutamide in transfeminine people and its potential risks. Nonetheless, a small but growing number of clinicians are using bicalutamide in transfeminine people or are willing to prescribe it, with these clinicians located particularly in the United States. A single small clinical study has assessed bicalutamide in transfeminine people so far, specifically as a puberty blocker in 13 transfeminine adolescents who were denied insurance coverage for GnRH agonists (Neyman, Fuqua, & Eugster, 2019). (Update: More studies of bicalutamide in transfeminine people have since been published, see Aly (2020).)
Bicalutamide is a much more potent androgen receptor antagonist than either spironolactone or CPA (Wiki; Neyman, Fuqua, & Eugster, 2019). It is typically used in transfeminine people at a dosage of 25 to 50 mg/day, although this dosage has been arbitrarily selected and is not based on clinical data. Nonetheless, due to its relatively high potency as an androgen receptor antagonist and concomitant suppression of testosterone levels by estradiol, these doses may be adequate for testosterone blockade for many transfeminine people. At higher doses (>50 mg/day), bicalutamide is able to substantially block male-range testosterone levels (>300 ng/dL [>10.4 nmol/L]) based on studies of bicalutamide monotherapy in cisgender men with prostate cancer (Wiki). This is something that spironolactone and CPA are not capable of in the same way. Owing to its selectivity for the androgen receptor, bicalutamide has no off-target hormonal activity and produces almost no side effects in women (Wiki; Erem, 2013; Moretti et al., 2018). The only apparent side effect of bicalutamide in a rigorous clinical trial of the drug for hirsutism in cisgender women was significantly increased total and LDL (“bad”) cholesterol levels (Moretti et al., 2018). Hence, bicalutamide tends to be very well-tolerated. The relative lack of side effects with bicalutamide is in contrast to other antiandrogens like spironolactone and CPA, which are not pure androgen receptor antagonists and have off-target hormonal actions like antimineralocorticoid activity or strong progestogenic activity with consequent side effects and risks.
As a selective androgen receptor antagonist, bicalutamide taken by itself does not decrease testosterone production or levels but rather increases them (Wiki). This is due to a loss of androgen receptor-mediated negative feedback on gonadotropin secretion and a consequent compensatory upregulation of gonadal testosterone production (Wiki). Bicalutamide more than blocks the effects of any increase in testosterone it causes, and in fact fundamentally cannot increase testosterone levels more than it can block them (Wiki). In addition, increases in testosterone levels with bicalutamide will be blunted or abolished if it is combined with an adequate dose of an antigonadotropin such as estradiol (Wiki; Wiki). Since estradiol is made from testosterone in the body, bicalutamide taken alone also preserves and increases estradiol production and levels (Wiki). Because of this, although bicalutamide has no other important intrinsic hormonal activity besides its antiandrogenic activity, it produces robust indirect estrogenic effects including feminization and breast development even when it is not combined with estrogen (Wiki; Wiki; Neyman, Fuqua, & Eugster, 2019). This has important implications for the use of bicalutamide as a puberty blocker in transfeminine adolescents, as bicalutamide does not actually block puberty like conventional puberty blockers (GnRH agonists) but instead has the effect of dose-dependently converting male puberty into female puberty (Wiki; Neyman, Fuqua, & Eugster, 2019).
Bicalutamide has certain health risks, which has been a major reason that it has not been more readily adopted in transfeminine hormone therapy (Aly, 2020). It has a small risk of liver toxicity (Wiki; Aly, 2020) and of lung toxicity (Wiki). Abnormal liver function tests (LFTs), such as elevated liver enzymes and elevated bilirubin, occurred in about 3.4% of men with bicalutamide monotherapy plus standard care versus 1.9% of men with placebo plus standard care in the Early Prostate Trial (EPC) clinical programme after 3.0 years of follow-up (Wiki). In clinical trials, treatment with bicalutamide had to be discontinued in about 0.3 to 1.5% of men due to LFTs that became too highly elevated and could have progressed to serious liver toxicity (Wiki). To date, there are around 10 published case reports of serious liver toxicity, including cases of death, with bicalutamide, all of which have been in men with prostate cancer (Wiki; Table; Aly, 2020). There have also been a few unpublished reports of serious liver toxicity including deaths with bicalutamide in transfeminine people (Aly, 2020). However, these reports have not been confirmed, and they may or may not be reliable. In addition to the preceding reports, hundreds of additional instances of liver complications in people taking bicalutamide exist in the United States FDA Adverse Event Reporting System (FAERS) database (Wiki; FDA). Abnormal LFTs with bicalutamide usually occur within the first 3 to 6 months of treatment (Kolvenbag & Blackledge, 1996; Casodex FDA Label), and all case reports of liver toxicity with bicalutamide have had an onset of less than 6 months (Table). The liver toxicity of bicalutamide is not known to be dose-dependent across its clinically used dose range (Wiki). Abnormal LFTs have occurred with bicalutamide (at rates of 2.9% to 11.4%) even at relatively low doses in cisgender women (e.g., 10–50 mg/day) (de Melo Carvalho, 2022). Due to its risk of liver toxicity, periodic liver monitoring is strongly advised with bicalutamide, especially within the first 6 months of treatment. Possible signs of liver toxicity include nausea, vomiting, abdominal pain, fatigue, appetite loss, flu-like symptoms, dark urine, and jaundice (yellowing of the skin/eyes) (Wiki).
In terms of its lung toxicity risk, bicalutamide has been associated rarely with interstitial pneumonitis, which can lead to pulmonary fibrosis and can be fatal, and also less often with eosinophilic lung disease (Wiki; Table). As of writing, 15 published case reports of interstitial pneumonitis and 2 case reports of eosinophilic lung disease in association with bicalutamide therapy exist, likewise all in men with prostate cancer (Table). As with liver toxicity, hundreds of additional cases of interstitial pneumonitis in people taking bicalutamide exist in the United States FAERS database (Wiki; FDA). It has been estimated that interstitial pneumonitis with bicalutamide occurs at a rate of around 1 in 10,000 people, although this may be an underestimate due to under-reporting (Wiki; Ahmad & Graham, 2003). Asian people may be especially likely to experience lung toxicity with bicalutamide and other NSAAs, as much higher incidences have been observed in this population (Mahler et al., 1996; Wu et al., 2022). There is no laboratory test for routine monitoring of lung changes with bicalutamide. Possible signs of relevant lung toxicity include dyspnea (difficulty breathing or shortness of breath), coughing, and pharyngitis (inflammation of the throat, typically manifesting as sore throat) (Wiki).
Aside from liver and lung toxicity, bicalutamide monotherapy has been found in cisgender men with prostate cancer to increase the risk of death due to causes other than prostate cancer (Iversen et al., 2004; Iversen et al., 2006; Wellington & Keam, 2006; Jia & Spratt, 2022; Wiki). This led to marketing authorization of bicalutamide for treatment of the earliest stage of prostate cancer being revoked and to the drug being abandoned for this use (Wiki). Bicalutamide remains approved and used for treatment of later stages of prostate cancer, as the antiandrogenic benefits of bicalutamide against prostate cancer outweigh any adverse influence it has on non-prostate-cancer mortality in these more severe stages. The mechanisms underlying the increase in risk of death with bicalutamide in men are unknown (Wiki). It is also unclear whether bicalutamide could likewise increase the risk of death in transfeminine people. Limitations of generalizing these studies to transfeminine people include the men in the trials being relatively old and ill, a relatively high dosage of bicalutamide (150 mg/day) being used in the trials for an extended duration (e.g., 5 years), the question of whether the risks were due to androgen deprivation or to specific drug-related toxicity of bicalutamide, and estradiol levels with bicalutamide monotherapy in men with prostate cancer being only about 30 to 50 pg/mL (110–184 pmol/L) (Wiki). The preceding estradiol levels are well above castrate levels and are sufficient for a substantial degree of estrogenic effect, but are nonetheless below those recommended for transfeminine people and potentially needed for full sex-hormone replacement (which are ≥50 pg/mL [≥184 pmol/L]). In any case, as the specific mechanisms underlying the increased mortality risk with bicalutamide seen in men with prostate cancer are uncertain, and as clinical safety data showing that the risk does not generalize do not exist, it remains a possibility that bicalutamide could also increase the risk of death in transfeminine people.
Bicalutamide is taken orally in the form of tablets (e.g., 50 and 150 mg) (Wiki). Due to saturation of absorption in the gastrointestinal tract, the oral bioavailability of bicalutamide progressively starts to decrease above a dosage of about 150 mg/day, and there is no further increase in bicalutamide levels above 300 mg/day (Wiki; Graph). Bicalutamide has a very long elimination half-life of about 6 to 10 days (Wiki; Graphs). As a result, it does not necessarily have to be taken daily, and can be dosed less often (in proportionally higher doses)—for instance twice weekly or even once weekly—if this is more convenient or otherwise desired. Due to its long half-life, bicalutamide requires about 4 to 12 weeks to fully reach steady-state levels (Wiki; Graph; Wiki). However, about 50% of steady state is reached within 1 week of administration of bicalutamide, and about 80 to 90% of steady state is reached after 3 to 4 weeks (Wiki; Graph; Wiki). Loading doses of bicalutamide can be taken to reach steady state more quickly if desired. Animal studies originally suggested that bicalutamide did not cross the blood–brain barrier and hence was peripherally selective (i.e., did not block androgen receptors in the brain) (Wiki). However, subsequent clinical studies found that this was not similarly the case in humans, in whom bicalutamide shows clear and robust centrally mediated antiandrogenic effects (Wiki).
Older NSAAs related to bicalutamide like flutamide (Eulexin) and nilutamide (Anandron, Nilandron) have much greater risks in comparison to bicalutamide and should not be used in transfeminine people. Nilutamide was previously characterized as an antiandrogen in transfeminine people in several studies, but was not further pursued probably due to its very high incidence of lung toxicity and other side effects (Aly, 2020; Wiki; Wiki). Flutamide has been used limitedly as an antiandrogen in transfeminine people in the past, but should no longer be used due to a much higher risk of liver toxicity than bicalutamide as well as other side effects and drawbacks (Aly, 2020; Wiki). Other newer and more-potent NSAAs like enzalutamide (Xtandi), apalutamide (Erleada), and darolutamide (Nubeqa) also have risks and have been studied and used little outside of prostate cancer to date.
5α-Reductase Inhibitors
Testosterone is converted into DHT within certain tissues in the body (Swerdloff et al., 2017). DHT is an androgen metabolite of testosterone with several-fold higher activity than testosterone. The transformation of testosterone into DHT is mediated by the enzyme 5α-reductase. The tissues in which 5α-reductase is present and testosterone is converted into DHT are limited but most importantly include the skin, hair follicles, and prostate gland. Although DHT is more potent than testosterone, it is thought to have minimal biological role as a circulating hormone (Horton, 1992; Swerdloff et al., 2017). Instead, testosterone serves as the main circulating androgen, and the role of DHT is thought to be mainly via local metabolism and potentiation of testosterone into DHT within certain tissues.
5α-Reductase inhibitors (5α-RIs), such as finasteride (Proscar, Propecia) and dutasteride (Avodart), inhibit 5α-reductase and thereby block the conversion of testosterone into DHT. This results in marked decreases in circulating and within-tissue levels of DHT. Due to the primary role of DHT as a mediator in tissues rather than as circulating hormone, the antiandrogenic efficacy of 5α-RIs is limited. This is evidenced by the fact that they are well-tolerated in cisgender men and do not cause notable demasculinization in these individuals (Hirshburg, 2016). The medical use of 5α-RIs is mainly restricted to the treatment of scalp hair loss in men and women, hirsutism (excessive facial/body hair) in women, and prostate enlargement in men. They might also be useful for acne in women, but evidence of this is very limited (Wiki). Due to their specificity, 5α-RIs are inappropriate as general antiandrogens in transfeminine people. Moreover, DHT levels decrease in tandem with testosterone levels with suppression of testosterone production in transfeminine hormone therapy, and routine use of 5α-RIs in transfeminine people with testosterone levels within the female range is of limited usefulness and can be considered unnecessary (Gooren et al., 2016; Irwig, 2020; Prince & Safer, 2020; Glintborg et al., 2021). In any case, 5α-RIs may be useful in transfeminine people on hormone therapy who have persistent body hair growth or scalp hair loss—as they have been shown to be in cisgender women (Barrionuevo et al., 2018; Prince & Safer, 2020). However, it is notable that evidence of effectiveness in cisgender women is better for androgen receptor antagonists for such indications (van Zuuren et al., 2015). This is intuitive as androgen receptor antagonists block both testosterone and DHT whereas 5α-RIs only prevent conversion of testosterone into DHT. Hence, although 5α-RIs strongly reduce or eliminate DHT and their net effect is antiandrogenic, they do not decrease testosterone levels and in fact increase them.
There are three subtypes of 5α-reductase. Dutasteride inhibits all three subtypes of 5α-reductase whereas finasteride only inhibits two of the subtypes. As a result of this, dutasteride is a more complete 5α-RI than finasteride. Dutasteride decreases DHT levels in the blood by up to 98% while finasteride can only decrease them by around 65 to 70%. As nearly all circulating DHT originates from synthesis in peripheral tissues, these decreases indicate parallel reductions in tissue DHT production (Horton, 1992). In accordance with these findings, dutasteride has been found to be more effective than finasteride in the treatment of scalp hair loss in men (Zhou et al., 2018; Dhurat et al., 2020; Wiki). For these reasons, although both finasteride and dutasteride are effective 5α-RIs, dutasteride may be the preferable choice if a 5α-RI is used (Zhou et al., 2018; Dhurat et al., 2020).
A potentially undesirable effect of 5α-RIs in transfeminine people is that they may increase circulating testosterone levels to a degree in those in whom testosterone production isn’t fully suppressed (Leinung, Feustel, & Joseph, 2018; Aly, 2019; Traish et al., 2019; Irwig, 2020; Glintborg et al., 2021). It appears that DHT adds significantly to negative feedback on gonadotropin secretion in the pituitary gland in people with testes who have low testosterone levels relative to the normal male range (Traish et al., 2019). The therapeutic implications of this for transfeminine people, if any, are uncertain.
Clinical dose-ranging studies have found that lower doses of finasteride and dutasteride than are typically used still provide substantial or near-maximal 5α-reductase inhibition (Gormley et al., 1990; Vermeulen et al., 1991; Sudduth & Koronkowski, 1993; Drake et al., 1999; Roberts et al., 1999; Clark et al., 2004; Frye, 2006; Olsen et al., 2006; Harcha et al., 2014; Kuhl & Wiegratz, 2017). In one study with finasteride for instance, DHT levels decreased by 49.5% at 0.05 mg/day, 68.6% at 0.2 mg/day, 71.4% at 1 mg/day, and 72.2% at 5 mg/day (Drake et al., 1999). Parallel reductions in DHT levels were seen locally in the scalp (Drake et al., 1999). In a study with dutasteride, DHT levels were decreased by 52.9% at 0.05 mg/day, 94.7% at 0.5 mg/day, 97.7% at 2.5 mg/day, and 98.4% at 5 mg/day (Clark et al., 2004). Based on these findings, 5α-RIs can potentially be taken at lower doses to help reduce medication costs if needed. Finasteride tablets can be split to achieve smaller doses. Conversely, dutasteride cannot be split as it is formulated as an oil capsule. However, dutasteride has a long half-life, and instead of dividing pills, it can be taken less frequently (e.g., once every few days) as a means of reducing dosage.
5α-Reductase inhibitors are taken orally in the form of tablets and capsules. Compoundedtopical formulations of finasteride also exist (Marks et al., 2020). However, caution is advised with these preparations as they have been found to be excessively dosed and to produce equivalent systemic DHT suppression as oral finasteride formulations (Marks et al., 2020). Lower-concentration formulations of topical finsteride on the other hand may be more locally selective (Marks et al., 2020).
Table 8: Available forms and recommended doses of 5α-reductase inhibitors for transfeminine people:
GnRH agonists and antagonists (GnRHa), also known as GnRH receptor agonists and antagonists or GnRH modulators, are antiandrogens which work by preventing the effects of GnRH in the pituitary gland and thereby suppressing LH and FSH secretion. Receptor agonists normally activate receptors while receptor antagonists block and thereby inhibit the activation of receptors. Due to a physiological quirk however, GnRH agonists and antagonists have the same effects in the pituitary gland. This is because GnRH is secreted in pulses under normal physiological circumstances, and when the GnRH receptor is unnaturally activated in a continuous manner, as with exogenous GnRH agonists, the GnRH receptor in the pituitary gland is strongly desensitized to the point of becoming inactive. Consequently, both GnRH agonists and GnRH antagonists have the effect of abolishing gonadal sex hormone production. This, in turn, reduces testosterone levels into the castrate or normal female range (both <50 ng/dL or <1.7 nmol/L) in people with testes. GnRHa are like a reversible gonadectomy, and for this reason, are also sometimes referred to as “medical castration”. Provided that an estrogen is taken in combination with a GnRHa to prevent sex hormone deficiency, these medications have essentially no known side effects or risks. For these reasons, GnRHa are the ideal antiandrogens for use in transfeminine people.
GnRHa are widely used to suppess puberty in adolescent transgender individuals. Unfortunately however, they are very expensive (e.g., ~US$10,000 per year) and medical insurance does not usually cover them for adult transgender people. Consequently, GnRHa are not commonly used in adult transfeminine people at this time. An exception is in the United Kingdom, where GnRH agonists are covered for all adult transgender people by the National Health Service (NHS). Another exception is buserelin (Suprefact), which has become available very inexpensively in its nasal spray form from certain Eastern European online pharmacies in recent years (Aly, 2018).
GnRH agonists cause a brief flare in testosterone levels at the start of therapy prior to the GnRH receptors in the pituitary gland becoming desensitized (Wiki). Testosterone levels increase by up to about 1.5- to 2-fold for about 1 week and then decrease thereafter (Wiki). Castrate or female-range levels of testosterone are generally reached within 2 to 4 weeks (Wiki). In contrast to GnRH agonists, there is no testosterone flare with GnRH antagonists and testosterone levels start decreasing immediately, reaching castrate levels within a few days (Wiki; Graph). This is because GnRH antagonists work by blocking the GnRH receptor without initially activating it, and hence desensitization of the receptor is not necessary for their action. If desired, the testosterone flare at the initiation of GnRH agonist therapy can be prevented or blunted with the use of antigonadotropins, for instance estrogens and progestogens, as well as with potent androgen receptor antagonists such as bicalutamide (Wiki).
GnRH agonists must be injected subcutaneously or intramuscularly once per day or once every one to six months depending on the formulation employed (buserelin, goserelin, leuprorelin, triptorelin). Alternatively, they can be surgically implanted once a year (histrelin, leuprorelin) or used as a nasal spray two to three times per day (buserelin, nafarelin). The first GnRH antagonists were developed for use by once-monthly intramuscular or subcutaneous injection (abarelix, degarelix). More recently, orally administered GnRH antagonists such as elagolix and relugolix have been introduced for medical use. They are taken in the form of tablets once or twice daily.
Table 9: Available forms and recommended doses of GnRH agonists for transfeminine people:
a 500 μg 3x/day for the first week then 200 μg/day. b 800 μg 3x/day for the first week then 400 μg 3x/day. c 500 μg 2x/day can be used instead of 400 μg 3x/day but is less effective (70% decrease in testosterone levels (to ~180 ng/dL [6.2 nmol/L]) instead of 90% decrease (to ~50 ng/dL [1.7 nmol/L]) per available studies of buserelin in men with prostate cancer) (Aly, 2018; Wiki).
Table 10: Available forms and recommended doses of GnRH antagonists for transfeminine people:
a First month is 240 mg then 80 mg per month thereafter. b 150 mg 1x/day is less effective than 200 mg 2x/day (which provides full gonadal sex-hormone suppression in cisgender women) (Wiki). c 80–120 mg/day for full gonadal sex-hormone suppression and 20–40 mg/day for substantial but partial gonadal sex-hormone suppression (MacLean et al., 2015; DailyMed).
Other Hormonal Medications
Androgens and Anabolic Steroids
In addition to estrogens, progestogens, and antiandrogens, androgens/anabolic steroids (AAS) are sometimes added to transfeminine hormone therapy. This is when testosterone levels are low (e.g., below the female average of 30 ng/dL [1.0 nmol/L]) and androgen replacement is desired. It has been proposed that adequate levels of testosterone may provide benefits such as increased sexual desire, improved mood and energy, positive effects on skin health and cellulite (Avram, 2004), and increased muscle size and strength (Huang & Basaria, 2017). However, there is insufficient clinical evidence to support such benefits at present, and androgens can produce adverse effects in cisgender women and transfeminine people, for instance acne, hirsutism, scalp hair loss, and masculinization (Wiki). For transfeminine people who nonetheless desire androgen replacement therapy, possible options for androgen medications include testosterone and its esters, dehydroepiandrosterone (DHEA; prasterone), and nandroloneesters such as nandrolone decanoate (ND) (Aly, 2020; Table), among others.
Monitoring of Therapy
Transfeminine people on hormone therapy should undergo regular laboratory monitoring in the form of blood work to assess efficacy and monitor for safety. Total estradiol levels and total testosterone levels should be measured to assess the effectiveness of therapy—that is, whether hormone levels are in appropriate ranges for cisgender females—and determine whether medication adjustments may be necessary. Levels of free testosterone, free estradiol, estrone (E1), dihydrotestosterone (DHT), luteinizing hormone (LH), follicle-stimulating hormone (FSH), and sex hormone-binding globulin (SHBG) can also be measured to provide further information although they’re not absolutely necessary. If progesterone is used as a part of hormone therapy, progesterone levels can be measured to provide insight on the degree of progesterone exposure. In addition to hormone blood tests, transfeminine people can monitor their physical changes with hormone therapy, such as breast development and other aspects of feminization, using various physical and digital measurement methods (e.g., Wiki).
Certain therapeutic situations can result in inaccurate lab blood work results. Monitoring of progesterone levels with oral progesterone using immunoassay-based blood tests can result in falsely high readings for progesterone levels due to cross-reactivity with high levels of progesterone metabolites such as allopregnanolone (Aly, 2018; Wiki). Instead of immunoassay-based tests, mass spectrometry-based tests should be used to determine progesterone levels with oral progesterone (Aly, 2018; Wiki). Conversely, either type of test may be used to measure progesterone levels with non-oral progesterone therapy. High-dose biotin (vitamin B7) supplements can interfere with the accuracy of immunoassay-based hormone blood tests, causing falsely low or falsely high readings (Samarasinghe et al., 2017; Avery, 2019; Bowen et al., 2019; FDA, 2019; Luong, Male, & Glennon, 2019). Transdermal estradiol formulations applied to the arm can result in contamination of blood draws taken from the same arm and can result in falsely high readings for estradiol levels (Vihtamäkia, Luukkaala, & Tuimala, 2004).
Certain cancers are known to be hormone-sensitive and their incidence can be influenced by hormone therapy. Screening for breast and prostate cancer is recommended in transfeminine people (Sterling & Garcia, 2020; Iwamoto et al., 2021). The risk of breast cancer appears to be dramatically increased with transfeminine hormone therapy, perhaps especially with progestogens (Aly, 2020). However, the risk still remains lower than in cisgender women (Aly, 2020). The incidence of prostate cancer is greatly decreased with hormone therapy in transfeminine people as a consequence of androgen deprivation, but the risk is not abolished and prostate cancer can still occur (de Nie et al., 2020). The prostate gland is not removed with vaginoplasty, so transfeminine people who have undergone vaginoplasty will also require monitoring for prostate cancer still. Testicular cancer is not known to be a hormone-dependent cancer and its incidence does not appear to be increased with hormone therapy in transfeminine people (Bensley et al., 2021; de Nie et al., 2021; Jacoby et al., 2021).
Ahmad, S. R., & Graham, D. J. (2003). Pneumonitis with Antiandrogens. Annals of Internal Medicine, 139(6), 528–529. [DOI:10.7326/0003-4819-139-6-200309160-00023]
Allen, A. N., Jiao, R., Day, P., Pagels, P., Gimpel, N., & SoRelle, J. A. (2020). Dynamic Impact of Hormone Therapy on Laboratory Values in Transgender Patients over Time. The Journal of Applied Laboratory Medicine, 6(1), 27–40. [DOI:10.1093/jalm/jfaa192]
Angus, L., Leemaqz, S., Ooi, O., Cundill, P., Silberstein, N., Locke, P., Zajac, J. D., & Cheung, A. S. (2019). Cyproterone acetate or spironolactone in lowering testosterone concentrations for transgender individuals receiving oestradiol therapy. Endocrine Connections, 8(7), 935–940. [DOI:10.1530/ec-19-0272]
Angus, L. M., Nolan, B. J., Zajac, J. D., & Cheung, A. S. (2020). A systematic review of antiandrogens and feminization in transgender women. Clinical Endocrinology, 94(5), 743–752. [DOI:10.1111/cen.14329]
Antoniou, T., Gomes, T., Mamdani, M. M., Yao, Z., Hellings, C., Garg, A. X., Weir, M. A., & Juurlink, D. N. (2011). Trimethoprim-sulfamethoxazole induced hyperkalaemia in elderly patients receiving spironolactone: nested case-control study. BMJ, 343, d5228. [DOI:10.1136/bmj.d5228]
Antoniou, T., Hollands, S., Macdonald, E. M., Gomes, T., Mamdani, M. M., & Juurlink, D. N. (2015). Trimethoprim–sulfamethoxazole and risk of sudden death among patients taking spironolactone. Canadian Medical Association Journal, 187(4), E138–E143. [DOI:10.1503/cmaj.140816]
Aufrère, M. B., & Benson, H. (1976). Progesterone: An overview and recent advances. Journal of Pharmaceutical Sciences, 65(6), 783–800. [DOI:10.1002/jps.2600650602]
Avery, G. (2019). Biotin interference in immunoassay: a review for the laboratory scientist. Annals of Clinical Biochemistry: International Journal of Laboratory Medicine, 56(4), 424–430. [DOI:10.1177/0004563219842231]
Avram, M. M. (2004). Cellulite: a review of its physiology and treatment. Journal of Cosmetic and Laser Therapy, 6(4), 181–185. [DOI:10.1080/14764170410003057]
Babich, J. S., Kalantar-Zadeh, K., & Joshi, S. (2022). Taking the Kale out of Hyperkalemia: Plant Foods and Serum Potassium in Patients With Kidney Disease. Journal of Renal Nutrition, 32(6), 641–649. [DOI:10.1053/j.jrn.2022.01.013]
Bäckström, T., Haage, D., Löfgren, M., Johansson, I., Strömberg, J., Nyberg, S., Andréen, L., Ossewaarde, L., van Wingen, G., Turkmen, S., & Bengtsson, S. (2011). Paradoxical effects of GABA-A modulators may explain sex steroid induced negative mood symptoms in some persons. Neuroscience, 191, 46–54. [DOI:10.1016/j.neuroscience.2011.03.061]
Barrionuevo, P., Nabhan, M., Altayar, O., Wang, Z., Erwin, P. J., Asi, N., Martin, K. A., & Murad, M. H. (2018). Treatment Options for Hirsutism: A Systematic Review and Network Meta-Analysis. The Journal of Clinical Endocrinology & Metabolism, 103(4), 1258–1264. [DOI:10.1210/jc.2017-02052]
Bazarra-Castro, M. A. (2009). Etiological aspects, therapy regimes, side effects and treatment satisfaction of transsexual patients. (Doctoral dissertation, Ludwig Maximilian University of Munich.) [DOI:10.5282/edoc.9984] [URN:urn:nbn:de:bvb:19-99840] [PDF]
Belisle, S., & Love, E. J. (1986). Clinical efficacy and safety of cyproterone acetate in severe hirsutism: results of a multicentered Canadian study. Fertility and Sterility, 46(6), 1015–1020. [DOI:10.1016/s0015-0282(16)49873-0]
Ben Salem, C., Badreddine, A., Fathallah, N., Slim, R., & Hmouda, H. (2014). Drug-Induced Hyperkalemia. Drug Safety, 37(9), 677–692. [DOI:10.1007/s40264-014-0196-1]
Bensley, J. G., Cheung, A. S., Grossmann, M., & Papa, N. (2022). Testicular Cancer in Trans People Using Feminising Hormone Therapy–A Brief Review. Urology, 160, 1–4. [DOI:10.1016/j.urology.2021.11.014]
Bessone, F., Lucena, M., Roma, M. G., Stephens, C., Medina-Cáliz, I., Frider, B., Tsariktsian, G., Hernández, N., Bruguera, M., Gualano, G., Fassio, E., Montero, J., Reggiardo, M. V., Ferretti, S., Colombato, L., Tanno, F., Ferrer, J., Zeno, L., Tanno, H., & Andrade, R. J. (2015). Cyproterone acetate induces a wide spectrum of acute liver damage including corticosteroid-responsive hepatitis: report of 22 cases. Liver International, 36(2), 302–310. [DOI:10.1111/liv.12899]
Boogers, L. S., Sardo Infirri, S. A., Bouchareb, A., Dijkman, B. A., Helder, D., de Blok, C. J., Liberton, N. P., den Heijer, M., van Trotsenburg, A. S., Dreijerink, K. M., Wiepjes, C. M., & Hannema, S. E. (2025). Variations in Volume: Breast Size in Trans Women in Relation to Timing of Testosterone Suppression. The Journal of Clinical Endocrinology & Metabolism, 110(5), e1404–e1410. [DOI:10.1210/clinem/dgae573]
Bowen, R., Benavides, R., Colón-Franco, J. M., Katzman, B. M., Muthukumar, A., Sadrzadeh, H., Straseski, J., Klause, U., & Tran, N. (2019). Best practices in mitigating the risk of biotin interference with laboratory testing. Clinical Biochemistry, 74, 1–11. [DOI:10.1016/j.clinbiochem.2019.08.012]
Brown, J., Farquhar, C., Lee, O., Toomath, R., & Jepson, R. G. (2009). Spironolactone versus placebo or in combination with steroids for hirsutism and/or acne. Cochrane Database of Systematic Reviews, 2009(2), CD000194. [DOI:10.1002/14651858.cd000194.pub2]
Burinkul, S., Panyakhamlerd, K., Suwan, A., Tuntiviriyapun, P., & Wainipitapong, S. (2021). Anti-Androgenic Effects Comparison Between Cyproterone Acetate and Spironolactone in Transgender Women: A Randomized Controlled Trial. The Journal of Sexual Medicine, 18(7), 1299–1307. [DOI:10.1016/j.jsxm.2021.05.003]
Callen-Lorde Community Health Center. (2018). Protocols for the Provision of Hormone Therapy. New York City: Callen-Lorde Community Health Center. [URL] [PDF]
Cappelletti, M., & Wallen, K. (2016). Increasing women’s sexual desire: The comparative effectiveness of estrogens and androgens. Hormones and Behavior, 78, 178–193. [DOI:10.1016/j.yhbeh.2015.11.003]
Carmina, E., Stanczyk, F. Z., & Lobo, R. A. (2019). Evaluation of Hormonal Status. In Strauss, J. F., & Barbieri, R. L. (Eds.). Yen and Jaffe’s Reproductive Endocrinology: Physiology, Pathophysiology, and Clinical Management, 8th Edition (pp. 887–915.e4). Philadelphia: Elsevier. [DOI:10.1016/b978-0-323-47912-7.00034-2]
Carvalho, R. d., Santos, L. D., Ramos, P. M., Machado, C. J., Acioly, P., Frattini, S. C., Barcaui, C. B., Donda, A. L., & Melo, D. F. (2022). Bicalutamide and the new perspectives for female pattern hair loss treatment: What dermatologists should know. Journal of Cosmetic Dermatology, 21(10), 4171–4175. [DOI:10.1111/jocd.14773]
Chang, J. J., Tran, N. K., Flentje, A., Lubensky, M. E., Obedin-Maliver, J., Lunn, M. R., & Ariel, D. (2024). 12330 Progestogen Experience And Perception Among Transfeminine Adults - A National Survey. Journal of the Endocrine Society, 8(Suppl 1), bvae163.1657. [DOI:10.1210/jendso/bvae163.1657]
Clark, R. V., Hermann, D. J., Cunningham, G. R., Wilson, T. H., Morrill, B. B., & Hobbs, S. (2004). Marked Suppression of Dihydrotestosterone in Men with Benign Prostatic Hyperplasia by Dutasteride, a Dual 5α-Reductase Inhibitor. The Journal of Clinical Endocrinology & Metabolism, 89(5), 2179–2184. [DOI:10.1210/jc.2003-030330]
Coleman, E., Radix, A. E., Bouman, W. P., Brown, G. R., de Vries, A. L., Deutsch, M. B., Ettner, R., Fraser, L., Goodman, M., Green, J., Hancock, A. B., Johnson, T. W., Karasic, D. H., Knudson, G. A., Leibowitz, S. F., Meyer-Bahlburg, H. F., Monstrey, S. J., Motmans, J., Nahata, L., … & Arcelus, J. (2022). [World Professional Association for Transgender Health (WPATH)] Standards of Care for the Health of Transgender and Gender Diverse People, Version 8. International Journal of Transgender Health, 23(Suppl 1), S1–S259. [DOI:10.1080/26895269.2022.2100644] [URL] [PDF]
Collaborative Group on Hormonal Factors in Breast Cancer. (2019). Type and timing of menopausal hormone therapy and breast cancer risk: individual participant meta-analysis of the worldwide epidemiological evidence. The Lancet, 394(10204), 1159–1168. [DOI:10.1016/s0140-6736(19)31709-x]
Collet, S., Gieles, N. C., Wiepjes, C. M., Heijboer, A. C., Reyns, T., Fiers, T., Lapauw, B., den Heijer, M., & T’Sjoen, G. (2022). Changes in Serum Testosterone and Adrenal Androgen Levels in Transgender Women With and Without Gonadectomy. The Journal of Clinical Endocrinology & Metabolism, 108(2), 331–338. [DOI:10.1210/clinem/dgac576]
Colonnello, E., Graziani, A., Rossetti, R., Voltan, G., Masi, D., Lubrano, C., Mariani, S., Watanabe, M., Isidori, A. M., Ferlin, A., & Gnessi, L. (2025). The Chronobiology of Hormone Administration: “Doctor, What Time Should I Take My Medication?”. Endocrine Reviews, bnaf013. [DOI:10.1210/endrev/bnaf013]
Connors, J. M., & Middeldorp, S. (2019). Transgender patients and the role of the coagulation clinician. Journal of Thrombosis and Haemostasis, 17(11), 1790–1797. [DOI:10.1111/jth.14626]
Cupisti, A., Kovesdy, C., D’Alessandro, C., & Kalantar-Zadeh, K. (2018). Dietary Approach to Recurrent or Chronic Hyperkalaemia in Patients with Decreased Kidney Function. Nutrients, 10(3), 261–261. [DOI:10.3390/nu10030261]
Cusan, L., Dupont, A., Gomez, J., Tremblay, R. R., & Labrie, F. (1994). Comparison of flutamide and spironolactone in the treatment of hirsutism: a randomized controlled trial. Fertility and Sterility, 61(2), 281–287. [DOI:10.1016/s0015-0282(16)56518-2]
de Blok, C. J., Wiepjes, C. M., Nota, N. M., van Engelen, K., Adank, M. A., Dreijerink, K. M., Barbé, E., Konings, I. R., & den Heijer, M. (2019). Breast cancer risk in transgender people receiving hormone treatment: nationwide cohort study in the Netherlands. BMJ, 365, l1652. [DOI:10.1136/bmj.l1652]
de Blok, C. J., Dijkman, B. A., Wiepjes, C. M., Staphorsius, A. S., Timmermans, F. W., Smit, J. M., Dreijerink, K. M., & den Heijer, M. (2021). Sustained Breast Development and Breast Anthropometric Changes in 3 Years of Gender-Affirming Hormone Treatment. The Journal of Clinical Endocrinology & Metabolism, 106(2), e782–e790. [DOI:10.1210/clinem/dgaa841]
de Nie, I., de Blok, C. J., van der Sluis, T. M., Barbé, E., Pigot, G. L., Wiepjes, C. M., Nota, N. M., van Mello, N. M., Valkenburg, N. E., Huirne, J., Gooren, L. J., van Moorselaar, R. J., Dreijerink, K. M., & den Heijer, M. (2020). Prostate Cancer Incidence under Androgen Deprivation: Nationwide Cohort Study in Trans Women Receiving Hormone Treatment. The Journal of Clinical Endocrinology & Metabolism, 105(9), e3293–e3299. [DOI:10.1210/clinem/dgaa412]
Deng, T., Duan, X., He, Z., Zhao, Z., & Zeng, G. (2020). Association Between 5-Alpha Reductase Inhibitor Use and The Risk of Depression: A Meta-Analysis. Urology Journal, 18(2), 144–150. [DOI:10.22037/uj.v16i7.5866]
Deutsch, M. B. (2016). Overview of feminizing hormone therapy. In Deutsch, M. B. (Ed.). Guidelines for the Primary and Gender-Affirming Care of Transgender and Gender Nonbinary People, 2nd Edition (pp. 26–48). San Francisco: University of California, San Francisco/UCSF Transgender Care. [URL] [PDF]
Dhurat, R., Sharma, A., Rudnicka, L., Kroumpouzos, G., Kassir, M., Galadari, H., Wollina, U., Lotti, T., Golubovic, M., Binic, I., Grabbe, S., & Goldust, M. (2020). 5‐Alpha reductase inhibitors in androgenetic alopecia: Shifting paradigms, current concepts, comparative efficacy, and safety. Dermatologic Therapy, 33(3), e13379. [DOI:10.1111/dth.13379]
Drake, L., Hordinsky, M., Fiedler, V., Swinehart, J., Unger, W. P., Cotterill, P. C., Thiboutot, D. M., Lowe, N., Jacobson, C., Whiting, D., Stieglitz, S., Kraus, S. J., Griffin, E. I., Weiss, D., Carrington, P., Gencheff, C., Cole, G. W., Pariser, D. M., Epstein, E. S., Tanaka, W., Dallob, A., Vandormael, K., Geissler, L., & Waldsteicher, J. (1999). The effects of finasteride on scalp skin and serum androgen levels in men with androgenetic alopecia. Journal of the American Academy of Dermatology, 41(4), 550–554. [DOI:10.1016/s0190-9622(99)80051-6]
Dyson, T. E., Cantrell, M. A., & Lund, B. C. (2020). Lack of Association between 5α-Reductase Inhibitors and Depression. Journal of Urology, 204(4), 793–798. [DOI:10.1097/ju.0000000000001079]
Erem, C. (2013). Update on idiopathic hirsutism: diagnosis and treatment. Acta Clinica Belgica, 68(4), 268–274. [DOI:10.2143/acb.3267]
Erenus, M., Gürbüz, O., Durmuşoğlu, F., Demirçay, Z., & Pekin, S. (1994). Comparison of the efficacy of spironolactone versus flutamide in the treatment of hirsutism. Fertility and Sterility, 61(4), 613–616. [DOI:10.1016/s0015-0282(16)56634-5]
Esoterix/LabCorp. (2020). Endocrinology Expected Values and S.I. Unit Conversion Tables. LabCorp/Endocrine Sciences. [PDF]
Even Zohar, N., Sofer, Y., Yaish, I., Serebro, M., Tordjman, K., & Greenman, Y. (2021). Low-Dose Cyproterone Acetate Treatment for Transgender Women. The Journal of Sexual Medicine, 18(7), 1292–1298. [DOI:10.1016/j.jsxm.2021.04.008]
Fertig, R., Shapiro, J., Bergfeld, W., & Tosti, A. (2016). Investigation of the Plausibility of 5-Alpha-Reductase Inhibitor Syndrome. Skin Appendage Disorders, 2(3–4), 120–129. [DOI:10.1159/000450617]
Food and Drug Administration. (2019). UPDATE: The FDA Warns that Biotin May Interfere with Lab Tests: FDA Safety Communication. Food and Drug Administration. [URL]
Fournier, A., Berrino, F., & Clavel-Chapelon, F. (2007). Unequal risks for breast cancer associated with different hormone replacement therapies: results from the E3N cohort study. Breast Cancer Research and Treatment, 107(1), 103–111. [DOI:10.1007/s10549-007-9523-x]
Frye, S. (2006). Discovery and Clinical Development of Dutasteride, a Potent Dual 5α-Reductase Inhibitor. Current Topics in Medicinal Chemistry, 6(5), 405–421. [DOI:10.2174/156802606776743101]
Gava, G., Mancini, I., Alvisi, S., Seracchioli, R., & Meriggiola, M. C. (2020). A comparison of 5-year administration of cyproterone acetate or leuprolide acetate in combination with estradiol in transwomen. European Journal of Endocrinology, 183(6), 561–569. [DOI:10.1530/eje-20-0370]
Getzenberg, R., & Itty, S. (2020). How do we define “castration” in men on androgen deprivation therapy? Asian Journal of Andrology, 22(5), 441–446. [DOI:10.4103/aja.aja_139_19]
Giltay, E. J., Gooren, L. J., Toorians, A. W., Katan, M. B., & Zock, P. L. (2004). Docosahexaenoic acid concentrations are higher in women than in men because of estrogenic effects. The American Journal of Clinical Nutrition, 80(5), 1167–1174. [DOI:10.1093/ajcn/80.5.1167]
Glintborg, D., T’Sjoen, G., Ravn, P., & Andersen, M. S. (2021). MANAGEMENT OF ENDOCRINE DISEASE: Optimal feminizing hormone treatment in transgender people. European Journal of Endocrinology, 185(2), R49–R63. [DOI:10.1530/eje-21-0059]
Goletiani, N. V., Keith, D. R., & Gorsky, S. J. (2007). Progesterone: Review of safety for clinical studies. Experimental and Clinical Psychopharmacology, 15(5), 427–444. [DOI:10.1037/1064-1297.15.5.427]
Goodfellow, A., Alaghband-Zadeh, J., Carter, G., Cream, J., Holland, S., Scully, J., & Wise, P. (1984). Oral spironolactone improves acne vulgaris and reduces sebum excretion. British Journal of Dermatology, 111(2), 209–214. [DOI:10.1111/j.1365-2133.1984.tb04045.x]
Gooren, L. J. (2016). The Endocrinology of Sexual Behavior and Gender Identity. In Jameson, J. L., & De Groot, L. J. (Eds.). Endocrinology: Adult and Pediatric, 7th Edition, Volume 2 (pp. 2163–2176.e4). Philadelphia: Saunders/Elsevier. [Google Books] [DOI:10.1016/B978-0-323-18907-1.00124-4]
Gooren, L. J., Harmsen-Louman, W., & Kessel, H. (1985). Follow-up of prolactin levels in long-term oestrogen-treated male-to-female transsexuals with regard to prolactinoma induction. Clinical Endocrinology, 22(2), 201–207. [DOI:10.1111/j.1365-2265.1985.tb01081.x]
Gooren, L., Rao, B., van Kessel, H., & Harmsen-Louman, W. (1984). Estrogen positive feedback on LH secretion in transsexuality. Psychoneuroendocrinology, 9(3), 249–259. [DOI:10.1016/0306-4530(84)90004-0]
Gormley, G. J., Stoner, E., Rittmaster, R. S., Gregg, H., Thompson, D. L., Lasseter, K. C., Vlasses, P. H., & Stein, E. A. (1990). Effects of Finasteride (MK-906), a 5α-Reductase Inhibitor, on Circulating Androgens in Male Volunteers. The Journal of Clinical Endocrinology & Metabolism, 70(4), 1136–1141. [DOI:10.1210/jcem-70-4-1136]
Grock, S., Weinreb, J., Williams, K. C., Weimer, A., Fadich, S., Patel, R., Geft, A., & Korenman, S. (2024). Priorities for efficacy trials of gender-affirming hormone therapy with estrogen: collaborative design and results of a community survey. Hormones, online ahead of print. [DOI:10.1007/s42000-024-00532-3]
Gubelin Harcha, W., Barboza Martínez, J., Tsai, T., Katsuoka, K., Kawashima, M., Tsuboi, R., Barnes, A., Ferron-Brady, G., & Chetty, D. (2014). A randomized, active- and placebo-controlled study of the efficacy and safety of different doses of dutasteride versus placebo and finasteride in the treatment of male subjects with androgenetic alopecia. Journal of the American Academy of Dermatology, 70(3), 489–498.e3. [DOI:10.1016/j.jaad.2013.10.049]
Gupta, P., Suppakitjanusant, P., Stevenson, M., Goodman, M., & Tangpricha, V. (2022). Potassium Concentrations in Transgender Women Using Spironolactone: A Retrospective Chart Review. Endocrine Practice, 28(11), 1113–1117. [DOI:10.1016/j.eprac.2022.08.007]
Hammerstein, J. (1990). Antiandrogens: Clinical Aspects. In Orfanos, C. E., & Happle, R. (Eds.). Hair and Hair Diseases (pp. 827–886). Berlin/Heidelberg: Springer. [DOI:10.1007/978-3-642-74612-3_35]
Hayes, H., Russell, R., Haugen, A., Nagavally, S., & Sarvaideo, J. (2022). The Utility of Monitoring Potassium in Transgender, Gender Diverse, and Nonbinary Individuals on Spironolactone. Journal of the Endocrine Society, 6(11), bvac133. [DOI:10.1210/jendso/bvac133]
Heinemann, L. A., Will-Shahab, L., van Kesteren, P., Gooren, L. J., & (1997). Safety of Cyproterone Acetate: Report of Active Surveillance. Pharmacoepidemiology and Drug Safety, 6(3), 169–178. [DOI:10.1002/(sici)1099-1557(199705)6:3<169::aid-pds263>3.0.co;2-3]
Hembree, W. C., Cohen-Kettenis, P. T., Gooren, L., Hannema, S. E., Meyer, W. J., Murad, M. H., Rosenthal, S. M., Safer, J. D., Tangpricha, V., & T’Sjoen, G. G. (2017). Endocrine Treatment of Gender-Dysphoric/Gender-Incongruent Persons: An Endocrine Society Clinical Practice Guideline. The Journal of Clinical Endocrinology and Metabolism, 102(11), 3869–3903. [DOI:10.1210/jc.2017-01658] [PDF]
Herndon, J. S., Maheshwari, A. K., Nippoldt, T. B., Carlson, S. J., Davidge-Pitts, C. J., & Chang, A. Y. (2023). Comparison of the Subcutaneous and Intramuscular Estradiol Regimens as Part of Gender-Affirming Hormone Therapy. Endocrine Practice, 29(5), 356–361. [DOI:10.1016/j.eprac.2023.02.006]
Hirshburg, J. M., Kelsey, P. A., Therrien, C. A., Gavino, A. C., & Reichenberg, J. S. (2016). Adverse Effects and Safety of 5-alpha Reductase Inhibitors (Finasteride, Dutasteride): A Systematic Review. The Journal of Clinical and Aesthetic Dermatology, 9(7), 56–62. [PubMed] [PubMed Central]
Hopkins, U., & Arias, C. Y. (2013). Large-volume IM injections: a review of best practices. Oncology Nurse Advisor, 4(1), 32–37. [Google Scholar] [URL] [PDF]
Horton, R. (1992). Dihydrotestosterone Is a Peripheral Paracrine Hormone. Journal of Andrology, 13(1), 23–27. [DOI:10.1002/j.1939-4640.1992.tb01621.x]
Huang, G., & Basaria, S. (2017). The Case for Androgens in Menopausal Women: When and How? In Pal, L., & Sayegh, R. A. (Eds.). Essentials of Menopause Management: A Case-Based Approach (pp. 173–196). Cham: Springer International Publishing. [DOI:10.1007/978-3-319-42451-4_10]
Igo, J., & Visram, H. (2021). Testosterone Suppression With Injectable Estrogen Therapy Alone in Male to Female Transgender Patients. Canadian Journal of Diabetes, 45(7 Suppl), S40–S40 (abstract no. 114). [DOI:10.1016/j.jcjd.2021.09.124] [URL]
Irwig, M. S. (2020). Is there a role for 5α‐reductase inhibitors in transgender individuals? Andrology, 9(6), 1729–1731. [DOI:10.1111/andr.12881]
Iversen, P., Johansson, J. E., Lodding, P., Lukkarinen, O., Lundmo, P., Klarskov, P., Tammela, T. L., Tasdemir, I., Morris, T., Carroll, K., & Scandinavian Prostatic Cancer Group. (2004). Bicalutamide (150 mg) versus placebo as immediate therapy alone or as adjuvant to therapy with curative intent for early nonmetastatic prostate cancer: 5.3-year median followup from the Scandinavian Prostate Cancer Group Study Number 6. The Journal of Urology, 172(5 Part 1), 1871–1876. [DOI:10.1097/01.ju.0000139719.99825.54]
Iversen, P., Johansson, J., Lodding, P., Kylmälä, T., Lundmo, P., Klarskov, P., Tammela, T. L., Tasdemir, I., Morris, T., Armstrong, J., & (2006). Bicalutamide 150 mg in addition to standard care for patients with early non-metastatic prostate cancer Updated results from the Scandinavian Prostate Cancer Period Group-6 Study after a median follow-up period of 7.1 years. Scandinavian Journal of Urology and Nephrology, 40(6), 441–452. [DOI:10.1080/00365590601017329]
Iwamoto, S. J., Defreyne, J., Rothman, M. S., Van Schuylenbergh, J., Van de Bruaene, L., Motmans, J., & T’Sjoen, G. (2019). Health considerations for transgender women and remaining unknowns: a narrative review. Therapeutic Advances in Endocrinology and Metabolism, 10, 204201881987116. [DOI:10.1177/2042018819871166]
Iwamoto, S. J., Grimstad, F., Irwig, M. S., & Rothman, M. S. (2021). Routine Screening for Transgender and Gender Diverse Adults Taking Gender-Affirming Hormone Therapy: a Narrative Review. Journal of General Internal Medicine, 36(5), 1380–1389. [DOI:10.1007/s11606-021-06634-7]
Jacoby, A., Rifkin, W., Zhao, L. C., & Bluebond-Langner, R. (2020). Incidence of Cancer and Premalignant Lesions in Surgical Specimens of Transgender Patients. Plastic & Reconstructive Surgery, 147(1), 194–198. [DOI:10.1097/prs.0000000000007452]
Jain, J., Kwan, D., & Forcier, M. (2019). Medroxyprogesterone Acetate in Gender-Affirming Therapy for Transwomen: Results From a Retrospective Study. The Journal of Clinical Endocrinology & Metabolism, 104(11), 5148–5156. [DOI:10.1210/jc.2018-02253]
James, J. F., Jamerson, T. A., & Aguh, C. (2022). Efficacy and safety profile of oral spironolactone use for androgenic alopecia: A systematic review. Journal of the American Academy of Dermatology, 86(2), 425–429. [DOI:10.1016/j.jaad.2021.07.048]
Jia, A. Y., & Spratt, D. E. (2022). Bicalutamide Monotherapy With Radiation Therapy for Localized Prostate Cancer: A Non-Evidence-Based Alternative. International Journal of Radiation Oncology*Biology*Physics, 113(2), 316–319. [DOI:10.1016/j.ijrobp.2022.01.037]
Jiang, Y., & Tian, W. (2017). The effects of progesterones on blood lipids in hormone replacement therapy. Lipids in Health and Disease, 16(1), 219. [DOI:10.1186/s12944-017-0612-5]
Kanhai, R. C., Hage, J. J., van Diest, P. J., Bloemena, E., & Mulder, J. W. (2000). Short-Term and Long-Term Histologic Effects of Castration and Estrogen Treatment on Breast Tissue of 14 Male-to-Female Transsexuals in Comparison With Two Chemically Castrated Men. The American Journal of Surgical Pathology, 24(1), 74–80. [DOI:10.1097/00000478-200001000-00009]
Kellner, M., & Wiedemann, K. (2008). Mineralocorticoid receptors in brain, in health and disease: Possibilities for new pharmacotherapy. European Journal of Pharmacology, 583(2–3), 372–378. [DOI:10.1016/j.ejphar.2007.07.072]
Kim, G. K., & Del Rosso, J. Q. (2012). Oral Spironolactone in Post-teenage Female Patients with Acne Vulgaris: Practical Considerations for the Clinician Based on Current Data and Clinical Experience. The Journal of Clinical and Aesthetic Dermatology, 5(3), 37–50. [PubMed] [PubMed Central]
King, S. R. (2012). Neurosteroids and the Nervous System. In King, S. R. Neurosteroids and the Nervous System (pp. 1–122). New York: Springer New York. [DOI:10.1007/978-1-4614-5559-2_1]
Krishnamurthy, N., Slack, D., Kyweluk, M., Kirkley, J., Trakhtenberg, E., Contreras-Castro, F., & Safer, J. (2023). Not All Transfeminine Individuals on Estradiol Can Reach Both Target Testosterone and Target Estradiol Levels—Time to Revisit Treatment Guidelines? USPATH Scientific Symposium, November 1-5, 2023, The Westin Westminster, Westminster, Colorado, Abstract Submissions, 94–94 (abstract no. SAT-B2-T4). [Symposium Schedule] [PDF] [Full Abstract Book]
Kolvenbag, G. J., & Blackledge, G. R. (1996). Worldwide activity and safety of bicalutamide: a summary review. Urology, 47(1), 70–79. [DOI:10.1016/s0090-4295(96)80012-4]
Kuhl, H. (2003). Östrogene für den Mann? [Estrogen for men?] Blickpunkt der Mann, 1(3), 6–12. [Google Scholar] [URL] [PDF]
Kuhl, H. (2005). Pharmacology of estrogens and progestogens: influence of different routes of administration. Climacteric, 8(Suppl 1), 3–63. [DOI:10.1080/13697130500148875] [PDF]
Kuhl, H., & Wiegratz, I. (2017). Das Post-Finasterid-Syndrom. [Post Finasteride Syndrome.] Gynäkologische Endokrinologie, 15(2), 153–163. [DOI:10.1007/s10304-017-0126-2]
Kuijpers, S. M., Wiepjes, C. M., Conemans, E. B., Fisher, A. D., T’Sjoen, G., & den Heijer, M. (2021). Toward a Lowest Effective Dose of Cyproterone Acetate in Trans Women: Results From the ENIGI Study. The Journal of Clinical Endocrinology & Metabolism, 106(10), e3936–e3945. [DOI:10.1210/clinem/dgab427]
Kumar, P., Reddy, S., Kulkarni, A., Sharma, M., & Rao, P. N. (2021). Cyproterone Acetate–Induced Acute Liver Failure: A Case Report and Review of the Literature. Journal of Clinical and Experimental Hepatology, 11(6), 739–741. [DOI:10.1016/j.jceh.2021.01.003]
Lauritzen, C. (1988). Natürliche und synthetische Sexualhormone – Biologische Grundlagen und Behandlungsprinzipien. [Natural and Synthetic Sexual Hormones – Biological Basis and Medical Treatment Principles.] In Lauritzen, C., Schneider, H. P. G., & Nieschlag, E. (Eds.). Grundlagen und Klinik der Menschlichen Fortpflanzung [Foundations and Clinic of Human Reproduction] (pp. 229–306). Berlin: de Gruyter. [Google Scholar] [Google Books] [OpenLibrary] [WorldCat] [URL] [PDF] [Translation]
Lax, E. (1987). Mechanisms of physiological and pharmacological sex hormone action on the mammalian liver. Journal of Steroid Biochemistry, 27(4–6), 1119–1128. [DOI:10.1016/0022-4731(87)90198-1]
Layton, A. M., Eady, E. A., Whitehouse, H., Del Rosso, J. Q., Fedorowicz, Z., & van Zuuren, E. J. (2017). Oral Spironolactone for Acne Vulgaris in Adult Females: A Hybrid Systematic Review. American Journal of Clinical Dermatology, 18(2), 169–191. [DOI:10.1007/s40257-016-0245-x]
Legro, R. S., Schlaff, W. D., Diamond, M. P., Coutifaris, C., Casson, P. R., Brzyski, R. G., Christman, G. M., Trussell, J. C., Krawetz, S. A., Snyder, P. J., Ohl, D., Carson, S. A., Steinkampf, M. P., Carr, B. R., McGovern, P. G., Cataldo, N. A., Gosman, G. G., Nestler, J. E., Myers, E. R., Santoro, N., Eisenberg, E., Zhang, M., & Zhang, H. (2010). Total Testosterone Assays in Women with Polycystic Ovary Syndrome: Precision and Correlation with Hirsutism. The Journal of Clinical Endocrinology & Metabolism, 95(12), 5305–5313. [DOI:10.1210/jc.2010-1123]
Leinung, M. C., Feustel, P. J., & Joseph, J. (2018). Hormonal Treatment of Transgender Women with Oral Estradiol. Transgender Health, 3(1), 74–81. [DOI:10.1089/trgh.2017.0035]
Liang, J. J., Jolly, D., Chan, K. J., & Safer, J. D. (2018). Testosterone Levels Achieved by Medically Treated Transgender Women in a United States Endocrinology Clinic Cohort. Endocrine Practice, 24(2), 135–142. [DOI:10.4158/ep-2017-0116]
Lobo, R. A., Shoupe, D., Serafini, P., Brinton, D., & Horton, R. (1985). The effects of two doses of spironolactone on serum androgens and anagen hair in hirsute women. Fertility and Sterility, 43(2), 200–205. [DOI:10.1016/s0015-0282(16)48373-1]
Loh, H. H., Yee, A., Loh, H. S., Kanagasundram, S., Francis, B., & Lim, L. (2020). Sexual dysfunction in polycystic ovary syndrome: a systematic review and meta-analysis. Hormones, 19(3), 413–423. [DOI:10.1007/s42000-020-00210-0]
Luong, J. H., Male, K. B., & Glennon, J. D. (2019). Biotin interference in immunoassays based on biotin-strept(avidin) chemistry: An emerging threat. Biotechnology Advances, 37(5), 634–641. [DOI:10.1016/j.biotechadv.2019.03.007]
MacLean, D. B., Shi, H., Faessel, H. M., & Saad, F. (2015). Medical Castration Using the Investigational Oral GnRH Antagonist TAK-385 (Relugolix): Phase 1 Study in Healthy Males. The Journal of Clinical Endocrinology & Metabolism, 100(12), 4579–4587. [DOI:10.1210/jc.2015-2770]
Mahler, C. (1996). A Review of the Clinical Studies with Nilutamide. In Denis, L. (Ed.). Antiandrogens in Prostate Cancer: A Key to Tailored Endocrine Treatment (ESO Monographs) (pp. 105–111). Berlin/Heidelberg: Springer Berlin Heidelberg. [DOI:10.1007/978-3-642-45745-6_10]
Maksym, R. B., Kajdy, A., & Rabijewski, M. (2019). Post-finasteride syndrome – does it really exist? The Aging Male, 22(4), 250–259. [DOI:10.1080/13685538.2018.1548589]
Marks, D. H., Prasad, S., De Souza, B., Burns, L. J., & Senna, M. M. (2019). Topical Antiandrogen Therapies for Androgenetic Alopecia and Acne Vulgaris. American Journal of Clinical Dermatology, 21(2), 245–254. [DOI:10.1007/s40257-019-00493-z]
Martinez-Martin, F. J., Kuzior, A., Hernandez-Lazaro, A., de Leon-Durango, R. J., Rios-Gomez, C., Santana-Ojeda, B., Perez-Rivero, J. M., Fernandez-Trujillo-Comenge, P. M., Gonzalez-Diaz, P., Arnas-Leon, C., Acosta-Calero, C., Perdomo-Herrera, E., Tocino-Hernandez, A. L., del Sol Sanchez-Bacaicoa, M., & del Pino Perez-Garcia, M. (2022). Incidence of hypertension in young transgender people after a 5-year follow-up: association with gender-affirming hormonal therapy. Hypertension Research, 46(1), 219–225. [DOI:10.1038/s41440-022-01067-z]
Masumori, N., Baba, T., Abe, T., & Niwa, K. (2021). What is the most anticipated change induced by treatment using gender‐affirming hormones in individuals with gender incongruence?. International Journal of Urology, 28(5), 526–529. [DOI:10.1111/iju.14499]
McFarlane, T., Zajac, J. D., & Cheung, A. S. (2018). Gender-affirming hormone therapy and the risk of sex hormone-dependent tumours in transgender individuals—A systematic review. Clinical Endocrinology, 89(6), 700–711. [DOI:10.1111/cen.13835]
Meriggiola, M. C., Bremner, W. J., Costantino, A., Bertaccini, A., Morselli-Labate, A. M., Huebler, D., Kaufmann, G., Oettel, M., & Flamigni, C. (2002). Twenty-One Day Administration of Dienogest Reversibly Suppresses Gonadotropins and Testosterone in Normal Men. The Journal of Clinical Endocrinology & Metabolism, 87(5), 2107–2113. [DOI:10.1210/jcem.87.5.8514]
Meyer, G., Mayer, M., Mondorf, A., Flügel, A. K., Herrmann, E., & Bojunga, J. (2020). Safety and rapid efficacy of guideline-based gender-affirming hormone therapy: an analysis of 388 individuals diagnosed with gender dysphoria. European Journal of Endocrinology, 182(2), 149–156. [DOI:10.1530/eje-19-0463]
Miles, R. A., Paulson, R. J., Lobo, R. A., Press, M. F., Dahmoush, L., & Sauer, M. V. (1994). Pharmacokinetics and endometrial tissue levels of progesterone after administration by intramuscular and vaginal routes: a comparative study. Fertility and Sterility, 62(3), 485–490. [DOI:10.1016/s0015-0282(16)56935-0]
Millington, K., Liu, E., & Chan, Y. (2019). The Utility of Potassium Monitoring in Gender-Diverse Adolescents Taking Spironolactone. Journal of the Endocrine Society, 3(5), 1031–1038. [DOI:10.1210/js.2019-00030]
Millward, C. P., Keshwara, S. M., Islim, A. I., Jenkinson, M. D., Alalade, A. F., & Gilkes, C. E. (2022). Development and Growth of Intracranial Meningiomas in Transgender Women Taking Cyproterone Acetate as Gender-Affirming Progestogen Therapy: A Systematic Review. Transgender Health, 7(6), 473–483. [DOI:10.1089/trgh.2021.0025]
Moretti, C., Guccione, L., Di Giacinto, P., Simonelli, I., Exacoustos, C., Toscano, V., Motta, C., De Leo, V., Petraglia, F., & Lenzi, A. (2017). Combined Oral Contraception and Bicalutamide in Polycystic Ovary Syndrome and Severe Hirsutism: A Double-Blind Randomized Controlled Trial. The Journal of Clinical Endocrinology & Metabolism, 103(3), 824–838. [DOI:10.1210/jc.2017-01186]
Nakamoto, J. (2016). Endocrine Testing. In Jameson, J. L., & De Groot, L. J. (Eds.). Endocrinology: Adult and Pediatric, 7th Edition (pp. 2655–2688.e1). Philadelphia: Saunders/Elsevier. [DOI:10.1016/B978-0-323-18907-1.00154-2]
Nakhjavani, M., Hamidi, S., Esteghamati, A., Abbasi, M., Nosratian-Jahromi, S., & Pasalar, P. (2009). Short term effects of spironolactone on blood lipid profile: a 3-month study on a cohort of young women with hirsutism. British Journal of Clinical Pharmacology, 68(4), 634–637. [DOI:10.1111/j.1365-2125.2009.03483.x]
Neyman, A., Fuqua, J. S., & Eugster, E. A. (2019). Bicalutamide as an Androgen Blocker With Secondary Effect of Promoting Feminization in Male-to-Female Transgender Adolescents. Journal of Adolescent Health, 64(4), 544–546. [DOI:10.1016/j.jadohealth.2018.10.296]
Nguyen, D., Marchese, M., Cone, E. B., Paciotti, M., Basaria, S., Bhojani, N., & Trinh, Q. (2021). Investigation of Suicidality and Psychological Adverse Events in Patients Treated With Finasteride. JAMA Dermatology, 157(1), 35–42. [DOI:10.1001/jamadermatol.2020.3385]
Nie, I., Wiepjes, C. M., Blok, C. J., Moorselaar, R. J., Pigot, G. L., Sluis, T. M., Barbé, E., Voorn, P., Mello, N. M., Huirne, J., & Heijer, M. (2021). Incidence of testicular cancer in trans women using gender‐affirming hormonal treatment: a nationwide cohort study. BJU International, 129(4), 491–497. [DOI:10.1111/bju.15575]
Nieschlag, E., Zitzmann, M., & Kamischke, A. (2003). Use of progestins in male contraception. Steroids, 68(10–13), 965–972. [DOI:10.1016/s0039-128x(03)00135-1]
Nieschlag, E. (2010). Clinical trials in male hormonal contraception. Contraception, 82(5), 457–470. [DOI:10.1016/j.contraception.2010.03.020]
Nieschlag, E., & Behre, H. M. (2012). The essential role of testosterone in hormonal male contraception. In Nieschlag, E., Behre, H. M., & Nieschlag, S. (Eds.). Testosterone: Action · Deficiency · Substitution, 4th Edition (pp. 470–493). Cambridge/New York: Cambridge University Press. [DOI:10.1017/cbo9781139003353.023]
Nishiyama, T. (2014). Serum testosterone levels after medical or surgical androgen deprivation: A comprehensive review of the literature. Urologic Oncology: Seminars and Original Investigations, 32(1), 38.e17–38.e28. [DOI:10.1016/j.urolonc.2013.03.007]
Nolan, B. J., & Cheung, A. S. (2021). Relationship Between Serum Estradiol Concentrations and Clinical Outcomes in Transgender Individuals Undergoing Feminizing Hormone Therapy: A Narrative Review. Transgender Health, 6(3), 125–131. [DOI:10.1089/trgh.2020.0077]
Nolan, B. J., Frydman, A. S., Leemaqz, S. Y., Carroll, M., Grossmann, M., Zajac, J. D., & Cheung, A. S. (2022). Effects of low-dose oral micronised progesterone on sleep, psychological distress, and breast development in transgender individuals undergoing feminising hormone therapy: a prospective controlled study. Endocrine Connections, 11(5), e220170. [DOI:10.1530/EC-22-0170]
Norman, A. W., & Henry, H. L. (2015). Androgens. In Norman, A. W., & Henry, H. L. Hormones, 3rd Edition (pp. 255–273). London: Academic Press/Elsevier. [DOI:10.1016/b978-0-08-091906-5.00012-4]
Norman, A. W., & Henry, H. L. (2015). Estrogens and Progestins. In Norman, A. W., & Henry, H. L. Hormones, 3rd Edition (pp. 275–296). London: Academic Press/Elsevier. [DOI:10.1016/b978-0-08-091906-5.00013-6]
Nota, N. M., Wiepjes, C. M., de Blok, C. J., Gooren, L. J., Peerdeman, S. M., Kreukels, B. P., & den Heijer, M. (2018). The occurrence of benign brain tumours in transgender individuals during cross-sex hormone treatment. Brain, 141(7), 2047–2054. [DOI:10.1093/brain/awy108]
North American Menopause Society. (2022). The 2022 hormone therapy position statement of The North American Menopause Society. Menopause, 29(7), 767–794. [DOI:10.1097/gme.0000000000002028]
O’Connell, M. B. (1995). Pharmacokinetic and Pharmacologic Variation Between Different Estrogen Products. The Journal of Clinical Pharmacology, 35(9S), 18S–24S. [DOI:10.1002/j.1552-4604.1995.tb04143.x]
Olsen, E. A., Hordinsky, M., Whiting, D., Stough, D., Hobbs, S., Ellis, M. L., Wilson, T., & Rittmaster, R. S. (2006). The importance of dual 5α-reductase inhibition in the treatment of male pattern hair loss: Results of a randomized placebo-controlled study of dutasteride versus finasteride. Journal of the American Academy of Dermatology, 55(6), 1014–1023. [DOI:10.1016/j.jaad.2006.05.007]
Plovanich, M., Weng, Q. Y., & Mostaghimi, A. (2015). Low Usefulness of Potassium Monitoring Among Healthy Young Women Taking Spironolactone for Acne. JAMA Dermatology, 151(9), 941–944. [DOI:10.1001/jamadermatol.2015.34]
Polyzos, S. A., Kountouras, J., Zavos, C., & Deretzi, G. (2011). Spironolactone Revisited. The Journal of Clinical Hypertension, 13(10), 783–784. [DOI:10.1111/j.1751-7176.2011.00484.x]
Powers, M. S., Schenkel, L., Darley, P. E., Good, W. R., Balestra, J. C., & Place, V. A. (1985). Pharmacokinetics and pharmacodynamics of transdermal dosage forms of 17β-estradiol: Comparison with conventional oral estrogens used for hormone replacement. American Journal of Obstetrics and Gynecology, 152(8), 1099–1106. [DOI:10.1016/0002-9378(85)90569-1]
Prince, J. C., & Safer, J. D. (2020). Endocrine treatment of transgender individuals: current guidelines and strategies. Expert Review of Endocrinology & Metabolism, 15(6), 395–403. [DOI:10.1080/17446651.2020.1825075]
Reiter, E. O., Mauras, N., McCormick, K., Kulshreshtha, B., Amrhein, J., De Luca, F., O’Brien, S., Armstrong, J., & Melezinkova, H. (2010). Bicalutamide plus Anastrozole for the Treatment of Gonadotropin-Independent Precocious Puberty in Boys with Testotoxicosis: A Phase II, Open-Label Pilot Study (BATT). Journal of Pediatric Endocrinology and Metabolism, 23(10), 999–1009. [DOI:10.1515/jpem.2010.161]
Rezende, H. D., Dias, M. F. R. G., & Trüeb, R. M. (2018). A Comment on the Post-Finasteride Syndrome. International Journal of Trichology, 10(6), 255–261. [PubMed] [PubMed Central] [DOI:10.4103/ijt.ijt_61_18]
Roberts, J. L., Fiedler, V., Imperato-McGinley, J., Whiting, D., Olsen, E., Shupack, J., Stough, D., DeVillez, R., Rietschel, R., Savin, R., Bergfeld, W., Swinehart, J., Funicella, T., Hordinsky, M., Lowe, N., Katz, I., Lucky, A., Drake, L., Price, V. H., Weiss, D., Whitmore, E., Millikan, L., Muller, S., Gencheff, C., Carrington, P., Binkowitz, B., Kotey, P., He, W., Bruno, K., Jacobsen, C., Terranella, L., Gormley, G. J., & Kaufman, K. D. (1999). Clinical dose ranging studies with finasteride, a type 2 5α-reductase inhibitor, in men with male pattern hair loss. Journal of the American Academy of Dermatology, 41(4), 555–563. [DOI:10.1016/s0190-9622(99)80052-8]
Roscioni, S. S., de Zeeuw, D., Bakker, S. J., & Lambers Heerspink, H. J. (2012). Management of hyperkalaemia consequent to mineralocorticoid-receptor antagonist therapy. Nature Reviews Nephrology, 8(12), 691–699. [DOI:10.1038/nrneph.2012.217]
Rose, A. J., Hughto, J. M., Dunbar, M. S., Quinn, E. K., Deutsch, M., Feldman, J., Radix, A., Safer, J. D., Shipherd, J. C., Thompson, J., & Jasuja, G. K. (2023). Trends in Feminizing Hormone Therapy for Transgender Patients, 2006–2017. Transgender Health, 8(2), 188–194. [DOI:10.1089/trgh.2021.0041]
Rosenfield, R. L., Cooke, D. W., & Radovick, S. (2008). Puberty and its disorders in the female. In Sperling, M. A. (Ed.). Pediatric Endocrinology, 3rd Edition (pp. 530–609). Philadelphia: Saunders. [Google Scholar] [Google Books] [OpenLibrary] [WorldCat]
Rosenfield, R. L., Cooke, D. W., & Radovick, S. (2021). Puberty in the Female and Its Disorders. In Sperling, M. A., Majzoub, J. A., Menon, R. K., & Stratakis, C. A. (Eds.). Sperling Pediatric Endocrinology, 5th Edition (pp. 528–626). Philadelphia: Elsevier. [DOI:10.1016/B978-0-323-62520-3.00016-6]
Samarasinghe, S., Meah, F., Singh, V., Basit, A., Emanuele, N., Emanuele, M. A., Mazhari, A., & Holmes, E. W. (2017). Biotin Interference with Routine Clinical Immunoassays: Understand the Causes and Mitigate the Risks. Endocrine Practice, 23(8), 989–998. [DOI:10.4158/ep171761.ra]
Schiller, C. E., Schmidt, P. J., & Rubinow, D. R. (2014). Allopregnanolone as a mediator of affective switching in reproductive mood disorders. Psychopharmacology, 231(17), 3557–3567. [DOI:10.1007/s00213-014-3599-x]
Schlatterer, K., Yassouridis, A., Werder, K. V., Poland, D., Kemper, J., & Stalla, G. K. (1998). Archives of Sexual Behavior, 27(5), 475–492. [DOI:10.1023/a:1018704630036]
Seaman, H. E., Langley, S. E., Farmer, R. D., & de Vries, C. S. (2007). Venous thromboembolism and cyproterone acetate in men with prostate cancer: a study using the General Practice Research Database. BJU International, 99(6), 1398–1403. [DOI:10.1111/j.1464-410x.2007.06859.x]
Shackleton, C. (2010). Clinical steroid mass spectrometry: A 45-year history culminating in HPLC–MS/MS becoming an essential tool for patient diagnosis. The Journal of Steroid Biochemistry and Molecular Biology, 121(3–5), 481–490. [DOI:10.1016/j.jsbmb.2010.02.017]
Shaw, J. C. (1996). Antiandrogen and hormonal treatment of acne. Dermatologic Clinics, 14(4), 803–811. [DOI:10.1016/s0733-8635(05)70405-8]
Slack, D., Krishnamurthy, N., Contreras-Castro, F., & Safer, J. D. (2023). Achieving Both Target Testosterone And Target Estradiol Levels May Not Be Practical In All Trans Feminine Users Of Estradiol - Which To Prioritize? Journal of the Endocrine Society, 7(Suppl 1), A1102–A1102 (abstract no. SAT404/bvad114.2075). [DOI:10.1210/jendso/bvad114.2075] [PubMed Central]
Sofer, Y., Yaish, I., Yaron, M., Bach, M. Y., Stern, N., & Greenman, Y. (2020). Differential Endocrine and Metabolic Effects of Testosterone Suppressive Agents in Transgender Women. Endocrine Practice, 26(8), 883–890. [DOI:10.4158/ep-2020-0032]
SoRelle, J. A., Jiao, R., Gao, E., Veazey, J., Frame, I., Quinn, A. M., Day, P., Pagels, P., Gimpel, N., & Patel, K. (2019). Impact of Hormone Therapy on Laboratory Values in Transgender Patients. Clinical Chemistry, 65(1), 170–179. [DOI:10.1373/clinchem.2018.292730]
St-Jules, D. E., Goldfarb, D. S., & Sevick, M. A. (2016). Nutrient Non-equivalence: Does Restricting High-Potassium Plant Foods Help to Prevent Hyperkalemia in Hemodialysis Patients? Journal of Renal Nutrition, 26(5), 282–287. [DOI:10.1053/j.jrn.2016.02.005]
St-Jules, D. E., & Fouque, D. (2020). Is it time to abandon the nutrient-based renal diet model? Nephrology Dialysis Transplantation, 36(4), 574–577. [DOI:10.1093/ndt/gfaa257]
St-Jules, D. E., & Fouque, D. (2022). Etiology-based dietary approach for managing hyperkalemia in people with chronic kidney disease. Nutrition Reviews, 80(11), 2198–2205. [DOI:10.1093/nutrit/nuac026]
Stanczyk, F. Z., & Clarke, N. J. (2010). Advantages and challenges of mass spectrometry assays for steroid hormones. The Journal of Steroid Biochemistry and Molecular Biology, 121(3–5), 491–495. [DOI:10.1016/j.jsbmb.2010.05.001]
Stanczyk, F. Z., Hapgood, J. P., Winer, S., & Mishell, D. R. (2012). Progestogens Used in Postmenopausal Hormone Therapy: Differences in Their Pharmacological Properties, Intracellular Actions, and Clinical Effects. Endocrine Reviews, 34(2), 171–208. [DOI:10.1210/er.2012-1008]
Stanczyk, F. Z., Mathews, B. W., & Cortessis, V. K. (2017). Does the type of progestin influence the production of clotting factors? Contraception, 95(2), 113–116. [DOI:10.1016/j.contraception.2016.07.007]
Stege, R., Gunnarsson, P. O., Johansson, C., Olsson, P., Pousette, Å., & Carlström, K. (1996). Pharmacokinetics and testosterone suppression of a single dose of polyestradiol phosphate (Estradurin®) in prostatic cancer patients. The Prostate, 28(5), 307–310. [DOI:10.1002/(sici)1097-0045(199605)28:5<307::aid-pros6>3.0.co;2-8]
Steinberger, E., Ayala, C., Hsi, B., Smith, K. D., Rodriguez-Rigau, L. J., Weidman, E. R., & Reimondo, G. G. (1998). Utilization of Commercial Laboratory Results in Management of Hyperandrogenism in Women. Endocrine Practice, 4(1), 1–10. [DOI:10.4158/ep.4.1.1]
Sterling, J., & Garcia, M. M. (2020). Cancer screening in the transgender population: a review of current guidelines, best practices, and a proposed care model. Translational Andrology and Urology, 9(6), 2771–2785. [DOI:10.21037/tau-20-954]
Strauss, J. F., & FitzGerald, G. A. (2019). Steroid Hormones and Other Lipid Molecules Involved in Human Reproduction. In Strauss, J. F., & Barbieri, R. L. (Eds.). Yen and Jaffe’s Reproductive Endocrinology: Physiology, Pathophysiology, and Clinical Management, 8th Edition (pp. 75–114.e7). Philadelphia: Elsevier. [Google Books] [DOI:10.1016/b978-0-323-47912-7.00004-4]
Stricker, R., Eberhart, R., Chevailler, M., Quinn, F. A., Bischof, P., & Stricker, R. (2006). Establishment of detailed reference values for luteinizing hormone, follicle stimulating hormone, estradiol, and progesterone during different phases of the menstrual cycle on the Abbott ARCHITECT® analyzer. Clinical Chemistry and Laboratory Medicine (CCLM), 44(7), 883–887. [DOI:10.1515/cclm.2006.160]
Styne, D. M. (2016). Laboratory Values for Pediatric Endocrinology. In Styne, D. M. Pediatric Endocrinology: A Clinical Handbook (pp. 385–434). Cham: Springer International Publishing. [DOI:10.1007/978-3-319-18371-8_16]
Sudduth, S. L., & Koronkowski, M. J. (1993). Finasteride: The First 5α-Reductase Inhibitor. Pharmacotherapy: The Journal of Human Pharmacology and Drug Therapy, 13(4), 309–329. [DOI:10.1002/j.1875-9114.1993.tb02739.x]
Sundström-Poromaa, I., Comasco, E., Sumner, R., & Luders, E. (2020). Progesterone – Friend or foe? Frontiers in Neuroendocrinology, 59, 100856. [DOI:10.1016/j.yfrne.2020.100856]
Swerdloff, R. S., Dudley, R. E., Page, S. T., Wang, C., & Salameh, W. A. (2017). Dihydrotestosterone: Biochemistry, Physiology, and Clinical Implications of Elevated Blood Levels. Endocrine Reviews, 38(3), 220–254. [DOI:10.1210/er.2016-1067]
T’Sjoen, G. G., Beguin, Y., Feyen, E., Rubens, R., Kaufman, J., & Gooren, L. (2005). Influence of exogenous oestrogen or (anti-) androgen administration on soluble transferrin receptor in human plasma. Journal of Endocrinology, 186(1), 61–67. [DOI:10.1677/joe.1.06112]
T’Sjoen, G., Arcelus, J., Gooren, L., Klink, D. T., & Tangpricha, V. (2018). Endocrinology of Transgender Medicine. Endocrine Reviews, 40(1), 97–117. [DOI:10.1210/er.2018-00011]
Tack, L. J., Heyse, R., Craen, M., Dhondt, K., Bossche, H. V., Laridaen, J., & Cools, M. (2017). Consecutive Cyproterone Acetate and Estradiol Treatment in Late-Pubertal Transgender Female Adolescents. The Journal of Sexual Medicine, 14(5), 747–757. [DOI:10.1016/j.jsxm.2017.03.251]
Thompson, J., Hopwood, R. A., deNormand, S., & Cavanaugh, T. (2021). Medical Care of Trans and Gender Diverse Adults. Boston: Fenway Health. [URL] [PDF]
Toorians, A. W., Thomassen, M. C., Zweegman, S., Magdeleyns, E. J., Tans, G., Gooren, L. J., & Rosing, J. (2003). Venous Thrombosis and Changes of Hemostatic Variables during Cross-Sex Hormone Treatment in Transsexual People. The Journal of Clinical Endocrinology & Metabolism, 88(12), 5723–5729. [DOI:10.1210/jc.2003-030520]
Traish, A. M., Krakowsky, Y., Doros, G., & Morgentaler, A. (2019). Do 5α-Reductase Inhibitors Raise Circulating Serum Testosterone Levels? A Comprehensive Review and Meta-Analysis to Explaining Paradoxical Results. Sexual Medicine Reviews, 7(1), 95–114. [DOI:10.1016/j.sxmr.2018.06.002]
Traish, A. M. (2020). Post-finasteride syndrome: a surmountable challenge for clinicians. Fertility and Sterility, 113(1), 21–50. [DOI:10.1016/j.fertnstert.2019.11.030]
Treleaven, M. M., Jackowich, R. A., Roberts, L., Wassersug, R. J., & Johnson, T. (2013). Castration and personality: Correlation of androgen deprivation and estrogen supplementation with the Big Five factor personality traits of adult males. Journal of Research in Personality, 47(4), 376–379. [DOI:10.1016/j.jrp.2013.03.005]
Usach, I., Martinez, R., Festini, T., & Peris, J. (2019). Subcutaneous Injection of Drugs: Literature Review of Factors Influencing Pain Sensation at the Injection Site. Advances in Therapy, 36(11), 2986–2996. [DOI:10.1007/s12325-019-01101-6]
van Zuuren, E. J., Fedorowicz, Z., Carter, B., & Pandis, N. (2015). Interventions for hirsutism (excluding laser and photoepilation therapy alone). Cochrane Database of Systematic Reviews, 2015, CD010334. [DOI:10.1002/14651858.cd010334.pub2]
Verdonk, S. J., Vesper, H. W., Martens, F., Sluss, P. M., Hillebrand, J. J., & Heijboer, A. C. (2019). Estradiol reference intervals in women during the menstrual cycle, postmenopausal women and men using an LC-MS/MS method. Clinica Chimica Acta, 495, 198–204. [DOI:10.1016/j.cca.2019.04.062]
Vermeulen, A., Giagulli, V., De Schepper, P., & Buntinx, A. (1991). Hormonal Effects of a 5α-Reductase Inhibitor (Finasteride) onHormonal Levels in Normal Men and in Patients withBenign Prostatic Hyperplasia. European Urology, 20(1), 82–86. [DOI:10.1159/000471752]
Vihtamäki, T., Luukkaala, T., & Tuimala, R. (2004). Skin contamination by oestradiol gel—a remarkable source of error in plasma oestradiol measurements during percutaneous hormone replacement therapy. Maturitas, 48(4), 347–353. [DOI:10.1016/s0378-5122(03)00043-4]
Wang, H., Liu, M., Fu, Q., & Deng, C. (2019). Pharmacokinetics of hard micronized progesterone capsules via vaginal or oral route compared with soft micronized capsules in healthy postmenopausal women: a randomized open-label clinical study. Drug Design, Development and Therapy, 13, 2475–2482. [DOI:10.2147/dddt.s204624]
Wang, Y., & Lipner, S. R. (2020). Retrospective analysis of adverse events with spironolactone in females reported to the United States Food and Drug Administration. International Journal of Women’s Dermatology, 6(4), 272–276. [DOI:10.1016/j.ijwd.2020.05.002]
Weill, A., Nguyen, P., Labidi, M., Cadier, B., Passeri, T., Duranteau, L., Bernat, A., Yoldjian, I., Fontanel, S., Froelich, S., & Coste, J. (2021). Use of High Dose Cyproterone Acetate and Risk of Intracranial Meningioma in Women: Cohort Study. BMJ, 372, n37. [DOI:10.1136/bmj.n37]
Welk, B., McArthur, E., Ordon, M., Anderson, K. K., Hayward, J., & Dixon, S. (2017). Association of Suicidality and Depression With 5α-Reductase Inhibitors. JAMA Internal Medicine, 177(5), 683–691. [DOI:10.1001/jamainternmed.2017.0089]
Wellington, K., & Keam, S. J. (2006). Bicalutamide 150mg: A Review of its Use in the Treatment of Locally Advanced Prostate Cancer. Drugs, 66(6), 837–850. [DOI:10.2165/00003495-200666060-00007]
Willemsen, W. N., Mastboom, J. L., Thomas, C. M., & Rolland, R. (1985). Absorption of 17β-estradiol in a neovagina constructed from the peritoneum. European Journal of Obstetrics & Gynecology and Reproductive Biology, 19(4), 247–253. [DOI:10.1016/0028-2243(85)90036-x]
Wilson, L. M., Baker, K. E., Sharma, R., Dukhanin, V., McArthur, K., & Robinson, K. A. (2020). Effects of antiandrogens on prolactin levels among transgender women on estrogen therapy: A systematic review. International Journal of Transgender Health, 21(4), 391–402. [DOI:10.1080/15532739.2020.1819505]
Wu, B., Shen, P., Yin, X., Yu, L., Wu, F., Chen, C., Li, J., & Xu, T. (2022). Analysis of adverse event of interstitial lung disease in men with prostate cancer receiving hormone therapy using the Food and Drug Administration Adverse Event Reporting System. British Journal of Clinical Pharmacology, 89(2), 440–448. [DOI:10.1111/bcp.15336]
Wu, F. C., Balasubramanian, R., Mulders, T. M., & Coelingh-Bennink, H. J. (1999). Oral Progestogen Combined with Testosterone as a Potential Male Contraceptive: Additive Effects between Desogestrel and Testosterone Enanthate in Suppression of Spermatogenesis, Pituitary-Testicular Axis, and Lipid Metabolism. The Journal of Clinical Endocrinology & Metabolism, 84(1), 112–122. [DOI:10.1210/jcem.84.1.5412]
Yaish, I., Gindis, G., Greenman, Y., Moshe, Y., Arbiv, M., Buch, A., Sofer, Y., Shefer, G., & Tordjman, K. (2023). Sublingual Estradiol Offers No Apparent Advantage Over Combined Oral Estradiol and Cyproterone Acetate for Gender-Affirming Hormone Therapy of Treatment-Naive Trans Women: Results of a Prospective Pilot Study. Transgender Health, 8(6), 485–493. [DOI:10.1089/trgh.2023.0022]
Zaenglein, A. L., Pathy, A. L., Schlosser, B. J., Alikhan, A., Baldwin, H. E., Berson, D. S., Bowe, W. P., Graber, E. M., Harper, J. C., Kang, S., Keri, J. E., Leyden, J. J., Reynolds, R. V., Silverberg, N. B., Stein Gold, L. F., Tollefson, M. M., Weiss, J. S., Dolan, N. C., Sagan, A. A., Stern, M., Boyer, K. M., & Bhushan, R. (2016). Guidelines of care for the management of acne vulgaris. Journal of the American Academy of Dermatology, 74(5), 945–973.e33. [DOI:10.1016/j.jaad.2015.12.037]
Zhang, J., & Stanczyk, F. Z. (2013). LC-MS Bioanalysis of Steroids. In Li, W., Zhang, J., & Tse, F. L. S. (Eds.). Handbook of LC-MS Bioanalysis: Best Practices, Experimental Protocols, and Regulations (pp. 573–590). Hoboken, New Jersey: John Wiley & Sons. [DOI:10.1002/9781118671276.ch45]
Zhou, Z., Song, S., Gao, Z., Wu, J., Ma, J., & Cui, Y. (2019). The efficacy and safety of dutasteride compared with finasteride in treating men with androgenetic alopecia: a systematic review and meta-analysis. Clinical Interventions in Aging, 14, 399–406. [DOI:10.2147/cia.s192435]
Zitzmann, M., Rohayem, J., Raidt, J., Kliesch, S., Kumar, N., Sitruk-Ware, R., & Nieschlag, E. (2017). Impact of various progestins with or without transdermal testosterone on gonadotropin levels for non-invasive hormonal male contraception: a randomized clinical trial. Andrology, 5(3), 516–526. [DOI:10.1111/andr.12328]
Zuuren, E., & Fedorowicz, Z. (2016). Interventions for hirsutism excluding laser and photoepilation therapy alone: abridged Cochrane systematic review including GRADE assessments. British Journal of Dermatology, 175(1), 45–61. [DOI:10.1111/bjd.14486]
\ No newline at end of file
diff --git a/transfemscience.org/articles/transfem-lactation-literature/index.html b/transfemscience.org/articles/transfem-lactation-literature/index.html
index 6b08f627..9767de07 100644
--- a/transfemscience.org/articles/transfem-lactation-literature/index.html
+++ b/transfemscience.org/articles/transfem-lactation-literature/index.html
@@ -1 +1 @@
-Published Case Reports of Lactation and/or Breastfeeding in Transfeminine People - Transfeminine Science
Published Case Reports of Lactation and/or Breastfeeding in Transfeminine People
By Aly | First published March 26, 2019 | Last modified March 29, 2024
Abstract / TL;DR
A number of case reports of hormonally induced lactation and breastfeeding in transfeminine people have been published. The earliest report of lactation in a transfeminine person was in the 1950s and the earliest report of breastfeeding was in the 1980s. Starting in 2019, more case reports have been published in the modern scientific literature. Unpublished cases also exist (e.g., that of Dr. Christine McGinn), and lactation has been induced or occurred in cisgender men as well. Lactation may be induced in transfeminine people with the use estrogens, progestogens, and/or prolactin releasers. Reviews discussing lactation induction in transfeminine people have recently been published.
Introduction
Last year, a case report of lactation and breastfeeding in a transgender woman was published:
Reisman, T., & Goldstein, Z. (2018). Case report: Induced lactation in a transgender woman. Transgender Health, 3(1), 24–26. [DOI:10.1089/trgh.2017.0044]
In the paper, the authors state the following:
We believe that this is the first formal report in the medical literature of induced lactation in a transgender woman.
However, this actually wasn’t the first case report of lactation and/or breastfeeding in a transfeminine person in the literature. There are various previous published cases dating back as far as the 1950s. These instances are provided below in the format of sources and excerpts.
Published Case Reports
Foss (1956)
Foss, G. L. (1956). Abnormalities of form and function of the human breast. Journal of Endocrinology, 14(4 Suppl) [Proceedings of the Society for Endocrinology: Fifty-Fourth Meeting. Symposium on Selected Aspects of the Practice of Hormone Administration in Animals and Man], vi–vii. [Google Scholar] [Google Books] [URL] [PDF]:
Based on the theories of lactogenesis and stimulated by the success of Lyons, Li, Johnson & Cole [1955], who succeeded in producing lactation in male rats, an attempt was made to initiate lactogenesis in a male transvestist. Six years ago this patient had been given oestrogens. Both testes and penis were then removed and an artificial vagina was constructed by plastic surgery. The patient was implanted with 500 mg oestradiol in September 1954, and 600 mg in July 1955. The breasts were then developed more intensively with daily injections of oestradiol dipropionate and progesterone for 6 weeks. Immediately following withdrawal of this treatment, prolactin 22·9 mg was injected daily for 3 days without effect. After a second month on oestradiol and progesterone daily, combined injections of prolactin and somatotrophin were given for 4 days and suction was applied by a breast pump—four times daily. On the 4th and 5th days a few drops of colostrum were expressed from the right nipple.
Tindal & McNaught (1958)
Tindal, J. S., & McNaught, M. L. (1958). Hormonal Factors in Breast Development and Milk Secretion. In Gardiner-Hill, H. (Ed.). Modern Trends in Endocrinology, Volume 1 (pp. 188–211) (Modern Trends). London: Butterworth. [Google Scholar] [Google Books] [OpenLibrary] [WorldCat] [Archive.org]:
Recently, an attempt has been made by Foss (1956) to initiate lactation in a castrated male transvestist. He was given an implant of 500 milligrams of oestradiol, and 10 months later, a further 600 milligrams of oestradiol, followed by daily injections of oestradiol dipropionate and progesterone for 6 weeks. Immediately after withdrawal of this treatment, 22·9 milligrams of prolactin were injected daily for 3 days but without effect. After a second month of treatment with oestradiol and progesterone daily, he was given combined injections of prolactin and somatotrophin for 4 days, suction with a breast-pump being employed 4 times daily. On the fourth and fifth days a few drops of colostrum were expressed from the right nipple. There is a possible application here of modern hormone knowledge to man, and further trials would be of interest.
Experimentally I have been able to induce lactogenesis in a male transvestite whose testes had been removed some years before and whose breasts had been well developed over a long period with stilbestrol and ethisterone.9 In July, 1955, 600 mg. of estradiol was implanted subcutaneously and weekly injections of 50 mg. of progesterone were given for four months. For the next month daily injections of 10 mg. estradiol dipropionate and 50 mg. progesterone were given. These injections were continued for another month, increasing progesterone to 100 mg. daily. Both hormones were then withdrawn, and daily injections of increasing doses of prolactin and somatotropin were given for four days; at the same time, the patient used a breast pump four times daily for 5 minutes on both sides. During this time the mammary veins were visibly enlarged and on the sixth and seventh days 1 to 2 cc. of milky fluid was collected.
Flückiger, Del Pozo, & von Werder (1982)
Flückiger, E., Del Pozo, E., & von Werder, K. (1982). Prolactin: Synthesis, Fate and Actions. In Flückiger, E. W., Del Pozo, E., & von Werder, K. (Eds.). Prolactin: Physiology, Pharmacology, and Clinical Findings (Monographs on Endocrinology, Volume 23) (pp. 1–23). Berlin/Heidelberg: Springer-Verlag. [Google Scholar] [Google Books] [DOI:10.1007/978-3-642-81721-2_1]:
An observation (Wyss and Del Pozo unpublished) in a male transsexual showed that induction of lactation can be similarly achieved in the human male.
Flückiger, E., Del Pozo, E., & von Werder, K. (1982). Nontumoral hyperprolactinemia. In Flückiger, E. W., Del Pozo, E., & von Werder, K. (Eds.). Prolactin: Physiology, Pharmacology, and Clinical Findings (Monographs on Endocrinology, Volume 23) (pp. 102–152). Berlin/Heidelberg: Springer-Verlag. [Google Scholar] [Google Books] [DOI:10.1007/978-3-642-81721-2_4]:
4.3.2 Effect of Hyperprolactinemia in Male Subjects
Although PRL circulates in male blood in appreciable concentrations its physiologic role has not been clarified. The lack of lactational requirements does not preclude that under adequate priming the male mammary gland will respond to a PRL challenge with milk production. Thus, Wyss and del Pozo (unpublished data) found that PRL stimulation with TRH was able to induce milk secretion in a male individual pretreated with estrogens. Certainly, the chronic ingestion of dopamine antagonists or estrogens may lead to sustained hyperprolactinemia, and the same effect can be expected in male subjects on chronic estrogen therapy of prostatic cancer or transsexualism (Frantz 1973; del Pozo, to be published).
Certainly, the prolonged intake of estrogens, in male subjects also, as observed in the treatment of prostatic carcinoma and in transsexuals, can lead to hyperprolactinemia (Frantz 1972b; del Pozo, to be published).
Kozlov, Mel’nichenko, & Golubeva (1985)
Kozlov, G. I., Mel’nichenko, G. A., & Golubeva, I. V. (1985). Случай лактореи у больного мужского пола с транссексуализмом. [Sluchai laktorei u bol’nogo muzhskogo pola s transseksualizmom. / Case of galactorrhea in a transsexual male patient.] Проблемы Эндокринологии [Problemy Èndokrinologii (Moskva) / Problems of Endocrinology (Moscow)], 31(1), 37–38. [ISSN:0375-9660] [Google Scholar 1] [Google Scholar 2] [PubMed] [DOI:10.14341/probl198531137-38] [PDF] [Translation] [Translated]:
The appearance of galactorrhea in men is most often a symptom of pituitary prolactinoma. Combined with gynecomastia and atrophy of the testicles, galactorrhea caused by adenomas of the pituitary gland in men is known as O’Connell syndrome (1).
In recent years, however, cases of galactorrhea have been described in men without radiological or clinical signs of pituitary adenoma (12). Of course, in these cases, the presence of undetected microadenomas of the pituitary gland cannot be excluded, especially since the level of prolactin in these patients is significantly increased (1, 2).
Some medications, especially antipsychotics and estrogen-containing oral contraceptives (7, 10), increase serum levels of prolactin and can lead to the development of galactorrhea.
There is information about the influence of psycho-emotional factors on the lactation process: the possibility of the development (induction) of psychogenic lactation during false pregnancy (3) is known, and, conversely, the possibility of the termination of lactation in nursing mothers after mental stress.
Accumulated clinical observations on the frequent development of depressive states in persistent galactorrhea–amenorrhea syndrome (4), cases of galactorrhea in the mentally ill, even in the absence of neuroleptics (7), as well as experimental observations on the effect of hyperprolactinemia on the behavioral responses of animals (5), require careful study of the relationship of hyperprolactinemia and psycho-emotional factors. In connection with this, we present the following observation.
The patient (P), was born a normal, full-term boy. He remembers well from 6 years. Early development was unremarkable, he did not differ from peers, but loved to play more with girls. He played with dolls and cars. At 10 years of age, there was a desire to wear women’s clothes. From the age of 12 he swam with girls in a shirt and shorts, as he was embarrassed by the lack of breasts. From the age of 14 he changed clothes in his mother’s dress, and only in such clothes “felt like a person”. From the same age in a woman’s dress he went to get acquainted with young men and got pleasure from it. At the age of 15, he came to the firm conviction that he was a girl, began to urinate like a girl, squatting, use lipstick, and put on powdered makeup. He suffered greatly from the presence of “deformities” – male genital organs. At the age of 17, while working as a “nurse” in a hospital, he began to self-inject himself with folliculin (estrogen) and progesterone, which caused the development of the breasts. With pleasure, he did women’s housework, and loved to tinker with children. Having received a passport, he redid it as female, thus resulting in a female civilian gender.
Twice he tried to commit suicide (he took sleeping pills), since he could not bear the duality of his existence. Twice he was treated in psychiatric hospitals about transsexualism, unsuccessfully.
During the examination in IEE and HCG at the age of 20 years, no abnormalities in somatic status were revealed: complex as a man, male genitals, shaved from 17 years of age daily. Erotic dreams were frequent, wherein he played the role of a woman, and denied emissions. The ejaculate was studied (obtained by vibratory massage): volume – 1.4 mL, pH 8.8 (norm 7.6–8.2), sperm count 31 million per 1 mL, mobility 57%, and morphologically normal 69%. Sex chromatin is negative.
At age 22, a course of treatment with cyproterone acetate was conducted at the Institute of Psychiatry of the Ministry of Health of the USSR. Muscle weakness, reduction of sexual hairiness, and appearance of colostrum excretion was noted.
When examined in IEE and HCG at 23 years, the breasts corresponded to the age of 15–16 years (on his own initiative he periodically took estrogens), and colostrum was secreted from the nipples (abundant drops when pressed – galactorrhea (++)). He insisted on castration and amputation of the penis, since, being a “woman”, he was ashamed of not having the appropriate genitals for his sex, which he called “deformities”.
On X-ray of the skull, the shape and size of the sella turcica were normal, but signs of increased intracranial pressure were revealed. On EEG against the background of the general phenomena of irritation, the focus of pathology was recorded in the left parietal lead. Indicators of the functional state of the thyroid gland were in the normal range. In the study of the radioimmunoassay method using standard kits from the Sorin company, some increase in prolactin level of 24 ng/mL was detected in the serum (normal for men is 4–15 ng/mL).
In connection with the repeated suicidal attempts, failure of psychiatric treatment, and in consideration of the fact that the patient has a female civilian sex and performs a female social role, castration and feminizing plastic surgery of the external genitalia were performed for the purpose of social rehabilitation.
Some time after the operation, the patient developed a renewed interest in life. After the surgical and hormonal correction, the patient irresistibly developed maternal instincts. Unmarried, the patient obtained permission for the adoption of a child, simulated pregnancy, and was discharged from the maternity hospital with a son. From the first days after the “birth”, galactorrhea sharply increased, and spontaneous outflow of milk appeared, with galactorrhea (+++). The baby was breastfed up to 6 months of age.
Thus, it can be thought that several factors played a role in the genesis of galactorrhea in this patient:
Increased prolactin levels with estrogen and cyproterone acetate. The hyperprolactic properties of estrogens have long been known; the ability of cyproterone acetate to increase serum prolactin levels was shown by K. Schmidt–Golewizer et al (9).
Increased intracranial pressure, the role of this factor and the genesis of neuroendocrine disorders and, in particular, in the development of galactorrhea was shown by R. Peterson (8).
Our message is the second in the world literature describing galactorrhea in a male patient with transsexualism. The first description of this kind was made in 1983 by R. Flüskiger et al. (6).
This observation demonstrates the independence of the mechanism of lactation development from one’s genetic sex and is alarming with regard to the possibility of drug-induced galactorrhea development in men.
Barber et al. (2004)
Barber, T., Basu, A., Rizvi, K., & Chapman, J. (2004). Normoprolactinaemic galactorrhoea in a male-to-female transsexual. Endocrine Abstracts, 7 [23rd Joint Meeting of the British Endocrine Societies with the European Federation of Endocrine Societies], 271–271. [Google Scholar] [URL]:
Hormonal therapies in the form of oestrogens, anti-androgens and progestogens are often used in the treatment of male-to-female transsexuals. We present the case of a 36 year old phenotypic male with karyotype 46XY who presented with normoprolactinaemic galactorrhoea likely to be related to prior oestrogen administration. He had been self-administering oestrogen and progesterone preparations continuously for 7 years (aged 26 - 33 years) in an attempt to develop female phenotypic characteristics in spite of a heterosexual desire. During this time he developed gynaecomastia with galactorrhoea, increased energy and libido, voice change and an attraction towards both men and women. However due to lack of financial resources to secure a complete gender change, he stopped self-medication with these preparations 3 years ago. Instead he embarked on a regime involving self-administered testosterone in an attempt to reverse the biological changes. After discontinuation of oestrogen the gynaecomastia regressed somewhat, although galactorrhoea continued and worsened with testosterone. Prior to referral he had been treated with dopamine agonists with little improvement in galactorrhoea and gynaecomastia.
Routine biochemistry and haematology are within their reference ranges. Baseline endocrinology is normal: Prolactin 197 milliUnits per litre, LH 2.9 Units per litre, FSH 7.9 Units per litre, free Testosterone 20 nanoMoles per litre, 17 beta-oestradiol less than 110 picoMoles per litre, TSH 0.96 milliUnits per litre and free T4 16.5 picoMoles per litre.
This case illustrates fascinating effects of exogenous oestrogen in the male. The effects of oestrogenic products of aromatised endogenous and briefly also exogenous testosterone acting on oestrogen-primed breast tissue may account for, at least in part, his continuing symptom of normoprolactinaemic galactorrhoea. However two other features do not have any direct explanations: the development of osteopenia during this period, and complete disappearance of vascular migraine, a condition worsened with oestrogens in the female. He is now on Tamoxifen although an opportunity to use the aromatase inhibitor, Anastrozole still remains.
Subsequent Case Reports
Moravek & Pasque (2019)
Moravek, M. B., & Pasque, K. B. (2019). Lactation Can Be Successfully Induced in Transgender Women While Maintaining Gender-Congruent Serum Hormone Levels. Reproductive Sciences, 26(Suppl 1), 136A–136A (abstract no. T-055). [Google Scholar] [DOI:10.1177/1933719119834079]:
Introduction: Transgender women may be interested in breastfeeding their children, but there are no established protocols for lactation induction in this population. The only case report of a lactation induction protocol in a transgender woman significantly lowered her estradiol dose, which would likely result in decreased serum estradiol and increased testosterone levels, with resultant increase in gender dysphoria. Our objective was to induce lactation in a transgender woman without interrupting her gendercongruent hormone profile.
Methods: A 34-year-old transgender woman with a 15-year history of gender-affirming hormone therapy with estradiol and spironolactone presented for lactation induction once her cisgender wife conceived. A modification of the Newman-Goldfarb method for adoptive mothers was used to induce lactation, and serum hormone levels followed.
Results: Baseline labs were obtained (time point 1), then medroxyprogesterone 1.25mg daily was added to her existing hormone regimen of estradiol 6mg daily and spironolactone 100mg twice daily (time point 2). Domperidone 10mg four times daily was initiated 1 month later. Approximately 5 weeks prior to the due date, the patient stopped medroxyprogesterone, decreased estradiol to 2mg daily, and began breast pumping (time point 3). Just prior to the infant’s birth, the patient was pumping 2-3 ounces of breastmilk every 3 hours (time point 4). Spironolactone was decreased to 50mg twice daily. Her son was born at term, via uncomplicated vaginal delivery. The infant was able to breastfeed from both mothers without difficulty, with both mothers pumping when they weren’t actively breastfeeding to maintain supply (time point 5). When the infant was approximately 2 months old, the patient noticed an increase in facial hair growth. Estradiol was increased to 3mg daily and spironolactone increased to 100mg twice daily, with resolution of hair growth and no decrease in milk supply (time point 6). The patient continued to breastfeed on this regimen for >6 months following her son’s birth. Serum hormone levels on the hormone regimens referenced at each time point throughout the patient’s course are displayed in table 1.
Conclusion: Lactation can be successfully induced in transgender women, without a significant decrease in estradiol supplementation. This regimen allows transgender women to breastfeed without developing male secondary sex characteristics incongruent with their gender identity
Table 1 Hormone profile at different time points.
Time Point
Estradiol (pg/mL)
Progesterone (ng/mL)
Testosterone (ng/mL)
Prolactin (ng/mL)
1
114
1.1
0.36
2
130
1.1
0.05
9
3
30
1.3
0.06
152
4
39
5
29
1.4
0.89
184
6
51
0.16
59
Unnithan, Elson, & Shenker (2020)
Unnithan, R., Elson, D. F., & Shenker, Y. (2020). Galactorrhea and Hyperprolactinemia in a Transgender Female. Journal of the Endocrine Society, 4(Suppl 1), A899–A899 (abstract no. SUN-043). [Google Scholar] [PubMed Central] [DOI:10.1210/jendso/bvaa046.1781] [PDF]:
Background: Galactorrhea is a rare manifestation of hyper-prolactinemia in males and post-menopausal females, however the hormonal milieu of the transgender female may increase its incidence
Clinical Case: A 43 year old transgender female presented with three years of bilateral breast discharge. She had chronic, stable headaches and fatigue, but no vision changes or other symptoms. Notably, she had breast augmentation surgery with saline breast implants placed shortly before the galactorrhea commenced. She was on a stable dose of estradiol tablets 1 mg twice daily for six years. On physical exam she had pronounced bilateral breast discharge of a milky quality with nipple compression. Prolactin levels were checked several times and were 40-50 ng/mL, TSH was 2.36 uIU/mL. An MRI showed a left inferior pituitary lesion measuring 6 mm x 3 mm x 5 mm with no mass effect on adjacent structures. Her breast discharge was not bothersome to her, and her pituitary lesion was small. It was unclear whether there was a relationship between her prolactin levels and the lesion seen on MRI, as we expected more pronounced prolactin elevation with a prolactinoma. Instead, given the timing of her symptoms in relation to her breast augmentation surgery, her galactorrhea and hyper-prolactinemia were thought to be the result of nipple irritation related to her breast implants combined with a hyper-estrogenemic state.
Clinical Lessons: In the setting of a prolactin secreting micro-adenoma, galactorrhea in a male is highly unusual. This case highlights the importance of recognizing that the unique medical and surgical characteristics of male to female transgender patients can lead to hyper-prolactinemia and galactorrhea.
Reference: Reisman T, Goldstein Z. Case report: induced lactation in a transgender woman. Transgender Health. 2018;3(1):24-26.
Wamboldt, Shuster, & Sidhu (2021)
Wamboldt, R., Shuster, S., & Sidhu, B. S. (2021). Lactation Induction in a Transgender Woman Wanting to Breastfeed: Case Report. The Journal of Clinical Endocrinology & Metabolism, 106(5), e2047–e2052. [DOI:10.1210/clinem/dgaa976]:
Context: Breastfeeding is known to have many health and wellness benefits to the mother and infant; however, breastfeeding in trans women has been greatly under-researched.
Objective: To review potential methods of lactation induction in trans women wishing to breastfeed and to review the embryological basis for breastfeeding in trans women.
Design: This article summarizes a case of successful lactation in a trans woman, in which milk production was achieved in just over 1 month.
Setting: This patient was followed in an outpatient endocrinology clinic.
Participant: A single trans woman was followed in our endocrinology clinic for a period of 9 months while she took hormone therapy to help with lactation.
Interventions: Readily available lactation induction protocols for nonpuerpural mothers were reviewed and used to guide hormone therapy selection. Daily dose of progesterone was increased from 100 mg to 200 mg daily. The galactogogue domperidone was started at 10 mg 3 times daily and titrated up to effect. She was encouraged to use an electric pump and to increase her frequency of pumping.
Main outcome measure: Lactation induction.
Results: At one month, she had noticed a significant increase in her breast size and fullness. Her milk supply had increased rapidly, and she was producing up to 3 to 5 ounces of milk per day with manual expression alone.
Conclusions: We report the second case in the medical literature to demonstrate successful breastfeeding in a trans woman through use of hormonal augmentation.
Further Case Reports
Delgado, D., Stellwagen, L., McCune, S., Sejane, K., & Bode, L. (2023). Experience of Induced Lactation in a Transgender Woman: Analysis of Human Milk and a Suggested Protocol. Breastfeeding Medicine, 18(11), 888–893. [DOI:10.1089/bfm.2023.0197]
Weimer, A. K. (2023). Lactation induction in a transgender woman: macronutrient analysis and patient perspectives. Journal of Human Lactation, 39(3), 488–494. [DOI:10.1177/08903344231170559]
van Amesfoort, J. E., Van Mello, N. M., & van Genugten, R. (2024). Lactation induction in a transgender woman: case report and recommendations for clinical practice. International Breastfeeding Journal, 19(1), 18. [DOI:10.1186/s13006-024-00624-1]
Trahair, E. D., Kokosa, S., Weinhold, A., Parnell, H., Dotson, A. B., & Kelley, C. E. (2024). Novel Lactation Induction Protocol for a Transgender Woman Wishing to Breastfeed: A Case Report. Breastfeeding Medicine, online ahead of print. [DOI:10.1089/bfm.2024.0012]
Dr. Christine McGinn
Dr. Christine McGinn is a transgender woman and well-known surgeon in Pennsylvania who performs gender-affirming surgeries for transgender people. When she had children with her cisgender female partner, McGinn induced a hormonal pseudopregnancy in herself and her and her partner breastfed their twins together. This was described in the media, including in books and television. McGinn’s case was never formally published as a case report in the scientific literature however.
The Oprah Winfrey Show (2010)
Terry, J. C. (Director), & Winfrey, O. G. (Presenter). (2010 September 29). The Mom Who “Fathered” Her Own Children, Plus the Cast of Modern Family [Television series episode]. The Oprah Winfrey Show (Season 25, Episode 13). Chicago: Harpo Studios. [URL 1] [URL 2] [URL 3]
Trans (2012)
Arnold, C. (Director), Schoen, M. (Producer), RoseWorks (Firm), & Sex Smart Films (Firm). (2012). Trans [DVD] (1:21:32–1:21:55). [WorldCat] [IMDB] [Amazon Prime Video]
Boylan (2014)
Boylan, J. F. (2014). Dr. Christine McGinn. In Boylan, J. F. Stuck in the Middle with You: A Memoir of Parenting in Three Genders (pp. 223–233). New York: Broadway Books. [Google Scholar] [Google Books 1] [Google Books 2] [WorldCat] [PDF]:
Dr. Christine McGinn is a surgeon, a mother of two, a backup flight surgeon for the space shuttle progarm, and a transgender woman. As a man, she saved her sperm before transition; ten years later she used that sperm to have children with her partner Lisa. The two of them are both biological mothers of their son and daughter, and each mother was able to breast-feed the twins. I sat down with Christine at her office in New Hope, Pennsylvania, on a hot summer day in 2011.
CM: […] Then there’s the scientist in me that knows that there is a difference, there is not a binary, but a gender spectrum. There are chemicals that are different in men and women. And when a transgender woman transitions, we are somewhere in the middle. Especialy having gone through a simulated pregnancy, in order to breast-feed, I felt the changes of those hormones. I felt my milk let down when not only my baby would cry, but a baby on TV would cry, and even, ridiculously, when a door would close and make a squeak.
JFB: You had to induce a false pregnancy in order to breast-feed? Tell me how you did that.
CM: As a doctor, I knew it was possible. I followed the protocol that involves simulating pregnancy with hormones. It’s estrogen and progesterone. My simulation pregnancy was over a month before Lisa delivered—with twins, we were expecting them to be born earlier. That entire month I was just pumping nonstop, every two hours. We had a whole freezer full of milk. And you know, the first couple of weeks it was no good, because it had all of the hormones in it. So we only saved, like, the last week or so. But still, it was a freezer full of milk.
Lisa had no idea about the way breast-feeding takes over your life, because this was her first. It was kind of funny that I went through that on my own, first, weeks before she did. And then it took her a couple of days to actually—for her milk to let down.
The children were so small when they were born. They were only five pounds. At first we had to feed them with a syringe. They were breast-feeding as well, but they weren’t latching that great on either of us.
JFB: What was it like when they finally muckled on to you?
CM: Oh, I can’t even put it in words. I really cannot put it in words. It was—I was just—oh.
JFB: Were you amazed? Were you afraid?
CM: It was heaven. I was afraid. I don’t know, it was uncharted territory. Like, I knew the milk was good. Lisa was a little concerned that it would be like skimmed milk, or something, you know. [Laughs] Like—she’s like, “Is it the same stuff?”
JFB: Is it the same milk?
CM: And she was a little dubious about, like, is this really all right? I think that’s totally natural for a mother, to be concerned.
I will just say that there are things snobody thinks about when two women are both breast-feeding. Like, technical stuff that you don’t think about. When you have a mother and a father, the mother decides when the kids get fed. Right? The father doesn’t, really. Right?
But you know, when you have two women who are filled with pregnancy hormones and have that, like, mother-bear attitude about how things should be done… It was really crazy.
JFB: So did that cause serious conflict between you and Lisa?
CM: Totally not serious conflict, because the most important thing are the babies.
Eden finally latched—I breast-fed her more than Luke. Luke was never really good. Lisa hated breast-feeding. Eventually we decided to stop.
I’m putting on my science hat again—when you decide to stop, there are hormonal issues. The strongest emotion a person can feel in their life comes frm oxytocin, which is the love drug.
JFB: Oxytocin?
CM: That’s what’s responsible for babies’ bonding during breastfeeding. So the baby latches on, breast-feeds, your brain just [makes oozing sounds], just like, oozes this gooey love substance, oxytocin. Fathers are proven to have higher oxytocin before the delivery, and just stroking your child’s head. You know, when the baby—when you smell a newborn’s head, it really—that smell, it’s like—
JFB: I just saw a friend’s newborn on Friday, and I was like, [makes sniffing sound]—
CM: My niece said it best. She came in and smell them, and she was five years old at the time, and she’s like, “They smell like cupcakes.” [Laughs] And it’s universal. When you ask me what that’s like, I can’t describe it, you know, and I’m a huge fan of food and cupcakes and chocolate, and so that’s the closest I can come to it—it’s like chocolate. [Laughs]
JFB: So when you stopped breast-feeding, was it a kind of a mourning, a loss?
CM: Yes. Lisa wanted to stop before I did. The problem is, once a baby gets a nipple, a plastic nipple, it gives more milk. And so they don’t have to work as hard.
It’s a unique situation that two breast-feeders in a relationship would experience, but a mother and father would not.
JFB: So did one of you stop breast-feeding before the other?
CM: Yes, Lisa did.
JFB: Lisa stopped. And how much longer did you keep it up?
CM: Not long, because they got the nipple.
They were both so small. We weren’t all that successful at it. We were so worried about their birth weight, and making sure they got enough with the syringes. There were definitely times where, you know, we both would breast-feed and, man, I will never forget that. Like, three ‘clock in the morning, four o’clock in the morning, in the little cocoon, nursing.
The heat of their body, their naked body on your chest. The amazing thing is, it really does kind of hurt when they really get going, you know. And you just… I don’t know how else to describe it. You feel like the life force is just coming out through you. It’s so powerful. It relieves that pain that you have in your breast. It releases that oxytocin, and it’s just—it’s even.
JFB: Did you ever do that thing where you would fall asleep with the children in the bed, and wake up with the children in the bed beside you?
CM: Yeah.
JFB: I loved that. It’s one of my stnogest memories of being a father. Having gotten up in the middle of the night. And they are so small, but such an incredibly powerful feeling, the two of you together surrounding the child. With us, we also had a dog at the bottom of the bed. [Laughs]
CM: And we have two, and that was also very important to me, too. We have miniature pinschers.
JFB: So how many months along did you stop breast-feeding?
CM: Three months. It was really emotionally painful, and I cried a lot. I was really sad.
I was pretty sure we were not going to have any more kids. So I’m like, “This is it.” It was very sad.
JFB: Is there a moment frm the last year and two months where you think, This is what it’s like to be a mother, this is it?
CM: Yes, immediately. It was hot as Hades outside. It was, like, a million degrees. We had just had the kids. It was like, May or June, and my mom was over, and it was, like, we had all this help, initially, because Lisa and I were just not getting any sleep and it was, like, round-the-clock feedings and the kids were small, and Lucas had an apnea monitor that he had to wear all the time, and it was just really hard. And there was a big thunderstorm, and the power went out.
And so, at this point, they weren’t really latching very well, so we both had to pump, and then feed them with the syringes. So Lisa and I are totally, like, engorged with milk. And the power’s out, and the pumps are electric. Right?
JFB: Right.
CM: So there’s no electricity, it’s hot as hell, we’re worried for the kids. Lisa and I are in pain. We’re both leaking. And it was the weirdest, funniest situation. And my mom’s there. She runs out to the store to get batteries, and you know, she’s just beng a mom. She’s getting everything, running around like an angel. And Lisa and I are in pain we’re miserable. When she finally came back, the batteries wouldn’t work on the pumps—something else was wrong. Lisa and I are dying.
And so, here’s the guy part of me… I get the pump that has the backup battery power and the backup car charger. Like, I got all tech on it. [Laughs] I’m out int he car trying to get the car charger to work on the pump in the pouring rain. And it’s ninety-five degrees out. It’s all wet inside, like, the humidity on the windows.
And I’m just trying to get some kind of relief.
And this stupid pump didn’t work that way, either. We come back in and my mom has candles lit.
And then the electricity comes back on. And we all just laugh and pump and breast-feed. And every one of us is in heaven.
Pfeffer (2017)
Pfeffer, C. A. (2017). Trans Partnerships and Families: Historical Traces and Contemporary Representations. In Pfeffer, C. A. Queering Families: The Postmodern Partnerships of Cisgender Women and Transgender Men (pp. 1–34). New York: Oxford University Press. [Google Scholar] [Google Books] [WorldCat] [DOI:10.1093/acprof:oso/9780199908059.003.0001]:
Just 2 years later, Winfrey would feature another interview that elicited many of the same audience reactions. In this 2010 episode, lesbian partners Dr. Christine McGinn and Lisa Bortz beamed with joy as they held their infant twins. Again, audience members’ jaws dropped when it was revealed that beautiful Christine was a male-to-female transsexual who used to be a handsome military officer Chris, and that Lisa had given birth to the couple’s biological children using sperm Chris banked prior to gender confirmation surgeries.10 And it was Winfrey’s chin that nearly hit the floor as she watched video of Christine breastfeeding the couples’ children (the episode is referred to online as “The Mom Who Fathered Her Own Children”).
Other Instances
Published
Estrogen plus cyproterone acetate has been reported to produce pregnancy-like breast changes—specifically, lobuloalveolar development of the breasts—in transfeminine people (Kanhai et al., 2000). Accordingly, galactorrhea (spontaneous or excessive lactation) has been reported as a low-incidence side effect (7–14%) of hormone therapy regimens containing estrogen plus cyproterone acetate in transfeminine people (Gooren, Harmsen-Louman, & van Kessel, 1985; Schlatterer et al., 1998; Bazarra-Castro, 2009). It has also been reported at low incidence (6%) for other hormone therapy regimens (Futterweit, 1980). Sudden cessation of hormone therapy regimens including cyproterone acetate has been reported to result in the onset of lactation as well (Levy, Crown, & Reid, 2003).
Unpublished
Many unpublished reports of lactation and breastfeeding in transfeminine people have been described on the web including at the following pages:
Richards, A. (2003). Lactation and the Transsexual Woman. Second Type Woman. [Updated August 2018] [URL] [PDF]
MacDonald, T. (2013). Trans Women and Breastfeeding: A Personal Interview. Milk Junkies. [URL]
MacDonald, T. (2013). Trans Women and Breastfeeding: The Health Care Provider. Milk Junkies. [URL]
MacDonald, T. (2017). Jenna’s Breastfeeding Journey: Trans Motherhood. Milk Junkies. [URL]
Burns, K. (2018). Yes, Trans Women Can Breastfeed — Here’s How. them. [URL]
Cisgender Men
Induction of lactation has been reported in cisgender men and is noteworthy:
Geschickter (1945)
Geschickter, C. F. (1945). Endocrine Physiology of the Breast. In Geschickter, C. F. Diseases of the Breast: Diagnosis, Pathology, Treatment, 2nd Edition (pp. 42–81). Philadelphia: J.B. Lippincott. [Google Scholar] [Google Books] [OpenLibrary] [WorldCat] [PDF]:
The results obtained indicate that a lactogenic substance in anterior pituitary extracts may cause mammary secretion in nonpregnant women when they have been previously stimulated with estrogenic hormone but true lactation does not occur. Secretion was also obtained in two adult men with gynecomastia after injections of lactogenic hormone.
Huggins (1949)
Huggins, C. (1949). Endocrine substances in the treatment of cancers. Journal of the American Medical Association, 141(11), 750–754. [DOI:10.1001/jama.1949.02910110002002]:
The administration of estrogen in effective amounts causes testicular atrophy and mammary hypertrophy. Growth of the breasts can be so extensive that lactation may be induced, as illustrated in the following case.
W. N., aged 64, had carcinoma of the prostate with osseous metastases, for which he was treated by a permanent suprapubic cystotomy in 1941. Diethylstilbestrol, 20 mg. daily, was given orally for two years beginning September 1942. In September 1944, 25 mg. (500 international units) of prolactin14 was injected daily for five days, and at the end of this time creamy milk could be expressed from both breasts. Orchiectomy and removal of the cystostomy tube were carried out September 6, when administration of estrogen was discontinued; both incisions healed promptly. Since then the patient has been clinically well but has continued to lactate, a large drop of milk being easily expressed from each breast at frequent intervals.
Huggins & Dao (1954)
Huggins, C., & Dao, T. L. (1954). Lactation induced by luteotrophin in women with mammary cancer. Growth of the breast of the human male following estrogenic treatment. Cancer Research, 14(4), 303–306. [Google Scholar] [PubMed] [URL]:
In the observations to be presented luteotrophin [prolactin] was employed as a stimulus for mammary secretion in patients with cancer of the breast, and the results throw new light on the physiology of women bearing this neoplasm. We shall also describe conditions which resulted in the induction of physiologic maturity in the human male, since knowledge of the action of hormones on the human breast is vague.
The effects of luteotrophin on the breast of women post partum has been extensively investigated, but otherwise few observations have been made in the human. Werner (14) administered a crude pituitary extract containing luteotrophin to eight castrate women 21–35 years of age; lactation was not observed, although in one woman “a few drops of colostrum-like fluid” could be expressed from the breasts. Goldzieher (4) treated menstrual disorders in women with luteotrophin, but mammary secretion was not described by him.
PROCEDURE
Luteotrophin,1 dissolved in physiological saline made slight ly alkaline (pH 9) with sodium hydroxide, was injected subcutaneously in daily amounts of 500 International Units; the solutions were freshly prepared, and the injections were continued for 7 days only.
This series comprised 21 female patients who had dis seminated mammary cancer, and all had been subjected to unilateral mastectomy. There were also three men with advanced prostatic carcinoma who had been treated for thera peutic purposes with oral diethylstilbestrol for 20 months, 2, and 6 years, respectively. There were eight persons without mammary or prostatic cancers who served as controls.
In each case of mammary cancer a biopsy of the breast was obtained for histological purposes, the material being stained with Sudan III.3
OBSERVATIONS
Lactation, when it occurred, was never profuse; it varied from a tiny drop to ca. 0.5 cc. from each breast. Clear colostrum was not observed, and the mammary secretion was always milk, as defined above.
Mammary growth in the human male.—Estrogenic substances had been administered to three men in the treatment of disseminated prostate cancer for many months; after luteotrophin injection two lactated and one did not lactate.
W. N. (reported in brief earlier [5]), age 64, had taken diethylstilbestrol, 20 mg/day, orally for 2 years, after which interval sub-areolar button-like masses of mammary tissue could be palpated bilaterally; luteotrophin was then injected for 5 days, and milk was expressed from the breast on the 6th day. Orchiectomy was then performed, and both luteotrophin and estrogenic substances were discontinued. This man continued to lactate for 7 years when the formation of milk gradually ceased.
In the case of A. W., age 62, diethylstilbestrol (5–15 mg/day) had been ingested for 20 months after bilateral orchiectomy; the breasts became slightly enlarged. Luteotrophin was injected, and lactation occurred on the 7th day. A biopsy of the breast showed moderately well developed mammary ducts and alveoli containing milk. In the case of E. G., age 59, diethylstilbestrol (5 mg/day) was ingested almost continuously for 6 years; this resulted in the development of large pendulous breasts, but no lactation occurred after injections of luteotrophin.
Lactation in humans without cancer.—Luteotrophin was administered to two normal males, age 51 and 59, and to four normal females, age 84–59, and none lactated.
DISCUSSION
It must be emphasized that lactation was not copious in any of the humans when it had been induced by luteotrophin; merely small amounts of milk were obtained. It was apparent, however, from the histological studies of the mammary tissue obtained by biopsy that the secretion of milk in any quantity was a criterion of maturity of mammary epithelium.
In the goat and guinea pig it is known that estrogenic substances can induce mammary ma turity without the intervention of exogenous synergistic steroids. In the experiments of Lewis and Turner (9) diethylstilbestrol was implanted in two castrate male goats; one of these animals failed to lactate, while the other produced a small quantity of milk without luteotrophin injections. They obtained small amounts of milk from a male kid similarly treated. Nelson (10) found that estrone induced mammary growth with, later, lactation in the male guinea pig. Our observations demonstrate that diethylstilbestrol ingested for prolonged periods of time can induce maturity of the breast in certain elderly human males. However, the human male differs from the animals just described in that spontaneous lactation was not observed; the injection of luteotrophin was necessary for milk formation.
The duration of lactation induced by luteo trophin was impressive, since milk commonly persisted for many months—and in one male for 7 years. The mechanism whereby this type of lactation is maintained for such long periods of time is at present unknown; we know that milk continues to be secreted both in the presence of the adrenal glands and in the absence of these structures and the gonads as well. Observations (8) have been made on experimental animals which are analogous to the clinical findings; most dogs with spontaneous mammary cancer possess lactation, and this characteristic persists for many months, at least, despite the removal of the adrenal glands and the ovaries.
SUMMARY
The breast of the human male can be induced to grow to a functionally mature state by the administration of estrogenic substances without additional exogenous steroid synergists. Spontaneous lactation was not observed in these men, but it was induced by luteotrophin.
The formation of milk in any amount by the breast is a criterion of functional maturity of the mammary epithelium. Luteotrophin induced the secretion of small amounts of milk in a group of women with mammary cancer and in a number of healthy women as well, and, in addition, in two human males to whom estrogenic substances had been administered for therapeutic purposes. Lactation did not occur in two normal males.
When lactation was induced in human beings, the secretion often persisted for many months; it lasted for 7 years in one man.
HUGGINS,C. Endocrine Substances in the Treatment of Cancers. J.A.M.A., 141:750–54, 1949.
Brodribb, W., & Academy of Breastfeeding Medicine. (2018). ABM Clinical Protocol #9: Use of galactogogues in initiating or augmenting maternal milk production, second revision 2018. Breastfeeding Medicine, 13(5), 307–314. [DOI:10.1089/bfm.2018.29092.wjb]
MacDonald, T. K. (2019). Lactation care for transgender and non-binary patients: Empowering clients and avoiding aversives. Journal of Human Lactation, 35(2), 223–226. [DOI:10.1177/0890334419830989]
Paynter, M. J. (2019). Medication and Facilitation of Transgender Women’s Lactation. Journal of Human Lactation, 35(2), 239–243. [DOI:10.1177/0890334419829729]
Cazorla-Ortiz, G., Obregón-Guitérrez, N., Rozas-Garcia, M. R., & Goberna-Tricas, J. (2020). Methods and Success Factors of Induced Lactation: A Scoping Review. Journal of Human Lactation, 36(4), 739–749. [DOI:10.1177/0890334420950321]
Ferri, R. L., Rosen-Carole, C. B., Jackson, J., Carreno-Rijo, E., Greenberg, K. B., & Academy of Breastfeeding Medicine. (2020). ABM Clinical Protocol #33: Lactation Care for Lesbian, Gay, Bisexual, Transgender, Queer, Questioning, Plus Patients. Breastfeeding Medicine, 15(5), 284–293. [DOI:10.1089/bfm.2020.29152.rlf]
García-Acosta, J. M., Juan-Valdivia, S., María, R., Fernández-Martínez, A. D., Lorenzo-Rocha, N. D., & Castro-Peraza, M. E. (2020). Trans* Pregnancy and Lactation: A Literature Review from a Nursing Perspective. International Journal of Environmental Research and Public Health, 17(1), 44. [DOI:10.3390/ijerph17010044]
LeCain, M., Fraterrigo, G., & Drake, W. M. (2020). Induced Lactation in a Mother Through Surrogacy With Complete Androgen Insensitivity Syndrome (CAIS). Journal of Human Lactation, 36(4), 791–794. [DOI:10.1177/0890334419888752]
Trautner, E., McCool-Myers, M., & Joyner, A. B. (2020). Knowledge and practice of induction of lactation in trans women among professionals working in trans health. International Breastfeeding Journal, 15(1), 63. [DOI:10.1186/s13006-020-00308-6]
References (Inline Citations)
Bazarra-Castro, M. A. (2009). Etiological aspects, therapy regimes, side effects and treatment satisfaction of transsexual patients. (Doctoral dissertation, Ludwig Maximilian University of Munich.) [DOI:10.5282/edoc.9984] [URN:urn:nbn:de:bvb:19-99840] [PDF]
Delgado, D., Stellwagen, L., McCune, S., Sejane, K., & Bode, L. (2023). Experience of Induced Lactation in a Transgender Woman: Analysis of Human Milk and a Suggested Protocol. Breastfeeding Medicine, 18(11), 888–893. [DOI:10.1089/bfm.2023.0197]
Futterweit, W. (1980). Endocrine management of transsexual. Hormonal profiles of serum prolactin, testosterone, and estradiol. New York State Journal of Medicine, 80(8), 1260–1264. [Google Scholar] [PubMed] [Archive.org] [PDF]
Gooren, L. J., Harmsen-Louman, W., & Kessel, H. (1985). Follow-up of prolactin levels in long-term oestrogen-treated male-to-female transsexuals with regard to prolactinoma induction. Clinical Endocrinology, 22(2), 201–207. [DOI:10.1111/j.1365-2265.1985.tb01081.x]
Greenblatt, R. B. (1972). Inappropriate lactation in men and women. Medical Aspects of Human Sexuality, 6(6), 25–33. [Google Scholar] [Google Books]
Greenblatt, R. B., & Leng, J. J. (1972). Lactation anormale chez l’homme. [Abnormal lactation in males.] Bordeaux Medical, 5(3), 241–243. [Google Scholar] [PubMed]
Kanhai, R. C., Hage, J. J., van Diest, P. J., Bloemena, E., & Mulder, J. W. (2000). Short-Term and Long-Term Histologic Effects of Castration and Estrogen Treatment on Breast Tissue of 14 Male-to-Female Transsexuals in Comparison With Two Chemically Castrated Men. The American Journal of Surgical Pathology, 24(1), 74–80. [DOI:10.1097/00000478-200001000-00009]
Levy, A., Crown, A., & Reid, R. (2003). Endocrine intervention for transsexuals. Clinical Endocrinology, 59(4), 409–418. [DOI:10.1046/j.1365-2265.2003.01821.x]
Schlatterer, K., Yassouridis, A., Werder, K. V., Poland, D., Kemper, J., & Stalla, G. K. (1998). Archives of Sexual Behavior, 27(5), 475–492. [DOI:10.1023/a:1018704630036]
Trahair, E. D., Kokosa, S., Weinhold, A., Parnell, H., Dotson, A. B., & Kelley, C. E. (2024). Novel Lactation Induction Protocol for a Transgender Woman Wishing to Breastfeed: A Case Report. Breastfeeding Medicine, online ahead of print. [DOI:10.1089/bfm.2024.0012]
van Amesfoort, J. E., Van Mello, N. M., & van Genugten, R. (2024). Lactation induction in a transgender woman: case report and recommendations for clinical practice. International Breastfeeding Journal, 19(1), 18.[DOI:10.1186/s13006-024-00624-1]
Weimer, A. K. (2023). Lactation induction in a transgender woman: macronutrient analysis and patient perspectives. Journal of Human Lactation, 39(3), 488–494. [DOI:10.1177/08903344231170559]
\ No newline at end of file
+Published Case Reports of Lactation and/or Breastfeeding in Transfeminine People - Transfeminine Science
Published Case Reports of Lactation and/or Breastfeeding in Transfeminine People
By Aly | First published March 26, 2019 | Last modified May 8, 2025
Abstract / TL;DR
A number of case reports of hormonally induced lactation and breastfeeding in transfeminine people have been published. The earliest report of lactation in a transfeminine person was in the 1950s and the earliest report of breastfeeding was in the 1980s. Starting in 2019, more case reports have been published in the modern scientific literature. Unpublished cases also exist (e.g., that of Dr. Christine McGinn), and lactation has been induced or occurred in cisgender men as well. Lactation may be induced in transfeminine people with the use estrogens, progestogens, and/or prolactin releasers. Reviews discussing lactation induction in transfeminine people have recently been published.
Introduction
Last year, a case report of lactation and breastfeeding in a transgender woman was published:
Reisman, T., & Goldstein, Z. (2018). Case report: Induced lactation in a transgender woman. Transgender Health, 3(1), 24–26. [DOI:10.1089/trgh.2017.0044]
In the paper, the authors state the following:
We believe that this is the first formal report in the medical literature of induced lactation in a transgender woman.
However, this actually wasn’t the first case report of lactation and/or breastfeeding in a transfeminine person in the literature. There are various previous published cases dating back as far as the 1950s. These instances are provided below in the format of sources and excerpts.
Published Case Reports
Foss (1956)
Foss, G. L. (1956). Abnormalities of form and function of the human breast. Journal of Endocrinology, 14(4 Suppl) [Proceedings of the Society for Endocrinology: Fifty-Fourth Meeting. Symposium on Selected Aspects of the Practice of Hormone Administration in Animals and Man], vi–vii. [Google Scholar] [Google Books] [URL] [PDF]:
Based on the theories of lactogenesis and stimulated by the success of Lyons, Li, Johnson & Cole [1955], who succeeded in producing lactation in male rats, an attempt was made to initiate lactogenesis in a male transvestist. Six years ago this patient had been given oestrogens. Both testes and penis were then removed and an artificial vagina was constructed by plastic surgery. The patient was implanted with 500 mg oestradiol in September 1954, and 600 mg in July 1955. The breasts were then developed more intensively with daily injections of oestradiol dipropionate and progesterone for 6 weeks. Immediately following withdrawal of this treatment, prolactin 22·9 mg was injected daily for 3 days without effect. After a second month on oestradiol and progesterone daily, combined injections of prolactin and somatotrophin were given for 4 days and suction was applied by a breast pump—four times daily. On the 4th and 5th days a few drops of colostrum were expressed from the right nipple.
Tindal & McNaught (1958)
Tindal, J. S., & McNaught, M. L. (1958). Hormonal Factors in Breast Development and Milk Secretion. In Gardiner-Hill, H. (Ed.). Modern Trends in Endocrinology, Volume 1 (pp. 188–211) (Modern Trends). London: Butterworth. [Google Scholar] [Google Books] [OpenLibrary] [WorldCat] [Archive.org]:
Recently, an attempt has been made by Foss (1956) to initiate lactation in a castrated male transvestist. He was given an implant of 500 milligrams of oestradiol, and 10 months later, a further 600 milligrams of oestradiol, followed by daily injections of oestradiol dipropionate and progesterone for 6 weeks. Immediately after withdrawal of this treatment, 22·9 milligrams of prolactin were injected daily for 3 days but without effect. After a second month of treatment with oestradiol and progesterone daily, he was given combined injections of prolactin and somatotrophin for 4 days, suction with a breast-pump being employed 4 times daily. On the fourth and fifth days a few drops of colostrum were expressed from the right nipple. There is a possible application here of modern hormone knowledge to man, and further trials would be of interest.
Experimentally I have been able to induce lactogenesis in a male transvestite whose testes had been removed some years before and whose breasts had been well developed over a long period with stilbestrol and ethisterone.9 In July, 1955, 600 mg. of estradiol was implanted subcutaneously and weekly injections of 50 mg. of progesterone were given for four months. For the next month daily injections of 10 mg. estradiol dipropionate and 50 mg. progesterone were given. These injections were continued for another month, increasing progesterone to 100 mg. daily. Both hormones were then withdrawn, and daily injections of increasing doses of prolactin and somatotropin were given for four days; at the same time, the patient used a breast pump four times daily for 5 minutes on both sides. During this time the mammary veins were visibly enlarged and on the sixth and seventh days 1 to 2 cc. of milky fluid was collected.
Flückiger, Del Pozo, & von Werder (1982)
Flückiger, E., Del Pozo, E., & von Werder, K. (1982). Prolactin: Synthesis, Fate and Actions. In Flückiger, E. W., Del Pozo, E., & von Werder, K. (Eds.). Prolactin: Physiology, Pharmacology, and Clinical Findings (Monographs on Endocrinology, Volume 23) (pp. 1–23). Berlin/Heidelberg: Springer-Verlag. [Google Scholar] [Google Books] [DOI:10.1007/978-3-642-81721-2_1]:
An observation (Wyss and Del Pozo unpublished) in a male transsexual showed that induction of lactation can be similarly achieved in the human male.
Flückiger, E., Del Pozo, E., & von Werder, K. (1982). Nontumoral hyperprolactinemia. In Flückiger, E. W., Del Pozo, E., & von Werder, K. (Eds.). Prolactin: Physiology, Pharmacology, and Clinical Findings (Monographs on Endocrinology, Volume 23) (pp. 102–152). Berlin/Heidelberg: Springer-Verlag. [Google Scholar] [Google Books] [DOI:10.1007/978-3-642-81721-2_4]:
4.3.2 Effect of Hyperprolactinemia in Male Subjects
Although PRL circulates in male blood in appreciable concentrations its physiologic role has not been clarified. The lack of lactational requirements does not preclude that under adequate priming the male mammary gland will respond to a PRL challenge with milk production. Thus, Wyss and del Pozo (unpublished data) found that PRL stimulation with TRH was able to induce milk secretion in a male individual pretreated with estrogens. Certainly, the chronic ingestion of dopamine antagonists or estrogens may lead to sustained hyperprolactinemia, and the same effect can be expected in male subjects on chronic estrogen therapy of prostatic cancer or transsexualism (Frantz 1973; del Pozo, to be published).
Certainly, the prolonged intake of estrogens, in male subjects also, as observed in the treatment of prostatic carcinoma and in transsexuals, can lead to hyperprolactinemia (Frantz 1972b; del Pozo, to be published).
Kozlov, Mel’nichenko, & Golubeva (1985)
Kozlov, G. I., Mel’nichenko, G. A., & Golubeva, I. V. (1985). Случай лактореи у больного мужского пола с транссексуализмом. [Sluchai laktorei u bol’nogo muzhskogo pola s transseksualizmom. / Case of galactorrhea in a transsexual male patient.] Проблемы Эндокринологии [Problemy Èndokrinologii (Moskva) / Problems of Endocrinology (Moscow)], 31(1), 37–38. [ISSN:0375-9660] [Google Scholar 1] [Google Scholar 2] [PubMed] [DOI:10.14341/probl198531137-38] [PDF] [Translation] [Translated]:
The appearance of galactorrhea in men is most often a symptom of pituitary prolactinoma. Combined with gynecomastia and atrophy of the testicles, galactorrhea caused by adenomas of the pituitary gland in men is known as O’Connell syndrome (1).
In recent years, however, cases of galactorrhea have been described in men without radiological or clinical signs of pituitary adenoma (12). Of course, in these cases, the presence of undetected microadenomas of the pituitary gland cannot be excluded, especially since the level of prolactin in these patients is significantly increased (1, 2).
Some medications, especially antipsychotics and estrogen-containing oral contraceptives (7, 10), increase serum levels of prolactin and can lead to the development of galactorrhea.
There is information about the influence of psycho-emotional factors on the lactation process: the possibility of the development (induction) of psychogenic lactation during false pregnancy (3) is known, and, conversely, the possibility of the termination of lactation in nursing mothers after mental stress.
Accumulated clinical observations on the frequent development of depressive states in persistent galactorrhea–amenorrhea syndrome (4), cases of galactorrhea in the mentally ill, even in the absence of neuroleptics (7), as well as experimental observations on the effect of hyperprolactinemia on the behavioral responses of animals (5), require careful study of the relationship of hyperprolactinemia and psycho-emotional factors. In connection with this, we present the following observation.
The patient (P), was born a normal, full-term boy. He remembers well from 6 years. Early development was unremarkable, he did not differ from peers, but loved to play more with girls. He played with dolls and cars. At 10 years of age, there was a desire to wear women’s clothes. From the age of 12 he swam with girls in a shirt and shorts, as he was embarrassed by the lack of breasts. From the age of 14 he changed clothes in his mother’s dress, and only in such clothes “felt like a person”. From the same age in a woman’s dress he went to get acquainted with young men and got pleasure from it. At the age of 15, he came to the firm conviction that he was a girl, began to urinate like a girl, squatting, use lipstick, and put on powdered makeup. He suffered greatly from the presence of “deformities” – male genital organs. At the age of 17, while working as a “nurse” in a hospital, he began to self-inject himself with folliculin (estrogen) and progesterone, which caused the development of the breasts. With pleasure, he did women’s housework, and loved to tinker with children. Having received a passport, he redid it as female, thus resulting in a female civilian gender.
Twice he tried to commit suicide (he took sleeping pills), since he could not bear the duality of his existence. Twice he was treated in psychiatric hospitals about transsexualism, unsuccessfully.
During the examination in IEE and HCG at the age of 20 years, no abnormalities in somatic status were revealed: complex as a man, male genitals, shaved from 17 years of age daily. Erotic dreams were frequent, wherein he played the role of a woman, and denied emissions. The ejaculate was studied (obtained by vibratory massage): volume – 1.4 mL, pH 8.8 (norm 7.6–8.2), sperm count 31 million per 1 mL, mobility 57%, and morphologically normal 69%. Sex chromatin is negative.
At age 22, a course of treatment with cyproterone acetate was conducted at the Institute of Psychiatry of the Ministry of Health of the USSR. Muscle weakness, reduction of sexual hairiness, and appearance of colostrum excretion was noted.
When examined in IEE and HCG at 23 years, the breasts corresponded to the age of 15–16 years (on his own initiative he periodically took estrogens), and colostrum was secreted from the nipples (abundant drops when pressed – galactorrhea (++)). He insisted on castration and amputation of the penis, since, being a “woman”, he was ashamed of not having the appropriate genitals for his sex, which he called “deformities”.
On X-ray of the skull, the shape and size of the sella turcica were normal, but signs of increased intracranial pressure were revealed. On EEG against the background of the general phenomena of irritation, the focus of pathology was recorded in the left parietal lead. Indicators of the functional state of the thyroid gland were in the normal range. In the study of the radioimmunoassay method using standard kits from the Sorin company, some increase in prolactin level of 24 ng/mL was detected in the serum (normal for men is 4–15 ng/mL).
In connection with the repeated suicidal attempts, failure of psychiatric treatment, and in consideration of the fact that the patient has a female civilian sex and performs a female social role, castration and feminizing plastic surgery of the external genitalia were performed for the purpose of social rehabilitation.
Some time after the operation, the patient developed a renewed interest in life. After the surgical and hormonal correction, the patient irresistibly developed maternal instincts. Unmarried, the patient obtained permission for the adoption of a child, simulated pregnancy, and was discharged from the maternity hospital with a son. From the first days after the “birth”, galactorrhea sharply increased, and spontaneous outflow of milk appeared, with galactorrhea (+++). The baby was breastfed up to 6 months of age.
Thus, it can be thought that several factors played a role in the genesis of galactorrhea in this patient:
Increased prolactin levels with estrogen and cyproterone acetate. The hyperprolactic properties of estrogens have long been known; the ability of cyproterone acetate to increase serum prolactin levels was shown by K. Schmidt–Golewizer et al (9).
Increased intracranial pressure, the role of this factor and the genesis of neuroendocrine disorders and, in particular, in the development of galactorrhea was shown by R. Peterson (8).
Our message is the second in the world literature describing galactorrhea in a male patient with transsexualism. The first description of this kind was made in 1983 by R. Flüskiger et al. (6).
This observation demonstrates the independence of the mechanism of lactation development from one’s genetic sex and is alarming with regard to the possibility of drug-induced galactorrhea development in men.
Barber et al. (2004)
Barber, T., Basu, A., Rizvi, K., & Chapman, J. (2004). Normoprolactinaemic galactorrhoea in a male-to-female transsexual. Endocrine Abstracts, 7 [23rd Joint Meeting of the British Endocrine Societies with the European Federation of Endocrine Societies], 271–271. [Google Scholar] [URL]:
Hormonal therapies in the form of oestrogens, anti-androgens and progestogens are often used in the treatment of male-to-female transsexuals. We present the case of a 36 year old phenotypic male with karyotype 46XY who presented with normoprolactinaemic galactorrhoea likely to be related to prior oestrogen administration. He had been self-administering oestrogen and progesterone preparations continuously for 7 years (aged 26 - 33 years) in an attempt to develop female phenotypic characteristics in spite of a heterosexual desire. During this time he developed gynaecomastia with galactorrhoea, increased energy and libido, voice change and an attraction towards both men and women. However due to lack of financial resources to secure a complete gender change, he stopped self-medication with these preparations 3 years ago. Instead he embarked on a regime involving self-administered testosterone in an attempt to reverse the biological changes. After discontinuation of oestrogen the gynaecomastia regressed somewhat, although galactorrhoea continued and worsened with testosterone. Prior to referral he had been treated with dopamine agonists with little improvement in galactorrhoea and gynaecomastia.
Routine biochemistry and haematology are within their reference ranges. Baseline endocrinology is normal: Prolactin 197 milliUnits per litre, LH 2.9 Units per litre, FSH 7.9 Units per litre, free Testosterone 20 nanoMoles per litre, 17 beta-oestradiol less than 110 picoMoles per litre, TSH 0.96 milliUnits per litre and free T4 16.5 picoMoles per litre.
This case illustrates fascinating effects of exogenous oestrogen in the male. The effects of oestrogenic products of aromatised endogenous and briefly also exogenous testosterone acting on oestrogen-primed breast tissue may account for, at least in part, his continuing symptom of normoprolactinaemic galactorrhoea. However two other features do not have any direct explanations: the development of osteopenia during this period, and complete disappearance of vascular migraine, a condition worsened with oestrogens in the female. He is now on Tamoxifen although an opportunity to use the aromatase inhibitor, Anastrozole still remains.
Subsequent Case Reports
Moravek & Pasque (2019)
Moravek, M. B., & Pasque, K. B. (2019). Lactation Can Be Successfully Induced in Transgender Women While Maintaining Gender-Congruent Serum Hormone Levels. Reproductive Sciences, 26(Suppl 1), 136A–136A (abstract no. T-055). [Google Scholar] [DOI:10.1177/1933719119834079]:
Introduction: Transgender women may be interested in breastfeeding their children, but there are no established protocols for lactation induction in this population. The only case report of a lactation induction protocol in a transgender woman significantly lowered her estradiol dose, which would likely result in decreased serum estradiol and increased testosterone levels, with resultant increase in gender dysphoria. Our objective was to induce lactation in a transgender woman without interrupting her gendercongruent hormone profile.
Methods: A 34-year-old transgender woman with a 15-year history of gender-affirming hormone therapy with estradiol and spironolactone presented for lactation induction once her cisgender wife conceived. A modification of the Newman-Goldfarb method for adoptive mothers was used to induce lactation, and serum hormone levels followed.
Results: Baseline labs were obtained (time point 1), then medroxyprogesterone 1.25mg daily was added to her existing hormone regimen of estradiol 6mg daily and spironolactone 100mg twice daily (time point 2). Domperidone 10mg four times daily was initiated 1 month later. Approximately 5 weeks prior to the due date, the patient stopped medroxyprogesterone, decreased estradiol to 2mg daily, and began breast pumping (time point 3). Just prior to the infant’s birth, the patient was pumping 2-3 ounces of breastmilk every 3 hours (time point 4). Spironolactone was decreased to 50mg twice daily. Her son was born at term, via uncomplicated vaginal delivery. The infant was able to breastfeed from both mothers without difficulty, with both mothers pumping when they weren’t actively breastfeeding to maintain supply (time point 5). When the infant was approximately 2 months old, the patient noticed an increase in facial hair growth. Estradiol was increased to 3mg daily and spironolactone increased to 100mg twice daily, with resolution of hair growth and no decrease in milk supply (time point 6). The patient continued to breastfeed on this regimen for >6 months following her son’s birth. Serum hormone levels on the hormone regimens referenced at each time point throughout the patient’s course are displayed in table 1.
Conclusion: Lactation can be successfully induced in transgender women, without a significant decrease in estradiol supplementation. This regimen allows transgender women to breastfeed without developing male secondary sex characteristics incongruent with their gender identity
Table 1 Hormone profile at different time points.
Time Point
Estradiol (pg/mL)
Progesterone (ng/mL)
Testosterone (ng/mL)
Prolactin (ng/mL)
1
114
1.1
0.36
2
130
1.1
0.05
9
3
30
1.3
0.06
152
4
39
5
29
1.4
0.89
184
6
51
0.16
59
Unnithan, Elson, & Shenker (2020)
Unnithan, R., Elson, D. F., & Shenker, Y. (2020). Galactorrhea and Hyperprolactinemia in a Transgender Female. Journal of the Endocrine Society, 4(Suppl 1), A899–A899 (abstract no. SUN-043). [Google Scholar] [PubMed Central] [DOI:10.1210/jendso/bvaa046.1781] [PDF]:
Background: Galactorrhea is a rare manifestation of hyper-prolactinemia in males and post-menopausal females, however the hormonal milieu of the transgender female may increase its incidence
Clinical Case: A 43 year old transgender female presented with three years of bilateral breast discharge. She had chronic, stable headaches and fatigue, but no vision changes or other symptoms. Notably, she had breast augmentation surgery with saline breast implants placed shortly before the galactorrhea commenced. She was on a stable dose of estradiol tablets 1 mg twice daily for six years. On physical exam she had pronounced bilateral breast discharge of a milky quality with nipple compression. Prolactin levels were checked several times and were 40-50 ng/mL, TSH was 2.36 uIU/mL. An MRI showed a left inferior pituitary lesion measuring 6 mm x 3 mm x 5 mm with no mass effect on adjacent structures. Her breast discharge was not bothersome to her, and her pituitary lesion was small. It was unclear whether there was a relationship between her prolactin levels and the lesion seen on MRI, as we expected more pronounced prolactin elevation with a prolactinoma. Instead, given the timing of her symptoms in relation to her breast augmentation surgery, her galactorrhea and hyper-prolactinemia were thought to be the result of nipple irritation related to her breast implants combined with a hyper-estrogenemic state.
Clinical Lessons: In the setting of a prolactin secreting micro-adenoma, galactorrhea in a male is highly unusual. This case highlights the importance of recognizing that the unique medical and surgical characteristics of male to female transgender patients can lead to hyper-prolactinemia and galactorrhea.
Reference: Reisman T, Goldstein Z. Case report: induced lactation in a transgender woman. Transgender Health. 2018;3(1):24-26.
Wamboldt, Shuster, & Sidhu (2021)
Wamboldt, R., Shuster, S., & Sidhu, B. S. (2021). Lactation Induction in a Transgender Woman Wanting to Breastfeed: Case Report. The Journal of Clinical Endocrinology & Metabolism, 106(5), e2047–e2052. [DOI:10.1210/clinem/dgaa976]:
Context: Breastfeeding is known to have many health and wellness benefits to the mother and infant; however, breastfeeding in trans women has been greatly under-researched.
Objective: To review potential methods of lactation induction in trans women wishing to breastfeed and to review the embryological basis for breastfeeding in trans women.
Design: This article summarizes a case of successful lactation in a trans woman, in which milk production was achieved in just over 1 month.
Setting: This patient was followed in an outpatient endocrinology clinic.
Participant: A single trans woman was followed in our endocrinology clinic for a period of 9 months while she took hormone therapy to help with lactation.
Interventions: Readily available lactation induction protocols for nonpuerpural mothers were reviewed and used to guide hormone therapy selection. Daily dose of progesterone was increased from 100 mg to 200 mg daily. The galactogogue domperidone was started at 10 mg 3 times daily and titrated up to effect. She was encouraged to use an electric pump and to increase her frequency of pumping.
Main outcome measure: Lactation induction.
Results: At one month, she had noticed a significant increase in her breast size and fullness. Her milk supply had increased rapidly, and she was producing up to 3 to 5 ounces of milk per day with manual expression alone.
Conclusions: We report the second case in the medical literature to demonstrate successful breastfeeding in a trans woman through use of hormonal augmentation.
Further Case Reports
Delgado, D., Stellwagen, L., McCune, S., Sejane, K., & Bode, L. (2023). Experience of Induced Lactation in a Transgender Woman: Analysis of Human Milk and a Suggested Protocol. Breastfeeding Medicine, 18(11), 888–893. [DOI:10.1089/bfm.2023.0197]
Weimer, A. K. (2023). Lactation induction in a transgender woman: macronutrient analysis and patient perspectives. Journal of Human Lactation, 39(3), 488–494. [DOI:10.1177/08903344231170559]
van Amesfoort, J. E., Van Mello, N. M., & van Genugten, R. (2024). Lactation induction in a transgender woman: case report and recommendations for clinical practice. International Breastfeeding Journal, 19(1), 18. [DOI:10.1186/s13006-024-00624-1]
Trahair, E. D., Kokosa, S., Weinhold, A., Parnell, H., Dotson, A. B., & Kelley, C. E. (2024). Novel Lactation Induction Protocol for a Transgender Woman Wishing to Breastfeed: A Case Report. Breastfeeding Medicine, online ahead of print. [DOI:10.1089/bfm.2024.0012]
Dr. Christine McGinn
Dr. Christine McGinn is a transgender woman and well-known surgeon in Pennsylvania who performs gender-affirming surgeries for transgender people. When she had children with her cisgender female partner, McGinn induced a hormonal pseudopregnancy in herself and her and her partner breastfed their twins together. This was described in the media, including in books and television. McGinn’s case was never formally published as a case report in the scientific literature however.
The Oprah Winfrey Show (2010)
Terry, J. C. (Director), & Winfrey, O. G. (Presenter). (2010 September 29). The Mom Who “Fathered” Her Own Children, Plus the Cast of Modern Family [Television series episode]. The Oprah Winfrey Show (Season 25, Episode 13). Chicago: Harpo Studios. [URL 1] [URL 2] [URL 3]
Trans (2012)
Arnold, C. (Director), Schoen, M. (Producer), RoseWorks (Firm), & Sex Smart Films (Firm). (2012). Trans [DVD] (1:21:32–1:21:55). [WorldCat] [IMDB] [Amazon Prime Video]
Boylan (2014)
Boylan, J. F. (2014). Dr. Christine McGinn. In Boylan, J. F. Stuck in the Middle with You: A Memoir of Parenting in Three Genders (pp. 223–233). New York: Broadway Books. [Google Scholar] [Google Books 1] [Google Books 2] [WorldCat] [PDF]:
Dr. Christine McGinn is a surgeon, a mother of two, a backup flight surgeon for the space shuttle progarm, and a transgender woman. As a man, she saved her sperm before transition; ten years later she used that sperm to have children with her partner Lisa. The two of them are both biological mothers of their son and daughter, and each mother was able to breast-feed the twins. I sat down with Christine at her office in New Hope, Pennsylvania, on a hot summer day in 2011.
CM: […] Then there’s the scientist in me that knows that there is a difference, there is not a binary, but a gender spectrum. There are chemicals that are different in men and women. And when a transgender woman transitions, we are somewhere in the middle. Especialy having gone through a simulated pregnancy, in order to breast-feed, I felt the changes of those hormones. I felt my milk let down when not only my baby would cry, but a baby on TV would cry, and even, ridiculously, when a door would close and make a squeak.
JFB: You had to induce a false pregnancy in order to breast-feed? Tell me how you did that.
CM: As a doctor, I knew it was possible. I followed the protocol that involves simulating pregnancy with hormones. It’s estrogen and progesterone. My simulation pregnancy was over a month before Lisa delivered—with twins, we were expecting them to be born earlier. That entire month I was just pumping nonstop, every two hours. We had a whole freezer full of milk. And you know, the first couple of weeks it was no good, because it had all of the hormones in it. So we only saved, like, the last week or so. But still, it was a freezer full of milk.
Lisa had no idea about the way breast-feeding takes over your life, because this was her first. It was kind of funny that I went through that on my own, first, weeks before she did. And then it took her a couple of days to actually—for her milk to let down.
The children were so small when they were born. They were only five pounds. At first we had to feed them with a syringe. They were breast-feeding as well, but they weren’t latching that great on either of us.
JFB: What was it like when they finally muckled on to you?
CM: Oh, I can’t even put it in words. I really cannot put it in words. It was—I was just—oh.
JFB: Were you amazed? Were you afraid?
CM: It was heaven. I was afraid. I don’t know, it was uncharted territory. Like, I knew the milk was good. Lisa was a little concerned that it would be like skimmed milk, or something, you know. [Laughs] Like—she’s like, “Is it the same stuff?”
JFB: Is it the same milk?
CM: And she was a little dubious about, like, is this really all right? I think that’s totally natural for a mother, to be concerned.
I will just say that there are things snobody thinks about when two women are both breast-feeding. Like, technical stuff that you don’t think about. When you have a mother and a father, the mother decides when the kids get fed. Right? The father doesn’t, really. Right?
But you know, when you have two women who are filled with pregnancy hormones and have that, like, mother-bear attitude about how things should be done… It was really crazy.
JFB: So did that cause serious conflict between you and Lisa?
CM: Totally not serious conflict, because the most important thing are the babies.
Eden finally latched—I breast-fed her more than Luke. Luke was never really good. Lisa hated breast-feeding. Eventually we decided to stop.
I’m putting on my science hat again—when you decide to stop, there are hormonal issues. The strongest emotion a person can feel in their life comes frm oxytocin, which is the love drug.
JFB: Oxytocin?
CM: That’s what’s responsible for babies’ bonding during breastfeeding. So the baby latches on, breast-feeds, your brain just [makes oozing sounds], just like, oozes this gooey love substance, oxytocin. Fathers are proven to have higher oxytocin before the delivery, and just stroking your child’s head. You know, when the baby—when you smell a newborn’s head, it really—that smell, it’s like—
JFB: I just saw a friend’s newborn on Friday, and I was like, [makes sniffing sound]—
CM: My niece said it best. She came in and smell them, and she was five years old at the time, and she’s like, “They smell like cupcakes.” [Laughs] And it’s universal. When you ask me what that’s like, I can’t describe it, you know, and I’m a huge fan of food and cupcakes and chocolate, and so that’s the closest I can come to it—it’s like chocolate. [Laughs]
JFB: So when you stopped breast-feeding, was it a kind of a mourning, a loss?
CM: Yes. Lisa wanted to stop before I did. The problem is, once a baby gets a nipple, a plastic nipple, it gives more milk. And so they don’t have to work as hard.
It’s a unique situation that two breast-feeders in a relationship would experience, but a mother and father would not.
JFB: So did one of you stop breast-feeding before the other?
CM: Yes, Lisa did.
JFB: Lisa stopped. And how much longer did you keep it up?
CM: Not long, because they got the nipple.
They were both so small. We weren’t all that successful at it. We were so worried about their birth weight, and making sure they got enough with the syringes. There were definitely times where, you know, we both would breast-feed and, man, I will never forget that. Like, three ‘clock in the morning, four o’clock in the morning, in the little cocoon, nursing.
The heat of their body, their naked body on your chest. The amazing thing is, it really does kind of hurt when they really get going, you know. And you just… I don’t know how else to describe it. You feel like the life force is just coming out through you. It’s so powerful. It relieves that pain that you have in your breast. It releases that oxytocin, and it’s just—it’s even.
JFB: Did you ever do that thing where you would fall asleep with the children in the bed, and wake up with the children in the bed beside you?
CM: Yeah.
JFB: I loved that. It’s one of my stnogest memories of being a father. Having gotten up in the middle of the night. And they are so small, but such an incredibly powerful feeling, the two of you together surrounding the child. With us, we also had a dog at the bottom of the bed. [Laughs]
CM: And we have two, and that was also very important to me, too. We have miniature pinschers.
JFB: So how many months along did you stop breast-feeding?
CM: Three months. It was really emotionally painful, and I cried a lot. I was really sad.
I was pretty sure we were not going to have any more kids. So I’m like, “This is it.” It was very sad.
JFB: Is there a moment frm the last year and two months where you think, This is what it’s like to be a mother, this is it?
CM: Yes, immediately. It was hot as Hades outside. It was, like, a million degrees. We had just had the kids. It was like, May or June, and my mom was over, and it was, like, we had all this help, initially, because Lisa and I were just not getting any sleep and it was, like, round-the-clock feedings and the kids were small, and Lucas had an apnea monitor that he had to wear all the time, and it was just really hard. And there was a big thunderstorm, and the power went out.
And so, at this point, they weren’t really latching very well, so we both had to pump, and then feed them with the syringes. So Lisa and I are totally, like, engorged with milk. And the power’s out, and the pumps are electric. Right?
JFB: Right.
CM: So there’s no electricity, it’s hot as hell, we’re worried for the kids. Lisa and I are in pain. We’re both leaking. And it was the weirdest, funniest situation. And my mom’s there. She runs out to the store to get batteries, and you know, she’s just beng a mom. She’s getting everything, running around like an angel. And Lisa and I are in pain we’re miserable. When she finally came back, the batteries wouldn’t work on the pumps—something else was wrong. Lisa and I are dying.
And so, here’s the guy part of me… I get the pump that has the backup battery power and the backup car charger. Like, I got all tech on it. [Laughs] I’m out int he car trying to get the car charger to work on the pump in the pouring rain. And it’s ninety-five degrees out. It’s all wet inside, like, the humidity on the windows.
And I’m just trying to get some kind of relief.
And this stupid pump didn’t work that way, either. We come back in and my mom has candles lit.
And then the electricity comes back on. And we all just laugh and pump and breast-feed. And every one of us is in heaven.
Pfeffer (2017)
Pfeffer, C. A. (2017). Trans Partnerships and Families: Historical Traces and Contemporary Representations. In Pfeffer, C. A. Queering Families: The Postmodern Partnerships of Cisgender Women and Transgender Men (pp. 1–34). New York: Oxford University Press. [Google Scholar] [Google Books] [WorldCat] [DOI:10.1093/acprof:oso/9780199908059.003.0001] [Archive.org]:
Just 2 years later, Winfrey would feature another interview that elicited many of the same audience reactions. In this 2010 episode, lesbian partners Dr. Christine McGinn and Lisa Bortz beamed with joy as they held their infant twins. Again, audience members’ jaws dropped when it was revealed that beautiful Christine was a male-to-female transsexual who used to be a handsome military officer Chris, and that Lisa had given birth to the couple’s biological children using sperm Chris banked prior to gender confirmation surgeries.10 And it was Winfrey’s chin that nearly hit the floor as she watched video of Christine breastfeeding the couples’ children (the episode is referred to online as “The Mom Who Fathered Her Own Children”).
Other Instances
Published
Estrogen plus cyproterone acetate has been reported to produce pregnancy-like breast changes—specifically, lobuloalveolar development of the breasts—in transfeminine people (Kanhai et al., 2000). Accordingly, galactorrhea (spontaneous or excessive lactation) has been reported as a low-incidence side effect (7–14%) of hormone therapy regimens containing estrogen plus cyproterone acetate in transfeminine people (Gooren, Harmsen-Louman, & van Kessel, 1985; Schlatterer et al., 1998; Bazarra-Castro, 2009). It has also been reported at low incidence (6%) for other hormone therapy regimens (Futterweit, 1980). Sudden cessation of hormone therapy regimens including cyproterone acetate has been reported to result in the onset of lactation as well (Levy, Crown, & Reid, 2003).
Unpublished
Many unpublished reports of lactation and breastfeeding in transfeminine people have been described on the web including at the following pages:
Richards, A. (2003). Lactation and the Transsexual Woman. Second Type Woman. [Updated August 2018] [URL] [PDF]
MacDonald, T. (2013). Trans Women and Breastfeeding: A Personal Interview. Milk Junkies. [URL]
MacDonald, T. (2013). Trans Women and Breastfeeding: The Health Care Provider. Milk Junkies. [URL]
MacDonald, T. (2017). Jenna’s Breastfeeding Journey: Trans Motherhood. Milk Junkies. [URL]
Burns, K. (2018). Yes, Trans Women Can Breastfeed — Here’s How. them. [URL]
Cisgender Men
Induction of lactation has been reported in cisgender men and is noteworthy:
Geschickter (1945)
Geschickter, C. F. (1945). Endocrine Physiology of the Breast. In Geschickter, C. F. Diseases of the Breast: Diagnosis, Pathology, Treatment, 2nd Edition (pp. 42–81). Philadelphia: J.B. Lippincott. [Google Scholar] [Google Books] [OpenLibrary] [WorldCat] [PDF]:
The results obtained indicate that a lactogenic substance in anterior pituitary extracts may cause mammary secretion in nonpregnant women when they have been previously stimulated with estrogenic hormone but true lactation does not occur. Secretion was also obtained in two adult men with gynecomastia after injections of lactogenic hormone.
Huggins (1949)
Huggins, C. (1949). Endocrine substances in the treatment of cancers. Journal of the American Medical Association, 141(11), 750–754. [DOI:10.1001/jama.1949.02910110002002]:
The administration of estrogen in effective amounts causes testicular atrophy and mammary hypertrophy. Growth of the breasts can be so extensive that lactation may be induced, as illustrated in the following case.
W. N., aged 64, had carcinoma of the prostate with osseous metastases, for which he was treated by a permanent suprapubic cystotomy in 1941. Diethylstilbestrol, 20 mg. daily, was given orally for two years beginning September 1942. In September 1944, 25 mg. (500 international units) of prolactin14 was injected daily for five days, and at the end of this time creamy milk could be expressed from both breasts. Orchiectomy and removal of the cystostomy tube were carried out September 6, when administration of estrogen was discontinued; both incisions healed promptly. Since then the patient has been clinically well but has continued to lactate, a large drop of milk being easily expressed from each breast at frequent intervals.
Huggins & Dao (1954)
Huggins, C., & Dao, T. L. (1954). Lactation induced by luteotrophin in women with mammary cancer. Growth of the breast of the human male following estrogenic treatment. Cancer Research, 14(4), 303–306. [Google Scholar] [PubMed] [URL]:
In the observations to be presented luteotrophin [prolactin] was employed as a stimulus for mammary secretion in patients with cancer of the breast, and the results throw new light on the physiology of women bearing this neoplasm. We shall also describe conditions which resulted in the induction of physiologic maturity in the human male, since knowledge of the action of hormones on the human breast is vague.
The effects of luteotrophin on the breast of women post partum has been extensively investigated, but otherwise few observations have been made in the human. Werner (14) administered a crude pituitary extract containing luteotrophin to eight castrate women 21–35 years of age; lactation was not observed, although in one woman “a few drops of colostrum-like fluid” could be expressed from the breasts. Goldzieher (4) treated menstrual disorders in women with luteotrophin, but mammary secretion was not described by him.
PROCEDURE
Luteotrophin,1 dissolved in physiological saline made slight ly alkaline (pH 9) with sodium hydroxide, was injected subcutaneously in daily amounts of 500 International Units; the solutions were freshly prepared, and the injections were continued for 7 days only.
This series comprised 21 female patients who had dis seminated mammary cancer, and all had been subjected to unilateral mastectomy. There were also three men with advanced prostatic carcinoma who had been treated for thera peutic purposes with oral diethylstilbestrol for 20 months, 2, and 6 years, respectively. There were eight persons without mammary or prostatic cancers who served as controls.
In each case of mammary cancer a biopsy of the breast was obtained for histological purposes, the material being stained with Sudan III.3
OBSERVATIONS
Lactation, when it occurred, was never profuse; it varied from a tiny drop to ca. 0.5 cc. from each breast. Clear colostrum was not observed, and the mammary secretion was always milk, as defined above.
Mammary growth in the human male.—Estrogenic substances had been administered to three men in the treatment of disseminated prostate cancer for many months; after luteotrophin injection two lactated and one did not lactate.
W. N. (reported in brief earlier [5]), age 64, had taken diethylstilbestrol, 20 mg/day, orally for 2 years, after which interval sub-areolar button-like masses of mammary tissue could be palpated bilaterally; luteotrophin was then injected for 5 days, and milk was expressed from the breast on the 6th day. Orchiectomy was then performed, and both luteotrophin and estrogenic substances were discontinued. This man continued to lactate for 7 years when the formation of milk gradually ceased.
In the case of A. W., age 62, diethylstilbestrol (5–15 mg/day) had been ingested for 20 months after bilateral orchiectomy; the breasts became slightly enlarged. Luteotrophin was injected, and lactation occurred on the 7th day. A biopsy of the breast showed moderately well developed mammary ducts and alveoli containing milk. In the case of E. G., age 59, diethylstilbestrol (5 mg/day) was ingested almost continuously for 6 years; this resulted in the development of large pendulous breasts, but no lactation occurred after injections of luteotrophin.
Lactation in humans without cancer.—Luteotrophin was administered to two normal males, age 51 and 59, and to four normal females, age 84–59, and none lactated.
DISCUSSION
It must be emphasized that lactation was not copious in any of the humans when it had been induced by luteotrophin; merely small amounts of milk were obtained. It was apparent, however, from the histological studies of the mammary tissue obtained by biopsy that the secretion of milk in any quantity was a criterion of maturity of mammary epithelium.
In the goat and guinea pig it is known that estrogenic substances can induce mammary ma turity without the intervention of exogenous synergistic steroids. In the experiments of Lewis and Turner (9) diethylstilbestrol was implanted in two castrate male goats; one of these animals failed to lactate, while the other produced a small quantity of milk without luteotrophin injections. They obtained small amounts of milk from a male kid similarly treated. Nelson (10) found that estrone induced mammary growth with, later, lactation in the male guinea pig. Our observations demonstrate that diethylstilbestrol ingested for prolonged periods of time can induce maturity of the breast in certain elderly human males. However, the human male differs from the animals just described in that spontaneous lactation was not observed; the injection of luteotrophin was necessary for milk formation.
The duration of lactation induced by luteo trophin was impressive, since milk commonly persisted for many months—and in one male for 7 years. The mechanism whereby this type of lactation is maintained for such long periods of time is at present unknown; we know that milk continues to be secreted both in the presence of the adrenal glands and in the absence of these structures and the gonads as well. Observations (8) have been made on experimental animals which are analogous to the clinical findings; most dogs with spontaneous mammary cancer possess lactation, and this characteristic persists for many months, at least, despite the removal of the adrenal glands and the ovaries.
SUMMARY
The breast of the human male can be induced to grow to a functionally mature state by the administration of estrogenic substances without additional exogenous steroid synergists. Spontaneous lactation was not observed in these men, but it was induced by luteotrophin.
The formation of milk in any amount by the breast is a criterion of functional maturity of the mammary epithelium. Luteotrophin induced the secretion of small amounts of milk in a group of women with mammary cancer and in a number of healthy women as well, and, in addition, in two human males to whom estrogenic substances had been administered for therapeutic purposes. Lactation did not occur in two normal males.
When lactation was induced in human beings, the secretion often persisted for many months; it lasted for 7 years in one man.
HUGGINS,C. Endocrine Substances in the Treatment of Cancers. J.A.M.A., 141:750–54, 1949.
Brodribb, W., & Academy of Breastfeeding Medicine. (2018). ABM Clinical Protocol #9: Use of galactogogues in initiating or augmenting maternal milk production, second revision 2018. Breastfeeding Medicine, 13(5), 307–314. [DOI:10.1089/bfm.2018.29092.wjb]
MacDonald, T. K. (2019). Lactation care for transgender and non-binary patients: Empowering clients and avoiding aversives. Journal of Human Lactation, 35(2), 223–226. [DOI:10.1177/0890334419830989]
Paynter, M. J. (2019). Medication and Facilitation of Transgender Women’s Lactation. Journal of Human Lactation, 35(2), 239–243. [DOI:10.1177/0890334419829729]
Cazorla-Ortiz, G., Obregón-Guitérrez, N., Rozas-Garcia, M. R., & Goberna-Tricas, J. (2020). Methods and Success Factors of Induced Lactation: A Scoping Review. Journal of Human Lactation, 36(4), 739–749. [DOI:10.1177/0890334420950321]
Ferri, R. L., Rosen-Carole, C. B., Jackson, J., Carreno-Rijo, E., Greenberg, K. B., & Academy of Breastfeeding Medicine. (2020). ABM Clinical Protocol #33: Lactation Care for Lesbian, Gay, Bisexual, Transgender, Queer, Questioning, Plus Patients. Breastfeeding Medicine, 15(5), 284–293. [DOI:10.1089/bfm.2020.29152.rlf]
García-Acosta, J. M., Juan-Valdivia, S., María, R., Fernández-Martínez, A. D., Lorenzo-Rocha, N. D., & Castro-Peraza, M. E. (2020). Trans* Pregnancy and Lactation: A Literature Review from a Nursing Perspective. International Journal of Environmental Research and Public Health, 17(1), 44. [DOI:10.3390/ijerph17010044]
LeCain, M., Fraterrigo, G., & Drake, W. M. (2020). Induced Lactation in a Mother Through Surrogacy With Complete Androgen Insensitivity Syndrome (CAIS). Journal of Human Lactation, 36(4), 791–794. [DOI:10.1177/0890334419888752]
Trautner, E., McCool-Myers, M., & Joyner, A. B. (2020). Knowledge and practice of induction of lactation in trans women among professionals working in trans health. International Breastfeeding Journal, 15(1), 63. [DOI:10.1186/s13006-020-00308-6]
References (Inline Citations)
Bazarra-Castro, M. A. (2009). Etiological aspects, therapy regimes, side effects and treatment satisfaction of transsexual patients. (Doctoral dissertation, Ludwig Maximilian University of Munich.) [DOI:10.5282/edoc.9984] [URN:urn:nbn:de:bvb:19-99840] [PDF]
Delgado, D., Stellwagen, L., McCune, S., Sejane, K., & Bode, L. (2023). Experience of Induced Lactation in a Transgender Woman: Analysis of Human Milk and a Suggested Protocol. Breastfeeding Medicine, 18(11), 888–893. [DOI:10.1089/bfm.2023.0197]
Futterweit, W. (1980). Endocrine management of transsexual. Hormonal profiles of serum prolactin, testosterone, and estradiol. New York State Journal of Medicine, 80(8), 1260–1264. [Google Scholar] [PubMed] [Archive.org] [PDF]
Gooren, L. J., Harmsen-Louman, W., & Kessel, H. (1985). Follow-up of prolactin levels in long-term oestrogen-treated male-to-female transsexuals with regard to prolactinoma induction. Clinical Endocrinology, 22(2), 201–207. [DOI:10.1111/j.1365-2265.1985.tb01081.x]
Greenblatt, R. B. (1972). Inappropriate lactation in men and women. Medical Aspects of Human Sexuality, 6(6), 25–33. [Google Scholar] [Google Books]
Greenblatt, R. B., & Leng, J. J. (1972). Lactation anormale chez l’homme. [Abnormal lactation in males.] Bordeaux Medical, 5(3), 241–243. [Google Scholar] [PubMed]
Kanhai, R. C., Hage, J. J., van Diest, P. J., Bloemena, E., & Mulder, J. W. (2000). Short-Term and Long-Term Histologic Effects of Castration and Estrogen Treatment on Breast Tissue of 14 Male-to-Female Transsexuals in Comparison With Two Chemically Castrated Men. The American Journal of Surgical Pathology, 24(1), 74–80. [DOI:10.1097/00000478-200001000-00009]
Levy, A., Crown, A., & Reid, R. (2003). Endocrine intervention for transsexuals. Clinical Endocrinology, 59(4), 409–418. [DOI:10.1046/j.1365-2265.2003.01821.x]
Neumann, F. V., von Berswordt-Wallrabe, R., Elger, W., Steinbeck, H., Hahn, J. D., & Kramer, M. (1970). Aspects of Androgen-Dependent Events as Studied by Antiandrogens. In Astwood, E. B. (Ed.). Proceedings of the 1969 Laurentian Hormone Conference (Recent Progress in Hormone Research, Volume 26) (pp. 337–410). New York/London: Academic Press. [DOI:10.1016/B978-0-12-571126-5.50013-3]
Schlatterer, K., Yassouridis, A., Werder, K. V., Poland, D., Kemper, J., & Stalla, G. K. (1998). Archives of Sexual Behavior, 27(5), 475–492. [DOI:10.1023/a:1018704630036]
Trahair, E. D., Kokosa, S., Weinhold, A., Parnell, H., Dotson, A. B., & Kelley, C. E. (2024). Novel Lactation Induction Protocol for a Transgender Woman Wishing to Breastfeed: A Case Report. Breastfeeding Medicine, online ahead of print. [DOI:10.1089/bfm.2024.0012]
van Amesfoort, J. E., Van Mello, N. M., & van Genugten, R. (2024). Lactation induction in a transgender woman: case report and recommendations for clinical practice. International Breastfeeding Journal, 19(1), 18. [DOI:10.1186/s13006-024-00624-1]
Weimer, A. K. (2023). Lactation induction in a transgender woman: macronutrient analysis and patient perspectives. Journal of Human Lactation, 39(3), 488–494. [DOI:10.1177/08903344231170559]




















 Figure 5. Meta-analysis of estradiol concentration-time data from cisgender women under EEn alone or EEn/DHPA. Fitted data curves from various studies individually and combined into a single-dose curve over 30 days were generated based on an informal meta-analysis of published estradiol concentration-time data from cisgender women under EEn or EEn/DHPA [17]. […]
Figure 5. Meta-analysis of estradiol concentration-time data from cisgender women under EEn alone or EEn/DHPA. Fitted data curves from various studies individually and combined into a single-dose curve over 30 days were generated based on an informal meta-analysis of published estradiol concentration-time data from cisgender women under EEn or EEn/DHPA [17]. […]












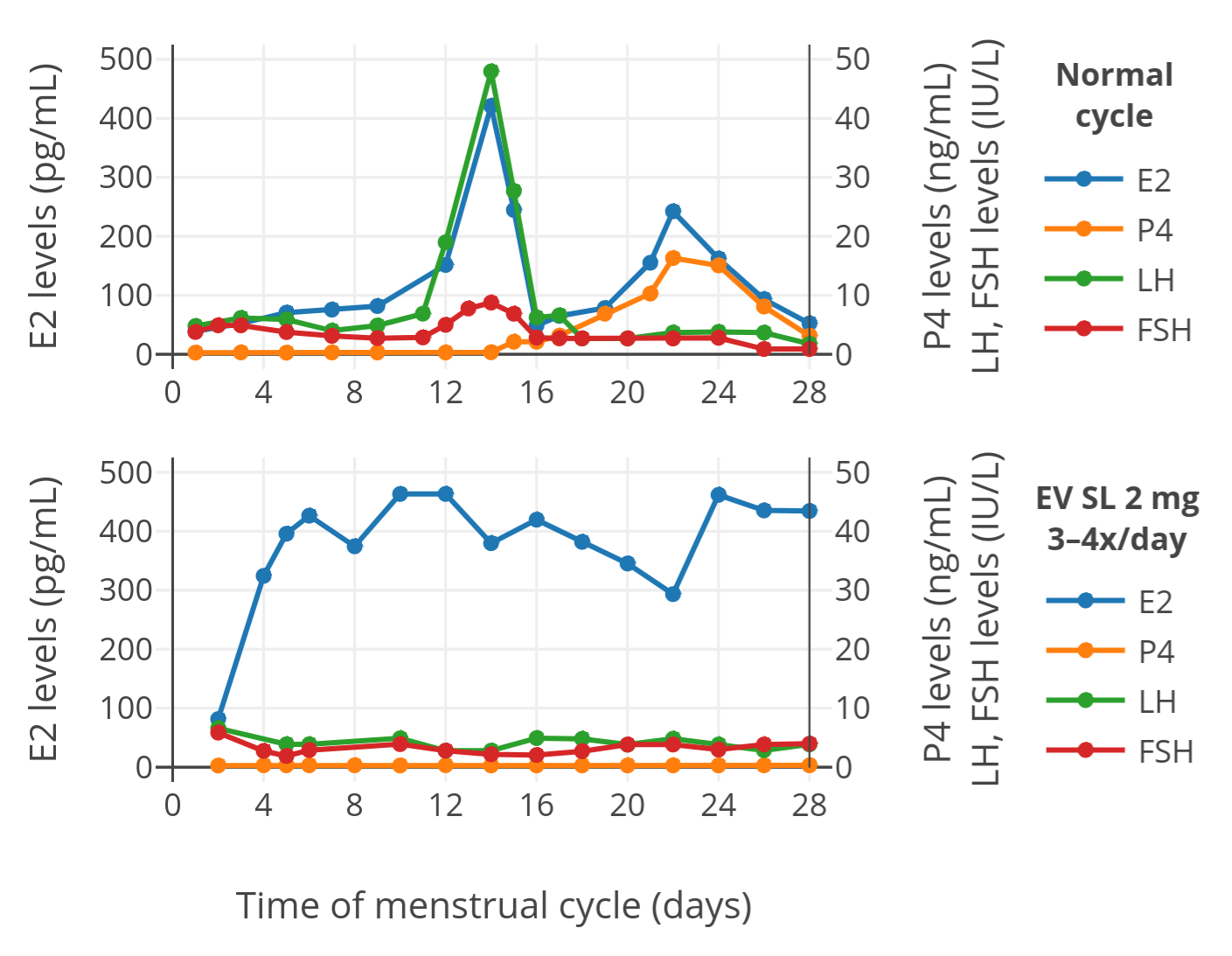

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
_in_postmenopausal_women.png){kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}